Resolving pelvic floor pain-A case report
Posted: September 25, 2015 Filed under: Breathing/respiration, Pain/discomfort, self-healing, stress management, Uncategorized | Tags: biofeedback, Breathing, electromyography, pain, posture, self-regulation, vulvodynia 10 CommentsAdapted from: Martinez Aranda, P. & Peper, E. (2015). The healing of vulvodynia from a client’s perspective. https://biofeedbackhealth.files.wordpress.com/2011/01/a-healing-of-vulvodynia-from-the-client-perspective-2015-06-15.pdf
It’s been a little over a year since I began practicing biofeedback and visualization strategies to overcome vulvodynia. Today, I feel whole, healed, and hopeful. I learned that through controlled and conscious breathing, I could unleash the potential to heal myself from chronic pain. Overcoming pain did not happen overnight; but rather, it was a process where I had to create and maintain healthy lifestyle habits and meditation. Not only am I thankful for having learned strategies to overcome chronic pain, but for acquiring skills that will improve my health for the rest of my life. –-24 year old woman who successfully resolved vulvodynia
Pelvic floor pain can be debilitating, and it is surprisingly common, affecting 10 to 25% of American women. Pelvic floor pain has numerous causes and names. It can be labeled as vulvar vestibulitis, an inflammation of vulvar tissue, interstitial cystitis (chronic pain or tenderness in the bladder), or even lingering or episodic hip, back, or abdominal pain. Chronic pain concentrated at the entrance to the vagina (vulva), is known as vulvodynia. It is commonly under-diagnosed, often inadequately treated, and can go on for months and years (Reed et al., 2007; Mayo Clinic, 2014). The discomfort can be so severe that sitting is uncomfortable and intercourse is impossible because of the extreme pain. The pain can be overwhelming and destructive of the patient’s life. As the participant reported,
I visited a vulvar specialist and he gave me drugs, which did not ease the discomfort. He mentioned surgical removal of the affected tissue as the most effective cure (vestibulectomy). I cried immediately upon leaving the physician’s office. Even though he is an expert on the subject, I felt like I had no psychological support. I was on Gabapentin to reduce pain, and it made me very depressed. I thought to myself: Is my life, as I know it, over?
Physically, I was in pain every single day. Sometimes it was a raging burning sensation, while other times it was more of an uncomfortable sensation. I could not wear my skinny jeans anymore or ride a bike. I became very depressed. I cried most days because I felt old and hopeless instead of feeling like a vibrant 23-year-old woman. The physical pain, combined with my negative feelings, affected my relationship with my boyfriend. We were unable to have sex at all, and because of my depressed status, we could not engage in any kind of fun. (For more details, read the published case report,Vulvodynia treated successfully with breathing biofeedback and integrated stress reduction: A case report).
The four-session holistic biofeedback interventions to successfully resolved vulvodynia included teaching diaphragmatic breathing to transform shallow thoracic breathing into slower diaphragmatic breathing, transforming feelings of powerlessness and hopelessness to empowerment and transforming her beliefs that she could reduce her symptoms and optimize her health. The interventions also incorporated self-healing imagery and posture-changing exercises. The posture changes consisted of developing awareness of the onset of moving into a collapsed posture and use this awareness to shift to an erect/empowered postures (Carney, Cuddy, & Yap, 2010; Peper, 2014; Peper, Booiman, Lin, & Harvey, in press). Finally, this case report build upon the seminal of electromyographic feedback protocol developed by Dr. Howard Glazer (Glazer & Hacad, 2015) and the integrated relaxation protocol developed Dr. David Wise (Wise & Anderson, 2007).
Through initial biofeedback monitoring of the lower abdominal muscle activity, chest, and abdomen breathing patterns, the participant observed that when she felt discomfort or was fearful, her lower abdomen muscles tended to tighten. After learning how to sense this tightness, she was able to remind herself to breathe lower and slower, relax the abdominal wall during inhalation and sit or stand in an erect power posture.
The self-mastery approach for healing is based upon a functional as compared to a structural perspective. The structural perspective implies that the problem can only be fixed by changing the physical structure such as with surgery or medications. The functional perspective assumes that if you can learn to change your dysfunctional psychophysiological patterns the disorder may disappear.
The functional approach assumed that an irritation of the vestibular area might have caused the participant to tighten her lower abdomen and pelvic floor muscles reflexively in a covert defense reaction. In addition, ongoing worry and catastrophic thinking (“I must have surgery, it will never go away, I can never have sex again, my boyfriend will leave me”) also triggered the defense reaction—further tightening of her lower abdomen and pelvic area, shallow breathing, and concurrent increases in sympathetic nervous activation—which together activated the trigger points that lead to increased chronic pain (Banks et al, 1998).
When the participant experienced a sensation or thought/worried about the pain, her body responded in a defense reaction by breathing in her chest and tightening the lower abdominal area as monitored with biofeedback. Anticipation of being monitored increased her shoulder tension, recalling the stressful memory increased lower abdominal muscle tension (pulling in the abdomen for protection), and the breathing became shallow and rapid as shown in Figure 1.
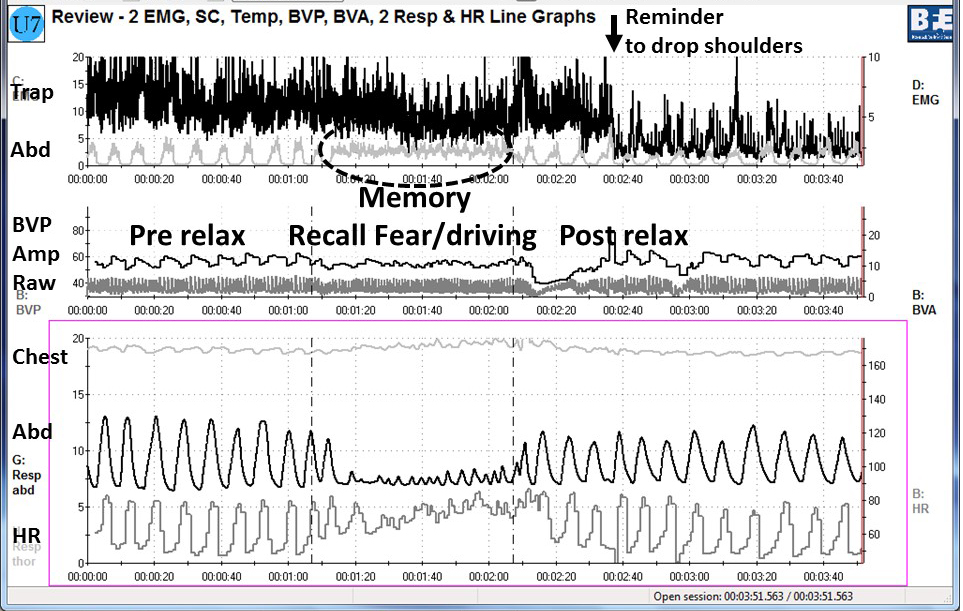
Figure 1. Physiological recording of pre-stressor relaxation, the recall of a fearful driving experience, and a post-stressor relaxation. The scalene to trapezius SEMG increased in anticipation while she recalled the experience, and then initially did not relax (from Peper, Martinez Aranda, & Moss, 2015).
This defense pattern became a conditioned response—initiating intercourse or being touched in the affected area caused the participant to tense and freeze up. She was unaware of these automatic protective patterns, which only worsened her chronic pain.
During the four sessions of training, the participant learned to reverse and interrupt the habitual defense reaction. For example, as she became aware of her breathing patterns she reported,
It was amazing to see on the computer screen the difference between my regular breathing pattern and my diaphragmatic breathing pattern. I could not believe I had been breathing that horribly my whole life, or at least, for who knows how long. My first instinct was to feel sorry for myself. Then, rather than practicing negative patterns and thoughts, I felt happy because I was learning how to breathe properly. My pain decreased from an 8 to alternating between a 0 and 3.
The mastery of slower and lower abdominal breathing within a holistic perspective resulted in the successful resolution of her vulvodynia. An essential component of the training included allowing the participant to feel safe, and creating hope by enabling her to experience a decrease in discomfort while doing a specific practice, and assisting her to master skills to promote self-healing. Instead of feeling powerless and believing that the only resolution was the removal of the affected area (vestibulectomy). The integrated biofeedback protocol offered skill mastery training, to promote self-healing through diaphragmatic breathing, somatic postural changes, reframing internal language, and healing imagery as part of a common sense holistic health approach.
For more details about the case report, download the published study, Peper, E., Martinez Aranda, P., & Moss, E. (2015). Vulvodynia treated successfully with breathing biofeedback and integrated stress reduction: A case report. Biofeedback. 43(2), 103-109.
The participant also wrote up her subjective experience of the integrated biofeedback process in the paper, Martinez Aranda & Peper (2015). Healing of vulvodynia from the client perspective. In this paper she articulated her understanding and experiences in resolving vulvodynia which sheds light on the internal processes that are so often skipped over in published reports.
At the five year follow-up on May 29, 2019, she wrote:
“I am doing very well, and I am very healthy. The vulvodynia symptoms have never come back. It migrated to my stomach a couple of years after, and I still have a sensitive stomach. My stomach has gotten much, much better, though. I don’t really have random pain anymore, now I just have to be watchful and careful of my diet and my exercise, which are all great things!”
References
Banks, S. L., Jacobs, D. W., Gevirtz, R., & Hubbard, D. R. (1998). Effects of autogenic relaxation training on electromyographic activity in active myofascial trigger points. Journal of Musculoskeletal Pain, 6(4), 23-32. https://www.researchgate.net/profile/David_Hubbard/publication/232035243_Effects_of_Autogenic_Relaxation_Training_on_Electromyographic_Activity_in_Active_Myofascial_Trigger_Points/links/5434864a0cf2dc341daf4377.pdf
Carney, D. R., Cuddy, A. J., & Yap, A. J. (2010). Power posing brief nonverbal displays affect neuroendocrine levels and risk tolerance. Psychological Science, 21(10), 1363-1368. Available from: https://www0.gsb.columbia.edu/mygsb/faculty/research/pubfiles/4679/power.poses_.PS_.2010.pdf
Glazer, H. & Hacad, C.R. (2015). The Glazer Protocol: Evidence-Based Medicine Pelvic Floor Muscle (PFM) Surface Electromyography (SEMG). Biofeedback, 40(2), 75-79. http://www.aapb-biofeedback.com/doi/abs/10.5298/1081-5937-40.2.4
Martinez Aranda, P. & Peper, E. (2015). Healing of vulvodynia from the client perspective. Available from: https://biofeedbackhealth.files.wordpress.com/2011/01/a-healing-of-vulvodynia-from-the-client-perspective-2015-06-15.pdf
Mayo Clinic (2014). Diseases and conditions: Vulvodynia. Available at http://www.mayoclinic.org/diseases-conditions/vulvodynia/basics/definition/con-20020326
Peper, E. (2014). Increasing strength and mood by changing posture and sitting habits. Western Edition, pp.10, 12. Available from: http://thewesternedition.com/admin/files/magazines/WE-July-2014.pdf
Peper, E., Booiman, A., Lin, I, M.,& Harvey, R. (in press). Increase strength and mood with posture. Biofeedback.
Peper, E., Martinez Aranda, P., & Moss, E. (2015). Vulvodynia treated successfully with breathing biofeedback and integrated stress reduction: A case report. Biofeedback. 43(2), 103-109. Available from: https://biofeedbackhealth.files.wordpress.com/2011/01/a-vulvodynia-treated-with-biofeedback-published.pdf
Reed, B. D., Haefner, H. K., Sen, A., & Gorenflo, D. W. (2008). Vulvodynia incidence and remission rates among adult women: a 2-year follow-up study. Obstetrics & Gynecology, 112(2, Part 1), 231-237. http://journals.lww.com/greenjournal/Abstract/2008/08000/Vulvodynia_Incidence_and_Remission_Rates_Among.6.aspx
Wise, D., & Anderson, R. U. (2006). A headache in the pelvis: A new understanding and treatment for prostatitis and chronic pelvic pain syndromes. Occidental, CA: National Center for Pelvic Pain Research.http://www.pelvicpainhelp.com/books/
Doctor Mike Evans: What’s the Best Diet? Healthy Eating 101
Posted: September 24, 2015 Filed under: Nutrition/diet, Uncategorized | Tags: diet, exercise, food, health 1 CommentA healthy diet is much more than just focusing on a single food. People focus so often on adding one type of food or eliminating another such as, “Don’t eat ice cream!”, “Eat chia seeds.” “No red meat.” In almost all cases, it is not just one thing, instead a healthy diet is embedded in awareness and healthy life style choices. Watch the superb common sense white board video presentation by Doctor Mike Evans, What’s the Best Diet? Healthy Eating 101. In this short presentation, he summarizes the best practices known. Implement his approach and your health will significantly improve.
