Playful practices to enhance health with biofeedback
Posted: May 4, 2024 Filed under: attention, behavior, biofeedback, Breathing/respiration, computer, Exercise/movement, health, Neck and shoulder discomfort, Pain/discomfort, self-healing, Uncategorized | Tags: exercise, Feldenkrais, pain, Play, somatics 1 CommentAdapted from: Gibney, K.H. & Peper, E. (2003). Exercise or play? Medicine of fun. Biofeedback, 31(2), 14-17.

Homework assignments are sometimes viewed as chore and one more thing to do. Changing the perception from that of work to fun by encouraging laughter and joy often supports the healing process. This blog focusses on utilizing childhood activities and paradoxical movement to help clients release tension patterns and improve range of motion. A strong emphasis is placed on linking diaphragmatic breathing to movement.
When I went home I showed my granddaughter how to be a tree swaying in the wind, she looked at me and said, “Grandma, I learned that in kindergarten!”
‘Betty’ laughed heartily as she relayed this story. Her delight in being able to sway her arms like the limbs of a tree starkly contrasted with her demeanor only a month prior. Betty was referred for biofeedback training after a series of 9 surgeries – wrists, fingers, elbows and shoulders. She arrived at her first session in tears with acute, chronic pain accompanied by frequent, incapacitating spasms in her shoulders and arms. She was unable to abduct her arms more than a few inches without triggering more painful spasms. Her protective bracing and rapid thoracic breathing probably exacerbated her pain and contributed to a limited range of motion of her arms. Unable to work for over a year, she was coping not only with pain, but also with weight gain, poor self-esteem and depression.
The biofeedback training began with effortless, diaphragmatic breathing which is often the foundation of health (Peper and Gibney, 1994). Each thoracic breath added to Betty’s chronic shoulder pain. Convincing Betty to drop her painful bracing pattern and to allow her arms to hang freely from her shoulders as she breathed diaphragmatically was the first major step in regaining mobility. She discovered in that first session that she could use her breathing to achieve control over muscle spasms when she initiated the movement during the exhalation phase of breathing as shown in Figure 1.

Figure 1. Initiate the physical activity after exhaling has begun and body is relaxing especially if the movement or procedure such as an injection would cause pain. Pause the movement when inhaling and then continue the movement again during the exhalation phase. The simple rule is to initiate the activity slightly after beginning exhaling and when the heart rate started to decrease (reproduced with permission from Gorter & Peper, 2012).
During the first week, she practiced her breathing assiduously at home and had fewer spasms. Betty was able to move better during her physical therapy sessions. Each time she felt the onset of muscle spasms she would stop all activity for a moment and ‘go into my trance’ to prevent a recurrence. For the first time in many months, she was feeling optimistic.
Subsequent sessions built upon the foundation of diaphragmatic breathing: boosting Betty’s confidence, increasing range of motion (ROM), and bringing back some fun in life. Activities included many childhood games: tossing a ball, swaying like a tree in the wind, pretending to conduct an orchestra, bouncing on gym balls, playing “Simon Says” (following the movements of the therapist), and dancing. Laughter and childlike joy became a common occurrence. She looked forward to receiving the sparkly star stickers she was given after successful sessions. With each activity, Betty gained more confidence, gradually increased ROM, and began losing weight. Although she had some days where the pain was strong and spasms threatened, Betty reframed the pain as occurring as a result of healing and expanding her ROM—she was no longer a victim of the pain. In addition, her family was proud of her, she was doing more fun activities, and she felt confident that she would return to work.
Betty’s story is similar to other clients whom we have seen. The challenge presented to therapists is to help the client better cope with pain, increase ROM, regain function and, often the most important, to reclaim a “joie de vivre”. Increasing function includes using the minimum amount of effort necessary for the task, allowing unnecessary muscles to remain relaxed (inhibition of dysponesis[i]), and quickly releasing muscle tension when the muscle is no longer required for the activity (work/rest) (Whatmore & Kohli, 1974; Peper et al, 2010; Sella, 2019). The challenge is to perform the task without concurrent evocation of components of the alarm reaction, which tend to be evoked when “we try to do it perfectly,” or “it has to work,” “If I do not do it correctly,” or “I will be judged.” For example, when people learn how to implement micro-breaks (1–2 second rest periods) at the computer, they often sit quietly believing that they are relaxed; however, they may continue a bracing pattern (Peper et al, 2006). Alternatively, tossing a small ball rather than resting at the keyboard will generally evoke laughter, encourage generalization of skills, and covertly induce more relaxation. In some cases, therapists in their desire to help clientss to get well assign structured exercises as homework that evoke striving for performance and boredom—this striving to perform the structured exercises may inhibit healing. Utilizing tools other than those found in the work setting helps the client achieve a broader perspective of the healing/preventive concepts that are taught.
To optimize success, clients are active participants in their own healing process which means that they learn the skills during the therapeutic session and practice at home and at work. Home practices are assigned to integrate the mastery of news skills into daily life. To help clients achieve increased health through physical activity three different approaches are often used: movement reeducation, youthful play, and pure exercise. How the client performs the activity may be monitored with surface electromyography (SEMG) to identify muscles tightening that are not needed for the task and how the muscle relaxes when not needed for the task performance. This monitoring can be done with a portable biofeedback device or multi-channel system when walking or performing the exercises. Clients can even use a single channel SEMG at home.
When working to improve ROM and physical function, explore the following:
- Maintain diaphragmatic breathing – rhythm or tempo may change but the breath must be generated from the diaphragm with emphasis on full exhalation. Use strain gauge feedback and/or SEMG feedback to monitor and train effortless breathing (Peper et al., 2016). Strain gauge feedback is used to teach a slower and diaphragmatic breathing pattern, while SEMG recorded from the scalene to trapezius is used to teach how to reduce shoulder and ancillary muscle tension during inhalation
- Perform activities or stretching/strengthening exercises so slowly that they don’t trigger or aggravate pain during the exhalation phase of breathing.
- Use the minimum amount of tension necessary for the task and let unnecessary muscles remain relaxed. Use SEMG feedback recorded from muscles not needed for the performance of the task to teach clients awareness of inappropriate muscle tension and to learn relaxation of those muscles.
- Release muscle tension immediately when the task is accomplished. Use SEMG feedback to monitor that the muscles are completely relaxed. If rapid relaxation is not achieved, first teach the person to relax the muscles before repeating the muscle activity.
- Perform the exercises as if you have never performed them and do them with a childlike, beginner’s mind, and exploratory attitude (Kabat-Zinn, 1990).
- Create exercises that are totally new and novel so that the participant has no expectancy of outcome can be surprised by their own experience. This approach is part of many somatic educational and therapeutic approaches such as Feldenkrais or Somatics (Hanna, 2004; Feldenkrais, 2009).
Movement and exercise can be taught as pure physical exercise, movement reeducation or youthful playing. Physical exercise is necessary for strength and endurance and at the same time, improves our mood (Thayer, 1996; Mahindru et al., 2023). However, many exercises are considered a burden and are often taught without a sense of lightness and fun, which results in the client thinking in terms that are powerless and helpless (depressive)—“I have to do them.” Helping your clients to understand that exercise is simply a part of every day life, that it encourages healing and improves health, and that they can “cheat” at it, may help them to reframe their attitudes toward it and accomplish their healing goals.
Pure Physical Exercise—Enjoyment through Strength and Flexibility
The major challenge of structured exercises is that the person is very serious and strives too hard to attain the goal. In the process of striving, the body is often held rigid: Breath is shallow and halted and shoulders are slightly braced. Maintaining a daily chart is an excellent tool to show improvement (e.g., more repetitions, more weight, increased flexibility; since, structured exercises are very helpful for improving ROM and strength. When using pure exercise, remember that injured person may have a sense of urgency – they want to get well quickly and, if work stress was a factor in developing pain, they often rush when they need to meet a deadline.
As much as possible make the exercise fun. Help the client understand that he/she can be quick while not rushed. For example, monitor SEMG from an upper trapezius muscle using a portable electromyography. For example, begin by walking slowly. Add a ramp or step to ensure that there is no bracing when climbing (a common occurrence). Walk around the room, down the hall, around the block. Maintain relaxed shoulders, an even swing of the arms, and diaphragmatic breathing. Walk more quickly while emphasizing relaxation with speed rather than rushing. Go faster and faster. Up the stairs. Down the stairs. Walk backward. Skip. Hop. Laugh.
Movement Reeducation – Be ‘Oppositional’ And Do It Differently
Movement reeducation, such as Feldenkrais, Alexander Technique or Hannah Somatics, involves conscious awareness of movement (Alexander, 2001; Hanna, 2004; Murphy, 1993). Many daily patterns of movement become imbedded in our consciousness and, over the years, may include a pain trigger. A common trigger is lifting the shoulders when reaching for the keyboard or mouse, people suffering from thoracic outlet syndrome (TOS) often have such patterns (Peper & Harvey, 2021). A keyboard can often inadvertently cue the client to trigger this dysponetic, and frequently painful, pattern. Have the client do movement reeducation exercises as they are guided through practices in which they have no expectancy and the movements are novel. The focus is on awareness without triggering any fight/flight or startle responses.
Ask the client to explore performing many functional activities with the opposite hand, such as brushing his/her hair or teeth, eating, blowing his/her hair dry, or doing household chores, such as vacuuming. (Explore this for yourself, as well!). Be aware of how much shoulder muscle tension is needed to raise the arms for combing or blow-drying the hair. Explore how little effort is required to hold a fork or knife (you might want to do this in the privacy of your own home!).
Do movements differently such as, practicing alternating hands when leading with the vacuum or when sweeping, changing routes when driving/walking to work or the store, getting out of bed differently. Break up habitual conditioned reflex patterns such as eye, head and hand coordination. For example, slowly rotate your head from left to right and simultaneously shift your eyes in the opposite direction (e.g., turn your head fully to the right while shifting your eyes fully to the left, and then reverse) or before reaching forward, drop your elbows to your sides then, bend your elbows and touch your shoulders with your thumbs then, reach forward. Often, when we change our patterns we increase our flexibility, inhibit bracing and reduce discomfort.
Free Your Neck and Shoulders (adapted from a demonstration by Sharon Keane and developed by Ilana Rubenfeld, 2001)
–Push away from the keyboard and sit at the edge of the chair with your knees bent at right angles and your feet shoulder-width apart and flat on the floor. Do the following movements slowly. Do NOT push yourself if you feel discomfort. Be gentle with yourself.
–Look to the right and gently turn your head and body as far as you can go to the right. When you have gone as far as you can comfortably go, look at the furthest spot on the wall and remember that spot. Gently rotate your head back to center. Close your eyes and relax.
–Reach up with your left hand; pass it over the top of your head and hold on to your right ear. Then, gently bend to the left lowering your elbow towards the floor. Slowly straighten up. Repeat for a few times feeling as if you are a sapling flexing in the breeze. Observe what your body is doing as it bends and comes back up to center. Notice the movements in your ribs, back and neck. Then, drop your arm to your lap and relax. Make sure you continue to breathe diaphragmatically throughout the exercise.
–Reach up with your right hand and pass it over the top of your head and hold on to your left ear. Repeat as above except bending to the right.
–Reach up with your left hand and pass it over the top of your head and hold on to your right ear. Then, look to the left with your eyes and rotate your head to the left as if you are looking behind you. Return to center and repeat the movement a few times. Then, drop your arm to your lap and relax for a few breaths.
–Again, reach over your head with your left hand and hold onto your right ear. Repeat the same rotating motion of your head to the left except that your eyes look to the right. Repeat this a few times then, drop your arm to your lap and relax for a few breaths.
–Reach up with your right hand and pass it over the top of your head and hold on to your left ear. Then, look to the right with your eyes and rotate your head to the right as if you are looking behind you. Return to center and repeat a few times. Then, drop your arm to your lap and relax for a few breaths.
–Again, reach over your head with your right hand and hold onto your left ear. Repeat the same rotating motion of your head to the right except that your eyes look to the left. Repeat this a few times then, drop your arm to your lap and relax for a few breaths.
–Now, look to the right and gently turn your head and body as far as you can go. When you can not go any further, look at that point on the wall. Did you rotate further than at the beginning of the exercise?
–Gently rotate your head back to center, close your eyes, relax and notice the feeling in your neck, shoulders and back.
Youthful Playing – Pavlovian Practice
Evoking positive past memories and actually acting them out may enhance health as is illustrated by the recovery of serious illness of Ivan Pavlov, the discovery of classical conditioning. When Pavlov quietly lay in his hospital bed, many, including his family, thought he was slipping into death. He then ask the nurse to get him a bowl of water with earth in it and the whole night long he gently played with the mud. He recreated the experience when as a child he was playing in mud along a river’s bank. Pavlov knew that evoking the playful joy of childhood would help to encourage mental and physical healing. The mud in hands was the conditioned stimulus to evoke the somatic experience of wellness (Peper, Gibney, & Holt, 2002).
Having clients play can encourage laughter and joie de vivre, which may help in physical healing. Being involved in childhood games and actually playing these games with children removes one from worries and concerns—both past and future—and allows one to be simply in the present. Just being present is associated with playfulness, timelessness, passive attention, creativity and humor. A state in which one’s preconceived mental images and expectancies—the personal, familial, cultural, and healthcare provider’s hypnotic suggestions—are by-passed and for that moment, the present and the future are yet undefined. This is often the opposite of the client’s expectancy; since, remembering the past experiences and the diagnosis creates a fixed mental image that may expect pain and limitation.
Explore some of the following practices as strategies to increase movement and flexibility without effort and to increase joy. Use your creativity and explore your own permutations of the practices. Observe how your mood improves and your energy increases when you play a childhood game instead of an equivalent exercise. For example, instead of dropping your hands to your lap or stretching at the computer terminal during a micro- or meso-break[ii], go over to your coworker and play “pattycake.” This is the game in which you and your partner face each other and then clap your hands and then touch each other’s palms. Do this in all variations of the game.
For increased ROM in the shoulders explore some of the following (remember the basics: diaphragmatic breathing, minimum effort, rapid release) in addition, do the practices to the rhythm of the music that you enjoyed as a young person.
Ball Toss: a hand-sized ball that is easily squeezed is best for this exercise. Monitor respiration patterns, and SEMG forearm extensors and/or flexors, and upper trapezii muscles. Sit quietly in a chair and focus on a relaxed breathing rhythm. Toss the ball in the air with your right hand and catch it with your left hand. As soon as you catch the ball, drop both hands to your lap. Toss the ball back only when you achieve relaxation—both with the empty hand and the hand holding the ball. Watch for over-efforting in the upper trapezii. Begin slowly and increase the pace as you train yourself to quickly release unnecessary muscle tension. Go faster and faster (just about everyone begins to laugh, especially each time they drop the ball).
Ball Squeeze/Toss: Expand upon the above by squeezing the ball prior to tossing. When working with a client, call out different degrees of pressure (e.g., 50%, 10%, 80%, etc.). The same rules apply as with the ball toss.
Ball Hand to Hand: Close your eyes and hand the ball back and forth. Go faster and faster and add ball squeezes prior to passing the ball.
Gym Ball Bounces: Sit on a gym ball and find your balance. Begin bouncing slowly up and down. Reach up and lower your left then, right hand. Abduct your arms forward then, laterally. Turn on the radio and bounce to music.
Simon Says: This can be done standing, sitting in a chair or on a gym ball. When on a gym ball, bounce during the game. Have your client do a mirror image of your movements: reaching up, down, left, right, forward or backward. Touch your head, nose, knees or belly. Have fun and go more quickly.
Back-To-Back Massage: With a partner, stand back-to-back. Lean against each other’s back so that you provide mutual support. Then each rub your back against each other’s back. Enjoy the wiggling movement and stimulation. Be sure to continue to breathe.
Summary: An Attitude of Fun
In summary, it is not what you do; it is also the attitude by which you do it that affects health. From this perspective,when exercises are performed playfully, flexibility, movement and health are enhanced while discomfort is decreased. Inducing laughter promotes healing and disrupts the automatic negative hypnotic suggestion/self-images of what is expected. The clients begins to live in the present moment and thereby decreases the anticipatory bracing and dysponetic activity triggered by striving. By decreasing striving and concern for results, clients may allow themselves to perform the practices with a passive attentive attitude that may facilitate healing. For that moment, the client forgets the painful past and a future expectances that are fraught with promises of continued pain and inactivity. At moment, the pain cycle is interrupted which provides hope for a healthier future.
References
Alexander, F.M. (2001). The Use of the Self. London: Orion Publishing. https://www.amazon.com/Use-Self-F-M-Alexander/dp/0752843915
Feldenkrais, M. (2009). Awareness Through Movement Easy-to-Do Health Exercises to Improve Your Posture, Vision, Imagination, and Personal Awareness. New York: HarperOne. https://www.amazon.com/Awareness-Through-Movement-Easy-Do/dp/0062503227
Gibney, K.H. & Peper, E. (2003). Exercise or play? Medicine of fun. Biofeedback, 31(2), 14-17. https://www.researchgate.net/publication/380317304_EXERCISE_OR_PLAY_MEDICINE_OF_FUN
Gorter, R. & Peper, E. (2012). Fighting Cancer- A Nontoxic Approach to Treatment. Berkeley: North Atlantic Books. https://www.amazon.com/Fighting-Cancer-Nontoxic-Approach-Treatment/dp/1583942483
Hanna, T. (2004). Somatics: Reawakening The Mind’s Control Of Movement, Flexibility, And Health. Da Capo Press. https://www.amazon.com/Somatics-Reawakening-Control-Movement-Flexibility/dp/0738209570
Kabat-Zinn, J. (1990). Full catastrophe living. New York: Delacorte Press.
Mahindru, A., Patil, P., & Agrawal, V. (2023). Role of Physical Activity on Mental Health and Well-Being: A Review. Cureus, I5(1), e33475. https://doi.org/10.7759/cureus.33475
Murphy, M. (1993). The future of the body. New York: Jeremy P. Tarcher/Perigee. https://www.amazon.com/Future-Body-Explorations-Further-Evolution/dp/0874777305
Peper, E., Booiman, A., Lin, I-M, Harvey, R., & Mitose, J. (2016). Abdominal SEMG Feedback for Diaphragmatic Breathing: A Methodological Note. Biofeedback. 44(1), 42-49. https://www.researchgate.net/publication/300365890_Abdominal_SEMG_Feedback_for_Diaphragmatic_Breathing_A_Methodological_Note
Peper, E., Booiman, A., Tallard, M., & Takebayashi, N. (2010). Surface electromyographic biofeedback to optimize performance in daily life: Improving physical fitness and health at the worksite. Japanese Journal of Biofeedback Research, 37(1), 19-28. https://doi.org/10.20595/jjbf.37.1_19
Peper, E., Gibney, K. & Holt, C. (2002). Make health happen: Training yourself to create wellness. Dubuque, IA: Kendall-Hunt. https://he.kendallhunt.com/product/make-health-happen-training-yourself-create-wellness
Peper, E. & Harvey, R. (2021). Causes of TechStress and ‘Technology-Associated Overuse’ Syndrome and Solutions for Reducing Screen Fatigue, Neck and Shoulder Pain, and Screen Addiction. Townsend Letter-The examiner of Alternative Medicine, Oct 28, 2021. https://www.townsendletter.com/article/459-techstress-how-technology-is-hurting-us
Peper, E., Harvey, R. & Tylova, H. (2006). Stress protocol for assessing computer related disorders. Biofeedback. 34(2), 57-62. https://www.researchgate.net/publication/242549995_FEATURE_Stress_Protocol_for_Assessing_Computer-Related_Disorders
Peper, E. & Tibbetts, V. (1994). Effortless diaphragmatic breathing. Physical Therapy Products. 6(2), 67-71. Also in: Electromyography: Applications in Physical Therapy. Montreal: Thought Technology Ltd. https://www.bfe.org/protocol/pro10eng.htm
Rubenfeld, I. (2001). The listening hands: Self-healing through Rubenfeld Synergy method of talk and touch. New York: Random House. https://www.amazon.com/Listening-Hand-Self-Healing-Through-Rubenfeld/dp/0553379836
Sella, G. E. (2019). Surface EMG (SEMG): A Synopsis. Biofeedback, 47(2), 36–43. https://doi.org/10.5298/1081-5937-47.1.05
Thayer, R.E. (1996). The origin of everyday moods—Managing energy, tension, and stress. New York: Oxford University Press. https://www.amazon.com/Origin-Everyday-Moods-Managing-Tension/dp/0195118057
Whatmore, G. and Kohli, D. The Physiopathology and Treatment of Functional Disorders. New York: Grune and Stratton, 1974. https://www.amazon.com/physiopathology-treatment-functional-disorders-biofeedback/dp/0808908510
[i] Dysponesis involves misplaced muscle activities or efforts that are usually covert and do not add functionally to the movement. From: Dys” meaning bad, faulty or wrong, and “ponos” meaning effort, work or energy (Whatmore and Kohli, 1974)
[ii] A meso-break is a 10 to 90 second break that consists of a change in work position, movement or a structured activity such as stretching that automatically relaxes those muscles that were previously activated while performing a task.
Is mindfulness training old wine in new bottles?
Posted: January 11, 2024 Filed under: attention, behavior, biofeedback, Breathing/respiration, CBT, cognitive behavior therapy, healing, health, meditation, self-healing, stress management | Tags: anxiety, autogenic training, biofeedback, health, meditation, mental-health, mindfulness, pain, passive attention, progressive muscle relaxation, wellness, yoga 2 CommentsAdapted from: Peper, E., Harvey, R., & Lin, I-M. (2019). Mindfulness training has themes common to other technique. Biofeedback. 47(3), 50-57. https://doi.org/10.5298/1081-5937-47.3.02
This extensive blog discusses the benefits of mindfulness-based meditation (MM) techniques and explores how similar beneficial outcomes occur with other mind-centered practices such as transcendental meditation, and body-centered practices such as progressive muscle relaxation (PMR), autogenic training (AT), and yoga. For example, many standardized mind-body techniques such as mindfulness-based stress reduction and mindfulness-based cognitive therapy (a) are associated with a reduction in symptoms of symptoms such as anxiety, pain and depression. This article explores the efficacy of mindfulness based techniques to that of other self-regulation techniques and identifies components shared between mindfulness based techniques and several previous self-regulation techniques, including PMR, AT, and transcendental meditation. The authors conclude that most of the commonly used self-regulation strategies have comparable efficacy and share many elements.
Mindfulness-based strategies are based in ancient Buddhist practices and have found acceptance as one of the major contemporary behavioral medicine techniques (Hilton et al, 2016; Khazan, 2013). Throughout this blog the term mindfulness will refer broadly to a mental state of paying total attention to the present moment, with a non-judgmental awareness of the inner and/ or outer experiences (Baer et al., 2004; Kabat-Zinn, 1994).
In 1979, Jon Kabat-Zinn introduced a manual for a standardized Mindfulness-Based Stress Reduction (MBSR) program at the University of Massachusetts Medical Center (Kabat-Zinn, 1994, 2003). The eight-week program combined mindfulness as a form of insight meditation with specific types of yoga breathing and movements exercises designed to focus on awareness of the mind and body, as well as thoughts, feelings, and behaviors.
There is a substantial body of evidence that mindfulness-based cognitive therapy (MBCT); Teasdale et al., 1995) and mindfulness-based stress reduction (MBSR) (Kabat-Zinn, 1994, 2003) have combined with skills of cognitive therapy for ameliorating stress symptoms such as negative thinking, anxiety and depression. For example, MBSR and MBCT has been confirmed to be clinical beneficial in alleviating a variety of mental and physical conditions, for people dealing with anxiety, depression, cancer-related pain and anxiety, pain disorder, or high blood pressure (The following are only a few of the hundred studies published: Andersen et al., 2013; Carlson et al., 2003; Fjorback et al., 2011; Greeson, & Eisenlohr-Moul, 2014; Hoffman et al., 2012; Marchand, 2012; Baer, 2015; Demarzo et al., 2015; Khoury et al, 2013; Khoury et al, 2015; Chapin et al., 2014; Witek Janusek et al., 2019). Currently, MBSR and MBCT techniques that are more standardized are widely applied in schools, hospitals, companies, prisons, and other environments.
The Relationship Between Mindfulness and Other Self-Regulation Techniques
This section addresses two questions: First, how do mindfulness-based interventions compare in efficacy to older self-regulation techniques? Second, and perhaps more basically, how new and different are mindfulness-based therapies from other self-regulation-oriented practices and therapies?
Is mindfulness more effective than other mind/body body/mind approaches?
Although mindfulness-based meditation (MM) techniques are effective, it does not mean that is is more effective than other traditional meditation or self-regulation approaches. To be able to conclude that MM is superior, it needs to be compared to equivalent well-coached control groups where the participants were taught other approaches such as progressive relaxation, autogenic training, transcendental meditation, or biofeedback training. In these control groups, the participants would be taught by practitioners who were self-experienced and had mastered the skills and not merely received training from a short audio or video clip (Cherkin et al, 2016). The most recent assessment by the National Centere for Complementary and Integrative Health, National Institutes of Health (NCCIH-NIH, 2024) concluded that generally “the effects of mindfulness meditation approaches were no different than those of evidence-based treatments such as cognitive behavioral therapy and exercise especially when they include how to generalize the skills during the day” (NCCIH, 2024). Generalizing the learned skills into daily life contributes to the successful outcome of Autogenic Training, Progressive Relaxation, integrated biofeedback stress management training, or the Quieting Response (Luthe, 1979; Davis et al., 2019; Wilson et al., 2023; Stroebel, 1982).
Unfortunately, there are few studies that compare the effective of mindfulness meditation to other sitting mental techniques such as Autogenic Training, Transcendental Meditation or similar meditative practices that are used therapeutically. When the few randomized control studies of MBSR versus autogenic training (AT) was done, no conclusions could be drawn as to the superior stress reduction technique among German medical students (Kuhlmann et al., 2016).
Interestingly, Tanner, et al (2009) in a waitlist study of students in Washington, D.C. area universities practicing TM used the concept of mindfulness, as measured by the Kentucky Inventory of Mindfulness Skills (KIM) (Baer et al, 2004) as a dependent variable, where TM practice resulted in greater degrees of ‘mindfulness.’ More direct comparisons of MM with body-focused techniques, such as progressive relaxation, or Autogenic training mindfulness-based approaches, have not found superior benefit. For example, Agee et al (2009) compared the stress management effects of a five-week Mindfulness Meditation (MM) to a five-week Progressive Muscle Relaxation (PMR) course and found no meaningful reports of superiority of one over the other program; both MM and PMR were effective in reducing symptoms of stress.
In a persuasive meta-analysis comparing MBSR with other similar stress management techniques used among military service members, Crawford, et al (2013) described various multimodal programs for addressing post-traumatic stress disorder (PTSD) and other military or combat-related stress reactions. Of note, Crawford, et al (2013) suggest that all of the multi-modal approaches that include Autogenic Training, Progressive Muscle Relaxation, movement practices including Yoga and Tai Chi, as well as Mindfulness Meditation, and various types of imagery, visualization and prayer-based contemplative practices ALL provide some benefit to service members experiencing PTSD.
An important observation by Crawford et al (2013) pointed out that when military service members had more physical symptoms of stress, the meditative techniques appeared to work best, and when the chief complaints were about cognitive ruminations, the body techniques such as Yoga or Tai Chi worked best to reduce symptoms. Whereas it may not be possible to say that mindfulness meditation practices are clearly superior to other mind-body techniques, it may be possible to raise questions about mechanisms that unite the mind-body approaches used in therapeutic settings.
Could there be negative side effects?
Another point to consider is the limited discussion of the possible absence of benefit or even harms that may be associated with mind-body therapies. For example, for some people, meditation does not promote prosocial behavior (Kreplin et al, 2018). For other people, meditation can evoke negative physical and/or psychological outcomes (Lindahl et al, 2017; Britton et al., 2021). There are other struggles with mind-body techniques when people only find benefit in the presence of a skilled clinician, practitioner, or guru, suggesting a type of psychological dependency or transference, rather than the ability to generalize the benefits outside of a set of conditions (e.g. four to eight weeks of one to four hour trainings) or a particular setting (e.g. in a natural and/or quiet space).
Whereas the detailed instructions for many mindfulness meditation trainings, along with many other types of mind-body practices (e.g. Transcendental Meditation, Autogenic Training, Progressive Muscle Relaxation, Yoga, Tai Chi…) create conditions that are laudable because they are standardized, a question is raised as to ‘critical ingredients’, using the metaphor of baking. The difference between a chocolate and a vanilla cake is not ingredients such as flour, or sugar, etc., which are common to all cakes, but rather the essential or critical ingredient of the chocolate or vanilla flavoring. So what are the essential or critical ingredients in mind-body techniques? Extending the metaphor, Crawford, et al (2013, p. 20) might say the critical ingredient common to the mind-body techniques they studied was that people “can change the way their body and mind react to stress by changing their thoughts, emotions, and behaviors…” with techniques that, relatively speaking, “involve minimal cost and training time.”
The skeptical view suggested here is that MM techniques share similar strategies with other mind-body approaches that encouraging learners to ‘pay attention and shift intention.’ This strategy is part of the instructions when learning Progressive Relaxation, Autogenic Training, Transcendental Meditation, movement meditation of Yoga and Tai Chi and, with instrumented self-regulation techniques such as bio/neurofeedback. In this sense, MM training repackages techniques that have been available for millennia and thus becomes ‘old wine sold in new bottles.’
We wonder if a control group for compassionate mindfulness training would report more benefits if they were asked not only to meditate on compassionate acts, but actually performed compassionate tasks such as taking care of person in pain, helping a homeless person, or actually writing and delivering a letter of gratitude to a person who has helped them in the past? The suggestion is to titrate the effects of MM techniques, moving from a more basic level of benefit to a more fully actualized level of benefit, generalizing their skill beyond a training setting, as measured by the Baer et al (2004) Kentucky Inventory of Mindfulness Skills.
Each generation of clinicians and educators rediscover principles without always recognizing that the similar principles were part of the previous clinical interventions. The analogies and language has changed; however, the underlying concepts may be the same. Mindfulness interventions are now the new, current and popular approach. Some of the underlying ‘mindfulness’ concepts that are shared in common with successfully other mind-body and self-regulation approaches include:
The practitioner must be self-experienced in mindfulness practice. This means that the practitioners do not merely believe the practice is effective; they know it is effective from self-experience. Inner confidence conveyed to clients and patients enhances the healing/placebo effect. It is similar to having sympathy or empathy for clients and patients that occurs from have similar life experiences, such as when a clinician speaks to a patient. For example, a male physician speaking to a female patient who has had a mastectomy may be compassionate; however, empathy occurs more easily when another mastectomy patient (who may also be a physician) shares how she struggled overcame her doubts and can still be loved by her partner.
There may also be a continuum of strengthening beliefs about the benefits of mindfulness techniques that leads to increase benefits for the approach. Knowing there are some kinds of benefits from initiating a practice of mindfulness increases empathy/compassion for others as they learn. Proving that mindfulness techniques are causing benefits after systematically comparing their effectiveness with other approaches strengthens the belief in the mindfulness approaches. Note that a similar process of strengthening one’s belief in an approach occurs gradually, over time as clients and patients progress through beginner, intermediate and advanced levels of mind-body practices.
Observing thoughts without being captured. Being a witness to the thoughts, emotions, and external events results in a type of covert global desensitization and skill mastery of NOT being captured by those thoughts and emotions. This same process of non-attachment and being a witness is one of the underpinnings of techniques that tacitly and sometime covertly support learning ways of controlling attention, such as with Autogenic Training; namely how to passively attend to a specific body part without judgment and, report on the subjective experience without comparison or judgment.
Ongoing daily practice. Participants take an active role in their own healing process as they learn to control and focus their attention. Participants are often asked to practice up to one hour a day and apply the practices during the day as mini-practices or awareness cues to interrupt the dysfunctional behavior. For example in Autogenic training, trainees are taught to practice partial formula (such my “neck and shoulders are heavy”) during the day to bring the body/mind back to balance. While with Progressive Relaxation, the trainee learns to identify when they tighten inappropriate muscles (dysponesis) and then inhibit this observed tension.
Peer support by being in a group. Peer support is a major factor for success as people can share their challenges and successes. Peer support tends to promote acceptance of self-and others and provides role modeling how to cope with stressors. It is possible that some peer support groups may counter the benefits of a mind-body technique, especially when the peers do not provide support or may in fact impede progress when they complain of the obstacles or difficulties in their process.
These concepts are not unique to Mindfulness Meditation (MM) training. Similar instructions have been part of the successful/educational intervention of Progressive Relaxation, Autogenic Training, Yogic practices, and Transcendental Meditation. These approaches have been most successful when the originators, and their initial students, taught their new and evolving techniques to clients and patients; however, they became less successful as later followers and practitioners used these approaches without learning an in-depth skill mastery. For example, Progressive relaxation as taught by Edmund Jacobson consisted of advanced skill mastery by developing subtle awareness of different muscle tension that was taught over 100 sessions (Mackereth & Tomlinson, 2010). It was not simply listening once to a 20-minute audio recording about tightening and relaxing muscles. Similarly, Autogenic training is very specific and teaches passive attention over a three to six-month time-period while the participant practices multiple times daily. Stating the obvious, learning Autogenic Training, Mindfulness, Progressive Relaxation, Bio/Neurofeedback or any other mind-body technique is much more than listening to a 20-minute audio recording.
The same instructions are also part of many movement practices. For many participants focusing on the movement automatically evoked a shift in attention. Their attention is with the task and they are instructed to be present in the movement.
Areas to explore.
Although Mindfulness training with clients and patients has resulted in remarkable beneficial outcomes for the participants, it is not clear whether mindfulness training is better than well taught PR, AT, TM or other mind/body or body/mind approaches. There are also numerous question to explore such as: 1) Who drops out, 2) Is physical exercise to counter sitting disease and complete the alarm reaction more beneficial, and 3) Strategies to cope with wandering attention.
- Who drops out?
We wonder if mindfulness is appropriate for all participants as sometimes participants drop out or experience negative abreactions. It not clear who those participants are. Interestingly, hints for whom the techniques may be challenging can be found in the observations of Autogenic Training that lists specific guidelines for contra-, relative- and non-indications (Luthe, 1970).
- Physical movement to counter sitting disease and complete the alarm reaction.
Although many mindfulness meditation practices may include yoga practices, most participants practice it in a sitting position. It may be possible that for some people somatic movement practices such as a slow Zen walk may quiet the inner dialogue more quickly. In our experience, when participants are upset and highly stressed, it is much easier to let go of agitation by first completing the triggered fight/flight response with vigorous physical activity such as rapidly walking up and downs stairs while focusing on the burning sensations of the thigh muscles. Once the physical stress reaction has been completed and the person feels physically calmer then the mind is quieter. Then have the person begin their meditative practice.
- Strategies to cope with wandering attention.
Some participants have difficulty staying on task, become sleepy, worry, and/or are preoccupied. We observed that first beginning with physical movement practices or Progressive Relaxation appears to be a helpful strategy to reduce wandering thoughts. If one has many active thoughts, progressive relaxation continuously pulls your attention to your body as you are directed to tighten and let go of muscle groups. Being guided supports developing the passive focus of attention to bring awareness back to the task at hand. Once internally quieter, it is easier hold their attention while doing Autogenic Training, breathing or Mindfullness Meditation.
By integrating somatic components with the mindfulness such as done in Progressive Relaxation or yoga practices facilitates the person staying present. Similarly, when teaching slower breathing, if a person has a weight on their abdomen while practicing breathing, it is easier to keep attending to the task: allow the weight to upward when inhaling and feeling the exhalation flowing out through the arms and legs.
Therapeutic and education strategies that implicitly incorporate mindfulness
Progressive relaxation
In the United States during the 1920 progressive relaxation (PR) was developed and taught by Edmund Jacobson (1938). This approach was clinically very successful for numerous illnesses ranging from hypertension, back pain, gastrointestinal discomfort, and anxiety; it included 50 year follow-ups. Patients were active participants and practiced the skills at home and at work and interrupt their dysfunctional patterns during the day such as becoming aware of unnecessary muscle tension (dyponetic activity) and then release the unnecessary muscle tension (Whatmore & Kohli, 1968). This structured approach is totally different than providing an audio recording that guides clients and patients through a series of tightening and relaxing of their muscles. The clinical outcome of PR when taught using the original specific procedures described by Jacobson (1938) was remarkable. The incorporation of Progressive Relaxation as the homework practice was an important cofactor in the successful outcome in the treatment of muscle tension headache using electromyography (EMG) biofeedback by Budzynski, Stoyva and Adler (1970).
Autogenic Training
In 1932 Johannes Schultz in Germany published a book about Autogenic Training describing the basic training procedure. The basic autogenic procedure, the standard exercises, were taught over a minimum period of three month in which the person practiced daily. In this practice they directed theri passive attention to the following cascading sequence: heaviness of their arms, warmth of their arms, heart beat calm and regular, breathing calm and regular or it breathes me, solar plexus is warm, forehead is cool, and I am at peace (Luthe, 1979). Three main principles of autonomic training mentioned by Luthe (1979) are: (1) mental repetition of topographically oriented verbal formulae for brief periods; (2) passive concentration; and (3) reduction of exteroceptive and proprioceptive afferent stimulation. The underlying concepts of Autogenic Therapy include as described by Peper and Williams (1980):
The body has an innate capacity for self-healing and it is this capacity that is allowed to become operative in the autogenic state. Neither the trainer nor trainee has the wisdom necessary to direct the course of the self-balancing process; hence, the capacity is allowed to occur and not be directed.
- Homeostatic self-regulation is encouraged.
- Much of the learning is done by the trainee at home; hence, the responsibility for the training lies primarily with the trainee.
- The trainer/teacher must be self-experience in the practice.
- The attitude necessary for successful practice is one of passive attention; active striving and concern with results impedes the learning process. An attitude of acceptance is cultivated, letting be whatever comes up. This quality of attention is known as “mindfulness’ in meditative traditions.
The clinical outcome for autogenic therapy is very promising. The detailed guided self-awareness training and uncontrolled studies showed benefits across a wide variety of psychosomatic illness such as asthma, cancer, hypertension, anxiety, pain irritable bowel disease, depression (Luthe & Schultz, 1970a; Luthe & Schultz, 1970b). Autogenic training components have also been integrated in biofeedback training. Elmer and Alice Green included the incorporation of autogenic training phrases with temperature biofeedback for the very successful treatment of migraines (Green & Green, 1989). Autonomic training combine with biofeedback in clinical practices produced better results than control group for headache population (Luthe, 1979). Empirical research found that autonomic training was applied efficiently in emotional and behavioral problems, and physical disorder (Klott, 2013), such as skin disorder (Klein & Peper, 2013), insomnia (Bowden et al., 2012), Meniere’s disease (Goto, Nakai, & Ogawa, 2011) and the multitude of stress related symptoms (Wilson et al., 2023).
Bio/neurofeedback training
Starting in the late 1960s, biofeedback procedures have been developed as a successful treatment approach for numerous illnesses ranging from headaches, hypertension, to ADHD (Peper et al., 1979; Peper & Shaffer, 2010; Khazan, 2013). In most cases, the similar instructions that are part of mindfulness meditation are also embedded in the bio/neurofeedback instructions. The participants are instructed to learn control over some physiological parameter and then practice the same skill during daily life. This means that during the learning process, the person learn passive attention and is not be captured by marauding thoughts and feeling. and during the day develop awareness Whenever they become aware of dysfunctional patterns, thoughts, emotions, they initiated their newly learned skill. The ongoing biological feedback signals continuously reminds them to focus.
Transcendental meditation
The next fad to hit the American shore was Transcendental Meditation (TM)– a meditation practice from the ancient Vedic tradition in India. The participant were given a mantra that they mentally repeated and if their attention wanders, they go back to repeating the mantra internally. The first study that captured the media’s attention was by Wallace (1970) published in the Journal Science which reported that “During meditation, oxygen consumption and heart rate decreased, skin resistance increased, and the electroencephalogram showed specific changes in certain frequencies. These results seem to distinguish the state produced by Transcendental Meditation from commonly encountered states of consciousness and suggest that it may have practical applications.” (Wallace, 1970).
The participants were to practice the mantra meditation twice a day for about 20 minutes. Meta-analysis studies have reported that those who practiced TM as compared to the control group experienced significant improved of numerous disorders such as CVD risk factors, anxiety, metabolic syndrome, drug abuse and hypertension (Paul-Labrador et al, 2006; Rainforth et al., 2007; Hawkins, 2003).
To make it more acceptable for the western audience, Herbert Benson, MD, adapted and simplified techniques from TM training and then labelled a core element, the ‘relaxation response’ (Benson et al., 1974) Instead of giving people a secret mantra and part of a spiritual tradition, he recommend using the word “one” as the mantra. Numerous studies have demonstrated that when patients practice the relaxation response, many clinical symptoms were reduced. The empirical research found that practiced transcendental meditation caused increasing prefrontal low alpha power (8-10Hz) and theta power of EEG; as well as higher prefrontal alpha coherence than other locations at both hemispheres. Moreover, some individuals also showed lower sympathetic activation and higher parasympathetic activation, increased respiratory sinus arrhythmic and frontal blood flow, and decreased breathing rate (Travis, 2001, 2014). Although TM and Benson’s relaxation response continues to be practiced, mindfulness has taking it place.
Conclusion
Mindfulness-Based Stress Reduction (MBSR) and Mindfulness-Based Cognitive Therapy (MBCT) are very beneficial and yet may be considered ‘old wine in new bottles’ where the metaphor refers to millennia old meditation techniques as ‘old wine’ and the acronyms such as MBSR or MBCT as ‘new bottles’. Like many other ‘new’ therapeutic approaches or for that matter, many other ‘new’ medications, use it now before it becomes stale and loses part of its placebo power. As long as the application of a new technique is taught with the intensity and dedication of the promotors of the approach, and as long as the participants are required to practice while receiving support, the outcomes will be very beneficial, and most likely similar in effect to other mind-body approaches.
The challenge facing mindfulness practices just as those from Autogenic Training, Progressive Relaxation and Transcendental Meditation, is that familiarity breeds contempt and that clients and therapists are continuously looking for a new technique that promises better outcome. Thus as Mindfulness training is taught to more and more people, it may become less promising. In addition, as mindfulness training is taught in less time, (e.g. fewer minutes and/or fewer sessions), and with less well-trained instructors, who may offer less support and supervision for people experiencing possible negative effects, the overall benefits may decrease. Thus, mindfulness practice, Autogenic training, progressive relaxation, Transcendental Meditation, movement practices, meditation, breathing practices as well as the many spiritual practices all appear to share common fate of fading over time. Whereas the core principles of mind-body techniques are ageless, the execution is not always assured.
References
Agee, J. D., Danoff-Burg, S., & Grant, C. A. (2009). Comparing brief stress management courses in a community sample: Mindfulness skills and progressive muscle relaxation. Explore: The Journal of Science and Healing, 5(2), 104-109. https://doi.org/10.1016/j.explore.2008.12.004
Andersen, S. R., Würtzen, H., Steding-Jessen, M., Christensen, J., Andersen, K. K., Flyger, H., … & Dalton, S. O. (2013). Effect of mindfulness-based stress reduction on sleep quality: Results of a randomized trial among Danish breast cancer patients. Acta Oncologica, 52(2), 336-344. https://doi.org/10.3109/0284186X.2012.745948
Alvarez-Jimenez, M., Gleeson, J. F., Bendall, S., Penn, D. L., Yung, A. R., Ryan, R. M., … Nelson, B. (2018). Enhancing social functioning in young people at Ultra High Risk (UHR) for psychosis: A pilot study of a novel strengths and mindfulness-based online social therapy. Schizophrenia Research, 202, 369-377 https://doi.org/10.1016/j.schres.2018.07.022
Baer, R. A. (2003). Mindfulness training as a clinical intervention: A conceptual and empirical review. Clinical Psychology: Science and Practice, 10, 125–143. https://doi.org/10.1093/clipsy/bpg015
Baer, R. A.. (2015). Mindfulness-based treatment approaches: Clinician’s guide to evidence base and applications. New York: Elsevier. https://www.elsevier.com/books/mindfulness-based-treatment-approaches/baer/978-0-12-416031-6
Baer, R., Smith, G., & Allen, K. (2004). Assessment of mindfulness by self-report: The Kentucky Inventory of Mindfulness Skills. Assessment, 11, 191–206. https://doi.org/10.1177/1073191104268029
Benson, H., Beary, J. F., & Carol, M. P. (1974).The Relaxation Response. Psychiatry, 37(1), 37-46. https://www.tandfonline.com/loi/upsy20
Bowden, A., Lorenc, A., & Robinson, N. (2012). Autogenic Training as a behavioural approach to insomnia: A prospective cohort study. Primary Health Care Research & Development, 13, 175-185. https://doi.org/10.1017/S1463423611000181
Britton, W.B., Lindahl, J.R., Coope, D.J., Canby, N.K., & Palitsky, R. (2021). Defining and Measuring Meditation-Related Adverse Effects in Mindfulness-Based Programs. Clinical Psychological Science, 9(6), 1185-1204. https://doi.org/10.1177/2167702621996340
Budzynski, T., Stoyva, J., & Adler, C. (1970). Feedback-induced muscle relaxation: Application to tension headache. Journal of Behavior Therapy and Experimental Psychiatry, 1(3), 205-211. https://doi.org/10.1016/0005-7916(70)90004-2
Carlson, L. E., Speca, M., Patel, K. D., & Goodey, E. (2003). Mindfulness‐based stress reduction in relation to quality of life, mood, symptoms of stress, and immune parameters in breast and prostate cancer outpatients. Psychosomatic Medicine, 65(4), 571-581. https://doi.org/10.1097/01.psy.0000074003.35911.41
Chapin, H. L., Darnall, B. D., Seppala, E. M., Doty, J. R., Hah, J. M., & Mackey, S. C. (2014). Pilot study of a compassion meditation intervention in chronic pain. J Compassionate Health Care, 1(4), 1-12. https://doi.org/10.1186/s40639-014-0004-x
Cherkin, D. C., Sherman, K. J., Balderson, B. H., Cook, A. J., Anderson, M. L., Hawkes, R. J., … & Turner, J. A. (2016). Effect of mindfulness-based stress reduction vs cognitive behavioral therapy or usual care on back pain and functional limitations in adults with chronic low back pain: A randomized clinical trial. JAMA, 315(12), 1240-1249. https://doi.org/10.1001/jama.2016.2323
Crawford, C., Wallerstedt, D. B., Khorsan, R., Clausen, S. S., Jonas, W. B., & Walter, J. A. (2013). A systematic review of biopsychosocial training programs for the self-management of emotional stress: Potential applications for the military. Evidence-Based Complementary and Alternative Medicine, 747694: 1-23. https://doi.org/10.1155/2013/747694
Davis, M., Eshelman, E.R., & McKay, M. (2019). The Relaxation and Stress Reduction Workbook. Oakland, CA: New Harbinger Publications. https://www.amazon.com/Relaxation-Reduction-Workbook-Harbinger-Self-Help/dp/1684033349
Demarzo, M. M., Montero-Marin, J., Cuijpers, P., Zabaleta-del-Olmo, E., Mahtani, K. R., Vellinga, A., Vincens, C., Lopez del Hoyo, Y., & García-Campayo, J. (2015). The efficacy of mindfulness-based interventions in primary care: A meta-analytic review. The Annals of Family Medicine, 13(6), 573-582. https://doi.org/10.1370/afm.1863
Fjorback, L. O., Arendt, M., Ørnbøl, E., Fink, P., & Walach, H. (2011). Mindfulness‐Based Stress Reduction and Mindfulness‐Based Cognitive Therapy–A systematic review of randomized controlled trials. Acta Psychiatrica Scandinavica, 124(2), 102-119. https://doi.org/10.1111/j.1600-0447.2011.01704.x
Goto, F., Nakai, K., & Ogawa, K. (2011). Application of autogenic training in patients with Meniere disease. European Archives of Oto-Rhino-Laryngology, 268(10), 1431-1435. https://doi.org/10.1007/s00405-011-1530-1
Greeson, J., & Eisenlohr-Moul, T. (2014). Mindfulness-based stress reduction for chronic pain. In R. A. Baer (Ed.), Mindfulness-Based Treatment Approaches: Clinician’s Guide to Evidence Base and Applications, 269-292. San Diego, CA: Academic Press. https://psycnet.apa.org/record/2014-40932-000
Green, E. and Green, A. (1989). Beyond Biofeedback. New York: Knoll. https://www.amazon.com/Beyond-Biofeedback-Elmer-Green/dp/0940267144
Hawkins, M. A. (2003). Effectiveness of the Transcendental Meditation program in criminal rehabilitation and substance abuse recovery. Journal of Offender Rehabilitation, 36(1-4), 47- 65. https://doi.org/10.1300/J076v36n01_03
Hilton, L., Hempel, S., Ewing, B. A., Apaydin, E., Xenakis, L., Newberry, S., …Maglione, M. A. (2016). Mindfulness meditation for chronic pain: Systematic review and meta-analysis. Annals of Behavioral Medicine, 51(2), 199-213. https://doi.org/10.1007/s12160-016-9844-2
Hoffman, C. J., Ersser, S. J., Hopkinson, J. B., Nicholls, P. G., Harrington, J. E., & Thomas, P. W. (2012). Effectiveness of mindfulness-based stress reduction in mood, breast-and endocrine-related quality of life, and well-being in stage 0 to III breast cancer: A randomized, controlled trial. Journal of Clinical Oncology, 30(12), 1335-1342. https://doi.org/10.1200/JCO.2010.34.0331
Jacobson, E. (1938). Progressive relaxation. Chicago, IL: University of Chicago Press. https://www.amazon.com/Progressive-Relaxation-Physiological-Investigation-Significance/dp/0226390594
Kabat-Zinn, J. (1994). Wherever you go, there you are: Mindfulness meditation in everyday life. New York: Hyperion. https://www.amazon.com/Wherever-You-There-Are-Mindfulness/dp/0306832011
Kabat-Zinn, J. (2003). Mindfulness-based stress reduction (MBSR). Constructivism in the Human Sciences, 8, 73–107. https://psycnet.apa.org/record/2004-19791-008
Khazan, I. Z. (2013). The clinical handbook of biofeedback: A step-by-step guide for training and practice with mindfulness. New York: John Wiley & Sons. https://www.amazon.com/Clinical-Handbook-Biofeedback-Step-Step/dp/1119993717
Klein, A., & Peper, E. (2013). There Is hope: Autogenic biofeedback training for the treatment of psoriasis. Biofeedback, 41 (4), 194-201. https://doi.org/10.5298/1081-5937-41.4.01
Khoury, B., Lecomte, T., Fortin, G., Masse, M., Therien, P., Bouchard, V., Chapleau, M., Paquin, K., & Hofmann, S. G. (2013). Mindfulness-based therapy: A comprehensive meta-analysis. Clinical Psychology Review, 33(6), 763-771. https://doi.org/10.1016/j.cpr.2013.05.005
Khoury, B., Sharma, M., Rush, S. E., & Fournier, C. (2015). Mindfulness-based stress reduction for healthy individuals: A meta-analysis. Journal of Psychosomatic Research, 78(6), 519-528.
Klott, O. (2013). Autogenic Training–a self-help technique for children with emotional and behavioural problems. Therapeutic Communities: The International Journal of Therapeutic Communities, 34(4), 152-158. https://doi.org/10.1108/TC-09-2013-0027
Kreplin, U., Farias, M., & Brazil, I. A. (2018). The limited prosocial effects of meditation: A systematic review and meta-analysis. Sci Rep, 8, 2403. https://doi.org/10.1038/s41598-018-20299-z
Kuhlmann, S. M., Huss, M., Bürger, A., & Hammerle, F. (2016). Coping with stress in medical students: results of a randomized controlled trial using a mindfulness-based stress prevention training (MediMind) in Germany. BMC Medical Education, 16(1), 316. https://doi.org/10.1186/s12909-016-0833-8
Lindahl, J. R., Fisher, N. E., Cooper, D. J., Rosen, R. K, & Britton, W. B. (2017). The varieties of contemplative experience: A mixed-methods study of meditation-related challenges in Western Buddhists. PLoSONE, 12(5): e0176239. https://doi.org/10.1371/journal.pone.0176239
Luthe, W. (1970). Autogenic therapy: Research and theory. New York: Grune and Stratton. https://www.cambridge.org/core/journals/the-british-journal-of-psychiatry/article/abs/autogenic-therapy-edited-by-wolfgang-luthe-volume-4-research-and-theory-by-wolfgang-luthe-grune-and-stratton-new-york-1970-pp-276-price-1475/6C8521C36C37254A08AAD1F2FE08211C
Luthe, W. (1979). About the Methods of Autogenic Therapy. In: Peper, E., Ancoli, S., Quinn, M. (eds). Mind/Body Integration. Springer, Boston, MA. https://doi.org/10.1007/978-1-4613-2898-8_12
Luthe, W. & Schultz, J. H. (1970a). Autogenic therapy: Medical applications. New York: Grune and Stratton. https://www.amazon.com/Autogenic-Therapy-II-Medical-Applications/dp/B001J9W7L6
Luthe, W. & Schultz, J. H. (1970b). Autogenic therapy: Applications in psychotherapy. New York: Grune and Stratton. https://www.amazon.com/Autogenic-Therapy-Applications-Psychotherapy-v/dp/0808902725
Mackereth, P.A. & Tomlinson, L. (2010). Progressive muscle relaxation. In Cawthorn, A. & Mackereth, P.A. eds. Integrative Hypnotherapy. London: Churchill Livingstone. https://www.amazon.com/Integrative-Hypnotherapy-Complementary-approaches-clinical/dp/0702030821
Marchand, W. R. (2012). Mindfulness-based stress reduction, mindfulness-based cognitive therapy, and Zen meditation for depression, anxiety, pain, and psychological distress. Journal of Psychiatric Practice, 18(4), 233-252. https://doi.org/10.1097/01.pra.0000416014.53215.86
NCCIH (2024). Meditation and Mindfulness: What You Need To Know. National Center for Complementary and Integrative Health, National Institutes of Health. Accessed January 31, 2024. https://www.nccih.nih.gov/health/meditation-and-mindfulness-what-you-need-to-know?
Paul-Labrador, M., Polk, D., Dwyer, J.H. et al. (2006). Effects of a randomized controlled trial of Transcendental Meditation on components of the metabolic syndrome in subjects with coronary heart disease. Archive of Internal Medicine, 166(11), 1218-1224. https://doi.org/10.1001/archinte.166.11.1218
Peper, E., Ancoli, S. & Quinn, M. (Eds). (1979). Mind/Body Integration: Essential Readings in Biofeedback. New York: Plenum. https://www.amazon.com/Mind-Body-Integration-Essential-Biofeedback/dp/0306401029
Peper, E. & Shaffer, F. (2010). Biofeedback History: An Alternative View. Biofeedback, 38 (4): 142–147. https://doi.org/10.5298/1081-5937-38.4.03
Peper, E., & Williams, E.A. (1980). Autogenic therapy. In A. C. Hastings, J. Fadiman, & J. S. Gordon (Eds.), Health for the whole person (pp137-141).. Boulder: Westview Press. https://biofeedbackhealth.files.wordpress.com/2016/02/autogenic-therapy-peper-and-williams.pdf
Rainforth, M.V., Schneider, R.H., Nidich, S.I., Gaylord-King, C., Salerno, J.W., & Anderson, J.W. (2007). Stress reduction programs in patients with elevated blood pressure: A systematic review and meta-analysis. Current Hypertension Reports, 9(6), 520–528. https://doi.org/10.1007/s11906-007-0094-3
Stroebel, C. (1982). QR: The Quieting Reflex. New York: Putnam Pub Group. https://www.amazon.com/Qr-Quieting-Charles-M-D-Stroebel/dp/0399126570
Tanner, M. A., Travis, F., Gaylord‐King, C., Haaga, D. A. F., Grosswald, S., & Schneider, R. H. (2009). The effects of the transcendental meditation program on mindfulness. Journal of Clinical Psychology 65(6), 574-589. https://doi.org/10.1002/jclp.20544
Teasdale, J. D., Segal, Z., & Williams, J. M. (1995). How does cognitive therapy prevent depressive relapse and why should attentional control (mindfulness) training help? Behaviour Research and Therapy, 33, 25–39. https://doi.org/10.1016/0005-7967(94)e0011-7
Travis, F. (2001). Autonomic and EEG patterns distinguish transcending from other experiences during transcendental meditation practice. International Journal of Psychophysiology, 42, 1–9. https://doi.org/10.1016/s0167-8760(01)00143-x
Travis, F. (2014). Transcendental experiences during meditation practice. Annals of the New York Academy of Sciences, 1307, 1–8. https://doi.og10.1111/nyas.12316
Wallace, K.W. (1970). Physiological Effects of Transcendental Meditation. Science, 167 (3926), 1751-1754. https://doi.org/10.1126/science.167.3926.1751
Whatmore, G. B., & Kohli, D. R. (1968). Dysponesis: A neurophysiologic factor in functional disorders. Behavioral Science, 13(2), 102–124. https://doi.org/10.1002/bs.3830130203
Wilson, V., Somers, K. & Peper, E. (2023). Differentiating Successful from Less Successful Males and Females in a Group Relaxation/Biofeedback Stress Management Program. Biofeedback, 51(3), 53–67. https://doi.org/10.5298/608570
Witek Janusek, L., Tel,l D., & Mathews, H.L. (2019). Mindfulness based stress reduction provides psychological benefit and restores immune function of women newly diagnosed with breast cancer: A randomized trial with active control. Brain Behav Immun, 80:358-373. https://doi.org/10.1016/j.bbi.2019.04.012
Reduce anxiety
Posted: March 23, 2022 Filed under: behavior, Breathing/respiration, CBT, cognitive behavior therapy, digital devices, education, emotions, health, mindfulness, posture, relaxation, self-healing, stress management | Tags: anxiety, concentration, insomnia, menstrual cramps, pain 3 Comments
The purpose of this blog is to describe how a university class that incorporated structured self-experience practices reduced self-reported anxiety symptoms (Peper, Harvey, Cuellar, & Membrila, 2022). This approach is different from a clinical treatment approach as it focused on empowerment and mastery learning (Peper, Miceli, & Harvey, 2016).
As a result of my practice, I felt my anxiety and my menstrual cramps decrease. — College senior
When I changed back to slower diaphragmatic breathin, I was more aware of my negative emotions and I was able to reduce the stress and anxiety I was feeling with the deep diaphragmatic breathing.– College junior
Background
More than half of college students now report anxiety (Coakley et al., 2021). In our recent survey during the first day of the spring semester class, 59% of the students reported feeling tired, dreading their day, being distracted, lacking mental clarity and had difficulty concentrating.
Before the COVID pandemic nearly one-third of students had or developed moderate or severe anxiety or depression while being at college (Adams et al., 2021. The pandemic accelerated a trend of increasing anxiety that was already occurring. “The prevalence of major depressive disorder among graduate and professional students is two times higher in 2020 compared to 2019 and the prevalence of generalized anxiety disorder is 1.5 times higher than in 2019” As reported by Chirikov et al (2020) from the UC Berkeley SERU Consortium Reports.
This increase in anxiety has both short and long term performance and health consequences. Severe anxiety reduces cognitive functioning and is a risk factor for early dementia (Bierman et al., 2005; Richmond-Rakerd et al, 2022). It also increases the risk for asthma, arthritis, back/neck problems, chronic headache, diabetes, heart disease, hypertension, pain, obesity and ulcer (Bhattacharya et al., 2014; Kang et al, 2017).
The most commonly used treatment for anxiety are pharmaceutical and cognitive behavior therapy (CBT) (Kaczkurkin & Foa, 2015). The anti-anxiety drugs are usually benzodiazepines (e.g., alprazolam (Xanax), clonazepam (Klonopin), chlordiazepoxide (Librium), diazepam (Valium) and lorazepam (Ativan). Although these drugs they may reduce anxiety, they have numerous side effects such as drowsiness, irritability, dizziness, memory and attention problems, and physical dependence (Shri, 2012; Crane, 2013).
Cognitive behavior therapy techniques based upon the assumption that anxiety is primarily a disorder in thinking which then causes the symptoms and behaviors associated with anxiety. Thus, the primary treatment intervention focuses on changing thoughts.
Given the significant increase in anxiety and the potential long term negative health risks, there is need to provide educational strategies to empower students to prevent and reduce their anxiety. A holistic approach is one that assumes that body and mind are one and that soma/body, emotions and thoughts interchangeably affect the development of anxiety. Initially in our research, Peper, Lin, Harvey & Perez (2017) reported that it was easier to access hopeless, helpless, powerless and defeated memories in a slouched position than an upright position and it was easier to access empowering positive memories in an upright position than a slouched position. Our research on transforming hopeless, helpless, depressive thought to empowering thoughts, Peper, Harvey & Hamiel (2019) found that it was much more effective if the person first shifts to an upright posture, then begins slow diaphragmatic breathing and finally reframes their negative to empowering/positive thoughts. Participants were able to reframe stressful memories much more easily when in an upright posture compared to a slouched posture and reported a significant reduction in negative thoughts, anxiety (they also reported a significant decrease in negative thoughts, anxiety and tension as compared to those attempting to just change their thoughts).
The strategies to reduce anxiety focus on breathing and posture change. At the same time there are many other factors that may contribute the onset or maintenance of anxiety such as social isolation, economic insecurity, etc. In addition, low glucose levels can increase irritability and may lower the threshold of experiencing anxiety or impulsive behavior (Barr, Peper, & Swatzyna, 2019; Brad et al, 2014). This is often labeled as being “hangry” (MacCormack & Lindquist, 2019). Thus, by changing a high glycemic diet to a low glycemic diet may reduce the somatic discomfort (which can be interpreted as anxiety) triggered by low glucose levels. In addition, people are also sitting more and more in front of screens. In this position, they tend to breathe quicker and more shallowly in their chest.
Shallow rapid breathing tends to reduce pCO2 and contributes to subclinical hyperventilation which could be experienced as anxiety (Lum, 1981; Wilhelm et al., 2001; Du Pasquier et al, 2020). Experimentally, the feeling of anxiety can rapidly be evoked by instructing a person to sequentially exhale about 70 % of the inhaled air continuously for 30 seconds. After 30 seconds, most participants reported a significant increase in anxiety (Peper & MacHose, 1993). Thus, the combination of sitting, shallow breathing and increased stress from the pandemic are all cofactors that may contribute to the self-reported increase in anxiety.
To reduce anxiety and discomfort, McGrady and Moss (2013) suggested that self-regulation and stress management approaches be offered as the initial treatment/teaching strategy in health care instead of medication. One of the useful approaches to reduce sympathetic arousal and optimize health is breathing awareness and retraining (Gilbert, 2003).
Stress management as part of a university holistic health class
Every semester since 1976, up to 180 undergraduates have enrolled in a three-unit Holistic Health class on stress management and self-healing (Klein & Peper, 2013). Students in the class are assigned self-healing projects using techniques that focus on awareness of stress, dynamic regeneration, stress reduction imagery for healing, and other behavioral change techniques adapted from the book, Make Health Happen (Peper, Gibney & Holt, 2002).
82% of students self-reported that they were ‘mostly successful’ in achieving their self-healing goals. Students have consistently reported achieving positive benefits such as increasing physical fitness, changing diets, reducing depression, anxiety, and pain, eliminating eczema, and even reducing substance abuse (Peper et al., 2003; Bier et al., 2005; Peper et al., 2014).
This assessment reports how students’ anxiety decreased after five weeks of daily practice. The students filled out an anonymous survey in which they rated the change in their discomfort after practicing effortless diaphragmatic breathing. More than 70% of the students reported a decrease in anxiety. In addition, they reported decreases in symptoms of stress, neck and shoulder pain as shown in Figure 1.

Figure 1. Self-report of decrease in symptoms after practice diaphragmatic breathing for a week.
In comparing the self-reported responses of the students in the holistic health class to those of the control group (N=12), the students in the holistic health class reported a significant decrease in symptoms since the beginning of the semester as compared to the control group as shown in Figure 2.

Figure 2. Change in self-reported symptoms after 6 weeks of practice the integrated holistic health skills as compared to the control group who did not practice these skills.
Changes in symptoms Most students also reported an increase in mental clarity and concentration that improved their study habits. As one student noted: Now that I breathe properly, I have less mental fog and feel less overwhelmed and more relaxed. My shoulders don’t feel tense, and my muscles are not as achy at the end of the day.
The teaching components for the first five weeks included a focus on the psychobiology of stress, the role of posture, and psychophysiology of respiration. The class included didactic presentations and daily self-practice
Lecture content
- Diadactic presentation on the physiology of stress and how posture impacts health.
- Self-observation of stress reactions; energy drain/energy gain and learning dynamic relaxation.
- Short experiential practices so that the student can experience how slouched posture allows easier access to helpless, hopeless, powerless and defeated memories.
- Short experiential breathing practices to show how breathing holding occurs and how 70% exhalation within 30 seconds increases anxiety.
- Didactic presentation on the physiology of breathing and how a constricted waist tends to have the person breathe high in their chest (the cause of neurasthemia) and how the fight/flight response triggers chest breathing, breath holding and/or shallow breathing.
- Explanation and practice of diaphragmatic breathing.
Daily self-practice
Students were assigned weekly daily self-practices which included both skill mastery by practicing for 20 minutes as well and implementing the skill during their daily life. They then recorded their experiences after the practice. At the end of the week, they reviewed their own log of week and summarized their observations (benefits, difficulties) and then met in small groups to discuss their experiences and extract common themes. These daily practices consisted of:
- Awareness of stress. Monitoring how they reacted to daily stressor
- Practicing dynamic relaxation. Students practiced for 20 minutes a modified progressive relaxation exercise and observed and inhibit bracing pattern
- Changing energy drain and energy gains. Students observed what events reduced or increased their subjective energy and implemented changes in their behavior to decrease events that reduced their energy and increased behaviors that increase their enery
- Creating a memory of wholeness practice
- Practicing effortless breathing. Students practiced slowly diaphragmatic abdominal breathing for 20 minutes per day and each time they become aware of dysfunctional breathing (breath holding, shallow chest breathing, gasping) during the day, they would shift to slower diaphragmatic breathing.
Discussion
Almost all students were surprised how beneficial these practices were to reduce their anxiety and symptoms. Generally, the more the students would interrupt their personal stress responses during the day by shifting to diaphragmatic breathing the more did they experience success. We hypothesize that some of the following factors contributed to the students’ improvement.
- Learning through self-mastery as an education approach versus clinical treatment.
- Generalizing the skills into daily life and activities. Practicing the skills during the day in which the cue of a stress reaction triggered the person to breathe slowly. The breathing would reduce the sympathetic activation.
- Interrupting escalating sympathetic arousal. Responding with an intervention reduced the sense of being overwhelmed and unable to cope by the participant by taking charge and performing an active task.
- Redirecting attention and thoughts away from the anxiety triggers to a positive task.
- Increasing heart rate variability. Through slow breathing heart rate variability increased which enhanced sympathetic parasympathetic balance.
- Reducing subclinical hyperventilation by breathing slower and thereby increasing pC02.
- Increasing social support by meeting in small groups. The class discussion group normalized the anxiety experiences.
- Providing hope. The class lectures, assigned readings and videos provide hope; since, it included reports how other students had reversed their chronic disorders such as irritable bowel disease, acid reflux, psoriasis with behavioral interventions.
Although the study lacked a control group and is only based upon self-report, it offers an economical non-pharmaceutical approach to reduce anxiety. These stress management strategies may not resolve anxiety for everyone. Nevertheless, we recommend that schools implement this approach as the first education intervention to improve health in which students are taught about stress management, learn and practice relaxation and diaphragmatic breathing and then practice these skills during the day whenever they experience stress or dysfunctional breathing.
I noticed that breathing helped tremendously with my anxiety. I was able to feel okay without having that dreadful feeling stay in my chest and I felt it escape in my exhales. I also felt that I was able to breathe deeper and relax better altogether. It was therapeutic, I felt more present, aware, and energized.
See the following blogs for detailed breathing instructions
References
Adams. K.L., Saunders KE, Keown-Stoneman CDG, et al. (2021). Mental health trajectories in undergraduate students over the first year of university: a longitudinal cohort study. BMJ Open 2021; 11:e047393. https://doi.org/10.1136/bmjopen-2020-047393
Barr, E. A., Peper, E. & Swatzyna, R.J. (2019). Slouched Posture, Sleep Deprivation, and Mood Disorders: Interconnection and Modulation by Theta Brain Waves. Neuroregulation, 6(4), 181–189 https://doi.org/10.15540/nr.6.41.181
Bhattacharya, R., Shen, C. & Sambamoorthi, U. (2014). Excess risk of chronic physical conditions associated with depression and anxiety. BMC Psychiatry 14, 10 (2014). https://doi.org/10.1186/1471-244X-14-10
Bier, M., Peper, E., & Burke, A. (2005). Integrated stress management with ‘Make Health Happen: Measuring the impact through a 5-month follow-up. Poster presentation at the 36th Annual Meeting of the Association for Applied Psychophysiology and Biofeedback. Abstract published in: Applied Psychophysiology and Biofeedback, 30(4), 400. https://biofeedbackhealth.files.wordpress.com/2013/12/2005-aapb-make-health-happen-bier-peper-burke-gibney3-12-05-rev.pdf
Bierman, E.J.M., Comijs, H.C. , Jonker, C. & Beekman, A.T.F. (2005). Effects of Anxiety Versus Depression on Cognition in Later Life. The American Journal of Geriatric Psychiatry,13(8), 686-693, https://doi.org/10.1097/00019442-200508000-00007.
Brad, J., Bushman, C., DeWall, N., Pond, R.S., &. Hanus, M.D. (2014).. Low glucose relates to greater aggression in married couples. PNAS, April 14, 2014. https://doi.org/10.1073/pnas.1400619111
Chirikov, I., Soria, K. M, Horgos, B., & Jones-White, D. (2020). Undergraduate and Graduate Students’ Mental Health During the COVID-19 Pandemic. UC Berkeley: Center for Studies in Higher Education. Retrieved from https://escholarship.org/uc/item/80k5d5hw
Coakley, K.E., Le, H., Silva, S.R. et al. Anxiety is associated with appetitive traits in university students during the COVID-19 pandemic. Nutr J 20, 45 (2021). https://doi.org/10.1186/s12937-021-00701-9
Crane,E.H. (2013).Highlights of the 2011 Drug Abuse Warning Network (DAWN) Findings on Drug-Related Emergency Department Visits. 2013 Feb 22. In: The CBHSQ Report. Rockville (MD): Substance Abuse and Mental Health Services Administration (US); 2013-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK384680/
Du Pasquier, D., Fellrath, J.M., & Sauty, A. (2020). Hyperventilation syndrome and dysfunctional breathing: update. Revue Medicale Suisse, 16(698), 1243-1249. https://europepmc.org/article/med/32558453
Gilbert C. Clinical Applications of Breathing Regulation: Beyond Anxiety Management. Behavior Modification. 2003;27(5):692-709. https://doi.org/10.1177/0145445503256322
Kaczkurkin, A.N. & Foa, E.B. (2015). Cognitive-behavioral therapy for anxiety disorders: an update on the empirical evidence. Dialogues Clin Neurosci. 17(3):337-46. https://doi.org/10.31887/DCNS.2015.17.3/akaczkurkin
Kang, H. J., Bae, K. Y., Kim, S. W., Shin, H. Y., Shin, I. S., Yoon, J. S., & Kim, J. M. (2017). Impact of Anxiety and Depression on Physical Health Condition and Disability in an Elderly Korean Population. Psychiatry investigation, 14(3), 240–248. https://doi.org/10.4306/pi.2017.14.3.240
Klein, A. & Peper, W. (2013). There is Hope: Autogenic Biofeedback Training for the Treatment of Psoriasis. Biofeedback, 41(4), 194–201. https://doi.org/10.5298/1081-5937-41.4.01
Lum, L. C. (1981). Hyperventilation and anxiety state. Journal of the Royal Society of Medicine, 74(1), 1-4. https://journals.sagepub.com/doi/pdf/10.1177/014107688107400101
MacCormack, J. K., & Lindquist, K. A. (2019). Feeling hangry? When hunger is conceptualized as emotion. Emotion, 19(2), 301–319. https://doi.org/10.1037/emo0000422
McGrady, A. & Moss, D. (2013). Pathways to illness, pathways to health. New York: Springer. https://link.springer.com/book/10.1007/978-1-4419-1379-1
Peper, E., Gibney, K.H., & Holt, C.F. (2002). Make health happen: Training yourself to create wellness. Dubuque, IA: Kendall/Hunt Publishing Company. https://he.kendallhunt.com/make-health-happen
Peper, E., Harvey, R., Cuellar, Y., & Membrila, C. (2022). Reduce anxiety. NeuroRegulation, 9(2), 91–97. https://doi.org/10.15540/nr.9.2.91 https://www.neuroregulation.org/article/view/22815/14575
Peper, E., Harvey, R., & Hamiel, D. (2019). Transforming thoughts with postural awareness to increase therapeutic and teaching efficacy. NeuroRegulation, 6(3),153-169. doi:10.15540/nr.6.3.1533-1 https://www.neuroregulation.org/article/view/19455/13261
Peper, E., Lin, I-M., Harvey, R., & Perez, J. (2017). How posture affects memory recall and mood. Biofeedback.45 (2), 36-41. https://doi.org/10.5298/1081-5937-45.2.01
Peper, E., Lin, I-M, Harvey, R., Gilbert, M., Gubbala, P., Ratkovich, A., & Fletcher, F. (2014). Transforming chained behaviors: Case studies of overcoming smoking, eczema and hair pulling (trichotillomania). Biofeedback, 42(4), 154-160. https://doi.org/10.5298/1081-5937-42.4.06
Peper, E., MacHose, M. (1993). Symptom prescription: Inducing anxiety by 70% exhalation. Biofeedback and Self-Regulation 18, 133–139). https://doi.org/10.1007/BF00999790
Peper, E., Miceli, B., & Harvey, R. (2016). Educational Model for Self-healing: Eliminating a Chronic Migraine with Electromyography, Autogenic Training, Posture, and Mindfulness. Biofeedback, 44(3), 130–137. https://doi.org/10.5298/1081-5937-44.3.03
Peper, E., Sato-Perry, K & Gibney, K. H. (2003). Achieving Health: A 14-Session Structured Stress Management Program—Eczema as a Case Illustration. 34rd Annual Meeting of the Association for Applied Psychophysiology and Biofeedback. Abstract in: Applied Psychophysiology and Biofeedback, 28(4), 308. Proceeding in: http://www.aapb.org/membersonly/articles/P39peper.pdf
Richmond-Rakerd, L.S., D’Souza, S, Milne, B.J, Caspi, A., & Moffitt, T.E. (2022). Longitudinal Associations of Mental Disorders with Dementia: 30-Year Analysis of 1.7 Million New Zealand Citizens. JAMA Psychiatry. Published online February 16, 2022. https://doi.org/10.1001/jamapsychiatry.2021.4377
Shri, R. (2012). Anxiety: Causes and Management. The Journal of Behavioral Science, 5(1), 100–118. Retrieved from https://so06.tci-thaijo.org/index.php/IJBS/article/view/2205
Wilhelm, F.H., Gevirtz, R., & Roth, W.T. (2001). Respiratory dysregulation in anxiety, functional cardiac, and pain disorders. Assessment, phenomenology, and treatment. Behav Modif, 25(4), 513-45. https://doi.org/10.1177/0145445501254003
Today is a new day-a new beginning
Posted: December 31, 2018 Filed under: behavior, health, Pain/discomfort, self-healing, Uncategorized | Tags: dance, hope, joy, pain, regenration, spinal injury 3 CommentsIn a world of turmoil, it is often challenging to think that tomorrow can be different and better. Yet, each day is an opportunity to accept whatever happened in the past and look forward to the unfolding present. So often, we anticipate that the future will be the same or worse especially if we feel depressed, suffer from ongoing pain, chronic illness, family or work stress, etc. At those moments, we forget that yesterday’s memories may contribute to how we experience and interpret the future. Most of us do not know what the future will bring, thus be open to new opportunities for growth and well-being. For the New Year, adapt a daily ritual that I learned from a remarkable healer Dora Kunz.
Each morning when you get out of bed, take a few slow deep breaths. Then think of someone who you feel loved by and makes you smile whether your grandmother, aunt or dog. Then when you get up and put your feet on the ground, say out loud, “Today is a new day- a new beginning.”
Watch the following two videos of people for whom the future appeared hopeless and yet had the courage to transcend their limitations and offer inspiration and joy.
Janine Shepherd: A broken body isn’t a broken person. Cross-country skier Janine Shepherd hoped for an Olympic medal — until she was hit by a truck during a training bike ride. She shares a powerful story about the human potential for recovery. Her message: you are not your body, and giving up old dreams can allow new ones to soar.
Ma Li and Zhai Xiaowei: Hand in Hand. This is a video of a broadcast that originally aired on China’s English-language CCTV channel 9 during a modern dance competition in Beijing, China in 2007. This very unique couple–she without an arm, he without a leg–was one of the finalists among 7000 competitors in the 4th CCTV national dance competition. It is the first time a handicapped couple had ever entered the competition. They won the silver medal and became an instant national hit. The young woman, in her 30’s, was a dancer who had trained since she was a little girl. Later in life, she lost her entire right arm in an automobile accident and fell into a state of depression for a few years. After rebounding, she decided to team with a young man who had lost his leg in a farming accident as a boy and who was completely untrained in dance. After a long and sometimes agonizing training regimen, this is the result. The dance is performed by Ma Li (馬麗) and Zhai Xiaowei (翟孝偉). The music “Holding Hands” is composed by San Bao and choreographed by Zhao Limin.
Breathing to improve well-being
Posted: November 17, 2017 Filed under: Breathing/respiration, Exercise/movement, Neck and shoulder discomfort, Pain/discomfort, self-healing, stress management, Uncategorized | Tags: anxiety, Breathing, health, mindfulness, pain, respiration, stress 9 CommentsBreathing affects all aspects of your life. This invited keynote, Breathing and posture: Mind-body interventions to improve health, reduce pain and discomfort, was presented at the Caribbean Active Aging Congress, October 14, Oranjestad, Aruba. www.caacaruba.com
The presentation includes numerous practices that can be rapidly adapted into daily life to improve health and well-being.
Healing irritable bowel syndrome with diaphragmatic breathing*
Posted: June 23, 2017 Filed under: Breathing/respiration, self-healing | Tags: abdominal pain, diaphragmatic breathing, food intolerances, health, Holistic health, IBS, irritable bowel syndrome, pain, recurrent abdominal pain, self-care, SIBO, stress, thoracic breathing 31 CommentsErik Peper, Lauren Mason and Cindy Huey
This blog was adapted and expanded from: Peper, E., Mason, L., & Huey, C. (2017). Healing irritable bowel syndrome with diaphragmatic breathing. Biofeedback. 45(4), 83-87. DOI: 10.5298/1081-5937-45.4.04 https://biofeedbackhealth.files.wordpress.com/2018/02/a-healing-ibs-published.pdf
After having constant abdominal pain, severe cramps, and losing 15 pounds from IBS, I found myself in the hospital bed where all the doctors could offer me was morphine to reduce the pain. I searched on my smart phone for other options. I saw that abdominal breathing could help. I put my hands on my stomach and tried to expand it while I inhaled. All that happened was that my chest expanded and my stomach did not move. I practiced and practiced and finally, I could breathe lower. Within a few hours, my pain was reduced. I continued breathing this way many times. Now, two years later, I no longer have IBS and have regained 20 pounds.
– 21-year old woman who previously had severe IBS
Irritable bowel syndrome(IBS) affects between 7% to 21% of the general population and is a chronic condition. The symptoms usually include abdominal cramping, discomfort or pain, bloating, loose or frequent stools and constipation and can significantly reduce the quality of life (Chey et al, 2015). A precursor of IBS in children is called recurrent abdominal pain (RAP) which affects between 0.3 to 19% of school children (Chitkara et al, 2005). Both IBS and RAP appear to be functional illnesses, as no organic causes have been identified to explain the symptoms. In the USA, this results in more than 3.1 physician visits and 5.9 million prescriptions written annually. The total direct and indirect cost of these services exceeds $20 billion (Chey et al, 2015). Multiple factors may contribute to IBS, such as genetics, food allergies, previous treatment with antibiotics, severity of infection, psychological status and stress. More recently, changes in the intestinal and colonic microbiome resulting in small intestine bacterial overgrowth are suggested as another risk factor (Dupont, 2014).
Generally, standard medical treatments (reassurance, dietary manipulation and of pharmacological therapy) are often ineffective in reducing abdominal IBS and other abdominal symptoms (Chey et al, 2015), while complementary and alternative approaches such as relaxation and cognitive therapy are more effective than traditional medical treatment (Vlieger et, 2008). More recently, heart rate variability training to enhance sympathetic/ parasympathetic balance appears to be a successful strategy to treat functional abdominal pain (FAB) in children (Sowder et al, 2010). Sympathetic/parasympathetic balance can be enhanced by increasing heart rate variability (HRV), which occurs when a person breathes at their resonant frequency which is usually between 5-7 breaths per minute. For most people, it means breathing much slower, as slow abdominal breathing appears to be a self-control strategy to reduce symptoms of IBS, RAP and FAP.
This article describes how a young woman healed herself from IBS with slow abdominal breathing without any therapeutic coaching, reviews how slower diaphragmatic breathing (abdominal breathing) may reduce symptoms of IBS, explores the possibility that breathing is more than increasing sympathetic/parasympathetic balance, and suggests some self-care strategies to reduce the symptoms of IBS.
Healing IBS-a case report
After being diagnosed with Irritable Bowel Syndrome her Junior year of high school, doctors told Cindy her condition was incurable and could only be managed at best, although she would have it throughout her entire life. With adverse symptoms including excessive weight loss and depression, Cindy underwent monthly hospital visits and countless tests, all which resulted in doctors informing her that her physical and psychological symptoms were due to her untreatable condition known as IBS, of which no one had ever been cured. When doctors offered her what they believed to be the best option: morphine, something Cindy describes now as a “band-aid,” she was left feeling discouraged. Hopeless and alone in her hospital bed, she decided to take matters into her own hands and began to pursue other options. From her cell phone, Cindy discovered something called “diaphragmatic breathing,” a technique which involved breathing through the stomach. This strategy could help to bring warmth to the abdominal region by increasing blood flow throughout abdomen, thereby relieving discomfort of the bowel. Although suspicious of the scientific support behind this method, previous attempts at traditional western treatment had provided no benefit to recovery; therefore, she found no harm in trying. Lying back flat against the hospital bed, she relaxed her body completely, and began to breathe. Immediately, Cindy became aware that she took her breath in her chest, rather than her stomach. Pushing out all of her air, she tried again, this time gasping with inhalation. Delighted, she watched as air flooded into her stomach, causing it to rise beneath her hands, while her chest remained still. Over time, Cindy began to develop more awareness and control over her newfound strategy. While practicing, she could feel her stomach and abdomen becoming warmer. Cindy shares that for the first time in years, she felt relief from pain, causing her to cry from happiness. Later that day, she was released from the hospital, after denying any more pain medication from doctors.
Cindy continues to practice her diaphragmatic breathing as much as she can, anywhere at all, at the sign of pain or discomfort, as well as preventatively prior to what she anticipates will be a stressful situation. Since beginning her practice, Cindy says that her IBS is pretty much non-existent now. She no longer feels depressed about her situation due to her developed ability to manage her condition. Overall, she is much happier. Moreover, since this time two years ago, Cindy has gained approximately 20 pounds, which she attributes to eating a lot more. In regard to her success, she believes it was her drive, motivation, and willingness to dedicate herself fully to the breathing practice which allowed for her to develop skills and prosper. Although it was not natural for her to breathe in her stomach at first, a trait which she says she often recognizes in others, Cindy explains it was due to necessity which caused her to shift her previously-ingrained way of breathing. Upon publicly sharing her story with others for the first time, Cindy reflects on her past, revealing that she experienced shame for a long time as she felt that she had a weird condition, related to abnormal functions, which no one ever talks about. On the experience of speaking out, she affirms that it was very empowering, and hopes to encourage others coping with a situation similar to hers that there is in fact hope for the future. Cindy continues to feel empowered, confident, and happy after taking control of her own body, and acknowledges that her condition is a part of her, something of which she is proud.
Watch the in-depth interview with Cindy Huey in which she describes her experience of discovering diaphragmatic breathing and how she used this to heal herself of IBS
Video 1. Interview with Cindy Huey describing how she healed herself from IBS.
Background perspective
“Why should the body digest food or repair itself, when it will be someone else’s lunch” (paraphrased from Sapolsky (2004), Why zebras do not get ulcers).
From an evolutionary perspective, we were prey and needed to be on guard (vigilant) to the presence of predators. In the long forgotten past, the predators were tigers, snakes, and the carnivore for whom we were food as well as other people. Today, the same physiological response pathways are still operating, except that the pathways are now more likely to be activated by time urgency, work and family conflict, negative mental rehearsal and self-judgment. This is reflected in the common colloquial phrases: “It makes me sick to my stomach,” “I have no stomach for it,” “He is gutless,” “It makes me queasy,” “Butterflies in my stomach,” “Don’t get your bowels in uproar,” “Gut feelings’, or “Scared shitless.”
Whether conscious or unconscious, when threatened, our body reacts with a fight/flight/freeze response in which the blood flow is diverted from the abdomen to deep muscles used for propulsion. This results in peristalsis being reduced. At the same time the abdomen tends to brace to protect it from injury. In almost all cases, the breathing patterns shift to thoracic breathing with limited abdominal movement. As the breathing pattern is predominantly in the chest, the person increases the risk of hyperventilation because the body is ready to run or fight.
In our clinical observations, people with IBS, small intestine bacterial overgrowth (SIBO), abdominal discomfort, anxiety and panic, and abdominal pain tend to breathe more in their chest, and when asked to take breathe, they tend to inhale in their upper chest with little or no abdominal displacement. Almost anyone who experiences abdominal pain tends to hold the abdomen rigid as if the splinting could reduce the pain. A similar phenomenon is observed with female students experiencing menstrual cramps. They tend to curl up to protect themselves and breathe shallowly in their chest instead of slowly in their abdomen, a body pattern which triggers a defense reaction and inhibits regeneration. If instead they breathe slowly and uncurl they report a significant decrease in discomfort (Gibney & Peper, 2003).
Paradoxically, this protective stance of bracing the abdomen and breathing shallowly in the chest increases breathing rate and reduces heart rate variability. It reduces and inhibits blood and lymph flow through the abdomen as the defensive posture evokes the physiology of fight/flight/freeze. The reduction in venous blood and lymph flow occurs because the ongoing compression and expansion in the abdomen is inhibited by the thoracic breathing and, moreover, the inhibition of diaphragmatic breathing. It also inhibits peristalsis and digestion. No wonder so many of the people with IBS report that they are reactive to some foods. If the GI track has reduced blood flow and reduced peristalsis, it may be less able to digest foods which would affect the bacteria in the small intestine and colon. We wonder if a risk factor that contributes to SIBO is chronic lack of abdominal movement and bracing.
Slow diaphragmatic abdominal breathing to establish health
“Digestion and regeneration occurs when the person feels safe.”
Effortless, slow diaphragmatic breathing occurs when the diaphragm descends and pushes the abdominal content downward during inhalation, which causes the abdomen to become bigger. As the abdomen expands, the pelvic floor relaxes and descends. During exhalation, the pelvic floor muscles tighten slightly, lifting the pelvic floor and the transverse and oblique abdominal muscles contract and push the abdominal content upward against the diaphragm, allowing the diaphragm to relax and go upward, pushing the air out. The following video, 3D view of the diaphragm, from www.3D-Yoga.com by illustrates the movement of the diaphragm.
Video 2. 3D view of diaphragm by sohambliss from www.3D-Yoga.com,
This expansion and constriction of the abdomen occurs most easily if the person is extended, whether sitting or standing erect or lying down, and the waist is not constricted. If the arches forward in a protected pattern and the spine is flexed in a c shape, it would compress the abdomen; instead, the body is long and the abdomen can move and expand during inhalation as the diaphragm descends (see figure 1). If the person holds their abdomen tight or it is constricted by clothing or a belt, it cannot expand during inhalation. Abdominal breathing occurs more easily when the person feels safe and expanded versus unsafe or fearful and collapsed or constricted.

Figure 1. Erect versus collapsed posture note that there is less space for the abdomen to expand in the protective collapsed position. Reproduced by permission from: Clinical Somatics (http://www.clinicalsomatics.ie/
When a person breathes slower and lower it encourages blood and lymph flow through the abdomen. As the person continues to practice slower, lower breathing, it reduces the arousal and vigilance. This is the opposite state of the flight, fight, freeze response so that blood flow is increased in abdomen, and peristalsis re-occurs. When the person practices slow exhalation and breathing and they slightly tighten the oblique and transverse abdominal muscles as well as the pelvic floor and allow these muscles to relax during inhalation. When they breathe in this pattern effortless they, they often will experience an increase in abdominal warmth and an initiation of abdominal sounds (stomach rumble or borborygmus) which indicates that peristalsis has begun to move food through the intestines (Peper et al., 2016). For a detailed description see https://peperperspective.com/2016/04/26/allow-natural-breathing-with-abdominal-muscle-biofeedback-1-2/
What can you do to reduce IBS
There are many factors that cause and effect IBS, some of which we have control over and some which are our out of our control, such as genetics. The purpose of proposed suggestions is to focus on those things over which you have control and reduce risk factors that negatively affect the gastrointestinal track. Generally, begin by integrating self-healing strategies that promote health which have no negative side effects before agreeing to do more aggressive pharmaceutical or even surgical interventions which could have negative side effects. Along the way, work collaboratively with your health care provider. Experiment with the following:
- Avoid food and drinks that may irritate the gastrointestinal tract. These include coffee, hot spices, dairy products, wheat and many others. If you are not sure whether you are reacting to a food or drink, keep a detailed log of what you eat and drink and how you feel. Do self-experimentation by eating or drinking the specific food by itself as the first food in the morning. Then observe how you feel in the next two hours. If possible, eat only organic foods that have not been contaminated by herbicides and pesticides (see: https://peperperspective.com/2015/01/11/are-herbicides-a-cause-for-allergies-immune-incompetence-and-adhd/).
- Identify and resolve stressors, conflicts and problems that negatively affect you and drain your energy. Keep a log to identify situations that drain or increase your subjective energy. Then do problem solving to reduce those situations that drain your energy and increase those situations that increase your energy. For a detailed description of the practice see https://peperperspective.com/2012/12/09/increase-energy-gains-decrease-energy-drains/
Often the most challenging situations that we cannot stomach are those where we feel defeated, helpless, hopeless and powerless or situations where we feel threatened– we do not feel safe. Reach out to other both friends and social services to explore how these situations can be resolved. In some cases, there is nothing that can be done except to accept what is and go on.
- Feel safe. As long as we feel unsafe, we have to be vigilant and are stressed which affects the GI track. Explore the following:
- What does safety mean for you?
- What causes you to feel unsafe from the past or the present?
- What do you need to feel safe?
- Who can offer support that you feel safe?
Reflect on these questions and then explore and implement ways by which you can create feeling more safe.
- Take breaks to regenerate. During the day, at work and at home, monitor yourself. Are you pushing yourself to complete tasks. In a 24/7 world with many ongoing responsibilities, we are unknowingly vigilant and do not allow ourselves to rest and relax to regenerate. Do not wait till you feel tired or exhausted. Stop earlier and take a short break. The break can be a short walk, a cup of tea or soup, or looking outside at a tree. During this break, think about positive events that have happened or people who love you and for whom you feel love. When you smile and think of someone who loves you, such as a grandparent, you may relax and for that moment as you feel safe which allows regeneration to begin.
- Observe how you inhale. Take a deep breath. If you feel you are moving upward and becoming a little bit taller, your breathing is wrong. Put one hand on your lower abdomen and the other on your chest and take a deep breath. If you observe your chest lifted upward and stomach did not expand, your breathing is wrong. You are not breathing diaphragmatically. Watch the following video, The correct way to breathe in, on how to observe your breathing and how to breathe diaphragmatically.
- Learn diaphragmatic breathing. Take time to practice diaphragmatic breathing. Practice while lying down and sitting or standing. Let the breathing rate slow down to about six breaths per minute. Exhale to the count of four and then let it trail off for two more counts, and inhale to the count of three and let it trail for another count. Practice this sitting and lying down (for more details on breathing see: https://peperperspective.com/2014/09/11/a-breath-of-fresh-air-improve-health-with-breathing/.
- Sitting position. Exhale by feeling your abdomen coming inward slightly for the count of four and trailing off for the count of two, then allow the lower ribs to widen, abdomen expand–the whole a trunk expands–as you inhale while the shoulders stay relaxed for a count of three. Allow it to trail off for one more count before you again begin to exhale. Be gentle, do not rush or force yourself. Practice this slower breathing for five minutes. Focus more on the exhalation and allowing the air to just flow in. Give yourself time during the transition between inhalation and exhalation.
- Lying down position. While lying on your back, place a two to five-pound weight such as a bag of rice on your stomach as shown in Figure 2.

Figure 2. Lying down and practicing breathing with two to five-pound weight on stomach (reproduced by permission from Gorter and Peper, 2011.
As you inhale push the weight upward and also feel your lower ribs widen. Then allow exhalation to occur by the weight pushing the abdominal content down which pushes the diaphragm upward. This causing the breath to flow out. As you exhale, imagine the air flowing out through your legs as if there were straws inside your legs. When your attention wanders, smile and bring it back to imagining the air flowing down your legs during exhalation. Practice this for twenty minutes. Many people report that during the practice the gurgling in their abdomen occurs which is a sign that peristalsis and healing is returning.
- Observe and change your breathing during the day. Observe your breathing pattern during the day. Each time you hold your breath, gasp or breathe in your chest, interrupt the pattern and substitute slow diaphragmatic breathing for the next five breaths. Do this the whole day long. Many people observe that when they think of stressor or are worried, they hold their breath or shallow breathe in the chest. If this occurs, acknowledge the worry and focus on changing your breathing. This does not mean that you dismiss the concern, instead for this moment you focus on breathing and then explore ways to solve the problem.
If you observed that under specific circumstance you held your breath or breathed shallowly in your chest, then whenever you anticipate that the same event will occur again, begin to breathe diaphragmatically. To do this consistently is very challenging and most people report that initially they only seem to breathe incorrectly. It takes practice, practice and practice—mindful practice– to change. Yet those who continue to practice often report a decrease in symptoms and feel more energy and improved quality of life.
Summary
Changing habitual health behaviors such as diet and breathing can be remarkably challenging; however, it is possible. Give yourself enough time, and practice it many times until it becomes automatic. It is no different from learning to play a musical instrument or mastering a sport. Initially, it feels impossible, and with lot of practice it becomes more and more automatic. We continue to be impressed that healing is possible. Among our students at San Francisco State University, who practice their self-healing skills for five weeks, approximately 80% report a significant improvement in their health (Peper et al., 2014).
* This blog was adapted and expanded from: Peper, E., Mason, L., & Huey, C. (2017). Healing irritable bowel syndrome with diaphragmatic breathing. Biofeedback. 45(4), 83-87. DOI: 10.5298/1081-5937-45.4.04 https://biofeedbackhealth.files.wordpress.com/2018/02/a-healing-ibs-published.pdf
References
Chey, W. D., Kurlander, J., & Eswaran, S. (2015). Irritable bowel syndrome: a clinical review. Jama, 313(9), 949-958.
Chitkara, D. K., Rawat, D. J., & Talley, N. J. (2005). The epidemiology of childhood recurrent abdominal pain in Western countries: a systematic review. American journal of Gastroenterology, 100(8), 1868-1875.
Dupont, H. L. (2014). Review article: evidence for the role of gut microbiota in irritable bowel syndrome and its potential influence on therapeutic targets. Alimentary pharmacology & therapeutics, 39(10), 1033-1042.
Gibney, H.K. & Peper, E. (2003). Taking control: Strategies to reduce hot flashes and premenstrual mood swings. Biofeedback, 31(3), 20-24.
Gorter, R. & Peper, E. (2011). Fighting Cancer-A NonToxic Approach to Treatment. Berkeley: North Atlantic.
Peper, E., Booiman, A., Lin, I-M, Harvey, R., & Mitose, J. (2016). Abdominal SEMG Feedback for Diaphragmatic Breathing: A Methodological Note. Biofeedback. 44(1), 42-49.
Peper, E., Lin, I-M, Harvey, R., Gilbert, M., Gubbala, P., Ratkovich, A., & Fletcher, F. (2014). Transforming chained behaviors: Case studies of overcoming smoking, eczema and hair pulling (trichotillomania). Biofeedback, 42(4), 154-160.
Sapolsky, R. (2004). Why Zebras Don’t Get Ulcers. New York: Owl Books
Sowder, E., Gevirtz, R., Shapiro, W., & Ebert, C. (2010). Restoration of vagal tone: a possible mechanism for functional abdominal pain. Applied psychophysiology and biofeedback, 35(3), 199-206.
Vlieger, A. M., Blink, M., Tromp, E., & Benninga, M. A. (2008). Use of complementary and alternative medicine by pediatric patients with functional and organic gastrointestinal diseases: results from a multicenter survey. Pediatrics, 122(2), e446-e451.
Enjoy laughter-It’s healing
Posted: April 21, 2017 Filed under: Uncategorized | Tags: health, humor, laughter, pain, stress management Leave a commentJoy and laughter are healing and contagious (Wang, 2006). When we laugh, our mood lightens, we feel better and our health improves (Bennett & Lengacher, 2006a; Bennett & Lengacher, 2006b; Bennett & Lengacher, 2008; Bennett & Lengacher, 2009). As Norman Cousins, who had ankylosing spondylitis (a degenerative disease causing the breakdown of collagen) which left him in severe pain that even morphine couldn’t touch, claimed that 10 minutes of belly laughter would give him two hours of pain-free sleep. He documented his remarkable recovery in his book Anatomy of an illness (Cousins, 2005). Laughter and joy has the ability to transform your health.
Despite the challenges you may face, the actual troubles that may occur during the day, or feeling frustrated or depressed, treat yourself to a moment of joy and laughter. Through laughing, we relax and support the intrinsic self-healing processes in our body. Even in suffering we have a choice of what to feed our brain. Enjoy watching the following videos.
Finally, watch Norman Cousins describe his own healing experience: https://www.youtube.com/watch?v=0LwKd68S15I
Also see the embedded videos posted on: http://www.laughteronlineuniversity.com/norman-cousins-a-laughterpain-case-study/
References:
Wang, S. (2006). Contagious behavior. American Psychological Society Observer, 19(2), 22-26.
Enjoy sex: Breathe away the pain*
Posted: March 19, 2017 Filed under: Breathing/respiration, Pain/discomfort, self-healing, Uncategorized | Tags: Breathing, dyspareunia, intercourse, intimacy, pain, pelvic floor, relaxation, Sexuality, vaginismus 15 CommentsAdapted from: Peper, E. & Cohen, T. (2017). Inhale to breathe away pelvic floor pain and enjoy intercourse. Biofeedback, 45(1), 21–24. https://doi.org/10.5298/1081-5937-45.1.04
“After two and a half years of trying, ups and downs, and a long period of thinking it will never happen, it did happen. I followed your advice by only applying pressure with the cones while inhaling and at the same time relaxing the pelvic floor. We succeeded! we had “real” sex in the first time.”
Millions of women experience involuntary contraction of the musculature of the outer third of the vagina (vaginismus) interfering with intercourse, causing distress and interpersonal difficulty (ter Kuile et, 2010) or pain during intercourse (dyspareunia). It is estimated that 1 to 6% of women have vaginismus (Lewis et al, 2004) and 6.5% to 45.0% in older women and from 14% to 34% in younger women experience dyspareunia (Van Lankveld et al, 2010; Gross & Brubaker, 2022). The most common treatment for vaginismus is sequential dilation of the vaginal opening with progressively larger cones, psychotherapy and medications to reduce the pain and anxiety. At times clients and health care professionals may be unaware of the biological processes that influence the muscle contraction and relaxation of the pelvic floor. Success is more likely if the client works in harmony with the biological processes while practicing self-healing and treatment protocols. These biological processes, described at the end of the blog significantly affects the opening of vestibule and vagina are: 1) feeling safe, 2) inhale during insertion to relax the pelvic floor, 3) stretch very, very slowly to avoid triggering the stretch reflex, and 4) being sexual aroused.
Successful case report: There is hope to resolve pain and vaginismus
Yesterday my husband and I had sex in the first time, after two and a half years of “trying”. Why did it take so long? Well, the doctor said “vaginismus”, the psychologist said “fear”, the physiotherapist said “constricted muscles”, and friends said “just relax, drink some wine and it will happen”.
Sex was always a weird, scary, complicated – and above all, painful – world to me. It may have started in high school: like many other teens, I thought a lot about sex and masturbated almost every night. Masturbation was a good feeling followed by tons of bad feelings – guilt, shame, and feeling disgusting. One of the ideas I had to accept, later in my progress, is that ‘feeling good is a good thing’. It is normal, permitted and even important and healthy.
My first experience, at age 20, was short, very painful, and without any love or even affection. He was…. well, not for me. And I was…. well, naive and with very little knowledge about my body. The experiences that came after that, with other guys, were frustrating. Neither of them knew how to handle the pain that sex caused me, and I didn’t know what to do.
The first gynecologist said that everything is fine and I just need to relax. No need to say I left her clinic very angry and in pain. The second gynecologist was the first one to give it a name: “vaginismus”. He said that there are some solutions to the problem: anesthetic ointment, physiotherapy (“which is rarely helps”, according to his optimistic view..), and if these won’t work “we will start thinking of surgery, which is very painful and you don’t want to go there”. Oh, I certainly didn’t want to go there.
After talking to a friend whose sister had the same problem, I started seeing a great physiotherapist who was an expert in these problems. She used a vaginal biofeedback sensor, that measured muscles’ tonus inside the vagina. My homework were 30 constrictions every day, plus working with “dilators” – plastic cones comes in 6 sizes, starting from a size of a small finger, to a size of a penis.
At this point I was already in a relationship with my husband, who was understanding, calm and most important – very patient. To be honest, we both never thought it would take so long. Practicing was annoying and painful, and I found myself thinking a lot “is it worth it?”. After a while, I felt that the physical practice is not enough, and I need a “psychological breakthrough”. So I stopped practicing and started seeing a psychologist, for about a half a year. We processed my past experiences, examined the thoughts and beliefs I had about sex, and that way we released some of the tension that was shrinking my body.
The next step was to continue practicing with the dilators, but honestly – I had no motivation. My husband and I had great sex without the actual penetration, and I didn’t want the painful practice again. Fortunately, I participated in a short course given by Professor Erik Peper, about biofeedback therapy. In his lecture he described a young woman, who suffered from vulvodynia, a problem that is a bit similar to vaginismus (Peper et al, 2015; See: https://peperperspective.com/2015/09/25/resolving-pelvic-floor-pain-a-case-report/). She learned how to relax her body and deal with the pain, and finally she had sex – and even enjoyed it! I was inspired.
Erik Peper gave me a very important advice: breathing in. Apparently, we can relax the muscles and open the vagina better while inhaling, instead of exhaling – as I tried before. During exhalation the pelvic floor tightens and goes upward while during inhalation the pelvic floor descends and relaxes especially when sitting up (Peper et al, 2016). He advised me to give myself a few minutes with the dilator, and in every inhale – imagine the area opening and insert the dilator a few millimeters. I started practicing again, but in a sitting position, which I found more comfortable and less painful. I advanced to the biggest dilator within a few weeks, and had a just little pain – sometimes without any pain at all. The most important thing I understood was not to be afraid of the pain. The fear is what made me even more tensed, and tension brings pain. Then, my husband and I started practicing with “the real thing”, very slowly and gently, trying to find the best position and angle for us. Finally, we did it. And it was a great feeling.
The biological factors that affect the relaxation/contraction of the pelvic floor and vaginal opening are:
Feeling safe and hopeful. When threatened, scared, anticipate pain, and worry, our body triggers a defense reaction. In this flexor response, labeled by Thomas Hanna as the Red Light Reflex, the body curls up in defense to protect itself which includes the shoulders to round, the chest to be depressed, the legs pressing together, the pelvic floor to tighten and the head to jut forward (Hanna, 2004). This is the natural response of fear, anxiety, prolonged stress or negative depressive thinking.
Before beginning to work on vaginismus, feel safe. This means accepting what is, accepting that it is not your fault, and that there are no demands for performance. It also means not anticipating that it will be again painful because with each anticipation the pelvic floor tends to tightens. Read the chapter on vaginismus in Dr. Lonnie Barbach’s book, For each other: Sharing sexual intimacy (Barbach, 1983).
Inhale during insertion to relax the pelvic floor and vaginal opening. This instruction is seldom taught because in most instances, we have been taught to exhale while relaxing. Exhaling while relaxing is true for most muscles; however, it is different for the pelvic floor. When inhalation occurs, the pelvic floor descends and relaxes. During exhalation the pelvic floor tightens and ascends to support breathing and push the diaphragm upward to exhale the air. Be sure to allow the abdomen to expand during inhalation without lifting the chest and allow the abdomen to constrict during exhalation as if inhalation fills the balloon in the abdomen and exhalation deflates the balloon (for detailed instructions see Peper et al, 2016). Do not inhale by lifting and expanding your chest which often occurs during gasping and and fear. It tends to tighten and lift the pelvic floor.
Experience the connection between diaphragmatic breathing and pelvic floor movement in the following practice.
While sitting upright make a hissing noise as the air escapes with pressure between your lips. As you are exhaling feel, your abdomen and your anus tightening. During the inhalation let your abdomen expand and feel how your anus descends and pelvic floor relaxes. With practice this will become easier.
Stretch very, very slowly to avoid triggering the stretch reflex. When a muscle is rapidly stretched, it triggers an automatic stretch reflex which causes the muscle to contract. This innate response occurs to avoid damaging the muscle by over stretching. The stretch reflex is also triggered by pain and puts a brake on the stretching. Always use a lubricant when practicing by yourself or with a partner. Practice inserting larger and larger diameter dilaters into the vagina. Start with a very small diameter and progress to a larger diameter. These can be different diameter cones, your finger, or other objects. Remember to inhale and feel the pelvic floor descending as you insert the probe or finger. If you feel discomfort/pain, stop pushing, keep breathing, relax your shoulders, relax your hips, legs, and toes and do not push inward and upward again until the discomfort has faded out.
Feel sexually aroused by allowing enough foreplay. When sexually aroused the tissue is more lubricated and may stretch easier. Continue to use a good lubricant.
Putting it all together.
When you feel safe, practice slow diaphragmatic breathing and be aware of the pelvic floor relaxing and descending during inhalation and contracting and going up during exhalation. When practicing stretching the opening with cones or your finger, go very, very slow. Only apply pressure of insertion during the mid-phase of inhalation, then wait during exhalation and then again insert slight more during the next inhalation. When you experience pain, relax your shoulders, keep breathing for four or five breaths till the pain subsides, then push very little during the next inhalation. Go much slower and with more tenderness.
Be patient. Explain to your partner that your body and mind need time to adjust to new feelings. However, don’t stop having sex – you can have great sex without penetration. Practice both alone and with your partner; together find the best angle and rate. Use different lubricants to check out what is best for you. Any little progress is getting you closer to having an enjoyable sex. I recommend watching this TED video of Emily Nagoski explaining the “dual control model” and practicing as she suggests: https://www.youtube.com/watch?v=HILY0wWBlBM
Finally, practice the exercises developed by Dr. Lonnie Barbach, who as one of the first co-directors of clinical training at the University of California San Francisco, Human Sexuality Program, created the women’s pre-orgasmic group treatment program. They are superbly described in her two books, For each other: Sharing sexual intimacy, and For yourself: The fulfillment of female sexuality, and are a must read for anyone desiring to increase sexual fulfillment and joy (Barbach, 2000; 1983).
References:
Barbach, L. (1983). For each other: Sharing sexual intimacy. New York: Anchor
Barbach, L. (2000). For yourself: The fulfillment of female sexuality. New York: Berkley.
BarLewis, R. W., Fugl‐Meyer, K. S., Bosch, R., Fugl‐Meyer, A. R., Laumann, E. O., Lizza, E., & Martin‐Morales, A. (2004). Epidemiology/risk factors of sexual dysfunction. The journal of sexual medicine, 1(1), 35-39. http://www.jsm.jsexmed.org/article/S1743-6095(15)30062-X/fulltext
Gross. E. & Brubaker, L. (2022). Dyspareunia in Women. JAMA. https://doi.org/10.1001/jama.2022.4853
Hanna, T. (2004). Somatics: Reawakening the mind’s control of movement, flexibility, and health. Boston: Da Capo Press.
Martinez Aranda, P. & Peper, E. (2015). The healing of vulvodynia from a client’s perspective. https://biofeedbackhealth.files.wordpress.com/2011/01/a-healing-of-vulvodynia-from-the-client-perspective-2015-06-15.pdf
Peper, E., Booiman, A., Lin, I-M, Harvey, R., & Mitose, J. (2016). Abdominal SEMG Feedback for Diaphragmatic Breathing: A Methodological Note. Biofeedback. 44(1), 42-49. https://biofeedbackhealth.files.wordpress.com/2011/01/1-abdominal-semg-feedback-published.pdf
Peper, E., Martinez Aranda, P., & Moss, E. (2015). Vulvodynia treated successfully with breathing biofeedback and integrated stress reduction: A case report. Biofeedback. 43(2), 103-109. https://biofeedbackhealth.files.wordpress.com/2011/01/a-vulvodynia-treated-with-biofeedback-published.pdf
Ter Kuile, M. M., Both, S., & van Lankveld, J. J. (2010). Cognitive behavioral therapy for sexual dysfunctions in women. Psychiatric Clinics of North America, 33(3), 595-610. https://www.researchgate.net/publication/45090259_Cognitive_Behavioral_Therapy_for_Sexual_Dysfunctions_in_Women
Van Lankveld, J. J., Granot, M., Weijmar Schultz, W., Binik, Y. M., Wesselmann, U., Pukall, C. F., . Achtrari, C. (2010). Women’s sexual pain disorders. The Journal of Sexual Medicine, 7(1pt2), 615-631. http://www.jsm.jsexmed.org/article/S1743-6095(15)32867-8/fulltext
*We thank Dr. Lonnie Barbach for her helpful feedback and support. Written collaboratively with Tal Cohen, biofeedback therapist (Israel) and Erik Peper.
Mind-Guided Body Scans for Awareness and Healing Youtube Interview of Erik Peper, PhD by Larry Berkelhammer, PhD
Posted: February 19, 2016 Filed under: Uncategorized | Tags: autogenic training, body scan, mind-body, mindfulness, pain, passive attention, stress management Leave a commentIn this interview psychophysiology expert Dr. Erik Peper explains the ways how a body scan can facilitate awareness and healing. The discussion describes how the mind-guided body scan can be used to improve immune function and maintain passive attention (mindfulness), and become centered. It explores the process of passive attentive process that is part of Autogenic Training and self-healing mental imagery. Mind-guided body scanning involves effortlessly observing and attending to body sensations through which we can observe our own physiological processes. Body scanning can be combined with imagery to be in a nonjudgmental state that supports self-healing and improves physiological functioning.
Resolving pelvic floor pain-A case report
Posted: September 25, 2015 Filed under: Breathing/respiration, Pain/discomfort, self-healing, stress management, Uncategorized | Tags: biofeedback, Breathing, electromyography, pain, posture, self-regulation, vulvodynia 10 CommentsAdapted from: Martinez Aranda, P. & Peper, E. (2015). The healing of vulvodynia from a client’s perspective. https://biofeedbackhealth.files.wordpress.com/2011/01/a-healing-of-vulvodynia-from-the-client-perspective-2015-06-15.pdf
It’s been a little over a year since I began practicing biofeedback and visualization strategies to overcome vulvodynia. Today, I feel whole, healed, and hopeful. I learned that through controlled and conscious breathing, I could unleash the potential to heal myself from chronic pain. Overcoming pain did not happen overnight; but rather, it was a process where I had to create and maintain healthy lifestyle habits and meditation. Not only am I thankful for having learned strategies to overcome chronic pain, but for acquiring skills that will improve my health for the rest of my life. –-24 year old woman who successfully resolved vulvodynia
Pelvic floor pain can be debilitating, and it is surprisingly common, affecting 10 to 25% of American women. Pelvic floor pain has numerous causes and names. It can be labeled as vulvar vestibulitis, an inflammation of vulvar tissue, interstitial cystitis (chronic pain or tenderness in the bladder), or even lingering or episodic hip, back, or abdominal pain. Chronic pain concentrated at the entrance to the vagina (vulva), is known as vulvodynia. It is commonly under-diagnosed, often inadequately treated, and can go on for months and years (Reed et al., 2007; Mayo Clinic, 2014). The discomfort can be so severe that sitting is uncomfortable and intercourse is impossible because of the extreme pain. The pain can be overwhelming and destructive of the patient’s life. As the participant reported,
I visited a vulvar specialist and he gave me drugs, which did not ease the discomfort. He mentioned surgical removal of the affected tissue as the most effective cure (vestibulectomy). I cried immediately upon leaving the physician’s office. Even though he is an expert on the subject, I felt like I had no psychological support. I was on Gabapentin to reduce pain, and it made me very depressed. I thought to myself: Is my life, as I know it, over?
Physically, I was in pain every single day. Sometimes it was a raging burning sensation, while other times it was more of an uncomfortable sensation. I could not wear my skinny jeans anymore or ride a bike. I became very depressed. I cried most days because I felt old and hopeless instead of feeling like a vibrant 23-year-old woman. The physical pain, combined with my negative feelings, affected my relationship with my boyfriend. We were unable to have sex at all, and because of my depressed status, we could not engage in any kind of fun. (For more details, read the published case report,Vulvodynia treated successfully with breathing biofeedback and integrated stress reduction: A case report).
The four-session holistic biofeedback interventions to successfully resolved vulvodynia included teaching diaphragmatic breathing to transform shallow thoracic breathing into slower diaphragmatic breathing, transforming feelings of powerlessness and hopelessness to empowerment and transforming her beliefs that she could reduce her symptoms and optimize her health. The interventions also incorporated self-healing imagery and posture-changing exercises. The posture changes consisted of developing awareness of the onset of moving into a collapsed posture and use this awareness to shift to an erect/empowered postures (Carney, Cuddy, & Yap, 2010; Peper, 2014; Peper, Booiman, Lin, & Harvey, in press). Finally, this case report build upon the seminal of electromyographic feedback protocol developed by Dr. Howard Glazer (Glazer & Hacad, 2015) and the integrated relaxation protocol developed Dr. David Wise (Wise & Anderson, 2007).
Through initial biofeedback monitoring of the lower abdominal muscle activity, chest, and abdomen breathing patterns, the participant observed that when she felt discomfort or was fearful, her lower abdomen muscles tended to tighten. After learning how to sense this tightness, she was able to remind herself to breathe lower and slower, relax the abdominal wall during inhalation and sit or stand in an erect power posture.
The self-mastery approach for healing is based upon a functional as compared to a structural perspective. The structural perspective implies that the problem can only be fixed by changing the physical structure such as with surgery or medications. The functional perspective assumes that if you can learn to change your dysfunctional psychophysiological patterns the disorder may disappear.
The functional approach assumed that an irritation of the vestibular area might have caused the participant to tighten her lower abdomen and pelvic floor muscles reflexively in a covert defense reaction. In addition, ongoing worry and catastrophic thinking (“I must have surgery, it will never go away, I can never have sex again, my boyfriend will leave me”) also triggered the defense reaction—further tightening of her lower abdomen and pelvic area, shallow breathing, and concurrent increases in sympathetic nervous activation—which together activated the trigger points that lead to increased chronic pain (Banks et al, 1998).
When the participant experienced a sensation or thought/worried about the pain, her body responded in a defense reaction by breathing in her chest and tightening the lower abdominal area as monitored with biofeedback. Anticipation of being monitored increased her shoulder tension, recalling the stressful memory increased lower abdominal muscle tension (pulling in the abdomen for protection), and the breathing became shallow and rapid as shown in Figure 1.
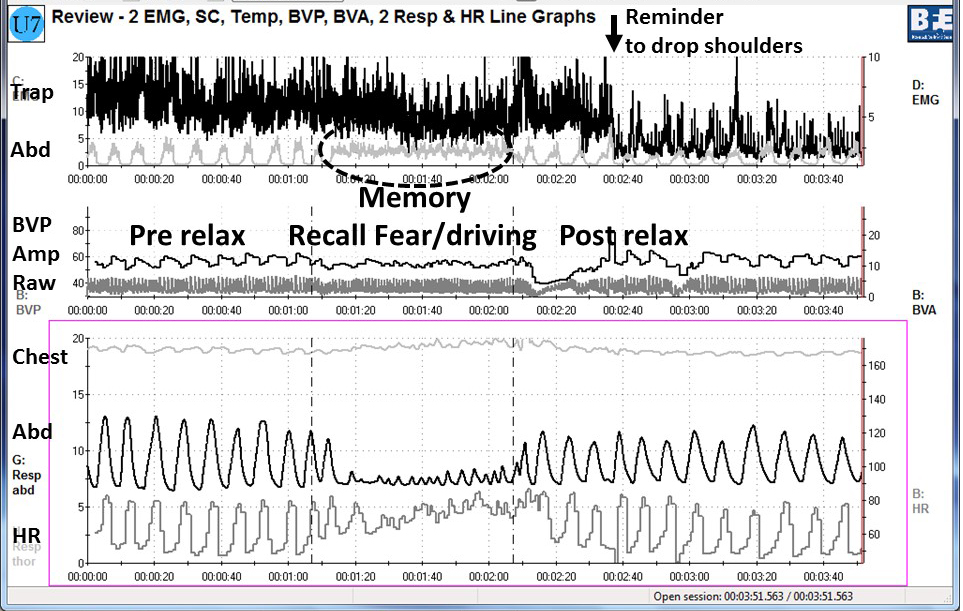
Figure 1. Physiological recording of pre-stressor relaxation, the recall of a fearful driving experience, and a post-stressor relaxation. The scalene to trapezius SEMG increased in anticipation while she recalled the experience, and then initially did not relax (from Peper, Martinez Aranda, & Moss, 2015).
This defense pattern became a conditioned response—initiating intercourse or being touched in the affected area caused the participant to tense and freeze up. She was unaware of these automatic protective patterns, which only worsened her chronic pain.
During the four sessions of training, the participant learned to reverse and interrupt the habitual defense reaction. For example, as she became aware of her breathing patterns she reported,
It was amazing to see on the computer screen the difference between my regular breathing pattern and my diaphragmatic breathing pattern. I could not believe I had been breathing that horribly my whole life, or at least, for who knows how long. My first instinct was to feel sorry for myself. Then, rather than practicing negative patterns and thoughts, I felt happy because I was learning how to breathe properly. My pain decreased from an 8 to alternating between a 0 and 3.
The mastery of slower and lower abdominal breathing within a holistic perspective resulted in the successful resolution of her vulvodynia. An essential component of the training included allowing the participant to feel safe, and creating hope by enabling her to experience a decrease in discomfort while doing a specific practice, and assisting her to master skills to promote self-healing. Instead of feeling powerless and believing that the only resolution was the removal of the affected area (vestibulectomy). The integrated biofeedback protocol offered skill mastery training, to promote self-healing through diaphragmatic breathing, somatic postural changes, reframing internal language, and healing imagery as part of a common sense holistic health approach.
For more details about the case report, download the published study, Peper, E., Martinez Aranda, P., & Moss, E. (2015). Vulvodynia treated successfully with breathing biofeedback and integrated stress reduction: A case report. Biofeedback. 43(2), 103-109.
The participant also wrote up her subjective experience of the integrated biofeedback process in the paper, Martinez Aranda & Peper (2015). Healing of vulvodynia from the client perspective. In this paper she articulated her understanding and experiences in resolving vulvodynia which sheds light on the internal processes that are so often skipped over in published reports.
At the five year follow-up on May 29, 2019, she wrote:
“I am doing very well, and I am very healthy. The vulvodynia symptoms have never come back. It migrated to my stomach a couple of years after, and I still have a sensitive stomach. My stomach has gotten much, much better, though. I don’t really have random pain anymore, now I just have to be watchful and careful of my diet and my exercise, which are all great things!”
References
Banks, S. L., Jacobs, D. W., Gevirtz, R., & Hubbard, D. R. (1998). Effects of autogenic relaxation training on electromyographic activity in active myofascial trigger points. Journal of Musculoskeletal Pain, 6(4), 23-32. https://www.researchgate.net/profile/David_Hubbard/publication/232035243_Effects_of_Autogenic_Relaxation_Training_on_Electromyographic_Activity_in_Active_Myofascial_Trigger_Points/links/5434864a0cf2dc341daf4377.pdf
Carney, D. R., Cuddy, A. J., & Yap, A. J. (2010). Power posing brief nonverbal displays affect neuroendocrine levels and risk tolerance. Psychological Science, 21(10), 1363-1368. Available from: https://www0.gsb.columbia.edu/mygsb/faculty/research/pubfiles/4679/power.poses_.PS_.2010.pdf
Glazer, H. & Hacad, C.R. (2015). The Glazer Protocol: Evidence-Based Medicine Pelvic Floor Muscle (PFM) Surface Electromyography (SEMG). Biofeedback, 40(2), 75-79. http://www.aapb-biofeedback.com/doi/abs/10.5298/1081-5937-40.2.4
Martinez Aranda, P. & Peper, E. (2015). Healing of vulvodynia from the client perspective. Available from: https://biofeedbackhealth.files.wordpress.com/2011/01/a-healing-of-vulvodynia-from-the-client-perspective-2015-06-15.pdf
Mayo Clinic (2014). Diseases and conditions: Vulvodynia. Available at http://www.mayoclinic.org/diseases-conditions/vulvodynia/basics/definition/con-20020326
Peper, E. (2014). Increasing strength and mood by changing posture and sitting habits. Western Edition, pp.10, 12. Available from: http://thewesternedition.com/admin/files/magazines/WE-July-2014.pdf
Peper, E., Booiman, A., Lin, I, M.,& Harvey, R. (in press). Increase strength and mood with posture. Biofeedback.
Peper, E., Martinez Aranda, P., & Moss, E. (2015). Vulvodynia treated successfully with breathing biofeedback and integrated stress reduction: A case report. Biofeedback. 43(2), 103-109. Available from: https://biofeedbackhealth.files.wordpress.com/2011/01/a-vulvodynia-treated-with-biofeedback-published.pdf
Reed, B. D., Haefner, H. K., Sen, A., & Gorenflo, D. W. (2008). Vulvodynia incidence and remission rates among adult women: a 2-year follow-up study. Obstetrics & Gynecology, 112(2, Part 1), 231-237. http://journals.lww.com/greenjournal/Abstract/2008/08000/Vulvodynia_Incidence_and_Remission_Rates_Among.6.aspx
Wise, D., & Anderson, R. U. (2006). A headache in the pelvis: A new understanding and treatment for prostatitis and chronic pelvic pain syndromes. Occidental, CA: National Center for Pelvic Pain Research.http://www.pelvicpainhelp.com/books/
