Tell Me Where It Hurts
Posted: April 24, 2026 Filed under: attention, behavior, biofeedback, Breathing/respiration, cancer, education, emotions, healing, health, Neck and shoulder discomfort, Pain/discomfort, self-healing, surgery | Tags: health, meditation, mental-health, mindfulness, wellness 2 Comments
In my biofeedback practice, I’ve repeatedly seen that healing rarely comes from a single technique. It emerges from observation, integration and practicing and integrating skills in daily life. When clients learn to combine biofeedback with other strategies to make it their own such as slower, more coherent breathing, guided imagery, shifts in internal dialogue, and practical lifestyle changes, something important happens: the body begins to reorganize itself toward health.
Again and again, clients report meaningful changes. Stress symptoms, headaches, eye problem, neck shoulder and back pain decrease or disappear. Gastrointestinal symptoms often fade out. Anxiety loosens its grip. Asthma improves. Chronic neck, shoulder, and pelvic pain diminish. These are not isolated outcomes; they reflect a pattern. When people gain the skills to regulate their physiology and reinterpret their internal experience, decrease in symptoms often follow (see the list of articles that describe successful outcomes).
Even though many of my clients benefit, I am continually searching for strategies and approaches that can improve their health and reduce suffering and for materials that I can recommend to them.
Now when I see a client who reports pain or who takes care of someone with pain, the first thing I do is to recommend the book, Tell Me Where It Hurts, by Rachel Zoffness, PhD, a leading pain expert and psychologist. The book offers a clear, science-based framework grounded in modern neuroscience, yet conveyed through compelling human stories. Her work aligns closely with what we observe in biofeedback: pain is not simply a signal from injured tissue. It is an experience shaped by the interaction of body, brain, emotions, beliefs, culture and context.
She makes a crucial point that pain may begin with injury or illness, but it is always modulated by factors such as physiological state, emotional meaning, cognitive interpretation, and social and cultural influences. In other words, pain is real, but it is also dynamic and changeable.
The first step she emphasizes is education. When people understand how pain actually works, fear often decreases. From there, the task becomes identifying what amplifies pain and what reduces it and then systematically strengthening the factors and behaviors and skills that support recovery.
One striking story captures this perfectly: a construction worker jumps from a plank onto what appears to be a 7” nail, which is driven through his boot. He experiences excruciating pain and is rushed to the emergency room. Yet when the boot is removed, the nail is found to have passed cleanly between his toes—there is no tissue damage. The pain was real, but it was driven by perception and expectation. This is not an anomaly; it is a powerful illustration of how the brain constructs pain.
Equally compelling are the recovery stories. Patients with severe chronic pain that continue and got worse after failed surgeries, long-term disability, or even amputation, find relief not through more invasive procedures or medication alone, but through learning how to retrain their nervous system. In many of these cases, even opioids had failed to provide meaningful relief. What made the difference was a shift in understanding, combined with evidence-based self-regulation strategies. They are no longer abstract ideas; they are lived experiences.
The larger message is both simple and profound: pain can change. And when people are given the right framework and tools, they can actively participate in that change. For anyone living with pain, or working professionally with those who do, this book is not just informative. It is practical, empowering, and, in many cases, transformative.
This is the book to read if you have pain or care for someone with pain. It is also the book every therapist who works with people with pain should read and recommend to their clients.
Zoffness, R. (2026). Tell me where it hurts. Grand Central. https://www.amazon.com/Tell-Me-Where-Hurts-Science/dp/1538758148/
I recommend listening to the excellent podcast generated with Google NotebookLM, which thoughtfully expands upon and clarifies the underlying research.isten to the expanded podcast based on this blog and created with Google Notebook LM.
The following blog has a link to a superb podcast featuring Rachel Zoffness.
Then listen to the podcast from Dolorology (PAIN) Encore with Dr. Rachel Zoffness. https://www.alieward.com/ologies/dolorologyencore
Examples of integrated biofeedback outcomes
Peper, E. (2015). Pain as a Contextual Experience. Townsend Letter-The Examiner of Alternative Medicine, 388, 63-66. https://townsendletter.com/peper-contextual-pain-09-11-15/
Peper, E., Booiman, A. & Harvey, R. (2025a). Pain-There is Hope. Biofeedback, 53(1), 1-9. http://doi.org/10.5298/1081-5937-53.01.16 Also, republished in Townsend Letter-Innovative Health Perspectives. https://townsendletter.com/pain-there-is-hope/
Peper, E., Chen, S., Heinz, N. & Harvey, R. (2023). Hope for menstrual cramps (dysmenorrhea) with breathing. Biofeedback,. 51(2), 44–51. https://doi.org/10.5298/1081-5937-51.2.04
Peper, E. & Cohen, T. (2017). Inhale to breathe away pelvic floor pain and enjoy intercourse. Biofeedback, 45(1), 21–24. https://doi.org/10.5298/1081-5937-45.1.04
Peper, E., Cosby, J., & Almendras, M. (2022a). Healing chronic back pain. NeuroRegulation, 9(3), 164–172. https://doi.org/10.15540/nr.9.3.164
Peper, E., Covell, A., & Matzembacker, N. (2021). How a chronic headache condition became resolved with one session of breathing and posture coaching. NeuroRegulation, 8(4), 194–197. https://doi.org/10.15540/nr.8.4.194
Peper, E. & Harvey, R. (2008). From technostress to technohealth. Japanese Journal of Biofeedback Research, 35(2), 107-114. https://www.jstage.jst.go.jp/article/jjbf/35/2/35_KJ00005060045/_pdf
Peper, E., Harvey, R., Chen, S., & Heinz, N. (2025b). Practicing diaphragmatic breathing reduces menstrual symptoms both during in-person and synchronous online teaching. Applied Psychophysiology and Biofeedback. https://do.org/10.1007/s10484-025-09745-7
Peper, E., Harvey, R., Cuellar, Y., & Membrila, C. (2022b). Reduce anxiety. NeuroRegulation, 9(2), 91–97. https://doi.org/10.15540/nr.9.2.91
Peper, E., Martinez Aranda, P., & Moss, E. (2015). Vulvodynia treated successfully with breathing biofeedback and integrated stress reduction: A case report. Biofeedback. 43(2), 103-109. https://doi.org/10.5298/1081-5937-43.2.04
Peper, E., Mason, L., Harvey, R., Wolski, L, & Torres, J. (2020). Can acid reflux be reduced by breathing? Townsend Letters-The Examiner of Alternative Medicine, 445/446, 44-47. https://www.townsendletter.com/article/445-6-acid-reflux-reduced-by-breathing/
Peper, E., Oded, Y., & Harvey, R. (2024). Quick somatic rescue techniques when stressed. Biofeedback, 52(1), 18–26. https://doi.org/10.5298/982312
Peper, E. & Tibbitts, V. (2003). Protocol for the treatment of asthma. In: Zheng, Y. (ed). Clinical Practice of Biofeedback. Beijing: High Education Press (HEP). 163-176. ISBN 7-04-011420-8 https://biofeedbackhealth.org/wp-content/uploads/2011/01/protocol-for-asthma-treatemtn2001-china.pdf
Peper, E. & Yirmiyahu, D. (2023). Transforming a “bad eye” to an “amazing eye”: a case report and protocol. Townsend Letters. The Examiner of Alternative Medicine, Saturday, July 29, 2023 https://townsendletter.com/transforming-a-bad-eye-to-an-amazing-eye-a-case-report-and-protocol/
Breathing for Health: Four Part Audio Series for Regeneration and Well-Being
Posted: March 12, 2026 Filed under: attention, behavior, Breathing/respiration, CBT, emotions, healing, health, meditation, mindfulness, Pain/discomfort, relaxation, self-healing, stress management, Uncategorized | Tags: audio files, health, meditation, mental-health, mindfulness, wellness 1 CommentAdapted from Peper, E. (1990). Breathing for Health with Biofeedback. Montreal: Thought Technology Ltd and produced by Larry Klein.

Breathing is the most intimate rhythm of life. From the moment we are born until our last breath, our breath is always there—quietly sustaining us. And yet, most of the time, we are unaware of how we breathe or how profoundly it shapes our health. Learn how to use your breath to optimize your health and enhance your well-being.
Dysfunctional breathing patterns contribute significantly to a range of illnesses, ranging from chronic pain and anxiety to fatigue and stress-related disorders. For example, when anxious, breathing often becomes rapid and shallow; when calm, breathing tends to slow and deepen. Symptoms can often be reduced, and health, resilience, and a deep sense of well-being can be enhanced after mastering and implementing effortless breathing. Breathing affects the mind, body, emotions, and spirit; when you change your breathing, you change your state of being.
The audio series by Erik Peper was conceived and produced by Larry Klein co-founder of Thought Technology, Ltd in 1990 to make the science and practice of breathing with biofeedback accessible to everyone. Although it was recorded more than 35 years ago, the principles and instructions remain as relevant and evidence-based today as they were then.
It was designed to help you observe your own breathing patterns and cultivate the foundational skill of effortless diaphragmatic breathing. Even more importantly, it guides you in integrating this breathing pattern into daily activities so that it becomes your default—whether you are working, speaking, exercising, or resting.
The discussion and guided practices are both simple and profound. When you change how you breathe, you change how you regulate yourself. Breathing both reflects and influences your physiology, emotions, and cognitions—often outside of conscious awareness.
As you listen to and practice the techniques in this four-part audio series, you will develop greater awareness, appreciation, and mastery of effortless breathing. Enjoy applying these practices in everyday life until they become automatic. Like any skill, effortless breathing is learned through gentle, consistent practice—practice makes permanent.
Part 1: Background Information on Breathing
Listen once to understand the scientific foundations and underlying rationale
Part 2: Learning Slow Diaphragmatic Breathing
Listen repeatedly and practice consistently until the skill becomes natural, effortless, and reliable.
Part 3: Integrating Breathing in All Conditions
Alternate between Parts 2 and 3. Practice during everyday activities so the skill generalizes beyond formal sessions and becomes your default way of breathing.
Part 4: Integrating Breathing, Imagery and Meditation for Health
Experience how guided imagery and meditative awareness deepen and amplify the benefits of effortless breathing.
Additional Recommended Blogs to Support the Learning and Generalization of Effortless Breathing
Additional Recommended Blogs: How Breathing Can Help Relieve Pain
Breathe Away Menstrual Pain- A Simple Practice That Brings Relief *
Posted: November 22, 2025 Filed under: attention, behavior, biofeedback, Breathing/respiration, cognitive behavior therapy, education, emotions, Neck and shoulder discomfort, Pain/discomfort, posture, relaxation, self-healing, stress management, Uncategorized | Tags: dysmenorrhea, health, meditation, menstrual cramps, mental-health, mindfulness, wellness 2 CommentsAdapted from: Peper, E. Harvey, R., Chen, & Heinz, N. (2025). Practicing diaphragmatic breathing reduces menstrual symptoms both during in-person and synchronous online teaching. Applied Psychophysiology and Biofeedback, Published online: 25 October 2025. https://rdcu.be/eMJqt https://doi.org/10.1007/s10484-025-09745-7
“Once again, the pain starts—sharp, deep, and overwhelming—until all I can do is curl up and wait for it to pass. There’s no way I can function like this, so I call in sick. The meds take the edge off, but they don’t really fix anything—they just mask it for a little while. I usually don’t tell anyone it’s menstrual pain; I just say I’m not feeling well. For the next couple of days, I’m completely drained, struggling just to make it through.
Many women experience discomfort during menstruation, from mild cramps to intense, even disabling pain. When the pain becomes severe, the body instinctively responds by slowing down—encouraging rest, curling up to protect the abdomen, and often reaching for medication in hopes of relief. For most, the symptoms ease within a day or two, occasionally stretching into three, before the body gradually returns to balance.
Another helpful approach is to practice slow abdominal breathing, guided by a breathing app FlowMD. In our study led by Mattia Nesse, PhD, in Italy, the response of one 22-year-old woman illustrated the power of this simple practice.
“Last night my period started, so I was a bit discouraged because I knew I’d get stomach pain, etc. On the other hand, I said, “Okay, let’s see if the breathing works,” and it was like magic — incredible. I’ll need to try it more times to understand whether it consistently has the same effect, but right now it truly felt magical. Just 3 minutes of deep breathing with the app were enough, and I’m not saying I don’t feel any pain anymore, but it has decreased a lot, so thank you! Thank you again for this tool… I’m really happy!”
The Silent Burden of Menstrual Pain
Menstrual pain, or dysmenorrhea, affects most women at some point in their lives — often silently. For many, the monthly cycle brings not only physical discomfort but also shame, fatigue, and interruptions to work or school. It is one of the leading causes of absenteeism and reduced productivity worldwide (Itani et al., 2022; Thakur & Pathania, 2022). In addition, the estimated health cost ranged from US $1367 to US$ 7043 per year (Huang et al., 2021). Yet, despite its prevalence, most women are never taught how to use their own physiology to ease these symptoms.
The Study (Peper et al, 2025)
Seventy-five university women participated across two upper-division Holistic Health courses. Forty-nine practiced 30 minutes per day of breathing and relaxation over five weeks as well as practicing the moment they anticipated or felt discomfort; twenty-six served as a comparison group without a specific daily self-care routine. Students rated change in menstrual symptoms on a scale from –5 (“much worse”) to +5 (“much better”). For the detailed steps in training, see the blog: https://peperperspective.com/2023/04/22/hope-for-menstrual-cramps-dysmenorrhea-with-breathing/ (Peper et al., 2023).
What changed
The results were striking. Women who practiced breathing and relaxation showed significant decrease in menstrual symptoms compared to the non-intervention group (p = 0.0008) as shown in Figure 1.
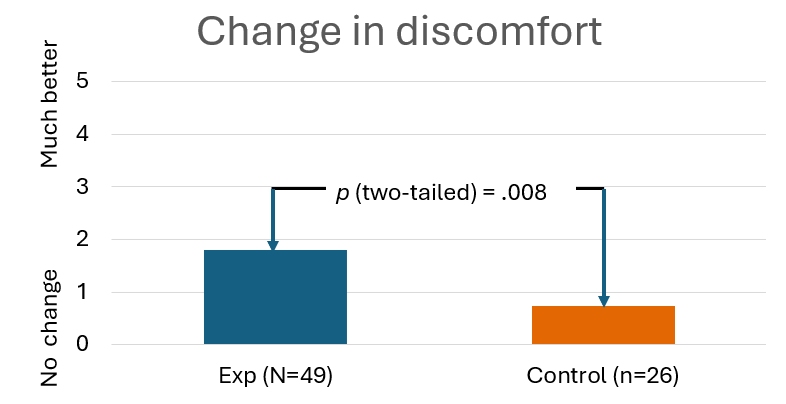
Figure 1. Decrease in menstrual symptoms as compared to the control group after implementing slow diaphragmatic breathing.
Why does breathing and posture change have a beneficial effect?
When you stay curled up, your abdomen becomes compressed, leaving little room for the lower belly to relax or for the diaphragm to move freely. The result? Tension builds, and pain often increases.
To reverse this, create space for relaxation. Gently loosen your waist and let your abdomen expand as you inhale. Uncurl your body—lengthen your spine and open your chest, as shown in Figure 2. With each easy breath, you invite calm and allow your body to shift from tension to ease.

Figure 2. Curling up compresses the abdomen and prevents relaxation of the lower belly. In contrast, lying flat with the body gently expanded allows the abdomen to move freely with each breath, which can help reduce menstrual discomfort.
In contrast, slow abdominal or diaphragmatic breathing activates the body’s natural relaxation response. It quiets the stress-driven sympathetic nervous system, calms the mind, and improves circulation in the abdominal area. With each slow breath in, the abdomen gently expands while the pelvic floor and abdominal muscles relax. As you exhale, these muscles naturally tighten slightly, helping to massage and move blood and lymph through the abdominal region. This rhythmic movement supports healing and ease, as illustrated in Figure 3.
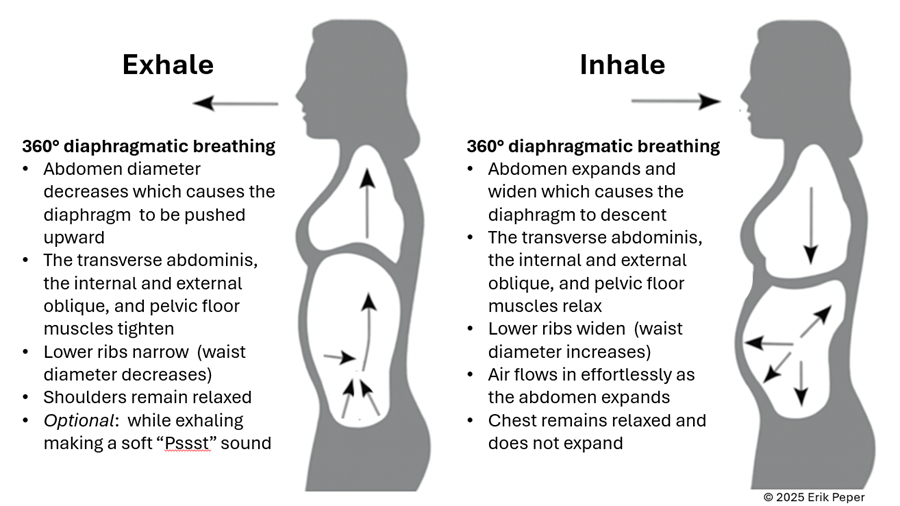
Figure 3. The dynamic process of diaphragmatic breathing.
The process of slower, lower diaphragmatic breathing
When lying down, rest comfortably on your back with your legs slightly apart. Allow your abdomen to rise naturally as you inhale and fall as you exhale. As you breathe out, imagine the air flowing through your abdomen, down your legs, and out through your feet. To deepen this sensation, you can ask a partner to gently stroke from your abdomen down your legs as you exhale—helping you sense the flow of release through your body.
Gently focus on slow, effortless diaphragmatic breathing. With each inhalation, your abdomen expands, and the lower belly softens. As you exhale, the abdomen gently goes down pushing the diaphragm upward and allowing the air to leave easily. Breathing slowly—about six breaths per minute—helps engage the body’s natural relaxation response.
If you notice that your breath is staying high in your chest instead of expanding through the abdomen, your symptoms may not improve and can even increase. One participant experienced this at first. After learning to let her abdomen expand with each inhalation while keeping her shoulders and chest relaxed, her next menstrual cycle was markedly easier and far less uncomfortable. The lesson is clear: technique matters.
“During times of pain, I practiced lying down and breathing through my stomach… and my cramps went away within ten minutes. It was awesome.” — 22-year-old college student
“Whenever I felt my cramps worsening, I practiced slow deep breathing for five to ten minutes. The pain became less debilitating, and I didn’t need as many painkillers.” — 18-year-old college student
These successes point out that it’s not just breathing — it’s how you breathe by providing space for the abdomen to expand during inhalation.
Practice: How to Do Diaphragmatic Breathing
- Find a quiet space. Lie on your back or sit comfortably erect with your shoulders relaxed.
- Place one hand on your chest and one on your abdomen.
- Inhale slowly through your nose for about 3–4 seconds. Let your abdomen expand as you breathe in — your chest should remain relaxed.
- Exhale gently through your mouth for 4—6 seconds, allowing the abdomen to fall or constrict naturally.
- As you exhale imagine the air moving down your arms, through your abdomen, down your legs, and out your feet
- Practice daily for 20 minutes and also for 5–10 minutes during the day when menstrual discomfort begins.
- Add warmth. Placing a warm towel or heating pad over your abdomen can enhance relaxation while lying on your back and breathing slowly.
With regular practice and implementing it during the day when stressed, this simple method can reduce cramps, promote calm, and reconnect you with your body’s natural rhythm.
Implement the ABCs during the day
The ABC sequence—adapted from the work of Dr. Charles Stroebel, who developed The Quieting Reflex (Stroebel, 1982)—teaches a simple way to interrupt stress reactions in real time. The moment you notice discomfort, pain, stress, or negative thoughts, interrupt the cycle with a simple ABC strategy:
A — Adjust your posture
Sit or stand tall, slightly arch your lower back and allowing the abdomen to expand while you inhale and look up. This immediately shifts your body out of the collapsed “defense posture’ and increases access to positive thoughts (Tsai et all, 2016; Peper et al., 2019)
B — Breathe
Allow your abdomen to expand as you inhale slowly and deeply. Let it get smaller as you exhale. Gently make a soft hissing sound as you exhale while helps the abdomen and pelvic floor to tighten. Then allow the abdomen to relax and widen which without effort draws the air in during inhalation. As you exhale, stay tall and imagine the air flowing through you and down your legs and out your feet.
C — Concentrate
Refocus your attention on what you want to do and add a gentle smile. This engages positive emotions, the smile helps downshift tension.
The video clip guides you through the ABCs process.
Integrate the breathing during the day by implementing your ABCs
When students practice relaxation technique and this method, they reported greater reductions in symptoms compared with a control group. By learning to notice tension and apply the ABC steps as soon as stress arises, they could shift their bodies and minds toward calm more quickly, as shown in Figure 4.

Figure 4. Change in symptoms after practicing a sequential relaxation and breathing techniques for four weeks.
Takeaway
Menstrual pain doesn’t have to be endured in silence or masked by medication alone. By practicing 30 minutes of slow diaphragmatic breathing daily and many times during the day, women may be able to reduce pain, stress, and discomfort — while building self-awareness and confidence in their body’s natural rhythms thereby having the opportunity to be more productive.
We recommend that schools and universities include self-care education—especially breathing and relaxation practices—as part of basic health curricula as this approach is scalable. Teaching young women to understand their bodies, manage stress, and talk openly about menstruation can profoundly improve well-being. It not only reduces physical discomfort but also helps dissolve the stigma that still surrounds this natural process,
Remember: Breathing is free—available anytime, anywhere and is helpful in reducing pain and discomfort. (Peper et al., 2025; Joseph et al., 2022)
See the following blogs for more in-depth information and practical tips on how to learn and apply diaphragmatic breathing:
REFERENCES
Itani, R., Soubra, L., Karout, S., Rahme, D., Karout, L., & Khojah, H.M.J. (2022). Primary Dysmenorrhea: Pathophysiology, Diagnosis, and Treatment Updates. Korean J Fam Med, 43(2), 101-108. https://doi.org/10.4082/kjfm.21.0103
Huang, G., Le, A. L., Goddard, Y., James, D., Thavorn, K., Payne, M., & Chen, I. (2022). A systematic review of the cost of chronic pelvic pain in women. Journal of Obstetrics and Gynaecology Canada, 44(3), 286–293.e3. https://doi.org/10.1016/j.jogc.2021.08.011
Joseph, A. E., Moman, R. N., Barman, R. A., Kleppel, D. J., Eberhart, N. D., Gerberi, D. J., Murad, M. H., & Hooten, W. M. (2022). Effects of slow deep breathing on acute clinical pain in adults: A systematic review and meta-analysis of randomized controlled trials. Journal of Evidence-Based Integrative Medicine, 27, 2515690X221078006. https://doi.org/10.1177/2515690X221078006
Peper, E., Booiman, A. & Harvey, R. (2025). Pain-There is Hope. Biofeedback, 53(1), 1-9. http://doi.org/10.5298/1081-5937-53.01.16
Peper, E., Chen, S., Heinz, N., & Harvey, R. (2023). Hope for menstrual cramps (dysmenorrhea) with breathing. Biofeedback, 51(2), 44–51. https://doi.org/10.5298/1081-5937-51.2.04
Peper, E., Harvey, R., Chen, S., & Heinz, N. (2025). Practicing diaphragmatic breathing reduces menstrual symptoms both during in-person and synchronous online teaching. Applied Psychophysiology and Biofeedback. Published online: 25 October 2025. https://rdcu.be/eMJqt https://doi.org/10.1007/s10484-025-09745-7
Peper, E., Harvey, R., & Hamiel, D. (2019). Transforming thoughts with postural awareness to increase therapeutic and teaching efficacy. NeuroRegulation, 6(3),153-169. https://doi.org/10.15540/nr.6.3.1533-1
Stroebel, C. (1982). The Quieting Reflex. New York: Putnam Pub Group. https://www.amazon.com/Qr-Quieting-Charles-M-D-Stroebel/dp/0399126570/
Thakur, P. & Pathania, A.R. (2022). Relief of dysmenorrhea – A review of different types of pharmacological and non-pharmacological treatments. MaterialsToday: Proceedings.18, Part 5, 1157-1162. https://doi.org/10.1016/j.matpr.2021.08.207
Tsai, H. Y., Peper, E., & Lin, I. M. (2016). EEG patterns under positive/negative body postures and emotion recall tasks. NeuroRegulation, 3(1), 23-27. https://doi.org/10.15540/nr.3.1.23
*Edited with the help of ChatGPT 5
Healing from the Inside Out: How Your Mind–Body Shapes Pain
Posted: June 9, 2025 Filed under: attention, behavior, Breathing/respiration, CBT, emotions, healing, health, mindfulness, Pain/discomfort, placebo, self-healing, Uncategorized | Tags: health, meditation, mental-health, mindfulness, Sufism, yoga 2 CommentsAdapted from Peper, E., Booiman, A. C., & Harvey, R. (2025). Pain-There is Hope. Biofeedback, 53(1), 1-9. http://doi.org/10.5298/1081-5937-53.01.16
Pain is more than a physical sensation—it’s shaped by our breath, thoughts, emotions, and beliefs. A striking example: a four-year-old received a vaccination with no pain, revealing the disconnect between what science knows about pain relief and what’s practiced.
The article highlights five key ways to reduce pain:
- Exhale during the painful moment – This activates the parasympathetic nervous system, calming the body. A yogi famously demonstrated this by pushing skewers through his tongue without bleeding or feeling pain.
- Create a sense of safety – Feeling secure can lessen pain and speed healing. Sufi mystics have shown this by pushing knives through their chest muscles without long-term damage, often healing rapidly.
- Distract the mind – Shifting focus can ease discomfort.
- Reduce anticipation – Fear of pain often amplifies it.
- Explore the personal meaning of pain – Understanding what pain symbolizes can shift how we experience it.
The blog also explores how the body regulates pain through mechanisms which influence inflammation and pain signals. In the end, hope, trust, and acceptance, along with mindful breathing, healing imagery, and meaningful engagement, emerge as powerful tools not just to reduce pain—but to promote true healing.
I took my four-year-old daughter to the pediatrician for a vaccination. As the nurse prepared to administer the shot in her upper arm. I instructed my daughter to exhale while breathing, understanding that this technique could influence her perception of pain. Despite my efforts, my daughter did not follow my instructions. At that point, the nurse interjected and said, “Please sit in front of your daughter.” Then turned to my daughter and said, “Do you see your father’s curly hair? Do you think you could blow the curls to move them back and forth?” My daughter thought this playful game was fun! As she blew at my hair, the curls moved back and forth while the nurse administered the injection. My daughter was unaware that she had received the shot and felt no pain.
My experience as a father and as a biofeedback practitioner was enlightening–it demonstrated the difference between theoretical knowledge of breathing techniques associated with pain perception and practical applications of clinical skills used by a pediatric nurse practitioner while administering an injection with children. An obvious question raised is: What processes are involved in the perception of pain?
There are many factors influencing pain perception, such as physical/physiological, behavioral and psychological/emotional factors related to the injection as described by St Clair-Jones et al., (2020). Physical and physiological considerations include device type such as needle gauge size as well as formulation volume and ingredients (e.g., adjuvants, pH, buffers), fluid viscosity, temperature, as well as possible sensitivity to coincidental exposures associated with an injection (e.g., sensitivity to latex exam gloves or some other irritant in the injection room).
There are overlapping physical and behavioral-related moderators that include weight and body fat composition, proclivity towards movements (e.g., activity level or ‘squirminess’), as well as co-morbid factors such as whether the person has body sensitization due to rheumatoid arthritis and/or fibromyalgia, for example. Other behavioral factors include a clinician selecting the injection site, along with the angle, speed or duration of injection. Psychological influences center around patient expectations including injection-anxiety or needle phobia, pain catastrophizing, as well as any nocebo effects such as white-coat hypertension.
Although the physical, behavioral and psychological categories allow for considering many physical and physiological factors (e.g., product-related factors), behavioral factors (e.g., injection-related behaviors) and psychological factors (e.g., person-related psychological attitudes, beliefs, cognitions and emotions), this article focuses on a figurative recipe for success associated with benefits of simple breathing to reduce pain perceptions.
Of the many categories of consideration related to pain perceptions, following are five key ‘recipe ingredients’ that contributed to a relatively painless experience:
- Exhaling During Painful Stimuli: Exhaling during a painful stimulus can activate parts of the parasympathetic nervous system leading to promotion of self-healing.
- Creating a Sense of Safety: Ensuring that the child feels safe and secure is crucial in managing pain. My lack of worry and concern and the nurse’s gentle and engaging approach created a comforting environment for my daughter.
- Using Distraction: Distraction techniques, such as focusing on the movement of the curls of the hair served to redirect my daughter’s attention away from the anticipated pain.
- Reducing Anticipation of Pain: My daughter’s previous visits were always enjoyable and as a parent, I was not anxious and was looking forward to the pediatrician visit and their helpful advice.
- Understanding the Personal Meaning of Pain: The approach taken by the nurse allowed the injection to be perceived as a non-event, thereby minimizing the psychological impact of the pain.
Exhaling During Painful Stimuli
Exhaling during painful stimuli facilitates a reduction in discomfort through several physiological mechanisms. During exhalation the parasympathetic nervous system is activated, which slows the heart rate and promotes relaxation, regeneration, reduces anxiety, and may counteract the effects of pain (Magnon et al., 2021). Breathing moderation of discomfort is observable through heart rate variability associated with slow, resonant breathing patterns, where heart rate increases with inhalation and decreases with exhalation (Lehrer & Gevirtz, 2014; Steffen et al., 2017). Physiological studies show that slow, resonant breathing at approximately six breaths per minute for adults, and a little faster for young children, causes the heart rate to increase during inhalation and decrease during exhalation, as illustrated in Figure 1.

Figure 1. Changes in heart rate as modulated by slower breathing at about six breaths per minute
One can experience how breathing affects discomfort when taking a cold shower under two conditions: As the cold water hits your skin: (1) gasping and holding your breath versus (2) exhaling slowly as the cold water hits you. Most people will report that slowly exhaling feels less uncomfortable, though they may still prefer a warm shower.
An Exercise for Use During Medical Procedures: Paring the procedure with inhalation and exhalation
A simple breathing technique can be used to reduce the experience of pain during a procedure or treatment, or during uncomfortable movement post-injury or post-surgery. Physiologically, inhalation tends to increase heart rate and sympathetic activation while exhalation reduces heart rate and increases parasympathetic activity. Often inhalation increases tension in the body, while during exhalation, one tends to relax and let go. The goal is to have the patient practice longer and slower breathing so that a procedure that might be uncomfortable is initiated during the exhalation phase. Applications of long, slow breathing techniques include having blood drawn, insertion of acupuncture needles in tender points, or movement that causes discomfort or pain. Slowly breathing is helpful in reducing many kinds of discomfort and pain perceptions (Joseph et al., 2022; Jafari et al., 2020).
Implementing the technique of exhaling during painful experiences can be deceptively simple yet challenging. When initially practicing this technique, the participants often try too hard by quickly inhaling and exhaling as the pain stimulus occurs. The effective technique involves allowing the abdomen to expand while inhaling, then allowing exhaled air to flow out while simultaneously relaxing the body and smiling slightly, and initiating the painful procedure only after about 25 percent of the air is exhaled.
Some physiological mechanisms that explain how slow breathing influences on pain perceptions have focused on baroreceptors that are mechanically sensitive to pressure and breathing dynamics. According to Suarez-Roca et al. (2021, p 29): “Several physiological factors moderate the magnitude and the direction of baroreceptor modulation of pain perception, including: (a) resting systolic and diastolic AP, (b) pain modality and dimension, (c) type of activated vagal afferent, and (d) the presence of a chronic pain condition It supports the parasympathetic activity that exert an anti-inflammatory influence, whereas the sympathetic activity is mostly pro-inflammatory. Although there are complex physiological interactions between cardiorespiratory systems, arterial pressure and baroreceptor sensitivity that influence pain perceptions, this report focuses on simpler reminders, such as creating a sense of safety for people as a result of better breathing techniques.
Creating a Sense of Safety
My young daughter did not know what to expect and totally trusted me and I was relaxed because the purpose was to enhance my daughter’s future health by giving her a vaccination to prevent being sick at a future time. Often, a parent’s anxiety is contagious to the child since expectations and emotional states influence the experience of medical procedures and pain (Sullivan et al., 2021). For my daughter, the nurse’s calm and confident demeanor contributed to a safe and reassuring environment. As a result, she was more engaged in a playful distraction, blowing at my hair, rather than focusing on the impending shot. This observation underscores an important psychological principle: when individuals do not anticipate pain and feel safe, they are more likely to experience surprise rather than distress. Conversely, anticipation of pain can amplify the perception of discomfort.
For instance, many people have experienced heightened anxiety at the dentist, where they may feel the pain of the needle before it is inserted. Anticipation evocates a past memory of pain that triggers a defensive reaction, increasing sympathetic arousal and sharpening awareness of potential danger. By providing the experience of feeling of safety, parents, caretakers, and medical professionals can play a crucial role in reducing the perceived pain of medical interventions.
Using Distraction
It is inherently difficult to attend to two tasks simultaneously; thus, focusing one’s attention on one task often diminishes awareness of pain and other stimuli (Rischer et al., 2020). For instance, when the nurse asked my daughter to see if she could blow hard enough to make the curls move back and forth, this task captured her attention in a fun and multisensory way. She was engaged visually by the movement of the curls, audibly by the sound of the rushing air, physically by the act of exhalation, and cognitively by following the instructions. Additionally, her success in moving the curls reinforced the activity as a positive and enjoyable experience.
In contrast, it is challenging to allow oneself to be distracted when anticipating discomfort, as numerous cues can continuously refocus attention on the procedure that may induce pain. This experience is akin to attempting to tickle oneself, which typically fails to elicit laughter due to the predictability and lack of external stimulation. Most of us have experienced how challenging it is to be self-directive and not focus on the sensations during dental procedures as discussed in the overview of music therapy for use in dentistry by Bradt and Teague (2018). The challenges are illustrated by my own experience during a dental cleaning
During a dental cleaning, I often attempt to distract myself by mentally visualizing the sensation of breathing down my legs while repeating an internal mantra or evoking joyful memories. Despite these efforts, I frequently find myself attending to the sound of the ultrasonic probe and the sensations in my mouth. To manage this distraction more effectively, I have found that external interventions such as listening to music or an engaging audio story through earphones is more beneficial.
From this perspective, we wished that the dentist could implement an external intervention by collaborating with a massage therapist to provide a simultaneous foot massage during the teeth cleaning. This dual stimulation would offer enough competing sensations to divert attention from the dental procedure to the comfort of the foot massage.
Reducing Anticipation of Pain
A crucial factor in the experience of pain is the anticipation and expectation of discomfort, which is often shaped by previous experiences (Henderson et al., 2020; Reicherts et al., 2017). When encountering a novel experience, we might interpret the sensations as novel rather than painful. Similar phenomena can be observed in young children when they fall or get hurt on the playground. They may initially react with surprise or shock and may look for their caretaker. Depending the reaction of their caregiver, they may begin to cry or they might cry briefly, stop and resume playing.
Conversely, the anticipation of pain can heighten sensitivity to any stimuli, causing them to be automatically perceived as painful. Anticipatory responses function as a form of mental rehearsal, where the body responds in a manner similar to the actual experience of pain. For example, Peper, et al. (2015) showed that when a pianist imagined playing the piano, her forearm flexor and extensor muscles exhibited slight contractions, even though there was no observable movement in her arm and the pianist was unaware of these contractions (see Figure 2).

Figure 2. The covert SEMG increase in forearm SEMG as the participant imagined playing the piano (reproduced by permission from Peper et al., 2015).
These kind of muscle reactions are also visible in sportsmen. For example, while mentally racing a lap on a motorbike, the arm muscles act like as if the person is racing in the dust of the circuit (Booiman 2018). The blood flow (BVP) and blood vessels are reacting even quicker than muscle tension on thoughts and expected (negative) experiences.
These findings underscore how anticipatory responses can mirror actual physical experiences, providing insights into how anticipation and expectancy can modify pain perception (Henderson et al., 2020). Understanding these mechanisms allows for the development of interventions aimed at managing pain through the modification of expectations and the introduction of distraction techniques.
The Personal Meaning of Pain (adapted from Peper, 2015)
The personal meaning of pain is a complex construct that varies significantly based on context and individual perception. For example, consider the case of a heart attack. Initially, the person might experience chest pain and dismiss it, which can be attributed to societal norms where people are conditioned to ignore pain. However, once the pain is assumed or diagnosed to be a heart attack, the same pain may become terrifying as it may signify the potential for life-threatening consequences. Following bypass surgery, the pain might actually be worse, but it is now reframed positively as a sign of the surgery’s success and a symbol of hope for survival. Thus, the meaning of pain evolves from one of fear to one of reassurance and recovery.
This notion that pain is defined by the context in which it occurs is crucial (Carlino et al., 2014). For instance, childbirth, despite being intensely painful, is understood within the context of a natural and temporary process that leads to the birth of a child. This perception is often reinforced nonverbally by a supportive midwife or doula. It may be helpful if the midwife or doula has given birth herself. Without words she communicates, “This is an experience that you can transcend, just as I did.” Psychologically/emotionally, the pain serves a higher purpose, to deliver a child into the world, which may also make the pain more bearable. There is a reward, namely the child. In addition, women who have had training and information about the process of childbirth have a significant faster delivery (about 2 hours faster).
Piercing the body without reporting pain or bleeding
To further illustrate this concept, Peper et al. (2006) and Kakigi et al. (2005) physiologically monitored the experiences of a Japanese Yogi Master, Mitsumasa Kawakami,who performed voluntary body piercing with unsterilized skewers, as depicted in Figure 3 (Peper, 2015).

Figure 3. Demonstration Japanese Yogi Master, Mitsumasa Kawakami, voluntary piercing the tongue and neck with unsterilized skewers while experiencing no pain, bleeding or infection (reproduced by permission from Peper et al., 2006).
See the video recording of tongue piercing study recorded November 11, 2000, at the annual Biofeedback Society Meeting of California, Monterey, CA, https://youtu.be/f7hafkUuoU4 (Peper & Gunkelman, 2007).
Despite the visual discomfort of seeing this procedure, physiological data from pulse, EEG and breathing patterns revealed that the yogi did not experience pain. During the piercing, his heart rate was elevated, his electrodermal activity was low and unresponsive, and his EEG showed predominant alpha waves, indicating a state of focused meditation rather than pain. This study suggests that conscious self-regulation, rather than dissociation, can be employed to control attention and responsiveness to painful stimuli and possibly benefit individuals with chronic pain (Peper et al., 2005).
A similar phenomenon was observed among a spiritual gathering of Kasnazani Sufi initiates in Amman, Jordan and physiologically monitored during demonstrations as part of a scientific meeting. The Kasnazani order is a branch of Sufism that has gained widespread popularity in Iraq and Iran, particularly among the Kurdish population. What sets the Kasnazani order apart is its inclusive approach—it welcomes both Sunni and Shia Muslims, making no distinction between them. During spiritual gatherings, some followers perform acts that might seem extreme to outsiders: piercing their bodies. These acts are seen as expressions of deep spiritual devotion and are performed in a state believed to be beyond normal physical sensation. With the permission of their Sheikh Mohammed Abdul Kareem Kasnazani, they pierced their face, neck arms, or chest and reported no pain or bleeding and heal quickly, as shown in Figure 4.

Figure 4. Voluntary piercing and with unsterilized skewers by Sufi initiates and subsequent tissue healing after 14 hours.
See the video recording of the actual piercing study organized by Erik Peper and Howard Hall with Thomas Collura recording the QEEG at the 2013 Annual Scientific Meeting of the Association for Applied Psychophysiology and Biofeedback, Portland, OR (Peper & Hall, 2013; Collura et al., 2014), https://www.youtube.com/watch?v=56nLZyG87oc
What Factors Decrease the Experience of Pain and Promote Rapid Healing with the Absence of Bleeding?
In the case of the Kasnazani Sufis, they framed their experience as a normal, spiritual phenomenon that occurs in a setting of religious faith and total trust in their spiritual leader (Hall, 2011). The Sufis reported that they had permission and support from their master, Sheikh Mohammed Abdul Kareem Kasnazani. Thus, they felt totally safe and protected—they had no doubt they could experience the piercing with reasonable composure and that their bodies would totally heal. Even if pain occurred, it was not to be feared but part of the process. The experience may be modulated by the psychological context of the group, the drumming, and the chanting. The phenomenon was not simply a matter of belief; they knew that healing would occur because they had seen it many times in the past. The knowledge that healing would occur rapidly was transmitted as a felt sense in the group that this is possible and following the expected normal pattern.
The most impressive finding was that the physiology markers (heart rate, skin conductance, and breathing) were normal and there was no notable change (Booiman et al., 2015; Peper & Hall, 2013) and the QEEG indicated the inhibition of pain (Collura et al., 2014).
Clinical implications
These observations underscore that the context of pain—whether through personal meaning, spiritual belief, or communal support—can significantly alter its perception and management. This concept is also reflected in clinical settings, where a lack of diagnosis or acknowledgment of pain can exacerbate suffering. An isolated individual, alone at night with the physical sensation of pain, may find the pain tremendously stressful, which tends to intensify the experience. In this situation, there are concerns about the future: “It may get worse, it will not go away, I’m going to die from this, maybe I’ll die alone,” and the worry continues.
If one can let go of these thoughts, breathe through the pain, relax the muscles and experience a feeling of hope, the pain is often reduced. On the other hand, focusing on the pain may intensify it. On the other hand, the meaning of pain implies survival or hope as sometimes is observed in injured soldiers. In context of the hospital setting: “I have survived and I am safe.”
What are the implications of these experiences in clinical settings in which the patient is in constant pain and yet has not received an accurate diagnosis? Or, in cases in which the patient has a diagnosis, such as fibromyalgia, but treatment has not reduced the pain significantly? Experiencing pain or illness that goes undiagnosed, and/or that is not acknowledged, may increase the level of stress and tension, which can contribute to more pain and discomfort. As long as we are resentful/angry/resigned to the pain or especially to the event that we believe has caused the pain, the pain often increases. Another way to phrase this is that chronic sympathetic arousal increases the sensitivity to pain and reduces healing potential (Kyle & McNeil, 2014).
Acknowledgement means having an accurate diagnosis, validating that the pain experience is legitimate and that it is not psychosomatic (imagined), because that simply makes the experience of pain worse. Once the patient has a more accurate diagnosis, treatment may be possible.
When one has constant, chronic, or unrelenting pain, this evokes hopelessness and the patient is more likely to get depressed (Sheng et al., 2017; Meda et al., 2022). The question is, What can be done? The first step for the patients is to acknowledge to themselves that it does not mean that the situation is unsolvable. It is important to focus on other options for diagnosis and treatment and take one’s own lead in the healing/recovery process. We have observed that a creative activity that uses the signals of pain to evoke images and thoughts to promote healing may reduce pain (Peper et al., 2022). Pain awareness may be reduced when the person initiates actions that contribute to improving the well-being of others.
Overall, pain appears to decrease when a person accepts without resignation what has happened or is happening. A useful practice that may change the pain experience is to do an appreciation practice. Namely, appreciate what that part of the body has done for you and how so often in the past you may have abused it. For example, if you experience hip pain, each time you are aware of the pain, thank the hip for all the work it has done for you in the past and how often you may have neglected it. Keep thanking it for how it has supported you.
Pain often increases when the person is resentful or wished that what has happened had not happened (Burns et al., 2011). If the person can accept where they are and focus on the new opportunities and new goals can achieve, pain may still occur; however, the quality is different. Focus on what you can do and not on what you cannot do. See Janine Shepherd’s 2012 empowering TED talk, “A broken body isn’t a broken person.”
Conclusion
The primary lessons from studying the yogi and the Sufis are the concepts that a sense of safety, acceptance, and purpose can transform the experience of pain. Expressing confidence in a patient’s recovery prospects places the focus on their ability to recover. Incorporating these elements into clinical care may offer new avenues for addressing chronic pain and improving patient outcomes (Booiman & Peper, 2021).
We propose the first step is to create an atmosphere of hope, trust and safety and to emphasize the improvements made (even small ones). Then master effortless breathing to increase slow diaphragmatic breathing and teach clients somato-cognitive techniques to refocus their attention during painful stimuli (mindfulness) (Pelletier & Peper, 1977; Peper et al., 2022). Using the slow breathing as the overlearned response would facilitate the recovery and regeneration following the painful situation. To develop mastery and be able to apply it under stressful situations requires training and over-learning. Yoga masters overlearned these skills with many years of meditation. With mastery, patients may learn to abort the escalating cycle of pain, worry, exhaustion, more pain, and hopelessness by shifting their attention and psychophysiological responses. In clinical practice, strategies such as hypnotic induction, multisensory distraction, self-healing visualizations, and mindfulness techniques can be employed to manage pain. A foundational principle is that healing is promoted when the participant feels safe and accepted, experiences suffering without blame, and looks forward to life with meaning and purpose.
Acknowledgement
We thank Mitsumasa Kawakami, Sheikh Mohammed Abdul Kareem Kasnazani, and Safaa Saleh for their generous participation in this research and I thank our research collegues Thomas Collura, Howard Hall and Jay Gunkelman for their support and collaboration.
Listen to the expanded podcast created from this blogpost by Google Notebook LM.
References
Booiman, A.C. (2018) Posture corrections and muscle control can prevent arm pump during motocross, a case study. Beweegreden, 14(3), 24–27. https://www.researchgate.net/publication/382853342
Booiman, A. C. & Peper, E. (2021) De pijnbeleving van Kaznazanisoefi’s, wat kan de fysiotherapeut daarvan leren? Physios Vol 13 (3) pp. 32–35. https://www.physios.nl/tijdschrift/editie/artikel/t/de-pijnbeleving-van-kaznazani-soefi-s-wat-kan-de-fysiotherapeut-daarvan-leren
Booiman, A., Peper, E., Saleh, S., Collura, T., & Hall, H. (2015). Soefi piercing een andere kijk op pijnervaring en pijnmanagement. https://biofeedbackhealth.files.wordpress.com/2011/01/soefi-en-pijn-management-08-12-20131.pdf
Bradt. J. & Teague, A. (2018). Music interventions for dental anxiety. Oral Diseases, 24(3), 300–306. https://doi.org/10.1111/odi.12615
Burns, J.W., Quartana, P., & Bruehl, S. (2011). Anger suppression and subsequent pain behaviors among chronic low back pain patients: moderating effects of anger regulation style. Annals of Behavioral Medicine, 42(1), 42–54. https://doi.org/10.1007/s12160-011-9270-4
Carlino, E., Frisaldi, E., & Benedetti, F. (2014). Pain and the context. Nature Reviews Rheumatology, 10(6), 348–355. https://doi.org/10.1038/nrrheum.2014.17
Collura, T. F., Hall, H., & Peper, E. (2014). A Sufi self-piercing analyzed with EEG and sLORETA. Applied Psychophysiology and Biofeedback, 39(3–4), 293–293. https://brainmaster.com/wp-content/uploads/2020/08/AAPB_BOS05_2015_Pain_Controll.pdf
Hall, H. (2011). Sufism and healing. In Neuroscience, Consciousness and Spirituality (pp. 263–278). Springer Netherlands. https://doi.org/10.1007/978-94-007-2079-4_16
Henderson, L. A., Di Pietro, F., Youseff, A. M. , Lee, S., Tam, S., Akhter, R., Mills, E.P., Murray, G. M., Peck, C.C., & Macey, P.M. (2020). Effect of expectation on pain processing: A psychophysics and functional MRI analysis. Frontiers in Neuroscience, 14. https://doi.org/10.3389/fnins.2020.00006
Jafari, H., Gholamrezaei, A., Franssen, M., Van Oudenhove, L., Aziz, Q., Van den Bergh, O., Vlaeyen, J. W. S., & Van Diest, I. (2020). The Journal of Pain, 21(9–10), 1018−1030. https://doi.org/10.1016/j.jpain.2019.12.010
Joseph, A. E., Moman, R. N., Barman, R. A., Kleppel, D. J., Eberhart, N. D., Gerberi, D. J., Murad, M. H., & Hooten, W. M. (2022). Effects of slow deep breathing on acute clinical pain in adults: A systematic review and meta-analysis of randomized controlled trials. Journal of Evidence-Based Integrative Medicine, 27, 2515690X221078006. https://doi.org/10.1177/2515690X221078006
Kakigi, R. Nakata, H., Inui, K., Hiroe,N. Nagata, O., Honda, M., Tanaka, S., Sadato, N. & Kawakami, M. (2005). Intracerebral pain processing in a Yoga Master who claims not to feel pain during meditation. European Journal of Pain. 9(5), 581–581. https://doi.org/10.1016/j.ejpain.2004.12.006
Kyle, B. N., & McNeil, D. W. (2014). Autonomic arousal and experimentally induced pain: a critical review of the literature. Pain Research Management, 19(3),159–167. https://doi.org/10.1155/2014/536859
Lehrer, P. & Gevirtz R. (2014). Heart rate variability biofeedback: How and why does it work? Frontiers in Psychology, 5,756. https://doi.org/10.3389/fpsyg.2014.00756
Magnon, V., Dutheil, F. & Vallet, G. T. (2021). Benefits from one session of deep and slow breathing on vagal tone and anxiety in young and older adults. Scientific Reports, 11, 19267. https://doi.org/10.1038/s41598-021-98736-9
Meda, R. T., Nuguru, S .P., Rachakonda, S., Sripathi, S., Khan, M. I., & Patel, N. (2022). Chronic paininduced depression: A review of prevalence and management. Cureus,14(8):e28416. https://doi.org/10.7759/cureus.28416
Pelletier, K. R. and Peper, E. (1977). Developing a biofeedback model: Alpha EEG as a means for pain control. International Journal of Clinical and Experimental Hypnosis, 24(4), 361–371. https://doi.org/10.1080/00207147708415991
Peper, E. (2015). Pain as a contextual experience. Townsend Letter—The Examiner of Alternative Medicine, 388, 63–66. https://www.researchgate.net/profile/Erik-Peper/publication/284721706_Pain_as_a_contextual_experience/links/5657483908ae1ef9297bab71/Pain-as-a-contextual-experience.pdf
Peper, E., Cosby, J., & Almendras, M. (2022). Healing chronic back pain. NeuroRegulation, 9(3), 164–172. https://doi.org/10.15540/nr.9.3.164
Peper, E. & Gunkelman, J. (2007). Tongue piercing by a yogi: QEEG observations and implications for pain control and health. Presented at the 2007 meeting of the Biofeedback Society of California. https://www.researchgate.net/publication/382394304_Tongue_Piercing_by_a_Yogi_QEEG_Observations_and_Implications_for_Pain_Control_and_Health
Peper, E. & Hall, H. (2013). What is possible: A discussion, physiological recording and actual demonstration in voluntary pain control by Kasnazani Sufis. Presented at the 44st Annual Meeting of the Association for Applied Psychophysiology and Biofeedback. Portland, OR.
Peper, E., Kawakami, M., Sata, M. & Wilson, V.S. (2005). The physiological correlates of body piercing by a yoga master: Control of pain and bleeding. Subtle Energies & Energy Medicine Journal, 14(3), 223–237. https://biofeedbackhealth.org/wp-content/uploads/2011/01/366-663-1-sm.pdf
Peper, E., Nemoto, S., Lin, I-M., & Harvey, R. (2015). Seeing is believing: Biofeedback a tool to enhance motivation for cognitive therapy. Biofeedback, 43(4), 168–172. https://doi.org/10.5298/1081-5937-43.4.03
Peper, E., Wilson, V.E., Gunkelman, J., Kawakami, M. Sata, M., Barton, W. & Johnston, J. (2006). Tongue piercing by a yogi: QEEG observations. Applied Psychophysiology and Biofeedback. 34(4), 331–338. https://doi.org/10.1007/s10484-006-9025-3
Reicherts, P., Wiemer, J., Gerdes, A.B.M., Schulz, S.M., Pauli, P., & Wieser, M.J. (2017). Anxious anticipation and pain: The influence of instructed vs conditioned threat on pain. Social Cognitive and Affective Neuroscience, 12(4), 544–554. https://doi.org/10.1093/scan/nsw181
Rischer, K. M., González-Roldán, A. M., Montoya, P., Gigl, S., Anton, F., & van der Meulen, M. (2020). Distraction from pain: The role of selective attention and pain catastrophizing. European Journal of Pain, 24(10),1880–1891. https://doi.org/10.1002/ejp.1634
Sheng, J., Liu, S., Wang, Y., Cui, R., & Zhang, X. (2017). The link between depression and chronic pain: Neural mechanisms in the brain. Neural Plasticity, 9724371. https://doi.org/10.1155/2017/9724371
Shepherd, J. (2012). A broken body isn’t a broken person. TEDxKC. Accessed July 19, 2024. https://www.ted.com/talks/janine_shepherd_a_broken_body_isn_t_a_broken_person?subtitle=en
Steffen, P.R., Austin, T., DeBarros, A., & Brown, T. (2017). The impact of resonance frequency breathing on measures of heart rate variability, blood pressure, and mood. Frontiers in Public Health, 5, 222. https://doi.org/10.3389/fpubh.2017.00222
St Clair-Jones, A., Prignano, F., Goncalves, J., Paul, M., & Sewerin, P. (2020). Understanding and minimising injection-site pain following subcutaneous administration of biologics: A narrative review. Rheumatology and therapy, 7, 741–757. https://doi.org/10.6084/m9.figshare.13034609
Suarez-Roca, H., Mamoun, N., Sigurdson, M. I., & Maixner, W. (2021). Baroreceptor modulation of the cardiovascular system, pain, consciousness, and cognition. Comprehensive Physiology, 11(2), 1373. https://doi.org/10.1002/cphy.c190038
Sullivan, V., Sullivan, D. H. & Weatherspoon, D. (2021). Parental and child anxiety perioperatively: Relationship, repercussions, and recommendations. Journal of PeriAnesthesia Nursing, 36(3), 305–309. https://doi.org/10.1016/j.jopan.2020.08.015
Wilber, K. (1997). An integral theory of consciousness. Journal of Consciousness Studies, 4(1), 71–92. https://www.ingentaconnect.com/content/imp/jcs/1997/00000004/00000001/748
Addicted to Your Phone? How to Separate from Your Phone for a Healthy Lifestyle
Posted: April 15, 2025 Filed under: ADHD, attention, cellphone, computer, digital devices, educationj, Evolutionary perspective, health, laptops, posture, screen fatigue, self-healing, stress management, techstress, zoom fatigue | Tags: cognitive function, digital detox, health, internet, mental-health, mindfulness, multi-tasking, social isolation, social media, technology 1 CommentFrom: Peper, E. (2025 April 15). Addicted to your phone? How to separate you’re your phone for a healthy lifestyle. Townsend Letter-Innovative Health Perspectives. https://townsendletter.com/addicted-to-your-phone-how-to-separate-from-your-phone-for-a-healthy-lifestyle/; Adapted from the book by Erik Peper, Richard Harvey and Nancy Faass, TechStress-How Technology is Hijacking our Lives, Strategies for Coping and Pragmatic Ergonomics, North Atlantic Press. https://www.amazon.com/Beyond-Ergonomics-Prevent-Fatigue-Burnout/dp/158394768X/

Abstract
In today’s hyper-connected world, technology has subtly ensnared us in evolutionary traps, exploiting innate survival instincts to capture and fragment our attention. Although digital devices offer unprecedented convenience, they simultaneously may harm our mental, physical, and emotional well-being through prolonged screen exposure, digital distraction, and sedentary behavior. The unintended consequences of constant connectivity may increase anxiety, loneliness, and cognitive overload. Social media, Zoom fatigue, and media multitasking reinforce a cycle of passivity and diminished memory retention and attention span, while also reshaping our posture, behavior, and social interactions. The evidence suggests a growing mental health crisis. Yet, with conscious interventions such as digital detoxes, posture awareness, scheduled breaks, and sleep hygiene, we can reclaim our well-being. Rather than reject technology, we must learn to engage with it mindfully, respecting both our evolutionary design and the need for balance in a digital age.
Our Evolutionary Traps with Technology
Maintaining and optimizing health at the computer means re-envisioning our relationship with technology—and reclaiming health, happiness, and sanity in a plugged-in world. We have the ability to control everything from our mobile phones without needing to get up from our seat. Work, social life, and online learning all involve the mobile phone or some type of smart devices.
A convenient little device that is supposed to simplify our lives has actually trapped us into a vicious cycle of relying on it for every single thing we must do. We spend most of our day being exposed to digital displays on our smartphones, computers, gaming consoles, and other digital devices, immersing ourselves in the content we are viewing. From work related emails or tasks, to spending our free time looking at the screen for texting, playing games, and updating social media sites on a play-by-play of what we are eating, wearing, and doing. We click on one hyperlink after the other and create a vicious cycle trapped for hours until we realize we need to move. We are unaware how much time has frittered away without actually doing anything productive and then, we realize we have wasted another day.
Below are some recent estimates of ‘daily active user’ minutes per day that use a screen
• Facebook about an hour per day
• Instagram just under an hour per day
• Texting about 45 minutes per day
• Internet browsing, about 45 minutes per day
• Snapchat, about 30 minutes per day
• Twitter, about 25 minutes per day
Adolescents and college students interact with media for over 40 hours per week, or around six hours per day. That is a lot of hours spent on staring at the screen, which makes it almost impossible not to be distracted by the digital screen. In time, we rehearse a variety of physical body postures as well as a variety of cognitive and behavioral states that impact our physical, mental, emotional, and social health. The powerful audiovisual formats override our desires to do something different, that some of us become enslaved to streaming videos, playing virtual games, or texting. We then tell ourselves that the task that needs to be done, will be finished later. That later becomes never by the end of the day, since the ongoing visual and auditory notifications from our apps interrupt and/or capture our attention. This difficulty to turn away from visual or auditory stimuli roots in our survival instincts.
Each time visual or auditory stimuli occur, we automatically check it out and see if it is a friend or foe, safety or danger. It is such an automatic response that we are unaware we are reacting. The good news is that we all have experienced this compelling effect. Even when we are waiting for a response and the notification has not arrived, we may anticipate or project that there may be new information on our social media accounts, and sometimes we become disappointed when the interval between notifications is long. As one student said, “Don’t worry, they’ll respond. It’s only been 30 seconds.” Anticipating responses from the media can interrupt what we are otherwise doing. Rather than finishing our work or task, we continuously check for updates on social media, even though we probably know that there are no new important messages to which we would have to respond right away. As a result our attention span has decreased from 150 seconds in 2004 to 44 seconds in 2021 (Mark, 2023).
Unfortunately, some forms of social media interactions also lead to a form of social isolation, loneliness–sometimes called phoneliness (Christodoulou, G., Majmundar, A., Chou, C-P, & Pentz, M.A., 2020; Kardaras, 2017). Digital content requires the individual to respond to the digital stimuli, without being aware of the many verbal and nonverbal communication cues (facial expressions, gestures, tone of voice, eye contact, body language, posture, touch, etc.) that are part of social communication (Remland, 2016).
It is no wonder that more and more adolescents are experiencing anxiety, depression, loneliness, and attention deficit disorders due to a constant “digital diet,” which some have argued includes not only media but also junk food. Mental health trends have significantly worsened, particularly since 2013. Pediatric mental health–related emergency department visits increased by 70% from 2011 to 2020, rising from 4.8 million to 7.5 million—a shift from 7.7% to 13.1% of all pediatric emergency visits. The greatest increases were observed among adolescents and across all sexes, races, and ethnicities. Suicide-related visits nearly quintupled from 2011 to 2023, increasing from 0.9% to 4.2% of all pediatric emergency department visits (Bommersbach et al., 2023).
In my class survey of 99 college students, 85% reported experiencing anxiety, 48% neck and shoulder tension, and 41% abdominal discomfort.
For the age groups 18–23 and 24–29—but not for those over 30—the rates of serious psychological distress and major depressive episodes nearly doubled from 2013 to 2019 (Braghieri et al, 2022). During this same period, there was also a significant decline in academic performance, with math scores for 8th graders and reading scores for 4th graders dropping from around 2013 to 2024, except among top-performing students (Mervosh, 2025).
We are not saying to avoid the beneficial parts of the digital age. Instead, it should be used in moderation and to be aware of how some material and digital platforms prey upon our evolutionary survival mechanisms. Unfortunately, most people – especially children – have not evolved skills to counter the negative impacts of some types of media exposure. Parental control and societal policies may be needed to mitigate the damage and enhance the benefits of the digital age.
Zoom Fatigue – How to Reduce it and Configure your Brain for Better Learning
Zoom became the preferred platform for academic teaching and learning for synchronous education during the pandemic. Thus, students and faculty have been sitting and looking at the screen for hours on end. While looking at the screen, the viewers were often distracted by events in their environment, notifications from their mobile phones, social media triggers, and emails; which promoted multitasking (Solis, 2019). These digital distractions cause people to respond to twice as many devices with half of our attention – a process labeled semi-tasking’– meaning getting twice as much done and half as well.
We now check our phones an average of 96 times a day – that is once every 10 minutes and an increase of 20% as compared to two years ago (Asurion Research, 2019). Those who do media multitasking such as texting while doing a task perform significantly worse on memory tasks than those who are not multitasking (Madore et al., 2020). Multitasking is negatively correlated with school performance (Giunchiglia et al, 2018). The best way to reduce multitasking is to turn off all notifications (e.g., email, texts, and social media) and let people know that you will look at the notifications and then respond in a predetermined time, so that you will not be interrupted while working or studying.
When students in my class chose to implement a behavior change to monitor mobile phone and media use and reduce the addictive behavior during a five-week self-healing project, many reported a significant improvement of health and performance. For example one student reported that when she reduced her mobile phone use, her stress level equally decreased as shown in Figure 1 (Peper et al, 2021).

Figure 1. Example of student changing mobile phone use and corresponding decrease in subjective stress level. Reproduced by permission from Peper et al. (2021).
During this class project, many students observed that the continuous responding to notifications and social media affected their health and productivity. As one student reported: The discovery of the time I wasted giving into distractions was increasing my anxiety, increasing my depression and making me feel completely inadequate. In the five-week period, I cut my cell phone usage by over half, from 32.5 hours to exactly 15 hours and used some of the time to do an early morning run in the park. Rediscovering this time makes me feel like my possibilities are endless. I can go to work full time, take online night courses reaching towards my goal of a higher degree, plus complete all my homework, take care of the house and chores, cook all my meals, and add reading a book for fun! –22-year-old College Student
Numerous students reported that it was much easier to be distracted and multitask, check social media accounts or respond to emails and texts than during face-to-face classroom sessions as illustrated by two student comments from San Francisco State University.
“Now that we are forced to stay at home, it’s hard to find time by myself/for myself, time to study, and or time to get away. It’s easy to get distracted and go a bit stir-crazy.”
“I find that online learning is more difficult for me because it’s harder for me to stay concentrated all day just looking at the screen.”
Students often reported that they had more difficulty remembering the material presented during synchronous presentations. Most likely, the passivity while watching Zoom presentations affected the encoding and consolidation of new material into retrievable long-term memory. The presented material was rapidly forgotten when the next screen image or advertisement appeared and competed with the course instructor for the student’s attention. We hypothesize that the many hours of watching TV and streaming videos have conditioned people to sit and take in information passively, while discouraging them to respond or initiate action (Mander, 1978; Mărchidan, 2019).
To reduce the deleterious impact of media use, China has placed time limits on cellphone use, gaming, and social media use for children. On February 2021 Chinese children were banned from taking their mobile phones into school (Wakefield, 2021), on August 2021 Children under 18 were banned from playing video games during the week and their play was restricted to just one hour on Fridays, weekends and holidays (McDonell, 2021) and beginning on September 20, 2021 children under 14 who have been authenticated using their real name can access Douyin, the Chinese version of Tik Tok, for maximum of 40 minutes a day between the hours of 6:00 and 22:00 (BBC, 2021).
Ways to Avoid Zoom
Say goodnight to your phone: It is common for people to use their mobile phone before going to bed, and then end up having difficulty falling asleep. The screen emits blue light that sends a signal to your brain that says it is daytime instead of night. This causes your body to suppress the production of the melatonin hormone, which tells your body that it is time to sleep. Reading or watching content also contributes, since it stimulates your mind and emotions and thereby promotes wakefulness (Hartley et al., 2022). Implement sleep hygiene and stop using your phone or watching screens 30-minutes before going to bed for a better night’s sleep.
Maintaining a healthy vision: We increase near visual stress and the risk of developing myopia when we predominantly look at nearby surfaces. We do not realize that eye muscles can only relax when looking at the far distance. For young children, the constant near vision remodels the shape of the eye and the child will likely develop near sightedness. The solutions are remarkably simple. Respect your evolutionary background and allow your eyes to spontaneously alternate between looking at near and far objects while being upright (Schneider, 2016; Peper, 2021; Peper, Harvey & Faass, 2020).
Interrupt sitting disease: We sit for the majority of the day while looking at screens that is a significant risk factor for diabetes, cardiovascular disease, depression and anxiety (Matthews et al., 2012; Smith et al., 2020). Interrupt sitting by getting up every 30 minutes and do a few stretches. You will tend to feel less sleepy, less discomfort and more productive. As one of our participants reported that when he got up, moved and exercised every 30 minutes at the end of the day he felt less tired. As he stated, “There is life after five,” which meant he had energy to do other activities after working at the computer the whole day. While working time flies and it is challenging to get up every 30 minutes. Thus, install a free app on your computer that reminds you to get up and move such as StretchBreak (www.stretchbreak.com).
Use slouching as a cue to change: Posture affects thoughts and emotions as well as, vice versa. When stressed or worried (e.g., school performance, job security, family conflict, undefined symptoms, or financial insecurity), our bodies tend to respond by slightly collapsing and shifting into a protective position.
When we collapse/slouch, we are more at risk to:
• Feel helpless (Riskind & Gotay, 1982).
• Feel powerless (Westfeld & Beresford, 1982; Cuddy, 2012).
• Recall and being more captured by negative memories (Peper, Lin, Harvey, & Perez, 2017; Tsai, Peper, & Lin, 2016).
• Experience cognitive difficulty (Peper, Harvey, Mason, & Lin, 2018).
When stressed, anxious or depressed, it is challenging to change. The negative feelings, thoughts and worries continue to undermine the practice of reframing the experience more positively. Our recent study found that a simple technique, that integrates posture with breathing and reframing, rapidly reduces anxiety, stress, and negative self-talk (Peper, Harvey, Hamiel, 2019). When you are captured by helpless defeated thoughts and slouch, use the thought or posture as the trigger to take change. The moment you are aware of the thoughts or slouched posture, sit up straight, look up, take a slow large diaphragmatic breath and only then think about reframing the problem positively (Peper, Harvey, Hamiel, 2019).
When we are upright and look up, we are more likely to:
• Have more energy (Peper & Lin, 2012).
• Feel stronger (Peper, Booiman, Lin, & Harvey, 2016).
• Find it easier to do cognitive activity (Peper, Harvey, Mason, & Lin, 2018).
• Feel more confident and empowered (Cuddy, 2012).
• Recall more positive autobiographical memories (Michalak, Mischnat,& Teismann, 2014).
The challenge is that we are usually unaware we have begun to slouch. A very useful solution is to use a posture feedback device to remind us, such as the UpRight Go (https://www.uprightpose.com/). This simple device and app signals you when you slouch. The device attaches to your neck and connects with blue tooth to your cellphone. After calibrating, it provides vibrational feedback on your neck each time you slouch. When participants use the vibration feedback to become aware of what is going on and interrupt their slouch by stretching and sitting up, they report a significant decrease in symptoms and an increase in productivity. As one student reported: “Having immediate feedback on my posture helped me to be more aware of my body and helped me to link my posture to my emotions. Before using the tracker, doing this was very difficult for me. It not only helped my posture but my awareness of my mental state as well.”
https://peperperspective.com/2023/08/30/techstress-building-healthier-computer-habits/
https://peperperspective.com/2024/09/04/cellphones-affects-social-communication-vision-breathing-and-health-what-to-do/
References
Asurion Research (November 19, 2019). Americans Check Their Phones 96 Times a Day. https://www.asurion.com/about/press-releases/americans-check-their-phones-96-times-a-day/#:~:text=Despite%20our%20attempts%20to%20curb,tech%20care%20company%20Asurion1.
BBC (2021, September 20). China: Children given daily time limit on Douyin – its version of TikTok. BBC. Accessed April 12, 2025. https://www.bbc.com/news/technology-58625934
Bommersbach, T.J., McKean, A.J., Olfson, M., & Rhee, T.G. (2023). National Trends in Mental Health-Related Emergency Department Visits Among Youth, 2011-2020. JAMA, (2), 329(17), 1469-1477. https://doi.org/10.1001/jama.2023.4809
Braghieri, Land and Levy, Ro’ee and Makarin, Alexey, Social Media and Mental Health (July 28, 2022). http://dx.doi.org/10.2139/ssrn.3919760
Christodoulou, G. Majmundar, A., Chou, C-P., & Pentz, M.A. (2020). Anhedonia, screen time, and substance use in early adolescents: A longitudinal mediation analysis, Journal of Adolescence, (78), 24-32. https://doi.org/10.1016/j.adolescence.2019.11.007
Cuddy, A. (2012). Your body language shapes who you are. Technology, Entertainment, and Design (TED) Talk. Accessed April 12, 2025. www.ted.com/talks/amy_cuddy_your_body_language_shapes_who_you_are
Giunchiglia, F. Zeni, M., Gobbi, E., Bignotti,E., & Bison, I. (2018). Mobile social media usage and academic performance, Computers in Human Behavior, 82, 177-185. https://doi.org/10.1016/j.chb.2017.12.04
Hartley, S., Royant-Parola, S., Zayoud, A., Gremy, I., & Matulonga, B. (2022). Do both timing and duration of screen use affect sleep patterns in adolescents?. PloS one, 17(10), e0276226. https://doi.org/10.1371/journal.pone.0276226
Kardaras, N. (2017). Glow Kids: How Screen Addiction Is Hijacking Our Kids – and How to Break the Trance. New York: St. Martin’s Griffin. https://www.amazon.com/Glow-Kids-Screen-Addiction-Hijacking/dp/1250146550/
Madore, K.P., Khazenzon, A.M., Backes, C.W. et al. (2020). Memory failure predicted by attention lapsing and media multitasking. Nature, 587, 87–91. https://doi.org/10.1038/s41586-020-2870-z
Mander, J. (1978). Four arguments for elimination of television. New York: William Morrow Paperbacks. https://www.amazon.com/Arguments-Elimination-Television-Jerry-Mander/dp/0688082742/
Mărchidan, A. (2019). More technologized is not more educated,” 2019 11th International Conference on Electronics, Computers and Artificial Intelligence (ECAI), Pitesti, Romania, pp. 1-4, https://doi.org/10.1109/ECAI46879.2019.9041993
Mark, G. (2023). Attention Span: A Groundbreaking Way to Restore Balance, Happiness and Productivity. Toronto, Canada: Hanover Square Press. https://www.amazon.com/Attention-Span-Finding-Fighting-Distraction/dp/1335449418
Matthews, C.E., George, S.M., Moore, S.C., Bowles, H.R. Blair, A.,. Park, I., Troiano, R.P., Hollenbeck, A., & Schatzkin, A. (2012). Amount of time spent in sedentary behaviors and cause-specific mortality in US adults. The American Journal of Clinical Nutrition, (92)@, 437-445. https://doi.org/10.3945/ajcn.111.019620
McDonell, S. (2021, August 30). China to limit children’s online gaming time. BBC World Business Report. Accessed April 12, 2025. https://www.bbc.co.uk/programmes/w172y48xs9s5l56
Mervosh, S. (2025, April 7). The Pandemic is not the only reason U.S. Students are losing ground. New York Times. https://www.nytimes.com/2025/04/07/us/low-performing-students-reasons.html?smid=nytcore-ios-share&referringSource=articleShare
Michalak, J., Mischnat, J., & Teismann, T. (2014). Sitting Posture Makes a Difference—Embodiment Effects on Depressive Memory Bias. Clinical Psychology & Psychotherapy, (21),6, 519-524. https://doi.org/10.1002/cpp.1890
Peper, E. (2021). Resolve Eyestrain and Screen Fatigue. Well Being Journal, (30), Wintger, 24-28. https://www.researchgate.net/publication/345123096_Resolve_Eyestrain_and_Screen_Fatigue
Peper, E., Booiman, A., Lin, I.M., & Harvey, R. (2016). Increase strength and mood with
posture. Biofeedback. 44(2), 66–72. https://doi.org/10.5298/1081-5937-44.2.04
Peper, E., Harvey, R. & Faass, N. (2020). TechStress: How Technology is Hijacking Our Lives, Strategies for Coping, and Pragmatic Ergonomics. Berkeley: North Atlantic Books. https://www.amazon.com/Beyond-Ergonomics-Prevent-Fatigue-Burnout/dp/158394768X
Peper, E., Harvey, R., & Hamiel, D. (2019). Transforming thoughts with postural awareness to increase therapeutic and teaching efficacy. NeuroRegulation, 6(3), 153-169. https://doi.org/10.15540/nr.6.3.1533-1
Peper, E., Harvey, R., Mason, L., & Lin, I.-M. (2018). Do better in math: How your body posture may change stereotype threat response. NeuroRegulation, 5(2), 67–74. http://dx.doi.org/10.15540/nr.5.2.67
Peper, E. & Lin, I-M. (2012). Increase or decrease depression-How body postures influence your energy level. Biofeedback, 40 (3), 126-130. https://doi.org/10.5298/1081-5937-40.3.01
Peper, E., Lin, I-M., Harvey, R., & Perez, J. (2017). How posture affects memory recall and mood. Biofeedback. 45 (2), 36-41. https://doi.org/10.5298/1081-5937-45.2.01
Peper, E., Wilson, V., Martin, M., Rosegard, E., & Harvey, R. (2021). Avoid Zoom fatigue, be present and learn. NeuroRegulation, 8(1), 47–56. https://doi.org/10.15540/nr.8.1.47
Remland, M.S. Nonverbal Communication in Everyday Life 4th Edition. Thousand Oaks, CA: Sage Publications. https://www.amazon.com/Nonverbal-Communication-Everyday-Martin-Remland/dp/1483370259
Riskind, J.H., Gotay, C.C. Physical posture: Could it have regulatory or feedback effects on motivation and emotion?. Motiv Emot 6, 273–298 (1982). https://doi.org/10.1007/BF00992249
Schneider, M. (2016). Vision for Life. Berkeley, CA: North Atlantic Books. https://www.amazon.com/Vision-Life-Revised-Eyesight-Improvement/dp/1623170087
Smith, L., Jacob, L., Trott, M., Yakkundi, A., Butler, L., Barnett, Y., Armstrong, N.C., McDermott, D., Schuch, F., Meyer, J., López-Bueno, R., Sánchez, G.F.L., Bradley, D., Tully, M.A. (2020). The association between screen time and mental health during COVID-19: A cross sectional study, Psychiatry Research, (292). https://doi.org/10.1016/j.psychres.2020.11333
Solis, B. (2019). How Managers Can Help Workers Tackle Digital Distractions. MIT Sloan Management Review, 60(4), 1-3. https://sloanreview.mit.edu/article/how-managers-can-help-workers-tackle-digital-distractions/
Tsai, H. Y., Peper, E., & Lin, I. M.* (2016). EEG patterns under positive/negative body postures and emotion recall tasks. NeuroRegulation, 3(1), 23-27. https://doi.org/10.15540/nr.3.1.23
Wakefield, J. (2021), February 2). China bans children from using mobile phones at school. BBC. Accessed April 12, 2025. https://www.bbc.com/news/technology-55902778
Weisfeld, G.E., Beresford, J.M. Erectness of posture as an indicator of dominance or success in humans. Motiv Emot 6, 113–131 (1982). https://doi.org/10.1007/BF00992459
Suggestions for mastering and generalizing breathing skills
Posted: October 30, 2024 Filed under: attention, behavior, biofeedback, Breathing/respiration, CBT, cellphone, cognitive behavior therapy, emotions, ergonomics, healing, health, mindfulness, Neck and shoulder discomfort, Pain/discomfort, posture, relaxation, self-healing, stress management, Uncategorized | Tags: abdominal beathing, anxiety, diaphragmatic braething, health, hyperventilation, meditation, mental-health, mindfulness, mouth breathing, Toning 4 CommentsAdapted from: Peper, E., Oded, Y., Harvey, R., Hughes, P., Ingram, H., & Martinez, E. (2024). Breathing for health: Mastering and generalizing breathing skills. Townsend Letter-Innovative Health Perspectives. November 15, 2024. https://townsendletter.com/suggestions-for-mastering-and-generalizing-breathing-skills/

Breathing techniques are commonly employed with complimentary treatments, biofeedback, neurofeedback or adjunctive therapeutic strategies to reduce stress and symptoms associated with excessive sympathetic arousal such as anxiety, high blood pressure, insomnia, or gastrointestinal discomfort. Even though it seems so simple, some participants experience difficulty in mastering effortless breathing and/or transferring slow breathing skills into daily life. The purpose of this article is to describe: 1) factors that may interfere with learning slow diaphragmatic breathing (also called cadence or paced breathing, HRV or resonant frequency breathing along with other names), 2) challenges that may occur when learning diaphragmatic breathing, and 3) strategies to generalize the effortless breathing into daily life.
Background
A simple two-item to-do list could be: ‘Breathe in, breathe out.’ Simple things are not always easy to master. Mastering and implementing effortless ‘diaphragmatic’ or ‘abdominal belly’ breathing may be simple, yet not easy. Breathing is a dynamic process that involves the diaphragm, abdominal, pelvic floor and intercostal muscles that can include synchronizing the functions of the heart and lungs and may result in cardio-respiratory synchrony or coupling, as well as ‘heart-rate variability breathing training (Codrons et al., 2014; Dick et al., 2014; Elstad et al., 2018; Maric et al., 2020; Matic et al., 2020). Improving heart-rate variability is a useful approach to reduce symptoms of stress and promotes health and reduce anxiety, asthma, blood pressure, insomnia, gastrointestinal discomfort and many other symptoms associated with excessive sympathetic activity (Lehrer & Gevirtz, 2014; Xiao et al., 2017; Jerath et al., 2019; Chung et al., 2021; Magnon et al., 2021; Peper et al., 2022).
Breathing can be effortful and In some cases people have dysfunctional breathing patterns such as breath holding, rapid breathing (hyperventilation), shallow breathing and lack of abdominal movement. This usually occurs without awareness and may contribute to illness onset and maintenance. When participants learn and implement effortless breathing, symptoms often are reduced. For example, when college students are asked to practice effortless diaphragmatic breathing twenty-minutes a day for one week, as well as transform during the day dysfunction breathing patterns into diaphragmatic breathing, they report a reduction in shallow breathing, breath holding,, and a decrease of symptoms as shown in Fig 1 (Peper et al, 2022).

Figure 1. Percent of people who reported that their initial symptoms improved after practicing slow diaphragmatic breathing for twenty minutes per day over the course of a week (reproduced from: Peper et al, 2022).
Most students became aware of their dysfunctional breathing and substituted slow, diaphragmatic breathing whenever they realized they were under stress; however, some students had difficulty mastering ‘effortless’ (e.g., automated, non-volitional) slow, diaphragmatic breathing that allowed abdominal expansion during inhalation.
Among those had more difficulty, they tended to have almost no abdominal movement (expansion during inhalation and abdominal constriction during exhalation). They tended to breathe shallowly as well as quickly in their chest using the accessory muscles of breathing (sternocleidomastoid, pectoralis major and minor, serratus anterior, latissimus dorsi, and serratus posterior superior).
The lack of abdominal movement during breathing reduced the movement of lymph as well as venous blood return in the abdomen; since; the movement of the diaphragm (the expansion and constriction of the abdomen) acts a pump. Breathing predominantly in the chest may increase the risk of anxiety, neck, back and shoulder pain as well as increase abdominal discomfort, acid reflux, irritable bowel, dysmenorrhea and pelvic floor pain (Banushi et al., 2023; Salah et al., 2023; Peper & Cohen, 2017; Peper et al., 2017; Peper et al., 2020, Peper et al., 2023). Learning slow, diaphragmatic or effortless breathing at about six breaths per minute (resonant frequency ) is also an ‘active ingredient’ in heartrate variability (HRV) training (Steffen et al., 2017; Shaffer & Meehan, 2020).
1. Factors that interfere with slow, diaphragmatic breathing
Difficulty allowing the skeletal and visceral muscles in the abdomen to expand or constrict in ‘three-dimensions’ (e.g., all around you in 360 degrees) during inhalation or exhalation. Whereas internal factors under volitional control and will mediate breathing practices, external factors can restrict and moderate the movement of the muscles. For example:
Clothing restrictions (designer jeans syndrome). The clothing is too tight around the abdomen; thereby, the abdomen cannot expand (MacHose & Peper, 1991; Peper et al., 2016). An extreme example were the corsets worn in the late 19th century that was correlated with numerous illnesses.
Suggested solutions and recommendations: Explain the physiology of breathing and how breathing occurs by the diaphragmatic movement. Discuss how babies and dogs breathe when they are relaxed; namely, the predominant movement is in the abdomen while the chest is relaxed. This would also be true when a person is sitting or standing tall. Discuss what happens when the person is eating and feels full and how they feel better when they loosen their waist constriction. When their belt is loosened or the waist button of their pants is undone, they usually feel better.
Experiential practice. If the person is wearing a belt, have the person purposely tighten their belt so that the circumference of the stomach is made much smaller. If the person is not wearing a belt, have them circle their waist with their hands and compress it so that the abdomen can not expand. Have them compare breathing with the constricted waist versus when the belt is loosened and then describe what they experienced.
Most participants will feel it is easier to breathe and much more comfortable when the abdomen is not constricted.
Previous abdominal injury. When a person has had abdominal surgery (e.g., Cesarean section, appendectomy, hernia repair, or episiotomy), they unknowingly may have learned to avoid pain by not moving (relaxing or tensing) the abdomen muscles (Peper et al., 2015; Peper et al., 2016). Each time the abdomen expands or constricts, it would have pulled on the injured area or stitches that would have cause pain. The body immediately learns to limit movement in the affected area to avoid pain. The reduction in abdominal movement becomes the new normal ‘feeling’ of abdominal muscle inactivity and is integrated in all daily activities. This is a process known as ‘learned disuse’ (Taub et al., 2006). In some cases, learned disuse may be combined with fear that abdominal movement may cause harm or injury such as after having a kidney transplant. The reduction in abdominal movement induces shallow thoracic breathing which could increase the risk of anxiety and would reduce abdominal venous and lymph circulation that my interfere with the healing.
Suggested solutions and recommendations. Discuss the concept of learned disuse and have participant practice abdominal movement and lower and slower breathing.
Experiential practices: Practicing abdominal movements
Sit straight up and purposely exhale while pulling the abdomen in and upward and inhale while expanding the abdomen. Even with these instructions, some people may continue to breathe in their chest. To limit chest movement, have the person interlock their hands and bring them up to the ceiling while going back as far as possible. This would lock the shoulders and allows the abdomen to elongate and thereby increase the diaphragmatic movement by allowing the abdomen to expand. If people initially have held their abdomen chronically tight then the initial expansion of abdomen by relaxing those muscle occurs with staccato movement. When the person becomes more skilled relaxing the abdominal muscles during inhalation the movement becomes smoother.
Make a “psssssst” sound while exhaling. Sit tall and erect and slightly pull in and up the abdominal wall and feel the anus tightening (pulling the pelvic floor up) while making the sound. Then allow inhalation to occur by relaxing the stomach and feeling the anus go down.
Use your hands as feedback. Sit up straight, placing one hand on the chest and another on the abdomen. While breathing feel the expansion of the abdomen and the contraction of the abdomen during exhalation. Use a mirror to monitor the chest-muscle movement to ensure there is limited rising and falling in this area.
Observe the effect of collapsed sitting. When sitting with the lower back curled, there is limited movement in the lower abdomen (between the pubic region and the umbilicus/belly button) and the breathing movement is shallower without any lower pelvic involvement (Kang et al., 2016). This is a common position of people who are working at their computer or looking at their cellphone.
Experiential practice: looking at your cellphone
Sit in a collapsed position and look down at your cellphone. Look at the screen and text as quickly as possible.
Compare this to sitting up and then lift the cell phone at eye level while looking straight ahead at the cellphone. Look at the screen and text as quickly as possible.
Observe how the position effected your breathing and peripheral awareness. Most likely, your experience is similar those reported by students. Close to 85%% of students who complete this activity reported that their breathing was shallower sitting slouched versus erect and about 85% of the students reported that their peripheral awareness and vision improved when sitting erect (Peper et al., 2024).
Suggested solutions and recommendations. Be aware how posture affect breathing. While sitting, place a rolled-up towel against the lower back so that the person sits more erect which would allow the abdomen to expand when inhaling.
Self-image, self-esteem, and confidence. Participants may hold their abdomen in because they want to look slim (sometimes labeled as the “hourglass syndrome” associate expanding the abdomen as unattractive (PTI, 2023). A flat abdomen is culturally reinforced by social media and fashion models and encouraged in some activities such as ballet. On the other hand, some people purposely puff up their chest to increase size and dominance (Cohen & Leung, 2009).
Suggested solutions and recommendations. Discuss the benefits of diaphragmatic breathing including its ability to reduce anxiety in social settings that may enhance confidence. Similar to an earlier suggestion, have the person explore clothing with a looser waist that still supports feelings of attractiveness and power.
Feeling anxious, fearful or threatened. The normal physiological stress reaction is a slight gasp with the tightening of the abdomen muscles for protection when a stressor occurs (Gilbert, 1998; Ekerholt & Bergland., 2008). The stressor can be an actual physical event, social situation or thoughts and emotions. Shallow breathing is a natural self-protective response. This pattern is often maintained until one feels ‘safe’ enough to relax, which for many can have a duration of the entire day or until finding the relative safety of sleep.
Suggested solutions and recommendations. Discuss how the physiological stress reaction is a normal response pattern that the person most likely learned in early childhood for self-protection. This pattern is often observed in clients who are emotionally sensitive and/or react excessively to a variety of stimuli. Note that some people have learned not to show their reactivity on their face or in the overt behaviors, yet they continue to breathe shallowly as a telltale sign of ‘distress.’ People who breath shallowly may experience this response as burdensome. Discuss with them how to reframe their sensitivity as a gift; namely, they are more aware of other people’s reactions and emotions. They just need to learn how not to respond automatically. Encourage awareness of their breath-holding and shallow breathing. Follow this by teaching them to replace the dysfunctional breathing with slow, diaphragmatic breathing at 6-breaths-per-minute. A possible training sequence is the following:
- Teach slow, diaphragmatic breathing
- Practice evoking a stressor and the moment the client senses the stress response, shallow breaths or holds their breath have them shift to slow, diaphragmatic breathing.
- If the person slouches in response to stress, the moment they become aware of slouching, have then sit erect, look up and then breathe diaphragmatically. (Peper et al., 2019)
Experiential practice: Transform stressful thoughts by looking up, breathing, and changing thoughts.
Evoke a stressor and then attempt to reframe the experience (cognitive behavior therapy or CBT approach).
Compare this to evoking a stressor, then shift to an upright position while looking up, take a few slow, diaphragmatic breaths, and reframe the experience.
In almost all cases, when the client shifts position, looks up and then reframes, the stress reaction is significantly reduced and it is much easier to reframe the experiences positively compared to when only attempting to reframe the experience (Peper et al., 2019).
Diaphragmatic breathing feels abnormal. How you breathe habitually is what feels normal unless there is overt illness such as asthma or emphysema. Any new pattern usually feels abnormal. When the person shifts their breathing pattern, such as in a transition from habitual shallow chest breathing to slower diaphragmatic abdominal breathing, it feels strange and wrong.
Suggested solutions and recommendations. Discuss the concept that habitual patterns are normal (e.g., a person who typically slouches when standing straight may experience that they are going to fall backwards). Emphasize the importance of making a shift in posture and leaning into the discomfort of the new experience. Often after practicing slow diaphragmatic breathing, the person may report feeling much more relaxed (e.g., sensing heaviness and warmth) with their fingers increasing in temperature.
2. Challenges that may occur when learning diaphragmatic breathing
Ideally, breathing is an effortless diaphragmatic process as described by the phrase, “it breathes me” (Luthe & Schultz, 1970; Luthe, 1979); however, some participants struggle to achieve this type of breathing. The following are common challenges and possible solutions:
Distraction and internal dialogue. Many people struggle with thoughts jumping from one area to another. Some people refer to this mental state as “monkey mind.”
Suggested solutions and recommendations. Validate that distraction and internal dialogue are normal and require continual managing and practice to overcome. Experimental Practice: Have the person train focus during diaphragmatic breathing techniques by focusing on 1 item in the room. Remind them that when thoughts arise, note them briefly instead of engaging with them and then refocus on the item. Start with increments of time and increase with practice.
Effect of gravity on breathing. In the vertical position, exhalation occurs when the abdomen constricts (slight tightening of the transverse and oblique abdominal muscles and the pelvic floor) pushes the diaphragm up, allowing the air to go out. It needs to push against gravity.
In the vertical position, inhalation occurs when the abdominal muscles and pelvic floor muscles relax and the abdomen widens in all directions (360 degrees) which causes the diaphragm to descend as it is being pulled down by gravity. This process allows effortless inhalation. The experience is the opposite when lying supine on one’s back. While lying down, gravity pulls on the abdomen that cause the diaphragm to go upward allowing the air to flow out during exhalation. Inhalation takes work because as the diaphragm descends it has to push the abdominal content upward against gravity.
Experiential practice: Erect versus supine
- Vertical position. Begin by exhaling completely by pulling the abdomen in and up while staying erect and not pressing/contracting the chest downward. At the end of exhalation, allow the abdomen to relax (pop out) and feel how the air is sucked in without trying to inhale
- Horizontal position. Begin by lying down, with the face pointing up. Inhale by expanding your abdomen and pushing your abdomen upward against gravity. Then let exhalation occur while totally relaxing as gravity pushes the abdomen downward, which pushes the diaphragm upward into the chest allowing the air to flow out. Optionally, place a small bag of rice/beans (e.g., approximately one to five pound or. One-half to two kilograms) on your lower abdomen while lying down. When you inhale, push the weight upward and away from you by allowing the stomach, but not the chest, to expand. Allow exhalation to occur as the weight pushes your abdomen down and upward into your chest. The weight is useful as it allows the mind to focus more easily on the task of feeling the movement of the abdomen.
Over breathing/hyperventilation. Even breathing at about six breaths per minute can cause hyperventilation can occur. Hyperventilation occurs when a person is breathing in excess of the metabolic needs of the body and thereby eliminating more carbon dioxide. The result is respiratory alkalosis and an elevated blood pH as the dissolved carbon dioxide (pCO2) in the blood is reduced (Folgering, 1999).
The most common symptoms of over breathing are colder sweaty hands and light-headedness. If this starts to occur, focus on decreasing the airflow during exhalation by exhaling through pursed lips making the sound, “Pssssssst.” While making this sound, make the sound softer with less airflow. Alternatively, have them imagine a holding a dandelion flower a few inches from their lips and blow so softly the seeds do not blow away. The blowing away of the seed is the feedback that you are blowing to hard as shown in Figure 2.

Figure 2. Dandelion seeds as feedback when the person is blowing with too much effort. Alternatively, we recommend that the client imagine smelling the scent/fragrance of a flower that usually causes nose inhalation and then exhale gently through pursed lips ast if the air flows over a candle and, the flame does not move back and forth.
Mouth breathing. Mouth breathing contributes to disturbed sleep, snoring, sleep apnea, dry mouth upon waking, fatigue, allergies, ear infections, attention deficit disorders, crowded miss-aligned teeth, and poorer quality of life (Kahn & Ehrlich, 2018). Even the risk of ear infections in children is 2.4 time higher for mouth breathers than nasal breathers (van Bon et al, 1989) and nine and ten year old children who mouth breath have significantly poorer quality of life and have higher use of medications (Leal et al, 2016).
Breathing through the nose is associated with deeper and slower breathing rate than mouth breathing. Nose breathing reduces airway irritation since the nose filters, humidifies, warms/cools the inhaled air as well as reduces the air turbulence in the upper airways. The epithelial cells of the nasal cavities produce nitric oxide that are carried into the lungs when inhaling during nasal breathing (Lundberg & Weitzberg, 1999). The nitric oxide contributes to healthy respiratory function by promoting vasodilation, aiding in airway clearance, exerting antimicrobial effects, and regulating inflammation (McKeown, 2019; Allen, 2024). Note that alternate nostril breathing, such as breathing in one nostril for 5-seconds and out of the other for 5-seconds is another technique which some people find beneficial.
Slower breathing approaches also facilitates sympathetic parasympathetic balance and reduces airway irritation. If the person breathes habitually through their mouth, refer them to health care provider to explore factors that may contribute to mouth breathing such as enlarged tonsils and adenoids or deviated septum. In addition, explore environmental factors that could contribute nasal inflammation such as allergies or foods such as dairy (Al-Raby, 2016).
Performance anxiety. Many participants are concerned about their performance. The direct instructions such as “follow the graphic” causes the person to try hard to breathe with too much effort. Explore some of the following indirect strategies to interrupt ongoing cognitive judgements and self-talk.
- Toning or humming (Peper et al., 2019a). While exhaling, have the person hum a sound with their mouth closed. Let the sound go for about 6 seconds, relax, inhale and hum again. Toning is very similar except you verbalize a tone such as “Oammm.” (For detailed instructions on toning, see: Anziani & Peper (2021)).
- Stroking down arms and legs during exhalation. Have a partner gently stroke down your arms from your shoulder past your fingertips as you are exhaling. The downward stroking is in rhythm with the exhalation. As the arm is being stroked, attend to the sensations going down the arms. Be sure that the toucher exhales at the same time and the stroking down the arm takes about six seconds. After being stroked for a few times, have the person imagine that each time they exhale they feel a flow down through their arms and out their fingers.
- Repeat the same process while stroking down the legs from the side of their hips to their toes.
- Finally, have the person imagine/feel the sensation streaming down their legs with each exhalation.
- Many participants will report that they sense a steaming going down their arms, that they hands warm up, and their thought have stopped.
- Integrated body movement with breathing especially flexion and contraction (Meehan & Shaffer, 2023). Integrate the normal response of flexion that induces exhalation and extension evokes inhalation. Be careful that the flexion movement does not encourage participants to compress their chest during exhalation, which tends to encourage chest breathing. Have the person focus on their head staying tall and erect. Have the person sit straight up with their feet slight apart and their hands palm down on their lap. Allow inhaling to initiate as the person simultaneously arches their lower back expanding the stomach, separating the knees and turning the hands palm up. Initiate exhalation while simultaneously bringing the knees together, turning the palms face down on the thighs and rolling the pelvic back slightly rounding the lower back. Do the movements smoothly while keeping the legs and shoulders relaxed.
Flooded by emotions. Although very rare, at times when the person allows the abdomen to relax, they may experience by the emotions from a past trauma as the habitual bracing patterns are relaxed.
Suggested solutions and recommendations. Validate these emotions for the person. Explain that this is a normal process that may occur if past trauma has occurred. Clients who have had past trauma often experience hypervigilance, which may interfere with the relaxation response that occurs during more optimal states of breathing. Transitioning to a more optimal rest state may be uncomfortable for a person who has experienced trauma because it reduces hypervigilance. This can feel uncomfortable as hypervigilance in these cases serves a protective role, even if it is an illusory feeling of protection from future harm. Since persistent hypervigilance can interfere with the relaxation response, the benefits of allowing a relaxation response to occur through slower breathing should be highlighted. Grounding techniques as described by Peper et al (2024a) can be useful to become centered.
3. Strategies to generalize the effortless breathing into daily life.
Generalizing the skill occurs after having mastered diaphragmatic breathing in different positions (sitting, standing, lying down, and while performing tasks). It is important to remember that our breathing patterns are conditioned with our behavior. Become aware how breathing affects cognitions and emotions and how emotions and cognitions affects breathing. The following are some strategies that may facilitate learning and generalizing the slower breathing skills.
Observing how our behavior affects our breathing: Anything that may evoke the alarm or defense reaction tends to cause the person gasp and/or hold their breath. For example, when a person is sitting peacefully, make an unexpected noise behind their back or movement in their periphery of vision. In most cases they will gasp or hold their breath. Usually, they are unaware of this process unless they are asked what happened to their breathing. The major reason for the breath holding is that the stimuli triggers an alarm/defense reaction and when we hold our breath our hearing is more acute (we can hear approaching danger earlier). The problem is that we give this response when there is no actual, immediate or present threat.
Experiential practice. Sit comfortably. Now as quickly as possible without rotating the head, look with your eyes to the extreme right and then left and back and forth as if trying to identify danger at the periphery. Do this for a few eye movements. Almost everyone holds their breath when doing this exercise. For generalizing the skill, ask the person to observe during the day situations in which they hold their breath, ask them if it was necessary and encourage them to start diaphragmatic breathing.
Observing how breathing affects our thoughts and emotions. Breathing patterns are intrinsically linked to our emotions and thoughts as illustrated in the many language phrases such as sigh of relief, full of hot air, waiting with bated breath. At the same time, our breathing patterns also affect our thoughts. For instance, when we breathe shallowly and more rapidly, we can induce feelings of fear or anxiety. If we gasp, we can experience thought stopping.
Experiential practices: Incomplete exhalation: Observe what happens when you exhale less than you inhale. Begin by exhaling only 70% of the air you inhaled, then inhale and exhale again only 70% of the air you just inhaled continue this for 30 seconds. Many people will experience the onset of anxiety symptoms, lightheadedness, dizziness, neck and shoulder tension, etc. (Peper & MacHose, 1993). If you experience symptoms during this exercise and you have experienced these symptoms in the past, it is likely that unknowingly breathing in a dysfunctional pattern could have evoked them. Therefore, practicing effortless breathing may interrupt and reduce the symptoms. Do this practice while observing the person carefully and immediately interrupt and distract the person if they start feeling dizzy, too anxious, or trigger the beginning of a panic attack or PTSD symptoms.
Experiential practice: Gasp or sniff-hold sniff. Observe what happens when you are performing a cognitive task and you rapidly gasp or do sniff-hold-sniff again before exhaling. Begin by sequentially subtracting mentally, the number 7 from 146 (e.g., 146, 139, 132….). Do this as rapidly as possible and do not make a mistake. While doing the subtracting, take a rapid gasp (such as one is triggered by surprise or fear), alternatively, take a quick sniff through your nose, hold your breath and take another sniff on top of the first one, then exhale. Whereas subtrating numbers is a skill most adults can perform, the ‘time pressure’ along with the direction to avoid mistakes may be the ‘immediate’ source of strain. Whether it was the time pressure, the direction to avoid mistakes or the direction to gasp, observe what happened to your thinking process. In almost all cases, your higher-order thoughts (doing the sequential subtraction under time pressure while gasping) have disappeared, replaced by the immediate thoughts of ‘performance anxiety.’
If you blank out on exams or experience anxiety, gasping and breath holding may be one of the factors that increases symptoms and affects your performance. If you are aware that you are holding your breath or gasped, use that as the cue to shift to slow diaphragmatic breathing and you may find that your performance improves. Therefore, observe when and where you were blanking out, gasping and/or holding your breathing then substitute slow, effortless diaphragmatic breathing.
How to develop awareness and interrupting of dysfunctional breathing response. Most participants are unaware of their somatic responses until symptoms occur. Being aware of the initiation of a somatic response may assist you in identifying triggers and interrupting the developing process. A significant component of the training is symptom prescription rehearsal.
Symptom prescription is a practice in which the participant simulates/acts out the psychophysiological pattern associated with their symptoms. They amplify the body pattern until they feel the onset of the actual symptoms. The moment the person feels the beginning of the symptom, they stop the practice and initiate slow breathing and relaxation. After practicing the symptom rehearsal, they are instructed to become aware of the onset of the symptom and then use that signal to trigger the effortless breathing while looking up and shifting the body into an upright sitting position (Peper et al., 2019). Gasping and breath holding are normal responses to unexpected stimuli; however, they may trigger sympathetic activation even when there is no actual danger.
Experiential practice: Developing awareness on neck and shoulder tension:
Sit comfortably and practice effortless breathing for a minute. Take a fearful gasp and observe what happens in your body (e.g., slight neck and upper chest tension, light headedness, slight radiating pain into the eye, etc.). Shift back to effortless breathing until all symptoms /sensations have disappeared.
- Now gasp with less effort and observe the first sensations, use the awareness of first sensations to trigger the effortless breathing and continue to breathe until symptoms have disappeared
- Continue this practice. Reduce the gasping effort each time.
- After having developed the initial somatic sensation then during the day observe what triggers this response and immediately shift to slower diaphragmatic breathing. After you have shifted to effortless breathing, reflect on the trigger. Was it necessary to react? If yes, explore strategies to resolve the issue.
The same process can be done to assist with desensitization to painful memories or stressful events. Each time the person becomes aware of their somatic reaction to an evoked memory or stressful event, they shift to effortless diaphragmatic breathing. If they find that it is difficult to interrupt the emotional memories and it triggers more and more negative thoughts and associations, use the sniff-hold-sniff technique and follow that with box-breathing or any of the other quick somatic rescue techniques (Peper et al., 2024a). Box-breathing in this context could include a brief breath-holding. A typical box-breathing technique is to breath in for a count of four, hold for a count of four, breath out for a count of four, then breath in again for a count of four, continuing the figurative 4-4-4-4 count of breathing.
Practice slower diaphragmatic breathing during the day. Implement effortless diaphragmatic breathing through regeneration and interrupting the stress response.
- Support regeneration. Each day set aside 10 to 20 minutes to practice slow effortless diaphragmatic breathing at about 6-breaths-per-minute. In the beginning 10 to 20 minutes may be too long, thus in some cases have the person practice a few times a day for two minutes and slowly build up to 10 or more minutes. The practice is not just a mechanical process of breathing it includes mindfulness training. Namely, as you are breathing each time you exhale imagine a flow doing down your arms and legs and as you inhale an energy coming into you. Whenever your attention drifts bring it back to the breathing.
- Integrate breathing with daily activities. Practice slower breather before eating, after putting the seat belt on in the car, or whenever a notification pops up on the cell phone.
- Set reminders and alarms on your phone to check how you are feeling and breathing. Leave notes on nearby furniture such as a nightstand, on the shower door, and/or on the kitchen table as reminders to be mindful of your breath. If stressed or breathing shallowly, take a moment to breathe slowly.
- Interrupt the stress response. During the day when you are aware that you shallow breathe, are holding your breath, feel anxious, experience neck and shoulder tightness, or worry and use that as a cue to shift position by sitting or standing more erect, looking upward and take a few slow diaphragmatic breaths.
- Use cue condition to facilitate this process. Each time you begin the practice smell a specific aroma or do some behavioral movement and then do the breathing. After a while the aroma or behavioral movement will become the classically conditioned cue to trigger the effortless breathing.
- Use role rehearsal and conditioning to generalize the skill. Generalizing the skills often takes more time than what may be expected. In a culture where instant relief is expected— implied message associated with medication— self-mastery techniques are different and challenging as they take time to master the skill and implement them during daily life. The process of mastery is similar to learning to play a musical instrument or sports. Learning to play the violin requires practice as well as practice with failures along the way until one is ready for more challenging musical pieces, recitals, or performances.
A useful strategy to implement the learning is role rehearsal in the office, at home at work, and in real life. It is usually much easier to practice these skills in a safe space such as your own room or, with a therapist compared to with other people or, at work. To generalize the skill most efficiently, it can be helpful to practice in a safe environment while imagining being in the actual stressful location This process is illustrated by the strategy to reduce social anxiety and menstrual cramps.
Social anxiety when seeing my supervisor. Master effortless breathing in a safe environment. Role rehearsal in imagery. If you observed that you held your breath when your supervisor is around, begin with imagery when your supervisor is not present. Sit, comfortably. Let go of muscle tension and breathe effortlessly, evoking a scenario where your supervisor is walking by and continue to breathe slowly as you imagine the scene. Role rehearsal in action. Ask another person to role-play your supervisor. Sit, comfortably. Let go of muscle tension and breathe effortlessly. Have this person walk into the room in a similar way that your supervisor would. Imagine that person is your supervisor while practicing your effortless breathing. Repeat until the effortless breathing is more automatic. Practice many times in real life. Whenever the rehearsed situation occurs, implement slower paced breathing.
Menstrual cramps that causes most women to curl up and breathe shallowly when experiencing menstrual cramps (Peper et al., 2023). Master effortless breathing in a safe environment. Practice breathing lying down. While lying down, breathe diaphragmatically by having a three-to-five-pound weight such as a bag of rice or hot water pad on your abdomen. If you have a partner, have the person stroke your legs from the abdomen to your toes while you exhale. Role rehearse experiencing pain and then practice lower diaphragmatic breathing. Namely, tighten your abdomen as if you have discomfort, then focus on relaxing the buttocks and sensing the air flowing down your legs and out your feet as you exhale. Practice in real life. A few days before you expected menstruation, practice slow diaphragmatic breathing several times for at least 5-10 minutes during the day. When your menstruation starts practice the slower and lower breathing while imagining the air flowing down the abdomen, through the legs and out the feet.
Summary/Conclusion
Breathing is the mind-body bridge. It usually occurs without awareness and breathing changes affect our thought, emotions and body. Mastering and implementing slower breathing during the day takes time and practice. By observing when breathing patterns change, participants may identify internal and external factors that affect breathing which provides an opportunity to implement effortless diaphragmatic breathing to optimize health as well as resolve some of the triggers. As one 20-year-old, female student reported,
The biggest benefit from learning diaphragmatic breathing was that it gave me the feeling of safety in many moments. My anxiety tended to make me feel unsafe in many situations but homing in and mastering diaphragmatic breathing helped tremendously. I shifted from constant chest breathing to acknowledging it and in turn, reminding myself to breathe with my diaphragm.
References
Allen, R. (2024). The health benefits of nose breathing. Nursing in General Practice. http://hdl.handle.net/10147/559021
Al-Rabia, M.W. (2016). Food-induced immunoglobulin E-mediated allergic rhinitis. J Microsc Ultrastruct, 4(2), 69-75. https://doi.org/doi.org/10.1016/j.jmau.2015.11.004
Anziani, M. & Peper, E. (2021). Healing from paralysis-Music (toning) to activate health. Peperperspective –ideas on illness, health and well-being from Erik Peper. Accessed April 16, 2024. https://peperperspective.com/2021/11/22/healing-from-paralysis-music-toning-to-activate-health/
Banushi, B., Brendle, M., Ragnhildstveit, A., Murphy, T., Moore, C., Egberts, J., & Robison, R. (2023). Breathwork Interventions for Adults with Clinically Diagnosed Anxiety Disorders: A Scoping Review. Brain Sci. 13(2), 256. https://doi.org/10.3390/brainsci13020256
Chung, A.H., Gevirtz, R.N., Gharbo, R.S. et al. (2021).Pilot Study on Reducing Symptoms of Anxiety with a Heart Rate Variability Biofeedback Wearable and Remote Stress Management Coach. Appl Psychophysiol Biofeedback 46, 347–358. https://doi.org/10.1007/s10484-021-09519-x
Cohen, D. & Leung, A.K.Y. (2009). The hard embodiment of culture. European Journal of Social Psychology, 9, 1278–1289 https://doi.org/10.1002/ejsp.671
Codrons, E., Bernardi, N. F., Vandoni, M., & Bernardi, L. (2014). Spontaneous group synchronization of movements and respiratory rhythms. PloS one, 9(9), e107538. https://doi.org/10.1371/journal.pone.0107538
Dick, T. E., Mims, J. R., Hsieh, Y. H., Morris, K. F., & Wehrwein, E. A. (2014). Increased cardio-respiratory coupling evoked by slow deep breathing can persist in normal humans. Respiratory physiology & neurobiology, 204, 99-111. https://doil.org/10.1016/j.resp.2014.09.013
Ekerholt, K. & Bergland, A. (2008). Breathing: A sign of life and a unique area for reflection and action. Physical therapy, 88(7), 832-840. https://doi.org/10.2522/ptj.20070316
Elstad, M., O’Callaghan, E. L., Smith, A. J., Ben-Tal, A., & Ramchandra, R. (2018). Cardiorespiratory interactions in humans and animals: rhythms for life. American Journal of Physiology-Heart and Circulatory Physiology, 315(1), H6-H17. https://doi.org/10.1152/ajpheart.00701.2017
Folgering, H. (1999). The pathophysiology of hyperventilation syndrome. Monaldi Arch Chest Dis, 54(4), 365-72. https://pubmed.ncbi.nlm.nih.gov/10546483/
Gilbert, C. (1998). Emotional sources of dysfunctional breathing. Journal of bodywork and movement therapies, 2(4), 224-23. https://doi.org/10.1016/S1360-8592(98)80019-3
Jerath, R., Beveridge, C., & Barnes, V.A. (2019). Self-Regulation of Breathing as an Adjunctive Treatment of Insomnia. Front Psychiatry, 9(780). https://doi.org/10.3389/fpsyt.2018.00780
Kahn, S. & Ehrlich, P.R. (2018). Jaws. Stanford, CA: Stanford University Press. https://www.amazon.com/Jaws-Hidden-Epidemic-Sandra-Kahn/dp/1503604136/ref=tmm_hrd_swatch_0?_encoding=UTF8&qid=1685135054&sr=1-1
Kang, K.W., Jung, S.I., Lee, do Y., Kim, K., & Lee, N.K. (2016) Effect of sitting posture on respiratory function while using a smartphone. J Phys Ther Sci, 28(5), 1496-8. https://doi.org/10.1589/jpts.28.1496
Leal, R.B., Gomes, M.C., Granville-Garcia, A.F., Goes, P.S.A., & de Menezes, V.A. (2016). Impact of Breathing Patterns on the Quality of Life of 9- to 10-year-old Schoolchildren. American Journal of Rhinology & Allergy, 30(5):e147-e152. https://doi.org/10.2500/ajra.2016.30.4363
Lehrer, P.M. & Gevirtz, R. (2014). Heart rate variability biofeedback: how and why does it work? Front Psychol. 5, 756. https://doi.org/10.3389/fpsyg.2014.00756
Lundberg, J.O. & Weitzberg, E. (1999). Nasal nitric oxide in man. Thorax. (10):947-52. https://doi.org/10.1136/thx.54.10.947
Luthe, W. (1979). About the Methods of Autogenic Therapy. In: Peper, E., Ancoli, S., Quinn, M. (eds). Mind/Body Integration. Springer, Boston, MA. https://doi.org/10.1007/978-1-4613-2898-8_12
Luthe, W. & Schultz, J. H. (1970). Autogenic therapy: Medical applications. New York: Grune and Stratton. https://www.amazon.com/Autogenic-Therapy-II-Medical-Applications/dp/B001J9W7L6
MacHose, M., & Peper, E. (1991). The effect of clothing on inhalation volume. Biofeedback and Self-Regulation, 16(3), 261–265. https://doi.org/10.1007/BF01000020
Magnon. V., Dutheil, F., & Vallet, G.T. (2021). Benefits from one session of deep and slow breathing on vagal tone and anxiety in young and older adults. Sci Rep. 11(1),19267. https://doi.org/10.1038/s41598-021-98736-9
Maric, V., Ramanathan, D., & Mishra, J. (2020). Respiratory regulation & interactions with neuro-cognitive circuitry. Neuroscience & Biobehavioral Reviews, 112, 95-106. https://doi.org/10.1016/j.neubiorev.2020.02.001
Matić, Z., Platiša, M. M., Kalauzi, A., & Bojić, T. (2020). Slow 0.1 Hz breathing and body posture induced perturbations of RRI and respiratory signal complexity and cardiorespiratory coupling. Frontiers in physiology, 11, 24. https://doi.org/10.3389/fphys.2020.00024
McKeown, P. (2021). The Breathing Cure: Develop New Habits for a Healthier, Happier, and Longer Life. Boca Raton, Fl “Humanix Books. https://www.amazon.com/BREATHING-CURE-Develop-Healthier-Happier/dp/1630061972/
Meehan, Z.M. & Shaffer, F. (2023). Adding Core Muscle Contraction to Wrist-Ankle Rhythmical Skeletal Muscle Tension Increases Respiratory Sinus Arrhythmia and Low-Frequency Power. Appl Psychophysiol Biofeedback. 48(1), 127-134. https://doi.org/10.1007/s10484-022-09568-w
McKeown, P. (2021). The breathing cure: Develop new habits for a healthier, happier, and longer life. Humanix Books. https://www.amazon.com/BREATHING-CURE-Develop-Healthier-Happier/dp/1630061972/
Peper, E., Booiman, A., Lin, I-M, Harvey, R., & Mitose, J. (2016). Abdominal SEMG Feedback for Diaphragmatic Breathing: A Methodological Note. Biofeedback. 44(1), 42-49. https://doi.org/10.5298/1081-5937-44.1.03
Peper, E., Chen, S., Heinz, N. & Harvey, R. (2023). Hope for menstrual cramps (dysmenorrhea) with breathing. Biofeedback, 51(2), 44–51. https://doi.org/10.5298/1081-5937-51.2.04
Peper, E. & Cohen, T. (2017). Inhale to Breathe Away Pelvic Floor Pain and Enjoy Intercourse. Biofeedback, 45 (1), 21–24. https://doi.org/10.5298/1081-5937-45.1.04
Peper, E., Gilbert, C.D., Harvey, R. & Lin, I-M. (2015). Did you ask about abdominal surgery or injury? A learned disuse risk factor for breathing dysfunction. Biofeedback. 34(4), 173-179. https://doi.org/10.5298/1081-5937-43.4.06
Peper, E., Harvey, R., Cuellar, Y., & Membrila, C. (2022). Reduce anxiety. NeuroRegulation, 9(2), 91–97. https://doi.org/10.15540/nr.9.2.91
Peper, E., Harvey, R., & Hamiel, D. (2019). Transforming thoughts with postural awareness to increase therapeutic and teaching efficacy. NeuroRegulation, 6(3),153-169. https://doi.org/10.15540/nr.6.3.153
Peper, E., Harvey, R. & Rosegard, E. (2024). Increase attention, concentration and school performance with posture feedback. Biofeedback, 52(2). https://doi.org/10.5298/1081-5937-52.02.07 or https://www.researchgate.net/publication/383151816_WHAT_ABOUT_THIS_Increase_Attention_Concentration_and_School_Performance_with_Posture_Feedback
Peper, E. & MacHose, M. (1993). Symptom prescription: Inducing anxiety by 70% exhalation. Applied Psychophysiology and Biofeedback, 18(3), 133-138. https://doi.org/10.1007/BF00999790
Peper, E., Mason, L., Harvey, R., Wolski, L, & Torres, J. (2020). Can acid reflux be reduced by breathing? Townsend Letters-The Examiner of Alternative Medicine, 445/446, 44-47. https://www.townsendletter.com/article/445-6-acid-reflux-reduced-by-breathing/
Peper, E., Mason, L., Huey, C. (2017). Healing irritable bowel syndrome with diaphragmatic breathing. Biofeedback. 45(4), 83–87. https://doi.org/10.5298/1081-5937-45.4.04
Peper, E., Oded, Y., & Harvey, R. (2024a). Quick somatic rescue techniques when stressed. Biofeedback, 52(1), 18–26. https://doi.org/10.5298/982312
Peper, E., Pollack, W., Harvey, R., Yoshino, A., Daubenmier, J. & Anziani, M. (2019a). Which quiets the mind more quickly and increases HRV: Toning or mindfulness? NeuroRegulation, 6(3), 128-133. https://doi.org/10.15540/nr.6.3.12
Peper, E., Swatzyna, R., & Ong, K. (2023). Mouth breathing and tongue position: a risk factor for health. Biofeedback. 51(3), 74–78 https://doi.org/10.5298/912512
PTI. (2023 August 3). Often suck your stomach in to look slimmer in pictures? It can lead to ‘hourglass syndrome.’ The Economic Times Panache. Accessed March 26, 2024. https://economictimes.indiatimes.com/magazines/panache/often-suck-your-stomach-in-to-look-slimmer-in-pictures-it-can-lead-to-hourglass-syndrome/articleshow/102392681.cms?from=mdr
Salah, H.M., Goldberg, L.R., Molinger, J., Felker, G.M., Applefeld, W., Rassaf, T., Tedford, R.J., Mirro, M., Cleland, J.GF., & Fudim, M. (2022). Diaphragmatic Function in Cardiovascular Disease: JACC Review Topic of the Week, Journal of the American College of Cardiology, 80(17), 1647-1659. https://doi.org/10.1016/j.jacc.2022.08.760
Shaffer, F. & Meehan, Z.M. (2020). A Practical Guide to Resonance Frequency Assessment for Heart Rate Variability Biofeedback. Frontiers in Neuroscience,14. https://www.frontiersin.org/journals/neuroscience/articles/10.3389/fnins.2020.570400
Steffen, P.R., Austin, T., DeBarros, A., & Brown, T. (2017). The Impact of Resonance Frequency Breathing on Measures of Heart Rate Variability, Blood Pressure, and Mood. Front Public Health, 5, 222. https://doi.org/10.3389/fpubh.2017.00222
Taub, E., Uswatte, G., Mark, V. W., Morris, D. M. (2006). The learned nonuse phenomenon: Implications for rehabilitation. Europa Medicophysica, 42(3), 241-256. https://pubmed.ncbi.nlm.nih.gov/17039223/
van Bon, M.J., Zielhuis, G.A., Rach, G.H., & van den Broek, P. (1989). Otitis media with effusion and habitual mouth breathing in Dutch preschool children. Int J Pediatr Otorhinolaryngol, (2), 119-25. https://doi.org/10.1016/0165-5876(89)90087-6
Xiao, M., Zi-Qi, Y., Gong, Z.Q., Zhang, H., Duan, N.Y., Shi, Y.T,, Wei, G.X., Li, Y.F. (2017).The Effect of Diaphragmatic Breathing on Attention, Negative Affect and Stress in Healthy Adults. Front Psychol. 8(874). https://doi.org/10.3389/fpsyg.2017.00874
Is mindfulness training old wine in new bottles?
Posted: January 11, 2024 Filed under: attention, behavior, biofeedback, Breathing/respiration, CBT, cognitive behavior therapy, healing, health, meditation, self-healing, stress management | Tags: anxiety, autogenic training, biofeedback, health, meditation, mental-health, mindfulness, pain, passive attention, progressive muscle relaxation, wellness, yoga 2 CommentsAdapted from: Peper, E., Harvey, R., & Lin, I-M. (2019). Mindfulness training has themes common to other technique. Biofeedback. 47(3), 50-57. https://doi.org/10.5298/1081-5937-47.3.02
This extensive blog discusses the benefits of mindfulness-based meditation (MM) techniques and explores how similar beneficial outcomes occur with other mind-centered practices such as transcendental meditation, and body-centered practices such as progressive muscle relaxation (PMR), autogenic training (AT), and yoga. For example, many standardized mind-body techniques such as mindfulness-based stress reduction and mindfulness-based cognitive therapy (a) are associated with a reduction in symptoms of symptoms such as anxiety, pain and depression. This article explores the efficacy of mindfulness based techniques to that of other self-regulation techniques and identifies components shared between mindfulness based techniques and several previous self-regulation techniques, including PMR, AT, and transcendental meditation. The authors conclude that most of the commonly used self-regulation strategies have comparable efficacy and share many elements.
Mindfulness-based strategies are based in ancient Buddhist practices and have found acceptance as one of the major contemporary behavioral medicine techniques (Hilton et al, 2016; Khazan, 2013). Throughout this blog the term mindfulness will refer broadly to a mental state of paying total attention to the present moment, with a non-judgmental awareness of the inner and/ or outer experiences (Baer et al., 2004; Kabat-Zinn, 1994).
In 1979, Jon Kabat-Zinn introduced a manual for a standardized Mindfulness-Based Stress Reduction (MBSR) program at the University of Massachusetts Medical Center (Kabat-Zinn, 1994, 2003). The eight-week program combined mindfulness as a form of insight meditation with specific types of yoga breathing and movements exercises designed to focus on awareness of the mind and body, as well as thoughts, feelings, and behaviors.
There is a substantial body of evidence that mindfulness-based cognitive therapy (MBCT); Teasdale et al., 1995) and mindfulness-based stress reduction (MBSR) (Kabat-Zinn, 1994, 2003) have combined with skills of cognitive therapy for ameliorating stress symptoms such as negative thinking, anxiety and depression. For example, MBSR and MBCT has been confirmed to be clinical beneficial in alleviating a variety of mental and physical conditions, for people dealing with anxiety, depression, cancer-related pain and anxiety, pain disorder, or high blood pressure (The following are only a few of the hundred studies published: Andersen et al., 2013; Carlson et al., 2003; Fjorback et al., 2011; Greeson, & Eisenlohr-Moul, 2014; Hoffman et al., 2012; Marchand, 2012; Baer, 2015; Demarzo et al., 2015; Khoury et al, 2013; Khoury et al, 2015; Chapin et al., 2014; Witek Janusek et al., 2019). Currently, MBSR and MBCT techniques that are more standardized are widely applied in schools, hospitals, companies, prisons, and other environments.
The Relationship Between Mindfulness and Other Self-Regulation Techniques
This section addresses two questions: First, how do mindfulness-based interventions compare in efficacy to older self-regulation techniques? Second, and perhaps more basically, how new and different are mindfulness-based therapies from other self-regulation-oriented practices and therapies?
Is mindfulness more effective than other mind/body body/mind approaches?
Although mindfulness-based meditation (MM) techniques are effective, it does not mean that is is more effective than other traditional meditation or self-regulation approaches. To be able to conclude that MM is superior, it needs to be compared to equivalent well-coached control groups where the participants were taught other approaches such as progressive relaxation, autogenic training, transcendental meditation, or biofeedback training. In these control groups, the participants would be taught by practitioners who were self-experienced and had mastered the skills and not merely received training from a short audio or video clip (Cherkin et al, 2016). The most recent assessment by the National Centere for Complementary and Integrative Health, National Institutes of Health (NCCIH-NIH, 2024) concluded that generally “the effects of mindfulness meditation approaches were no different than those of evidence-based treatments such as cognitive behavioral therapy and exercise especially when they include how to generalize the skills during the day” (NCCIH, 2024). Generalizing the learned skills into daily life contributes to the successful outcome of Autogenic Training, Progressive Relaxation, integrated biofeedback stress management training, or the Quieting Response (Luthe, 1979; Davis et al., 2019; Wilson et al., 2023; Stroebel, 1982).
Unfortunately, there are few studies that compare the effective of mindfulness meditation to other sitting mental techniques such as Autogenic Training, Transcendental Meditation or similar meditative practices that are used therapeutically. When the few randomized control studies of MBSR versus autogenic training (AT) was done, no conclusions could be drawn as to the superior stress reduction technique among German medical students (Kuhlmann et al., 2016).
Interestingly, Tanner, et al (2009) in a waitlist study of students in Washington, D.C. area universities practicing TM used the concept of mindfulness, as measured by the Kentucky Inventory of Mindfulness Skills (KIM) (Baer et al, 2004) as a dependent variable, where TM practice resulted in greater degrees of ‘mindfulness.’ More direct comparisons of MM with body-focused techniques, such as progressive relaxation, or Autogenic training mindfulness-based approaches, have not found superior benefit. For example, Agee et al (2009) compared the stress management effects of a five-week Mindfulness Meditation (MM) to a five-week Progressive Muscle Relaxation (PMR) course and found no meaningful reports of superiority of one over the other program; both MM and PMR were effective in reducing symptoms of stress.
In a persuasive meta-analysis comparing MBSR with other similar stress management techniques used among military service members, Crawford, et al (2013) described various multimodal programs for addressing post-traumatic stress disorder (PTSD) and other military or combat-related stress reactions. Of note, Crawford, et al (2013) suggest that all of the multi-modal approaches that include Autogenic Training, Progressive Muscle Relaxation, movement practices including Yoga and Tai Chi, as well as Mindfulness Meditation, and various types of imagery, visualization and prayer-based contemplative practices ALL provide some benefit to service members experiencing PTSD.
An important observation by Crawford et al (2013) pointed out that when military service members had more physical symptoms of stress, the meditative techniques appeared to work best, and when the chief complaints were about cognitive ruminations, the body techniques such as Yoga or Tai Chi worked best to reduce symptoms. Whereas it may not be possible to say that mindfulness meditation practices are clearly superior to other mind-body techniques, it may be possible to raise questions about mechanisms that unite the mind-body approaches used in therapeutic settings.
Could there be negative side effects?
Another point to consider is the limited discussion of the possible absence of benefit or even harms that may be associated with mind-body therapies. For example, for some people, meditation does not promote prosocial behavior (Kreplin et al, 2018). For other people, meditation can evoke negative physical and/or psychological outcomes (Lindahl et al, 2017; Britton et al., 2021). There are other struggles with mind-body techniques when people only find benefit in the presence of a skilled clinician, practitioner, or guru, suggesting a type of psychological dependency or transference, rather than the ability to generalize the benefits outside of a set of conditions (e.g. four to eight weeks of one to four hour trainings) or a particular setting (e.g. in a natural and/or quiet space).
Whereas the detailed instructions for many mindfulness meditation trainings, along with many other types of mind-body practices (e.g. Transcendental Meditation, Autogenic Training, Progressive Muscle Relaxation, Yoga, Tai Chi…) create conditions that are laudable because they are standardized, a question is raised as to ‘critical ingredients’, using the metaphor of baking. The difference between a chocolate and a vanilla cake is not ingredients such as flour, or sugar, etc., which are common to all cakes, but rather the essential or critical ingredient of the chocolate or vanilla flavoring. So what are the essential or critical ingredients in mind-body techniques? Extending the metaphor, Crawford, et al (2013, p. 20) might say the critical ingredient common to the mind-body techniques they studied was that people “can change the way their body and mind react to stress by changing their thoughts, emotions, and behaviors…” with techniques that, relatively speaking, “involve minimal cost and training time.”
The skeptical view suggested here is that MM techniques share similar strategies with other mind-body approaches that encouraging learners to ‘pay attention and shift intention.’ This strategy is part of the instructions when learning Progressive Relaxation, Autogenic Training, Transcendental Meditation, movement meditation of Yoga and Tai Chi and, with instrumented self-regulation techniques such as bio/neurofeedback. In this sense, MM training repackages techniques that have been available for millennia and thus becomes ‘old wine sold in new bottles.’
We wonder if a control group for compassionate mindfulness training would report more benefits if they were asked not only to meditate on compassionate acts, but actually performed compassionate tasks such as taking care of person in pain, helping a homeless person, or actually writing and delivering a letter of gratitude to a person who has helped them in the past? The suggestion is to titrate the effects of MM techniques, moving from a more basic level of benefit to a more fully actualized level of benefit, generalizing their skill beyond a training setting, as measured by the Baer et al (2004) Kentucky Inventory of Mindfulness Skills.
Each generation of clinicians and educators rediscover principles without always recognizing that the similar principles were part of the previous clinical interventions. The analogies and language has changed; however, the underlying concepts may be the same. Mindfulness interventions are now the new, current and popular approach. Some of the underlying ‘mindfulness’ concepts that are shared in common with successfully other mind-body and self-regulation approaches include:
The practitioner must be self-experienced in mindfulness practice. This means that the practitioners do not merely believe the practice is effective; they know it is effective from self-experience. Inner confidence conveyed to clients and patients enhances the healing/placebo effect. It is similar to having sympathy or empathy for clients and patients that occurs from have similar life experiences, such as when a clinician speaks to a patient. For example, a male physician speaking to a female patient who has had a mastectomy may be compassionate; however, empathy occurs more easily when another mastectomy patient (who may also be a physician) shares how she struggled overcame her doubts and can still be loved by her partner.
There may also be a continuum of strengthening beliefs about the benefits of mindfulness techniques that leads to increase benefits for the approach. Knowing there are some kinds of benefits from initiating a practice of mindfulness increases empathy/compassion for others as they learn. Proving that mindfulness techniques are causing benefits after systematically comparing their effectiveness with other approaches strengthens the belief in the mindfulness approaches. Note that a similar process of strengthening one’s belief in an approach occurs gradually, over time as clients and patients progress through beginner, intermediate and advanced levels of mind-body practices.
Observing thoughts without being captured. Being a witness to the thoughts, emotions, and external events results in a type of covert global desensitization and skill mastery of NOT being captured by those thoughts and emotions. This same process of non-attachment and being a witness is one of the underpinnings of techniques that tacitly and sometime covertly support learning ways of controlling attention, such as with Autogenic Training; namely how to passively attend to a specific body part without judgment and, report on the subjective experience without comparison or judgment.
Ongoing daily practice. Participants take an active role in their own healing process as they learn to control and focus their attention. Participants are often asked to practice up to one hour a day and apply the practices during the day as mini-practices or awareness cues to interrupt the dysfunctional behavior. For example in Autogenic training, trainees are taught to practice partial formula (such my “neck and shoulders are heavy”) during the day to bring the body/mind back to balance. While with Progressive Relaxation, the trainee learns to identify when they tighten inappropriate muscles (dysponesis) and then inhibit this observed tension.
Peer support by being in a group. Peer support is a major factor for success as people can share their challenges and successes. Peer support tends to promote acceptance of self-and others and provides role modeling how to cope with stressors. It is possible that some peer support groups may counter the benefits of a mind-body technique, especially when the peers do not provide support or may in fact impede progress when they complain of the obstacles or difficulties in their process.
These concepts are not unique to Mindfulness Meditation (MM) training. Similar instructions have been part of the successful/educational intervention of Progressive Relaxation, Autogenic Training, Yogic practices, and Transcendental Meditation. These approaches have been most successful when the originators, and their initial students, taught their new and evolving techniques to clients and patients; however, they became less successful as later followers and practitioners used these approaches without learning an in-depth skill mastery. For example, Progressive relaxation as taught by Edmund Jacobson consisted of advanced skill mastery by developing subtle awareness of different muscle tension that was taught over 100 sessions (Mackereth & Tomlinson, 2010). It was not simply listening once to a 20-minute audio recording about tightening and relaxing muscles. Similarly, Autogenic training is very specific and teaches passive attention over a three to six-month time-period while the participant practices multiple times daily. Stating the obvious, learning Autogenic Training, Mindfulness, Progressive Relaxation, Bio/Neurofeedback or any other mind-body technique is much more than listening to a 20-minute audio recording.
The same instructions are also part of many movement practices. For many participants focusing on the movement automatically evoked a shift in attention. Their attention is with the task and they are instructed to be present in the movement.
Areas to explore.
Although Mindfulness training with clients and patients has resulted in remarkable beneficial outcomes for the participants, it is not clear whether mindfulness training is better than well taught PR, AT, TM or other mind/body or body/mind approaches. There are also numerous question to explore such as: 1) Who drops out, 2) Is physical exercise to counter sitting disease and complete the alarm reaction more beneficial, and 3) Strategies to cope with wandering attention.
- Who drops out?
We wonder if mindfulness is appropriate for all participants as sometimes participants drop out or experience negative abreactions. It not clear who those participants are. Interestingly, hints for whom the techniques may be challenging can be found in the observations of Autogenic Training that lists specific guidelines for contra-, relative- and non-indications (Luthe, 1970).
- Physical movement to counter sitting disease and complete the alarm reaction.
Although many mindfulness meditation practices may include yoga practices, most participants practice it in a sitting position. It may be possible that for some people somatic movement practices such as a slow Zen walk may quiet the inner dialogue more quickly. In our experience, when participants are upset and highly stressed, it is much easier to let go of agitation by first completing the triggered fight/flight response with vigorous physical activity such as rapidly walking up and downs stairs while focusing on the burning sensations of the thigh muscles. Once the physical stress reaction has been completed and the person feels physically calmer then the mind is quieter. Then have the person begin their meditative practice.
- Strategies to cope with wandering attention.
Some participants have difficulty staying on task, become sleepy, worry, and/or are preoccupied. We observed that first beginning with physical movement practices or Progressive Relaxation appears to be a helpful strategy to reduce wandering thoughts. If one has many active thoughts, progressive relaxation continuously pulls your attention to your body as you are directed to tighten and let go of muscle groups. Being guided supports developing the passive focus of attention to bring awareness back to the task at hand. Once internally quieter, it is easier hold their attention while doing Autogenic Training, breathing or Mindfullness Meditation.
By integrating somatic components with the mindfulness such as done in Progressive Relaxation or yoga practices facilitates the person staying present. Similarly, when teaching slower breathing, if a person has a weight on their abdomen while practicing breathing, it is easier to keep attending to the task: allow the weight to upward when inhaling and feeling the exhalation flowing out through the arms and legs.
Therapeutic and education strategies that implicitly incorporate mindfulness
Progressive relaxation
In the United States during the 1920 progressive relaxation (PR) was developed and taught by Edmund Jacobson (1938). This approach was clinically very successful for numerous illnesses ranging from hypertension, back pain, gastrointestinal discomfort, and anxiety; it included 50 year follow-ups. Patients were active participants and practiced the skills at home and at work and interrupt their dysfunctional patterns during the day such as becoming aware of unnecessary muscle tension (dyponetic activity) and then release the unnecessary muscle tension (Whatmore & Kohli, 1968). This structured approach is totally different than providing an audio recording that guides clients and patients through a series of tightening and relaxing of their muscles. The clinical outcome of PR when taught using the original specific procedures described by Jacobson (1938) was remarkable. The incorporation of Progressive Relaxation as the homework practice was an important cofactor in the successful outcome in the treatment of muscle tension headache using electromyography (EMG) biofeedback by Budzynski, Stoyva and Adler (1970).
Autogenic Training
In 1932 Johannes Schultz in Germany published a book about Autogenic Training describing the basic training procedure. The basic autogenic procedure, the standard exercises, were taught over a minimum period of three month in which the person practiced daily. In this practice they directed theri passive attention to the following cascading sequence: heaviness of their arms, warmth of their arms, heart beat calm and regular, breathing calm and regular or it breathes me, solar plexus is warm, forehead is cool, and I am at peace (Luthe, 1979). Three main principles of autonomic training mentioned by Luthe (1979) are: (1) mental repetition of topographically oriented verbal formulae for brief periods; (2) passive concentration; and (3) reduction of exteroceptive and proprioceptive afferent stimulation. The underlying concepts of Autogenic Therapy include as described by Peper and Williams (1980):
The body has an innate capacity for self-healing and it is this capacity that is allowed to become operative in the autogenic state. Neither the trainer nor trainee has the wisdom necessary to direct the course of the self-balancing process; hence, the capacity is allowed to occur and not be directed.
- Homeostatic self-regulation is encouraged.
- Much of the learning is done by the trainee at home; hence, the responsibility for the training lies primarily with the trainee.
- The trainer/teacher must be self-experience in the practice.
- The attitude necessary for successful practice is one of passive attention; active striving and concern with results impedes the learning process. An attitude of acceptance is cultivated, letting be whatever comes up. This quality of attention is known as “mindfulness’ in meditative traditions.
The clinical outcome for autogenic therapy is very promising. The detailed guided self-awareness training and uncontrolled studies showed benefits across a wide variety of psychosomatic illness such as asthma, cancer, hypertension, anxiety, pain irritable bowel disease, depression (Luthe & Schultz, 1970a; Luthe & Schultz, 1970b). Autogenic training components have also been integrated in biofeedback training. Elmer and Alice Green included the incorporation of autogenic training phrases with temperature biofeedback for the very successful treatment of migraines (Green & Green, 1989). Autonomic training combine with biofeedback in clinical practices produced better results than control group for headache population (Luthe, 1979). Empirical research found that autonomic training was applied efficiently in emotional and behavioral problems, and physical disorder (Klott, 2013), such as skin disorder (Klein & Peper, 2013), insomnia (Bowden et al., 2012), Meniere’s disease (Goto, Nakai, & Ogawa, 2011) and the multitude of stress related symptoms (Wilson et al., 2023).
Bio/neurofeedback training
Starting in the late 1960s, biofeedback procedures have been developed as a successful treatment approach for numerous illnesses ranging from headaches, hypertension, to ADHD (Peper et al., 1979; Peper & Shaffer, 2010; Khazan, 2013). In most cases, the similar instructions that are part of mindfulness meditation are also embedded in the bio/neurofeedback instructions. The participants are instructed to learn control over some physiological parameter and then practice the same skill during daily life. This means that during the learning process, the person learn passive attention and is not be captured by marauding thoughts and feeling. and during the day develop awareness Whenever they become aware of dysfunctional patterns, thoughts, emotions, they initiated their newly learned skill. The ongoing biological feedback signals continuously reminds them to focus.
Transcendental meditation
The next fad to hit the American shore was Transcendental Meditation (TM)– a meditation practice from the ancient Vedic tradition in India. The participant were given a mantra that they mentally repeated and if their attention wanders, they go back to repeating the mantra internally. The first study that captured the media’s attention was by Wallace (1970) published in the Journal Science which reported that “During meditation, oxygen consumption and heart rate decreased, skin resistance increased, and the electroencephalogram showed specific changes in certain frequencies. These results seem to distinguish the state produced by Transcendental Meditation from commonly encountered states of consciousness and suggest that it may have practical applications.” (Wallace, 1970).
The participants were to practice the mantra meditation twice a day for about 20 minutes. Meta-analysis studies have reported that those who practiced TM as compared to the control group experienced significant improved of numerous disorders such as CVD risk factors, anxiety, metabolic syndrome, drug abuse and hypertension (Paul-Labrador et al, 2006; Rainforth et al., 2007; Hawkins, 2003).
To make it more acceptable for the western audience, Herbert Benson, MD, adapted and simplified techniques from TM training and then labelled a core element, the ‘relaxation response’ (Benson et al., 1974) Instead of giving people a secret mantra and part of a spiritual tradition, he recommend using the word “one” as the mantra. Numerous studies have demonstrated that when patients practice the relaxation response, many clinical symptoms were reduced. The empirical research found that practiced transcendental meditation caused increasing prefrontal low alpha power (8-10Hz) and theta power of EEG; as well as higher prefrontal alpha coherence than other locations at both hemispheres. Moreover, some individuals also showed lower sympathetic activation and higher parasympathetic activation, increased respiratory sinus arrhythmic and frontal blood flow, and decreased breathing rate (Travis, 2001, 2014). Although TM and Benson’s relaxation response continues to be practiced, mindfulness has taking it place.
Conclusion
Mindfulness-Based Stress Reduction (MBSR) and Mindfulness-Based Cognitive Therapy (MBCT) are very beneficial and yet may be considered ‘old wine in new bottles’ where the metaphor refers to millennia old meditation techniques as ‘old wine’ and the acronyms such as MBSR or MBCT as ‘new bottles’. Like many other ‘new’ therapeutic approaches or for that matter, many other ‘new’ medications, use it now before it becomes stale and loses part of its placebo power. As long as the application of a new technique is taught with the intensity and dedication of the promotors of the approach, and as long as the participants are required to practice while receiving support, the outcomes will be very beneficial, and most likely similar in effect to other mind-body approaches.
The challenge facing mindfulness practices just as those from Autogenic Training, Progressive Relaxation and Transcendental Meditation, is that familiarity breeds contempt and that clients and therapists are continuously looking for a new technique that promises better outcome. Thus as Mindfulness training is taught to more and more people, it may become less promising. In addition, as mindfulness training is taught in less time, (e.g. fewer minutes and/or fewer sessions), and with less well-trained instructors, who may offer less support and supervision for people experiencing possible negative effects, the overall benefits may decrease. Thus, mindfulness practice, Autogenic training, progressive relaxation, Transcendental Meditation, movement practices, meditation, breathing practices as well as the many spiritual practices all appear to share common fate of fading over time. Whereas the core principles of mind-body techniques are ageless, the execution is not always assured.
References
Agee, J. D., Danoff-Burg, S., & Grant, C. A. (2009). Comparing brief stress management courses in a community sample: Mindfulness skills and progressive muscle relaxation. Explore: The Journal of Science and Healing, 5(2), 104-109. https://doi.org/10.1016/j.explore.2008.12.004
Andersen, S. R., Würtzen, H., Steding-Jessen, M., Christensen, J., Andersen, K. K., Flyger, H., … & Dalton, S. O. (2013). Effect of mindfulness-based stress reduction on sleep quality: Results of a randomized trial among Danish breast cancer patients. Acta Oncologica, 52(2), 336-344. https://doi.org/10.3109/0284186X.2012.745948
Alvarez-Jimenez, M., Gleeson, J. F., Bendall, S., Penn, D. L., Yung, A. R., Ryan, R. M., … Nelson, B. (2018). Enhancing social functioning in young people at Ultra High Risk (UHR) for psychosis: A pilot study of a novel strengths and mindfulness-based online social therapy. Schizophrenia Research, 202, 369-377 https://doi.org/10.1016/j.schres.2018.07.022
Baer, R. A. (2003). Mindfulness training as a clinical intervention: A conceptual and empirical review. Clinical Psychology: Science and Practice, 10, 125–143. https://doi.org/10.1093/clipsy/bpg015
Baer, R. A.. (2015). Mindfulness-based treatment approaches: Clinician’s guide to evidence base and applications. New York: Elsevier. https://www.elsevier.com/books/mindfulness-based-treatment-approaches/baer/978-0-12-416031-6
Baer, R., Smith, G., & Allen, K. (2004). Assessment of mindfulness by self-report: The Kentucky Inventory of Mindfulness Skills. Assessment, 11, 191–206. https://doi.org/10.1177/1073191104268029
Benson, H., Beary, J. F., & Carol, M. P. (1974).The Relaxation Response. Psychiatry, 37(1), 37-46. https://www.tandfonline.com/loi/upsy20
Bowden, A., Lorenc, A., & Robinson, N. (2012). Autogenic Training as a behavioural approach to insomnia: A prospective cohort study. Primary Health Care Research & Development, 13, 175-185. https://doi.org/10.1017/S1463423611000181
Britton, W.B., Lindahl, J.R., Coope, D.J., Canby, N.K., & Palitsky, R. (2021). Defining and Measuring Meditation-Related Adverse Effects in Mindfulness-Based Programs. Clinical Psychological Science, 9(6), 1185-1204. https://doi.org/10.1177/2167702621996340
Budzynski, T., Stoyva, J., & Adler, C. (1970). Feedback-induced muscle relaxation: Application to tension headache. Journal of Behavior Therapy and Experimental Psychiatry, 1(3), 205-211. https://doi.org/10.1016/0005-7916(70)90004-2
Carlson, L. E., Speca, M., Patel, K. D., & Goodey, E. (2003). Mindfulness‐based stress reduction in relation to quality of life, mood, symptoms of stress, and immune parameters in breast and prostate cancer outpatients. Psychosomatic Medicine, 65(4), 571-581. https://doi.org/10.1097/01.psy.0000074003.35911.41
Chapin, H. L., Darnall, B. D., Seppala, E. M., Doty, J. R., Hah, J. M., & Mackey, S. C. (2014). Pilot study of a compassion meditation intervention in chronic pain. J Compassionate Health Care, 1(4), 1-12. https://doi.org/10.1186/s40639-014-0004-x
Cherkin, D. C., Sherman, K. J., Balderson, B. H., Cook, A. J., Anderson, M. L., Hawkes, R. J., … & Turner, J. A. (2016). Effect of mindfulness-based stress reduction vs cognitive behavioral therapy or usual care on back pain and functional limitations in adults with chronic low back pain: A randomized clinical trial. JAMA, 315(12), 1240-1249. https://doi.org/10.1001/jama.2016.2323
Crawford, C., Wallerstedt, D. B., Khorsan, R., Clausen, S. S., Jonas, W. B., & Walter, J. A. (2013). A systematic review of biopsychosocial training programs for the self-management of emotional stress: Potential applications for the military. Evidence-Based Complementary and Alternative Medicine, 747694: 1-23. https://doi.org/10.1155/2013/747694
Davis, M., Eshelman, E.R., & McKay, M. (2019). The Relaxation and Stress Reduction Workbook. Oakland, CA: New Harbinger Publications. https://www.amazon.com/Relaxation-Reduction-Workbook-Harbinger-Self-Help/dp/1684033349
Demarzo, M. M., Montero-Marin, J., Cuijpers, P., Zabaleta-del-Olmo, E., Mahtani, K. R., Vellinga, A., Vincens, C., Lopez del Hoyo, Y., & García-Campayo, J. (2015). The efficacy of mindfulness-based interventions in primary care: A meta-analytic review. The Annals of Family Medicine, 13(6), 573-582. https://doi.org/10.1370/afm.1863
Fjorback, L. O., Arendt, M., Ørnbøl, E., Fink, P., & Walach, H. (2011). Mindfulness‐Based Stress Reduction and Mindfulness‐Based Cognitive Therapy–A systematic review of randomized controlled trials. Acta Psychiatrica Scandinavica, 124(2), 102-119. https://doi.org/10.1111/j.1600-0447.2011.01704.x
Goto, F., Nakai, K., & Ogawa, K. (2011). Application of autogenic training in patients with Meniere disease. European Archives of Oto-Rhino-Laryngology, 268(10), 1431-1435. https://doi.org/10.1007/s00405-011-1530-1
Greeson, J., & Eisenlohr-Moul, T. (2014). Mindfulness-based stress reduction for chronic pain. In R. A. Baer (Ed.), Mindfulness-Based Treatment Approaches: Clinician’s Guide to Evidence Base and Applications, 269-292. San Diego, CA: Academic Press. https://psycnet.apa.org/record/2014-40932-000
Green, E. and Green, A. (1989). Beyond Biofeedback. New York: Knoll. https://www.amazon.com/Beyond-Biofeedback-Elmer-Green/dp/0940267144
Hawkins, M. A. (2003). Effectiveness of the Transcendental Meditation program in criminal rehabilitation and substance abuse recovery. Journal of Offender Rehabilitation, 36(1-4), 47- 65. https://doi.org/10.1300/J076v36n01_03
Hilton, L., Hempel, S., Ewing, B. A., Apaydin, E., Xenakis, L., Newberry, S., …Maglione, M. A. (2016). Mindfulness meditation for chronic pain: Systematic review and meta-analysis. Annals of Behavioral Medicine, 51(2), 199-213. https://doi.org/10.1007/s12160-016-9844-2
Hoffman, C. J., Ersser, S. J., Hopkinson, J. B., Nicholls, P. G., Harrington, J. E., & Thomas, P. W. (2012). Effectiveness of mindfulness-based stress reduction in mood, breast-and endocrine-related quality of life, and well-being in stage 0 to III breast cancer: A randomized, controlled trial. Journal of Clinical Oncology, 30(12), 1335-1342. https://doi.org/10.1200/JCO.2010.34.0331
Jacobson, E. (1938). Progressive relaxation. Chicago, IL: University of Chicago Press. https://www.amazon.com/Progressive-Relaxation-Physiological-Investigation-Significance/dp/0226390594
Kabat-Zinn, J. (1994). Wherever you go, there you are: Mindfulness meditation in everyday life. New York: Hyperion. https://www.amazon.com/Wherever-You-There-Are-Mindfulness/dp/0306832011
Kabat-Zinn, J. (2003). Mindfulness-based stress reduction (MBSR). Constructivism in the Human Sciences, 8, 73–107. https://psycnet.apa.org/record/2004-19791-008
Khazan, I. Z. (2013). The clinical handbook of biofeedback: A step-by-step guide for training and practice with mindfulness. New York: John Wiley & Sons. https://www.amazon.com/Clinical-Handbook-Biofeedback-Step-Step/dp/1119993717
Klein, A., & Peper, E. (2013). There Is hope: Autogenic biofeedback training for the treatment of psoriasis. Biofeedback, 41 (4), 194-201. https://doi.org/10.5298/1081-5937-41.4.01
Khoury, B., Lecomte, T., Fortin, G., Masse, M., Therien, P., Bouchard, V., Chapleau, M., Paquin, K., & Hofmann, S. G. (2013). Mindfulness-based therapy: A comprehensive meta-analysis. Clinical Psychology Review, 33(6), 763-771. https://doi.org/10.1016/j.cpr.2013.05.005
Khoury, B., Sharma, M., Rush, S. E., & Fournier, C. (2015). Mindfulness-based stress reduction for healthy individuals: A meta-analysis. Journal of Psychosomatic Research, 78(6), 519-528.
Klott, O. (2013). Autogenic Training–a self-help technique for children with emotional and behavioural problems. Therapeutic Communities: The International Journal of Therapeutic Communities, 34(4), 152-158. https://doi.org/10.1108/TC-09-2013-0027
Kreplin, U., Farias, M., & Brazil, I. A. (2018). The limited prosocial effects of meditation: A systematic review and meta-analysis. Sci Rep, 8, 2403. https://doi.org/10.1038/s41598-018-20299-z
Kuhlmann, S. M., Huss, M., Bürger, A., & Hammerle, F. (2016). Coping with stress in medical students: results of a randomized controlled trial using a mindfulness-based stress prevention training (MediMind) in Germany. BMC Medical Education, 16(1), 316. https://doi.org/10.1186/s12909-016-0833-8
Lindahl, J. R., Fisher, N. E., Cooper, D. J., Rosen, R. K, & Britton, W. B. (2017). The varieties of contemplative experience: A mixed-methods study of meditation-related challenges in Western Buddhists. PLoSONE, 12(5): e0176239. https://doi.org/10.1371/journal.pone.0176239
Luthe, W. (1970). Autogenic therapy: Research and theory. New York: Grune and Stratton. https://www.cambridge.org/core/journals/the-british-journal-of-psychiatry/article/abs/autogenic-therapy-edited-by-wolfgang-luthe-volume-4-research-and-theory-by-wolfgang-luthe-grune-and-stratton-new-york-1970-pp-276-price-1475/6C8521C36C37254A08AAD1F2FE08211C
Luthe, W. (1979). About the Methods of Autogenic Therapy. In: Peper, E., Ancoli, S., Quinn, M. (eds). Mind/Body Integration. Springer, Boston, MA. https://doi.org/10.1007/978-1-4613-2898-8_12
Luthe, W. & Schultz, J. H. (1970a). Autogenic therapy: Medical applications. New York: Grune and Stratton. https://www.amazon.com/Autogenic-Therapy-II-Medical-Applications/dp/B001J9W7L6
Luthe, W. & Schultz, J. H. (1970b). Autogenic therapy: Applications in psychotherapy. New York: Grune and Stratton. https://www.amazon.com/Autogenic-Therapy-Applications-Psychotherapy-v/dp/0808902725
Mackereth, P.A. & Tomlinson, L. (2010). Progressive muscle relaxation. In Cawthorn, A. & Mackereth, P.A. eds. Integrative Hypnotherapy. London: Churchill Livingstone. https://www.amazon.com/Integrative-Hypnotherapy-Complementary-approaches-clinical/dp/0702030821
Marchand, W. R. (2012). Mindfulness-based stress reduction, mindfulness-based cognitive therapy, and Zen meditation for depression, anxiety, pain, and psychological distress. Journal of Psychiatric Practice, 18(4), 233-252. https://doi.org/10.1097/01.pra.0000416014.53215.86
NCCIH (2024). Meditation and Mindfulness: What You Need To Know. National Center for Complementary and Integrative Health, National Institutes of Health. Accessed January 31, 2024. https://www.nccih.nih.gov/health/meditation-and-mindfulness-what-you-need-to-know?
Paul-Labrador, M., Polk, D., Dwyer, J.H. et al. (2006). Effects of a randomized controlled trial of Transcendental Meditation on components of the metabolic syndrome in subjects with coronary heart disease. Archive of Internal Medicine, 166(11), 1218-1224. https://doi.org/10.1001/archinte.166.11.1218
Peper, E., Ancoli, S. & Quinn, M. (Eds). (1979). Mind/Body Integration: Essential Readings in Biofeedback. New York: Plenum. https://www.amazon.com/Mind-Body-Integration-Essential-Biofeedback/dp/0306401029
Peper, E. & Shaffer, F. (2010). Biofeedback History: An Alternative View. Biofeedback, 38 (4): 142–147. https://doi.org/10.5298/1081-5937-38.4.03
Peper, E., & Williams, E.A. (1980). Autogenic therapy. In A. C. Hastings, J. Fadiman, & J. S. Gordon (Eds.), Health for the whole person (pp137-141).. Boulder: Westview Press. https://biofeedbackhealth.files.wordpress.com/2016/02/autogenic-therapy-peper-and-williams.pdf
Rainforth, M.V., Schneider, R.H., Nidich, S.I., Gaylord-King, C., Salerno, J.W., & Anderson, J.W. (2007). Stress reduction programs in patients with elevated blood pressure: A systematic review and meta-analysis. Current Hypertension Reports, 9(6), 520–528. https://doi.org/10.1007/s11906-007-0094-3
Stroebel, C. (1982). QR: The Quieting Reflex. New York: Putnam Pub Group. https://www.amazon.com/Qr-Quieting-Charles-M-D-Stroebel/dp/0399126570
Tanner, M. A., Travis, F., Gaylord‐King, C., Haaga, D. A. F., Grosswald, S., & Schneider, R. H. (2009). The effects of the transcendental meditation program on mindfulness. Journal of Clinical Psychology 65(6), 574-589. https://doi.org/10.1002/jclp.20544
Teasdale, J. D., Segal, Z., & Williams, J. M. (1995). How does cognitive therapy prevent depressive relapse and why should attentional control (mindfulness) training help? Behaviour Research and Therapy, 33, 25–39. https://doi.org/10.1016/0005-7967(94)e0011-7
Travis, F. (2001). Autonomic and EEG patterns distinguish transcending from other experiences during transcendental meditation practice. International Journal of Psychophysiology, 42, 1–9. https://doi.org/10.1016/s0167-8760(01)00143-x
Travis, F. (2014). Transcendental experiences during meditation practice. Annals of the New York Academy of Sciences, 1307, 1–8. https://doi.og10.1111/nyas.12316
Wallace, K.W. (1970). Physiological Effects of Transcendental Meditation. Science, 167 (3926), 1751-1754. https://doi.org/10.1126/science.167.3926.1751
Whatmore, G. B., & Kohli, D. R. (1968). Dysponesis: A neurophysiologic factor in functional disorders. Behavioral Science, 13(2), 102–124. https://doi.org/10.1002/bs.3830130203
Wilson, V., Somers, K. & Peper, E. (2023). Differentiating Successful from Less Successful Males and Females in a Group Relaxation/Biofeedback Stress Management Program. Biofeedback, 51(3), 53–67. https://doi.org/10.5298/608570
Witek Janusek, L., Tel,l D., & Mathews, H.L. (2019). Mindfulness based stress reduction provides psychological benefit and restores immune function of women newly diagnosed with breast cancer: A randomized trial with active control. Brain Behav Immun, 80:358-373. https://doi.org/10.1016/j.bbi.2019.04.012
Breathing to improve well-being
Posted: November 17, 2017 Filed under: Breathing/respiration, Exercise/movement, Neck and shoulder discomfort, Pain/discomfort, self-healing, stress management, Uncategorized | Tags: anxiety, Breathing, health, mindfulness, pain, respiration, stress 9 CommentsBreathing affects all aspects of your life. This invited keynote, Breathing and posture: Mind-body interventions to improve health, reduce pain and discomfort, was presented at the Caribbean Active Aging Congress, October 14, Oranjestad, Aruba. www.caacaruba.com
The presentation includes numerous practices that can be rapidly adapted into daily life to improve health and well-being.
Mind-Guided Body Scans for Awareness and Healing Youtube Interview of Erik Peper, PhD by Larry Berkelhammer, PhD
Posted: February 19, 2016 Filed under: Uncategorized | Tags: autogenic training, body scan, mind-body, mindfulness, pain, passive attention, stress management Leave a commentIn this interview psychophysiology expert Dr. Erik Peper explains the ways how a body scan can facilitate awareness and healing. The discussion describes how the mind-guided body scan can be used to improve immune function and maintain passive attention (mindfulness), and become centered. It explores the process of passive attentive process that is part of Autogenic Training and self-healing mental imagery. Mind-guided body scanning involves effortlessly observing and attending to body sensations through which we can observe our own physiological processes. Body scanning can be combined with imagery to be in a nonjudgmental state that supports self-healing and improves physiological functioning.
Letting go of stress and worry*
Posted: January 15, 2016 Filed under: Uncategorized | Tags: mindfulness, stress management, visualization, worry 7 Comments One evening an old Cherokee told his grandson about a battle that goes on inside people. He said, “My son, the battle is between two wolves inside us all.”
One evening an old Cherokee told his grandson about a battle that goes on inside people. He said, “My son, the battle is between two wolves inside us all.”
“One is Evil – It is anger, envy, jealousy, sorrow, regret, greed, arrogance, self-pity, guilt, resentment, inferiority, lies, false pride, superiority, and ego.”
“The other is Good – It is joy, peace, love, hope, serenity, humility, kindness, benevolence, empathy, generosity, truth, compassion and faith.”
The grandson thought about it for a minute and then asked his grandfather: “Which wolf wins?”
The old Cherokee simply replied, “The one you feed.”
–Author and source unknown
Are you stressed and worrying what will happen? Are you thinking of all that could go wrong? Do you feel overwhelmed and anxious?
It is very challenging to let go of negative thoughts, images, memories and anticipations. These negative worries can be useful if they mobilize you towards active planning and action; however, in most cases, the thoughts continue to go around and around in our heads. The more we worry, the worse we feel. Often our shoulders and neck tighten and our stomach churns. The worries and concerns may become a pain in the neck and we no longer can stomach the stress.
Begin to take charge and realize that even though health and healing is not our control, we can contribute and support the healing process. Regardless how overwhelmed we are, begin with the basics. Start the day by respecting your body so that it can run well. It needs:
Proper fuel. Begin by having breakfast—not the sugar coated cereals or snack bars on the run—but an egg, oatmeal, and some fruit or other non-processed foods. Even when you think you do not have the time, fuel up your body so your body engine can work well. Drink only one cup of coffee with little sugar. Drink water or tea and avoid all soft drinks and any low calorie drinks. Remember that people who drink low calorie soft drinks increase their abdominal girth by three inches as compared to people who do not drink low calorie soft drinks (Fowler et al, 2015).
Follow-up with lunch and dinner, do not skip meals! Many of my college students do not eat breakfast or lunch before coming to class, as a group they are more reactive, anxious and perform significantly poorer on exams than the ones who do eat.
If you haven’t eaten, or eaten only high sugary snack foods an hour or two before, your blood sugar will lower and you become more reactive “Hangry” (the combination of hungry and angry). As the blood sugar drops, the brain reactivity pattern changes and you become much more impulsive (Peper et al, 2009).
Dynamic movement. The moment you do some movement your urge to snack, smoke, or ruminate is significantly reduced. When you begin physical movement (especially when you do not want to), the built up tension from the personal and interpersonal stress will decrease. You are completing the biological alarm reaction. When you physically move, you dissipate the fight/flight response and are shifting your body to a state of regeneration. As the alarm reaction response decreases, it becomes easier to do problem solving and abstract thinking. As long as you are in the alarm state, you tend to react defensively to the immediate events. Thus, when you feel uptight and stressed, take a hike. Walk up the stairs instead of taking the escalator, get off Muni one stop earlier and walk rapidly to your destination.
Positive and peaceful thoughts. Remember your thoughts, memories and images affect your body and vice versa. Experience how your thoughts effect your body. Have someone read the following to you. It takes only a few minutes.
Sit comfortably, and gently close your eyes and imagine a lemon. Notice the deep yellow color, and the two stubby ends. Imagine placing the lemon on a cutting board and cutting it in half with your favorite kitchen knife. Notice the pressure of the knife in your hand as you cut the lemon. Feel the drop of lemon juice against your skin. After cutting the lemon in half, put the knife down and pick up one half of the lemon.

As you look at it, notice the drops of juice glistening in the light, the half-cut seeds, the outer yellow rind, and the pale inner rind. Now get a glass and squeeze this half of lemon so the juice goes into the glass. As you squeeze, notice the pressure in your fingers and forearm. Feel droplets of lemon juice squirting against your skin. Smell the pungent, sharp fragrance. Now take the other half of lemon and squeeze the juice into the glass. Now take the glass in your hand. Feel the coolness of the glass and bring it to your lips. Feel the juice against your lips, and then sip the lemon juice. Taste the tart juice and swallow the lemon juice. Observe the pulp and seeds as you swallow (Adapted from Gorter and Peper, 2011).
What did you notice? As you imagined the lemon, did you notice that you experienced an increase in salivation, or that your mouth puckered? Almost everyone who does this exercise experiences some of these physical changes. The increase in salivation demonstrates that these thoughts and images have a direct effect on our bodies. Similarly, when we have thoughts of anger, resentment, frustration, or anxiety, they also affect our bodies. Unknowingly we may tighten our shoulders or our abdomen. We may unconsciously hold our breath or breathe shallowly. This response interferes with our ability to relax and heal. If this kind of tension is a constant habit, it reduces the body’s ability to regenerate.
Although we may dismiss our experience when we did the imagery exercise with an imaginary lemon—it was only an imaginary lemon, after all—it is fundamentally important. Every minute, every hour, every day, our bodies are subtly affected by thoughts, emotions, and images. Just as the image of the lemon caused us to salivate, our thoughts and emotions also cause physiological change.
What to do when consumed by worry. Although it seems impossible, you have a choice to focus on the negative or positive thoughts. When you feel stressed and overwhelmed, ask yourself, do I have control over this situation?
If “No”, acknowledge that you feel frustrated and stuck. Recognize you want to let it go and have no control. Ask yourself “does this thought serve any purpose or help me in any way” If not, let go of the thought and the sensations in your body” If there is a purpose or value act upon the thought (go feed the parking meter, make that call). Then do the following thought interrupting practice.
Sit up and make yourself tall on your sitz bones with your lower spine slightly arched at the same time look up and take a breath in. While inhaling, think of someone who loves you such as your grandmother an aunt. For that moment feel their love. Exhale softly while slightly smiling while still looking upward. As you exhale think of someone for whom you care for and wish them well.
Each time your brain begins to rehash that specific event, do not argue with it, do not continue with it, instead, initiate the thought interrupting practice. Many people report when they do this many, many, times a day, their energy, mood and productivity significantly increases. Initially it seems impossible, yet, the more you practice, the more the benefits occur.
If “yes,” make a list of all the things over which you have control and that need to be done. Acknowledge that this list appears overwhelming and you do not even know where to start. Begin by doing one small project. Remember, you do not have to finish it today. It is a start. And, if possible, share your list and challenge with friends or family members and ask them for support. The most important part is to move into action. Then, each time your brain worries, “I do not have enough time”, or “there is too much to do,” practice the thought interrupting practice.
Watch your thoughts; they become words.
Watch your words; they become actions.
Watch your actions; they become habits.
Watch your habits; they become character.
Watch your character; it becomes you
– Frank Outlaw (1977)
Reference:
Fowler, S. P., Williams, K., & Hazuda, H. P. (2015). Diet Soda Intake Is Associated with Long‐Term Increases in Waist Circumference in a Biethnic Cohort of Older Adults: The San Antonio Longitudinal Study of Aging. Journal of the American Geriatrics Society, 63(4), 708-715. http://onlinelibrary.wiley.com/doi/10.1111/jgs.13376/pdf
Peper, E., Harvey, R., Takabayashi, N., & Hughes, P. (2009). How to do clinical biofeedback in psychosomatic medicine: An illustrative brief therapy example for self-regulation. Japanese Journal of Biofeedback Research..36 (2), 1-16. https://biofeedbackhealth.files.wordpress.com/2011/01/howdoyouclinicalbiofeedback19.pdf
Gorter, R. & Peper, E. (2011). Fighting Cancer-A Non Toxic Approach to Treatment. Berkeley: North Atlantic: Random House. http://www.amazon.com/Fighting-Cancer-Nontoxic-Approach-Treatment-ebook/dp/B004C43GAQ/ref=sr_1_1?s=books&ie=UTF8&qid=1452923651&sr=1-1&keywords=fighting+cancer
Outlaw, F (1977). What They’re Saying Quote Page 7-B, San Antonio Light (NArch Page 28), Column 4, 1San Antonio, Texas, May 18, 1977 (NewspaperArchive).
*Adapted from: Peper, E. (2016). Legend of two wolves is a beacon across time for healthy thinking. Western Edition. January, pp 6, 8. http://thewesternedition.com/admin/files/magazines/WE-January-2016.pdf

{kind=link}
{kind=link}
{kind=link}