Hope for abdominal discomfort
Posted: June 21, 2022 Filed under: behavior, biofeedback, Breathing/respiration, emotions, Evolutionary perspective, healing, health, Pain/discomfort | Tags: functional abdominal pain, heart rate variability, HRV, IBS, irritable bowel syndrome, neurasthenia, Rap, recurrent abdominal pain, respiration 3 CommentsAdapted from: Peper, E. & Harvey, R. (2022). Nausea and GI discomfort: A biofeedback assessment model to create a rational for training. Biofeedback, 50(1), 24–32. https://doi.org/10.5298/1081-5937-50.1.05
Abdominal discomfort and pain such as functional abdominal pain, acid reflux or irritable bowel affects many people. Teaching slower biofeedback-assisted HRV breathing with biofeedback is a useful strategy by which the person may be able to reduce symptoms. This essay provides detailed instruction for a first session assessment for clients who have abdominal discomfort (functional abdominal pain). Descriptions include how the physiological recording can be used to understand a possible etiology of the illness, to create a biological/evolutionary based explanation that is readily understood by the client, and finally to offer self-regulation suggestions to improve health.
Background of abdominal discomfort (irritable bowel syndrome, acid reflux, functional abdominal pain, recurrent abdominal pain)
Irritable bowel syndrome (IBS) affects 7% to 21% of the general population in Western cultures with a global prevalence estimated at around 11% (Fairbrass, Costantino, Gracie, & Ford, 2020). The chronic symptoms (i.e., lasting more than 30 days) usually include abdominal cramping, discomfort or pain, bloating, loose or frequent stools and constipation, which can significantly reduce the quality of life (Chey et al., 2015). A precursor of IBS in children is called recurrent abdominal pain (RAP), which affects 0.3% to 19% of school children (Chitkara et al., 2005). Both IBS and RAP appear to be functional illnesses, as no organic causes have been identified to explain the symptoms. IBS and RAP are contrasted to various types of diseases such as Crohn’s disease, inflammatory bowel disease or ulcerative colitis.
Multiple factors may contribute to IBS, such as genetics, food allergies, previous treatment with antibiotics, infections, psychological status and stress. More recently, dietary factors contributing to changes in the intestinal and colonic microbiome resulting in small intestine bacterial overgrowth have been suggested as another risk factor (Dupont, 2014). Generally, standard medical treatments (reassurance, dietary manipulation and of pharmacological therapy) are often ineffective in reducing IBS symptoms (Chey et al., 2015). On the other hand, complementary and alternative approaches such as biofeedback-assisted relaxation techniques (Davidoff & Whitehead, 1996; Goldenberg et al., 2019; Stern et al. 2014), autogenic training (Luthe & Schultz, 1969) and cognitive therapy are more effective than traditional medical treatment (Vlieger et al., 2008).
Biofeedback-assisted relaxation training typically moderates IBS or RAP symptoms by restoring balance in the nervous system (sympathetic/parasympathetic autonomic balance), such as through heart rate variability (HRV) breathing training. For example, Sowder et al. (2010) as well as Sun et al. (2016) demonstrated that functional abdominal pain can be reduced with HRV feedback training. In most cases, increased vagal tone was achieved by breathing at about six breaths per minute. While Taneja et al. (2004) reported that yogic breathing decreased diarrhea-predominant irritable bowel syndrome symptoms significantly more than conventional treatment in a randomized control study.Sympathetic/parasympathetic balance can be enhanced by increasing HRV, which occurs when a person breathes at their resonant frequency, which is usually 5–7 breaths per minute. For most people, the HRV training means breathing at much slower rate. A benefit of slow abdominal breathing appears to be a self-control strategy that can reduce symptoms of IBS, RAP and similar functional abdominal pain symptoms.
Mastery of effortless diaphragmatic breathing can be affected by injury, surgery or similar insults to the abdominal area (Peper et al., 2015). In addition, dysregulation of diaphragm, which is enervated by the phrenic nerve and the vagus nerve, along with dysregulation of other abdominal muscles appears to be associated with irritable bowel syndrome (Bordoni & Morabito, 2018). It is likely that slower biofeedback-assisted HRV breathing training restores abdominal muscles and diaphragmatic movement, theoretically by tonic and phasic regulation of the phrenic and vagal nerve activity (cf. Marchenko et al., 2015; Streeter et al., 2012). The theory, simply stated, is that HRV breathing training at an individual’s resonant frequency produces increases in regulatory neurotransmitters, particularly gamma amino butyric acid (GABA). Many of our students who complain of abdominal discomfort report reductions of symptoms following HRV breathing training.
Consistently for more than 40 years, we have taught undergraduate students a semester-long integrated stress management program that includes modified progressive relaxation, slow diaphragmatic breathing and changing internal language as outlined in the book, Make Health Happen, by Peper, Gibney & Holt (2002). At the end of each semester, numerous students report that their anxiety, gastrointestinal distress and other symptoms related to self-described IBS or RAP have decreased or disappeared (Peper et al., 2014; Peper, Miceli, & Harvey, 2016; Peper, Mason, Huey, 2017; Peper et al., 2020). Abdominal discomfort is prevalent experience of distress by college students. In our recent survey of 99 undergraduate students, 41% self-reported abdominal discomfort (25% irritable bowel or acid reflux), 86% self-reported anxiety, 70% neck and shoulder tension and 48% headaches. After practicing slower breathing (i.e., typically directing them to breath abdominally at a rate of about six breaths a minute) and focus on slower exhalation and allowing the air to flow in without effort as the abdominal wall expands, as a homework assignment for a week, many reported that their symptoms significantly decreased (Peper, Harvey, Cuellar, & Membrila, in press).
Case example illustrating how to use the physiological recording to guide the client discussion and provide motivation
A 16-year-old high school junior suffered from abdomen discomfort for years. The symptoms mainly consisted of frequent constipation, and when it occurred, great discomfort from nausea. After having been diagnosed and undergoing all the necessary tests by the gastroenterologist, there was no identifiable cause of the chief complaints. Biofeedback was suggested as an alternative to medications for symptom reduction. During the biofeedback assessment and training session, the client discussed what she would like to learn from the session. It was challenging for her to respond to those questions. Not being able to report what the client would like from a training session is also a very common experience when working with students. A useful strategy is to describe experiences of other students that the clients could relate to, and imply that their abdominal discomfort is somewhat commonplace in other students.
Discussed during the session was the link between being very sensitive and reactive to other people’s feeling and being concerned about what others think of her. The client nodded her head in agreement. When describing herself, she discussed being very perfectionistic using a scale from being lackadaisical/undemanding to being perfectionistic (i.e., self-oriented perfectionism, self-worth contingencies, concern over mistakes, doubts about actions, self-criticism, socially prescribed perfectionism, other-oriented perfectionism, hypercriticism; see Smith, Saklofske, Stoeber, & Sherry, 2016).
Furthermore, the client sat slouched in the chair. Possibly her slouched posture implied a state of powerlessness instead of empowerment, a state of being ready to react and protect (Carney, Cuddy, & Yap, 2010; Cuddy, 2012; Peper, Lin, & Harvey, 2017).
Working hypotheses. The client was very sensitive and continuously reacted to external and internal signals with sympathetic arousal, while masking her reactions. These ongoing flight/flight responses would decrease intestinal peristalsis and abdominal blood flow, which would result in nausea, constipation and abdominal distress. Namely, the body reacts to the stimuli as signals of danger and blood flow is shunted away from the abdomen into the large muscles to run and fight. To paraphrase Stanford University professor Robert Sapolsky (2004): Why should the body digest food and repair itself, if it is going to be the predator’s lunch? It is only when we are safe that we can digest and regenerate.
The session began by exploring how pressure on the abdomen could potentially affect experiences of nausea and abdominal distress. After explaining how the diaphragm descends and how abdominal content in the stomach can be displaced (spread out) during inhalation, we systematically changed her posture by placing and adjusting a small pillow behind her middle back so that she could sit tall. The tall posture resulted in an open feeling of empowerment not felt during slouching. She observed that breathing was slightly easier and felt there was more space in her abdomen. As she began to feel more comfortable during the training session, we discussed the impact of posture on the body. We also discussed the relationship between thoughts of perfectionism and abdominal discomfort. The discussion also included an exploration of why some people tend to curl-up and slouch in a protective posture (e.g., head down to protect the neck region and big bones of the arms and legs positioned to protect the core organs) when feeling self-consciousness or perfectionistic about body image.
Biofeedback monitoring for assessment
Psychophysiology was recorded with multichannel physiological system (Procomp Infinity System running Biograph Infinity software version 6.7.1, Thought Technology Ltd). Respiration was monitored with strain-gauge sensors placed around the abdomen and thoracic regions (for a discussion on sensor placement see Peper et al., 2016 and Chu et al., 2019). Blood volume pulse was recorded with the sensor placed on the left thumb. The thumb was used because the participant had small and cold fingers (for a discussion about blood volume pulse, see Peper et al, 2007 and Peper, Shafer, & Lin, 2010). Skin conductance was recorded with the sensor wrapped around the left index and middle fingers with the electrodes on the finger pads (for a discussion about skin conductance and normal values, see Khazan, 2019, and Shafer et al, 2016).
After sensors were attached and the signals explained, the client sat comfortably while looking at the screen. Unexpectedly the clinician clapped his hands and made a loud noise. The client reacted with a momentary startle and smile. The physiological response, showed an increase in skin conductance, decrease in pulse amplitude, decrease in abdominal diameter, and increase in heart rate, is shown in Figure 1.

Figure 1. Physiological response to a loud noise (clap) (1) increased skin conductance, (2) decrease in pulse amplitude, (3) decrease in decreased abdominal circumference, and (4) increased heart rate and decreased heart rate variability.
The client was aware that she reacted to the clap; however, she was totally unaware how much her body responded. The computer screen display of her physiological reaction made the invisible visible. It provided the opportunity to discuss how various body reactions related to heart rate, breathing, and skin conductance could contribute to experiences of abdominal discomfort.
She was unaware that skin conductance did not return to baseline levels for more than 20 minutes. An elevated skin conductance level may mean that the body’s reaction to the hand-clap noise triggered a defense reaction and maintained the increased sympathetic activity for more than 20 minutes. Having a sustained flight/fight reaction to external stimuli such as a hand-clap would most likely affect digestive and peristalsis processes, contributing to symptoms found in IBS and RAP. The observations made during biofeedback monitoring led to a discussion of how sympathetic activation affects the gastrointestinal track.
Blood volume pulse amplitude decreased, which indicated a decrease in blood flow through her hands, which would decrease hand temperature and again indicated a systemic sympathetic activation.
Abdominal circumference decreased, which indicated that she tightened her abdominal muscles as a protective response to the hand-clap. She was unaware of the abdominal muscles tightening; however, she stated that she was aware that her breathing had changed. The abdominal muscle, which pulled the abdomen in, took almost two minutes to relax. The sustained muscle constriction around the abdomen increased pressure around the core organs, which may contribute to ongoing abdominal discomfort. A fight-flight reaction includes body bracing (e.g. tightened muscles, head down to protect the neck, big bones of arms and legs curled to protect core organs), and she confirmed that she experienced neck and shoulder tensions.
The discussion of abdominal muscle tension led to another discussion of how holding your stomach in may relate to self-image. For example, tight clothing can contribute to constricted movement around the abdomen. Wearing corsets contributed to psychophysiological symptoms, mainly for women in the late 19th and early 20th centuries, during a time when women who wore very tight corsets were diagnosed with neurasthenia. Simply stated, neurasthenia was characterized as a condition of mental and/or physical fatigue with at least two of the following symptoms: dyspepsia, dizziness, muscular aches or pains, tension headaches, inability to relax, irritability and sleep disturbance.
“Dyspepsia” was the commonly reported symptom of neurasthenia, which included upset stomach, a gnawing or burning stomach pain, heartburn, bloating, and or burping, nausea, and vomiting. The constricted waist region that resulted from wearing a corset in the name of fashion compromises the functions of both digestion and breathing. When the person inhales, the abdomen cannot expand as the diaphragm is flattening and pushing downward. Thus, the person is forced to breathe more shallowly by lifting their ribs; this increases neck and shoulder tension as well as the risk of anxiety, heart palpitation, and fatigue (Cohen & White, 1947; Courtney, 2009).
It also can contribute to abdominal discomfort since the abdomen is being squeezed by the corset and forcing the abdominal organs upward. Even architects of the Victorian era recognized a need for a place to position a chair or chaise lounge, such as at the top of some stairs, because people wearing corsets could faint, pass out or otherwise experience breathlessness through the effort of climbing the stairs with restrictive clothing around their abdomen (Melissa, 2015). Many of these symptoms could be easily reduced by wearing looser clothing and learning slower diaphragmatic breathing. In modern times, a related phenomenon results when people wear items of clothing that are too tight around their waist or abdomen (e.g., tight jeans) in service to fashion trends often labeled as designer jean syndrome (MacHose & Peper, 1991; Stonehewer, 2009). Similarly, when people wear garments that are too tight around their chest or thoracic region (e.g., tight vests) in service to external protection (e.g., athletes, industrial workers, police or soldiers wearing heavy, restrictive gear), then restrictive ventilatory disorders can occur (Harty et al., 1999). Simply stated, when the muscles related to breathing are restricted from moving, respiration is affected.
The client’s heart rate increased and stayed high for more than 30 seconds. The first decrease in heart rate at about 20 seconds after the hand-clap was a long sigh of relief as breathing (i.e., oxygen/carbon dioxide exchange) started again. It took almost 90 seconds before breathing and heart rate returned to normal as reflected by measures of HRV. The computer screen showing increased heart rate was reviewed with the client to explain how her body reacted with a fight-flight response to the hand-clap, as well as how regulating breathing through biofeedback training could lower the heart rate and reduce the sympathetic activation and enhance the parasympathetic activation.
Body responds to cognitive stressful thoughts
After discussion about the psychophysiological response to the hand-clap (a physical external stressor) and how other external stressors (e.g., startling noise) or internal stressors (e.g., perfectionistic ruminations) could trigger a similar response of abdominal muscle tightening, the assessment was repeated by having her relax and then think about a mental stressor, as shown in Figure 2.

Figure 2. Physiological responses to thinking about a past stressor (1) increased skin conductance, (2) decreased pulse amplitude, (3) decreased abdominal circumference, and (4) increased heart rate and decreased HRV.
The physiological response pattern to thinking about a past stressor was similar to the bodily reaction to a loud noise. The skin conductance increased and blood volume pulse amplitude decreased immediately after hearing (e.g., anticipating) the task of evoking/thinking of a past stressor. Most likely, the initial response was triggered by performance anxiety, then 6 seconds later the heart rate increased and breathing changed as she began experiencing the somatic reaction evoked by the recall of a negative stressor. The recordings also showed that her pulse amplitude decreased. The decrease in pulse amplitude suggested that her hands would probably become colder, which was confirmed by her self-report that she often experienced cold hands and feet. She reported being aware of the feeling an emotional reaction, but mainly noticing the change of breathing in her chest, and she was unaware of the abdominal changes. The client was surprised by how her body reacted to emotional thoughts. The recording viewed on the computer screen demonstrated objectively that her thoughts (initial performance anxiety) had a physical effect on her body. Specifically, experiencing the emotions that were evoked by recalling the stressful memory had a direct effect on the body in the same way that a physical external threat leads to a fight-flight response.
Building a psychophysiological model
Using these recorded computer images reflecting physical reactions to the hand clap and emotional thoughts, the discussion focused on how abdominal discomfort could be the result of activating a normal biological survival response. Survival responses would occur hundreds of times throughout a day, especially when worrying. Each thought would evoke the response, and the awareness of body reaction would evoke another reaction. Similar to how awareness of blushing amplifies blushing.
The client shared that she was very sensitive and reactive especially when other people were upset. She reported feeling “cursed” by their sensitivity and reactivity. The linguistic metaphor that could be used to describe her reactions is “she could not stomach what was going on.”
The discussion about physiological reactions provided the client with a model how her disorder (IBS and RAP) could have developed and been maintained over the years. The model matched her subjective experience: when stressed, the discomfort often increased. The discussion shifted to reframing her internal labels. Instead of describing her sensitivity as a curse, the sensitivity was reframed and labeled a gift; namely, she could sense many people’s emotional reactions, to which they would react in a variety of ways. She just needed to learn how to manage this sensitivity. Once she learned to manage it, she would have many advantages in interpersonal relations at home and at work. She would be able to sense what other people are experiencing. By reframing her symptoms as a result of a survival physiological response pattern, it reduces self- blame and offers solutions about how to master and change reactions and thereby have more control in the world.
Training to demonstrate control is possible.
The discussion was followed by teaching her diaphragmatic breathing in sitting and lying down positions. As she had no history of abdominal injuries, similar to many of our students, she rapidly demonstrated slower diaphragmatic breathing as shown in Figures 3 and 4.

Figure 3. The client practiced a few slower diaphragmatic breaths in the sitting and reclining position, which increased heart rate variability, decreased skin conductance and increased blood volume pulse amplitude.

Figure 4. Practicing slower diaphragmatic breathing at about six breaths per minute in a reclining position increased HRV.
With tactile coaching, she demonstrated that she could breathe at about six breaths per minute with the heart rate increasing during inhalation and decreasing during exhalation. She reported feeling more relaxed and that the sensations of nausea had disappeared. Additionally, her hands felt warmer. This recording provided proof that there was hope and that she could do something about her body’s psychophysiological responses.
The discussion focused on how breathing affecting heart rate variability. Namely, if she allowed exhalation to occur without effort, her heart rate decreased (the vagal response of slowing the heart) and thereby increased the parasympathetic activation that would support digestion and gastrointestinal functioning. Often when people practice effortless diaphragmatic breathing, abdominal noises (borborygmus)– the gurgling, rumbling, or squeaking noise from the abdomen–occur and indicate that intestinal activity is being activated, and that food, liquids and digestive juice are moving through the intestines. It is usually a positive indicator that the person is relaxing and sympathetic activity has been reduced.
During the last part of session, we reviewed how posture affects physiology, emotions and cognitions, as well as how posture and breathing would be the first step in beginning to reduce symptoms and enhance health. To provide additional information using video and bibliotherapy/education, we suggested that she watches the embedded videos in the blogs listed at the end of the article.
Recommendations for future sessions and home practice
The recommended strategies for future sessions would focus on teaching the client to master slow diaphragmatic breathing and practicing that for 10–20 minutes per day. The teaching techniques would incorporate imagery to imagine air flowing down their arms and legs as she exhaled. . More importantly, the focus would shift to generalize the skill during the day; namely, whenever she would become aware of feeling stressed or observed herself holding her breath or breathing in her chest, she would use that as the cue to shift to slower abdominal breathing. Had the client continued training, future sessions would focus on mastering slower diaphragmatic breathing. The training would include relaxing the lower abdominal muscles during inhalation, increasing control of HRV, practicing imagining stress and use image to trigger slower breathing, and cognitive reframing practices to interrupt worrying and promote self-acceptance. The final goal is to generalize these skills into daily life as illustrated in the successful cases described in the following blogs
Blogs on posture:
References
Bordoni, B. & Morabito, B. (2018). Symptomatology correlations between the diaphragm and irritable bowel syndrome. Cureus, 10(7), e3036. https://doi.org/10.7759/cureus.3036
Carney, D. R., Cuddy, A. J., & Yap, A. J. (2010). Power posing: brief nonverbal displays affect neuroendocrine levels and risk tolerance. Psychological Science, 10, 1363-1368. https://dx.doi.org/10.1177/0956797610383437
Chey, W. D., Kurlander, J., & Eswaran, S. (2015). Irritable bowel syndrome: a clinical review. Jama, 313(9), 949–958. https://doi.org/10.1001/jama.2015.0954
Chitkara, D. K., Rawat, D. J., & Talley, N. J. (2005). The epidemiology of childhood recurrent abdominal pain in Western countries: a systematic review. American journal of Gastroenterology, 100(8), 1868–1875. https://doi.org/10.1111/j.1572-0241.2005.41893.x
Chu, M., Nguyen, T., Pandey, V., Zhou, Y., Pham, H. N., Bar-Yoseph, R., Radom-Aizik, S., Jain, R., Cooper, D. M., & Khine, M. (2019). Respiration rate and volume measurements using wearable strain sensors. NPJ digital medicine, 2(1), 1–9. https://doi.org/10.1038/s41746-019-0083-3
Cohen, M. E. & White, P. D. (1947). Studies of breathing, pulmonary ventilation and subjective awareness of shortness of breath (dyspnea) in neurocirculatory asthenia, effort syndrome, anxiety neurosis. Journal of Clinical Investigation, 26(3), 520–529. https://doi.org/10.1172/JCI101836
Courtney, R. (2009). The functions of breathing and its dysfunctions and their relationship to breathing therapy. International Journal of Osteopathic Medicine, 12, 78–85. https://doi.org/10.1016/j.ijosm.2009.04.002
Cuddy, A. (2012). Your body language shapes who you are. Technology, Entertainment, and Design (TED) Talk, available at: http://www.ted.com/talks/amy_cuddy_your_body_language_shapes_who_you_are
Davidoff, A. L., & Whitehead, W. E. (1996). Biofeedback, relaxation training, and cognitive behavior modification: Treatments for functional GI disorders, In Olden, K, W. (ed). Handbook of Functional Gastrointestinal Disorders. CRC Press, 361–384.
Dupont, H. L. (2014). Review article: evidence for the role of gut microbiota in irritable bowel syndrome and its potential influence on therapeutic targets. Alimentary Pharmacology & Therapeutics, 39(10), 1033–1042. https://doi.org/10.1111/apt.12728
Fairbrass, K. M., Costantino, S. J., Gracie, D. J., & Ford, A. C. (2020). Prevalence of irritable bowel syndrome-type symptoms in patients with inflammatory bowel disease in remission: a systematic review and meta-analysis. The Lancet Gastroenterology & Hepatology, 5(12), 1053–162. https://doi.org/10.1016/s2468-1253(20)30300-9
Goldenberg, J. Z., Brignall, M., Hamilton, M., Beardsley, J., Batson, R. D., Hawrelak, J., Lichtenstein, B., & Johnston, B. C. (2019). Biofeedback for treatment of irritable bowel syndrome. Cochrane Database of Systematic Reviews, (11). https://doi.org/10.1002/14651858.CD012530.pub2
Harty, H. R., Corfield, D. R., Schwartzstein, R. M., & Adams, L. (1999). External thoracic restriction, respiratory sensation, and ventilation during exercise in men. Journal of Applied Physiology, 86(4), 1142–1150. https://doi.org/10.1152/jappl.1999.86.4.1142
Khazan, I. (2019). A guide to normal values for biofeedback. Biofeedback, 47(1), 2–5. https://doi.org/10.5298/1081-5937-47.1.03
Luthe, W. & Schultz, J. H. (1969). Autogenic Therapy Volume II: Medical Applications. Grune & Stratton.
MacHose, M., & Peper, E. (1991). The effect of clothing on inhalation volume. Biofeedback and Self-Regulation, 16(3), 261–265. https://doi.org/10.1007/BF01000020
Marchenko, V., Ghali, M. G., & Rogers, R. F. (2015). The role of spinal GABAergic circuits in the control of phrenic nerve motor output. American Journal of Physiology-Regulatory, Integrative and Comparative Physiology, 308(11), R916–R926. https://doi.org/10.1152/ajpregu.00244.2014
Melissa. (2015). Why women fainted so much in the 19th century. May 20, 2015. Downloaded October 2, 2021. http://www.todayifoundout.com/index.php/2015/05/women-fainted-much-19th-century/
Peper, E., Gibney, K. H., & Holt, C. F. (2002). Make Health Happen—Training Yourself to Create Wellness. Kendall/Hunt Publishing Company.
Peper, E., Gilbert, C. D., Harvey, R. & Lin, I-M. (2015). Did you ask about abdominal surgery or injury? A learned disuse risk factor for breathing dysfunction. Biofeedback. 34(4), 173–179. https://doi.org/10.5298/1081-5937-43.4.06
Peper, E., Groshans, G. H., Johnston, J., Harvey, R., & Shaffer, F. (2016). Calibrating respiratory strain gauges: What the numbers mean for monitoring respiration. Biofeedback, 44(2), 101–105. https://doi.org/10.5298/1081-5937-44.2.06
Peper, E., Harvey, R., Cuellar, Y., & Membrila, C.(in press). Reduce anxiety. NeuroRegulation.
Peper, E., Harvey, R., Lin, I. M., Tylova, H., & Moss, D. (2007). Is there more to blood volume pulse than heart rate variability, respiratory sinus arrhythmia, and cardiorespiratory synchrony? Biofeedback, 35(2), 54–61. https://www.researchgate.net/publication/259560204_Is_There_More_to_Blood_Volume_Pulse_Than_Heart_Rate_Variability_Respiratory_Sinus_Arrhythmia_and_Cardiorespiratory_Synchrony
Peper, E., Lin, I-M, & Harvey, R. (2017). Posture and mood: Implications and applications to therapy. Biofeedback, 35(2), 42–48. https://doi.org/10.5298/1081-5937-45.2.03
Peper, E., Lin, I-M, Harvey, R., Gilbert, M., Gubbala, P., Ratkovich, A., & Fletcher, F. (2014). Transforming chained behaviors: Case studies of overcoming smoking, eczema and hair pulling (trichotillomania). Biofeedback, 42(4), 154–160. https://doi.org/10.5298/1081-5937-42.4.06
Peper, E., Mason, L., Harvey, R., Wolski, L, & Torres, J. (2020). Can acid reflux be reduced by breathing? Townsend Letters-The Examiner of Alternative Medicine, 445/446, 44–47. https://www.townsendletter.com/article/445-6-acid-reflux-reduced-by-breathing/
Peper, E., Mason, L., Huey, C. (2017). Healing irritable bowel syndrome with diaphragmatic breathing. Biofeedback, 45(4), 83–87. https://doi.org/10.5298/1081-5937-45.4.04
Peper, E., Miceli, B., & Harvey, R. (2016). Educational model for self-healing: Eliminating a chronic migraine with electromyography, autogenic training, posture, and mindfulness. Biofeedback, 44(3), 130–137. https://www.aapb.org/files/publications/biofeedback/2016/biof-44-03-130-137.pdf
Peper, E., Shaffer, F., & Lin, I. M. (2010). Garbage in; Garbage out—Identify blood volume pulse (BVP) artifacts before analyzing and interpreting BVP, blood volume pulse amplitude, and heart rate/respiratory sinus arrhythmia data. Biofeedback, 38(1), 19–23. https://doi.org/10.5298/1081-5937-38.1.19
Sapolsky, R. (2004). Why Zebras Don’t Get Ulcers. Owl Books ISBN: 978-0805073690
Shaffer, F., Combatalade, D., Peper, E., & Meehan, Z. M. (2016). A guide to cleaner electrodermal activity measurements. Biofeedback, 44( 2), 90–100. https://doi.org/10.5298/1081-5937-44.2.01
Smith, M. M., Saklofske, D. H., Stoeber, J., & Sherry, S. B. (2016). The big three perfectionism scale: A new measure of perfectionism. Journal of Psychoeducational Assessment, 34(7), 670–687. https://doi.org/10.1177/0734282916651539
Sowder, E., Gevirtz, R., Shapiro, W., & Ebert, C. (2010). Restoration of vagal tone: a possible mechanism for functional abdominal pain. Applied Psychophysiology and Biofeedback, 35(3), 199–206. https://doi.org/10.1007/s10484-010-9128-8
Stern, M. J., Guiles, R. A., & Gevirtz, R. (2014). HRV biofeedback for pediatric irritable bowel syndrome and functional abdominal pain: A clinical replication series. Applied Psychophysiology and Biofeedback, 39(3), 287–291. https://doi.org/10.1007/s10484-014-9261-x
Stonehewer, L. (2009). Dysfunctional breathing for women’s health physiotherapists. Journal of the Association of Chartered Physiotherapists in Women’s Health, 104, 38–40. https://pogp.csp.org.uk/system/files/stonehewer_hr.pdf
Streeter, C. C., Gerbarg, P. L., Saper, R. B., Ciraulo, D. A., & Brown, R. P. (2012). Effects of yoga on the autonomic nervous system, gamma-aminobutyric-acid, and allostasis in epilepsy, depression, and post-traumatic stress disorder. Medical hypotheses, 78(5), 571–579. https://doi.org/10.1016/j.mehy.2012.01.021
Sun, X., Shang, W., Wang, Z., Liu, X., Fang, X., & Ke, M. (2016). Short-term and long-term effect of diaphragm biofeedback training in gastroesophageal reflux disease: An open-label, pilot, randomized trial. Diseases of the Esophagus, 29(7), 829–836. https://doi.org/10.1111/dote.12390
Taneja. I., Deepak, K.K., Poojary, G., Acharya, I.N., Pandey, R.M., & Sharma, M.P. (2004). Yogic versus conventional treatment in diarrhea-predominant irritable bowel syndrome: a randomized control study. Appl Psychophysiol Biofeedback, 29(1), 19-33. https://doi.org/10.1023/b:apbi.0000017861.60439.95
Vlieger, A. M., Blink, M., Tromp, E., & Benninga, M. A. (2008). Use of complementary and alternative medicine by pediatric patients with functional and organic gastrointestinal diseases: results from a multicenter survey. Pediatrics, 122(2), e446–e451. https://doi.org/10.1542/peds.2008-0266
A breath of fresh air: Breathing and posture to optimize health
Posted: April 3, 2022 Filed under: behavior, Breathing/respiration, CBT, cognitive behavior therapy, emotions, ergonomics, Exercise/movement, health, mindfulness, Neck and shoulder discomfort, Pain/discomfort, posture, self-healing, stress management, Uncategorized | Tags: respiration 2 CommentsMost people breathe 22,000 breaths per day. We tend to breathe more rapidly when stressed, anxious or in pain. While a slower diaphragmatic breathing supports recovery and regeneration. We usually become aware of our dysfunctional breathing when there are problems such as nasal congestion, allergies, asthma, emphysema, or breathlessness during exertion. Optimal breathing is much more than the absence of symptoms and is influenced by posture. Dysfunctional posture and breathing are cofactors in illness. We often do not realize that posture and breathing affect our thoughts and emotions and that our thoughts and emotions affect our posture and breathing. Watch the video, A breath of fresh air: Breathing and posture to optimize health, that was recorded for the 2022 Virtual Ergonomics Summit.
Useful resources about breathing, phytonutrients and exercise
Posted: June 30, 2021 Filed under: behavior, Breathing/respiration, cancer, Evolutionary perspective, health, Nutrition/diet, self-healing, Uncategorized | Tags: diet, exercise, immune system, nasal breathing, phytonutrients, respiration 1 Comment
Dysfunctional breathing, eating highly processed foods, and lack of movement contribute to development of illnesses such as cancer, diabetes, cardiovascular disease and many chronic diseases. They also contributes to immune dysregulation that increases vulnerability to infectious diseases, allergies and autoimmune diseases. If you wonder what breathing patterns optimize health, what foods have the appropriate phytonutrients to support your immune system, or what the evidence is that exercise reduces illness and promotes longevity, look at the following resources.
Breath: the mind-body connector that underlies health and illness
Read the outstanding article by Martin Petrus (2021). How to breathe.
https://psyche.co/guides/how-to-breathe-your-way-to-better-health-and-transcendence
You are the food you eat
Watch the superb webinar presentation by Deanna Minich, MS., PHD., FACN, CNS, (2021) Phytonutrient Support for a Healthy Immune System.
Movement is life
Explore the summaries of recent research that has demonstrated the importance of exercise to increase healthcare saving and reduce hospitalization and death.
Do nose breathing FIRST in the age of COVID-19
Posted: May 30, 2020 Filed under: Breathing/respiration, health, self-healing, Uncategorized | Tags: anxiety, COVID-19, HRV, nasal breathing, respiration 4 Comments
Breathing affects every cell of our body and should be the first intervention strategy to improve physical and mental well-being (Peper & Tibbetts, 1994). Breathing patterns are much more subtle than indicated by the respiratory function tests (spirometry, lung capacity, airway resistance, diffusing capacity and blood gas analysis) or commonly monitored in medicine and psychology (breathing rate, tidal volume, peak flow, oxygen saturation, end-tidal carbon dioxide) (Gibson, Loddenkemper, Sibille & Lundback, 2019).
When a person feels safe, healthy and peaceful, the breathing is effortless and the breath flows in and out of the nose without awareness. Functional and dysfunctional breathing patterns includes an assessment of the whole body pattern by which breathing occurs such as nose versus mouth breathing, alternation of nasal patency, the rate of air flow rate during inhalation and exhalation, the length of time during inhalation and exhalation, the post exhalation pause time. the pattern of transition between inhaling and exhaling, the location and timing of expansion in the truck, the range of diaphragmatic movement, and the subjective quality of breathing effort (Gilbert, 2019; Peper, Gilbert, Harvey & Lin, 2015; Nestor, 2020).
Breathing patterns affect sympathetic and parasympathetic nervous systems (Levin & Swoap, 2019). Inhaling tends to activate the sympathetic nervous system (fight/flight response) while exhaling activates the parasympathetic nervous system (rest and repair response) (Lehrer & Gevirtz, 2014). To observe how breathing affects your heart rate, monitor your pulse from either the radial artery in the wrist or the carotid artery in your neck as shown in Figure 1 and practice the following.
After sensing the baseline rate of your pulse, continue to feel your radial artery pulse in your wrist or at the carotid artery in your neck. Then inhale for the count of four hold for a moment and gently exhale for the count of 5 or 6. Repeat two or three times.
Most people observe that during inhalation, their heart rate increased (sympathetic activation for action) and during exhalation, the heart rate decreases (restoration during safety).
Nearly everyone who is anxious tends to breathe rapidly and shallowly or when stressed, unknowingly gasp or holds their breath–they may even freeze up and blank out (Peper et al, 2016). In addition, many people habitually breathe through their mouth instead of their nose and wake up tired with a dry mouth with bad breath. Mouth breathing combined with chest breathing in the absence of slower diaphragmatic breathing (the lower ribs and abdomen expand during inhalation and constrict during exhalation) is a risk factor for disorders such as irritable bowel syndrome, hypertension, tiredness, anxiety, panic attacks, asthma, dysmenorrhea, epilepsy, cold hands and feet, emphysema, and insomnia. Many of our clients who aware of their dysfunctional breathing patterns and are able to implement effortless breathing report significant reduction in symptoms (Chaitow, Bradley, & Gilbert, 2013; Peper, Mason, Huey, 2017; Peper & Cohen, 2017; Peper, Martinez Aranda, & Moss, 2015).
Breathing is usually overlooked as a first treatment strategy-it is not as glamorous as drugs, surgery or psychotherapy. Teaching breathing takes skill since practitioners needs to be experienced. Namely, they need to be able to demonstrate in action how to breathe effortlessly before teaching it to others. Although it seems unbelievable, a small change in our breathing pattern can have major physical, mental, and emotional effects as can be experienced in the following practice.
Begin by breathing normally and then exhale only 70% of the inhaled air, and inhale normally and again exhale only 70% of the inhaled air. With each exhalation exhale on 70% of the inhaled air. Continue this for 30 seconds. Stop and note how you feel.
Almost every reports that the 30 seconds feels like a minute and experience some of the following symptoms listed in table 1.
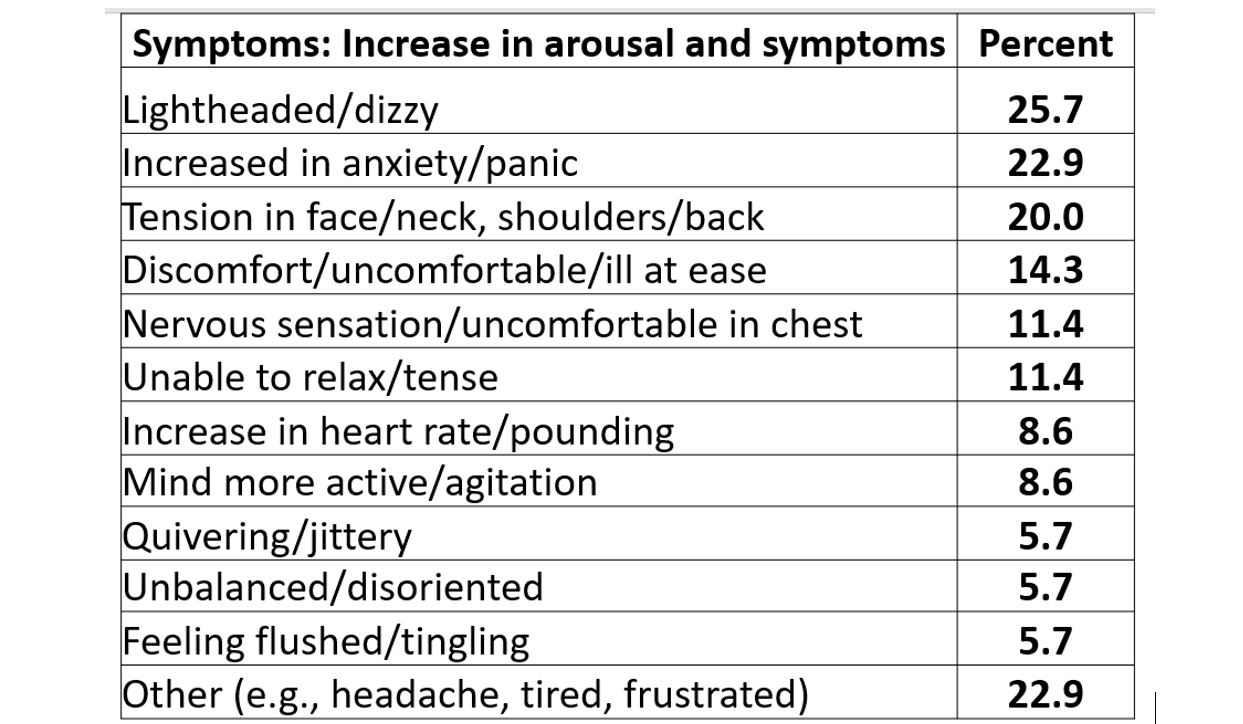
Table 1. Symptoms experienced after 30-45 seconds of sequentially exhaling 70% percent of the inhales air (Peper & MacHose, 1993).
Even though many therapists have long pointed out that breathing is essential, it is usually the forgotten ingredient. It is now being rediscovered in the age of the COVID-19 as respiratory health may reduce the risk of COVID-19.
Simply having very sick patients lie on their side or stomach can improve gas exchange. By lying on your side or prone, breathing is easier as the lung can expand more which appears to reduce the utilization of respirators and intubation (Long & Singh, 2020; Farkas, 2020). This side or prone breathing approach is thousands of years old.
One of the natural and health promoting breathing patterns to promote lung health is to breathe predominantly through the nose. The nose filters, warms, moisturizes and slows the airflow so that airway irritation is reduced. Nasal breathing also increases nitric oxide production that significantly increases oxygen absorption in the body. More importantly for dealing with COVID-19, nitric oxide, produced and released inside the nasal cavities and the lining of the blood vessels, acts as an anti-viral and is a secondary strategy to protect against viral infections (Mehta, Ashkar & Mossman, 2012). During inspiration through the nose, the nitric oxide helps dilate the airways in your lungs and blood vessels (McKeown, 2016).
To increase your health, breathe through your nose, yes, even at night (McKeown, 2020). As you practice this during the day be sure that the lower ribs and abdomen expand during inhalation and decrease in diameter during exhalation. It is breathing without effort although many people will report that it initially feels unnatural. Exhale to the count of about 5 or 6 and inhale (allow the air to flow in) to the count of 4 or 5. Mastering nasal breathing takes practice, practice and practice. See the following for more information.
Watch the Youtube presentation by Patrick McKeown author of the Oxygen Advantage, Practical 40 minute free breathing session with Patrick McKeown to improve respiratory health. https://www.youtube.com/watch?v=AiwrtgWQeDc&t=680s
Listen to Terry Gross interviewing James Nestor on “How The ‘Lost Art’ Of Breathing Can Impact Sleep And Resilience” on May 27, 2020 on the NPR radio show, Fresh Air.
Look at the Peperperspective blogs that focus on breathing in the age of Covid-19.
Read science writer James Nestor’s book, Breath The new science of a lost art, Breath The new science of a lost art.
References
Allen, R. (2017).The health benefits of nose breathing. Nursing in General Practice.
Christopher, G. (2019). A Guide to Monitoring Respiration. Biofeedback, 47(1), 6-11.
Farkas, J. (2020). PulmCrit – Awake Proning for COVID-19. May 5, 2020.
Long, L. & Singh, S. (2020). COVID-19: Awake Repositioning / Proning. EmDocs
McKeown, P. (2016). Oxygen advantage. New York: William Morrow.
Nestor, James. (2020). Breath The new science of a lost art. New York: Riverhead Books
Family or work? The importance of value clarification
Posted: May 4, 2018 Filed under: Breathing/respiration, mindfulness, Neck and shoulder discomfort, Pain/discomfort, relaxation, stress management, Uncategorized | Tags: meaning, regeneration, relaxation, respiration, stress management, values clarification 1 CommentRichard Harvey, PhD and Erik Peper, PhD

In a technologically modern world, many people have the option of spending 24 hours a day/ 7 days a week continuously interacting via telephone, text, work and personal emails or internet websites and various social media platforms such as Facebook, What’s App, Instagram, Twitter, LinkedIn and Snapchat. How many people do we know who work too many hours, watch too many episodes on digital screens, commute too many hours, or fill loneliness with online versions of retail therapy? In the rush of work-a-day survival as well as being nudged and bombarded with social media notifications, or advertisements for material goods, we forget to nurture meaningful friendships and family relationships (Peper and Harvey, 2018). The following ‘values clarification’ practice may help us identify what is most important to us and help keep sight of those things that are most relevant in our lives (Hofmann, 2008; Knott, Ribar, & Duson, 1989; Twohig & Crosby, 2009;. Peper, 2014).
Give yourself about 12 minutes of uninterrupted time to do this practice. Do this practice by yourself, in a group, or with family and friends. Have a piece of paper ready. Be guided by the two video clips at the end of the blog. Begin with the Touch Relaxation and Regeneration Practice to relax and let go of thoughts and worries, then follow it with the Value Clarification Practice.
Touch Relaxation and Regeneration Practice
Turn off your cell phone and let other know not to interrupt for the next 12 minutes, then engage in the following six-minute relaxation exercise. If your attention wanders during the practice, then bring your attention back to the various sensations in your body.
- Sit comfortably, then lift your arms from your lap, holding them parallel to the floor and tighten your arms while making a fist in each hand. While holding your fists tightly closed, keep breathing for a total of 10 seconds before dropping the arms to your lap while you relax all of your muscles. Attend for 20 seconds to the changing sensations in arms and hands as they relax. If your attention wanders bring it back to the sensations in your arm and hands.
- Tighten your buttock muscles and bend your ankles so that the toes move upwards in a direction towards your knees. Keep breathing and hold your toes upwards for 10 seconds and then let the toes move down to the floor, letting go and relaxing all the muscles of the lower trunk and legs. Feel your knees widening and feel your buttock muscles relaxing. Continue attending to the body and muscle sensations for the next 20 seconds. If your attention wanders bring it back to the sensations in your body.
- Tighten your whole body by pressing your knees together, lifting your arms up from your lap, making a fist and wrinkling your face. Hold the tension while continuing to breath for 10 seconds. Let go and relax and feel the whole body sinking and relaxing and being supported by the chair for the next 20 seconds.
- Bring your right hand to your left shoulder. Over the next 10 seconds, inhale for three or four seconds and as you exhale for five or six seconds, with your right hand stroke down your left arm from your shoulder to past your hand. Imagine that the exhaled air is flowing through your arm and out your hand. Repeat at least once more.
- Bring your left hand to your right shoulder. Inhale for three or four seconds and as you exhale for five or six seconds with your left hand stroke down your right arm from your shoulder to past your hand. Imagine that the exhaled air is flowing through your arm and out your hand. Repeat at least once more.
- Bring both hands to the sides of your hips. Inhale for three or four seconds and as you exhale for five or six seconds stroke your legs with your hands from the hips to the ankles. Imagine that the exhaled air is flowing through your legs and out your feet. Repeat a least once more.
- Close your eyes and inhale for three or four seconds, then hold your breath for seven seconds slowly exhale for eight seconds. Imagine as you exhale the air flowing through your arms and out your hands and through your legs and out your feet. Continue breathing easily and slowly such as inhaling for three or four seconds, and out for five to seven seconds. If your attention wanders just bring it back to the sensations going down your arms and legs. Feel the relaxation and peacefulness.
- Take another deep breath and then stretch and continue with the Value Clarification
Value Clarification Practice
Get the paper and pen and do the following Value Clarification Practice.
- Quickly (e.g. 30-60 seconds) list the 10 most important things in your life. For the activity to work, the list must contain 10 important things that may be concrete or abstract, ranging from material things such as a smart phone or a car to immaterial things such as family, love, god, health… If you need to, break up a larger category into smaller pieces. For example, if one item on the list is family, and you only have seven items on the list, assuming you have a family of four, then identify separate family members in order to complete a list of 10 important things.
- To start off, in only 10 seconds, please cross off three items from the list, then explain why you removed those three. If done in a group of people turn to the person explain why you made these choices.
- Next, in only 10 seconds, please cross off three more, then explain why you kept what you kept. If done in a group of people turn to the person explain why you made these choices.
- Finally, in only 10 seconds, please cross off three more, then reveal the one most important thing on your list. Share your choice for the item you kept and how you felt while crossing items from the list or keeping them.
- When engaging with this type of values clarification practice, please remind yourself and others that the items on the list were never gone, they are always in your life to the extent that you can honor the presence of those things in your life.
We have done these exercises with thousands of student and adults. The most common final item on the list is family or an individual family member. Sometimes, categories such as health or god appear, however it is extremely rare that material items make it to the final round. For example, no one would report that their last item is their job, their bank account, their house, or their smart phone. It is common that people have difficulty choosing the last item on their list, often taking more than 10 seconds to choose. For example, they find that they cannot choose between eliminating individual family members. For those who find the activity too difficult, remind them that the exercise is voluntary and meant as a ‘thought experiment’ which they may stop at any time.
Reflect how much of your time is spent nurturing what is most important to you? In many cases we feel compelled to finish some employment priorities instead of making time for nurturing our family relationship. And when we become overwhelmed with work demands, we retreat to sooth our difficulties by checking our email or browsing social media rather than supporting the family connections that are so important to us.
Organize an action plan to honor and support your commitment to the items on your list that you value the most. If possible let other people know what you are doing.
- Describe in detail what you will do in real life and in real time in service to honor and support your relationships with the things that you value.
- Describe in detail what you will do, when you will do it, with whom you will do it, at what time you will do it, and anticipate what will get in the way of doing it. For example, how will you resolve any conflicts between what you plan and what you actually do when there is not enough time to carry out your plans?
- Schedule a time during the following week for feedback about your plans to honor and support the things you value.
Summary
Many people experience that it is challenging to make time to honor and support their primary values given the ongoing demands of daily living. To be congruent with our values means making ongoing choices such as listening and sharing experiences with your partner versus binging on videos or, using your smartphone for answering email or texting instead of watching your child play ball.
The values you previously identified are similar to those identified by patients who are in hospice and dying. For them as they look back on their lives, the five most common regret are (Ware, 2009; Ware, 2012):
- I wish I’d the courage to live a life true to myself, not the life others expected of me.
- I wish I hadn’t worked so hard.
- I wish I had the courage to express my feelings.
- I wish I had stayed in touch with my friends.
- I wish I had let myself be happier.
Take the time to plan actions that support your identified values. Feel free to watch the following videos that guide you through the activities described here.
References
Hofmann, S.G. (2008). Acceptance and commitment therapy: New wave or Morita therapy?. Clinical Psychology: Science and Practice, 15(4), 280-285. https://doi.org/10.1111/j.1468-2850.2008.00138.x
Knott, J.E., Ribar, M.C. & Duson, B.M. (1989). Thanatopics: Activities and Exercises for Confronting Death, Lexington Books: Lexington, MA. https://www.amazon.com/Thanatopics-Activities-Exercise-Confronting-Death/dp/066920871X
Peper, E. (October 19, 2014). Choices-Creating meaningful days. https://peperperspective.com/2014/10/19/choices-creating-meaningful-days/
Peper, E. & Harvey, R. (2018). Digital addiction: increased loneliness, depression, and anxiety. NeuroRegulation. 5(1),3–8. doi:10.15540/nr.5.1.3 http://www.neuroregulation.org/article/view/18189/11842
Twohig, M.P. & Crosby, J.M. (2009). Values clarification. In: O’Donohue & W.T., Fisher, J.E., Eds. Cognitive behavior therapy: applying empirically supported techniques in your practice. Wiley: Hoeboken, N.J., p. 681-686.
Ware, B. (2009). Regrets of the dying. https://bronnieware.com/blog/regrets-of-the-dying/
Ware, B. (2012). The top five regrets of dying: A life transformed by the dearly departing. Hay House. ISBN: 978-1401940652
Breathing to improve well-being
Posted: November 17, 2017 Filed under: Breathing/respiration, Exercise/movement, Neck and shoulder discomfort, Pain/discomfort, self-healing, stress management, Uncategorized | Tags: anxiety, Breathing, health, mindfulness, pain, respiration, stress 9 CommentsBreathing affects all aspects of your life. This invited keynote, Breathing and posture: Mind-body interventions to improve health, reduce pain and discomfort, was presented at the Caribbean Active Aging Congress, October 14, Oranjestad, Aruba. www.caacaruba.com
The presentation includes numerous practices that can be rapidly adapted into daily life to improve health and well-being.
Do you blank out on exams? Improve school performance with breathing* **
Posted: September 18, 2016 Filed under: Breathing/respiration, stress management, Uncategorized | Tags: anxiety, fear, gasping, math, memory, performance, respiration 3 Comments “I opened the exam booklet and I went blank.”
“I opened the exam booklet and I went blank.”
“When I got anxious, I took a slow breath, reminded myself that I would remember the material. I successfully passed the exam.”
“I was shocked, when I gasped, I could not remember my girlfriend’s name and then I could not remember my mother’s name. When breathed slowly, I had no problem and easily remembered both”
Blanking out the memorized information that you have studied on an exam is a common experiences of students even if they worked hard (Arnsten, Mazure, & Sinha, 2012). Fear and poor study habits often contribute to forgetting the material (Fitkov-Norris, & Yeghiazarian, 2013). Most students study while listening to music, responding to text message, or monitoring social network sites such as, Facebook, twitter, Instagram, or Pinterest (David et al., 2015).. Other students study the material for one class then immediately shift and study material from another class. While at home they study while sitting or lying on their bed. Numerous students have internalized the cultural or familial beliefs that math is difficult and you do not have the aptitude for the material—your mother and father were also poor in math (Cherif, Movahedzadeh, Adams, & Dunning, 2013). These beliefs and dysfunctional study habits limit learning (Neal, Wood, & Drolet, 2013).
Blanking out on an exam or class presentation is usually caused by fear or performance anxiety which triggers a stress response (Hodges, 2015; Spielberger, Anton, & Bedell, 2015). At that moment, the brain is flooded with thoughts such as, I can’t do it,” “I will fail,” “I used to know this, but…”, or “What will people think?” The body responds with a defense reaction as if you are being threatened and your survival is at stake. The emotional reactivity and anxiety overwhelms cognition, resulting in an automatic ‘freeze’ response of breath holding or very shallow breathing. At that moment, you blank out (Hagenaars, Oitzl, & Roelofs, 2014; Sink et al., 2013; Von Der Embse, Barterian, & Segool, 2013).
Experience how your thinking is affected by your breathing pattern. Do the following practice with another person.
Have the person ask you a question and the moment you hear the beginning of the question, gasp as if you are shocked or surprised. React just as quickly and automatically as you would if you see a car speeding towards you. At that moment of shock or surprise, you do not think, you don’t spend time identifying the car or look at who is driving. You reflexively and automatically jump out of the way. Similarly in this exercise, when you are asked to answer a question, act as if you are as shocked or surprised to see a car racing towards you.
Practice gasping at the onset of hearing the beginning of a question such as, “What day was it yesterday?” At the onset of the sound, gasp as if startled or afraid. During the first few practices, many people wait until they have heard the whole phrase before gasping. This would be similar to seeing a car racing towards you and first thinking about the car, at that point you would be hit. Repeat this a few times till it is automatic.
Now change the breathing pattern from gasping to slow breathing and practice this for a few times.
When you hear the beginning of the question breathe slowly and then exhale.” Inhale slowly for about 4 seconds while allowing your abdomen to expand and then exhale softly for about 5 or six seconds. Repeat practicing slow breathing in response to hearing the onset of the question until it is automatic.
Now repeat the two breathing patterns (gasping and slow breathing) while the person asks you a subtraction or math questions such as, “Subtract 7 from 93.”
In research with more than 100 college students, we found that students had significantly more self-reported anxiety and difficulty in solving math problems when gasping as compared to slow breathing as shown Figure 1 (Lee et al, 2016; Peper, Lee, Harvey & Lin, 2016).
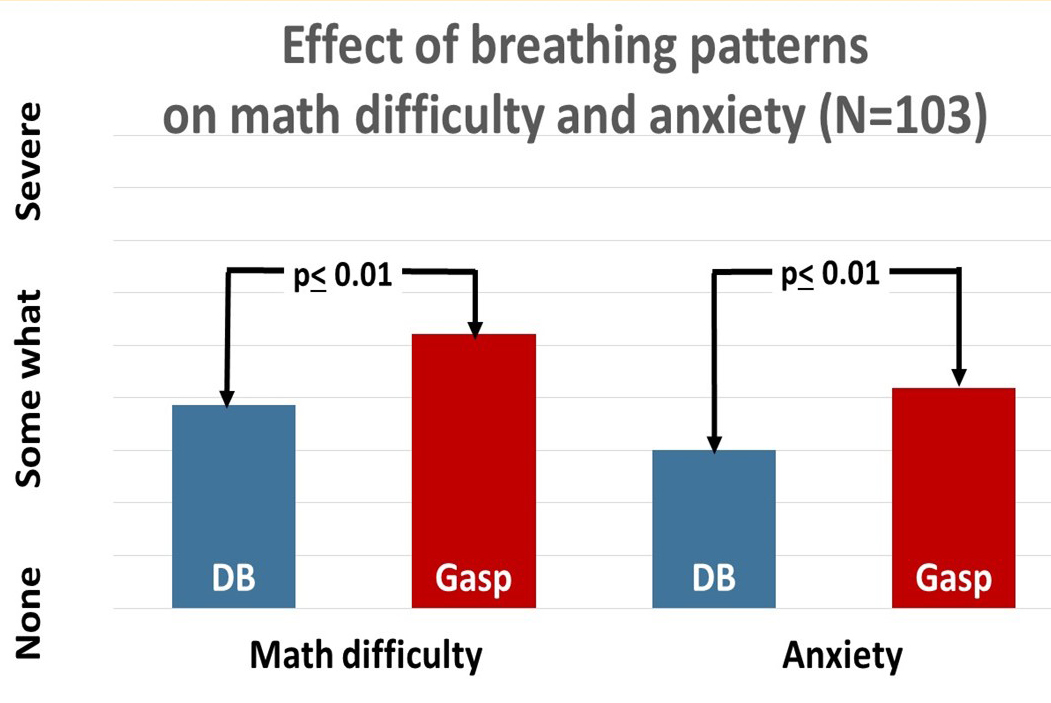
Fig 1. The effect of breathing style on math performance. Diaphragmatic breathing significantly increased math performance and decreased anxiety (from: Peper, Lee, Harvey & Lin, 2016).
As one 20 year old college student said, “When I gasped, my mind went blank and I could not do the subtraction. When I breathed slowly, I had no problem doing the subtractions. I never realized that breathing had such a big effect upon my performance.”
When you are stressed and blank out, take a slow diaphragmatic breath to improve performance; however, it is only effective if you have previously studied the materials effectively. To improve effective learning incorporate the following concepts when studying.
- Approached learning with a question. When you begin to study the material or attend a class, ask yourself a question that you would like to be answered. When you have a purpose, it is easier to stay emotionally present and remember the material (Osman, & Hannafin, 1994).
- Process what you are learning with as many sensory cues as possible. Take hand written notes when reading the text or listening to your teacher. Afterwards meet with your friends in person, on Skype and again discuss and review the materials. As you discuss the materials, add comments to your notes. Do not take notes on your computer because people can often type almost as quickly as someone speaks. The computer notes are much less processed and are similar to the experience of a court or medical transcriptionist where the information flows from the ears to the fingers without staying in between. College students who take notes in class on a computer or tablets perform worse on exams than students who write notes. When you write your notes you have to process the material and extract and synthesis relevant concepts.
- Review the notes and material before going to sleep. Research has demonstrated that whatever material is in temporary memory before going to sleep will be more likely be stored in long term memory (Gais et al., 2006; Diekelmann et al., 2009). When you study material is stored in temporary memory, and then when you study something else, the first material tends to displaced by the more recent material. The last studied material is more likely stored in long term memory. When you watch a movie after studying, the movie content is preferentially stored in permanent memory during sleep. In addition, what is emotionally most important to you is usually stored first. Thus, instead of watching movies and chatting on social media, discuss and review the materials just before you go to sleep.
- Learning is state dependent. Study and review the materials under similar conditions as you will be tested. Without awareness the learned content is covertly associated with environmental, emotional, social and kinesthetic cues. Thus when you study in bed, the material is most easily accessed while lying down. When you study with music, the music become retrieval trigger. Without awareness the materials are encoded with the cues of lying down or the music played in the background. When you come to the exam room, none of those cues are there, thus it is more difficult to recall the material (Eich, 2014).
- Avoid interruptions. When studying each time you become distracted by answering a text message or responding to social media, your concentration is disrupted (Swingle, 2016). Imagine that learning is like scuba diving and the learning occurs mainly at the bottom. Each interruption forces you to go to the surface and it takes time to dive down again. Thus you learn much less than if you stayed at the bottom for the whole time period.
- Develop study rituals. Incorporate a ritual before beginning studying and repeat it during studying such as three slow breaths. The ritual can become the structure cue associated with the learned material. When you come to exam and you do not remember or are anxious, perform the same ritual which will allow easier access to the memory.
- Change your internal language. What we overtly or covertly say and believe is what we become. When you say, “I am stupid”, “I can’t do math,” or “It is too difficult to learn,” you become powerless which increases your stress and inhibits cognitive function. Instead, change your internal language so that it implies that you can master the materials such as, “I need more time to study and to practice the material,” “Learning just takes time and at this moment it may take a bit longer than for someone else,” or “I need a better tutor,”
When you take charge of your study habits and practice slower breathing during studying and test taking, you may experience a significant improvement in learning, remembering, accessing, and processing information.
References
Arnsten, A., Mazure, C. M., & Sinha, R. (2012). This is your brain in meltdown. Scientific American, 306(4), 48-53.
Cherif, A. H., Movahedzadeh, F., Adams, G. E., & Dunning, J. (2013). Why Do Students Fail?. Higher Learning, 227, 228.
David, P., Kim, J. H., Brickman, J. S., Ran, W., & Curtis, C. M. (2015). Mobile phone distraction while studying. new media & society, 17(10), 1661-1679.
Diekelmann, S., Wilhelm, I., & Born, J. (2009). The whats and whens of sleep-dependent memory consolidation. Sleep medicine reviews, 13(5), 309-321.
Eich, J. E. (2014). State-dependent retrieval of information in human episodic memory. Alcohol and Human Memory (PLE: Memory), 2, 141.
Fitkov-Norris, E. D., & Yeghiazarian, A. (2013). Measuring study habits in higher education: the way forward?. In Journal of Physics: Conference Series (Vol. 459, No. 1, p. 012022). IOP Publishing.
Gais, S., Lucas, B., & Born, J. (2006). Sleep after learning aids memory recall. Learning & Memory, 13(3), 259-262.
Hagenaars, M. A., Oitzl, M., & Roelofs, K. (2014). Updating freeze: aligning animal and human research. Neuroscience & Biobehavioral Reviews, 47, 165-176.
Hodges, W. F. (2015). The psychophysiology of anxiety. Emotions and Anxiety (PLE: Emotion): New Concepts, Methods, and Applications, 12, 175.
Lee, S., Sanchez, J., Peper, E., & Harvey, R. (2016). Effect of Breathing Style on Math Problem Solving. Presented at the 47th Annual Meeting of the Association for Applied Psychophysiology and Biofeedback, Seattle WA, March 9-12, 2016
Neal, D. T., Wood, W., & Drolet, A. (2013). How do people adhere to goals when willpower is low? The profits (and pitfalls) of strong habits. Journal of Personality and Social Psychology, 104(6), 959.
Osman, M. E., & Hannafin, M. J. (1994). Effects of advance questioning and prior knowledge on science learning. The Journal of Educational Research,88(1), 5-13.
Peper, E., Lee, S., Harvey, R., & Lin, I-M. (2016). Breathing and math performance: Implication for performance and neurotherapy. NeuroRegulation, 3(4),142–149.
Spielberger, C. D., Anton, W. D., & Bedell, J. (2015). The nature and treatment of test anxiety. Emotions and anxiety: New concepts, methods, and applications, 317-344.
Sink, K. S., Walker, D. L., Freeman, S. M., Flandreau, E. I., Ressler, K. J., & Davis, M. (2013). Effects of continuously enhanced corticotropin releasing factor expression within the bed nucleus of the stria terminalis on conditioned and unconditioned anxiety. Molecular psychiatry, 18(3), 308-319.
Swingle, M. (2016). i-Minds: How cell phones, computers, gaming and social media are changing our brains, our behavior, and the evolution of our species. Gabriola Island, BC, Canada: New Society Publishers.
Von Der Embse, N., Barterian, J., & Segool, N. (2013). Test anxiety interventions for children and adolescents: A systematic review of treatment studies from 2000–2010. Psychology in the Schools, 50(1), 57-71.
*I thank Richard Harvey, PhD. for his constructive feedback and comments and Shannon Lee for her superb research.
** This blog was adapted from: Lee, S., Sanchez, J., Peper, E., & Harvey, R. (2016). Effect of Breathing Style on Math Problem Solving. Presented at the 47th Annual Meeting of the Association for Applied Psychophysiology and Biofeedback, Seattle WA, March 9-12, 2016
Allow natural breathing with abdominal muscle biofeedback [1, 2]
Posted: April 26, 2016 Filed under: Breathing/respiration, self-healing, Uncategorized | Tags: abdominal breathing, biofeedback, EMG, Muscle feedback, respiration 7 CommentsWhen I allowed my lower abdomen to expand during inhalation without any striving and slightly constrict during exhalation, breathing was effortless. At the end of exhalation, I just paused and then the air flowed in without any effort. I felt profoundly relaxed and safe. With each effortless breath my hurry-up sickness dissipated.
Effortless breathing from a developmental perspective is a whole body process previously described by the works of Elsa Gindler, Charlotte Selver and Bess M. Mensendieck (Brooks, 1986; Bucholtz, 1994; Gilbert 2016, Mensendieck, 1954). These concepts underlie the the research and therapeutic approach of Jan van Dixhoorn (2008, 2014) and is also part of the treatment processes of Mensendieck/Cesar therapists (Profile Mensendeick) . During inhalation the body expands and during exhalation the body contracts. While sitting or standing, during exhalation the abdominal wall contracts and during inhalation the abdominal wall relaxes. This whole body breathing pattern is often absent in clients who tend to lift their chest and do not expand or sometimes even constrict their abdomen when they inhale . Even if their breathing includes some abdominal movement, often only the upper abdomen above the belly button moves while the lower abdomen shows limited or no movement. This may be associated with physical and emotional discomfort such as breathing difficulty, digestive problems, abdominal and pelvic floor pains, back pain, hyper vigilance, and anxiety. (The background, methodology to monitor and train with muscle biofeedback, and pragmatic exercises are described in detail in our recent published article, Peper, E., Booiman, A.C, Lin, I-M, Harvey, R., & Mitose, J. (2016). Abdominal SEMG Feedback for Diaphragmatic Breathing: A Methodological Note. Biofeedback. 44(1), 42-49.)
Some of the major factors that contribute to the absence of abdominal movement during breathing are (Peper et, 2015):
- ‘Designer jean syndrome’ (the modern girdle): The abdomen is constricted by a waist belt, tight pants or slimming underwear such as Spanx and in former days by the corset as shown in Figure 1 (MacHose & Peper, 1991; Peper & Tibbitts, 1994).
- Self-image: The person tends to pull his or her abdomen inward in an attempt to look slim and attractive.
- Defense reaction: The person unknowingly tenses the abdominal wall –a flexor response-in response to perceived threats (e.g., worry, external threat, loud noises, feeling unsafe). Defense reactions are commonly seen in clients with anxiety, panic or phobias.
- Learned disuse: The person covertly learned to inhibit any movement in the abdominal wall to protect themselves from experiencing pain because of prior abdominal injury or surgery (e.g., hernia or cesarean), abdominal pain (e.g., irritable bowel syndrome, dysmenorrhea, vulvodynia, pelvic floor pain, low back pain).
- Inability to engage abdominal muscles because of the lack of muscle tone.
 Figure 1. How clothing constricts abdominal movement. Previously it was a corset as shown on the left and now it is Spanx or very tight clothing which restricts the waist.
Figure 1. How clothing constricts abdominal movement. Previously it was a corset as shown on the left and now it is Spanx or very tight clothing which restricts the waist.
Whether the lower abdominal muscles are engaged or not (either by chronic tightening or lack of muscle activation), the resultant breathing pattern tends to be more thoracic, shallow, rapid, irregular and punctuated with sighst. Over time participants may not able to activate or relax the lower abdominal muscles during the respiratory cycle. Thus it is no longer involved in whole body movement which can usually be observed in infants and young children.
In our published paper by Peper, E., Booiman, A.C, Lin, I-M, Harvey, R., & Mitose, J. (2016), we describe a methodology to re-establish effortless whole body breathing with the use of surface electromyography (SEMG) recorded from the lower abdominal muscles (external/ internal abdominal oblique and transverse abdominis) and strategies to teach engagement of these lower abdominal muscles. Using this methodology, the participants can once again learn how to activate the lower abdominal muscles to flatten the abdominal wall thereby pushing the diaphragm upward during exhalation. Then, during inhalation they can relax the muscles of the abdominal wall to expand the abdomen and allow the diaphragm to descend as shown in Figure 2.
 Figure 2. Correspondence between respiratory strain gauge changes and SEMG activity during breathing. When the person exhales, the lower abdominal SEMG activity increases and when the person inhales the SEMG decreases.
Figure 2. Correspondence between respiratory strain gauge changes and SEMG activity during breathing. When the person exhales, the lower abdominal SEMG activity increases and when the person inhales the SEMG decreases.
The published article discusses the factors that contribute to the breathing dysregulation and includes guidelines for using SEMG abdominal recording. It describes in detail–with illustrations–numerous practices such as tactile awareness of the lower abdomen, active movements such as pelvic rocking and cats and dogs exercises that people can practice to facilitate lower abdominal breathing. One of these practices, Sensing the lower abdomen during breathing, is developed and described by Annette Booiman, Mensendieck therapist
Sensing the lower abdomen during breathing
The person place their hands below their belly button with the outer edge of hands resting on the groin. During inhalation, they practice bringing their lower abdomen/belly into their hands so that the person can feel the lower abdomen expanding. During exhalation, they pull their lower abdomen inward and away from their palms as shown in Figure 3.
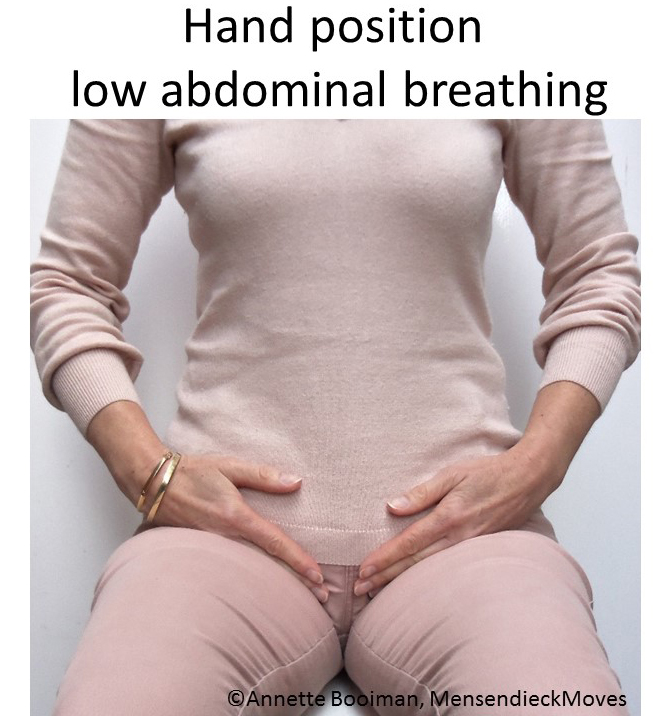
Figure 3. Hands placed below the belly button to sense the movement of the lower abdomen.
Lower abdominal SEMG feedback is useful in retraining breathing for people with depression, rehabilitation after pregnancy, abdomen or chest surgery (e.g., Cesarean surgery, hernia, or appendectomy operations), anxiety, hyperventilation, stress-related disorders, difficulty to become pregnant or maintain pregnancy, pelvic floor problems, headache, low back pain, and lung diseases. As one participant reported:
“Biofeedback might be the single thing that helped me the most. When I began to focus on breathing, I realized that it was almost impossible for me since my body was so tightened. However, I am getting much better at breathing diaphragmatically because I practice every day. This has helped my body and it relaxes my muscles, which in turn help reduce the vulvar pain.”
REFERENCES
Mensendieck, B.M. (1954). Look better, feel better. Pymble, NSW, Australia: HarperCollins.
van Dixhoorn, J. (2008). Whole body breathing. Biofeedback. 3I(2), 54-58
Gilbert, C. (2016). Working with breathing , some early influences. Paper presented at the 47th Annual Meeting of the Association for Applied Psychophysiology and Biofeedback, Seattle WA, March 9-12, 2016.
1. Adapted from: Peper, E., Booiman, A., Lin, I-M, Harvey, R., & Mitose, J. (2016). Abdominal SEMG Feedback for Diaphragmatic Breathing: A Methodological Note. Biofeedback. 44(1), 42-49.
2. .I thank Annette Booiman for her constructive feedback in writing this blog.
Can abdominal surgery cause epilepsy, panic and anxiety and be reversed with breathing biofeedback?*
Posted: March 5, 2016 Filed under: Breathing/respiration, self-healing, stress management, Uncategorized | Tags: anxiety, biofeedback, Breathing, epilepsy, iatrogenic illness, learned disuse, panic, respiration, surgery 4 Comments“I had colon surgery six months ago. Although I made no connection to my anxiety, it just started to increase and I became fearful and I could not breathe. The asthma medication did not help. Learning effortless diaphragmatic breathing and learning to expand my abdomen during inhalation allowed me to breathe comfortably without panic and anxiety—I could breathe again.” (72 year old woman)
“One year after my appendectomy, I started to have twelve seizures a day. After practicing effortless diaphragmatic breathing and changing my lifestyle, I am now seizure-free.” (24 year old male college student)
One of the hidden long term costs of surgery and injury is covert learned disuse. Learned disuse occurs when a person inhibits using a part of their body to avoid pain and compensates by using other muscle patterns to perform the movements (Taub et al, 2006). This compensation to avoid discomfort creates a new habit pattern. However, the new habit pattern often induces functional impairment and creates the stage for future problems.
Many people have experienced changing their gait while walking after severely twisting their ankle or breaking their leg. While walking, the person will automatically compensate and avoid putting weight on the foot of the injured leg or ankle. These compensations may even leads to shoulder stiffness and pain in the opposite shoulder from the injured leg. Even after the injury has healed, the person may continue to move in the newly learned compensated gait pattern. In most cases, the person is totally unaware that his/her gait has changed. These new patterns may place extra strain on the hip and back and could become a hidden factor in developing hip pain and other chronic symptoms.
Similarly, some women who have given birth develop urinary stress incontinence when older. This occurred because they unknowingly avoided tightening their pelvic floor muscles after delivery because it hurt to tighten the stretched or torn tissue. Even after the tissue was healed, the women may no longer use their pelvic floor muscles appropriately. With the use of pelvic floor muscle biofeedback, many women with stress incontinence can rapidly learn to become aware of the inhibited/forgotten muscle patterns (learned disuse) and regain functional control in nine sessions of training (Burgio et al., 1998; Dannecker et al., 2005). The process of learned disuse is the result of single trial learning to avoid pain. Many of us as children have experienced this process when we touched a hot stove—afterwards we tended to avoid touching the stove even when it was cold.
Often injury will resolve/cure the specific problem. It may not undo the covert newly learned dysfunctional patterns which could contribute to future iatrogenic problems or illnesses (treatment induced illness). These iatrogenic illnesses are treated as a new illness without recognizing that they were the result of functional adaptations to avoid pain and discomfort in the recovery phase of the initial illness.
Surgery creates instability at the incision site and neighboring areas, so our bodies look for the path of least resistance and the best place to stabilize to avoid pain. (Adapted from Evan Osar, DC).
After successful surgical recovery do not assume you are healed!
Yes, you may be cured of the specific illness or injury; however, the seeds for future illness may be sown. Be sure that after injury or surgery, especially if it includes pain, you learn to inhibit the dysfunctional patterns and re-establish the functional patterns once you have recovered from the acute illness. This process is described in the two cases studies in which abdominal surgeries appeared to contribute to the development of anxiety and uncontrolled epilepsy.
How abdominal surgery can have serious, long-term effect on changing breathing patterns and contributing to the development of chronic illness.
When recovering from surgery or injury to the abdomen, it is instinctual for people to protect themselves and reduce pain by reducing the movement around the incision. They tend to breathe more shallowly as not to create discomfort or disrupt the healing process (e.g., open a stitch or staple. Prolonged shallow breathing over the long term may result in people experiencing hyperventilation induced panic symptoms or worse. This process is described in detail in our recent article, Did You Ask about Abdominal Surgery or Injury? A Learned Disuse Risk Factor for Breathing Dysfunction (Peper et al., 2015). The article describes two cases studies in which abdominal surgeries led to breathing dysfunction and ultimately chronic, serious illnesses.
Reducing epileptic seizures from 12 per week to 0 and reducing panic and anxiety
A routine appendectomy caused a 24-year-old male to develop rapid, shallow breathing that initiated a series of up to 12 seizures per week beginning a year after surgery. After four sessions of breathing retraining and incorporating lifestyle changes over a period of three months his uncontrolled seizures decreased to zero and is now seizure free. In the second example, a 39-year-old woman developed anxiety, insomnia, and panic attacks after her second kidney transplant probably due to shallow rapid breathing only in her chest. With biofeedback, she learned to change her breathing patterns from 25 breaths per minute without any abdominal movement to 8 breathes a minute with significant abdominal movement. Through generalization of the learned breathing skills, she was able to achieve control in situations where she normally felt out of control. As she practiced this skill her symptoms were significantly reduced and stated:
“What makes biofeedback so terrific in day-to-day situations is that I can do it at any time as long as I can concentrate. When I feel I can’t concentrate, I focus on counting and working with my diaphragm muscles; then my concentration returns. Because of the repetitive nature of biofeedback, my diaphragm muscles swing into action as soon as I started counting. When I first started, I had to focus on those muscles to get them to react. Getting in the car, I find myself starting these techniques almost immediately. Biofeedback training is wonderful because you learn techniques that can make challenging situations more manageable. For me, the best approach to any situation is to be calm and have peace of mind. I now have one more way to help me achieve this.” (From: Peper et al, 2001).
The commonality between these two participants was that neither realized that they were bracing the abdomen and were breathing rapidly and shallowly in the chest. I highly recommend that anyone who has experienced abdominal insults or surgery observe their breathing patterns and relearn effortless breathing/diaphragmatically breathing instead of shallow, rapid chest breathing often punctuated with breath holding and sighs.
It is important that medical practitioners and post-operative surgery patients recognize the common covert learned disuse patters such as shifting to shallow breathing to avoid pain. The sooner these patterns are identified and unlearned, the less likely will the person develop future iatrogenic illnesses. Biofeedback is an excellent tool to help identify and retrain these patterns and teach patients how to reestablish healthy/natural body patterns.
The full text of the article see: “Did You Ask About Abdominal Surgery or Injury? A Learned Disuse Risk Factor for Breathing Dysfunction,”
*Adapted from: Biofeedback Helps to Control Breathing Dysfunction.http://www.prweb.com/releases/2016/02/prweb13211732.htm
References
Burgio, K. L., Locher, J. L., Goode, P. S., Hardin, J. M., McDowell, B. J., Dombrowski, M., & Candib, D. (1998). Behavioral vs drug treatment for urge urinary incontinence in older women: a randomized controlled trial. Jama, 280(23), 1995-2000.
Dannecker, C., Wolf, V., Raab, R., Hepp, H., & Anthuber, C. (2005). EMG-biofeedback assisted pelvic floor muscle training is an effective therapy of stress urinary or mixed incontinence: a 7-year experience with 390 patients. Archives of Gynecology and Obstetrics, 273(2), 93-97.
Osar, E. (2016). http://www.fitnesseducationseminars.com/
Peper, E., Castillo, J., & Gibney, K. H. (2001, September). Breathing biofeedback to reduce side effects after a kidney transplant. In Applied Psychophysiology and Biofeedback (Vol. 26, No. 3, pp. 241-241). 233 Spring St., New York, NY 10013 USA: Kluwer Academic/Plenum Publ.
Peper, E., Gilbert, C.D., Harvey, R. & Lin, I-M. (2015). Did you ask about abdominal surgery or injury? A learned disuse risk factor for breathing dysfunction. Biofeedback. 34(4), 173-179. DOI: 10.5298/1081-5937-43.4.06
Taub, E., Uswatte, G., Mark, V. W., Morris, D. M. (2006). The learned nonuse phenomenon: Implications for rehabilitation. Europa Medicophysica, 42(3), 241-256.
Reduce hot flashes and premenstrual symptoms with breathing
Posted: February 18, 2015 Filed under: Breathing/respiration, Pain/discomfort, self-healing, stress management, Uncategorized | Tags: biofeedback, Breathing, diaphragmatic breathing, heart rate variability, hormone replacement therapy, hot flashes, HRT, Menopause, respiration, sighs, stress, sympathetic activity 6 CommentsAfter the first week to my astonishment, I have fewer hot flashes and they bother me less. Each time I feel the warmth coming, I breathe out slowly and gently. To my surprise they are less intense and are much less frequent. I keep breathing slowly throughout the day. This is quite a surprise because I was referred for biofeedback training because of headaches that occurred after getting a large electrical shock. After 5 sessions my headaches have decreased and I can control them, and my hot flashes have decreased from 3-4 per day to 1-2 per week. -50 year old client
After students in my Holistic Health class at San Francisco State University practiced slower diaphragmatic breathing and begun to change their dysfunctional shallow breathing, gasping, sighing, and breath holding to diaphragmatic breathing. A number of the older female students students reported that their hot flashes decreased. Some of the younger female students reported that their menstrual cramps and discomfort were reduced by 80 to 90% when they laid down and breathed slower and lower into their abdomen.
 The recent study in JAMA reported that many women continue to experience menopausal triggered hot flashes for up to 14 years. Although the article described the frequency and possible factors that were associated with the prolonged hot flashes, it did not offer helpful solutions.
The recent study in JAMA reported that many women continue to experience menopausal triggered hot flashes for up to 14 years. Although the article described the frequency and possible factors that were associated with the prolonged hot flashes, it did not offer helpful solutions.
Another understanding of the dynamics of hot flashes is that the decrease in estrogen accentuates the sympathetic/ parasympathetic imbalances that probably already existed. Then any increase in sympathetic activation can trigger a hot flash. In many cases the triggers are events and thoughts that trigger a stress response, emotional responses such as anger, anxiety, or worry, increase caffeine intake and especially shallow chest breathing punctuated with sighs. Approximately 80% of American women tend to breathe thoracically often punctuated with sighs and these women are more likely to experience hot flashes. On the other hand, the 20% of women who habitually breathe diaphragmatically tend to have fewer and less intense hot flashes and often go through menopause without any discomfort. In the superb study Drs. Freedman and Woodward (1992), taught women who experience hot flashes to breathe slowly and diaphragmatically which increased their heart rate variability as an indicator of sympathetic/parasympathetic balance and most importantly it reduced the the frequency and intensity of hot flashes by 50%.
Test the breathing connection if you experience hot flashes
Take a breath into your chest and rapidly exhale with a sigh. Repeat this quickly five times. In most cases, one minute later you will experience the beginning sensations of a hot flash. Similarly, when you practice slow diaphragmatic breathing throughout the day and interrupt every gasp, breath holding moment, sigh or shallow chest breathing with slower diaphragmatic breathing, you will experience a significant reduction in hot flashes.
Although this breathing approach has been well documented, many people are unaware of this simple behavioral approach unlike the common recommendation for the hormone replacement therapies (HRT) to ameliorate menopausal symptoms. This is not surprising since pharmaceutical companies spent nearly five billion dollars per year in direct to consumer advertising for drugs and very little money is spent on advertising behavioral treatments. There is no profit for pharmaceutical companies teaching effortless diaphragmatic breathing unlike prescribing HRTs. In addition, teaching and practicing diaphragmatic breathing takes skill training and practice time–time which is not reimbursable by third party payers.
For more information, research data and breathing skills to reduce hot flash intensity, see our article which is reprinted below.
Gibney, H.K. & Peper, E. (2003). Taking control: Strategies to reduce hot flashes and premenstrual mood swings. Biofeedback, 31(3), 20-24.
Taking control: Strategies to reduce hot flashes and premenstrual mood swings*
Erik Peper, Ph.D**., and Katherine H. Gibney
San Francisco State University
After the first week to my astonishment, I have fewer hot flashes and they bother me less. Each time I feel the warmth coming, I breathe out slowly and gently. To my surprise they are less intense and are much less frequent. I keep breathing slowly throughout the day. This is quite a surprise because I was referred for biofeedback training because of headaches that occurred after getting a large electrical shock. After 5 sessions my headaches have decreased and I can control them, and my hot flashes have decreased from 3-4 per day to 1-2 per week. -50 year old client
For the first time in years, I experienced control over my premenstrual mood swings. Each time I could feel myself reacting, I relaxed, did my autogenic training and breathing. I exhaled. It brought me back to center and calmness. -26 year old student
Abstract
Women have been troubled by hot flashes and premenstrual syndrome for ages. Hormone replacement therapy, historically the most common treatment for hot flashes, and other pharmacological approaches for pre-menstrual syndrome (PMS) appear now to be harmful and may not produce significant benefits. This paper reports on a model treatment approach based upon the early research of Freedman & Woodward to reduce hot flashes and PMS using biofeedback training of diaphragmatic breathing, relaxation, and respiratory sinus arrhythmia. Successful symptom reduction is contingent upon lowering sympathetic arousal utilizing slow breathing in response to stressors and somatic changes. We strongly recommend that effortless diaphragmatic breathing be taught as the first step to reduce hot flashes and PMS symptoms.
A long and uncomfortable history
Women have been troubled by hot flashes and premenstrual syndrome for ages. Hot flashes often result in red faces, sweating bodies, and noticeable and embarrassing discomfort. They come in the middle of meetings, in the middle of the night, and in the middle of romantic interludes. Premenstrual syndrome also arrives without notice, bringing such symptoms as severe mood swings, anger, crying, and depression.
Hormone replacement therapy (HRT) was the most common treatment for hot flashes for decades. However, recent randomized controlled trials show that the benefits of HRT are less than previously thought and the risks—especially of invasive breast cancer, coronary artery disease, dementia, stroke and venous thromboembolism—are greater (Humphries & Gill, 2003; Shumaker, et al, 2003; Wassertheil-Smoller, et al, 2003). In addition, there is no evidence of increased quality of life improvements (general health, vitality, mental health, depressive symptoms, or sexual satisfaction) as claimed for HRT (Hays et al, 2003).
“As a result of recent studies, we know that hormone therapy should not be used to prevent heart disease. These studies also report an increased risk of heart attack, stroke, breast cancer, blood clots, and dementia…” -Wyeth Pharmaceuticals (2003)
Because of the increased long-term risk and lack of benefit, many physicians are weaning women off HRT at a time when the largest population of maturing women in history (‘baby boomers’) is entering menopausal years. The desire to find a reliable remedy for hot flashes is on the front burner of many researchers’ minds, not to mention the minds of women suffering from these ‘uncontrollable’ power surges. Yet, many women are becoming increasingly leery of the view that menopause is an illness. There is a rising demand to find a natural remedy for this natural stage in women’s health and development.
For younger women a similar dilemma occurs when they seek treatment of discomfort associated with their menstrual cycle. Is premenstrual syndrome (PMS) just a natural variation in energy and mood levels? Or, are women expected to adapt to a masculine based environment that requires them to override the natural tendency to perform in rhythm with their own psychophysiological states? Instead of perceiving menstruation as a natural occurrence in which one has different moods and/or energy levels, women in our society are required to perform at the status quo, which may contribute to PMS. The feelings and mood changes are quickly labeled as pathology that can only be treated with medication.
Traditionally, premenstrual syndrome is treated with pharmaceuticals, such as birth control pills or Danazol. Although medications may alleviate some symptoms, many women experience unpleasant side effects, such as bloating or acne, and still experience a variety of PMS symptoms. Many cannot tolerate the medications. Thus, millions of women (and families) suffer monthly bouts of ‘uncontrollable’ PMS symptoms
For both hot flashes and PMS the biomedical model tends to frame the symptoms as a “structural biological problem.” Namely, the pathology occurs because the body is either lacking in, or has an excess of, some hormone. All that needs to be done is either augment or suppress hormones/symptoms with some form of drug. Recently, for example, medicine has turned to antidepressant medications to address menopausal hot flashes (Stearns, Beebe, Iyengar, & Dube, 2003).
The biomedical model, however, is only one perspective. The opposite perspective is that the dysfunction occurs because of how we use ourselves. Use in this sense means our thoughts, emotions and body patterns. As we use ourselves, we change our physiology and, thereby, may affect and slowly change the predisposing and maintaining factors that contribute to our dysfunction. By changing our use, we may reduce the constraints that limit the expression of the self-healing potential that is intrinsic in each person.
The intrinsic power of self-healing is easily observed when we cut our finger. Without the individual having to do anything, the small cut bleeds, clotting begin and tissue healing is activated. Obviously, we can interfere with the healing process, such as when we scrape the scab, rub dirt in the wound, reduce blood flow to the tissue or feel anxious or afraid. Conversely, cleaning the wound, increasing blood flow to the area, and feeling “safe” and relaxed can promote healing. Healing is a dynamic process in which both structure and use continuously affect each other. It is highly likely that menopausal hot flashes and PMS mood swings are equally an interaction of the biological structure (hormone levels) and the use factor (sympathetic/parasympathetic activation).
Uncontrollable or overly aroused?
Are the hot flashes and PMS mood swings really ‘uncontrollable?’ From a physiological perspective, hot flashes are increased by sympathetic arousal. When the sympathetic system is activated, whether by medication or by emotions, hot flashes increase and similarly, when sympathetic activity decreases hot flashes decrease. Equally, PMS, with its strong mood swings, is aggravated by sympathetic arousal. There are many self-management approaches that can be mastered to change and reduce sympathetic arousal, such as breathing, meditation, behavioral cognitive therapy, and relaxation.
Breathing patterns are closely associated with hot flashes. During sleep, a sigh generally occurs one minute before a hot flash as reported by Freedman and Woodward (1992). Women who habitually breathe thoracically (in the chest) report much more discomfort and hot flashes than women who habitually breathe diaphragmatically. Freedman, Woodward, Brown, Javaid, and Pandey (1995) and Freedman and Woodward (1992) found that hot flash rates during menopause decreased in women who practiced slower breathing for two weeks. In their studies, the control groups received alpha electroencephalographic feedback and did not benefit from a reduction of hot flashes. Those who received training in paced breathing reduced the frequency of their hot flashes by 50% when they practiced slower breathing. This data suggest that the slower breathing has a significant effect on the sympathetic and parasympathetic balance.
Women with PMS appear similarly able to reduce their discomfort. An early study utilizing Autogenic Training (AT) combined with an emphasis on warming the lower abdomen resulted in women noting improvement in dysfunctional bleeding (Luthe & Schultz, 1969, pp. 144-148). Using a similar approach, Mathew, Claghorn, Largen, and Dobbins (1979) and Dewit (1981) found that biofeedback temperature training was helpful in reducing PMS symptoms.. A later study by Goodale, Domar, and Benson (1990) found that women with severe PMS symptoms who practiced the relaxation response reported a 58% improvement in overall symptomatology as compared to a 27.2% improvement for the reading control group and a 17.0% improvement for the charting group.
Teaching control and achieving results
Teaching women to breathe effortlessly can lead to positive results and an enhanced sense of control. By effortless breathing, the authors refer to their approach to breath training, which involves a slow, comfortable respiration, larger volume of air exchange, and a reliance upon action of the muscles of the diaphragm rather than the chest (Peper, 1990). For more instructions see the recent blog, A breath of fresh air: Improve health with breathing.
Slowing breathing helps to limit the sighs common to rapid thoracic breathing—sighs that often precede menopausal hot flashes. Effortless breathing is associated with stress reduction—stress and mood swings are common concerns of women suffering from PMS. In a pilot study Bier, Kazarian, Peper, and Gibney (2003) at San Francisco State University (SFSU) observed that when the subject practiced diaphragmatic breathing throughout the month, combined with Autogenic Training, her premenstrual psychological symptoms (anger, depressed mood, crying) and premenstrual responses to stressors were significantly reduced as shown in Figure 1.
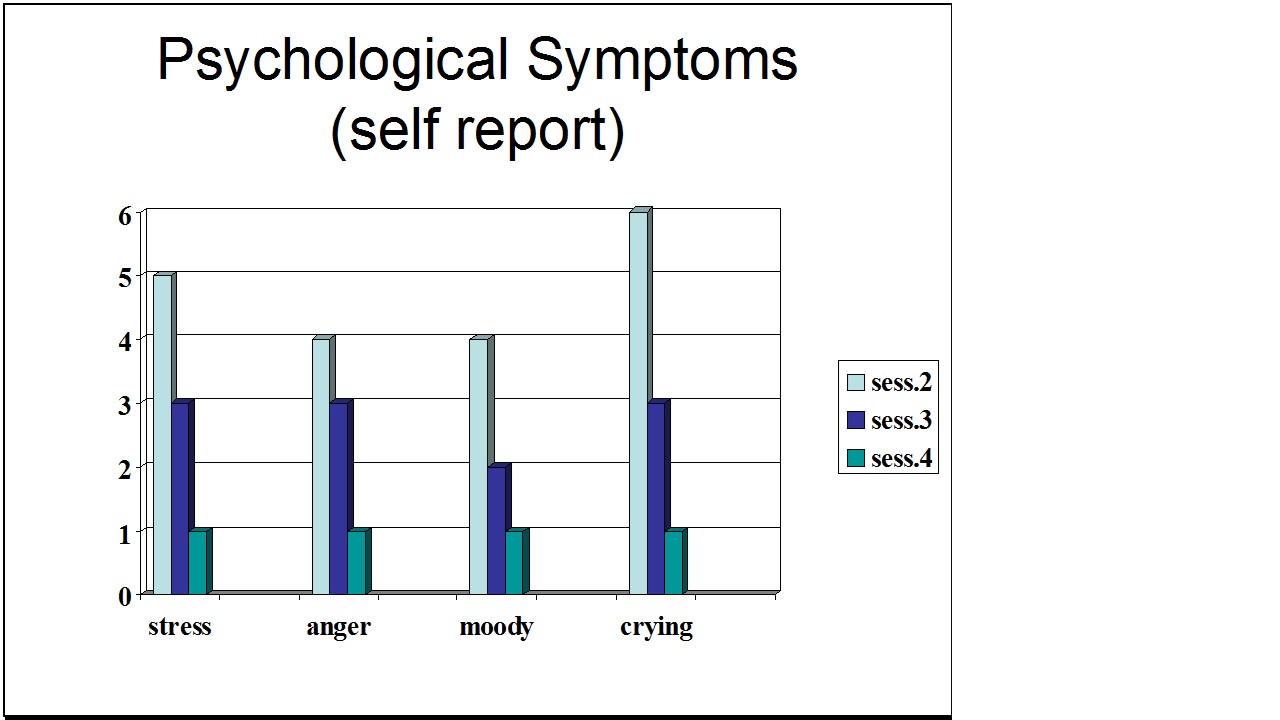
Figure 1. Student’s Individual Subjective Rating in Response to PMS Symptoms.
In another pilot study at SFSU, Frobish, Peper, and Gibney (2003) trained a volunteer who suffered from frequent hot flashes to breathe diaphragmatically. The training goals included modifying breathing patterns, producing a Respiratory Sinus Arrhythmia (RSA), and peripheral hand warming. RSA refers to a pattern of slow, regular breathing during which variations in heart rate enter into a synchrony with the respiration. Each inspiration is accompanied by an increase in heart rate, and each expiration is accompanied by a decrease in heart rate (with some phase differences depending on the rate of breathing). The presence of the RSA pattern is an indication of optimal balance between sympathetic and parasympathetic nervous activity.
During the 11-day study period, the subject charted the occurrence of hot flashes and noted a significant decrease by day 5. However, on the evening of day 7 she sprained her ankle and experienced a dramatic increase in hot flashes on day 8. Once the subject recognized her stress response, she focused more on breathing and was able to reduce the flashes as shown in Figure 2. 
Figure 2. Subjective rating of intensity, frequency and bothersomeness of hot flashes. The increase in hot flashes coincided with increased frustration about an ankle injury.
Our clinical experience confirms the SFSU pilot studies and the previously referenced research by Freedman and Woodward (1992) and Freedman et al. (1995). When arousal is lowered and breathing is effortless, women are better able to cope with stress and report a reduction in symptoms. Habitual rapid thoracic breathing tends to increase arousal while slower breathing, especially slower exhalation, tends to relax and reduce arousal. Learning and then applying effortless breathing reduces excessive sympathetic arousal. It also interrupts the cycle of cognitive activation, anxiety, and somatic arousal. The anticipation and frustration at having hot flashes becomes the cue to shift attention and “breathe slower and lower.” This process stops the cognitively mediated self-activation.
Successful self-regulation and the return to health begin with cognitive reframing: We are not only a genetic biological fixed (deficient) structure but also a dynamic changing system in which all parts (thoughts, emotions, behavior, diet, stress, and physiology) affect and are effected by each other. Within this dynamic changing system, there is an opportunity to implement and practice behaviors and life patterns that promote health.
Learning Diaphragmatic Breathing with and without Biofeedback
Although there are many strategies to modify respiration, biofeedback monitoring combined with respiration training is very useful as it provides real-time feedback. Chest and abdominal movement are recorded with strain gauges and heart rate can be monitored either by an electrocardiogram (EKG) or by a photoplethysmograph sensor on a finger or thumb. Peripheral temperature and electrodermal activity (EDA) biofeedback are also helpful in training. The training focuses on teaching effortless diaphragmatic breathing and encouraging the participant to practice many times during the day, especially when becoming aware of the first sensations of discomfort.
Learning and integrating effortless diaphragmatic breathing into daily life is one of the biofeedback strategies that has been successfully used as a primary or adjunctive/complementary tool for the reversal of disorders such as hypertension, migraine headaches, repetitive strain injury, pain, asthma and anxiety (Schwartz & Andrasik, 2003), as well as hot flashes and PMS.
The biofeedback monitoring provides the trainer with a valuable tool to:
- Observe & identify: Dysfunctional rapid thoracic breathing patterns, especially in response to stressors, are clearly displayed in real-time feedback.
- Demonstrate & train: The physiological feedback display helps the person see that she is breathing rapidly and shallowly in her chest with episodic sighs. Coaching with feedback helps her to change her breathing pattern to one that promotes a more balanced homeostasis.
- Motivate, persuade and change beliefs: The person observes her breathing patterns change concurrently with a felt shift in physiology, such as a decrease in irritability, or an increase in peripheral temperature, or a reduction in the incidence of hot flushes. Thus, she has a confirmation of the importance of breathing diaphragmatically.
In addition, we suggest exercises that integrate verbal and kinesthetic instructions, such as the following: “Exhale gently,” and “Breathe down your leg with a partner.”
Exhale Gently:
Imagine that you are holding a baby. Now with your shoulders relaxed, inhale gently so that your abdomen widens. Then as you exhale, purse your lips and very gently and softly blow over the baby’s hair. Allow your abdomen to narrow when exhaling. Blow so softly that the baby’s hair barely moves. At the same time, imagine that you can allow your breath to flow down and through your legs. Continue imagining that you are gently blowing on the baby’s hair while feeling your breath flowing down your legs. Keep blowing very softly and continuously.
Practice exhaling like this the moment that you feel any sensation associated with hot flashes or PMS symptoms. Smile sweetly as you exhale.
Breathe Down Your Legs with a Partner
Sit or lie comfortably with your feet a shoulder width apart. As you exhale softly whisper the sound “Haaaaa….” Or, very gently press your tongue to your pallet and exhale while making a very soft hissing sound.
Have your partner touch the side of your thighs. As you exhale have your partner stroke down your thighs to your feet and beyond, stroking in rhythm with your exhalation. Do not rush. Apply gentle pressure with the stroking. Do this for four or five breaths.
Now, continue breathing as you imagine your breath flowing through your legs and out your feet.
During the day remember the feeling of your breath flowing downward through your legs and out your feet as you exhale.
Learning Strategies in Biofeedback Assisted Breath Training
Common learning strategies that are associated with the more successful amelioration of hot flashes and PMS include:
- Master effortless diaphragmatic breathing, and concurrently increase respiratory sinus arrhythmia (RSA). Instead of breathing rapidly, such as at 18 breaths per minute, the person learns to breathe effortlessly and slowly (about 6 to 8 breaths per minute). This slower breathing and increased RSA is an indication of sympathetic-parasympathetic balance as shown in Figure 3.
- Practice slow effortless diaphragmatic breathing many times during the day and, especially in response to stressors.
- Use the physical or emotional sensations of a hot flash or mood alteration as the cue to exhale, let go of anxiety, breathe diaphragmatically and relax.
- Reframe thoughts by accepting the physiological processes of menstruation or menopause, and refocus the mind on positive thoughts, and breathing rhythmically.
- Change one’s lifestyle and allow personal schedules to flow in better balance with individual, dynamic energy levels.
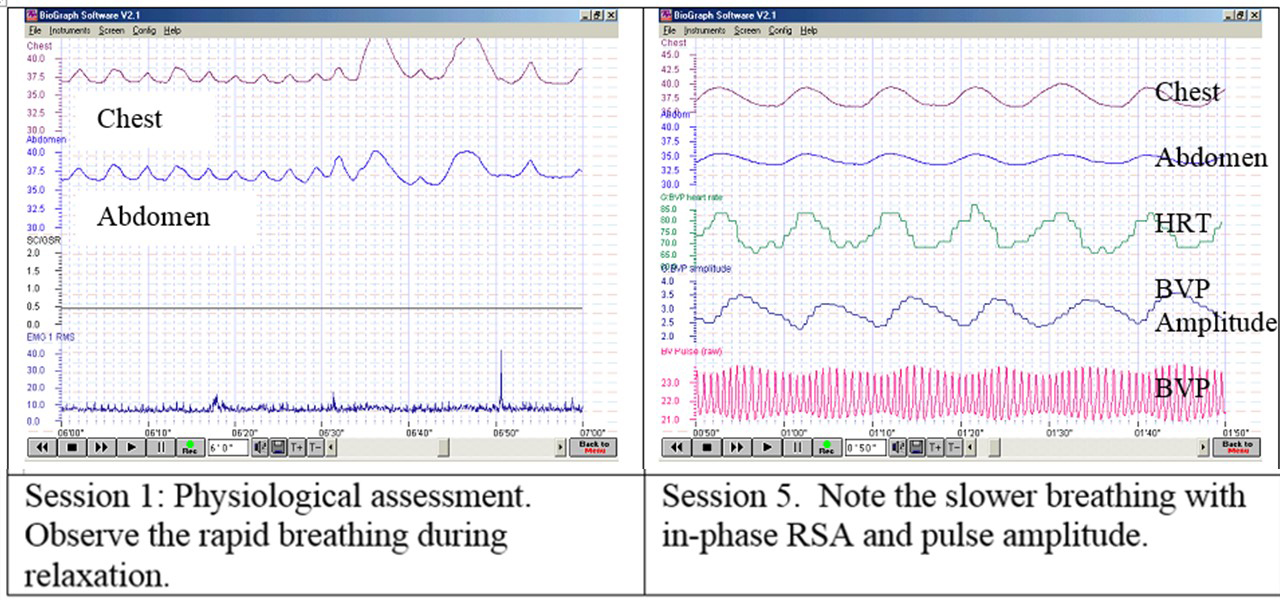 Figure 3. Physiological Recordings of a Participant with PMS. This subject learned effortless diaphragmatic breathing by the fifth session and experienced a significant decrease in symptoms.
Figure 3. Physiological Recordings of a Participant with PMS. This subject learned effortless diaphragmatic breathing by the fifth session and experienced a significant decrease in symptoms.
Generalizing skills and interrupting the pattern
The limits of self-regulation are unknown, often held back only by the practitioner’s and participant’s beliefs. Biofeedback is a powerful self-regulation tool for individuals to observe and modify their covert physiological reactions. Other skills that augment diaphragmatic breathing are Quieting Reflex (Stroebel, 1982), Autogenic Training (Schultz & Luthe, 1969), and mindfulness training (Kabat-Zinn, 1990). In all skill learning, generalization is a fundamental factor underlying successful training. Integrating the learned psychophysiological skills into daily life can significantly improve health—especially in anticipation of and response to stress. The anticipated stress can be a physical, cognitive or social trigger, or merely the felt onset of a symptom.
As the person learns and applies effortless breathing to daily activities, she becomes more aware of factors that affect her breathing. She also experiences an increased sense of control: She can now take action (a slow effortless breath) in moments when she previously felt powerless. The biofeedback-mastered skill interrupts the evoked frustrations and irritations associated with an embarrassing history of hot flashes or mood swings. Instead of continuing with the automatic self-talk, such as “Damn, I am getting hot, why doesn’t it just stop?” (language fueling sympathetic arousal), she can take a relaxing breath in response to the internal sensations, stop the escalating negative self-talk and allows more acceptance—a process reducing sympathetic arousal.
In summary, effortless breathing appears to be a non-invasive behavioral strategy to reduce hot flashes and PMS symptoms. Practicing effortless diaphragmatic breathing contributes to a sense of control, supports a healthier homeostasis, reduces symptoms, and avoids the negative drug side effects. We strongly recommend that effortless diaphragmatic breathing be taught as the first step to reduce hot flashes and PMS symptoms.
I feel so much cooler. I can’t believe that my hand temperature went up. I actually feel calmer and can’t even feel the threat of a hot flash. Maybe this breathing does work! –Menopausal patient after initial training in diaphragmatic breathing
References
Bier, M., Kazarian, D., Peper, E., & Gibney, K. (2003). Reducing the severity of PMS symptoms with diaphragmatic breathing, autogenic training and biofeedback. Unpublished report.
Freedman, R.R., & Woodward, S. (1992). Behavioral treatment of menopausal hot flushes: Evaluation by ambulatory monitoring. American Journal of Obstetrics and Gynecology, 167 (2), 436-439.
Freedman, R.R., Woodward, S., Brown, B., Javaid, J.I., & Pandey, G.N. (1995). Biochemical and thermoregulatory effects of behavioral treatment for menopausal hot flashes. Menopause: The Journal of the North American Menopause Society, 2 (4), 211-218.
Frobish,C., Peper, E. & Gibney, K. H. (2003). Menopausal Hot Flashes: A Self-Regulation Case Study. Poster presentation at the 35th Annual Meeting of the Association for Applied Psychophysiology and Biofeedback. Abstract in: Applied Psychophysiology and Biofeedback. 29 (4), 302.
Goodale, I.L., Domar, A.D., & Benson, H. (1990). Alleviation of Premenstrual Syndrome symptoms with the relaxation response. Obstetrics and Gynecological Journal, 75 (5), 649-55.
Hays, J., Ockene, J.K., Brunner, R.L., Kotchen, J.M., Manson, J.E., Patterson, R.E., Aragaki, A.K., Shumaker, S.A., Brzyski, R.G., LaCroix, A.Z., Granek, I.A, & Valanis, B.G., Women’s Health Initiative Investigators. (2003). Effects of estrogen plus progestin on health-related quality of life. New England Journal of Medicine, 348, 1839-1854.
Humphries, K.H.., & Gill, s. (2003). Risks and benefits of hormone replacement therapy: the evidence speaks. Canadian Medical Association Journal, 168(8), 1001-10.
Kabat-Zinn, J. (1990). Full catastrophe living. New York: Delacorte Press.
Luthe, W. & Schultz, J.H. (1969). Autogenic therapy: Vol II: Medical applications. New York: Grune & Stratton.
Mathew, R.J.; Claghorn, J.L.; Largen, J.W.; & Dobbins, K. (1979). Skin Temperature control for premenstrual tension syndrome:A pilot study. American Journal of Clinical Biofeedback, 2 (1), 7-10.
Peper, E. (1990). Breathing for health. Montreal: Thought Technology Ltd.
Schultz, J.H., & Luthe, W. (1969). Autogenic therapy: Vol 1. Autogenic methods. New York: Grune and Stratton.
Schwartz, M.S. & Andrasik, F.(2003). Biofeedback: A practitioner’s guide, 3nd edition. New York: Guilford Press.
Shumaker, S.A., Legault, C., Thal, L., Wallace, R.B., Ockene, J., Hendrix, S., Jones III, B., Assaf, A.R., Jackson, R. D., Morley Kotchen, J., Wassertheil-Smoller, S.; & Wactawski-Wende, J. (2003). Estrogen plus progestin and the incidence of dementia and mild cognitive impairment in post menopausal women: The Women’s Health Initiative memory study: A randomized controlled trial. Journal of the American Medical Association, 289 (20), 2651-2662.
Stearns, V., Beebe, K. L., Iyengar, M., & Dube, E. (2003). Paroxetine controlled release in the treatment of menopausal hot flashes. Journal of the American Medical Association, 289 (21), 2827-2834.
Stroebel, C. F. (1982). QR, the quieting reflex. New York: G. P. Putnam’s Sons.
van Dixhoorn, J.J. (1998). Ontspanningsinstructie Principes en Oefeningen (Respiration instructions: Principles and exercises). Maarssen, Netherlands: Elsevier/Bunge.
Wassertheil-Smoller, S., Hendrix, S., Limacher, M., Heiss, G., Kooperberg, C., Baird, A., Kotchen, T., Curb, Dv., Black, H., Rossouw, J.E., Aragaki, A., Safford, M., Stein, E., Laowattana, S., & Mysiw, W.J. (2003). Effect of estrogen plus progestin on stroke in postmenopausal women: The Women’s Health Initiative: A randomized trial. Journal of the American Medical Association, 289 (20), 2673-2684.
Wyeth Pharmaceuticals (2003, June 4). A message from Wyeth: Recent reports on hormone therapy and where we stand today. San Francisco Chronicle, A11.
*We thank Candy Frobish, Mary Bier and Dalainya Kazarian for their helpful contributions to this research.
**For communications contact: Erik Peper, Ph.D., Institute for Holistic Healing Studies, San Francisco State University, 1600 Holloway Avenue, San Francisco, CA 94132; Tel: (415) 338 7683; Email: epeper@sfsu.edu; website: http://www.biofeedbackhealth.org; blog: http://www.peperperspective.come
