Hope for abdominal discomfort
Posted: June 21, 2022 Filed under: behavior, biofeedback, Breathing/respiration, emotions, Evolutionary perspective, healing, health, Pain/discomfort | Tags: functional abdominal pain, heart rate variability, HRV, IBS, irritable bowel syndrome, neurasthenia, Rap, recurrent abdominal pain, respiration 3 CommentsAdapted from: Peper, E. & Harvey, R. (2022). Nausea and GI discomfort: A biofeedback assessment model to create a rational for training. Biofeedback, 50(1), 24–32. https://doi.org/10.5298/1081-5937-50.1.05
Abdominal discomfort and pain such as functional abdominal pain, acid reflux or irritable bowel affects many people. Teaching slower biofeedback-assisted HRV breathing with biofeedback is a useful strategy by which the person may be able to reduce symptoms. This essay provides detailed instruction for a first session assessment for clients who have abdominal discomfort (functional abdominal pain). Descriptions include how the physiological recording can be used to understand a possible etiology of the illness, to create a biological/evolutionary based explanation that is readily understood by the client, and finally to offer self-regulation suggestions to improve health.
Background of abdominal discomfort (irritable bowel syndrome, acid reflux, functional abdominal pain, recurrent abdominal pain)
Irritable bowel syndrome (IBS) affects 7% to 21% of the general population in Western cultures with a global prevalence estimated at around 11% (Fairbrass, Costantino, Gracie, & Ford, 2020). The chronic symptoms (i.e., lasting more than 30 days) usually include abdominal cramping, discomfort or pain, bloating, loose or frequent stools and constipation, which can significantly reduce the quality of life (Chey et al., 2015). A precursor of IBS in children is called recurrent abdominal pain (RAP), which affects 0.3% to 19% of school children (Chitkara et al., 2005). Both IBS and RAP appear to be functional illnesses, as no organic causes have been identified to explain the symptoms. IBS and RAP are contrasted to various types of diseases such as Crohn’s disease, inflammatory bowel disease or ulcerative colitis.
Multiple factors may contribute to IBS, such as genetics, food allergies, previous treatment with antibiotics, infections, psychological status and stress. More recently, dietary factors contributing to changes in the intestinal and colonic microbiome resulting in small intestine bacterial overgrowth have been suggested as another risk factor (Dupont, 2014). Generally, standard medical treatments (reassurance, dietary manipulation and of pharmacological therapy) are often ineffective in reducing IBS symptoms (Chey et al., 2015). On the other hand, complementary and alternative approaches such as biofeedback-assisted relaxation techniques (Davidoff & Whitehead, 1996; Goldenberg et al., 2019; Stern et al. 2014), autogenic training (Luthe & Schultz, 1969) and cognitive therapy are more effective than traditional medical treatment (Vlieger et al., 2008).
Biofeedback-assisted relaxation training typically moderates IBS or RAP symptoms by restoring balance in the nervous system (sympathetic/parasympathetic autonomic balance), such as through heart rate variability (HRV) breathing training. For example, Sowder et al. (2010) as well as Sun et al. (2016) demonstrated that functional abdominal pain can be reduced with HRV feedback training. In most cases, increased vagal tone was achieved by breathing at about six breaths per minute. While Taneja et al. (2004) reported that yogic breathing decreased diarrhea-predominant irritable bowel syndrome symptoms significantly more than conventional treatment in a randomized control study.Sympathetic/parasympathetic balance can be enhanced by increasing HRV, which occurs when a person breathes at their resonant frequency, which is usually 5–7 breaths per minute. For most people, the HRV training means breathing at much slower rate. A benefit of slow abdominal breathing appears to be a self-control strategy that can reduce symptoms of IBS, RAP and similar functional abdominal pain symptoms.
Mastery of effortless diaphragmatic breathing can be affected by injury, surgery or similar insults to the abdominal area (Peper et al., 2015). In addition, dysregulation of diaphragm, which is enervated by the phrenic nerve and the vagus nerve, along with dysregulation of other abdominal muscles appears to be associated with irritable bowel syndrome (Bordoni & Morabito, 2018). It is likely that slower biofeedback-assisted HRV breathing training restores abdominal muscles and diaphragmatic movement, theoretically by tonic and phasic regulation of the phrenic and vagal nerve activity (cf. Marchenko et al., 2015; Streeter et al., 2012). The theory, simply stated, is that HRV breathing training at an individual’s resonant frequency produces increases in regulatory neurotransmitters, particularly gamma amino butyric acid (GABA). Many of our students who complain of abdominal discomfort report reductions of symptoms following HRV breathing training.
Consistently for more than 40 years, we have taught undergraduate students a semester-long integrated stress management program that includes modified progressive relaxation, slow diaphragmatic breathing and changing internal language as outlined in the book, Make Health Happen, by Peper, Gibney & Holt (2002). At the end of each semester, numerous students report that their anxiety, gastrointestinal distress and other symptoms related to self-described IBS or RAP have decreased or disappeared (Peper et al., 2014; Peper, Miceli, & Harvey, 2016; Peper, Mason, Huey, 2017; Peper et al., 2020). Abdominal discomfort is prevalent experience of distress by college students. In our recent survey of 99 undergraduate students, 41% self-reported abdominal discomfort (25% irritable bowel or acid reflux), 86% self-reported anxiety, 70% neck and shoulder tension and 48% headaches. After practicing slower breathing (i.e., typically directing them to breath abdominally at a rate of about six breaths a minute) and focus on slower exhalation and allowing the air to flow in without effort as the abdominal wall expands, as a homework assignment for a week, many reported that their symptoms significantly decreased (Peper, Harvey, Cuellar, & Membrila, in press).
Case example illustrating how to use the physiological recording to guide the client discussion and provide motivation
A 16-year-old high school junior suffered from abdomen discomfort for years. The symptoms mainly consisted of frequent constipation, and when it occurred, great discomfort from nausea. After having been diagnosed and undergoing all the necessary tests by the gastroenterologist, there was no identifiable cause of the chief complaints. Biofeedback was suggested as an alternative to medications for symptom reduction. During the biofeedback assessment and training session, the client discussed what she would like to learn from the session. It was challenging for her to respond to those questions. Not being able to report what the client would like from a training session is also a very common experience when working with students. A useful strategy is to describe experiences of other students that the clients could relate to, and imply that their abdominal discomfort is somewhat commonplace in other students.
Discussed during the session was the link between being very sensitive and reactive to other people’s feeling and being concerned about what others think of her. The client nodded her head in agreement. When describing herself, she discussed being very perfectionistic using a scale from being lackadaisical/undemanding to being perfectionistic (i.e., self-oriented perfectionism, self-worth contingencies, concern over mistakes, doubts about actions, self-criticism, socially prescribed perfectionism, other-oriented perfectionism, hypercriticism; see Smith, Saklofske, Stoeber, & Sherry, 2016).
Furthermore, the client sat slouched in the chair. Possibly her slouched posture implied a state of powerlessness instead of empowerment, a state of being ready to react and protect (Carney, Cuddy, & Yap, 2010; Cuddy, 2012; Peper, Lin, & Harvey, 2017).
Working hypotheses. The client was very sensitive and continuously reacted to external and internal signals with sympathetic arousal, while masking her reactions. These ongoing flight/flight responses would decrease intestinal peristalsis and abdominal blood flow, which would result in nausea, constipation and abdominal distress. Namely, the body reacts to the stimuli as signals of danger and blood flow is shunted away from the abdomen into the large muscles to run and fight. To paraphrase Stanford University professor Robert Sapolsky (2004): Why should the body digest food and repair itself, if it is going to be the predator’s lunch? It is only when we are safe that we can digest and regenerate.
The session began by exploring how pressure on the abdomen could potentially affect experiences of nausea and abdominal distress. After explaining how the diaphragm descends and how abdominal content in the stomach can be displaced (spread out) during inhalation, we systematically changed her posture by placing and adjusting a small pillow behind her middle back so that she could sit tall. The tall posture resulted in an open feeling of empowerment not felt during slouching. She observed that breathing was slightly easier and felt there was more space in her abdomen. As she began to feel more comfortable during the training session, we discussed the impact of posture on the body. We also discussed the relationship between thoughts of perfectionism and abdominal discomfort. The discussion also included an exploration of why some people tend to curl-up and slouch in a protective posture (e.g., head down to protect the neck region and big bones of the arms and legs positioned to protect the core organs) when feeling self-consciousness or perfectionistic about body image.
Biofeedback monitoring for assessment
Psychophysiology was recorded with multichannel physiological system (Procomp Infinity System running Biograph Infinity software version 6.7.1, Thought Technology Ltd). Respiration was monitored with strain-gauge sensors placed around the abdomen and thoracic regions (for a discussion on sensor placement see Peper et al., 2016 and Chu et al., 2019). Blood volume pulse was recorded with the sensor placed on the left thumb. The thumb was used because the participant had small and cold fingers (for a discussion about blood volume pulse, see Peper et al, 2007 and Peper, Shafer, & Lin, 2010). Skin conductance was recorded with the sensor wrapped around the left index and middle fingers with the electrodes on the finger pads (for a discussion about skin conductance and normal values, see Khazan, 2019, and Shafer et al, 2016).
After sensors were attached and the signals explained, the client sat comfortably while looking at the screen. Unexpectedly the clinician clapped his hands and made a loud noise. The client reacted with a momentary startle and smile. The physiological response, showed an increase in skin conductance, decrease in pulse amplitude, decrease in abdominal diameter, and increase in heart rate, is shown in Figure 1.

Figure 1. Physiological response to a loud noise (clap) (1) increased skin conductance, (2) decrease in pulse amplitude, (3) decrease in decreased abdominal circumference, and (4) increased heart rate and decreased heart rate variability.
The client was aware that she reacted to the clap; however, she was totally unaware how much her body responded. The computer screen display of her physiological reaction made the invisible visible. It provided the opportunity to discuss how various body reactions related to heart rate, breathing, and skin conductance could contribute to experiences of abdominal discomfort.
She was unaware that skin conductance did not return to baseline levels for more than 20 minutes. An elevated skin conductance level may mean that the body’s reaction to the hand-clap noise triggered a defense reaction and maintained the increased sympathetic activity for more than 20 minutes. Having a sustained flight/fight reaction to external stimuli such as a hand-clap would most likely affect digestive and peristalsis processes, contributing to symptoms found in IBS and RAP. The observations made during biofeedback monitoring led to a discussion of how sympathetic activation affects the gastrointestinal track.
Blood volume pulse amplitude decreased, which indicated a decrease in blood flow through her hands, which would decrease hand temperature and again indicated a systemic sympathetic activation.
Abdominal circumference decreased, which indicated that she tightened her abdominal muscles as a protective response to the hand-clap. She was unaware of the abdominal muscles tightening; however, she stated that she was aware that her breathing had changed. The abdominal muscle, which pulled the abdomen in, took almost two minutes to relax. The sustained muscle constriction around the abdomen increased pressure around the core organs, which may contribute to ongoing abdominal discomfort. A fight-flight reaction includes body bracing (e.g. tightened muscles, head down to protect the neck, big bones of arms and legs curled to protect core organs), and she confirmed that she experienced neck and shoulder tensions.
The discussion of abdominal muscle tension led to another discussion of how holding your stomach in may relate to self-image. For example, tight clothing can contribute to constricted movement around the abdomen. Wearing corsets contributed to psychophysiological symptoms, mainly for women in the late 19th and early 20th centuries, during a time when women who wore very tight corsets were diagnosed with neurasthenia. Simply stated, neurasthenia was characterized as a condition of mental and/or physical fatigue with at least two of the following symptoms: dyspepsia, dizziness, muscular aches or pains, tension headaches, inability to relax, irritability and sleep disturbance.
“Dyspepsia” was the commonly reported symptom of neurasthenia, which included upset stomach, a gnawing or burning stomach pain, heartburn, bloating, and or burping, nausea, and vomiting. The constricted waist region that resulted from wearing a corset in the name of fashion compromises the functions of both digestion and breathing. When the person inhales, the abdomen cannot expand as the diaphragm is flattening and pushing downward. Thus, the person is forced to breathe more shallowly by lifting their ribs; this increases neck and shoulder tension as well as the risk of anxiety, heart palpitation, and fatigue (Cohen & White, 1947; Courtney, 2009).
It also can contribute to abdominal discomfort since the abdomen is being squeezed by the corset and forcing the abdominal organs upward. Even architects of the Victorian era recognized a need for a place to position a chair or chaise lounge, such as at the top of some stairs, because people wearing corsets could faint, pass out or otherwise experience breathlessness through the effort of climbing the stairs with restrictive clothing around their abdomen (Melissa, 2015). Many of these symptoms could be easily reduced by wearing looser clothing and learning slower diaphragmatic breathing. In modern times, a related phenomenon results when people wear items of clothing that are too tight around their waist or abdomen (e.g., tight jeans) in service to fashion trends often labeled as designer jean syndrome (MacHose & Peper, 1991; Stonehewer, 2009). Similarly, when people wear garments that are too tight around their chest or thoracic region (e.g., tight vests) in service to external protection (e.g., athletes, industrial workers, police or soldiers wearing heavy, restrictive gear), then restrictive ventilatory disorders can occur (Harty et al., 1999). Simply stated, when the muscles related to breathing are restricted from moving, respiration is affected.
The client’s heart rate increased and stayed high for more than 30 seconds. The first decrease in heart rate at about 20 seconds after the hand-clap was a long sigh of relief as breathing (i.e., oxygen/carbon dioxide exchange) started again. It took almost 90 seconds before breathing and heart rate returned to normal as reflected by measures of HRV. The computer screen showing increased heart rate was reviewed with the client to explain how her body reacted with a fight-flight response to the hand-clap, as well as how regulating breathing through biofeedback training could lower the heart rate and reduce the sympathetic activation and enhance the parasympathetic activation.
Body responds to cognitive stressful thoughts
After discussion about the psychophysiological response to the hand-clap (a physical external stressor) and how other external stressors (e.g., startling noise) or internal stressors (e.g., perfectionistic ruminations) could trigger a similar response of abdominal muscle tightening, the assessment was repeated by having her relax and then think about a mental stressor, as shown in Figure 2.

Figure 2. Physiological responses to thinking about a past stressor (1) increased skin conductance, (2) decreased pulse amplitude, (3) decreased abdominal circumference, and (4) increased heart rate and decreased HRV.
The physiological response pattern to thinking about a past stressor was similar to the bodily reaction to a loud noise. The skin conductance increased and blood volume pulse amplitude decreased immediately after hearing (e.g., anticipating) the task of evoking/thinking of a past stressor. Most likely, the initial response was triggered by performance anxiety, then 6 seconds later the heart rate increased and breathing changed as she began experiencing the somatic reaction evoked by the recall of a negative stressor. The recordings also showed that her pulse amplitude decreased. The decrease in pulse amplitude suggested that her hands would probably become colder, which was confirmed by her self-report that she often experienced cold hands and feet. She reported being aware of the feeling an emotional reaction, but mainly noticing the change of breathing in her chest, and she was unaware of the abdominal changes. The client was surprised by how her body reacted to emotional thoughts. The recording viewed on the computer screen demonstrated objectively that her thoughts (initial performance anxiety) had a physical effect on her body. Specifically, experiencing the emotions that were evoked by recalling the stressful memory had a direct effect on the body in the same way that a physical external threat leads to a fight-flight response.
Building a psychophysiological model
Using these recorded computer images reflecting physical reactions to the hand clap and emotional thoughts, the discussion focused on how abdominal discomfort could be the result of activating a normal biological survival response. Survival responses would occur hundreds of times throughout a day, especially when worrying. Each thought would evoke the response, and the awareness of body reaction would evoke another reaction. Similar to how awareness of blushing amplifies blushing.
The client shared that she was very sensitive and reactive especially when other people were upset. She reported feeling “cursed” by their sensitivity and reactivity. The linguistic metaphor that could be used to describe her reactions is “she could not stomach what was going on.”
The discussion about physiological reactions provided the client with a model how her disorder (IBS and RAP) could have developed and been maintained over the years. The model matched her subjective experience: when stressed, the discomfort often increased. The discussion shifted to reframing her internal labels. Instead of describing her sensitivity as a curse, the sensitivity was reframed and labeled a gift; namely, she could sense many people’s emotional reactions, to which they would react in a variety of ways. She just needed to learn how to manage this sensitivity. Once she learned to manage it, she would have many advantages in interpersonal relations at home and at work. She would be able to sense what other people are experiencing. By reframing her symptoms as a result of a survival physiological response pattern, it reduces self- blame and offers solutions about how to master and change reactions and thereby have more control in the world.
Training to demonstrate control is possible.
The discussion was followed by teaching her diaphragmatic breathing in sitting and lying down positions. As she had no history of abdominal injuries, similar to many of our students, she rapidly demonstrated slower diaphragmatic breathing as shown in Figures 3 and 4.

Figure 3. The client practiced a few slower diaphragmatic breaths in the sitting and reclining position, which increased heart rate variability, decreased skin conductance and increased blood volume pulse amplitude.

Figure 4. Practicing slower diaphragmatic breathing at about six breaths per minute in a reclining position increased HRV.
With tactile coaching, she demonstrated that she could breathe at about six breaths per minute with the heart rate increasing during inhalation and decreasing during exhalation. She reported feeling more relaxed and that the sensations of nausea had disappeared. Additionally, her hands felt warmer. This recording provided proof that there was hope and that she could do something about her body’s psychophysiological responses.
The discussion focused on how breathing affecting heart rate variability. Namely, if she allowed exhalation to occur without effort, her heart rate decreased (the vagal response of slowing the heart) and thereby increased the parasympathetic activation that would support digestion and gastrointestinal functioning. Often when people practice effortless diaphragmatic breathing, abdominal noises (borborygmus)– the gurgling, rumbling, or squeaking noise from the abdomen–occur and indicate that intestinal activity is being activated, and that food, liquids and digestive juice are moving through the intestines. It is usually a positive indicator that the person is relaxing and sympathetic activity has been reduced.
During the last part of session, we reviewed how posture affects physiology, emotions and cognitions, as well as how posture and breathing would be the first step in beginning to reduce symptoms and enhance health. To provide additional information using video and bibliotherapy/education, we suggested that she watches the embedded videos in the blogs listed at the end of the article.
Recommendations for future sessions and home practice
The recommended strategies for future sessions would focus on teaching the client to master slow diaphragmatic breathing and practicing that for 10–20 minutes per day. The teaching techniques would incorporate imagery to imagine air flowing down their arms and legs as she exhaled. . More importantly, the focus would shift to generalize the skill during the day; namely, whenever she would become aware of feeling stressed or observed herself holding her breath or breathing in her chest, she would use that as the cue to shift to slower abdominal breathing. Had the client continued training, future sessions would focus on mastering slower diaphragmatic breathing. The training would include relaxing the lower abdominal muscles during inhalation, increasing control of HRV, practicing imagining stress and use image to trigger slower breathing, and cognitive reframing practices to interrupt worrying and promote self-acceptance. The final goal is to generalize these skills into daily life as illustrated in the successful cases described in the following blogs
Blogs on posture:
References
Bordoni, B. & Morabito, B. (2018). Symptomatology correlations between the diaphragm and irritable bowel syndrome. Cureus, 10(7), e3036. https://doi.org/10.7759/cureus.3036
Carney, D. R., Cuddy, A. J., & Yap, A. J. (2010). Power posing: brief nonverbal displays affect neuroendocrine levels and risk tolerance. Psychological Science, 10, 1363-1368. https://dx.doi.org/10.1177/0956797610383437
Chey, W. D., Kurlander, J., & Eswaran, S. (2015). Irritable bowel syndrome: a clinical review. Jama, 313(9), 949–958. https://doi.org/10.1001/jama.2015.0954
Chitkara, D. K., Rawat, D. J., & Talley, N. J. (2005). The epidemiology of childhood recurrent abdominal pain in Western countries: a systematic review. American journal of Gastroenterology, 100(8), 1868–1875. https://doi.org/10.1111/j.1572-0241.2005.41893.x
Chu, M., Nguyen, T., Pandey, V., Zhou, Y., Pham, H. N., Bar-Yoseph, R., Radom-Aizik, S., Jain, R., Cooper, D. M., & Khine, M. (2019). Respiration rate and volume measurements using wearable strain sensors. NPJ digital medicine, 2(1), 1–9. https://doi.org/10.1038/s41746-019-0083-3
Cohen, M. E. & White, P. D. (1947). Studies of breathing, pulmonary ventilation and subjective awareness of shortness of breath (dyspnea) in neurocirculatory asthenia, effort syndrome, anxiety neurosis. Journal of Clinical Investigation, 26(3), 520–529. https://doi.org/10.1172/JCI101836
Courtney, R. (2009). The functions of breathing and its dysfunctions and their relationship to breathing therapy. International Journal of Osteopathic Medicine, 12, 78–85. https://doi.org/10.1016/j.ijosm.2009.04.002
Cuddy, A. (2012). Your body language shapes who you are. Technology, Entertainment, and Design (TED) Talk, available at: http://www.ted.com/talks/amy_cuddy_your_body_language_shapes_who_you_are
Davidoff, A. L., & Whitehead, W. E. (1996). Biofeedback, relaxation training, and cognitive behavior modification: Treatments for functional GI disorders, In Olden, K, W. (ed). Handbook of Functional Gastrointestinal Disorders. CRC Press, 361–384.
Dupont, H. L. (2014). Review article: evidence for the role of gut microbiota in irritable bowel syndrome and its potential influence on therapeutic targets. Alimentary Pharmacology & Therapeutics, 39(10), 1033–1042. https://doi.org/10.1111/apt.12728
Fairbrass, K. M., Costantino, S. J., Gracie, D. J., & Ford, A. C. (2020). Prevalence of irritable bowel syndrome-type symptoms in patients with inflammatory bowel disease in remission: a systematic review and meta-analysis. The Lancet Gastroenterology & Hepatology, 5(12), 1053–162. https://doi.org/10.1016/s2468-1253(20)30300-9
Goldenberg, J. Z., Brignall, M., Hamilton, M., Beardsley, J., Batson, R. D., Hawrelak, J., Lichtenstein, B., & Johnston, B. C. (2019). Biofeedback for treatment of irritable bowel syndrome. Cochrane Database of Systematic Reviews, (11). https://doi.org/10.1002/14651858.CD012530.pub2
Harty, H. R., Corfield, D. R., Schwartzstein, R. M., & Adams, L. (1999). External thoracic restriction, respiratory sensation, and ventilation during exercise in men. Journal of Applied Physiology, 86(4), 1142–1150. https://doi.org/10.1152/jappl.1999.86.4.1142
Khazan, I. (2019). A guide to normal values for biofeedback. Biofeedback, 47(1), 2–5. https://doi.org/10.5298/1081-5937-47.1.03
Luthe, W. & Schultz, J. H. (1969). Autogenic Therapy Volume II: Medical Applications. Grune & Stratton.
MacHose, M., & Peper, E. (1991). The effect of clothing on inhalation volume. Biofeedback and Self-Regulation, 16(3), 261–265. https://doi.org/10.1007/BF01000020
Marchenko, V., Ghali, M. G., & Rogers, R. F. (2015). The role of spinal GABAergic circuits in the control of phrenic nerve motor output. American Journal of Physiology-Regulatory, Integrative and Comparative Physiology, 308(11), R916–R926. https://doi.org/10.1152/ajpregu.00244.2014
Melissa. (2015). Why women fainted so much in the 19th century. May 20, 2015. Downloaded October 2, 2021. http://www.todayifoundout.com/index.php/2015/05/women-fainted-much-19th-century/
Peper, E., Gibney, K. H., & Holt, C. F. (2002). Make Health Happen—Training Yourself to Create Wellness. Kendall/Hunt Publishing Company.
Peper, E., Gilbert, C. D., Harvey, R. & Lin, I-M. (2015). Did you ask about abdominal surgery or injury? A learned disuse risk factor for breathing dysfunction. Biofeedback. 34(4), 173–179. https://doi.org/10.5298/1081-5937-43.4.06
Peper, E., Groshans, G. H., Johnston, J., Harvey, R., & Shaffer, F. (2016). Calibrating respiratory strain gauges: What the numbers mean for monitoring respiration. Biofeedback, 44(2), 101–105. https://doi.org/10.5298/1081-5937-44.2.06
Peper, E., Harvey, R., Cuellar, Y., & Membrila, C.(in press). Reduce anxiety. NeuroRegulation.
Peper, E., Harvey, R., Lin, I. M., Tylova, H., & Moss, D. (2007). Is there more to blood volume pulse than heart rate variability, respiratory sinus arrhythmia, and cardiorespiratory synchrony? Biofeedback, 35(2), 54–61. https://www.researchgate.net/publication/259560204_Is_There_More_to_Blood_Volume_Pulse_Than_Heart_Rate_Variability_Respiratory_Sinus_Arrhythmia_and_Cardiorespiratory_Synchrony
Peper, E., Lin, I-M, & Harvey, R. (2017). Posture and mood: Implications and applications to therapy. Biofeedback, 35(2), 42–48. https://doi.org/10.5298/1081-5937-45.2.03
Peper, E., Lin, I-M, Harvey, R., Gilbert, M., Gubbala, P., Ratkovich, A., & Fletcher, F. (2014). Transforming chained behaviors: Case studies of overcoming smoking, eczema and hair pulling (trichotillomania). Biofeedback, 42(4), 154–160. https://doi.org/10.5298/1081-5937-42.4.06
Peper, E., Mason, L., Harvey, R., Wolski, L, & Torres, J. (2020). Can acid reflux be reduced by breathing? Townsend Letters-The Examiner of Alternative Medicine, 445/446, 44–47. https://www.townsendletter.com/article/445-6-acid-reflux-reduced-by-breathing/
Peper, E., Mason, L., Huey, C. (2017). Healing irritable bowel syndrome with diaphragmatic breathing. Biofeedback, 45(4), 83–87. https://doi.org/10.5298/1081-5937-45.4.04
Peper, E., Miceli, B., & Harvey, R. (2016). Educational model for self-healing: Eliminating a chronic migraine with electromyography, autogenic training, posture, and mindfulness. Biofeedback, 44(3), 130–137. https://www.aapb.org/files/publications/biofeedback/2016/biof-44-03-130-137.pdf
Peper, E., Shaffer, F., & Lin, I. M. (2010). Garbage in; Garbage out—Identify blood volume pulse (BVP) artifacts before analyzing and interpreting BVP, blood volume pulse amplitude, and heart rate/respiratory sinus arrhythmia data. Biofeedback, 38(1), 19–23. https://doi.org/10.5298/1081-5937-38.1.19
Sapolsky, R. (2004). Why Zebras Don’t Get Ulcers. Owl Books ISBN: 978-0805073690
Shaffer, F., Combatalade, D., Peper, E., & Meehan, Z. M. (2016). A guide to cleaner electrodermal activity measurements. Biofeedback, 44( 2), 90–100. https://doi.org/10.5298/1081-5937-44.2.01
Smith, M. M., Saklofske, D. H., Stoeber, J., & Sherry, S. B. (2016). The big three perfectionism scale: A new measure of perfectionism. Journal of Psychoeducational Assessment, 34(7), 670–687. https://doi.org/10.1177/0734282916651539
Sowder, E., Gevirtz, R., Shapiro, W., & Ebert, C. (2010). Restoration of vagal tone: a possible mechanism for functional abdominal pain. Applied Psychophysiology and Biofeedback, 35(3), 199–206. https://doi.org/10.1007/s10484-010-9128-8
Stern, M. J., Guiles, R. A., & Gevirtz, R. (2014). HRV biofeedback for pediatric irritable bowel syndrome and functional abdominal pain: A clinical replication series. Applied Psychophysiology and Biofeedback, 39(3), 287–291. https://doi.org/10.1007/s10484-014-9261-x
Stonehewer, L. (2009). Dysfunctional breathing for women’s health physiotherapists. Journal of the Association of Chartered Physiotherapists in Women’s Health, 104, 38–40. https://pogp.csp.org.uk/system/files/stonehewer_hr.pdf
Streeter, C. C., Gerbarg, P. L., Saper, R. B., Ciraulo, D. A., & Brown, R. P. (2012). Effects of yoga on the autonomic nervous system, gamma-aminobutyric-acid, and allostasis in epilepsy, depression, and post-traumatic stress disorder. Medical hypotheses, 78(5), 571–579. https://doi.org/10.1016/j.mehy.2012.01.021
Sun, X., Shang, W., Wang, Z., Liu, X., Fang, X., & Ke, M. (2016). Short-term and long-term effect of diaphragm biofeedback training in gastroesophageal reflux disease: An open-label, pilot, randomized trial. Diseases of the Esophagus, 29(7), 829–836. https://doi.org/10.1111/dote.12390
Taneja. I., Deepak, K.K., Poojary, G., Acharya, I.N., Pandey, R.M., & Sharma, M.P. (2004). Yogic versus conventional treatment in diarrhea-predominant irritable bowel syndrome: a randomized control study. Appl Psychophysiol Biofeedback, 29(1), 19-33. https://doi.org/10.1023/b:apbi.0000017861.60439.95
Vlieger, A. M., Blink, M., Tromp, E., & Benninga, M. A. (2008). Use of complementary and alternative medicine by pediatric patients with functional and organic gastrointestinal diseases: results from a multicenter survey. Pediatrics, 122(2), e446–e451. https://doi.org/10.1542/peds.2008-0266
Toning quiets the mind and increases HRV more quickly than mindfulness practice
Posted: September 21, 2019 Filed under: behavior, Breathing/respiration, emotions, health, mindfulness, Pain/discomfort, relaxation, self-healing, stress management, Uncategorized | Tags: heart rate variability, intrusive thoughts, meditation, rumination 6 CommentsDisruptive thoughts, ruminations and worrying are common experiences especially when stressed. Numerous clinical strategies such as cognitive behavioral therapy attempt to teach clients to reduce negative ruminations (Kopelman-Rubin, Omer, & Dar, 2017). Over the last ten years, many people and therapists practice meditative techniques to let go and not be captured by negative ruminations, thoughts, and emotions. However, many people continue to struggle with distracting and wandering thoughts.
Just think back when you’re upset, hurt, angry or frustrated. Attempting just to observe without judgment can be very, very challenging as the mind keeps rehearsing and focusing on what happened. Telling yourself to stop being upset often doesn’t work because your mind is focused on how upset you are. If you can focus on something else or perform physical activity, the thoughts and feelings often subside.
Over the last fifteen years, mindfulness meditation has been integrated and adapted for use in behavioral medicine and psychology (Peper, Harvey, & Lin, 2019). It has also been implemented during bio- and neurofeedback training (Khazan, 2013; Khazan, 2019). Part of the mindfulness instruction is to recognize the thoughts without judging or becoming experientially “fused” with them. A process referred to as “meta-awareness” (Dahl, Lutz, & Davidson, 2015). Mindfulness training combined with bio- and neurofeedback training can improve a wide range of psychological and physical health conditions associated with symptoms of stress, such as anxiety, depression, chronic pain, and addiction (Creswell, 2015, Khazan, 2019).
Mindfulness is an effective technique; however, it may not be more effective than other self-regulations strategies (Peper et al, 2019). Letting go of worrying thoughts and rumination is even more challenging when one is upset, angry, or captured by stressful life circumstances. Is it possible that other strategies beside mindfulness may more rapidly reduce wandering and intrusive thoughts? In 2015, researchers van der Zwan, de Vente, Huiznik, Bogels, & de Bruin found that physical activity, mindfulness meditation and heart rate variability biofeedback were equally effective in reducing stress and its related symptoms when practiced for five weeks.
Our research explored whether other techniques from the ancient wisdom traditions could provide participants tools to reduce rumination and worry. We investigated the physiological effects and subject experiences of mindfulness and toning. Toning is vocalizing long and sustained sounds as a form of mediation. (Watch the video the toning demonstration by sound healer and musician, Madhu Anziani at the end of the blog.)
COMPARING TONING AND MINDFULNESS
The participants were 91 undergraduate college students (35 males, 51 females and 5 unspecified; average age, 22.4 years, (SD = 3.5 years).
After sitting comfortably in class, each student practiced either mindfulness or toning for three minutes each. After each practice, the students rated the extent of mind wandering, occurrence of intrusive thoughts and sensations of vibration on a scale from 0 (not all) to 10 (all the time). They also rated pre and post changes in peacefulness, relaxation, stress, warmth, anxiety and depression. After completing the assessment, they practice the other practice and after three minutes repeated the assessment.
The physiological changes that may occur during mindfulness practice and toning practice was recorded in a separate study with 11 undergraduate students (4 males, 7 females; average age 21.4 years. Heart rate and respiration were monitored with ProComp Infiniti™ system (Thought Technology, Ltd., Montreal, Canada). Respiration was monitored from the abdomen and upper thorax with strain gauges and heartrate was monitored with a blood volume pulse sensor placed on the thumb.
After the sensors were attached, the participants faced away from the screen so they did not receive feedback. They then followed the same procedure as described earlier, with three minutes of mindfulness, or toning practice, counterbalanced. After each condition, they completed a subjective assessment form rating experiences as described above.
RESULTS: SUBJECTIVE FINDINGS
Toning was much more successful in reducing mind wandering and intrusive thoughts than mindfulness. Toning also significantly increased awareness of body vibration as compared to mindfulness as shown in Figure 1.
Figure 1. Differences between mindfulness and toning practice.
There was no significant difference between toning and mindfulness in the increased self-report of peacefulness, warmth, relaxation, and decreased self-report of anxiety and depression as shown in Figure 2.
Figure 2. No significant difference between toning and mindfulness practice in relaxation or stress reports.
RESULTS: PHYSIOLOGICAL FINDINGS
Respiration rate was significantly lower during toning (4.6 br/min) as compared to mindfulness practice (11.6 br/min); heart rate standard deviation (SDNN) was much higher during toning condition (11.6) (SDNN 103.7 ms) than mindfulness (6.4) (SDNN 61.9 ms). Two representative physiological recording are shown in Figure 3.

Figure 3. Representative recordings of breathing and heart rate during mindfulness and toning practice. During toning the respiration rate (chest and abdomen) was much slower than during mindfulness and baseline conditions. Also, during toning heart rate variability was much larger than during mindfulness or baseline conditions.
DISCUSSION
Toning practice is a useful strategy to reduce mind wandering as well as inhibit intrusive thoughts and increase heart rate variability (HRV). Most likely toning uses the same neurological pathways as self-talk and thus inhibits the negative and hopeless thoughts. Toning is a useful meditation alternative because it instructs people to make a sound that vibrates in their body and thus they attend to the sound and not to their thoughts.
Physiologically, toning immediately changed the respiration rate to less than 6 breaths per minute and increases heart rate variability. This increase in heart rate variability occurs without awareness or striving. We recommend that toning is integrated as a strategy to complement bio-neurofeedback protocols. It may be a useful approach to enhance biofeedback-assisted HRV training since toning increases HRV without trying and it may be used as an alternative to mindfulness, or used in tandem for maximum effectiveness.
TAKE HOME MESSAGE
1) When people report feeling worried and anxious and have difficulty interrupting ruminations that they first practice toning before beginning mindfulness meditation or bio-neurofeedback training.
2) When training participants to increase heart rate variability, toning could be a powerful technique to increase HRV without striving
TONING DEMONSTRATION AND INSTRUCTION BY SOUND HEALER MADHU ANZIANI
For the published article see: Peper, E., Pollack, W., Harvey, R., Yoshino, A., Daubenmier, J. & Anziani, M. (2019). Which quiets the mind more quickly and increases HRV: Toning or mindfulness? NeuroRegulation, 6(3), 128-133.
REFERENCES
Creswell, J. D. (2015). Mindfulness Interventions. Annual Review of Psychology, 68, 491-516.
van der Zwan, J. E., de Vente, W., Huizink, A. C., Bogels, S. M., & de Bruin, E. I. (2015). Physical activity, mindfulness meditation, or heart rate variability biofeedback for stress reduction: A randomized controlled trial. Applied Psychophysiology and Biofeedback, 40(4), 257-268. https://doi.org/10.1007/s10484-015-9293-x
Reduce hot flashes and premenstrual symptoms with breathing
Posted: February 18, 2015 Filed under: Breathing/respiration, Pain/discomfort, self-healing, stress management, Uncategorized | Tags: biofeedback, Breathing, diaphragmatic breathing, heart rate variability, hormone replacement therapy, hot flashes, HRT, Menopause, respiration, sighs, stress, sympathetic activity 6 CommentsAfter the first week to my astonishment, I have fewer hot flashes and they bother me less. Each time I feel the warmth coming, I breathe out slowly and gently. To my surprise they are less intense and are much less frequent. I keep breathing slowly throughout the day. This is quite a surprise because I was referred for biofeedback training because of headaches that occurred after getting a large electrical shock. After 5 sessions my headaches have decreased and I can control them, and my hot flashes have decreased from 3-4 per day to 1-2 per week. -50 year old client
After students in my Holistic Health class at San Francisco State University practiced slower diaphragmatic breathing and begun to change their dysfunctional shallow breathing, gasping, sighing, and breath holding to diaphragmatic breathing. A number of the older female students students reported that their hot flashes decreased. Some of the younger female students reported that their menstrual cramps and discomfort were reduced by 80 to 90% when they laid down and breathed slower and lower into their abdomen.
 The recent study in JAMA reported that many women continue to experience menopausal triggered hot flashes for up to 14 years. Although the article described the frequency and possible factors that were associated with the prolonged hot flashes, it did not offer helpful solutions.
The recent study in JAMA reported that many women continue to experience menopausal triggered hot flashes for up to 14 years. Although the article described the frequency and possible factors that were associated with the prolonged hot flashes, it did not offer helpful solutions.
Another understanding of the dynamics of hot flashes is that the decrease in estrogen accentuates the sympathetic/ parasympathetic imbalances that probably already existed. Then any increase in sympathetic activation can trigger a hot flash. In many cases the triggers are events and thoughts that trigger a stress response, emotional responses such as anger, anxiety, or worry, increase caffeine intake and especially shallow chest breathing punctuated with sighs. Approximately 80% of American women tend to breathe thoracically often punctuated with sighs and these women are more likely to experience hot flashes. On the other hand, the 20% of women who habitually breathe diaphragmatically tend to have fewer and less intense hot flashes and often go through menopause without any discomfort. In the superb study Drs. Freedman and Woodward (1992), taught women who experience hot flashes to breathe slowly and diaphragmatically which increased their heart rate variability as an indicator of sympathetic/parasympathetic balance and most importantly it reduced the the frequency and intensity of hot flashes by 50%.
Test the breathing connection if you experience hot flashes
Take a breath into your chest and rapidly exhale with a sigh. Repeat this quickly five times. In most cases, one minute later you will experience the beginning sensations of a hot flash. Similarly, when you practice slow diaphragmatic breathing throughout the day and interrupt every gasp, breath holding moment, sigh or shallow chest breathing with slower diaphragmatic breathing, you will experience a significant reduction in hot flashes.
Although this breathing approach has been well documented, many people are unaware of this simple behavioral approach unlike the common recommendation for the hormone replacement therapies (HRT) to ameliorate menopausal symptoms. This is not surprising since pharmaceutical companies spent nearly five billion dollars per year in direct to consumer advertising for drugs and very little money is spent on advertising behavioral treatments. There is no profit for pharmaceutical companies teaching effortless diaphragmatic breathing unlike prescribing HRTs. In addition, teaching and practicing diaphragmatic breathing takes skill training and practice time–time which is not reimbursable by third party payers.
For more information, research data and breathing skills to reduce hot flash intensity, see our article which is reprinted below.
Gibney, H.K. & Peper, E. (2003). Taking control: Strategies to reduce hot flashes and premenstrual mood swings. Biofeedback, 31(3), 20-24.
Taking control: Strategies to reduce hot flashes and premenstrual mood swings*
Erik Peper, Ph.D**., and Katherine H. Gibney
San Francisco State University
After the first week to my astonishment, I have fewer hot flashes and they bother me less. Each time I feel the warmth coming, I breathe out slowly and gently. To my surprise they are less intense and are much less frequent. I keep breathing slowly throughout the day. This is quite a surprise because I was referred for biofeedback training because of headaches that occurred after getting a large electrical shock. After 5 sessions my headaches have decreased and I can control them, and my hot flashes have decreased from 3-4 per day to 1-2 per week. -50 year old client
For the first time in years, I experienced control over my premenstrual mood swings. Each time I could feel myself reacting, I relaxed, did my autogenic training and breathing. I exhaled. It brought me back to center and calmness. -26 year old student
Abstract
Women have been troubled by hot flashes and premenstrual syndrome for ages. Hormone replacement therapy, historically the most common treatment for hot flashes, and other pharmacological approaches for pre-menstrual syndrome (PMS) appear now to be harmful and may not produce significant benefits. This paper reports on a model treatment approach based upon the early research of Freedman & Woodward to reduce hot flashes and PMS using biofeedback training of diaphragmatic breathing, relaxation, and respiratory sinus arrhythmia. Successful symptom reduction is contingent upon lowering sympathetic arousal utilizing slow breathing in response to stressors and somatic changes. We strongly recommend that effortless diaphragmatic breathing be taught as the first step to reduce hot flashes and PMS symptoms.
A long and uncomfortable history
Women have been troubled by hot flashes and premenstrual syndrome for ages. Hot flashes often result in red faces, sweating bodies, and noticeable and embarrassing discomfort. They come in the middle of meetings, in the middle of the night, and in the middle of romantic interludes. Premenstrual syndrome also arrives without notice, bringing such symptoms as severe mood swings, anger, crying, and depression.
Hormone replacement therapy (HRT) was the most common treatment for hot flashes for decades. However, recent randomized controlled trials show that the benefits of HRT are less than previously thought and the risks—especially of invasive breast cancer, coronary artery disease, dementia, stroke and venous thromboembolism—are greater (Humphries & Gill, 2003; Shumaker, et al, 2003; Wassertheil-Smoller, et al, 2003). In addition, there is no evidence of increased quality of life improvements (general health, vitality, mental health, depressive symptoms, or sexual satisfaction) as claimed for HRT (Hays et al, 2003).
“As a result of recent studies, we know that hormone therapy should not be used to prevent heart disease. These studies also report an increased risk of heart attack, stroke, breast cancer, blood clots, and dementia…” -Wyeth Pharmaceuticals (2003)
Because of the increased long-term risk and lack of benefit, many physicians are weaning women off HRT at a time when the largest population of maturing women in history (‘baby boomers’) is entering menopausal years. The desire to find a reliable remedy for hot flashes is on the front burner of many researchers’ minds, not to mention the minds of women suffering from these ‘uncontrollable’ power surges. Yet, many women are becoming increasingly leery of the view that menopause is an illness. There is a rising demand to find a natural remedy for this natural stage in women’s health and development.
For younger women a similar dilemma occurs when they seek treatment of discomfort associated with their menstrual cycle. Is premenstrual syndrome (PMS) just a natural variation in energy and mood levels? Or, are women expected to adapt to a masculine based environment that requires them to override the natural tendency to perform in rhythm with their own psychophysiological states? Instead of perceiving menstruation as a natural occurrence in which one has different moods and/or energy levels, women in our society are required to perform at the status quo, which may contribute to PMS. The feelings and mood changes are quickly labeled as pathology that can only be treated with medication.
Traditionally, premenstrual syndrome is treated with pharmaceuticals, such as birth control pills or Danazol. Although medications may alleviate some symptoms, many women experience unpleasant side effects, such as bloating or acne, and still experience a variety of PMS symptoms. Many cannot tolerate the medications. Thus, millions of women (and families) suffer monthly bouts of ‘uncontrollable’ PMS symptoms
For both hot flashes and PMS the biomedical model tends to frame the symptoms as a “structural biological problem.” Namely, the pathology occurs because the body is either lacking in, or has an excess of, some hormone. All that needs to be done is either augment or suppress hormones/symptoms with some form of drug. Recently, for example, medicine has turned to antidepressant medications to address menopausal hot flashes (Stearns, Beebe, Iyengar, & Dube, 2003).
The biomedical model, however, is only one perspective. The opposite perspective is that the dysfunction occurs because of how we use ourselves. Use in this sense means our thoughts, emotions and body patterns. As we use ourselves, we change our physiology and, thereby, may affect and slowly change the predisposing and maintaining factors that contribute to our dysfunction. By changing our use, we may reduce the constraints that limit the expression of the self-healing potential that is intrinsic in each person.
The intrinsic power of self-healing is easily observed when we cut our finger. Without the individual having to do anything, the small cut bleeds, clotting begin and tissue healing is activated. Obviously, we can interfere with the healing process, such as when we scrape the scab, rub dirt in the wound, reduce blood flow to the tissue or feel anxious or afraid. Conversely, cleaning the wound, increasing blood flow to the area, and feeling “safe” and relaxed can promote healing. Healing is a dynamic process in which both structure and use continuously affect each other. It is highly likely that menopausal hot flashes and PMS mood swings are equally an interaction of the biological structure (hormone levels) and the use factor (sympathetic/parasympathetic activation).
Uncontrollable or overly aroused?
Are the hot flashes and PMS mood swings really ‘uncontrollable?’ From a physiological perspective, hot flashes are increased by sympathetic arousal. When the sympathetic system is activated, whether by medication or by emotions, hot flashes increase and similarly, when sympathetic activity decreases hot flashes decrease. Equally, PMS, with its strong mood swings, is aggravated by sympathetic arousal. There are many self-management approaches that can be mastered to change and reduce sympathetic arousal, such as breathing, meditation, behavioral cognitive therapy, and relaxation.
Breathing patterns are closely associated with hot flashes. During sleep, a sigh generally occurs one minute before a hot flash as reported by Freedman and Woodward (1992). Women who habitually breathe thoracically (in the chest) report much more discomfort and hot flashes than women who habitually breathe diaphragmatically. Freedman, Woodward, Brown, Javaid, and Pandey (1995) and Freedman and Woodward (1992) found that hot flash rates during menopause decreased in women who practiced slower breathing for two weeks. In their studies, the control groups received alpha electroencephalographic feedback and did not benefit from a reduction of hot flashes. Those who received training in paced breathing reduced the frequency of their hot flashes by 50% when they practiced slower breathing. This data suggest that the slower breathing has a significant effect on the sympathetic and parasympathetic balance.
Women with PMS appear similarly able to reduce their discomfort. An early study utilizing Autogenic Training (AT) combined with an emphasis on warming the lower abdomen resulted in women noting improvement in dysfunctional bleeding (Luthe & Schultz, 1969, pp. 144-148). Using a similar approach, Mathew, Claghorn, Largen, and Dobbins (1979) and Dewit (1981) found that biofeedback temperature training was helpful in reducing PMS symptoms.. A later study by Goodale, Domar, and Benson (1990) found that women with severe PMS symptoms who practiced the relaxation response reported a 58% improvement in overall symptomatology as compared to a 27.2% improvement for the reading control group and a 17.0% improvement for the charting group.
Teaching control and achieving results
Teaching women to breathe effortlessly can lead to positive results and an enhanced sense of control. By effortless breathing, the authors refer to their approach to breath training, which involves a slow, comfortable respiration, larger volume of air exchange, and a reliance upon action of the muscles of the diaphragm rather than the chest (Peper, 1990). For more instructions see the recent blog, A breath of fresh air: Improve health with breathing.
Slowing breathing helps to limit the sighs common to rapid thoracic breathing—sighs that often precede menopausal hot flashes. Effortless breathing is associated with stress reduction—stress and mood swings are common concerns of women suffering from PMS. In a pilot study Bier, Kazarian, Peper, and Gibney (2003) at San Francisco State University (SFSU) observed that when the subject practiced diaphragmatic breathing throughout the month, combined with Autogenic Training, her premenstrual psychological symptoms (anger, depressed mood, crying) and premenstrual responses to stressors were significantly reduced as shown in Figure 1.
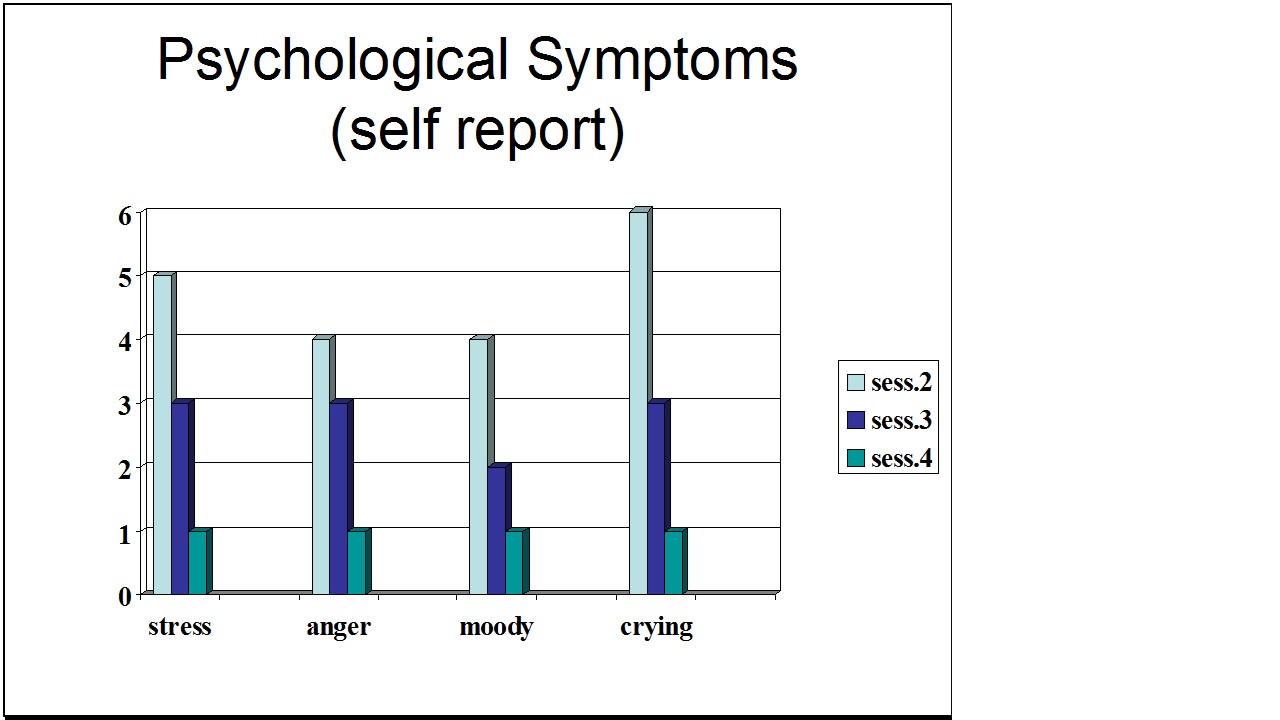
Figure 1. Student’s Individual Subjective Rating in Response to PMS Symptoms.
In another pilot study at SFSU, Frobish, Peper, and Gibney (2003) trained a volunteer who suffered from frequent hot flashes to breathe diaphragmatically. The training goals included modifying breathing patterns, producing a Respiratory Sinus Arrhythmia (RSA), and peripheral hand warming. RSA refers to a pattern of slow, regular breathing during which variations in heart rate enter into a synchrony with the respiration. Each inspiration is accompanied by an increase in heart rate, and each expiration is accompanied by a decrease in heart rate (with some phase differences depending on the rate of breathing). The presence of the RSA pattern is an indication of optimal balance between sympathetic and parasympathetic nervous activity.
During the 11-day study period, the subject charted the occurrence of hot flashes and noted a significant decrease by day 5. However, on the evening of day 7 she sprained her ankle and experienced a dramatic increase in hot flashes on day 8. Once the subject recognized her stress response, she focused more on breathing and was able to reduce the flashes as shown in Figure 2. 
Figure 2. Subjective rating of intensity, frequency and bothersomeness of hot flashes. The increase in hot flashes coincided with increased frustration about an ankle injury.
Our clinical experience confirms the SFSU pilot studies and the previously referenced research by Freedman and Woodward (1992) and Freedman et al. (1995). When arousal is lowered and breathing is effortless, women are better able to cope with stress and report a reduction in symptoms. Habitual rapid thoracic breathing tends to increase arousal while slower breathing, especially slower exhalation, tends to relax and reduce arousal. Learning and then applying effortless breathing reduces excessive sympathetic arousal. It also interrupts the cycle of cognitive activation, anxiety, and somatic arousal. The anticipation and frustration at having hot flashes becomes the cue to shift attention and “breathe slower and lower.” This process stops the cognitively mediated self-activation.
Successful self-regulation and the return to health begin with cognitive reframing: We are not only a genetic biological fixed (deficient) structure but also a dynamic changing system in which all parts (thoughts, emotions, behavior, diet, stress, and physiology) affect and are effected by each other. Within this dynamic changing system, there is an opportunity to implement and practice behaviors and life patterns that promote health.
Learning Diaphragmatic Breathing with and without Biofeedback
Although there are many strategies to modify respiration, biofeedback monitoring combined with respiration training is very useful as it provides real-time feedback. Chest and abdominal movement are recorded with strain gauges and heart rate can be monitored either by an electrocardiogram (EKG) or by a photoplethysmograph sensor on a finger or thumb. Peripheral temperature and electrodermal activity (EDA) biofeedback are also helpful in training. The training focuses on teaching effortless diaphragmatic breathing and encouraging the participant to practice many times during the day, especially when becoming aware of the first sensations of discomfort.
Learning and integrating effortless diaphragmatic breathing into daily life is one of the biofeedback strategies that has been successfully used as a primary or adjunctive/complementary tool for the reversal of disorders such as hypertension, migraine headaches, repetitive strain injury, pain, asthma and anxiety (Schwartz & Andrasik, 2003), as well as hot flashes and PMS.
The biofeedback monitoring provides the trainer with a valuable tool to:
- Observe & identify: Dysfunctional rapid thoracic breathing patterns, especially in response to stressors, are clearly displayed in real-time feedback.
- Demonstrate & train: The physiological feedback display helps the person see that she is breathing rapidly and shallowly in her chest with episodic sighs. Coaching with feedback helps her to change her breathing pattern to one that promotes a more balanced homeostasis.
- Motivate, persuade and change beliefs: The person observes her breathing patterns change concurrently with a felt shift in physiology, such as a decrease in irritability, or an increase in peripheral temperature, or a reduction in the incidence of hot flushes. Thus, she has a confirmation of the importance of breathing diaphragmatically.
In addition, we suggest exercises that integrate verbal and kinesthetic instructions, such as the following: “Exhale gently,” and “Breathe down your leg with a partner.”
Exhale Gently:
Imagine that you are holding a baby. Now with your shoulders relaxed, inhale gently so that your abdomen widens. Then as you exhale, purse your lips and very gently and softly blow over the baby’s hair. Allow your abdomen to narrow when exhaling. Blow so softly that the baby’s hair barely moves. At the same time, imagine that you can allow your breath to flow down and through your legs. Continue imagining that you are gently blowing on the baby’s hair while feeling your breath flowing down your legs. Keep blowing very softly and continuously.
Practice exhaling like this the moment that you feel any sensation associated with hot flashes or PMS symptoms. Smile sweetly as you exhale.
Breathe Down Your Legs with a Partner
Sit or lie comfortably with your feet a shoulder width apart. As you exhale softly whisper the sound “Haaaaa….” Or, very gently press your tongue to your pallet and exhale while making a very soft hissing sound.
Have your partner touch the side of your thighs. As you exhale have your partner stroke down your thighs to your feet and beyond, stroking in rhythm with your exhalation. Do not rush. Apply gentle pressure with the stroking. Do this for four or five breaths.
Now, continue breathing as you imagine your breath flowing through your legs and out your feet.
During the day remember the feeling of your breath flowing downward through your legs and out your feet as you exhale.
Learning Strategies in Biofeedback Assisted Breath Training
Common learning strategies that are associated with the more successful amelioration of hot flashes and PMS include:
- Master effortless diaphragmatic breathing, and concurrently increase respiratory sinus arrhythmia (RSA). Instead of breathing rapidly, such as at 18 breaths per minute, the person learns to breathe effortlessly and slowly (about 6 to 8 breaths per minute). This slower breathing and increased RSA is an indication of sympathetic-parasympathetic balance as shown in Figure 3.
- Practice slow effortless diaphragmatic breathing many times during the day and, especially in response to stressors.
- Use the physical or emotional sensations of a hot flash or mood alteration as the cue to exhale, let go of anxiety, breathe diaphragmatically and relax.
- Reframe thoughts by accepting the physiological processes of menstruation or menopause, and refocus the mind on positive thoughts, and breathing rhythmically.
- Change one’s lifestyle and allow personal schedules to flow in better balance with individual, dynamic energy levels.
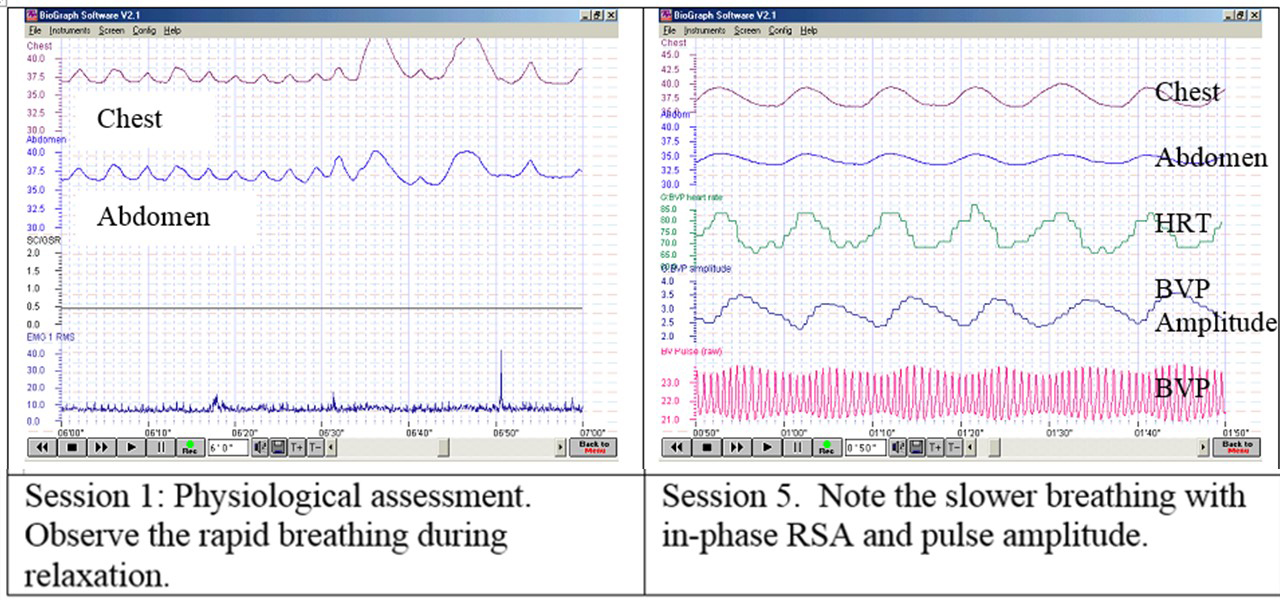 Figure 3. Physiological Recordings of a Participant with PMS. This subject learned effortless diaphragmatic breathing by the fifth session and experienced a significant decrease in symptoms.
Figure 3. Physiological Recordings of a Participant with PMS. This subject learned effortless diaphragmatic breathing by the fifth session and experienced a significant decrease in symptoms.
Generalizing skills and interrupting the pattern
The limits of self-regulation are unknown, often held back only by the practitioner’s and participant’s beliefs. Biofeedback is a powerful self-regulation tool for individuals to observe and modify their covert physiological reactions. Other skills that augment diaphragmatic breathing are Quieting Reflex (Stroebel, 1982), Autogenic Training (Schultz & Luthe, 1969), and mindfulness training (Kabat-Zinn, 1990). In all skill learning, generalization is a fundamental factor underlying successful training. Integrating the learned psychophysiological skills into daily life can significantly improve health—especially in anticipation of and response to stress. The anticipated stress can be a physical, cognitive or social trigger, or merely the felt onset of a symptom.
As the person learns and applies effortless breathing to daily activities, she becomes more aware of factors that affect her breathing. She also experiences an increased sense of control: She can now take action (a slow effortless breath) in moments when she previously felt powerless. The biofeedback-mastered skill interrupts the evoked frustrations and irritations associated with an embarrassing history of hot flashes or mood swings. Instead of continuing with the automatic self-talk, such as “Damn, I am getting hot, why doesn’t it just stop?” (language fueling sympathetic arousal), she can take a relaxing breath in response to the internal sensations, stop the escalating negative self-talk and allows more acceptance—a process reducing sympathetic arousal.
In summary, effortless breathing appears to be a non-invasive behavioral strategy to reduce hot flashes and PMS symptoms. Practicing effortless diaphragmatic breathing contributes to a sense of control, supports a healthier homeostasis, reduces symptoms, and avoids the negative drug side effects. We strongly recommend that effortless diaphragmatic breathing be taught as the first step to reduce hot flashes and PMS symptoms.
I feel so much cooler. I can’t believe that my hand temperature went up. I actually feel calmer and can’t even feel the threat of a hot flash. Maybe this breathing does work! –Menopausal patient after initial training in diaphragmatic breathing
References
Bier, M., Kazarian, D., Peper, E., & Gibney, K. (2003). Reducing the severity of PMS symptoms with diaphragmatic breathing, autogenic training and biofeedback. Unpublished report.
Freedman, R.R., & Woodward, S. (1992). Behavioral treatment of menopausal hot flushes: Evaluation by ambulatory monitoring. American Journal of Obstetrics and Gynecology, 167 (2), 436-439.
Freedman, R.R., Woodward, S., Brown, B., Javaid, J.I., & Pandey, G.N. (1995). Biochemical and thermoregulatory effects of behavioral treatment for menopausal hot flashes. Menopause: The Journal of the North American Menopause Society, 2 (4), 211-218.
Frobish,C., Peper, E. & Gibney, K. H. (2003). Menopausal Hot Flashes: A Self-Regulation Case Study. Poster presentation at the 35th Annual Meeting of the Association for Applied Psychophysiology and Biofeedback. Abstract in: Applied Psychophysiology and Biofeedback. 29 (4), 302.
Goodale, I.L., Domar, A.D., & Benson, H. (1990). Alleviation of Premenstrual Syndrome symptoms with the relaxation response. Obstetrics and Gynecological Journal, 75 (5), 649-55.
Hays, J., Ockene, J.K., Brunner, R.L., Kotchen, J.M., Manson, J.E., Patterson, R.E., Aragaki, A.K., Shumaker, S.A., Brzyski, R.G., LaCroix, A.Z., Granek, I.A, & Valanis, B.G., Women’s Health Initiative Investigators. (2003). Effects of estrogen plus progestin on health-related quality of life. New England Journal of Medicine, 348, 1839-1854.
Humphries, K.H.., & Gill, s. (2003). Risks and benefits of hormone replacement therapy: the evidence speaks. Canadian Medical Association Journal, 168(8), 1001-10.
Kabat-Zinn, J. (1990). Full catastrophe living. New York: Delacorte Press.
Luthe, W. & Schultz, J.H. (1969). Autogenic therapy: Vol II: Medical applications. New York: Grune & Stratton.
Mathew, R.J.; Claghorn, J.L.; Largen, J.W.; & Dobbins, K. (1979). Skin Temperature control for premenstrual tension syndrome:A pilot study. American Journal of Clinical Biofeedback, 2 (1), 7-10.
Peper, E. (1990). Breathing for health. Montreal: Thought Technology Ltd.
Schultz, J.H., & Luthe, W. (1969). Autogenic therapy: Vol 1. Autogenic methods. New York: Grune and Stratton.
Schwartz, M.S. & Andrasik, F.(2003). Biofeedback: A practitioner’s guide, 3nd edition. New York: Guilford Press.
Shumaker, S.A., Legault, C., Thal, L., Wallace, R.B., Ockene, J., Hendrix, S., Jones III, B., Assaf, A.R., Jackson, R. D., Morley Kotchen, J., Wassertheil-Smoller, S.; & Wactawski-Wende, J. (2003). Estrogen plus progestin and the incidence of dementia and mild cognitive impairment in post menopausal women: The Women’s Health Initiative memory study: A randomized controlled trial. Journal of the American Medical Association, 289 (20), 2651-2662.
Stearns, V., Beebe, K. L., Iyengar, M., & Dube, E. (2003). Paroxetine controlled release in the treatment of menopausal hot flashes. Journal of the American Medical Association, 289 (21), 2827-2834.
Stroebel, C. F. (1982). QR, the quieting reflex. New York: G. P. Putnam’s Sons.
van Dixhoorn, J.J. (1998). Ontspanningsinstructie Principes en Oefeningen (Respiration instructions: Principles and exercises). Maarssen, Netherlands: Elsevier/Bunge.
Wassertheil-Smoller, S., Hendrix, S., Limacher, M., Heiss, G., Kooperberg, C., Baird, A., Kotchen, T., Curb, Dv., Black, H., Rossouw, J.E., Aragaki, A., Safford, M., Stein, E., Laowattana, S., & Mysiw, W.J. (2003). Effect of estrogen plus progestin on stroke in postmenopausal women: The Women’s Health Initiative: A randomized trial. Journal of the American Medical Association, 289 (20), 2673-2684.
Wyeth Pharmaceuticals (2003, June 4). A message from Wyeth: Recent reports on hormone therapy and where we stand today. San Francisco Chronicle, A11.
*We thank Candy Frobish, Mary Bier and Dalainya Kazarian for their helpful contributions to this research.
**For communications contact: Erik Peper, Ph.D., Institute for Holistic Healing Studies, San Francisco State University, 1600 Holloway Avenue, San Francisco, CA 94132; Tel: (415) 338 7683; Email: epeper@sfsu.edu; website: http://www.biofeedbackhealth.org; blog: http://www.peperperspective.come
Breathing: The Mind/Body Connection. Youtube interviews of Erik Peper, PhD by Larry Berkelhammer, PhD
Posted: December 19, 2012 Filed under: Breathing/respiration, Uncategorized | Tags: anxiety, asthma, biofeedback breathing, Breathing, heart rate variability, meditation, panic, relaxation, stress management 4 CommentsErik Peper, Respiration & Health
How we breathe is intimately connected to our state of health. We can speed up breathing to energize or slow it for a calming effect. Practice becoming more aware of the speed and depth of your breathing. Breathing diaphragmatically at 6 to 7 breaths per minute is regenerative. Breathing patterns alter physiological, psychological, and emotional processes. Conscious regulation of breathing can improve asthma, panic disorder and many other conditions. A simple change in breathing can induce symptoms or resolve them. Learn to observe breath-holding. Devices like Stress Eraser and Em-Wave teach healthy breathing at home. When we start taking charge there’s more hope. Focus on skills not pills.
Erik Peper, Mastery Through Conscious Breathing Practices
In this interview of Dr. Erik Peper, we discuss the power of Tumo breathing. This form of conscious breathing has been studied by Dr. Herbert Benson of Harvard and many other Western researchers. It is a special form of conscious respiration that increases metabolic rate and allows Buddhist monks and others who practice it to prove to themselves that they can use their minds to alter physiology. The value of such intense practices is that they allow us to gain mastery and the absolute knowledge that we have the ability to exert voluntary control over mental and physiological processes. Most Buddhist practices lead to the possibility of gaining a certain degree of mastery of consciousness.
