What do numbers mean? How much does Walmart’s wage raise affect profits?
Posted: February 22, 2015 Filed under: Uncategorized | Tags: economics, salaries, stress 1 Comment Walmart created news when it announced that it will be paying its 500,000 employees more than the minimum wage. The largest increase would be an increase of the entry-level wage from the US minimum $7.25 to $9 an hour; howver, the overall increase in minimal. As Jody Knauss and Mary Bottari point out, The company forecasts the average hourly wage for full-time workers to rise 15 cents an hour, from $12.85 to $13.00, while the average for part-timers will bump up from $9.48 to $10.00 per hour. This will still still leave most of its workers beneath the poverty level and relying on food stamps to make ends meet.
Walmart created news when it announced that it will be paying its 500,000 employees more than the minimum wage. The largest increase would be an increase of the entry-level wage from the US minimum $7.25 to $9 an hour; howver, the overall increase in minimal. As Jody Knauss and Mary Bottari point out, The company forecasts the average hourly wage for full-time workers to rise 15 cents an hour, from $12.85 to $13.00, while the average for part-timers will bump up from $9.48 to $10.00 per hour. This will still still leave most of its workers beneath the poverty level and relying on food stamps to make ends meet.
The actual cost of this wage raise for Walmart is one billion dollars. This seems impressive; however, this number is not meaningful without knowing the financial state of the company. The company’s estimated profit for 2014 was $16.36 billion on annual sales of $485 Billion. For more details see the Walmart’s financial summary.
The one billion dollars to increase the salaries is an impressive sound bite, but it only a 6.1% decreases the company’s profits. It will still leave more than 15 billion dollar in profit and more than 150 billion dollar wealth for its owners. Given the profits and wealth, Walmart should be ashamed to keep its employees in poverty. It should offer its employees an actually living wage of at least $15 per hour.
Reduce hot flashes and premenstrual symptoms with breathing
Posted: February 18, 2015 Filed under: Breathing/respiration, Pain/discomfort, self-healing, stress management, Uncategorized | Tags: biofeedback, Breathing, diaphragmatic breathing, heart rate variability, hormone replacement therapy, hot flashes, HRT, Menopause, respiration, sighs, stress, sympathetic activity 6 CommentsAfter the first week to my astonishment, I have fewer hot flashes and they bother me less. Each time I feel the warmth coming, I breathe out slowly and gently. To my surprise they are less intense and are much less frequent. I keep breathing slowly throughout the day. This is quite a surprise because I was referred for biofeedback training because of headaches that occurred after getting a large electrical shock. After 5 sessions my headaches have decreased and I can control them, and my hot flashes have decreased from 3-4 per day to 1-2 per week. -50 year old client
After students in my Holistic Health class at San Francisco State University practiced slower diaphragmatic breathing and begun to change their dysfunctional shallow breathing, gasping, sighing, and breath holding to diaphragmatic breathing. A number of the older female students students reported that their hot flashes decreased. Some of the younger female students reported that their menstrual cramps and discomfort were reduced by 80 to 90% when they laid down and breathed slower and lower into their abdomen.
 The recent study in JAMA reported that many women continue to experience menopausal triggered hot flashes for up to 14 years. Although the article described the frequency and possible factors that were associated with the prolonged hot flashes, it did not offer helpful solutions.
The recent study in JAMA reported that many women continue to experience menopausal triggered hot flashes for up to 14 years. Although the article described the frequency and possible factors that were associated with the prolonged hot flashes, it did not offer helpful solutions.
Another understanding of the dynamics of hot flashes is that the decrease in estrogen accentuates the sympathetic/ parasympathetic imbalances that probably already existed. Then any increase in sympathetic activation can trigger a hot flash. In many cases the triggers are events and thoughts that trigger a stress response, emotional responses such as anger, anxiety, or worry, increase caffeine intake and especially shallow chest breathing punctuated with sighs. Approximately 80% of American women tend to breathe thoracically often punctuated with sighs and these women are more likely to experience hot flashes. On the other hand, the 20% of women who habitually breathe diaphragmatically tend to have fewer and less intense hot flashes and often go through menopause without any discomfort. In the superb study Drs. Freedman and Woodward (1992), taught women who experience hot flashes to breathe slowly and diaphragmatically which increased their heart rate variability as an indicator of sympathetic/parasympathetic balance and most importantly it reduced the the frequency and intensity of hot flashes by 50%.
Test the breathing connection if you experience hot flashes
Take a breath into your chest and rapidly exhale with a sigh. Repeat this quickly five times. In most cases, one minute later you will experience the beginning sensations of a hot flash. Similarly, when you practice slow diaphragmatic breathing throughout the day and interrupt every gasp, breath holding moment, sigh or shallow chest breathing with slower diaphragmatic breathing, you will experience a significant reduction in hot flashes.
Although this breathing approach has been well documented, many people are unaware of this simple behavioral approach unlike the common recommendation for the hormone replacement therapies (HRT) to ameliorate menopausal symptoms. This is not surprising since pharmaceutical companies spent nearly five billion dollars per year in direct to consumer advertising for drugs and very little money is spent on advertising behavioral treatments. There is no profit for pharmaceutical companies teaching effortless diaphragmatic breathing unlike prescribing HRTs. In addition, teaching and practicing diaphragmatic breathing takes skill training and practice time–time which is not reimbursable by third party payers.
For more information, research data and breathing skills to reduce hot flash intensity, see our article which is reprinted below.
Gibney, H.K. & Peper, E. (2003). Taking control: Strategies to reduce hot flashes and premenstrual mood swings. Biofeedback, 31(3), 20-24.
Taking control: Strategies to reduce hot flashes and premenstrual mood swings*
Erik Peper, Ph.D**., and Katherine H. Gibney
San Francisco State University
After the first week to my astonishment, I have fewer hot flashes and they bother me less. Each time I feel the warmth coming, I breathe out slowly and gently. To my surprise they are less intense and are much less frequent. I keep breathing slowly throughout the day. This is quite a surprise because I was referred for biofeedback training because of headaches that occurred after getting a large electrical shock. After 5 sessions my headaches have decreased and I can control them, and my hot flashes have decreased from 3-4 per day to 1-2 per week. -50 year old client
For the first time in years, I experienced control over my premenstrual mood swings. Each time I could feel myself reacting, I relaxed, did my autogenic training and breathing. I exhaled. It brought me back to center and calmness. -26 year old student
Abstract
Women have been troubled by hot flashes and premenstrual syndrome for ages. Hormone replacement therapy, historically the most common treatment for hot flashes, and other pharmacological approaches for pre-menstrual syndrome (PMS) appear now to be harmful and may not produce significant benefits. This paper reports on a model treatment approach based upon the early research of Freedman & Woodward to reduce hot flashes and PMS using biofeedback training of diaphragmatic breathing, relaxation, and respiratory sinus arrhythmia. Successful symptom reduction is contingent upon lowering sympathetic arousal utilizing slow breathing in response to stressors and somatic changes. We strongly recommend that effortless diaphragmatic breathing be taught as the first step to reduce hot flashes and PMS symptoms.
A long and uncomfortable history
Women have been troubled by hot flashes and premenstrual syndrome for ages. Hot flashes often result in red faces, sweating bodies, and noticeable and embarrassing discomfort. They come in the middle of meetings, in the middle of the night, and in the middle of romantic interludes. Premenstrual syndrome also arrives without notice, bringing such symptoms as severe mood swings, anger, crying, and depression.
Hormone replacement therapy (HRT) was the most common treatment for hot flashes for decades. However, recent randomized controlled trials show that the benefits of HRT are less than previously thought and the risks—especially of invasive breast cancer, coronary artery disease, dementia, stroke and venous thromboembolism—are greater (Humphries & Gill, 2003; Shumaker, et al, 2003; Wassertheil-Smoller, et al, 2003). In addition, there is no evidence of increased quality of life improvements (general health, vitality, mental health, depressive symptoms, or sexual satisfaction) as claimed for HRT (Hays et al, 2003).
“As a result of recent studies, we know that hormone therapy should not be used to prevent heart disease. These studies also report an increased risk of heart attack, stroke, breast cancer, blood clots, and dementia…” -Wyeth Pharmaceuticals (2003)
Because of the increased long-term risk and lack of benefit, many physicians are weaning women off HRT at a time when the largest population of maturing women in history (‘baby boomers’) is entering menopausal years. The desire to find a reliable remedy for hot flashes is on the front burner of many researchers’ minds, not to mention the minds of women suffering from these ‘uncontrollable’ power surges. Yet, many women are becoming increasingly leery of the view that menopause is an illness. There is a rising demand to find a natural remedy for this natural stage in women’s health and development.
For younger women a similar dilemma occurs when they seek treatment of discomfort associated with their menstrual cycle. Is premenstrual syndrome (PMS) just a natural variation in energy and mood levels? Or, are women expected to adapt to a masculine based environment that requires them to override the natural tendency to perform in rhythm with their own psychophysiological states? Instead of perceiving menstruation as a natural occurrence in which one has different moods and/or energy levels, women in our society are required to perform at the status quo, which may contribute to PMS. The feelings and mood changes are quickly labeled as pathology that can only be treated with medication.
Traditionally, premenstrual syndrome is treated with pharmaceuticals, such as birth control pills or Danazol. Although medications may alleviate some symptoms, many women experience unpleasant side effects, such as bloating or acne, and still experience a variety of PMS symptoms. Many cannot tolerate the medications. Thus, millions of women (and families) suffer monthly bouts of ‘uncontrollable’ PMS symptoms
For both hot flashes and PMS the biomedical model tends to frame the symptoms as a “structural biological problem.” Namely, the pathology occurs because the body is either lacking in, or has an excess of, some hormone. All that needs to be done is either augment or suppress hormones/symptoms with some form of drug. Recently, for example, medicine has turned to antidepressant medications to address menopausal hot flashes (Stearns, Beebe, Iyengar, & Dube, 2003).
The biomedical model, however, is only one perspective. The opposite perspective is that the dysfunction occurs because of how we use ourselves. Use in this sense means our thoughts, emotions and body patterns. As we use ourselves, we change our physiology and, thereby, may affect and slowly change the predisposing and maintaining factors that contribute to our dysfunction. By changing our use, we may reduce the constraints that limit the expression of the self-healing potential that is intrinsic in each person.
The intrinsic power of self-healing is easily observed when we cut our finger. Without the individual having to do anything, the small cut bleeds, clotting begin and tissue healing is activated. Obviously, we can interfere with the healing process, such as when we scrape the scab, rub dirt in the wound, reduce blood flow to the tissue or feel anxious or afraid. Conversely, cleaning the wound, increasing blood flow to the area, and feeling “safe” and relaxed can promote healing. Healing is a dynamic process in which both structure and use continuously affect each other. It is highly likely that menopausal hot flashes and PMS mood swings are equally an interaction of the biological structure (hormone levels) and the use factor (sympathetic/parasympathetic activation).
Uncontrollable or overly aroused?
Are the hot flashes and PMS mood swings really ‘uncontrollable?’ From a physiological perspective, hot flashes are increased by sympathetic arousal. When the sympathetic system is activated, whether by medication or by emotions, hot flashes increase and similarly, when sympathetic activity decreases hot flashes decrease. Equally, PMS, with its strong mood swings, is aggravated by sympathetic arousal. There are many self-management approaches that can be mastered to change and reduce sympathetic arousal, such as breathing, meditation, behavioral cognitive therapy, and relaxation.
Breathing patterns are closely associated with hot flashes. During sleep, a sigh generally occurs one minute before a hot flash as reported by Freedman and Woodward (1992). Women who habitually breathe thoracically (in the chest) report much more discomfort and hot flashes than women who habitually breathe diaphragmatically. Freedman, Woodward, Brown, Javaid, and Pandey (1995) and Freedman and Woodward (1992) found that hot flash rates during menopause decreased in women who practiced slower breathing for two weeks. In their studies, the control groups received alpha electroencephalographic feedback and did not benefit from a reduction of hot flashes. Those who received training in paced breathing reduced the frequency of their hot flashes by 50% when they practiced slower breathing. This data suggest that the slower breathing has a significant effect on the sympathetic and parasympathetic balance.
Women with PMS appear similarly able to reduce their discomfort. An early study utilizing Autogenic Training (AT) combined with an emphasis on warming the lower abdomen resulted in women noting improvement in dysfunctional bleeding (Luthe & Schultz, 1969, pp. 144-148). Using a similar approach, Mathew, Claghorn, Largen, and Dobbins (1979) and Dewit (1981) found that biofeedback temperature training was helpful in reducing PMS symptoms.. A later study by Goodale, Domar, and Benson (1990) found that women with severe PMS symptoms who practiced the relaxation response reported a 58% improvement in overall symptomatology as compared to a 27.2% improvement for the reading control group and a 17.0% improvement for the charting group.
Teaching control and achieving results
Teaching women to breathe effortlessly can lead to positive results and an enhanced sense of control. By effortless breathing, the authors refer to their approach to breath training, which involves a slow, comfortable respiration, larger volume of air exchange, and a reliance upon action of the muscles of the diaphragm rather than the chest (Peper, 1990). For more instructions see the recent blog, A breath of fresh air: Improve health with breathing.
Slowing breathing helps to limit the sighs common to rapid thoracic breathing—sighs that often precede menopausal hot flashes. Effortless breathing is associated with stress reduction—stress and mood swings are common concerns of women suffering from PMS. In a pilot study Bier, Kazarian, Peper, and Gibney (2003) at San Francisco State University (SFSU) observed that when the subject practiced diaphragmatic breathing throughout the month, combined with Autogenic Training, her premenstrual psychological symptoms (anger, depressed mood, crying) and premenstrual responses to stressors were significantly reduced as shown in Figure 1.
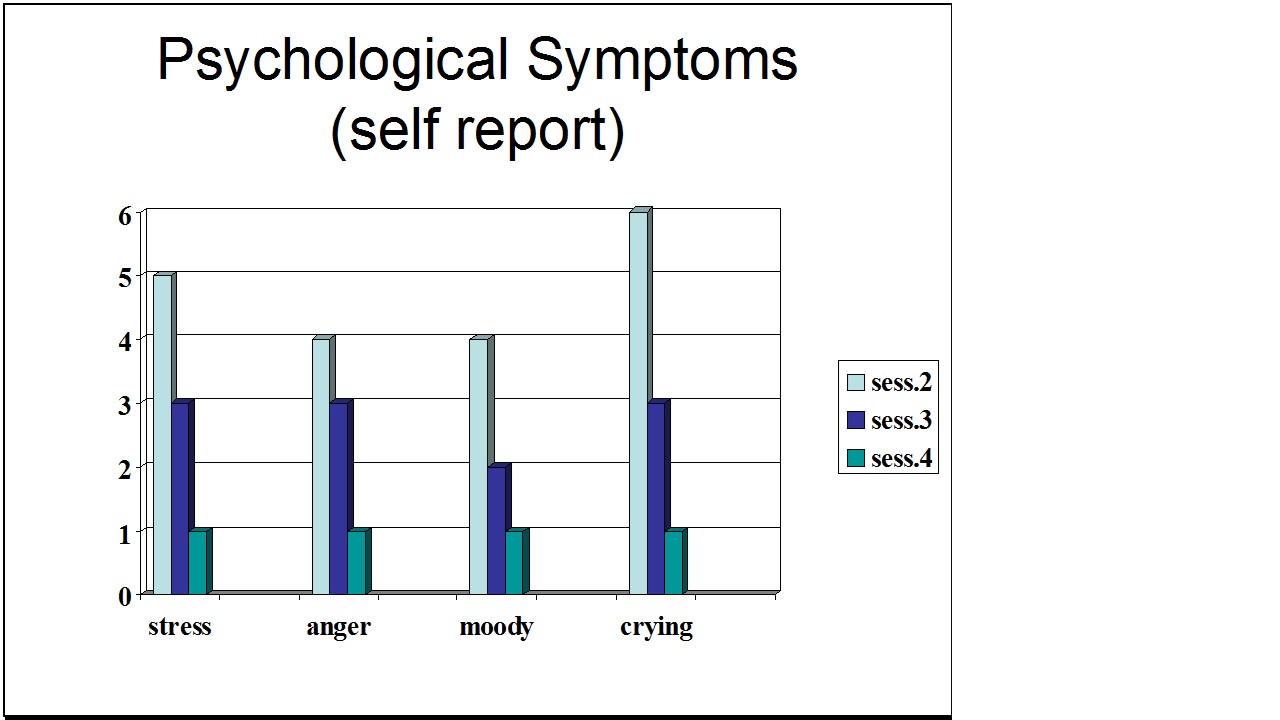
Figure 1. Student’s Individual Subjective Rating in Response to PMS Symptoms.
In another pilot study at SFSU, Frobish, Peper, and Gibney (2003) trained a volunteer who suffered from frequent hot flashes to breathe diaphragmatically. The training goals included modifying breathing patterns, producing a Respiratory Sinus Arrhythmia (RSA), and peripheral hand warming. RSA refers to a pattern of slow, regular breathing during which variations in heart rate enter into a synchrony with the respiration. Each inspiration is accompanied by an increase in heart rate, and each expiration is accompanied by a decrease in heart rate (with some phase differences depending on the rate of breathing). The presence of the RSA pattern is an indication of optimal balance between sympathetic and parasympathetic nervous activity.
During the 11-day study period, the subject charted the occurrence of hot flashes and noted a significant decrease by day 5. However, on the evening of day 7 she sprained her ankle and experienced a dramatic increase in hot flashes on day 8. Once the subject recognized her stress response, she focused more on breathing and was able to reduce the flashes as shown in Figure 2. 
Figure 2. Subjective rating of intensity, frequency and bothersomeness of hot flashes. The increase in hot flashes coincided with increased frustration about an ankle injury.
Our clinical experience confirms the SFSU pilot studies and the previously referenced research by Freedman and Woodward (1992) and Freedman et al. (1995). When arousal is lowered and breathing is effortless, women are better able to cope with stress and report a reduction in symptoms. Habitual rapid thoracic breathing tends to increase arousal while slower breathing, especially slower exhalation, tends to relax and reduce arousal. Learning and then applying effortless breathing reduces excessive sympathetic arousal. It also interrupts the cycle of cognitive activation, anxiety, and somatic arousal. The anticipation and frustration at having hot flashes becomes the cue to shift attention and “breathe slower and lower.” This process stops the cognitively mediated self-activation.
Successful self-regulation and the return to health begin with cognitive reframing: We are not only a genetic biological fixed (deficient) structure but also a dynamic changing system in which all parts (thoughts, emotions, behavior, diet, stress, and physiology) affect and are effected by each other. Within this dynamic changing system, there is an opportunity to implement and practice behaviors and life patterns that promote health.
Learning Diaphragmatic Breathing with and without Biofeedback
Although there are many strategies to modify respiration, biofeedback monitoring combined with respiration training is very useful as it provides real-time feedback. Chest and abdominal movement are recorded with strain gauges and heart rate can be monitored either by an electrocardiogram (EKG) or by a photoplethysmograph sensor on a finger or thumb. Peripheral temperature and electrodermal activity (EDA) biofeedback are also helpful in training. The training focuses on teaching effortless diaphragmatic breathing and encouraging the participant to practice many times during the day, especially when becoming aware of the first sensations of discomfort.
Learning and integrating effortless diaphragmatic breathing into daily life is one of the biofeedback strategies that has been successfully used as a primary or adjunctive/complementary tool for the reversal of disorders such as hypertension, migraine headaches, repetitive strain injury, pain, asthma and anxiety (Schwartz & Andrasik, 2003), as well as hot flashes and PMS.
The biofeedback monitoring provides the trainer with a valuable tool to:
- Observe & identify: Dysfunctional rapid thoracic breathing patterns, especially in response to stressors, are clearly displayed in real-time feedback.
- Demonstrate & train: The physiological feedback display helps the person see that she is breathing rapidly and shallowly in her chest with episodic sighs. Coaching with feedback helps her to change her breathing pattern to one that promotes a more balanced homeostasis.
- Motivate, persuade and change beliefs: The person observes her breathing patterns change concurrently with a felt shift in physiology, such as a decrease in irritability, or an increase in peripheral temperature, or a reduction in the incidence of hot flushes. Thus, she has a confirmation of the importance of breathing diaphragmatically.
In addition, we suggest exercises that integrate verbal and kinesthetic instructions, such as the following: “Exhale gently,” and “Breathe down your leg with a partner.”
Exhale Gently:
Imagine that you are holding a baby. Now with your shoulders relaxed, inhale gently so that your abdomen widens. Then as you exhale, purse your lips and very gently and softly blow over the baby’s hair. Allow your abdomen to narrow when exhaling. Blow so softly that the baby’s hair barely moves. At the same time, imagine that you can allow your breath to flow down and through your legs. Continue imagining that you are gently blowing on the baby’s hair while feeling your breath flowing down your legs. Keep blowing very softly and continuously.
Practice exhaling like this the moment that you feel any sensation associated with hot flashes or PMS symptoms. Smile sweetly as you exhale.
Breathe Down Your Legs with a Partner
Sit or lie comfortably with your feet a shoulder width apart. As you exhale softly whisper the sound “Haaaaa….” Or, very gently press your tongue to your pallet and exhale while making a very soft hissing sound.
Have your partner touch the side of your thighs. As you exhale have your partner stroke down your thighs to your feet and beyond, stroking in rhythm with your exhalation. Do not rush. Apply gentle pressure with the stroking. Do this for four or five breaths.
Now, continue breathing as you imagine your breath flowing through your legs and out your feet.
During the day remember the feeling of your breath flowing downward through your legs and out your feet as you exhale.
Learning Strategies in Biofeedback Assisted Breath Training
Common learning strategies that are associated with the more successful amelioration of hot flashes and PMS include:
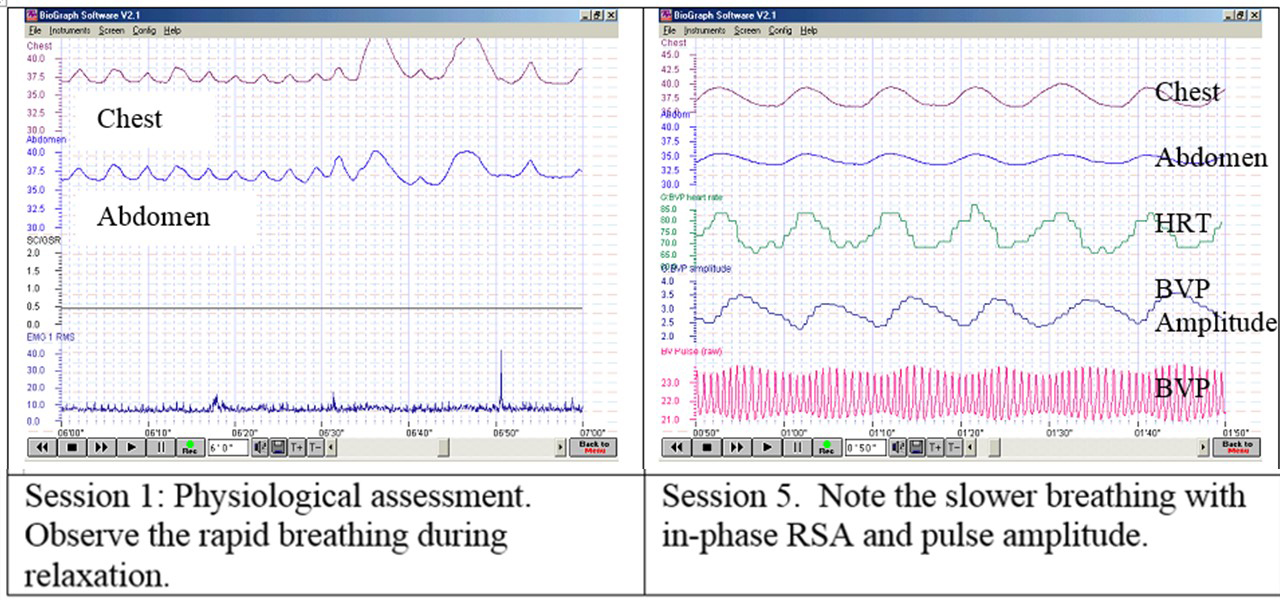
- Master effortless diaphragmatic breathing, and concurrently increase respiratory sinus arrhythmia (RSA). Instead of breathing rapidly, such as at 18 breaths per minute, the person learns to breathe effortlessly and slowly (about 6 to 8 breaths per minute). This slower breathing and increased RSA is an indication of sympathetic-parasympathetic balance as shown in Figure 3.
- Practice slow effortless diaphragmatic breathing many times during the day and, especially in response to stressors.
- Use the physical or emotional sensations of a hot flash or mood alteration as the cue to exhale, let go of anxiety, breathe diaphragmatically and relax.
- Reframe thoughts by accepting the physiological processes of menstruation or menopause, and refocus the mind on positive thoughts, and breathing rhythmically.
- Change one’s lifestyle and allow personal schedules to flow in better balance with individual, dynamic energy levels.
 Figure 3. Physiological Recordings of a Participant with PMS. This subject learned effortless diaphragmatic breathing by the fifth session and experienced a significant decrease in symptoms.
Figure 3. Physiological Recordings of a Participant with PMS. This subject learned effortless diaphragmatic breathing by the fifth session and experienced a significant decrease in symptoms.
Generalizing skills and interrupting the pattern
The limits of self-regulation are unknown, often held back only by the practitioner’s and participant’s beliefs. Biofeedback is a powerful self-regulation tool for individuals to observe and modify their covert physiological reactions. Other skills that augment diaphragmatic breathing are Quieting Reflex (Stroebel, 1982), Autogenic Training (Schultz & Luthe, 1969), and mindfulness training (Kabat-Zinn, 1990). In all skill learning, generalization is a fundamental factor underlying successful training. Integrating the learned psychophysiological skills into daily life can significantly improve health—especially in anticipation of and response to stress. The anticipated stress can be a physical, cognitive or social trigger, or merely the felt onset of a symptom.
As the person learns and applies effortless breathing to daily activities, she becomes more aware of factors that affect her breathing. She also experiences an increased sense of control: She can now take action (a slow effortless breath) in moments when she previously felt powerless. The biofeedback-mastered skill interrupts the evoked frustrations and irritations associated with an embarrassing history of hot flashes or mood swings. Instead of continuing with the automatic self-talk, such as “Damn, I am getting hot, why doesn’t it just stop?” (language fueling sympathetic arousal), she can take a relaxing breath in response to the internal sensations, stop the escalating negative self-talk and allows more acceptance—a process reducing sympathetic arousal.
In summary, effortless breathing appears to be a non-invasive behavioral strategy to reduce hot flashes and PMS symptoms. Practicing effortless diaphragmatic breathing contributes to a sense of control, supports a healthier homeostasis, reduces symptoms, and avoids the negative drug side effects. We strongly recommend that effortless diaphragmatic breathing be taught as the first step to reduce hot flashes and PMS symptoms.
I feel so much cooler. I can’t believe that my hand temperature went up. I actually feel calmer and can’t even feel the threat of a hot flash. Maybe this breathing does work! –Menopausal patient after initial training in diaphragmatic breathing
References
Bier, M., Kazarian, D., Peper, E., & Gibney, K. (2003). Reducing the severity of PMS symptoms with diaphragmatic breathing, autogenic training and biofeedback. Unpublished report.
Freedman, R.R., & Woodward, S. (1992). Behavioral treatment of menopausal hot flushes: Evaluation by ambulatory monitoring. American Journal of Obstetrics and Gynecology, 167 (2), 436-439.
Freedman, R.R., Woodward, S., Brown, B., Javaid, J.I., & Pandey, G.N. (1995). Biochemical and thermoregulatory effects of behavioral treatment for menopausal hot flashes. Menopause: The Journal of the North American Menopause Society, 2 (4), 211-218.
Frobish,C., Peper, E. & Gibney, K. H. (2003). Menopausal Hot Flashes: A Self-Regulation Case Study. Poster presentation at the 35th Annual Meeting of the Association for Applied Psychophysiology and Biofeedback. Abstract in: Applied Psychophysiology and Biofeedback. 29 (4), 302.
Goodale, I.L., Domar, A.D., & Benson, H. (1990). Alleviation of Premenstrual Syndrome symptoms with the relaxation response. Obstetrics and Gynecological Journal, 75 (5), 649-55.
Hays, J., Ockene, J.K., Brunner, R.L., Kotchen, J.M., Manson, J.E., Patterson, R.E., Aragaki, A.K., Shumaker, S.A., Brzyski, R.G., LaCroix, A.Z., Granek, I.A, & Valanis, B.G., Women’s Health Initiative Investigators. (2003). Effects of estrogen plus progestin on health-related quality of life. New England Journal of Medicine, 348, 1839-1854.
Humphries, K.H.., & Gill, s. (2003). Risks and benefits of hormone replacement therapy: the evidence speaks. Canadian Medical Association Journal, 168(8), 1001-10.
Kabat-Zinn, J. (1990). Full catastrophe living. New York: Delacorte Press.
Luthe, W. & Schultz, J.H. (1969). Autogenic therapy: Vol II: Medical applications. New York: Grune & Stratton.
Mathew, R.J.; Claghorn, J.L.; Largen, J.W.; & Dobbins, K. (1979). Skin Temperature control for premenstrual tension syndrome:A pilot study. American Journal of Clinical Biofeedback, 2 (1), 7-10.
Peper, E. (1990). Breathing for health. Montreal: Thought Technology Ltd.
Schultz, J.H., & Luthe, W. (1969). Autogenic therapy: Vol 1. Autogenic methods. New York: Grune and Stratton.
Schwartz, M.S. & Andrasik, F.(2003). Biofeedback: A practitioner’s guide, 3nd edition. New York: Guilford Press.
Shumaker, S.A., Legault, C., Thal, L., Wallace, R.B., Ockene, J., Hendrix, S., Jones III, B., Assaf, A.R., Jackson, R. D., Morley Kotchen, J., Wassertheil-Smoller, S.; & Wactawski-Wende, J. (2003). Estrogen plus progestin and the incidence of dementia and mild cognitive impairment in post menopausal women: The Women’s Health Initiative memory study: A randomized controlled trial. Journal of the American Medical Association, 289 (20), 2651-2662.
Stearns, V., Beebe, K. L., Iyengar, M., & Dube, E. (2003). Paroxetine controlled release in the treatment of menopausal hot flashes. Journal of the American Medical Association, 289 (21), 2827-2834.
Stroebel, C. F. (1982). QR, the quieting reflex. New York: G. P. Putnam’s Sons.
van Dixhoorn, J.J. (1998). Ontspanningsinstructie Principes en Oefeningen (Respiration instructions: Principles and exercises). Maarssen, Netherlands: Elsevier/Bunge.
Wassertheil-Smoller, S., Hendrix, S., Limacher, M., Heiss, G., Kooperberg, C., Baird, A., Kotchen, T., Curb, Dv., Black, H., Rossouw, J.E., Aragaki, A., Safford, M., Stein, E., Laowattana, S., & Mysiw, W.J. (2003). Effect of estrogen plus progestin on stroke in postmenopausal women: The Women’s Health Initiative: A randomized trial. Journal of the American Medical Association, 289 (20), 2673-2684.
Wyeth Pharmaceuticals (2003, June 4). A message from Wyeth: Recent reports on hormone therapy and where we stand today. San Francisco Chronicle, A11.
*We thank Candy Frobish, Mary Bier and Dalainya Kazarian for their helpful contributions to this research.
**For communications contact: Erik Peper, Ph.D., Institute for Holistic Healing Studies, San Francisco State University, 1600 Holloway Avenue, San Francisco, CA 94132; Tel: (415) 338 7683; Email: epeper@sfsu.edu; website: http://www.biofeedbackhealth.org; blog: http://www.peperperspective.come
Relax and Relax More*
Posted: February 6, 2015 Filed under: Uncategorized | Tags: awareness, electromyography, muscle biofeedback, relaxation, shoulder pain 4 CommentsAfter raising my shoulders and then relaxing it, I felt relaxed. I was totally surprised that the actual muscle tension recorded with surface electromyographic (SEMG) still showed tension. Only when I gave myself the second instruction, relax even more, that my SEMG activity decreased.
In our experiences, we (Vietta E. Wilson and Erik Peper, 2014) have observed that muscle tension often does not decrease completely after a person is instructed to relax. The complete relaxation only occurs after the second instruction, relax more, let go, drop, or feel the heaviness of gravity. The person is totally unaware that after the first relaxation their muscless have not totally relaxed. Their physiology does not match their perception (Peper et, 2010; Whatmore & Kohli, 1974). The low level of muscle tension appears more prevalent in people who are have a history of muscle stiffness or pain, or in athletes whose coaches report they look ‘tight.’ It is only after the second command, relax and release even more, that the individual notices a change and experiences a deeper relaxation.
The usefulness of giving a second instruction, relax more, after the first instruction, relax, is illustrated below by the surface electromyographic (SEMG) recording from the upper left and right trapezius muscle of a 68 year old male with chronic back pain. While sitting upright without experiencing any pain, he was instructed to lift his shoulders, briefly hold the tension, and then relax (Sella, 1997; Peper et al, 2008). When the SEMG of the trapezius muscles did not decrease to the relaxed state, he was asked to relax more as is shown in Figure 1.

Figure 1. SEMG recordings of the left and right upper trapezius when the client was asked to lift his shoulders, hold, relax, and relax more. Only after the second instruction did the muscle tension decrease to the relaxed baseline level. Reprinted from Wilson and Peper, 2014.
Although the subject felt that he was relaxed after the first relaxation instruction, he continued to hold a low level of muscle tension. We have observed this same process in hundreds of clients and students while teaching SEMG guided relaxation and progressive muscle relaxation.
For numerous people, even the second commands to relax even more is not sufficient for the SEMG to show muscle relaxation and for them to ‘feel’ or know when they are totally relaxed. These individuals may benefit from SEMG biofeedback to identify and quantify the degree of muscle tension. With this information the person can make the invisible muscle contractions ‘ visible,’ the un-felt tension ‘felt,’ and thus develop awareness and control (Peper et al, 2014).
In summary
- Instruct people to relax after tightening and then repeat the instruction to relax even more.
- Use surface electromyography to confirm whether the person’s subjective experience of being muscularly relaxed corresponds to the actual physiological SEMG recording.
- Use the SEMG biofeedback to train the person to increase awareness and learn relaxation (Peper et al, 2014).
- Read the complete article from which this blog was adapted: Wilson, E. & Peper, E. (2014). Clinical Tip: Relax and Relax More. 42(4), 163-164.
References
Peper, E., Booiman, A., Lin, I-M., & Shaffer, F. (2014). Making the Unaware Aware-Surface electromyography to unmask tension and teach awareness. Biofeedback. 42(1), 16-23.
Peper, E., Booiman, A., Tallard, M., & Takebayashi, N. (2010). Surface electromyographic biofeedback to optimize performance in daily life: Improving physical fitness and health at the worksite. Japanese Journal of Biofeedback Research, 37(1), 19-28.
Peper, E., Tylova, H., Gibney, K.H., Harvey, R., & Combatalade, D. (2008). Biofeedback mastery-An experiential teaching and self-training manual. Wheat Ridge, CO: AAPB.
*This blogpost is adapted from, Wilson, E. & Peper, E. (2014). Clinical tip: Relax and relax more. Biofeedback. 42(4), 163-164.
The surprising and powerful links between posture and mood
Posted: February 3, 2015 Filed under: Uncategorized | Tags: anxiety, depression, mind-body, posture, stress, stress management Leave a commentEnjoy Vivian Giang’s superb blog, The surprising and powerful links between posture and mood, published by Fast Company and reprinted with permission. It summarizes in a very readable way how posture affects health and well being.
The Surprising and Powerful Links between Posture and Mood
Why feeling taller tricks your brain into making you feel more confident and why your smartphone addiction might be making you depressed.
The next time you’re feeling sad and depressed, pay close attention to your posture. According to cognitive scientists, you’ll likely be slumped over with your neck and shoulders curved forward and head looking down.
While it’s true that you’re sitting this way because you’re sad, it’s also true that you’re sad because you’re sitting this way. This philosophy, known as embodied cognition, is the idea that the relationship between our mind and body runs both ways, meaning our mind influences the way our body reacts, but the form of our body also triggers our mind.
In large part due to Amy Cuddy’s widly popular 2012 TED talk, most of us know that two minutes of “power poses” a day can change how we feel about ourselves. This isn’t just about displaying confidence to others around; this is about actually changing your hormones—increased levels of testosterone and decreased levels of cortisol, or the stress hormone, in the brain.
“The brain has an area that reflects confidence, but once that area is triggered it doesn’t matter exactly how it’s triggered,” says Richard Petty, professor of psychology at Ohio State University. “It can be difficult to distinguish real confidence from confidence that comes from just standing up straight … these things go both ways just like happiness leads to smiling, but also smiling leads to happiness.”
When it comes to posture, Petty explains that the way we ultimately feel has a lot to do with the associations we have with being taller. For example, if you take two people and you put one on a chair that’s above the other person, the one that’s looking down will feel more powerful because “we have all these associations” with height and power that “gets triggered automatically when certain movements are made,” he says. The function of your body posture tells your brain that you’re powerful, which, in turn, affects your attitude.
In a 2009 study published in the European Journal of Social Psychology, Petty along with other researchers instructed 71 college students to either “sit up straight” and “push out [their] chest” or “sit slouched forward” with their “face looking at [their] knees.” While holding their assigned posture, the students were asked to list either three positive or negative personal traits they thought would contribute to their future job satisfaction and professional performance. Afterward, the students were asked to take a survey where they rated themselves on how well they thought they would perform as a future professional.
The researchers found that how the students rated themselves depended on the posture they kept when they wrote the positive or negative traits. Those who were in the upright position believed in the positive and negative traits they wrote down while those in the slouched over position weren’t convinced of their positive or negative traits. In other words, when the students were in the upright, confident position, they trusted their own thoughts whether those thoughts were positive or negative. On the other hand, when the students sat in a powerless position, they didn’t trust anything they wrote down whether it was positive or negative.
However, those in the upright position likely had an easier time thinking of “empowering, positive” traits about themselves to write down while those in the slouched over position probably had an easier time recalling “hopeless, helpless, powerless, and negative” feelings, according to Erik Peper, professor of Holistic Health at San Francisco State University.
In a series of experiments, Peper found that sitting in a collapsed, helpless position makes it easier for negative thoughts and memories to appear while sitting in an upright, powerful position makes it easier to have empowering thoughts and memories.
“Emotions and thoughts affect our posture and energy levels; conversely, posture and energy affect our emotions and thoughts,” says one of Peper’s studies from 2012, and two minutes of skipping versus walking in a slouched position can make a significant difference on our energy levels. Like Cuddy, Peper’s research finds that it only takes two minutes to change your hormones, meaning you can basically change the chemistry in your brain while waiting for your food to heat up in the microwave.
Since posture affects our mood and thoughts so much, the increase of collapsed sitting and walking—from sitting in front of our computer to looking down at our smartphones—may very much have an effect on the rise of depression in recent years. Peper and his team of researchers suggest that posture is a significant contributor to decreased energy levels and depression. Slouching is also known to result in frequent headaches and neck and shoulder pains.
With so much research proving the influence posture has on our mind, Peper suggests hanging photos of people you love slightly higher on the wall or above your desk so that you have to look up. Also, adjust your rear view mirror slightly higher so that you have to sit up taller while driving. If you need reminders, Petty advises setting reminders on your phone, computer, or even a Post-It note. When you do have negative thoughts, instead of validating them by slumping over or bending your head, Petty says that you should write them down on a piece of paper, then throw that piece of paper away in the trash.
“People who throw those negative thoughts into the trash can are less affected by them then people who had the same thoughts but symbolically put them in their pocket,” he says. “It’s this idea that it’s not what we think that’s important; it’s how much we trust what we think.”
Reprinted by permission from Vivian Giang
Overdiagnosed: Should I have more tests or treatments?
Posted: February 1, 2015 Filed under: Uncategorized | Tags: cancer, diagnosis, health, medication, prevention 2 CommentsOne Computerized tomography (CT) scan of the abdomen and pelvis will expose you to more radiation than the residents of Fukushima, Japan absorbed after the Fukushima Daiichi nuclear power plant accident in 2011. –Consumer Reports, March 2015, Vol.80 No.3, 39.
High-risk patients with heart failure and cardiac arrest hospitalized in teaching hospitals had a significantly lower 30-day mortality when admitted during dates of national cardiology meetings (70% survival when doctors attended meeting as compared to 60% survival when doctors did not attend the meetings). –-Jena et al, 2014.
There are so many questions
I feel healthy but worry that cancer could be lurking in the background, should I do a preventative body scan?
I sometimes have slightly higher blood pressure especially when the doctor measures it. It is probably borderline, should I go on medication?
Should I have my PSA tested?
I am a healthy fifty year old, should I have a mammogram?
Should I have an annual physical?
In the quest to stay healthy or prevent disease, we are bombarded by information that preventative testing would save lives and improve health. Only in the United States and New Zealand allow direct to consumer medical advertising which tends to increase excessive drug use and medical testing (Liang & Mackey, 2011). The messages imply that medical screening and testing (e.g., body scan or stress tests) can identify early stages of a disease and implying that earlier treatment will improve quality of life and survival. Similar messages encourage basically healthy people to take drugs for borderline conditions (e.g., borderline hypertension, osteopenia, increased cholesterol levels. What is not shared is the possible risk of unnecessary medical interventions or the harm caused by drug or treatment side effects especially when they are used for a long time period. When unbiased research such as the Cochran Reviews are done, even the annual physical exam appears to offer no benefits (Krogsbøll et al, 2013). Similarly, mammograms and PSA testing for a healthy population appears to offer no benefits and may increase risks. It is truly difficult to accept that an annual health check up is worthless or that a routine mammogram or PSA test may do more harm than good since for many years the public message has been the opposite: to get more screening and testing. There are many reasons for this approach such as:
- Genuine belief, although not evidence based, that an early intervention and more testing would reduce suffering.
- Financial incentives for the parties that perform testing and preventative screening or encourage increased drugs sales for borderline conditions for which the risk and benefits are not well documented.
- Fear of lawsuits by medical providers. If a patient develops an illness which possibly could have been diagnosed by screening, even though the screening may not have affected the actual outcome, the health professional could be sued.
Become an informed consumer
When you have a symptom and do not feel well, see your doctor and get diagnosed, it may safe your life. At the same time be an educated consumer and when unexpected findings are discovered and not related to your specific symptom/complaint, ask questions before agreeing to have more tests or treatments. Ask your provider some of the following questions which were initially outlined by Dr. Eugene Robins (1984):
- Why are you doing this test or procedure?
- What are the risks and what are the benefits?
- What are the risks of treatment and what are the benefits of treatment?
- How accurate is the test?
- How will the test results change the treatment strategy?
- Are there less invasive strategies that could be used? Be very careful of exposing yourself and especially children to CT scans. It is estimated that for every 1000 children who have an abdominal CT scan, one will develop cancer as a result (2015, Consumer Report, March 16).
To be able to navigate the complexities of diagnosis and to understand the risks and benefits of treatment and testing, read the recent two articles in the New York Times, Can this treatment help me? There is a statistic for that, How to Measure a Medical Treatment’s Potential for Harm and the superb book, Over-diagnosed-Making people sick in the pursuit of health, by Drs. H. Gilbert Welch, Lisa M Schwartz, and Steven Woloshin who are professors at Darthmouth Institute for Health Policy and Clinical Practice. This book is a must read for every patient and health care provider. 
References:
(2015). Overexposed. Consumer Reports, 80(3), 37-41. http://www.consumerreports.org/cro/2015/01/when-to-skip-ct-scans-and-x-rays/index.htm
Carroll, A.E. & Frakt, A. (2015). How to Measure a Medical Treatment’s Potential for Harm. New York Times, February 2.
Frakt, A. & Carroll, A.T. (2015). Can This Treatment Help Me? There’s a Statistic for That, New York Times, January 26.
Jena, A. B., Prasad, V., Goldman, D. P., & Romley, J. (2014). Mortality and Treatment Patterns Among Patients Hospitalized With Acute Cardiovascular Conditions During Dates of National Cardiology Meetings. JAMA internal medicine. doi:10.1001/jamainternmed.2014.6781 http://www.drperlmutter.com/wp-content/uploads/2015/01/Cardiac-outcome.pdf
Krogsbøll, L. T., Jørgensen, K. J., & Gøtzsche, P. C. (2013). General health checks in adults for reducing morbidity and mortality from disease. JAMA, 309(23), 2489-2490. http://drkney.com/pdfs/WAC_A_061913.pdf
Liang, B. A., & Mackey, T. (2011). Direct-to-consumer advertising with interactive internet media: global regulation and public health issues. JAMA, 305(8), 824-825. http://jama.jamanetwork.com/article.aspx?articleid=645713
Robins, E. D. (1984). Matter of Life & Death: Risks vs. Benefits of Medical Care. New York: W.H. Freeman and Company
Welch, H.G., Schwartz, L.M., & Woloshin, S. (2011). Over-diagnosed-Making people sick in the pursuit of health. Boston: Beacon Press.
