Posture and mood: implications and applications to health and therapy
Posted: November 28, 2017 Filed under: Neck and shoulder discomfort, posture, self-healing, Uncategorized | Tags: back pain, electromyography, ergonomics, neck and shoulder tension, posture, spinal alignment, stress management 7 CommentsThis blog has been reprinted from: Peper, E., Lin, I-M, & Harvey, R. (2017). Posture and mood: Implications and applications to therapy. Biofeedback.35(2), 42-48.
Slouched posture is very common and tends to increase access to helpless, hopeless, powerless and depressive thoughts as well as increased head, neck and shoulder pain. Described are five educational and clinical strategies that therapists can incorporate in their practice to encourage an upright/erect posture. These include practices to experience the negative effects of a collapsed posture as compared to an erect posture, watching YouTube video to enhance motivation, electromyography to demonstrate the effect of posture on muscle activity, ergonomic suggestions to optimize posture, the use of a wearable posture biofeedback device, and strategies to keep looking upward. When clients implement these changes, they report a more positive outlook and reduced neck and shoulder discomfort.
Background
Most people slouch without awareness when looking at their cellphone, tablet, or the computer screen (Guan et al., 2016) as shown in Figure 1. Many clients in psychotherapy and in biofeedback or neurofeedback training experience concurrent rumination and depressive thoughts with their physical symptoms. In most therapeutic sessions, clients sit in a comfortable chair, which automatically creates a posterior pelvic tilt and encourages the spine to curve so that the client sits in a slouched position. While at home, they sit on an easy chair or couch, which lets them slouch as they watch TV or surf the web.
Figure 1. (A). Employee working on his laptop. (B). Boy with ADHD being trained with neurofeedback in a clinic. (C). Student looking at cell phone. When people slouch and look at the screen, they tend to slouch and scrunch their neck.
In many cases, the collapsed position also causes people to scrunch their necks, which puts pressure on their necks that may contribute to developing headache or becoming exhausted. Repetitive strain on the neck and cervical spine may trigger a cervical neuromuscular syndrome that involves chronic neck pain, autonomic imbalance and concomitant depression and anxiety (Matsui & Fujimoto, 2011), and may contribute to vertebrobasilar insufficiency –a reduction in the blood supply to the hindbrain through the left and right vertebral arteries and basilar arteries (Kerry, Taylor, Mitchell, McCarthy, & Brew, 2008). From a biomechanical perspective, slouching also places more stress is on the cervical spine, as shown in Figure 2. When the neck compression is relieved, the symptoms decrease (Matsui & Fujimoto, 2011).
 Figure 2. The more the head tilts forward, the more stress is placed on the cervical spine. Reproduced by permission from: Hansraj, K. K. (2014). Assessment of stresses in the cervical spine caused by posture and position of the head. Surgical Technology International, 25, 277–279.
Figure 2. The more the head tilts forward, the more stress is placed on the cervical spine. Reproduced by permission from: Hansraj, K. K. (2014). Assessment of stresses in the cervical spine caused by posture and position of the head. Surgical Technology International, 25, 277–279.
Most people are totally unaware of slouching positions and postures until they experience neck, shoulder, and/or back discomfort. Neither clients nor therapists are typically aware that slouching may decrease energy levels and increase the prevalence of negative (hopeless, helpless, powerless, or defeated) memories and thoughts (Peper & Lin, 2012; Peper et al, 2017)
Recommendations for posture awareness and training in treatment/education
The first step in biofeedback training and therapy is to systematically increase awareness and training of posture before attempting further bio/neurofeedback training and/or cognitive behavior therapy. If the client is sitting in a collapsed position in therapy, then it will be much more difficult for them to access positive thoughts, which interferes with further training and effective therapy. For example, research by Tsai, Peper, & Lin (2016) showed that engaging in positive thinking while slouched requires greater mental effort then when sitting erect. Sitting erect and tall contributes to elevated mood and positive thinking. An upright posture supports positive outcomes that may be akin to the beneficial effects of exercise for the treatment of depression (Schuch, Vancampfort, Richards, Rosenbaum, Ward, & Stubbs., 2016).
Most people know that posture affects health; however, they are unaware of how rapidly a slouching posture can impact their physical and mental health. We recommend the following educational and clinical strategies to teach this awareness.
- Practicing activities that raise awareness about a collapsed posture as compared to an erect posture
Guide clients through the practices so that they experience how posture can affect memory recall, physical strength, energy level, and possible triggering of headaches.
A. The effect of collapsed and erect posture on memory recall. Participants reported that it is much easier evoke powerless, hopeless, helpless, and defeated memories when sitting in a collapsed position than when sitting upright. Guide the client through the procedure described in the article, How posture affects memory recall and mood (Peper, Lin, Harvey, and Perez, 2017) and in the blog Posture affects memory recall and mood.
B. The effects of collapsed and erect posture on perceived physical strength. Participants experience much more difficulty in resisting downward pressure at the wrist of an outstretched arm when slouched rather than upright. Guide the client through the exercise described in the article, Increase strength and mood with posture (Peper, Booiman, Lin, & Harvey, 2016) and the blog, Increase strength and mood with posture.
C. The effect of slouching versus skipping on perceived energy levels. Participants experience a significant increase in subjective energy after skipping than walking slouched. Guide the client through the exercises as described in the article, Increase or decrease depression—How body postures influence your energy level (Peper & Lin, 2012).
D. The effect of neck compression to evoke head pressure and headache sensations. In our unpublished study with students and workshop participants, almost all participants who are asked to bring their head forward, then tilt the chin up and at the same time compress the neck (scrunching the neck), report that within thirty seconds they feel a pressure building up in the back of the head or the beginning of a headache. To their surprise, it may take up to 5 to 20 minutes for the discomfort to disappear. Practicing similar awareness activities can be a useful demonstration for clients with dizziness or headaches to experience how posture can increase their symptoms.
- Watching a Youtube video to enhance motivation.
Have clients watch Professor Amy Cuddy’s 2012 TED (Technology, Entertainment, and Design) Talk, Your body language shape who you are, which describes the hormonal changes that occur when adapting a upright power versus collapsed defeated posture.
- Electromyographic (EMG) feedback to demonstrate how posture affects muscle activity.
Record EMG from muscles such as around the cervical spine, trapezius, frontalis, and masseters or beneath the chin (submental lead) to demonstrate that having the head is forward and/or the neck compressed will increase EMG activity, as shown in Figure 3.

Figure 3. Electromyographic recording of the muscle under the chin while alternating between bringing the head forward or holding it back, feeling erect and tall.
The client can then learn awareness of the head and neck position. For example, one client with severe concussion experienced significant increase in head pressure and dizziness when she slouched or looked at a computer screen as well as feeling she would never get better. She then practiced the exercise of alternating her awareness by bringing her head forward and then back, and then bringing her neck back while her chin was down, thereby elongating the neck while she continued to breathe. With her head forward, she would feel her molars touching and with her neck back she felt an increase in space between the molars. When she elongated her neck in an erect position, she felt the pressure draining out of her head and her dizziness and tinnitus significantly decrease.
- Assessing ergonomics to optimize posture.
Change the seated posture of both the therapist and the client during treatment and training. Although people may be aware of their posture, it is much easier to change the external environment so that they automatically sit in a more erect power posture. Possible options include:
A. Seat insert or cushions. Sit in upright chairs that encourage an anterior pelvic tilt by having the seat pan slightly lower in the front than in the back or using a seat insert to facilitate a more erect posture (Schwanbeck, Peper, Booiman, Harvey, & Lin, 2015) as shown in Figure 4.

Figure 4. An example of how posture can be impacted covertly when one sits on a seat insert that rotates the pelvis anteriorly (The seat insert shown in the diagram and used in research is produced by BackJoy™).
B. Back cushion. Place a small pillow or rolled up towel at the kidney level so that the spine is slight arched, instead of sitting collapsed, as shown in Figure 5.
 Figure 5. An example of how a small pillow, placed between the back of the chair and the lower back, changes posture from collapsed to erect.
Figure 5. An example of how a small pillow, placed between the back of the chair and the lower back, changes posture from collapsed to erect.
C. Check ergonomic and work site computer use to ensure that the client can sit upright while working at the computer. For some, that means checking their vision if they tend to crane forward and crunch their neck to read the text. For those who work on laptops, it means using either an external keyboard, a monitor, or a laptop stand so the screen is at eye level, as shown in Figure 6.
 Figure 6. Posture is collapsed when working on a laptop and can be improved by using an external keyboard and monitor. Reproduced by permission from: Bakker Elkhuizen. (n.d.). Office employees are like professional athletes! (2017).
Figure 6. Posture is collapsed when working on a laptop and can be improved by using an external keyboard and monitor. Reproduced by permission from: Bakker Elkhuizen. (n.d.). Office employees are like professional athletes! (2017).
- Wearable posture biofeedback training device
The wearable biofeedback device, UpRight™, consists of a small sensor placed on the spine and works as an app on the cell phone. After calibration the erect and slouched positions, the posture device gives vibratory feedback each time the participant slouches, as shown in Figure 7.
Figure 7. Illustration of a posture feedback device, UpRight™. It provides vibratory feedback to the wearer to indicate that they are beginning to slouch.
Clinically, we have observed that clients can learn to identify conditions that are associated with slouching, such as feeling tired, thinking depressive/hopeless thoughts or other situations that evoke slouching. When people wear a posture feedback device during the day, they rapidly become aware of these subjective experiences whenever they slouch. The feedback reminds them to sit in an erect position, and they subsequently report an improvement in health (Colombo et al., 2017). For example, a 26-year-old man who works more than 8 hours a day on computer reported, “I have an improved awareness of my posture throughout my day. I also notice that I had less back pain at the end of the day.”
- Integrating posture awareness and position changes throughout the day
After clients have become aware of their posture, additional training included having them observe their posture as well and negative changes in mood, energy level or tension in their neck and head. When they become aware of these changes, they use it as a cue to slightly arch their back and look upward. If possible have the clients look outside at the tops of trees and notice details such as how the leaves and branches move. Looking at the details interrupts any ongoing rumination. At the same time, have them think of an uplifting positive memory. Then have them take another breath, wiggling, and return to the task at hand. Recommend to clients to go outside during breaks and lunchtime to look upward at the trees, the hills, or the clouds. Each time one is distracted, return to appreciate the natural patterns. This mental break concludes by reminding oneself that humans are like trees.
Trees are rooted in the earth and reach upward to the light. Despite the trauma of being buffeted by the storms, they continue to reach upward. Similarly, clouds reflect the natural beauty of the world, and are often visible in the densest city environment. The upward movement reflects our intrinsic resilience and growth. –Erik Peper
Have clients place family photos and art slightly higher on the wall at home so they automatically look upward to see the pictures. A similar strategy can be employed in the office, using art to evoke positive feelings. When clients integrate an erect posture into their daily lives, they experience a more positive outlook and reduced neck and shoulder discomfort.
Compliance with Ethical Standards:
Conflict of Interest: Author Erik Peper has received donations of 15 UpRight posture feedback devices from UpRight (http://www.uprightpose.com/) and 12 BackJoy seat inserts from Backjoy (https://www.backjoy.com) for use in research. Co-authors I-Mei Lin and Richard Harvey declare that they have no conflict of interest.
This report evaluated a convenience sample of a student classroom activity related to posture and the information was anonymous collected. As an evaluation of a classroom activity, this report of findings was exempted from Institutional Review Board oversight
References:
Bakker Elkhuizen. (n.d.). Office employees are like professional athletes! (2017). Retrieved from https://www.bakkerelkhuizen.com/knowledge-center/whitepaper-improving-work-performance-with-insights-from-pro-sports/
Cuddy, A. (2012). Your body language shapes who you are. Technology, Entertainment, and Design (TED) Talk, available at: www.ted.com/talks/amy_cuddy_your_body_language_shapes_who_you_are
We thank Frank Andrasik for his constructive comments.
Enhance Yoga with Biofeedback*
Posted: August 6, 2017 Filed under: Uncategorized | Tags: asana, awareness, biofeedback, Breathing, electromyography, meditation, posture, yoga Leave a commentHow can you demonstrate that yoga practices are beneficial?
How do you know you are tightening the correct muscles or relaxing the muscle not involved in the movement when practicing asanas?
How can you know that the person is mindful and not sleepy or worrying when meditating?
How do you know the breathing pattern is correct when practicing pranayama?
The obvious answer would be to ask the instructor or check in with the participant; however, it is often very challenging for the teacher or student to know. Many participants think that they are muscularly relaxed while in fact there is ongoing covert muscle tension as measured by electromyography (EMG). Some participants after performing an asana, do not relax their muscles even though they report feeling relaxed. Similarly, some people practice specific pranayama breathing practice with the purpose of restoring the sympathetic/parasympathetic system; however, they may not be doing it correctly. Similarly, when meditating, a person may become sleepy or their attention wanders and is captured by worries, dreams, and concerns instead of being present with the mantra. These problems may be resolved by integrating bio- and neurofeedback with yoga instruction and practice. Biofeedback monitors the physiological signals produced by the body and displays them back to the person as shown in Figure 1.

Figure 1: Biofeedback is a methodology by which the participant receives ongoing feedback of the physiological changes that are occurring within the body. Reproduced with permission from Peper et al, 2008.
With the appropriate biofeedback equipment, one can easily record muscle tension, temperature, blood flow and pulse from the finger, heart rate, respiration, sweating response, posture alignment, etc.** Neurofeedback records the brainwaves (electroencephalography) and can selectively feedback certain EEG patterns. In most cases participants are unaware of subtle physiological changes that can occur. However, when the physiological signals are displayed so that the person can see or hear the changes in their physiology they learn internal awareness that is associated with these physiological changes and learn mastery and control. Biofeedback and neuro feedback is a tool to make the invisible, visible; the unfelt, felt and the undocumented, documented.
Biofeedback can be used to document that a purported yoga practice actually affects the psychophysiology. For example, in our research with the Japanese Yogi, Mr. Kawakami, who was bestowed the title “Yoga Samrat’ by the Indian Yoga Culture Federation in 1983, we measured his physiological responses while breathing at two breaths a minute as well as when he inserted non-sterilized skewers through his tongue tongue (Arambula et al, 2001; Peper et al, 2005a; Peper et al, 2005b). The physiological recordings confirmed that his Oxygen saturation stayed normal while breathing two breaths per minute and that he did not trigger any physiological arousal during the skewer piercing. The electroencephalographic recordings showed that there was no response or registration of pain. A useful approach of using biofeedback with yoga instruction is to monitor muscle activity to measure whether the person is performing the movement appropriately. Often the person tightens the wrong muscles or performs with too much effort, or does not relax after performing. An example of recording muscle tension as shown in Figure 2.

Figure 2: Recording the muscle tension with Biograph Infinity while performing an asana.
In our research it is clear that many people are unaware that they tighten muscles. For example, Mcphetridge et al, (2011) showed that when participants were asked to bend forward slowly to touch their toes and then hang relaxed in a forward fold, most participants reported that they were totally relaxed in their neck. In actuality, they were not relaxed as their neck muscles were still contracting as recorded by electromyography (EMG). After muscle biofeedback training, they all learned to let their neck muscles be totally relaxed in the hanging fold position as shown in Figure 3 & 4.
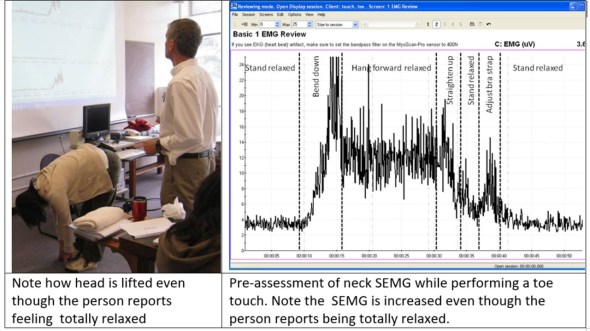
Figure 3: Initial assessment of neck SEMG while performing a toe touch. Reproduced from Harvey, E. & Peper, E. (2011).
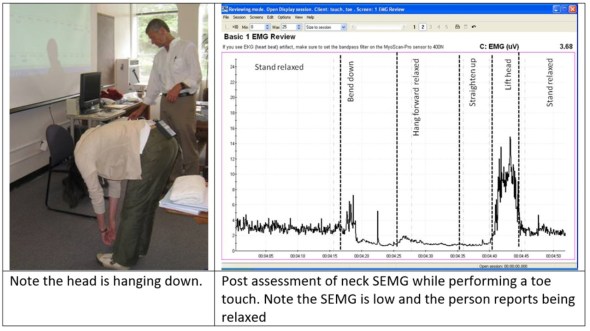
Figure 4: Toe touch after feedback training. The neck is now relaxed; however, the form is still not optimum. . Reproduced from Harvey, E. & Peper, E. (2011).
Thus, muscle feedback is a superb tool to integrate with teaching yoga so that participants can perform asanas with least amount of inappropriate tension and also can relax totally after having tightened the muscles. Biofeedback can similarly be used to monitor body posture during meditation. Often participants become sleepy or their attention drifts and gets captured by imagery or worries. When they become sleepy, they usually begin to slouch. This change in body position can be readily be monitored with a posture feedback device. The UpRight,™ (produced by Upright Technologies, Ltd https://www.uprightpose.com/) is a small sensor that is placed on the upper or lower spine and connects with Bluetooth to the cell phone. After calibration of erect and slouched positions, the device gives vibratory feedback each time the participant slouches and reminds the participant to come back to sitting upright as shown in Figure 5.

Figure 5: UpRigh™ device placed on the upper spine to provide feedback during meditation. Each time person slouches which often occurs when they become sleepy or loose meditative focus, the device provides feedback by vibrating.
Alternatively, the brainwaves patterns (electroencephalography could be monitored with neurofeedback and whenever the person drifts into sleep or becomes excessively aroused by worry, neurofeedback could remind the person to be let go and be centered. Finally, biofeedback can be used with pranayama practice. When a person is breathing approximately six breaths per minute heart rate variability can increase. This means that during inhalation heart rate increases and during exhalation heart rate decreases. When the person breathes so that the heart rate variability increases, it optimizes sympathetic/parasympathetic activity. There are now many wearable biofeedback devices that can accurately monitor heart rate variability and display the changes in heart rate as modulated by breathing.
Conclusion: Biofeedback is a useful strategy to enhance yoga practice as it makes the invisible visible. It allows the teacher and the student to become aware of the dysfunctional patterns that may be occurring beneath awareness.
References
*Reprinted from: Peper, E. (2017). Enhancing Yoga with Biofeedback. J Yoga & Physio.2(2).*55584. DOI: 10.19080/JYP.2017.02.555584
**Biofeedback and neurofeedback takes skill and training. For information on certification, see http://www.bcia.org Two useful websites are:
Winning the Gold in weight lifting-Using biofeedback, imagery and cognitive change*
Posted: June 12, 2017 Filed under: Uncategorized | Tags: biofeedback, electromyography, Imagery, peak performance, visualization, weight lifting 5 CommentsErik Peper [1], [2] and Jo Aita
“It was the best meet of my life.” -Jo Aita
Setting a personal best and winning the Gold medal is a remarkable feat. Jo Aita, age 46 and weighing 58 kg, set the Masters World Records and Masters Games Records in Snatch, Clean & Jerk and Total Olympic weight lifting at the World Masters Games in Auckland, New Zealand, April 26th, 2017. She lifted 71 kg in the Snatch and 86 kg in the Clean and Jerk Olympic lifts in the 45-49-year-old age group (see video in figure 1). What makes this more remarkable is that her combined lifts were 3 kilograms more than her life-time best in previous competition. She refuted the conventional wisdom that weight lifters peak in their mid to late twenties. There is hope for improvement as aging may not mean we have to decline.
Figure 1. Video of Jo Aita successful lift at the World Masters Games in Auckland, NZ., April 26, 2017.
There are many factors–and many more which we do not know–which contribute to this achievement such as genetics, diligent training and superb coaching at the Max’ Gym in Oakland as a member of Team Juggernauts. In the last three years, Jo Aita also incorporated biofeedback and visualization training to help optimize her performance. This report summarizes how breathing and electromyography feedback combined with imagery may have contributed to achieving her personal best[3]. As Jo Aita stated, “I recommend this to everyone and hope that you can work with athletes in my gym.”
Components of the 30 sessions of biofeedback, internal language and visualization training program
The training was started in September 2014 to reduce anxiety and improve performance. The components embedded in the training are listed sequentially; however, training did not occur sequentially. They were dynamically interwoven throughout the many sessions and augmented with homework practices, as well as storytelling of other people achieving success using similar approaches. The major components included:
1. Mastering effortless slow diaphragmatic breathing in which the abdomen expanded during inhalations and constricted during exhalation. The respiration feedback and training was recorded with BioGraph Infinity respiration sensors and recorded from the abdomen and upper chest. Her homework included monitoring situations where she held her breath and then anticipate breath holding by continuing to breathe. She also practiced slower breathing with heart rate variability feedback from a Stress Eraser. Practicing these allowed her to become centered and regenerate more quickly. As she stated, “It helped me during the day when I am anxious to calm down.” Throughout the training, the focus was to use breathing to rapidly regenerate after exertion especially after training.
2. Learning to relax her shoulder muscles with electromyography (EMG) feedback to regenerate and learn awareness of minimal trapezius muscle tension. She could use this awareness to identify her emotional reactivity (Peper, Booiman, Lin, & Shaffer, 2014). Often emotional reactivity increases muscle tension. She learned to relax here muscles quickly after muscle contractions to allow regeneration
3. Experiencing how cognition affect performance. This was initially demonstrated by arm resistance test. In this experiential practice, she extended her arm and attempted to resist the downward pressure applied to her wrist while she recalled either a hopeless, helpless, powerless or defeated memory or an empowered positive memory (for detailed description see, Gorter and Peper, pp 186-188, 2011). When she recalled the powerless memory she was significantly weaker than when she recalled the empowering memory. This experience demonstrated to her the power of her thoughts.
4. Rewriting failure into success. Each time she missed the lift, she would think, “I should not have done that,” or “I was doubtful or nervous during competition,” she shifted her focus to:
- Accepting what happened by acknowledging she did the best she could have done under the circumstances.
- Exploring how she could have done it differently and imagine herself doing it in the new optimum way.
- Using the trigger of the beginning thought of failure or defeat to evoke the new empowering memory thus interrupting the chained behavior.
The underlying concept was that what we mentally rehearse is what we may become and that our thoughts affect performance which she previously experienced by the arm resistance test. If you keep thinking about a defeat you are training the physiological pattern of defeat. This practice of transforming self-defeating thoughts into empowering thoughts can be applied to all phases of one’s life and was continued throughout the training sessions. The focus was to acknowledge and realize that whatever you did, it was the only thing you could have done because you did not yet have the skills to do it differently. She would then create a new strategy of mental rehearsal that lead to a positive outcome (for detailed description of this practice see Peper, Harvey, Lin, & Duvvuri, 2014).
5. Identifying whether imagery rehearsal is somatically connected. It is our bias that imagery rehearsal is useful if the body responds in a similar pattern when the person images the task as it would during an actual activity (Hall, 2001; Peper et al, 2015). The concurrent physiological activity would indicate that the person is experientially involved in the task and not just observing as a witness/second party.
Her performance is weightlifting and this would involve major muscle activity. Surface EMG was recorded from muscles that would be activated during the actual performance of the task to identify if they would be activated during mental rehearsal. The muscle activity during mental rehearsal is usually at a much smaller amplitude than that occurred during actual physical performance; however, should follow a similar timing sequence. In our experience there are three responses:
- Muscle activity in the appropriate muscles that are in the same timing as in and actual performance. This implies that mental rehearsal is actually training the motor pattern and facilitate performance. Thus continue practicing with mental rehearsal.
- Muscle activity in the appropriate muscles are not generally in the same timing sequence as the actual performance. This may mean that the person was performing too slow or was skipping sequences in the mental rehearsal and mental training may not be useful. The person needs to master and exhibit the same muscle pattern during mental rehearsal as during actual performance of the task.
- No muscle activity or inappropriate muscle activity during the during the mental rehearsal. This implies that during mental rehearsal there is no motor pattern training and the approach would not be useful unless the person learned to activate appropriate motor activity. It is possible that some people who have experienced past traumas may have coped by shutting off feelings and sensations in their bodies.
When Jo Aita initially practiced mental rehearsal while being monitored with surface EMG recorded with Myoscan Pro sensors (filter set narrow 100-200Hz) from the right and left upper trapezius muscles, there was no corresponding muscle activity as shown in Figure 2. Although she imaged, she did not feel/experience the lifting. The training focused upon reconnecting imagery and body experience.

Figure 2. Left and right upper trapezius EMG showed no increase in activity while Jo Aita mentally imaged performing her lift.
6. Integrating imagery and body experience with EMG. After identifying that imagery did not elicit concurrent muscle activity, the training focused on developing the imagery muscle connection. The training consisted of:
- Monitoring EMG activity from her right and left quadriceps and right and left upper trapezius muscle and have her simulate her actually lifting in practice and competition by going through the complete sequence which included standing and waiting till her name was called, caulking her hands, performing a ritual activity to be ready to lift the weights, lifting the weights, and releasing them. The pattern is shown in Figure 3.

Figure 3. Simulating the actual Snatch and Jerk lift (Clean is lifting the weights to the chest and punching Jerk is pushing the weigh upward is labelled).
- Practicing imagery by going through the same procedure and purposely slightly activating the movements which were necessary to lift the weight. As she stated, “I learned to do mental rehearsal in a more structured way and visualized the total sequence from chalking up to doing all six lifts”. This was monitored by the EMG to see that there occurred EMG activation of the muscles. This was repeated numerous times till, the activation occurred in imagery as shown in Figure 4.[1]

Figure 4. EMG activity during mental rehearsal.
She then reported that imagery was a real experience.
7. Training mental rehearsal and imagery for peak performance (Cumming, Hall, & Shambrook, 2004). The major components of the mental rehearsal focused upon performing perfectly, visualizing lifting more weight easily than actually lifted in the gym, performing in the gym as she would during competing, practicing performing when interruptions occurred, and punching the weight through the ceiling.
- Performing perfectly. During the day she would mentally rehearse practicing lifting perfectly. In addition, as part of her readiness routine she would image performing the lift perfectly.
- Practicing recovery and being centered when interruptions would occur. For example, she was asked to role play competition and waiting for the judge to give the signal to start, I delayed giving her the signal to begin and told her the weights had to be adjusted because they had miss-loaded the bar. This way there would be no novelty during actual competition. This concept of coping with the unexpected was illustrated by Michael Phelps swimming the 200-meter butterfly in 2012 Being Olympics when his googles filled up with water when he dove in. Michael still won his 10th gold medal even though he swam part of the race blind (Fanning, E., June 25, 2012). He could do this because numerous time in the past, his coach had purposely trained Michael to swim with leaking googles
- Imagining lifting 10 kg more while competing. The concept of feeling/imagining yourself performing more that you can do at this moment creates the possibility for improvement since the limits of imagination may limit the experience/performance. As she reported, “This was incredibly helpful last year in competition when I needed to lift more than I had done before to qualify for the American Open, so I had mentally done it so often, then I just did it and made the qualifying lift.”
- Feeling your arms extending way up into the ceiling. Extending beyond your mental boundary of the test allows more power because the body tends to stop at the boundary. For example, when running 100 meters you want to see the finish line at least ten meters beyond the actual finish line this way you continue to run at maximum speed through the finish. If you focus on the actual finish line, you often slow down before reaching it. I told her how we used this concept with young male gymnasts to be able to do the iron cross for the first time by thinking of their arms being an iron beam and extending through the rings into the wall. In the case of lifting, you want to feel yourself punching the weight through the ceiling instead of just driving it upward. This portion of the lift when punching up into the ceiling is call the Jerk. This concept was experientially demonstrated by the following Aikido exercise of the iron arm.
Two people pair up and face each other. One stretches his arm straight out and rests the wrist and back of the palm on the shoulder of his partner. The partner put both hands on the elbow and then then pulls down trying to bend the elbow while his partner is try resist the downward force and try not to bend it as shown in Figure 5. 
Figure 5. Testing the effect of imagery on resisting downward pull at the elbow with wrist facing palm up.
Then relax, and repeat the same exercise except the person imagines that his arm is like a metal bar extending from their shoulders out through his hand into the wall. Once the person is imaging this, then the partner again attempts to bend the arm.
In almost all cases, when the person imagines the arm extending like an iron bar into the wall, it is much stronger and much more difficult to bend. Jo integrated this felt imagery in her lifting during practice and she experienced increased strength while imagining/feeling the iron bar and reported that she had the “best Jerks in her life.”
Discussion
Achieving a new world and personal record at age 46 in the master’s competition is a remarkable tribute to the athlete’s dedication and coaching. Although I (EP) may think I contributed, and hopefully what I taught was beneficial, in the end it is the athlete herself who has to perform in the competition–she is alone stands on the platform to lift the weights. When I (EP) asked whether the biofeedback visualization training was useful, Jo inequitably said, “Yes, and I would recommend this approach and training to everyone!” Watch the in-depth interview with Jo Aita in which she describes her experience of integrating imagery techniques and biofeedback to enhance performance on May 26, 2017.
What is interesting to ask is, how come a 46-year-old woman could lift 3 kg more than at any other time during her competitive career of Olympic lifting? It gives hope that loss of strength that commonly occurs as we age may be due less to aging than to learned disuse, injuries and lack of recovery. Most important factors are personal motivation and hope—you want to perform your best and know/believe that it is possible (Wilson and Peper, 2011). As Jo stated, “It helped for me to focus on doing my personal best.” I love Olympic lifting, I like taking care of my body, and I like feeling strong.” Finally, Jo is a recent athlete in her sport. She started lifting when she was 33 and competed one year later. She then took time out to give birth to her son and in a couple of months came back quickly and continued to become stronger. As she stated, “I always wanted to get stronger no matter what my age was.”
From a performance perspective it is interesting that she lifted more than ever before. Would it be possible that she is similar to many performers who achieve maximum performance after about 10 to 15 years of dedicated training? As she gets older, she improves her skills, increases efficiency of here muscles and neural connections. Is a possible that loss of performance as we age less due to aging than loss of motivation after years of practice, competition and achieving your goal. At that point life may offer other challenges and new opportunities.
* This blog was adapted and expanded from: Peper, E. & Aita, J. (2017). Winning the Gold in Weightlifting Using Biofeedback, Imagery and Cognitive Change. Biofeedback, 45(4), 77–82. DOI: 10.5298/1081-5937-45.4.01 https://biofeedbackhealth.files.wordpress.com/2018/02/a-winning-the-gold-in-weightlifting-published.pdf
References
Cumming, J., Hall, C., & Shambrook, C. (2004). The influence of an imagery workshop on athletes’ use of imagery. Athletic insight, 6(1), 52-73.
Fanning, E. (June 25, 2012). 50 stunning Olympic Moments No 42: Michael Phelps goes big in Being. Downloaded May 30, 2017 from https://www.theguardian.com/sport/blog/2012/jun/25/50-stunning-olympic-moments-michael-phelps
Gorter, R. & Peper, E. (2011). Fighting Cancer-A Non Toxic Approach to Treatment. Berkeley: North Atlantic.
Hall, C. (2001). Imagery in sport and exercise. In R. Singer, H. Hausenblas, & C. Janelle (Eds.), Handbook of Sport Psychology (pp. 529 – 549). New York, NY: John Wiley & Sons, Inc.
Peper, E., Harvey, R., Lin, I-M, & Duvvuri, P. (2014). Increase productivity, decrease procrastination and increase energy. Biofeedback, 42(2), 82-87.
Peper, E., Booiman, A., Lin, I-M., & Shaffer, F. (2014). Making the Unaware Aware-Surface Electromyography to Unmask Tension and Teach Awareness. Biofeedback.42(1), 16-23.
Footnotes:
[1] Correspondence: Erik Peper, Ph.D., Institute for Holistic Health Studies, Department of Health Education, San Francisco State University, 1600 Holloway Avenue, San Francisco, CA 94132. email: epeper@sfsu.edu; web: www.biofeedbackhealth.org; blog: www.peperperspective.com
[2] We thank Dr. Sue Wilson for her helpful and constructive feedback.
[3] We purposely use the word “may” because it is a case report and not a controlled study. Coaches, sport psychologist, or anyone who has had contact with an athlete who does extremely well usually claims that their suggestions were the magic ingredient; however, it could be synchronicity and not due to the actual skills taught. It may be due to unidentified factors or covert factors embedded in the coaching or teaching such as transforming hope and belief.
[4] Be aware that when people learn to reconnect with their body or learns slow diaphragmatic breathing and allow their lower abdomen to relax and expand, it is possible that past traumatic memories could be released. This release is a healthy process and we usually adapt an Autogenic Therapy/Training perspective by which the person accepts, allows discharge and continues with the task at hand.
Education versus treatment for self-healing: Eliminating a headache[1]
Posted: November 18, 2016 Filed under: Pain/discomfort, self-healing, stress management, Uncategorized | Tags: autogenic training, biofeedback, education, electromyography, headache, Holistic health, migraine, posture, treatment 3 Comments“I have had headaches for six years, at first occurring almost every day. When I got put on an antidepressant, they slowed to about 3 times a week (sometimes more) and continued this way until I learned relaxation techniques. I am 20 years old and now headache free. Everyone should have this educational opportunity to heal themselves.” -Melinda, a 20 year old student
Health and wellness is a basic right for all people. When students learn stress management skills which include awareness of stress, progressive muscle relaxation, Autogenic phrases, slower breathing, posture change, transforming internal language, self-healing imagery, the role of diet, exercise embedded within an evolutionary perspective as part of a college class their health often improves. When students systematically applied these self-awareness techniques to address a self-selected illness or health behavior (e.g., eczema, diet, exercise, insomnia, or migraine headaches), 80% reported significant improvement in their health during that semester (Peper et al., 2014b; Tseng, et al., 2016). The semester long program is based upon the practices described in the book, Make Health Happen, (Peper, Gibney, & Holt, 2002).
The benefits often last beyond the semester. Numerous students reported remarkable outcomes at follow-up many months after the class had ended because they had mastered the self-regulation skills and continued to implement these skills into their daily lives. The educational model utilized in holistic health courses is often different from the clinical/treatment model.
Educational approach: I am a student and I have an illness (most of me is healthy and only part of me is sick).
Clinical treatment approach: I am a patient and I am sick (all of me is sick)
Some of the concepts underlying the differences between the educational and the clinical approach are shown in Table 1.
| Educational approach | Clinic/treatment approach |
| Focuses on growth and learning | Focuses on remediation |
| Focuses on what is right | Focuses on what is wrong |
| Focuses on what people can do for themselves | Focuses on how the therapist can help patients |
| Assumes students as being competent | Implies patients are damaged and incompetent |
| Students defined as being competent to master the skills | Patients defined as requiring others to help them |
| Encourages active participation in the healing process | Assumes passive participation in the healing process |
| Students keep logs and write integrative and reflective papers, which encourage insight and awareness | Patients usually do not keep logs nor are asked to reflect at the end of treatment to see which factors contributed to success |
| Students meet in small groups, develop social support and perspective | Patients meet only with practitioners and stay isolated |
| Students experience an increased sense of mastery and empowerment | Patients experience no change or possibly a decrease in sense of mastery |
| Students develop skills and become equal or better than the instructor | Patients are healed, but therapist is always seen as more competent than patient |
| Students can become colleagues and friends with their teachers | Patients cannot become friends of the therapist and thus are always distanced |
Table 1. Comparison of an educational versus clinical/treatment approach
The educational approach focuses on mastering skills and empowerment. As part of the course work, students become more mindful of their health behavior patterns and gradually better able to transform their previously covert harm promoting patterns. This educational approach is illustrated in a case report which describes how a student reduced her chronic migraines.
Case Example: Elimination of Chronic Migraines
Melinda, a 20-year-old female student, experienced four to five chronic migraines per week since age 14. A neurologist had prescribed several medications including Imitrex (used to treat migraines) and Topamax (used to prevent seizures as well as migraine headaches), although they were ineffective in treating her migraines. Nortriptyline (a tricyclic antidepressant) and Excedrin Migraine (which contains caffeine, aspirin, and acetaminophen) reduced the frequency of symptoms to three times per week.
She was enrolled in a university biofeedback class that focused on learning self-regulation and biofeedback skills. All these students were taught the fundamentals of biofeedback and practiced Autogenic Training (AT) every day during the semester (Luthe, 1979; Luthe & Schultz, 1969; Peper & Williams, 1980).
In the class, students practiced with surface electromyography (SEMG) feedback to identify the presence of shoulder muscle overexertion (dysponesis), as well as awareness of minimum muscle tension. Additional practices included hand warming, awareness of thoracic and diaphragmatic breathing, and other biofeedback or somatic awareness approaches. In parallel with awareness of physical sensations, students practiced behavioral awareness such as alternating between a slouching body posture (associated with feeling self-critical and powerless) and an upright body posture (associated with feeling powerful and in control). Psychological awareness was focused on transforming negative thoughts and self-judgments to positive empowering thoughts (Harvey and Peper, 2011; Peper et al., 2014a; Peper et al, 2015). Taken together, students systematically increased awareness of physical, behavioral, and psychological aspects of their reactions to stress.
The major determinant for success is to generalize training at school, home and at work. Each time Melinda felt her shoulders tightening, she learned to relax and release the tension in her shoulders, practiced Autogenic Training with the phrase “my neck and shoulders are heavy.” In addition, whenever she felt her body beginning to slouch or noticed a negative self-critical thought arising in her mind, she shifted her body to an upright empowered posture, and substituted positive thoughts to reduce her cortisol level and increase access to positive thoughts (Carney & Cuddy, 2010; Cuddy, 2012; Tsai, et al., 2016). Postural feedback was also informally given by Melinda’s instructor. Every time the instructor noticed her slouching in class or the hallway, he visually changed his own posture to remind her to be erect.
Results
Melinda’s headaches reduced from between three and five per week before enrolling in the class to zero following the course, as shown in Figure 2. She has learned to shift her posture from slouching to upright and relaxed. In addition, she reported feeling empowered, mentally clear, and her acne cleared up. All medications were eliminated. At a two year follow-up, she reported that since she took the class, she had only few headaches which were triggered by excessive stress. 
Figure 2. Frequency of migraine and the implementation of self-practices.
The major factors that contributed to success were:
- Becoming aware of muscle tension through the SEMG feedback. Melinda realized that she had tension when she thought she was relaxed.
- Keeping detailed logs and developing a third person perspective by analyzing her own data and writing a report. A process that encouraged acceptance of self, thereby becoming less judgmental.
- Acquiring a new belief that she could learn to overcome her headaches, facilitated by class lecture and verbal feedback from the instructor.
- Taking active control by becoming aware of the initial negative thoughts or sensations and interrupting the escalating chain of negative thoughts and sensations by shifting the attention to positive empowering thoughts and sensations–a process that integrated mindfulness, acceptance and action. Thus, transforming judgmental thoughts into accepting and positive thoughts.
- Becoming more aware throughout the day, at school and at home, of initial triggers related to body collapse and muscle tension, then changing her body posture and relaxing her shoulders. This awareness was initially developed because the instructor continuously gave feedback whenever she started to slouch in class or when he saw her slouching in the hallways.
- Practicing many, many times during the day. Namely, increasing her ongoing mindfulness of posture, neck, and shoulder tension, and of negative internal dialogue without judgment.
The benefits of this educational approach is captured by Melinda’s summary, “The combined Autogenic biofeedback awareness and skill with the changes in posture helped me remarkably. It improved my self-esteem, empowerment, reduced my stress, and even improved the quality of my skin. It proves the concept that health is a whole system between mind, body, and spirit. When I listen carefully and act on it, my overall well-being is exceptionally improved.”
References:
Carney, D. R., Cuddy, A. J., & Yap, A. J. (2010). Power posing brief nonverbal displays affect neuroendocrine levels and risk tolerance. Psychological Science, 21(10), 1363-1368.
Cuddy, A. (2012). Your body language shapes who you are. Technology, Entertainment, and Design (TED) Talk, available at: http://www.ted.com/talks/amy_cuddy_your_body_language_shapes_who_you_are
Harvey, E. & Peper, E. (2011). I thought I was relaxed: The use of SEMG biofeedback for training awareness and control (pp. 144-159). In W. A. Edmonds, & G. Tenenbaum (Eds.), Case studies in applied psychophysiology: Neurofeedback and biofeedback treatments for advances in human performance. West Sussex, UK: Wiley-Blackwell.
Luthe, W. (1979). About the methods of autogenic therapy (pp. 167-186). In E. Peper, S. Ancoli, & M. Quinn, Mind/body integration. New York: Springer.
Luthe, W., & Schultz, J.H. (1969). Autogenic therapy (Vols. 1-6). New York, NY: Grune and Stratton.
Peper, E., Booiman, A., Lin, I-M., & Shaffer, F. (2014a). Making the unaware aware-Surface electromyography to unmask tension and teach awareness. Biofeedback. 42(1), 16-23.
Peper, E., Gibney, K.H. & Holt. C. (2002). Make health happen: Training yourself to create wellness. Dubuque, IA: Kendall-Hunt. ISBN-13: 978-0787293314
Peper, E., Lin, I-M, Harvey, R., Gilbert, M., Gubbala, P., Ratkovich, A., & Fletcher, F. (2014b). Transforming chained behaviors: Case studies of overcoming smoking, eczema and hair pulling (trichotillomania). Biofeedback, 42(4), 154-160.
Peper, E., Nemoto, S., Lin, I-M., & Harvey, R. (2015). Seeing is believing: Biofeedback a tool to enhance motivation for cognitive therapy. Biofeedback, 43(4), 168-172. doi: 10.5298/1081-5937-43.4.03
Peper, E. & Williams, E.A. (1980). Autogenic therapy (pp. 131-137). In: A. C. Hastings, J. Fadiman, & J. S. Gordon (Eds.). Health for the whole person. Boulder: Westview Press.
Tsai, H. Y., Peper, E., & Lin, I. M. (2016). EEG patterns under positive/negative body postures and emotion recall tasks. NeuroRegulation, 3(1), 23-27.
Tseng, C., Abili, R., Peper, E., & Harvey, R. (2016). Reducing acne-stress and an integrated self-healing approach. Poster presented at the 47th Annual Meeting of the Association for Applied Psychophysiology and Biofeedback, Seattle WA, March 9-12, 2016.
[1] Adapted from: Peper, E., Miceli, B., & Harvey, R. (2016). Educational Model for Self-healing: Eliminating a Chronic Migraine with Electromyography, Autogenic Training, Posture, and Mindfulness. Biofeedback, 44(3), 130–137. https://biofeedbackhealth.files.wordpress.com/2011/01/a-educational-model-for-self-healing-biofeedback.pdf
Resolving pelvic floor pain-A case report
Posted: September 25, 2015 Filed under: Breathing/respiration, Pain/discomfort, self-healing, stress management, Uncategorized | Tags: biofeedback, Breathing, electromyography, pain, posture, self-regulation, vulvodynia 10 CommentsAdapted from: Martinez Aranda, P. & Peper, E. (2015). The healing of vulvodynia from a client’s perspective. https://biofeedbackhealth.files.wordpress.com/2011/01/a-healing-of-vulvodynia-from-the-client-perspective-2015-06-15.pdf
It’s been a little over a year since I began practicing biofeedback and visualization strategies to overcome vulvodynia. Today, I feel whole, healed, and hopeful. I learned that through controlled and conscious breathing, I could unleash the potential to heal myself from chronic pain. Overcoming pain did not happen overnight; but rather, it was a process where I had to create and maintain healthy lifestyle habits and meditation. Not only am I thankful for having learned strategies to overcome chronic pain, but for acquiring skills that will improve my health for the rest of my life. –-24 year old woman who successfully resolved vulvodynia
Pelvic floor pain can be debilitating, and it is surprisingly common, affecting 10 to 25% of American women. Pelvic floor pain has numerous causes and names. It can be labeled as vulvar vestibulitis, an inflammation of vulvar tissue, interstitial cystitis (chronic pain or tenderness in the bladder), or even lingering or episodic hip, back, or abdominal pain. Chronic pain concentrated at the entrance to the vagina (vulva), is known as vulvodynia. It is commonly under-diagnosed, often inadequately treated, and can go on for months and years (Reed et al., 2007; Mayo Clinic, 2014). The discomfort can be so severe that sitting is uncomfortable and intercourse is impossible because of the extreme pain. The pain can be overwhelming and destructive of the patient’s life. As the participant reported,
I visited a vulvar specialist and he gave me drugs, which did not ease the discomfort. He mentioned surgical removal of the affected tissue as the most effective cure (vestibulectomy). I cried immediately upon leaving the physician’s office. Even though he is an expert on the subject, I felt like I had no psychological support. I was on Gabapentin to reduce pain, and it made me very depressed. I thought to myself: Is my life, as I know it, over?
Physically, I was in pain every single day. Sometimes it was a raging burning sensation, while other times it was more of an uncomfortable sensation. I could not wear my skinny jeans anymore or ride a bike. I became very depressed. I cried most days because I felt old and hopeless instead of feeling like a vibrant 23-year-old woman. The physical pain, combined with my negative feelings, affected my relationship with my boyfriend. We were unable to have sex at all, and because of my depressed status, we could not engage in any kind of fun. (For more details, read the published case report,Vulvodynia treated successfully with breathing biofeedback and integrated stress reduction: A case report).
The four-session holistic biofeedback interventions to successfully resolved vulvodynia included teaching diaphragmatic breathing to transform shallow thoracic breathing into slower diaphragmatic breathing, transforming feelings of powerlessness and hopelessness to empowerment and transforming her beliefs that she could reduce her symptoms and optimize her health. The interventions also incorporated self-healing imagery and posture-changing exercises. The posture changes consisted of developing awareness of the onset of moving into a collapsed posture and use this awareness to shift to an erect/empowered postures (Carney, Cuddy, & Yap, 2010; Peper, 2014; Peper, Booiman, Lin, & Harvey, in press). Finally, this case report build upon the seminal of electromyographic feedback protocol developed by Dr. Howard Glazer (Glazer & Hacad, 2015) and the integrated relaxation protocol developed Dr. David Wise (Wise & Anderson, 2007).
Through initial biofeedback monitoring of the lower abdominal muscle activity, chest, and abdomen breathing patterns, the participant observed that when she felt discomfort or was fearful, her lower abdomen muscles tended to tighten. After learning how to sense this tightness, she was able to remind herself to breathe lower and slower, relax the abdominal wall during inhalation and sit or stand in an erect power posture.
The self-mastery approach for healing is based upon a functional as compared to a structural perspective. The structural perspective implies that the problem can only be fixed by changing the physical structure such as with surgery or medications. The functional perspective assumes that if you can learn to change your dysfunctional psychophysiological patterns the disorder may disappear.
The functional approach assumed that an irritation of the vestibular area might have caused the participant to tighten her lower abdomen and pelvic floor muscles reflexively in a covert defense reaction. In addition, ongoing worry and catastrophic thinking (“I must have surgery, it will never go away, I can never have sex again, my boyfriend will leave me”) also triggered the defense reaction—further tightening of her lower abdomen and pelvic area, shallow breathing, and concurrent increases in sympathetic nervous activation—which together activated the trigger points that lead to increased chronic pain (Banks et al, 1998).
When the participant experienced a sensation or thought/worried about the pain, her body responded in a defense reaction by breathing in her chest and tightening the lower abdominal area as monitored with biofeedback. Anticipation of being monitored increased her shoulder tension, recalling the stressful memory increased lower abdominal muscle tension (pulling in the abdomen for protection), and the breathing became shallow and rapid as shown in Figure 1.
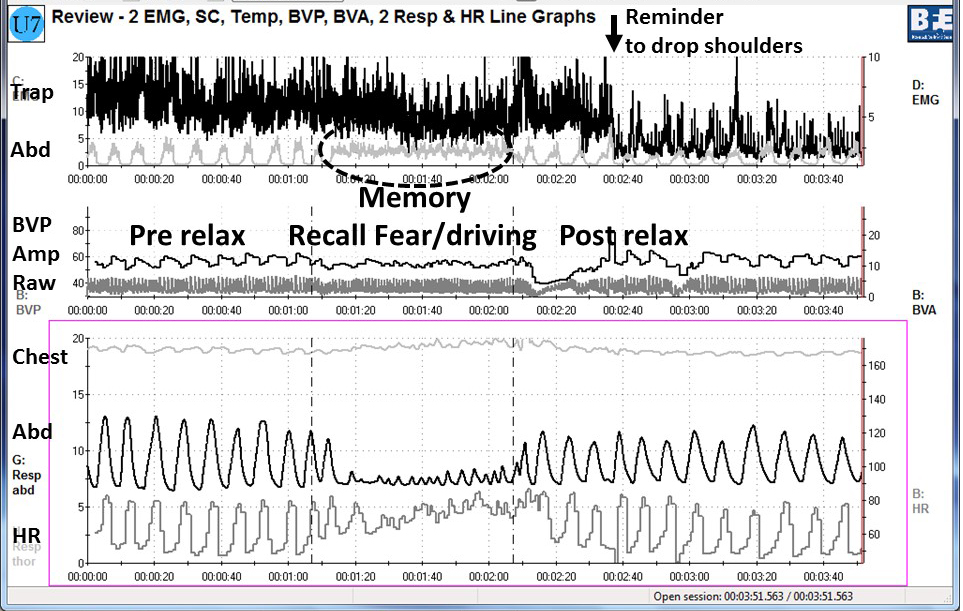
Figure 1. Physiological recording of pre-stressor relaxation, the recall of a fearful driving experience, and a post-stressor relaxation. The scalene to trapezius SEMG increased in anticipation while she recalled the experience, and then initially did not relax (from Peper, Martinez Aranda, & Moss, 2015).
This defense pattern became a conditioned response—initiating intercourse or being touched in the affected area caused the participant to tense and freeze up. She was unaware of these automatic protective patterns, which only worsened her chronic pain.
During the four sessions of training, the participant learned to reverse and interrupt the habitual defense reaction. For example, as she became aware of her breathing patterns she reported,
It was amazing to see on the computer screen the difference between my regular breathing pattern and my diaphragmatic breathing pattern. I could not believe I had been breathing that horribly my whole life, or at least, for who knows how long. My first instinct was to feel sorry for myself. Then, rather than practicing negative patterns and thoughts, I felt happy because I was learning how to breathe properly. My pain decreased from an 8 to alternating between a 0 and 3.
The mastery of slower and lower abdominal breathing within a holistic perspective resulted in the successful resolution of her vulvodynia. An essential component of the training included allowing the participant to feel safe, and creating hope by enabling her to experience a decrease in discomfort while doing a specific practice, and assisting her to master skills to promote self-healing. Instead of feeling powerless and believing that the only resolution was the removal of the affected area (vestibulectomy). The integrated biofeedback protocol offered skill mastery training, to promote self-healing through diaphragmatic breathing, somatic postural changes, reframing internal language, and healing imagery as part of a common sense holistic health approach.
For more details about the case report, download the published study, Peper, E., Martinez Aranda, P., & Moss, E. (2015). Vulvodynia treated successfully with breathing biofeedback and integrated stress reduction: A case report. Biofeedback. 43(2), 103-109.
The participant also wrote up her subjective experience of the integrated biofeedback process in the paper, Martinez Aranda & Peper (2015). Healing of vulvodynia from the client perspective. In this paper she articulated her understanding and experiences in resolving vulvodynia which sheds light on the internal processes that are so often skipped over in published reports.
At the five year follow-up on May 29, 2019, she wrote:
“I am doing very well, and I am very healthy. The vulvodynia symptoms have never come back. It migrated to my stomach a couple of years after, and I still have a sensitive stomach. My stomach has gotten much, much better, though. I don’t really have random pain anymore, now I just have to be watchful and careful of my diet and my exercise, which are all great things!”
References
Banks, S. L., Jacobs, D. W., Gevirtz, R., & Hubbard, D. R. (1998). Effects of autogenic relaxation training on electromyographic activity in active myofascial trigger points. Journal of Musculoskeletal Pain, 6(4), 23-32. https://www.researchgate.net/profile/David_Hubbard/publication/232035243_Effects_of_Autogenic_Relaxation_Training_on_Electromyographic_Activity_in_Active_Myofascial_Trigger_Points/links/5434864a0cf2dc341daf4377.pdf
Carney, D. R., Cuddy, A. J., & Yap, A. J. (2010). Power posing brief nonverbal displays affect neuroendocrine levels and risk tolerance. Psychological Science, 21(10), 1363-1368. Available from: https://www0.gsb.columbia.edu/mygsb/faculty/research/pubfiles/4679/power.poses_.PS_.2010.pdf
Glazer, H. & Hacad, C.R. (2015). The Glazer Protocol: Evidence-Based Medicine Pelvic Floor Muscle (PFM) Surface Electromyography (SEMG). Biofeedback, 40(2), 75-79. http://www.aapb-biofeedback.com/doi/abs/10.5298/1081-5937-40.2.4
Martinez Aranda, P. & Peper, E. (2015). Healing of vulvodynia from the client perspective. Available from: https://biofeedbackhealth.files.wordpress.com/2011/01/a-healing-of-vulvodynia-from-the-client-perspective-2015-06-15.pdf
Mayo Clinic (2014). Diseases and conditions: Vulvodynia. Available at http://www.mayoclinic.org/diseases-conditions/vulvodynia/basics/definition/con-20020326
Peper, E. (2014). Increasing strength and mood by changing posture and sitting habits. Western Edition, pp.10, 12. Available from: http://thewesternedition.com/admin/files/magazines/WE-July-2014.pdf
Peper, E., Booiman, A., Lin, I, M.,& Harvey, R. (in press). Increase strength and mood with posture. Biofeedback.
Peper, E., Martinez Aranda, P., & Moss, E. (2015). Vulvodynia treated successfully with breathing biofeedback and integrated stress reduction: A case report. Biofeedback. 43(2), 103-109. Available from: https://biofeedbackhealth.files.wordpress.com/2011/01/a-vulvodynia-treated-with-biofeedback-published.pdf
Reed, B. D., Haefner, H. K., Sen, A., & Gorenflo, D. W. (2008). Vulvodynia incidence and remission rates among adult women: a 2-year follow-up study. Obstetrics & Gynecology, 112(2, Part 1), 231-237. http://journals.lww.com/greenjournal/Abstract/2008/08000/Vulvodynia_Incidence_and_Remission_Rates_Among.6.aspx
Wise, D., & Anderson, R. U. (2006). A headache in the pelvis: A new understanding and treatment for prostatitis and chronic pelvic pain syndromes. Occidental, CA: National Center for Pelvic Pain Research.http://www.pelvicpainhelp.com/books/
Relax and Relax More*
Posted: February 6, 2015 Filed under: Uncategorized | Tags: awareness, electromyography, muscle biofeedback, relaxation, shoulder pain 4 CommentsAfter raising my shoulders and then relaxing it, I felt relaxed. I was totally surprised that the actual muscle tension recorded with surface electromyographic (SEMG) still showed tension. Only when I gave myself the second instruction, relax even more, that my SEMG activity decreased.
In our experiences, we (Vietta E. Wilson and Erik Peper, 2014) have observed that muscle tension often does not decrease completely after a person is instructed to relax. The complete relaxation only occurs after the second instruction, relax more, let go, drop, or feel the heaviness of gravity. The person is totally unaware that after the first relaxation their muscless have not totally relaxed. Their physiology does not match their perception (Peper et, 2010; Whatmore & Kohli, 1974). The low level of muscle tension appears more prevalent in people who are have a history of muscle stiffness or pain, or in athletes whose coaches report they look ‘tight.’ It is only after the second command, relax and release even more, that the individual notices a change and experiences a deeper relaxation.
The usefulness of giving a second instruction, relax more, after the first instruction, relax, is illustrated below by the surface electromyographic (SEMG) recording from the upper left and right trapezius muscle of a 68 year old male with chronic back pain. While sitting upright without experiencing any pain, he was instructed to lift his shoulders, briefly hold the tension, and then relax (Sella, 1997; Peper et al, 2008). When the SEMG of the trapezius muscles did not decrease to the relaxed state, he was asked to relax more as is shown in Figure 1.

Figure 1. SEMG recordings of the left and right upper trapezius when the client was asked to lift his shoulders, hold, relax, and relax more. Only after the second instruction did the muscle tension decrease to the relaxed baseline level. Reprinted from Wilson and Peper, 2014.
Although the subject felt that he was relaxed after the first relaxation instruction, he continued to hold a low level of muscle tension. We have observed this same process in hundreds of clients and students while teaching SEMG guided relaxation and progressive muscle relaxation.
For numerous people, even the second commands to relax even more is not sufficient for the SEMG to show muscle relaxation and for them to ‘feel’ or know when they are totally relaxed. These individuals may benefit from SEMG biofeedback to identify and quantify the degree of muscle tension. With this information the person can make the invisible muscle contractions ‘ visible,’ the un-felt tension ‘felt,’ and thus develop awareness and control (Peper et al, 2014).
In summary
- Instruct people to relax after tightening and then repeat the instruction to relax even more.
- Use surface electromyography to confirm whether the person’s subjective experience of being muscularly relaxed corresponds to the actual physiological SEMG recording.
- Use the SEMG biofeedback to train the person to increase awareness and learn relaxation (Peper et al, 2014).
- Read the complete article from which this blog was adapted: Wilson, E. & Peper, E. (2014). Clinical Tip: Relax and Relax More. 42(4), 163-164.
References
Peper, E., Booiman, A., Lin, I-M., & Shaffer, F. (2014). Making the Unaware Aware-Surface electromyography to unmask tension and teach awareness. Biofeedback. 42(1), 16-23.
Peper, E., Booiman, A., Tallard, M., & Takebayashi, N. (2010). Surface electromyographic biofeedback to optimize performance in daily life: Improving physical fitness and health at the worksite. Japanese Journal of Biofeedback Research, 37(1), 19-28.
Peper, E., Tylova, H., Gibney, K.H., Harvey, R., & Combatalade, D. (2008). Biofeedback mastery-An experiential teaching and self-training manual. Wheat Ridge, CO: AAPB.
*This blogpost is adapted from, Wilson, E. & Peper, E. (2014). Clinical tip: Relax and relax more. Biofeedback. 42(4), 163-164.
Muscle biofeedback makes the invisible visible
Posted: January 6, 2012 Filed under: Uncategorized | Tags: back pain, biofeedback, electromyography, muscle tension, neck pain, performance, shoulder pain 3 Comments“I feel much more relaxed and realize now how unaware I was of the unnecessary tension I’ve been holding” is a common response after muscle biofeedback training. Many people experience exhaustion, stiffness, tightness, neck, shoulder and back pain while working long hours at the computer or while exercising. As we get older, we assume that discomforts are the result of aging. You just have to accept it and live with it–grin and bear it–or you need to be more careful while doing your job or performing your hobby. The discomfort in many cases is the result of misuse of your body. Observes what happens when you perform the following experiential practice Threading the needle.
Perform this task so that an observer would think it was real and would not know that you are only simulating threading a needle.
Imagine that you are threading a needle — really imagine it by picturing it in your mind and acting it out. Hold the needle between your left thumb and index finger. Hold the thread between the thumb and index finger of your right hand. Bring the tip of the thread to your mouth and put it between your lips to moisten it and make it into a sharp point. Then attempt to thread the needle, which has a very small eye. The thread is almost as thick as the eye of the needle.
As you are concentrating on threading this imaginary needle, observed what happened? While acting out the imagery, did you raise or tighten your shoulders, stiffen your trunk, clench your teeth, hold your breath or stare at the thread and needle without blinking?
Most people are surprised that they have tightened their shoulders and braced their trunk while threading the needle. Awareness only occurred after their attention was directed to the covert muscle bracing patterns.
In many cases muscles are tense even though the person senses and feels that they are relaxed. This lack of awareness can be resolved with muscle biofeedback–it makes invisible visible. Muscle biofeedback (electromyographic feedback) is used to monitor the muscle activity, teach the person awareness of the previously unperceived muscle tension and learn relax and control it. For more information of the use of muscle biofeedback to improve health and performance at work or in the gym, see the published chapter, I thought I was relaxed: The use of SEMG biofeedback for training awareness and control, by Richard Harvey and Erik Peper. It was published in W. A. Edmonds, & G. Tenenbaum (Eds.). (2012), Case studies in applied psychophysiology: Neurofeedback and biofeedback treatments for advances in human performance. West Sussex, UK: Wiley-Blackwell, 144-159.
