Reversing Pandemic-Related Increases in Back Pain
Posted: August 30, 2022 Filed under: behavior, Breathing/respiration, digital devices, ergonomics, Exercise/movement, health, laptops, Neck and shoulder discomfort, Pain/discomfort, posture, relaxation, self-healing, stress management, Uncategorized | Tags: back pain 2 Comments
By: Chris Graf
Reproduced by permission from: https://www.paintreatmentdirectory.com/posts/reversing-pandemic-related-increases-in-back-pain
Back pain increased significantly during the pandemic
Google searches for the words “back pain” reached an all-time high in January 2022. In a Harris Poll in September 2021, 56% of respondents said they had chronic pain, up from about 30% before the pandemic. There are probably multiple reasons for the uptick in pain in general and back pain in particular related to COVID, including added stress and ongoing symptoms of long COVID. Poor posture while working at home is another likely contributor.
Back pain and Ergonomics
According to Dr. Erik Peper, co-author of Tech Stress: How Technology is Hijacking Our Lives, Strategies for Coping, and Pragmatic Ergonomics, It is likely that poor ergonomics in the home office are partially to blame for the apparent rise in back pain. “With COVID, ergonomics have become a disaster—especially with people who use laptops.” Peper, an internationally known expert in biofeedback and Professor of Holistic Health Studies at San Francisco State University, said that it is “almost impossible” to sit correctly when using a laptop. “In order for the hands to be at the correct level for the keyboard, the head must be tilted down. The more the head tilts forward, the most stress that is placed on the cervical spine,” he said, noting that the arms will no longer be in the proper position if the laptop is placed on a stand to raise it to eye level.
For laptop users, Peper recommends using either an external monitor or external keyboard. When using an external keyboard, a laptop stand can be used to elevate the screen to the proper eye level. University of California at Berkeley recommends other tips for ergonomic laptop positioning.
When using both laptops and desktops, attention should be focused on proper sitting posture. Ergonomic chairs are only part of the equation when it comes to achieving proper posture.
“A good chair only gives you the opportunity to sit correctly,” Peper said. The goal is to achieve anterior pelvic tilt by having the seat pan slightly lower in the front that in the back. He recommends using a seat insert or cushion to achieve proper positioning (see figure 1).

Figure 1. A small pillow or rolled up towel can be placed behind the back at kidney level in order to keep the spine slightly arched (see figure 2).

Figure 2. Sitting Disease: Cause of Back Pain and Much More
According to Peper, people who spend extended periods of time at their computers are at risk of developing sitting disease—a condition of increased sedentary behavior associated with adverse health effects. A study that appeared in the American Journal of Preventative Medicine found that prolonged sitting was associated with an increased risk of 34 chronic diseases and conditions including chronic back and musculoskeletal pain. According to the study, “Being seated alters the activation patterns of multiple weight-bearing muscles and, therefore, excessive desk use is associated with adverse back curvature, back pain and upper extremity problems such as carpel tunnel syndrome.”
To Avoid Back Pain, Don’t Slouch!
Sitting for prolonged periods of time can cause back, neck, arm, and leg pain, but slouching is even worse and can damage spinal structures. “Most people slouch at computer, and when you slouch, our spine becomes more like the letter C, our abdomen is compressed, the diaphragm goes up which causes us to shallow breathe in our upper chest,” Peper said. “That impacts our back and digestion and many other things.”
According to Peper, slouching can also impact our mood. “Slouching is the posture associated with depression and low energy. That posture collapse may evoke negative and hopeless emotions. If I sit up and look up, I have less of that. I can have more positive and uplifting thinking.”
Peper recommends a simple device to help people improve their posture. Called an Upright Go, it attaches to the neck and provides vibrational feedback when slouching occurs. “Every time it starts buzzing, it’s a reminder to stop slouching and to get up, wiggle, and move,” he said. “We have published some studies on it, but I have no investment in the company.”
Peper’s 4 Basic Tips for Avoiding Back Pain and Other Sitting Diseases:
#1 Get Up and Move
“Rule one is to take many breaks—wiggle and move,” he said. “People are unaware that they slightly raise their shoulders and their arm goes slightly forward—in their mousing especially. By the end of the day, they feel stiffness in their shoulders or back. So, you need to take many wiggly breaks. Get up from your chair every 15 minutes.”
Use Stretch Break or one of the other apps that remind people to get up out of their chairs and stretch.
Walk around while on the phone and wear a headset to improve posture while on the phone.
For back pain, skip in place or lift the right arm at the same time as the left knee followed by the left arm and right knee–exercises that cause a diagonal stretch along the back.
#2 Just Breathe
- “Learn to practice lower breathing,” Peper said. “When you sit, you are forced to breath higher in your chest. You want to practice slow diaphragmatic breathing. Breathe deeply and slowly to restore a natural rhythm. Take three deep breaths, inhaling for five seconds, then exhale very slowly for six seconds.” For more instructions on slower diaphragmatic breathing visit Peper’s blog on the subject.
#3 Take Visual Breaks:
- Our blinking rate significantly decreases while looking at a screen, which contributes to eye strain. To relax the eyes, look at the far distance. “Looking out into the distance disrupts constant near-focus muscle tension in the eyes,” he said. By looking into the distance, near-focus muscle tension in the eyes is disrupted.
- If you have children, make sure they are taking frequent visual breaks from their screens. According to Peper, there has been a 20 percent increase in myopia (nearsightedness) in young children as a result of COVID-related distance learning. “The eyes are being formed and shaped during childhood, and if you only focus on the screen, that changes the muscle structure of our eyes over time leading to more myopia.”
#4 Pay Attention to Ergonomics
- “If you are working on a desktop, the top of screen should be at eyebrow level,” Peper said. “Your feet should be on the ground, and the angle of the knees should be about 110 degrees. You should feel support in mid back and low back and be able to sit, lean back, and be comfortable.”
- Peper recommends adjustable sit/stand desks and regularly alternating between sitting and standing.
For more specific guidance on ergonomics for prolonged sitting, UCLA School of Medicine offers detailed guidelines. And don’t forget to check out Dr. Peper’s book on ergonomics as well as his blog, The Peper Perspective, where you can use the search feature to help you find exactly what you are looking for.
But in the meantime, Dr. Peper said, “It’s time for you to get up and wiggle!”
Find a Provider Who Can Help with Back Pain
Christine Graf is a freelance writer who lives in Ballston Lake, New York. She is a regular contributor to several publications and has written extensively about health, mental health, and entrepreneurship.
Healing chronic back pain
Posted: July 31, 2022 Filed under: behavior, Breathing/respiration, CBT, cognitive behavior therapy, education, healing, health, meditation, relaxation, self-healing, stress management, surgery | Tags: back pain, Imagery, self-care, visualization 4 CommentsErik Peper, PhD, BCB, Jillian Cosby, and Monica Almendras
Adapted from Peper, E. Cosby, J. & Amendras, M. (2022).Healing chronic back pain. NeuroRegulation, 9(3), 165-172. https://doi.org/10.15540/nr.9.3.164

In at the beginning of 2021, I broke my L3 vertebra during a motor cycle accident and underwent two surgeries in which surgeons replaced my shattered L3 with a metal “cage” (looks like a spring) and fused this cage to the L4 and L2 vertebrae with bars. I also broke both sides of my jaw and fractured my left shoulder. I felt so overwhelmed and totally discouraged by the ongoing pain. A year later, after doing the self-healing project as part of the university class assignment, I feel so much better all the time, stopped taking all prescription pain medications and eliminated the sharp pains in my back. This project has taught me that I have the skill set needed to be whole and healthy. –J.C., 28-year-old college student
Chronic pain is defined as a pain that persist or recurs for more than 3 months (Treede et al., 2019). It is exhausting and often associated with reduced quality of life and increased medical costs (Yong, Mullins, & Bhattacharyya, 2022). Pain and depression co-exacerbate physical and psychological symptoms and can lead to hopelessness (IsHak, 2018; Von Korff & Simon, 1996). To go to bed with pain and anticipate that pain is waiting for you as you wake up is often debilitating. One in five American adults experience chronic pain most frequently in back, hip, knee or foot (Yong, Mullins, & Bhattacharyya, 2022). Patients are often prescribed analgesic medications (“pain killers”) to reduce pain. Although, the analgesic medications can be effective in the short term to reduce pain, the efficacy is marginal for relieving chronic pain (Eriksen et al., 2006; Tan, & Jensen, 2007). Recent research by Parisien and colleagues (2022) reported that anti-inflammatory drugs were associated with increased risk of persistent pain. This suggest that anti-inflammatory treatments might have negative effects on pain duration. In addition, the long-term medication use is a major contributor to opioid epidemic and increased pain sensitivity (NIH– NIDA, 2022; Higgins, Smith, & Matthews, 2019; Koop, 2020). Pain can often be successfully treated with a multidisciplinary approach that incorporates non-pharmacologic approaches. These include exercise, acceptance and commitment therapy, as well as hypnosis (Warraich, 2022). This paper reports how self-healing strategies as taught as part of an undergraduate university class can be an effective approach to reduce the experience of chronic pain and improve health.
Each semester, about 100 to 150 junior and senior college students at San Francisco State University enroll in a holistic health class that focused on ‘whole-person’ Holistic Health curriculum. The class includes an assessment of complementary medicine and holistic health. It is based upon the premise that mind/emotions affect body and body affect mind/emotions that Green, Green & Walters (1970) called the psychophysiological principle.
“Every change in the physiological state is accompanied by an appropriate change in the mental emotional state, conscious or unconscious, and conversely, every change in the mental emotional state, conscious or unconscious, is accompanied by an appropriate change in the physiological state.”
The didactic components of the class includes the psychobiology of stress, the role of posture, psychophysiology of respiration, lifestyle and other health factors, reframing internal language, guided and self-healing imagery. Students in the class are assigned self-healing projects using techniques that focus on awareness of stress, dynamic regeneration, stress reduction imagery for healing, and other behavioral change techniques adapted from the book, Make Health Happen (Peper, Gibney, & Holt, 2002).
The self-practices during the last six weeks of the class focus on identifying, developing and implementing a self-healing project to optimize their personal health. The self-healing project can range from simple life style changes to reducing chronic pain. Each student identifies their project such as increasing physical activity, eating a healthy diet and reducing sugar and junk food, stopping vaping/smoking, reducing anxiety or depression, stopping hair pulling, reducing headaches, decreasing ezema, or back pain, etc. At the end of the semester, 80% or more of the students report significant reduction in symptoms (Peper, Sato-Perry, & Gibney, 2003; Peper, Lin, Harvey, Gilbert, Gubbala, Ratkovich, & Fletcher, 2014; Peper, Miceli, & Harvey, 2016; Peper, Harvey, Cuellar, & Membrila, 2022). During the last five semesters, 13 percent of the students focused reducing pain (e.g., migraines, neck and shoulder pain, upper or lower back pain, knee pain, wrist pain, and abdominal pain). The students successfully improved their symptoms an average of 8.8 on a scale from 0 (No benefit) to 10 (total benefit/improvement). The success for improving their symptoms correlates 0.63 with their commitment and persistence to the project (Peper, Amendras, Heinz, & Harvey, in prep).
The purposes of this paper is to describe a case example how a student with severe back pain reduced her symptoms and eliminated medication by implementing an integrated self-healing process as part of a class assignment and offer recommendations how this could be useful for others.
Participant: A 28-year-old female student (J.C.) who on January 28, 2021 broke her L3 vertebra in a motor cycle accident. She underwent two surgeries in which surgeons replaced her shattered L3 with a metal “cage” (which she describes as looking like a spring) and fused this cage to the L2 and L4 vertebrae with bars. She also broke both sides of her jaw and fractured her left shoulder. More than a year later, at the beginning of the self-healing project, she continue to take 5-10 mgs of Baclofen and 300 mgs of Gabapentin three times a day to reduce pain.
Goal of the self-healing project: To decrease the sharp pain/discomfort in her lower back that resulted from the motor cycle accident and, although not explicitly listed, to decrease the pain medications.
Self-healing process
During the last six weeks of the 2022 Spring semester, the student implemented her self-healing practices for her personal project which consisted of the following steps.
1. Create a self-healing plan that included exploring the advantage and disadvantage of her illness.
2. Develop a step-by-step plan with specific goals to relief her tension and pain in her lower back. This practice allowed her to quantify her problem and the solutions. Like so many people with chronic pain, she focused on the problem and feelings (physical and emotional) associated with the pain. As a result, she often feel hopeless and worried that it would not change.
3. Observe and evaluate when pain sensations changed. She recognized that she automatically anticipated and focused on the pain and anxiety whenever she needed to bend down into a squat. She realized that she had been anticipating pain even before she began to squat. This showed that she needed to focus on healing the movement of this area of her body.
Through her detailed observations, she realized that her previous general rating of back pain could be separated into muscle tightness/stiffness and pain. With this realization, she changed the way she was recording her pain level. She changed it from “pain level” into into two categories: tightness and sharp pains.
4. Ask questions of her unconscious through a guided practice of accessing an inner guide through imagery (For detailed instructions, see Peper, Gibney, & Holt, 2002, pages 197-206). In this self-guided imagery the person relaxes and imagines being in a special healing place where you felt calm, safe and secure. Then as you relaxed, you become aware of another being (wise one or guide) approaching you (the being can be a person, animal, light, spirit, etc.). The being is wise and knows you well. In your mind, you ask this being or guide questions such as, “What do I need to do to assist in my own healing?” Then you wait and listen for an answer. The answer may take many forms such as in words, a pictures, a sense of knowing, or it may come later in dreams or in other forms. When students are assigned this practice for a week, almost all report experiencing some form of guide and many find the answers meaningful for their self-healing project.
Through this imagery of the inner guide script, she connected with her higher self and the wise one told her to “Wait.” This connecting with the wise one was key in accepting that the project was not as daunting as she initially thought. She realized that pain was not going to be forever in her future. She also interpreted that as reminder to have patience with herself. Change takes practice, time and practice such as she previously experienced while correcting her posture to manage her emotions and edit her negative thoughts into positive ones (Peper, Harvey, Cuellar, & Membrila, 2022). Whenever she would have pain or feel discouraged because of external circumstances, she would remind herself of three things:
A. I need to have patience with myself.
B. I have all the healing tools inside me and I am learning to use them.
C. If I do not make time for my wellness, I’ll be forced to make time for my illness.
5. Practice self-healing imagery as described by Peper, Gibney, & Holt (2002) and adapted from the work by Dr. Martin Rossman (Rossman, 2000). Imagery can be the communication channel between the conscious/voluntary and the unconscious/autonomic/involuntary nervous system (Bressler, 2005; Hadjibalassi et al, 2018; Rossman, 2019). It appears to act as the template and post-hypnotic suggestion to implement behavior change and may offer insight and ways to mobilize the self-healing potential (Battino, 2020). Imagery is dynamic and changeable.
The process of self-healing imagery consists of three parts.
- Inspection the problem and drawing a graphic illustration of the problem as it is experienced at that moment of time.
- Drawing of how that area/problem would look when being completely well/whole or disappeared.
- Creation of a self-healing process by which the problem would become transformed into health (Peper, Gibney & Holt, 2002, pp. 217-236). The process focused on what the person could do for themselves; namely, each time they became aware of, anticipated, or felt the problem, they would focus on the self-healing process. It provideshope; since, the person now focuses on the healing of the problem and becoming well.
The drawings of inspection of the pain and problem she experienced at that moment of time are shown in Figure 1.

Figure 1. Illustration of the problem of the pain. Thorns dug deep, muscles tight, and frozen vertebrates grinding.
The resolution of the problem and being well/whole are illustrated in Figure 2.

Figure 2. Resolution of the problem in which her muscles are warm, full of blood, free of thorns, relaxed and flexible and being whole happy and healthy in which her spine is warm, her muscles are warm, her back is flexible and full of movement.
Although she utilized the first image of the muscles warm, full of blood, free of thorns and the muscles relaxed and flexible, her second image of her fully being healed was inspired through a religious statue of Yemaya that she had in her room (Yemaya is a major water spirit from the Yoruba religion Santeria and Orisha of the seas and protector of women). Each time she saw the statue, she thought of the image of herself fully healed and embodying the spirit Orisha. Therefore, this image remained important to her all the time.
Her healing imagery process by which she transforms the image of inspecting of the problem to being totally well are illustrated in Figure 3.

Figure 3. The healing process: The sun’s warm fingers thaw my muscles, lubricate my vertebra, thorns fall out, and blood returns.
For five weeks as she implemented her self-healing project by creating a self-healing plan, asking questions of her unconscious, drawing her self-healing imagery. She also incorporated previously learned skills from the first part of the semester such diaphragmatic breathing, hand warming, shifting slouching to upright posture, and changing language. Initially she paired hand warming with the self-healing imagery and she could feel an increase in body warmth each time she practiced the imagery. She practiced the self-healing imagery as an in-depth daily practice and throughout the day when she became aware of her back as described in one of her log entries.
I repeated the same steps as the day prior today. I did my practice in the early morning but focused on the details of the slowed down movements of the sun’s hands. I saw them as they stretched out to my back, passed through my skin, wrapped around my muscles, and began to warm them. I focused on this image and tried to see, in realistic detail, my muscles with a little ice still on them, feeling hard through and through, the sun’s glowing yellow-orange fingers wrapped around my muscles. I imaged the thorns still in my muscles, though far fewer than when I started, and then I imaged the yellow-orange glow start to seep out from the sun’s palms and fingers and spread over my muscles. I imaged the tendons developing as the muscle tissue thawed and relaxed, the red of the muscle brightened, the ice on and within my muscles started to melt, and the condensation formed as it ran down into collected droplets at the bottom of my muscles. I imaged the thorns lose their grip and fall out, one at a time, in tandem with the droplets falling. I continued this process and imaged my muscles expanding with warmth and relaxation as they stayed engulfed in the warmth of the sun.
At the end of my practice, I did a small stretch session. I felt extremely refreshed and ready for yet another extremely busy day between internship, graduation, and school. I would say I felt warm and relaxed all the way into the afternoon, about 6 hours after my practice. This was by far the most detailed and impactful imagery practice I have had.
The self-healing imagery practice provided me with the ability to conceptualize more than my problem as it showed me the tools to (and the importance of) conceptualizing my solution, both the tool and end result.
Results
Pain and tightness decreased and she stopped her medication by the third week as shown in Figure 4.

Figure 4. Self-rating of sharp pains and tightness during the self-healing project.
At the 14-week follow-up, she has continued to improve, experiences minimal discomfort, and no longer takes medication. As she stated, I was so incredibly shocked how early on [in the project] I was able to stop taking pain medications that I had already taken every day for over a year.
Discussion
This individual case example provides hope that health can be improved when shifting the focus from pain and discomfort to focusing on actively participating in the self-healing process. As she wrote, The lesson was self- empowerment in regard to my health. I brought comfort to my back. There is metal in my back for the rest of my life and this is something I have accepted. I used to look at that as a horrible thing to have to handle forever. I now look at it as a beautiful contraption that has allowed me to walk across a graduation stage despite having literally shattered a vertebra. I am reintegrating these traumatized parts of my body back into a whole health state of mind and body. Doctors did not do this, surgeries did not, PT didn’t and neither did pain medications. MY body and MY mind did it. I did this.
Besides the self-healing imagery and acting upon the information she received from the asking questions from the unconscious there were many other factors contributed to her healing. These included the semester long self-practices and mastery of different stress management techniques, learning how stress impacts health and what can the person can do to self-regulate, as well as being introduced to the many case examples and research studies that suggested healing could be possible even in cases where it seemed impossible.
The other foundational components that was part of the class teachings included attending the weekly classes session and completing the assign homework practices. These covered discussion about placebo/nocebo, possibilities and examples of self-healing with visualization, the role of nutrition, psychophysiology of stress and factors are associated with healthy aging across cultures. The asynchronous assignments investigated factors that promoted or inhibited health and the role of hope. The discussions pointed out that not everyone may return to health; however, they can always be whole. For example, if a person loses a limb, the limb will not regrow. The healing process includes acceptance and creating new goals to achieve and live a meaningful life.
The possibility that students could benefit by implementing the different skills and concepts taught in the class were illustrated by sharing previous students’ successes in reversing disorders such as hair pulling, anxiety, psoriasis, and pain. In addition, students were assigned to watch and comment on videos of people who had overcome serious illness. These included Janine Shepherd’s 2012 TED talk, A broken body isn’t a broken person, and Dr. Terry Wahl’s 2011 TEDxIowaCity talk, Minding your mitochondria. Janine Shepard shared how she recovered from a very serious accident in which she became paralyzed to becoming an aecrobatic pilot instructor while Dr. Terry Wahl shares how she he used diet to cure her MS and get out of her wheelchair (Shepherd, 2012; Wahl, 2011). Other assignments included watching Madhu Anziani’s presentation, Healing from paralysis-Music (toning) to activate health, in which he discussed his recovery from being a quadriplegic to becoming an inspirational musician (Anziani, & Peper, 2021). The students as read and commented on student case examples of reversing acid reflux, irritable bowel and chronic headaches (Peper, Mason, & Huey, 2017a; Peper, Mason, & Huey, 2017b; Peper, 2018; Peper et al., 2020; Peper, Covell, & Matzembacker, 2021; Peper, 2022).
Although self-healing imagery appears to be the major component that facilitated the healing, it cannot be separated from the many other concepts and practices that may have contributed. For example, the previous practices of learning slow diaphragmatic breathing and hand warming may have allowed the imagery to become a real kinesthetic experience. In addition, by seeing how other students overcame chronic disorders, the class provided a framework to mobilize one’s health.
Lessons extracted from this case example that others may be able use to mobilize health.
- Take action to shifts from being hopeless and powerless to becoming empowered and active agent in the healing process.
- Change personal beliefs through experiential practices and storytelling that provides a framework that healing and improvement are possible.
- Teach the person self-regulation skills such as slower breathing, muscle relaxation, cognitive internal language changes, hand warming by which the person experiences changes.
- Provide believable role models who shared their struggle in overcoming traumatic injury, watch inspirational talks, and share previous clients or students’ self-reports who had previously improved.
- Transform the problem from global description into behavioral specific parts. For example, being depressed is a global statement and too big to work on. Breaking the global concept into specific behaviors such as, my energy is too low to do exercise or I have negative thoughts, would provide specific interventions to work on such as, increasing exercise or changing thoughts. In JC’s case, she changed the general rating of pain into ratings of muscle tightness and sharp pains. This provided the bases for strategies to relax and warm her muscles.
- Focus on what you can do at that moment versus focusing on the past, what happened, who caused it, or blaming yourself and others. Explore and ask what you now can do now to support your healing process and reframe the problem as a new opportunity for growth and development.
- Practice, practice, and practice with a childlike exploratory attitude. Focus on the small positive benefits that occur as a result of the practices. It is not mindless practice; it is practice while being present and being gentle with yourself. Do not discard very small changes. The benefits accrue as you practice more and more, just many people have experienced when learning to play a musical instrument or mastering a sport. Even though many participants think that practicing 15 minutes a day is enough, it usually takes much more time. Reflect on how a baby learns to walk or climb. The toddler practices day-long and takes naps to regenerate and grow. When the toddler is not yet successful in walking or climbing, it does not give up or interpret it as failure or blaming himself that he cannot do it, it just means more practice.
- Have external reminders to evoke the self-healing practices. In JC’s case, the small statue of Yemaya in her room was the reminder. It reminded her to thinks of the image of herself fully healed each time she saw it.
- Guide yourself through the wise one imagery, ask yourself a question and listen and act on the intuitional answers.
- Develop a self-healing imagery process that transforms the dysfunction to health or wholeness. Often the person only perceives the limitations and focusses on describing the problem. Instead, acknowledge, accept what was and is, and focus on developing a process to promote healing. What many people do not realize that if they think/imagine how their injury/illness was caused, it may reactivate and recreate the initial trauma. This can be illustrated through imagery. When we think or imagine something, it changes our physiology. For example, when one imagines eating a lemon, many people will salivate. The image affects physiology. Thus, focus on processes that support healing.
- While practicing the imagery, experience it as if it is real and feel it happening inside yourself. Many people initially find this challenging as they see it outside themselves. One way to increase the “felt sense” is to incorporate more body involvement such as acting out the imagery with hand and body movements.
- When having a relapse, remind yourself to keep going. Every morning is the beginning of a new day, do each practices anew. In addition, reflect of something that was challenging in the past but that you successfully overcame. Focus on that success. As JC wrote, I was also successful in that I gave myself slack and reminded myself that relapses will happen and what matters more is the steps I take to move forward.
- Make your healing a priority that means doing it often during the day. Allow the self-healing imagery and process to run in the back of the head all the time just as a worry can be present in the background. So often people practice for a few minutes (which is great and better than not practicing at all); however, at other times during the day they are captured by their worry, negative thoughts or focus on the limitations of the disorder. When a person focuses on the limitations, it may interrupt the self-healing process. The analogy we often use is that the healing process is similar to healing from a small cut in the skin. Initially a scab forms and eventually the scab falls off and the skin is healed. On the other hand, if you keep moving the skin or pick on the scab, healing is much slower. By focusing on the limitations and past visualization of the injury, self-healing is reduced. This is similar to removing the scab before the skin has healed. As JC stated, “If you don’t make time for your wellness, you’ll be forced to make time for your illness” was 100% a motivating factor in my success.
- Explore resources for providers and people living with pain. See Dr. Rachel Zoffness website which provides a trove of high quality articles, books, videos, apps, and podcasts. https://www.zoffness.com/resources
In summary, we do not know the limits of self-healing; however, this case example illustrates that by implementing self-healing strategies health and recovery occurred. As JC wrote:
To have broken a vertebra in my back and experience all the injuries that came with the accident when I already did not have the strongest mind-body connection was incredibly intense and really heartbreaking and discouraging in my life. And, that made things difficult because I was not able to 100% focus on my healing because I felt so overwhelmed by the feeling of discouragement that I felt. Experiencing this self-healing project, seeing the imagery that helped me not just feel so much better all the time but be able to stop taking all prescription pain medications and eliminate the sharp pains in my back has taught me that I have the skill set needed to be whole and healthy.
Watch the interview will Jillian Cosby inwhich she describes her self-healing process.
References
Anziani, M. & Peper, E. (2021). Healing from paralysis-Music (toning) to activate health. The peperperspective. https://peperperspective.com/2021/11/22/healing-from-paralysis-music-toning-to-activate-health/
Battino, R. (2020). Using Guided Imagery and Hypnosis in Brief Therapy and Palliative Care. New York: Routledge.
Bresler, D. (2005).Physiological Consequences of Guided Imagery. Pract Pain Manag, 5(6). https://www.practicalpainmanagement.com/treatments/complementary/biobehavioral/physiological-consequences-guided-imagery
Eriksen, J., Sjøgren, P., Bruera, E., et al. (2006). Critical issues on opioids in chronic non-cancer pain: An epidemiologic study. Pain, 125,172–179. https://doi.org/10.1016/j.pain.2006.06.009
Green, E. E., Green, A. M., & Walters, E. D. (1970). Voluntary control of internal states: Psychological and physiological. The Journal of Transpersonal Psychology, 2(1), 1. https://atpweb.org/jtparchive/trps-02-70-01-001.pdf
Hadjibalassi, M., Lambrinou, E.., Papastavrou,E., & Papathanassoglou, E. (2018). The effect of guided imagery on physiological and psychological outcomes of adult ICU patients: A systematic literature review and methodological implications, Australian Critical Care, 31(2), 73-86. https://doi.org/10.1016/j.aucc.2017.03.001
Higgins, C, Smith, B.H., & Matthews, K. (2019). Evidence of opioid-induced hyperalgesia in clinical populations after chronic opioid exposure: a systematic review and meta-analysis, British Journal of Anaesthesia, 122(6), e114-e126. https://doi.org/10.1016/j.bja.2018.09.019
IsHak, W.W., Wen, R.Y., Naghdechi, L., Vanle, B., Dang, J., Knosp, M., Dascal, J., Lobsang, Gohar, Y.,; Eskander, L., Yadegar, J., Hanna, S., Sadek, A., Aguilar-Hernandez, L., Danovitch, I., Louy, C. (2018). Pain and Depression: A Systematic Review, Harvard Review of Psychiatry, 11/12, 26(6), 352-363. https://doi.org/10.1097/HRP.0000000000000198
Koob, G.F. (2020). Neurobiology of Opioid Addiction: Opponent Process, Hyperkatifeia, and Negative Reinforcement, Biological Psychiatry, 87(1), 44-53. https://doi.org/10.1016/j.biopsych.2019.05.023
Mullins, P.M., & Bhattacharyya, N. (2022). Prevalence of chronic pain among adults in the United States, Pain, 163(2), e328-e332. https://doi.org/10.1097/j.pain.0000000000002291NIH–
NIDA (2022). Opioid Overdose Crisis. Downloaded June 30, 2022. https://nida.nih.gov/research-topics/opioids/opioid-overdose-crisis
Parisien, M., Lima, L.V., Dagostino, C., El-Hachem, N., Drury, G.L., Grant, A.V., Huising, J., Verma, V…. .(2022). Acute inflammatory response via neutrophil activation protects against the development of chronic pain. Science Translational Medicine, 14(644). https://doi.org/10.1126/scitranslmed.abj99
Peper, E. (2018). Breathing reduces acid reflux and dysmenorrhea discomfort. the peperperspective. https://peperperspective.com/2018/10/04/breathing-reduces-acid-reflux-and-dysmenorrhea-discomfort/
Peper, E. (2022). Resolving a chronic headache with posture feedback and breathing. the peperperspective. https://peperperspective.com/2022/01/04/resolving-a-chronic-headache-with-posture-feedback-and-breathing/
Peper, E., Almedras, M., Heinz, N. & Harvey, R. (in prep). How attending a Holistic Health class reduced symptoms.
Peper, E. Cosby, J. & Amendras, M. Healing chronic back pain. NeuroRegulation, 9I(3), 165-172. https://doi.org/10.15540/nr.9.3.164
Peper, E., Covell, A., & Matzembacker, N. (2021). How a chronic headache condition became resolved with one session of breathing and posture coaching. NeuroRegulation, 8(4), 194–197. https://doi.org/10.15540/nr.8.4.194
Peper, E., Gibney, K.H. & Holt. C. (2002). Make Health Happen: Training Yourself to Create Wellness. Dubuque, IA: Kendall-Hunt.ISBN: 978-0787293314 https://he.kendallhunt.com/make-health-happen
Peper, E., Harvey, R., Cuellar, Y., & Membrila, C. (2022). Reduce anxiety. NeuroRegulation, 9(2), 91–97. https://doi.org/10.15540/nr.9.2.91 https://www.neuroregulation.org/article/view/22815/14575
Peper, E., Lin, I-M., Harvey, r., Gilbert, M. Gubbala, P, Ratkovich, A., & Fletcher, L. (2014). Transforming Chained Behaviors: Case Studies of Overcoming Smoking, Eczema, and Hair Pulling (Trichotillomania), Biofeedback, 42 (4), 154–160. https://doi.org/10.5298/1081-5937-42.4.06
Peper, E., Mason, L, & Huey, C. (2017a). Healing irritable bowel syndrome with diaphragmatic breathing. the peperperspective. https://peperperspective.com/2017/06/23/healing-irritable-bowel-syndrome-with-diaphragmatic-breathing/
Peper, E., Mason, L., Huey, C. (2017b). Healing irritable bowel syndrome with diaphragmatic breathing. Biofeedback. (45-4). https://doi.org/10.5298/1081-5937-45.4.04
Peper, E., Mason, L., Harvey, R., Wolski, L, & Torres, J. (2020). Can acid reflux be reduced by breathing? Townsend Letters-The Examiner of Alternative Medicine, 445/446, 44-47. https://www.townsendletter.com/article/445-6-acid-reflux-reduced-by-breathing/
Peper, E., Miceli, B., & Harvey, R. (2016). Educational Model for Self-healing: Eliminating a Chronic Migraine with Electromyography, Autogenic Training, Posture, and Mindfulness. Biofeedback, 44(3), 130–137. https://doi.org/10.5298/1081-5937-44.3.03
Peper, E., Sato-Perry, K & Gibney, K. H. (2003). Achieving Health: A 14-Session Structured Stress Management Program—Eczema as a Case Illustration. 34rd Annual Meeting of the Association for Applied Psychophysiology and Biofeedback. Abstract in: Applied Psychophysiology and Biofeedback, 28(4), 308. https://biofeedbackhealth.files.wordpress.com/2013/12/2003-aapb-poster-peper-keiko-long1.pdf
Peper, E., Lin, I-M, Harvey, R., Gilbert, M., Gubbala, P., Ratkovich, A., & Fletcher, F. (2014). Transforming chained behaviors: Case studies of overcoming smoking, eczema and hair pulling (trichotillomania). Biofeedback, 42(4), 154-160. https://doi.org/10.5298/1081-5937-42.4.06
Rossman, M. L.(2000). Guided imagery for self-healing. New York: New World Library. https://www.amazon.com/Guided-Imagery-Self-Healing-Martin-Rossman/dp/091581188X/ref=sr_1_3?crid=3M8I1Y1NV3A5N&keywords=martin+rossman&qid=1657649675&s=books&sprefix=rossman%2C+M%2Cstripbooks%2C131&sr=1-3
Rossman, M. L. (2019). Imagine health! Imagery in medical self-care. InSheikh, A.A. (ed). Imagination and healing (pp. 231-258). Routledge. https://www.amazon.com/Imagination-Healing-Imagery-Human-Development-ebook/dp/B07QB4RGSW/ref=sr_1_9?crid=3C7V3E5ZN92R&keywords=Imagination+and+healing&qid=1657818303&s=books&sprefix=imagination+and+healing+%2Cstripbooks%2C105&sr=1-9
Sheng, J., Liu, S., Wang, Y., Cui, R., & Zhang, X. (2017). The link between depression and chronic pain: Neural mechanisms in the brain. Neural Plasticity, 2017, Article 9724371. https://doi.org/10.1155/2017/9724371
Shepherd, Janine. (2012). A broken body isn’t a broken person. TEDxKC. https://www.ted.com/talks/janine_shepherd_a_broken_body_isn_t_a_broken_person
Tan, G., & Jensen, M. P. (2007). Integrating complementary and alternative medicine into multidisciplinary chronic pain treatment. In Chronic Pain Management (pp. 75-99). CRC Press. https://www.taylorfrancis.com/chapters/edit/10.3109/9781420045130-6/integrating-complementary-alternative-medicine-multidisciplinary-chronic-pain-treatment-gabriel-tan-mark-jensen
Treede, R-D., Rief, W., Barke, A., Aziz, Q., Bennett, M.I., Benoliel, R., Cohen, M., Evers, S., Finnerup, N.B., First, M.B., Giamberardino, M.A., Kaasa, S., Korwisi, B., Kosek, E., Lavand’homme, P., ; Nicholas, M., Perrot, S., Scholz, J., Schug, S., Smith, B.H., ; Svensson, P., Vlaeyen, J.S., & Wang, S-J. (2019). Chronic pain as a symptom or a disease: the IASP Classification of Chronic Pain for the International Classification of Diseases (ICD-11), Pain, 160(1), 19-27. https://do.org/10.1097/j.pain.0000000000001384
Von Korff, M. & Simon, G. (1996). The relationship between pain and depression. British Journal of Psychiatry, 168(S30), 101-108. https://doi.org/10.1192/S0007125000298474
Wahl, T. (2011). Minding your mitochondria. TEDzIowaCity. https://www.youtube.com/watch?v=KLjgBLwH3Wc
Warraich, H. (2022). Medicine has failed chronic pain patients. Here’s what they need. Pscyhe, Aeon, https://psyche.co/ideas/medicine-has-failed-chronic-pain-patients-heres-what-they-need
Yong, R. J., Mullins, P. M., & Bhattacharyya, N. (2022). Prevalence of chronic pain among adults in the United States. Pain, 163(2), e328-e332. https://doi.org/10.1097/j.pain.0000000000002291
Freedom of movement with the Alexander Technique
Posted: April 26, 2022 Filed under: behavior, computer, digital devices, education, emotions, ergonomics, Exercise/movement, healing, health, Pain/discomfort, posture, screen fatigue, self-healing, stress management, Uncategorized | Tags: Alexander Technique, back pain, neck and shoulder pain, somatics 3 CommentsErik Peper and Elyse Shafarman
After taking Alexander Technique lessons I felt lighter and stood taller and I have learned how to direct myself differently. I am much more aware of my body, so that while I am working at the computer, I notice when I am slouching and contracting. Even better, I know what to do so that I have no pain at the end of the day. It’s as though I’ve learned to allow my body to move freely.
The Alexander Technique is one of the somatic techniques that optimize health and performance (Murphy, 1993). Many people report that after taking Alexander lessons, many organic and functional disorders disappear. Others report that their music or dance performances improve. The Alexander Technique has been shown to improve back pain, neck pain, knee pain walking gait, and balance (Alexander technique, 2022; Hamel, et al, 2016; MacPherson et al., 2015; Preece, et al., 2016). Benefits are not just physical. Studying the technique decreases performance anxiety in musicians and reduces depression associated with Parkinson’s disease (Klein, et al, 2014; Stallibrass et al., 2002).
Background
The Alexander Technique was developed in the late 19th century by the Australian actor, Frederick Matthias Alexander (Alexander, 2001). It is an educational method that teaches students to align, relax and free themselves from limiting tension habits (Alexander, 2001; Alexander technique, 2022). F.M Alexander developed this technique to resolve his own problem of becoming hoarse and losing his voice when speaking on stage.
Initially he went to doctors for treatment but nothing worked except rest. After resting, his voice was great again; however, it quickly became hoarse when speaking. He recognized that it must be how he was using himself while speaking that caused the hoarseness. He understood that “use” was not just a physical pattern, but a mental and emotional way of being. “Use” included beliefs, expectations and feelings. After working on himself, he developed the educational process known as the Alexander Technique that helps people improve the way they move, breathe and react to the situations of life.
The benefits of this approach has been documented in a large randomized controlled trial of one-on-one Alexander Technique lessons which showed that it significantly reduced chronic low back pain and the benefits persisted a year after treatment (Little, et al, 2008). Back pain as well as shoulder and neck pain often is often related to stress and how we misuse ourselves. When experiencing discomfort, we quickly tend to blame our physical structure and assume that the back pain is due to identifiable structural pathology identified by X-ray or MRI assessments. However, similar structural pathologies are often present in people who do not experience pain and the MRI findings correlate poorly with the experience of discomfort (Deyo & Weinstein, 2001; Svanbergsson et al., 2017). More likely, the causes and solutions involve how we use ourselves (e.g., how we stand, move, or respond to stress). A functional approach may include teaching awareness of the triggers that precede neck and back tension, skills to prevent the tensing of those muscles not needed for task performance, resolving psychosocial stress and improving the ergonomic factors that contribute to working in a stressed position (Peper, Harvey & Faass, 2020). Conceptually, how we are use ourselves (thoughts, emotions, and body) affects and transforms our physical structure and then our physical structure constrains how we use ourselves.

Watch the video with Alexander Teacher, Elyse Shafarman, who describes the Alexander Technique and guides you through practices that you can use immediately to optimize your health while sitting and moving.
See also the following posts:
References
Alexander, F.M. (2001). The Use of the Self. London: Orion Publishing. https://www.amazon.com/Use-Self-F-M-Alexander/dp/0752843915
Alexander technique. (2022). National Health Service. Retrieved 19 April, 2022/. https://www.nhs.uk/conditions/alexander-technique/
Deyo, R.A. & Weinstein, J.N. (2001). Low back pain. N Engl J Med., 344(5),363-70. https://doi.org/10.1056/NEJM200102013440508
Hamel, K.A., Ross, C., Schultz, B., O’Neill, M., & Anderson, D.I. (2016). Older adult Alexander Technique practitioners walk differently than healthy age-matched controls. J Body Mov Ther. 20(4), 751-760. https://doi.org/10.1016/j.jbmt.2016.04.009
Klein, S. D., Bayard, C., & Wolf, U. (2014). The Alexander Technique and musicians: a systematic review of controlled trials. BMC complementary and alternative medicine, 14, 414. https://doi.org/10.1186/1472-6882-14-414
Little, P. Lewith, W G., Webley, F., Evans, M., …(2008). Randomised controlled trial of Alexander technique lessons, exercise, and massage (ATEAM) for chronic and recurrent back pain. BMJ, 337:a884. https://doi.org/10.1136/bmj.a884
MacPherson, H., Tilbrook, H., Richmond, S., Woodman, J., Ballard, K., Atkin, K., Bland, M., et al. (2015). Alexander Technique Lessons or Acupuncture Sessions for Persons With Chronic Neck Pain: A Randomized Trial. Ann Intern Med, 163(9), 653-62. https://doi.org/10.7326/M15-0667
Murphy, M. (1993). The Future of the Body. New York: Jeremy P. Tarcher/Perigee.
Preece, S.J., Jones, R.K., Brown, C.A. et al. (2016). Reductions in co-contraction following neuromuscular re-education in people with knee osteoarthritis. BMC Musculoskelet Disord 17, 372. https://doi.org/10.1186/s12891-016-1209-2
Stallibrass, C., Sissons, P., & Chalmers. C. (2002). Randomized controlled trial of the Alexander technique for idiopathic Parkinson’s disease. Clin Rehabil, 16(7), 695-708. https://doi.org/10.1191/0269215502cr544oa
Svanbergsson, G., Ingvarsson, T., & Arnardóttir RH. (2017). [MRI for diagnosis of low back pain: Usability, association with symptoms and influence on treatment]. Laeknabladid, 103(1):17-22. Icelandic. https://doi.org/10.17992/lbl.2017.01.116
Tuomilehto, J., Lindström, J., Eriksson, J.G., Valle, T.T., Hämäläinen, H., Ilanne-Parikka, P., Keinänen-Kiukaanniemi, S., Laakso, M., Louheranta, A., Rastas, M., et al. (2001). Prevention of type 2 diabetes mellitus by changes in lifestyle among subjects with impaired glucose tolerance. N. Engl. J. Med., 344, 1343–1350. https://doi.org/10.1056/NEJM200105033441801
Uusitupa, Mm, Khan, T.A., Viguiliouk, E., Kahleova, H., Rivellese, A.A., Hermansen, K., Pfeiffer, A., Thanopoulou, A., Salas-Salvadó, J., Schwab, U., & Sievenpiper. J.L. (2019). Prevention of Type 2 Diabetes by Lifestyle Changes: A Systematic Review and Meta-Analysis. Nutrients, 11(11)2611. https://doi.org/10.3390/nu11112611
Posture and mood: implications and applications to health and therapy
Posted: November 28, 2017 Filed under: Neck and shoulder discomfort, posture, self-healing, Uncategorized | Tags: back pain, electromyography, ergonomics, neck and shoulder tension, posture, spinal alignment, stress management 7 CommentsThis blog has been reprinted from: Peper, E., Lin, I-M, & Harvey, R. (2017). Posture and mood: Implications and applications to therapy. Biofeedback.35(2), 42-48.
Slouched posture is very common and tends to increase access to helpless, hopeless, powerless and depressive thoughts as well as increased head, neck and shoulder pain. Described are five educational and clinical strategies that therapists can incorporate in their practice to encourage an upright/erect posture. These include practices to experience the negative effects of a collapsed posture as compared to an erect posture, watching YouTube video to enhance motivation, electromyography to demonstrate the effect of posture on muscle activity, ergonomic suggestions to optimize posture, the use of a wearable posture biofeedback device, and strategies to keep looking upward. When clients implement these changes, they report a more positive outlook and reduced neck and shoulder discomfort.
Background
Most people slouch without awareness when looking at their cellphone, tablet, or the computer screen (Guan et al., 2016) as shown in Figure 1. Many clients in psychotherapy and in biofeedback or neurofeedback training experience concurrent rumination and depressive thoughts with their physical symptoms. In most therapeutic sessions, clients sit in a comfortable chair, which automatically creates a posterior pelvic tilt and encourages the spine to curve so that the client sits in a slouched position. While at home, they sit on an easy chair or couch, which lets them slouch as they watch TV or surf the web.
Figure 1. (A). Employee working on his laptop. (B). Boy with ADHD being trained with neurofeedback in a clinic. (C). Student looking at cell phone. When people slouch and look at the screen, they tend to slouch and scrunch their neck.
In many cases, the collapsed position also causes people to scrunch their necks, which puts pressure on their necks that may contribute to developing headache or becoming exhausted. Repetitive strain on the neck and cervical spine may trigger a cervical neuromuscular syndrome that involves chronic neck pain, autonomic imbalance and concomitant depression and anxiety (Matsui & Fujimoto, 2011), and may contribute to vertebrobasilar insufficiency –a reduction in the blood supply to the hindbrain through the left and right vertebral arteries and basilar arteries (Kerry, Taylor, Mitchell, McCarthy, & Brew, 2008). From a biomechanical perspective, slouching also places more stress is on the cervical spine, as shown in Figure 2. When the neck compression is relieved, the symptoms decrease (Matsui & Fujimoto, 2011).
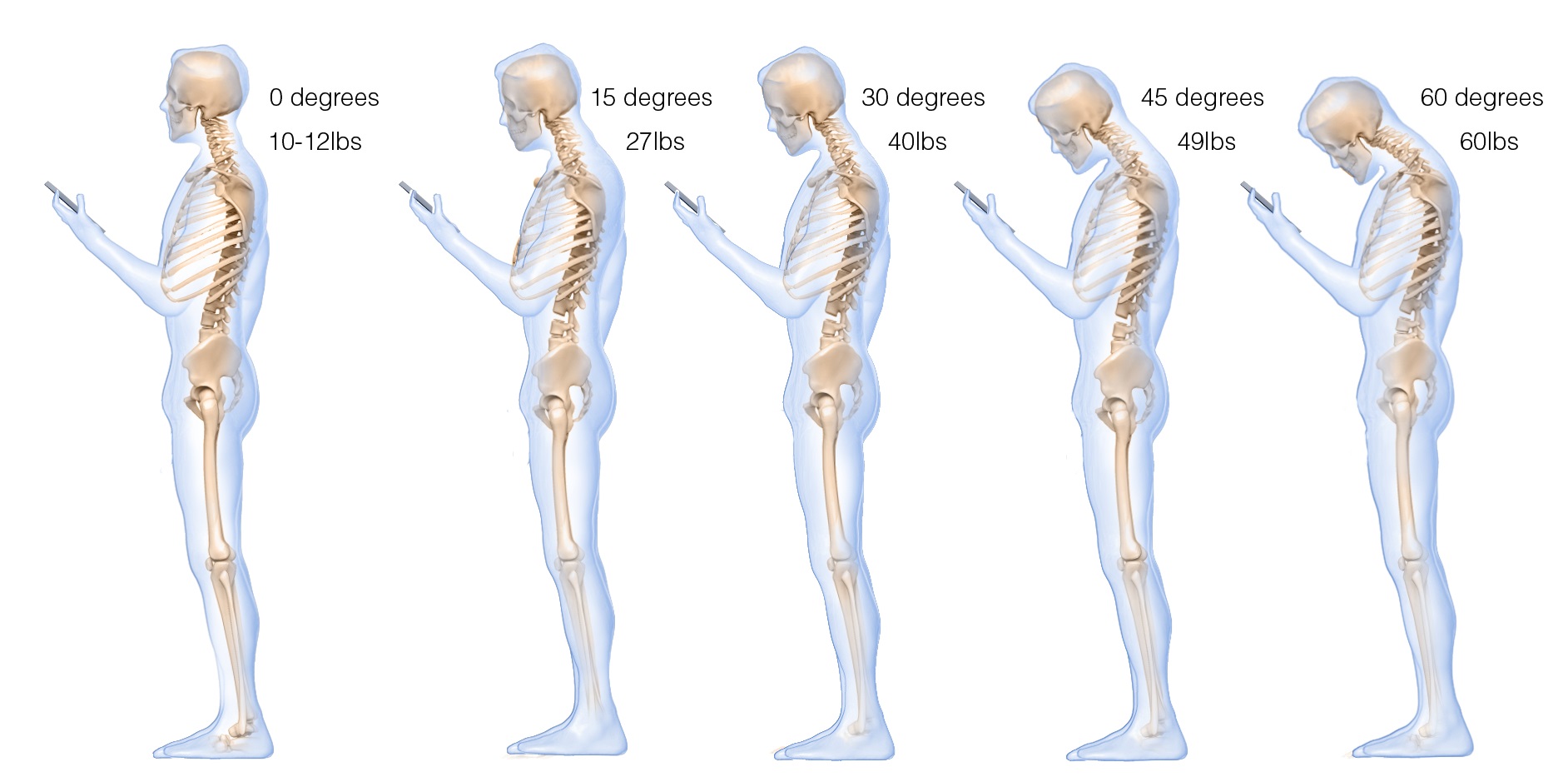 Figure 2. The more the head tilts forward, the more stress is placed on the cervical spine. Reproduced by permission from: Hansraj, K. K. (2014). Assessment of stresses in the cervical spine caused by posture and position of the head. Surgical Technology International, 25, 277–279.
Figure 2. The more the head tilts forward, the more stress is placed on the cervical spine. Reproduced by permission from: Hansraj, K. K. (2014). Assessment of stresses in the cervical spine caused by posture and position of the head. Surgical Technology International, 25, 277–279.
Most people are totally unaware of slouching positions and postures until they experience neck, shoulder, and/or back discomfort. Neither clients nor therapists are typically aware that slouching may decrease energy levels and increase the prevalence of negative (hopeless, helpless, powerless, or defeated) memories and thoughts (Peper & Lin, 2012; Peper et al, 2017)
Recommendations for posture awareness and training in treatment/education
The first step in biofeedback training and therapy is to systematically increase awareness and training of posture before attempting further bio/neurofeedback training and/or cognitive behavior therapy. If the client is sitting in a collapsed position in therapy, then it will be much more difficult for them to access positive thoughts, which interferes with further training and effective therapy. For example, research by Tsai, Peper, & Lin (2016) showed that engaging in positive thinking while slouched requires greater mental effort then when sitting erect. Sitting erect and tall contributes to elevated mood and positive thinking. An upright posture supports positive outcomes that may be akin to the beneficial effects of exercise for the treatment of depression (Schuch, Vancampfort, Richards, Rosenbaum, Ward, & Stubbs., 2016).
Most people know that posture affects health; however, they are unaware of how rapidly a slouching posture can impact their physical and mental health. We recommend the following educational and clinical strategies to teach this awareness.
- Practicing activities that raise awareness about a collapsed posture as compared to an erect posture
Guide clients through the practices so that they experience how posture can affect memory recall, physical strength, energy level, and possible triggering of headaches.
A. The effect of collapsed and erect posture on memory recall. Participants reported that it is much easier evoke powerless, hopeless, helpless, and defeated memories when sitting in a collapsed position than when sitting upright. Guide the client through the procedure described in the article, How posture affects memory recall and mood (Peper, Lin, Harvey, and Perez, 2017) and in the blog Posture affects memory recall and mood.
B. The effects of collapsed and erect posture on perceived physical strength. Participants experience much more difficulty in resisting downward pressure at the wrist of an outstretched arm when slouched rather than upright. Guide the client through the exercise described in the article, Increase strength and mood with posture (Peper, Booiman, Lin, & Harvey, 2016) and the blog, Increase strength and mood with posture.
C. The effect of slouching versus skipping on perceived energy levels. Participants experience a significant increase in subjective energy after skipping than walking slouched. Guide the client through the exercises as described in the article, Increase or decrease depression—How body postures influence your energy level (Peper & Lin, 2012).
D. The effect of neck compression to evoke head pressure and headache sensations. In our unpublished study with students and workshop participants, almost all participants who are asked to bring their head forward, then tilt the chin up and at the same time compress the neck (scrunching the neck), report that within thirty seconds they feel a pressure building up in the back of the head or the beginning of a headache. To their surprise, it may take up to 5 to 20 minutes for the discomfort to disappear. Practicing similar awareness activities can be a useful demonstration for clients with dizziness or headaches to experience how posture can increase their symptoms.
- Watching a Youtube video to enhance motivation.
Have clients watch Professor Amy Cuddy’s 2012 TED (Technology, Entertainment, and Design) Talk, Your body language shape who you are, which describes the hormonal changes that occur when adapting a upright power versus collapsed defeated posture.
- Electromyographic (EMG) feedback to demonstrate how posture affects muscle activity.
Record EMG from muscles such as around the cervical spine, trapezius, frontalis, and masseters or beneath the chin (submental lead) to demonstrate that having the head is forward and/or the neck compressed will increase EMG activity, as shown in Figure 3.

Figure 3. Electromyographic recording of the muscle under the chin while alternating between bringing the head forward or holding it back, feeling erect and tall.
The client can then learn awareness of the head and neck position. For example, one client with severe concussion experienced significant increase in head pressure and dizziness when she slouched or looked at a computer screen as well as feeling she would never get better. She then practiced the exercise of alternating her awareness by bringing her head forward and then back, and then bringing her neck back while her chin was down, thereby elongating the neck while she continued to breathe. With her head forward, she would feel her molars touching and with her neck back she felt an increase in space between the molars. When she elongated her neck in an erect position, she felt the pressure draining out of her head and her dizziness and tinnitus significantly decrease.
- Assessing ergonomics to optimize posture.
Change the seated posture of both the therapist and the client during treatment and training. Although people may be aware of their posture, it is much easier to change the external environment so that they automatically sit in a more erect power posture. Possible options include:
A. Seat insert or cushions. Sit in upright chairs that encourage an anterior pelvic tilt by having the seat pan slightly lower in the front than in the back or using a seat insert to facilitate a more erect posture (Schwanbeck, Peper, Booiman, Harvey, & Lin, 2015) as shown in Figure 4.

Figure 4. An example of how posture can be impacted covertly when one sits on a seat insert that rotates the pelvis anteriorly (The seat insert shown in the diagram and used in research is produced by BackJoy™).
B. Back cushion. Place a small pillow or rolled up towel at the kidney level so that the spine is slight arched, instead of sitting collapsed, as shown in Figure 5.
 Figure 5. An example of how a small pillow, placed between the back of the chair and the lower back, changes posture from collapsed to erect.
Figure 5. An example of how a small pillow, placed between the back of the chair and the lower back, changes posture from collapsed to erect.
C. Check ergonomic and work site computer use to ensure that the client can sit upright while working at the computer. For some, that means checking their vision if they tend to crane forward and crunch their neck to read the text. For those who work on laptops, it means using either an external keyboard, a monitor, or a laptop stand so the screen is at eye level, as shown in Figure 6.
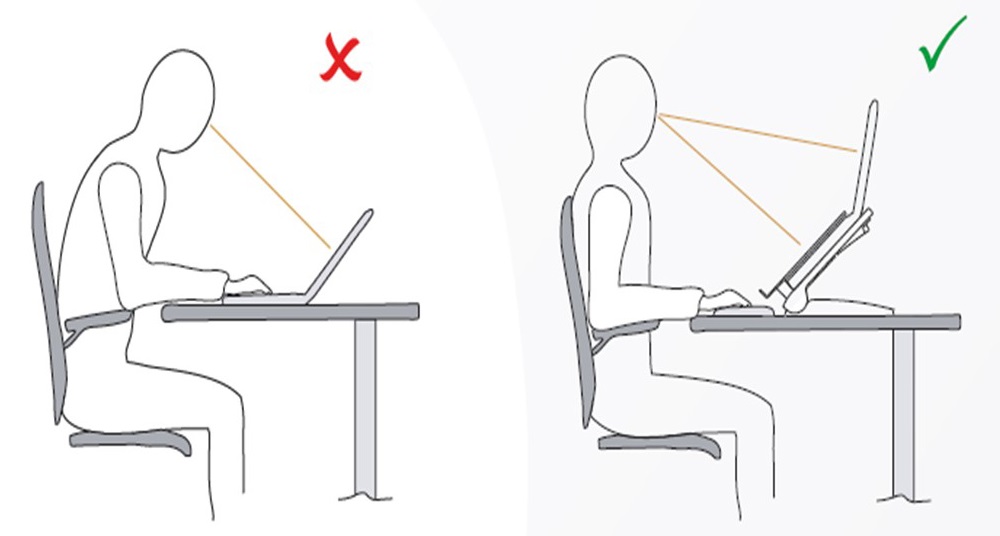 Figure 6. Posture is collapsed when working on a laptop and can be improved by using an external keyboard and monitor. Reproduced by permission from: Bakker Elkhuizen. (n.d.). Office employees are like professional athletes! (2017).
Figure 6. Posture is collapsed when working on a laptop and can be improved by using an external keyboard and monitor. Reproduced by permission from: Bakker Elkhuizen. (n.d.). Office employees are like professional athletes! (2017).
- Wearable posture biofeedback training device
The wearable biofeedback device, UpRight™, consists of a small sensor placed on the spine and works as an app on the cell phone. After calibration the erect and slouched positions, the posture device gives vibratory feedback each time the participant slouches, as shown in Figure 7.
Figure 7. Illustration of a posture feedback device, UpRight™. It provides vibratory feedback to the wearer to indicate that they are beginning to slouch.
Clinically, we have observed that clients can learn to identify conditions that are associated with slouching, such as feeling tired, thinking depressive/hopeless thoughts or other situations that evoke slouching. When people wear a posture feedback device during the day, they rapidly become aware of these subjective experiences whenever they slouch. The feedback reminds them to sit in an erect position, and they subsequently report an improvement in health (Colombo et al., 2017). For example, a 26-year-old man who works more than 8 hours a day on computer reported, “I have an improved awareness of my posture throughout my day. I also notice that I had less back pain at the end of the day.”
- Integrating posture awareness and position changes throughout the day
After clients have become aware of their posture, additional training included having them observe their posture as well and negative changes in mood, energy level or tension in their neck and head. When they become aware of these changes, they use it as a cue to slightly arch their back and look upward. If possible have the clients look outside at the tops of trees and notice details such as how the leaves and branches move. Looking at the details interrupts any ongoing rumination. At the same time, have them think of an uplifting positive memory. Then have them take another breath, wiggling, and return to the task at hand. Recommend to clients to go outside during breaks and lunchtime to look upward at the trees, the hills, or the clouds. Each time one is distracted, return to appreciate the natural patterns. This mental break concludes by reminding oneself that humans are like trees.
Trees are rooted in the earth and reach upward to the light. Despite the trauma of being buffeted by the storms, they continue to reach upward. Similarly, clouds reflect the natural beauty of the world, and are often visible in the densest city environment. The upward movement reflects our intrinsic resilience and growth. –Erik Peper
Have clients place family photos and art slightly higher on the wall at home so they automatically look upward to see the pictures. A similar strategy can be employed in the office, using art to evoke positive feelings. When clients integrate an erect posture into their daily lives, they experience a more positive outlook and reduced neck and shoulder discomfort.
Compliance with Ethical Standards:
Conflict of Interest: Author Erik Peper has received donations of 15 UpRight posture feedback devices from UpRight (http://www.uprightpose.com/) and 12 BackJoy seat inserts from Backjoy (https://www.backjoy.com) for use in research. Co-authors I-Mei Lin and Richard Harvey declare that they have no conflict of interest.
This report evaluated a convenience sample of a student classroom activity related to posture and the information was anonymous collected. As an evaluation of a classroom activity, this report of findings was exempted from Institutional Review Board oversight
References:
Bakker Elkhuizen. (n.d.). Office employees are like professional athletes! (2017). Retrieved from https://www.bakkerelkhuizen.com/knowledge-center/whitepaper-improving-work-performance-with-insights-from-pro-sports/
Cuddy, A. (2012). Your body language shapes who you are. Technology, Entertainment, and Design (TED) Talk, available at: www.ted.com/talks/amy_cuddy_your_body_language_shapes_who_you_are
We thank Frank Andrasik for his constructive comments.
Muscle biofeedback makes the invisible visible
Posted: January 6, 2012 Filed under: Uncategorized | Tags: back pain, biofeedback, electromyography, muscle tension, neck pain, performance, shoulder pain 3 Comments“I feel much more relaxed and realize now how unaware I was of the unnecessary tension I’ve been holding” is a common response after muscle biofeedback training. Many people experience exhaustion, stiffness, tightness, neck, shoulder and back pain while working long hours at the computer or while exercising. As we get older, we assume that discomforts are the result of aging. You just have to accept it and live with it–grin and bear it–or you need to be more careful while doing your job or performing your hobby. The discomfort in many cases is the result of misuse of your body. Observes what happens when you perform the following experiential practice Threading the needle.
Perform this task so that an observer would think it was real and would not know that you are only simulating threading a needle.
Imagine that you are threading a needle — really imagine it by picturing it in your mind and acting it out. Hold the needle between your left thumb and index finger. Hold the thread between the thumb and index finger of your right hand. Bring the tip of the thread to your mouth and put it between your lips to moisten it and make it into a sharp point. Then attempt to thread the needle, which has a very small eye. The thread is almost as thick as the eye of the needle.
As you are concentrating on threading this imaginary needle, observed what happened? While acting out the imagery, did you raise or tighten your shoulders, stiffen your trunk, clench your teeth, hold your breath or stare at the thread and needle without blinking?
Most people are surprised that they have tightened their shoulders and braced their trunk while threading the needle. Awareness only occurred after their attention was directed to the covert muscle bracing patterns.
In many cases muscles are tense even though the person senses and feels that they are relaxed. This lack of awareness can be resolved with muscle biofeedback–it makes invisible visible. Muscle biofeedback (electromyographic feedback) is used to monitor the muscle activity, teach the person awareness of the previously unperceived muscle tension and learn relax and control it. For more information of the use of muscle biofeedback to improve health and performance at work or in the gym, see the published chapter, I thought I was relaxed: The use of SEMG biofeedback for training awareness and control, by Richard Harvey and Erik Peper. It was published in W. A. Edmonds, & G. Tenenbaum (Eds.). (2012), Case studies in applied psychophysiology: Neurofeedback and biofeedback treatments for advances in human performance. West Sussex, UK: Wiley-Blackwell, 144-159.
