Hope for menstrual cramps (dysmenorrhea) with breathing
Posted: April 22, 2023 Filed under: behavior, biofeedback, Breathing/respiration, healing, health, meditation, Pain/discomfort, posture, relaxation, self-healing, stress management, Uncategorized | Tags: dysmenorrhea, Imagery, menstrual cramps, stroking, visualization 7 CommentsAdapted from: Peper, E., Chen, S., Heinz, N., & Harvey, R. (2023). Hope for menstrual cramps (dysmenorrhea) with breathing. Biofeedback, 51(2), 44–51. https://doi.org/10.5298/1081-5937-51.2.04; Republished in Townsend E-Letter – 18 November, 2023 https://www.townsendletter.com/e-letter-22-breath-affects-stress-and-menstrual-cramps/

“I have always had extremely painful periods. They would get so painful that I would have to call in sick and take some time off from school. I have been to many doctors and medical professionals, and they told me there is nothing I could do. I am currently on birth control, and I still get some relief from the menstrual pain, but it would mess up my moods. I tried to do the diaphragmatic breathing so that I would be able to continue my life as a normal woman. And to my surprise it worked. I was simply blown away with how well it works. I have almost no menstrual pain, and I wouldn’t bloat so much after the diaphragmatic breathing.” -22 year old student
Each semester numerous students report that their cramps and dysmenorrhea symptoms decrease or disappear during the semester when they implement the relaxation and breathing practices that are taught in the semester long Holistic Health class. Given that so many young women suffer from dysmenorrhea, many young women could benefit by using this integrated approach as the first self-care intervention before relying on pain reducing medications or hormones to reduce pain or inhibit menstruation. Another 28-year-old student reported:
“Historically, my menstrual cramps have always required ibuprofen to avoid becoming distracting. After this class, I started using diaphragmatic breath after pain started for some relief. True benefit came when I started breathing at the first sign of discomfort. I have not had to use any pain medication since incorporating diaphragmatic breath work.”
This report describes students practicing self-regulation and effortless breathing to reduce stress symptoms, explores possible mechanisms of action, and suggests a protocol for reducing symptoms of menstrual cramps. Watch the short video how diaphragmatic breathing eliminated recurrent severe dysmenorrhea (pain and discomfort associated with menstruation).
Background: What is dysmenorrhea?
Dysmenorrhea is one of the most common conditions experienced by women during menstruation and affects more than half of all women who menstruate (Armour et al., 2019). Most commonly dysmenorrhea is defined by painful cramps in the lower abdomen often accompanied by pelvic pain that starts either a couple days before or at the start of menses. Symptoms also increase with stress (Wang et al., 2003) with pain symptoms usually decreasing in severity as women get older and, after pregnancy.
Economic cost of dysmenorrhea
Dysmenorrhea can significantly interfere with a women’s ability to be productive in their occupation and/or their education. It is “one of the leading causes of absenteeism from school or work, translating to a loss of 600 million hours per year, with an annual loss of $2 billion in the United States” (Itani et al, 2022). For students, dysmenorrhea has a substantial detrimental influence on academic achievement in high school and college (Thakur & Pathania, 2022). Despite the frequent occurrence and negative impact in women’s lives, many young women struggle without seeking or having access to medical advice or, without exploring non-pharmacological self-care approaches (Itani et al, 2022).
Treatment
The most common pharmacological treatments for dysmenorrhea are nonsteroidal anti-inflammatory drugs (NSAIDs) (e.g., Ibuprofen, Aspirin, and Naproxen Sodium) along with hormonal contraceptives. NSAIDs act by preventing the action of cyclooxygenase which prevents the production of prostaglandins. Itani et al (2022) suggested that prostaglandin production mechanisms may be responsible for the disorder. Hormonal contraceptives also prevent the production of prostaglandins by suppressing ovulation and endometrial proliferation.
The pharmacological approach is predominantly based upon the model that increased discomfort appears to be due to an increase in intrauterine secretion of prostaglandins F2α and E2 that may be responsible for the pain that defines this condition (Itani et al, 2022). Pharmaceuticals which influence the presence of prostaglandins do not cure the cause but mainly treat the symptoms.
Treatment with medications has drawbacks. For example, NSAIDs are associated with adverse gastrointestinal and neurological effects and also are not effective in preventing pain in everyone (Vonkeman & van de Laar, 2010). Hormonal contraceptives also have the possibility of adverse side effects (ASPH, 2023). Acetaminophen is another commonly used treatment; however, it is less effective than other NSAID treatments.
Self-regulation strategies to reduce stress and influence dysmenorrhea
Common non-pharmacological treatments include topical heat application and exercise. Both non-medication approaches can be effective in reducing the severity of pain. According to Itani et al. (2022), the success of integrative holistic health treatments can be attributed to “several mechanisms, including increasing pelvic blood supply, inhibiting uterine contractions, stimulating the release of endorphins and serotonin, and altering the ability to receive and perceive pain signals.”
Although less commonly used, self-regulation strategies can significantly reduce stress levels associated menstrual discomfort as well as reduce symptoms. More importantly, they do not have adverse side effects, but the effectiveness of the intervention varies depending on the individual.
- Autogenic Training (AT), is a hundred year old treatment approach developed by the German psychiatrist Johannes Heinrich Schultz that involves three 15 minute daily practice of sessions, resulted in a 40 to 70 percent decrease of symptoms in patient suffering from primary and secondary dysmenorrhea (Luthe & Schultz, 1969). In a well- controlled PhD dissertation, Heczey (1978) compared autogenic training taught individually, autogenic training taught in a group, autogenic training plus vaginal temperature training and a no treatment control in a randomized controlled study. All treatment groups except the control group reported a decrease in symptoms and the most success was with the combined autogenic training and vaginal temperature training in which the subjects’ vaginal temperature increased by .27 F degrees.
- Progressive muscle relaxation developed by Edmund Jacobson in the 1920s and imagery are effective treatments for dysmenorrhea (Aldinda et al., 2022; Chesney & Tasto, 1975; Çelik, 2021; Jacobson, 1938; Proctor et al., 2007).
- Rhythmic abdominal massage as compared to non-treatment reduces dysmenorrhea symptoms (Suryantini, 2022; Vagedes et al., 2019):
- Biofeedback strategies such as frontalis electromyography feedback (EMG) and peripheral temperature training (Hart, Mathisen, & Prater, 1981); trapezius EMG training (Balick et al, 1982); lower abdominal EMG feedback training and relaxation (Bennink, Hulst, & Benthem, 1982); and integrated temperature feedback and autogenic training (Dietvorts & Osborne, 1978) all successfully reduced the symptoms of dysmenorrhea.
- Breathing relaxation for 5 to 30 minutes resulted in a decrease in pain or the pain totally disappeared in adolescents (Hidayatunnafiah et al., 2022). While slow deep breathing in combination with abdominal massage is more effective than applying hot compresses (Ariani et al., 2020). Slow pranayama (Nadi Shodhan) breathing the quality of life and pain scores improved as compared to fast pranayama (Kapalbhati) breathing and improved quality of life and reduces absenteeism and stress levels (Ganesh et al. 2015). When students are taught slow diaphragmatic breathing, many report a reduction in symptoms compared to the controls (Bier et al., 2005).
Observations from Integrated stress management program
This study reports on changes in dysmenorrhea symptoms by students enrolled in a University Holistic Health class that included homework assignment for practicing stress awareness, dynamic relaxation, and breathing with imagery.
Respondents: 32 college women, average age 24.0 years (S.D. 4.5 years)
Procedure: Students were enrolled in a three-unit class in which they were assigned daily home practices which changed each week as described in the book, Make Health Happen (Peper, Gibney & Holt, 2002). The first five weeks consisted of the following sequence: Week 1 focused on monitoring one’s reactions to stressor; week 2 consisted of daily practice for 30 minutes of a modified progressive relaxation and becoming aware of bracing and reducing the bracing during the day; Week 3 consisted of practicing slow diaphragmatic breathing for 30 minutes a day and during the day becoming aware of either breath holding or shallow chest breath and then use that awareness as cue to shift to lower slower diaphragmatic breathing; week 4 focused on evoking a memory of wholeness and relaxing; and week 5 focused on learning peripheral hand warming.
During the class, students observed lectures about stress and holistic health and met in small groups to discuss their self-regulation experiences. During the class discussion, some women discussed postures and practices that were beneficial when experiencing menstrual discomfort, such as breathing slowly while lying on their back, focusing on slow abdominal awareness in which their abdomen expanded during inhalation and contracted during exhalation. While exhaling they focused on imagining a flow of air initially going through their arms and then through their abdomen, down their legs and out their feet. This kinesthetic feeling was enhanced by first massaging down the arm while exhaling and then massaging down their abdomen and down their thighs when exhaling. In most cases, the women also experienced that their hands and feet warmed. In addition, they were asked to shift to slower diaphragmatic breathing whenever they observed themselves gasping, shallow breathing or holding their breath. After five weeks, the students filled out a short assessment questionnaire in which they rated the change in dysmenorrhea symptoms since the beginning of the class.
Results.
About two-thirds of all respondents reported a decrease in overall discomfort symptoms. In addition to any ‘treatment as usual’ (TAU) strategies already being used (e.g. medications or other treatments such as NSAIDs or birth control pills), 91% (20 out 22 women) who reported experiencing dysmenorrhea reported a decrease in symptoms when they practiced the self-regulation and diaphragmatic breathing techniques as shown in Figure 1.

Figure 1. Self-report in dysmenorrhea symptoms after 5 weeks.
Discussion
Many students reported that their symptoms were significantly reduced and they could be more productive. Generally, the more they practiced the relaxation and breathing self-regulation skills, the more they experienced a decrease in symptoms. The limitation of this report is that it is an observational study; however, the findings are similar to those reported by earlier self-care and biofeedback approaches. This suggests that women should be taught the following simple self-regulation strategies as the first intervention to prevent and when they experience dysmenorrhea symptoms.
Why would breathing reduce dysmenorrhea?
Many women respond by ‘curling up’ a natural protective defense response when they experience symptoms. This protective posture increases abdominal and pelvic muscle tension, inhibits lymph and blood flow circulation, increases shallow breathing rate, and decreases heart rate variability. Intentionally relaxing the abdomen with slow lower breathing when lying down with the legs extended is often the first step in reducing discomfort.
By focusing on diaphragmatic breathing with relaxing imagery, it is possible to restore abdominal expansion during inhalation and slight constriction during exhalation. This dynamic breathing while lying supine would enhance abdominal blood and lymph circulation as well as muscle relaxation (Peper et al., 2016). While practicing, participants were asked to wear looser clothing that did not constrict the waist to allow their abdomen to expand during inhalation; since, waist constriction by clothing (designer jean syndrome) interferes with abdominal expansion. Allowing the abdomen to fully extend also increased acceptance of self, that it was okay to let the abdomen expand instead of holding it in protectively. The symptoms were reduced most likley by a combination of the following factors.
- Abdominal movement is facilitated during the breathing cycle. This means reducing the factors that prevent the abdomen expanding during inhalation or constricting during exhalation (Peper et al., 2016).
- Eliminate‘Designer jean syndrome’ (the modern girdle). Increase the expansion of your abdomen by loosening the waist belt, tight pants or slimming underwear (MacHose & Peper, 1991).
- Accept yourself as you are. Allow your stomach to expand without pulling it in.
- Free up learned disuse: Allow the abdomen to expand and constrict instead of inhibiting movement to avoid pain that occurred following a prior abdominal injury/surgery (e.g., hernia surgery, appendectomy, or cesarean operation), abdominal pain (e.g., irritable bowel syndrome, recurrent abdominal pain, ulcers, or acid reflux), pelvic floor pain (e.g., pelvic floor pain, pelvic girdle pain, vulvodynia, or sexual abuse).
- The ‘defense response’ is reduced. Many students described that they often would curl up in a protective defense posture when experiencing menstrual cramps. This protective defense posture would maintain pelvic floor muscle contractions and inhibit blood and lymph flow in the abdomen, increase shallow rapid thoracic breathing and decrease pCO2 which would increase vasoconstriction and muscle constriction (Peper et al., 2015; Peper et al., 2016). By having the participant lie relaxed in a supine position with their legs extended while practicing slow abdominal breathing, the pelvic floor and abdominal wall muscles can relax and thereby increase abdominal blood and lymph circulation and parasympathetic activity. The posture of lying down implies feeling safe which is a state that facilitates healing.
- The pain/fear cycle is interrupted. The dysmenorrhea symptoms may trigger more symptoms because the person anticipates and reacts to the discomfort. The breathing and especially the kinesthetic imagery where the attention goes from the abdomen and area of discomfort to down the legs and out the feet acts as a distraction technique (not focusing on the discomfort).
- Support sympathetic-parasympathetic balance. The slow breathing and kinesthetic imagery usually increases heart rate variability and hand and feet temperature and supports sympathetic parasympathetic balance.
- Interrupt the classical conditioned response of the defense reaction. For some young girls, the first menstruation occurred unexpectedly. All of a sudden, they bled from down below without any understanding of what is going on which could be traumatic. For some this could be a defense reaction and a single trial condition response (somatic cues of the beginning of menstruation triggers the defense reaction). Thus, when the girl later experiences the initial sensations of menstruation, the automatic conditioned response causes her to tense and curl up which would amplify the discomfort. Informal interviews with women suggests that those who experienced their first menstruation experience as shameful, unexpected, or traumatic (“I thought I was dying”) thereafter framed their menstruation negatively. They also tended to report significantly more symptoms than those women who reported experiencing their first menstruation positively as a conformation that they have now entered womanhood.
How to integrate self-care to reduce dysmenorrhea
Be sure to consult your healthcare provider to rule out treatable underlying conditions before implementing learning effortless diaphragmatic breathing.
- Allow the abdomen to expand during inhalation and become smaller during exhalation. This often means, loosen belt and waist constriction, acceptance of allowing the stomach to be larger and reversing learned disuse and protective response caused by stress.
- Master diaphragmatic breathing (see: Peper & Tibbetts, 1994 and the blogs listed at the end of the article).
- Practice slow effortless diaphragmatic breathing lying down with warm water bottle on stomach in a place that feels safe.
- Include kinesthetic imagery as you breathe at about 6 breaths per minute (e.g. slowly inhale for 4 or 5 seconds and then exhale for 5 or 6 seconds, exhaling slightly longer than inhaling). Imaging that when you exhale you can sense healing energy flow through your abdomen, down the legs and out the feet.
- If possible, integrate actual touch with the exhalation can provide added benefit. Have a partner first stroke or massage down the arms from the shoulder to your fingertips as you exhale and, then on during next exhalation stroke gently from your abdomen down your legs and feet. Stroke in rhythm the exhalation.
- Exhale slowly and shift to slow and soft diaphragmatic breathing each time you become aware of neck and shoulder tension, breath holding, shallow breathing, or anticipating stressful situations. At the same time imagine /sense when exhaling a streaming going through the abdomen and out the feet when exhaling. Do this many times during the day.
- Practice and apply general stress reduction skills into daily life since stress can increase symptoms. Anticipate when stressful event could occur and implement stress reducing strategies.
- Be respectful of the biological changes that are part of the menstrual cycle. In some cases adjust your pace and slow down a bit during the week of the menstrual cycle; since, the body needs time to rest and regenerate. Be sure to get adequate amount of rest, hydration, and nutrition to optimize health.
- Use self-healing imagery and language to transform negative association with menstruation to positive associations (e.g., “curse” to confirmation “I am healthy”).
Conclusion
There are many ways to alleviate dysmenorrhea. Women can find ways to anticipate and empower themselves by practicing stress reduction, wearing more comfortable clothing, using heat compression, practicing daily diaphragmatic breathing techniques, visualizing relaxed muscles, and positive perception towards menstrual cycles to reduce the symptoms of dysmenorrhea. These self-regulation methods should be taught as a first level intervention to all young women starting in middle and junior high school so that they are better prepared for the changes that occur as they age.
“I have been practicing the breathing techniques for two weeks prior and I also noticed my muscles, in general, are more relaxed. Of course, I also avoided the skinny jeans that I like to wear and it definitely helped.
I have experienced a 90% improvement from my normal discomfort. I was still tired – and needed more rest and sleep but haven’t experienced any “terrible” physical discomfort. Still occasionally had some sharp pains or bloating but minor discomfort, unlike some days when I am bedridden and unable to move for half a day. – and this was a very positive experience for me “ — Singing Chen (Chen, 2023).
Listen to the expanded podcast created from this blogpost by Google Notebook LM.
Useful blogs to learn diaphragmatic breathing
References
Aldinda, T. W., Sumarni, S., Mulyantoro, D. K., & Azam, M. (2022). Progressive muscle relaxation application (PURE App) for dysmenorrhea. Medisains Jurnal IlmiahLlmiah LLmu-LLmu Keshatan, 20(2), 52-57. https://doi.org/10.30595/medisains.v20i2.14351
Ariani, D., Hartiningsih, S.S., Sabarudin, U. Dane, S. (2020). The effectiveness of combination effleurage massage and slow deep breathing technique to decrease menstrual pain in university students. Journal of Research in Medical and Dental Science, 8(3), 79-84. https://www.jrmds.in/articles/the-effectiveness-of-combination-effleurage-massage-and-slow-deep-breathing-technique-to-decrease-menstrual-pain-in-university-stu-53607.html
Armour, M., Parry, K., Manohar, N., Holmes, K., Ferfolja, T., Curry, C., MacMillan, F., & Smith, C. A. (2019). The prevalence and academic impact of dysmenorrhea in 21,573 young women: a systematic review and meta-analysis. Journal of women’s health, 28(8), 1161-1171.https://doi.org/10.1089/jwh.2018.7615
ASPH. (2023). Estrogen and Progestin (Oral Contraceptives). MedlinePlus. Assessed March 3, 2023. https://medlineplus.gov/druginfo/meds/a601050.html
Balick, L., Elfner, L., May. J., Moore, J.D. (1982). Biofeedback treatment of dysmenorrhea. Biofeedback Self Regul, 7(4), 499-520. https://doi.org/10.1007/BF00998890
Bennink, C.D., Hulst, L.L. & Benthem, J.A. (1982). The effects of EMG biofeedback and relaxation training on primary dysmenorrhea. J Behav Med, 5(3), 329-341.https://doi.org/10.1007/BF00846160
Bier, M., Kazarian, D. & Peper, E. (2005). Reducing PMS through biofeedback and breathing. Poster presentation at the 36th Annual Meeting of the Association for Applied Psychophysiology and Biofeedback. Abstract published in: Applied Psychophysiology and Biofeedback. 30 (4), 411-412.
Çelik, A.S. & Apay, S.E. (2021). Effect of progressive relaxation exercises on primary dysmenorrhea in Turkish students: A randomized prospective controlled trial. Complement Ther Clin Pract, Feb 42,101280. https://doi.org/10.1016/j.ctcp.2020.101280
Chen, S. (2023). Diaphragmatic breathing reduces dysmenorrhea symptoms-a testimonial. YouTube. Accessed March 3, 2023. https://youtu.be/E45iGymVe3U
De Sanctis, V., Soliman, A., Bernasconi, S., Bianchin, L., Bona, G., Bozzola, M., Buzi, F., De Sanctis, C., Tonini, G., Rigon, F., & Perissinotto, E. (2015). Primary Dysmenorrhea in Adolescents: Prevalence, Impact and Recent Knowledge. Pediatr Endocrinol Rev. 13(2), 512-20. PMID: 26841639. https://pubmed.ncbi.nlm.nih.gov/26841639/
De Sanctis, V., Soliman, A. T., Daar, S., Di Maio, S., Elalaily, R., Fiscina, B., & Kattamis, C. (2020). Prevalence, attitude and practice of self-medication among adolescents and the paradigm of dysmenorrhea self-care management in different countries. Acta Bio Medica: Atenei Parmensis, 91(1), 182. https://doi.org/10.23750/abm.v91i1.9242
Dietvorst, T.F. & Osborne, D. (1978). Biofeedback-Assisted Relaxation Training
for Primary Dysmenorrhea: A Case Study. Biofeedback and Self-Regulation, 3(3), 301-305. https://doi.org/10.1007/BF00999298
Chesney, M. A., & Tasto, D. L. (1975).The effectiveness of behavior modification with spasmodic and congestive dysmenorrhea. Behaviour Research and Therapy, 13, 245-253. https://doi.org/10.1016/0005-7967(75)90029-7
Ganesh, B.R., Donde, M.P., & Hegde, A.R. (2015). Comparative study on effect of slow and fast phased pranayama on quality of life and pain in physiotherapy girls with primary dysmenorrhea: Randomize clinical trial. International Journal of Physiotherapy and Research, 3(2), 960-965. https://doi.org/10.16965/ijpr.2015.115
Hart, A.D., Mathisen, K.S. & Prater, J.S. A comparison of skin temperature and EMG training for primary dysmenorrhea. Biofeedback and Self-Regulation 6, 367–373 (1981). https://doi.org/10.1007/BF01000661
Heczey, M. D. (1978). Effects of biofeedback and autogenic training on menstrual experiences: relationship among anxiety, locus of control and dysmenorrhea. City University of New York ProQuest Dissertations Publishing, 7805763. https://www.proquest.com/openview/088e0d68511b5b59de1fa92dec832cc8/1?pq-origsite=gscholar&cbl=18750&diss=y
Hidayatunnafiah, F., Mualifah, L., Moebari, M., & Iswantiningsih, E. (2022). The Effect of Relaxation Techniques in Reducing Dysmenorrhea in Adolescents. The International Virtual Conference on Nursing. in The International Virtual Conference on Nursing, KnE Life Sciences, 473–480. https://doi.org/10.18502/kls.v7i2.10344
Itani, R., Soubra, L., Karout, S., Rahme, D., Karout, L., & Khojah, H.M.J. (2022). Primary Dysmenorrhea: Pathophysiology, Diagnosis, and Treatment Updates. Korean J Fam Med, 43(2), 101-108. https://doi.org/10.4082/kjfm.21.0103
Jacobson, E. (1938). Progressive Relaxation: A Physiological and Clinical Investigation of Muscular States and Their Significance in Psychology and Medical Practice. Chicago: University of Chicago Press
Ju, H., Jones, M., & Mishra, G. (2014). The prevalence and risk factors of dysmenorrhea. Epidemiol Rev, 36, 104-13. https://doi.org/10.1093/epirev/mxt009
Karout, S., Soubra, L., Rahme, D. et al. Prevalence, risk factors, and management practices of primary dysmenorrhea among young females. BMC Women’s Health 21, 392 (2021). https://doi.org/10.1186/s12905-021-01532-w
Iacovides, S., Avidon,I, & Baker, F.C. (2015).What we know about primary dysmenorrhea today: a critical review, Human Reproduction Update, 21(6), 762–778. https://doi.org/10.1093/humupd/dmv039
Luthe, W. & Schultz, J.H. (1969). Autogenic Therapy, Volume II Medical Applications. New York: Grune & Stratton, pp144-148.
MacHose, M. & Peper, E. (1991). The effect of clothing on inhalation volume. Biofeedback and Self-Regulation, 16(3), 261–265. https://doi.org/10.1007/BF01000020
Peper, E., Booiman, A., Lin, I-M, Harvey, R., & Mitose, J. (2016). Abdominal SEMG Feedback for Diaphragmatic Breathing: A Methodological Note. Biofeedback. 44(1), 42-49. https://doi.org/10.5298/1081-5937-44.1.03
Peper, E., Gibney, H. K. & Holt, C. (2002). Make Health Happen. Dubuque, Iowa: Kendall-Hunt. ISBN: 978-0787293314 https://he.kendallhunt.com/make-health-happen
Peper, E., Gilbert, C.D., Harvey, R. & Lin, I-M. (2015). Did you ask about abdominal surgery or injury? A learned disuse risk factor for breathing dysfunction. Biofeedback. 34(4), 173-179. https://doi.org/10.5298/1081-5937-43.4.06
Peper, E. & Tibbetts, V. (1994). Effortless diaphragmatic breathing. Physical Therapy Products. 6(2), 67-71. Also in: Electromyography: Applications in Physical Therapy. Montreal: Thought Technology Ltd. https://biofeedbackhealth.files.wordpress.com/2011/01/peper-and-tibbets-effortless-diaphragmatic.pdf
Proctor, M. & Farquhar, C. (2006). Diagnosis and management of dysmenorrhoea. BMJ. 13, 332(7550), 1134-8. https://doi.org/10.1136/bmj.332.7550
Proctor, M.L, Murphy, P.A., Pattison, H.M., Suckling, J., & Farquhar, C.M. (2007). Behavioural interventions for primary and secondary dysmenorrhoea. Cochrane Database Syst Rev, (3):CD002248. https://doi.org/10.1002/14651858.CD002248.pub3
Suryantini, N. P. (2022). Effleurage Massage: Alternative Non-Pharmacological Therapy in Decreasing Dysmenorrhea Pain. Women, Midwives and Midwifery, 2(3), 41-50. https://wmmjournal.org/index.php/wmm/article/view/71/45
Thakur, P. & Pathania, A.R. (2022). Relief of dysmenorrhea – A review of different types of pharmacological and non-pharmacological treatments. MaterialsToday: Proceedings.18, Part 5, 1157-1162. https://doi.org/10.1016/j.matpr.2021.08.207
Vagedes, J., Fazeli, A., Boening, A., Helmert, E., Berger, B. & Martin, D. (2019). Efficacy of rhythmical massage in comparison to heart rate variability biofeedback in patients with dysmenorrhea—A randomized, controlled trial. Complementary Therapies in Medicine, 42, 438-444. https://doi.org/10.1016/j.ctim.2018.11.009
Vonkeman, H.E. & van de Laar, M,A. (2010). Nonsteroidal anti-inflammatory drugs: adverse effects and their prevention, Semin Arthritis Rheum, 39(4), 294-312. https://doi.org/10.1016/j.semarthrit.2008.08.001
Wang, L., Wand, X., Wang, W., Chen, C. Ronnennberg, A.G., Guang, W. Huang, A. Fang, Z. Zang, T., Wang, L. & Xu, X. (2003).Stress and dysmenorrhoea: a population based prospective study. Occupation and Environmental Medicine, 61(12). http://dx.doi.org/10.1136/oem.2003.012302
Healing chronic back pain
Posted: July 31, 2022 Filed under: behavior, Breathing/respiration, CBT, cognitive behavior therapy, education, healing, health, meditation, relaxation, self-healing, stress management, surgery | Tags: back pain, Imagery, self-care, visualization 4 CommentsErik Peper, PhD, BCB, Jillian Cosby, and Monica Almendras
Adapted from Peper, E. Cosby, J. & Amendras, M. (2022).Healing chronic back pain. NeuroRegulation, 9(3), 165-172. https://doi.org/10.15540/nr.9.3.164

In at the beginning of 2021, I broke my L3 vertebra during a motor cycle accident and underwent two surgeries in which surgeons replaced my shattered L3 with a metal “cage” (looks like a spring) and fused this cage to the L4 and L2 vertebrae with bars. I also broke both sides of my jaw and fractured my left shoulder. I felt so overwhelmed and totally discouraged by the ongoing pain. A year later, after doing the self-healing project as part of the university class assignment, I feel so much better all the time, stopped taking all prescription pain medications and eliminated the sharp pains in my back. This project has taught me that I have the skill set needed to be whole and healthy. –J.C., 28-year-old college student
Chronic pain is defined as a pain that persist or recurs for more than 3 months (Treede et al., 2019). It is exhausting and often associated with reduced quality of life and increased medical costs (Yong, Mullins, & Bhattacharyya, 2022). Pain and depression co-exacerbate physical and psychological symptoms and can lead to hopelessness (IsHak, 2018; Von Korff & Simon, 1996). To go to bed with pain and anticipate that pain is waiting for you as you wake up is often debilitating. One in five American adults experience chronic pain most frequently in back, hip, knee or foot (Yong, Mullins, & Bhattacharyya, 2022). Patients are often prescribed analgesic medications (“pain killers”) to reduce pain. Although, the analgesic medications can be effective in the short term to reduce pain, the efficacy is marginal for relieving chronic pain (Eriksen et al., 2006; Tan, & Jensen, 2007). Recent research by Parisien and colleagues (2022) reported that anti-inflammatory drugs were associated with increased risk of persistent pain. This suggest that anti-inflammatory treatments might have negative effects on pain duration. In addition, the long-term medication use is a major contributor to opioid epidemic and increased pain sensitivity (NIH– NIDA, 2022; Higgins, Smith, & Matthews, 2019; Koop, 2020). Pain can often be successfully treated with a multidisciplinary approach that incorporates non-pharmacologic approaches. These include exercise, acceptance and commitment therapy, as well as hypnosis (Warraich, 2022). This paper reports how self-healing strategies as taught as part of an undergraduate university class can be an effective approach to reduce the experience of chronic pain and improve health.
Each semester, about 100 to 150 junior and senior college students at San Francisco State University enroll in a holistic health class that focused on ‘whole-person’ Holistic Health curriculum. The class includes an assessment of complementary medicine and holistic health. It is based upon the premise that mind/emotions affect body and body affect mind/emotions that Green, Green & Walters (1970) called the psychophysiological principle.
“Every change in the physiological state is accompanied by an appropriate change in the mental emotional state, conscious or unconscious, and conversely, every change in the mental emotional state, conscious or unconscious, is accompanied by an appropriate change in the physiological state.”
The didactic components of the class includes the psychobiology of stress, the role of posture, psychophysiology of respiration, lifestyle and other health factors, reframing internal language, guided and self-healing imagery. Students in the class are assigned self-healing projects using techniques that focus on awareness of stress, dynamic regeneration, stress reduction imagery for healing, and other behavioral change techniques adapted from the book, Make Health Happen (Peper, Gibney, & Holt, 2002).
The self-practices during the last six weeks of the class focus on identifying, developing and implementing a self-healing project to optimize their personal health. The self-healing project can range from simple life style changes to reducing chronic pain. Each student identifies their project such as increasing physical activity, eating a healthy diet and reducing sugar and junk food, stopping vaping/smoking, reducing anxiety or depression, stopping hair pulling, reducing headaches, decreasing ezema, or back pain, etc. At the end of the semester, 80% or more of the students report significant reduction in symptoms (Peper, Sato-Perry, & Gibney, 2003; Peper, Lin, Harvey, Gilbert, Gubbala, Ratkovich, & Fletcher, 2014; Peper, Miceli, & Harvey, 2016; Peper, Harvey, Cuellar, & Membrila, 2022). During the last five semesters, 13 percent of the students focused reducing pain (e.g., migraines, neck and shoulder pain, upper or lower back pain, knee pain, wrist pain, and abdominal pain). The students successfully improved their symptoms an average of 8.8 on a scale from 0 (No benefit) to 10 (total benefit/improvement). The success for improving their symptoms correlates 0.63 with their commitment and persistence to the project (Peper, Amendras, Heinz, & Harvey, in prep).
The purposes of this paper is to describe a case example how a student with severe back pain reduced her symptoms and eliminated medication by implementing an integrated self-healing process as part of a class assignment and offer recommendations how this could be useful for others.
Participant: A 28-year-old female student (J.C.) who on January 28, 2021 broke her L3 vertebra in a motor cycle accident. She underwent two surgeries in which surgeons replaced her shattered L3 with a metal “cage” (which she describes as looking like a spring) and fused this cage to the L2 and L4 vertebrae with bars. She also broke both sides of her jaw and fractured her left shoulder. More than a year later, at the beginning of the self-healing project, she continue to take 5-10 mgs of Baclofen and 300 mgs of Gabapentin three times a day to reduce pain.
Goal of the self-healing project: To decrease the sharp pain/discomfort in her lower back that resulted from the motor cycle accident and, although not explicitly listed, to decrease the pain medications.
Self-healing process
During the last six weeks of the 2022 Spring semester, the student implemented her self-healing practices for her personal project which consisted of the following steps.
1. Create a self-healing plan that included exploring the advantage and disadvantage of her illness.
2. Develop a step-by-step plan with specific goals to relief her tension and pain in her lower back. This practice allowed her to quantify her problem and the solutions. Like so many people with chronic pain, she focused on the problem and feelings (physical and emotional) associated with the pain. As a result, she often feel hopeless and worried that it would not change.
3. Observe and evaluate when pain sensations changed. She recognized that she automatically anticipated and focused on the pain and anxiety whenever she needed to bend down into a squat. She realized that she had been anticipating pain even before she began to squat. This showed that she needed to focus on healing the movement of this area of her body.
Through her detailed observations, she realized that her previous general rating of back pain could be separated into muscle tightness/stiffness and pain. With this realization, she changed the way she was recording her pain level. She changed it from “pain level” into into two categories: tightness and sharp pains.
4. Ask questions of her unconscious through a guided practice of accessing an inner guide through imagery (For detailed instructions, see Peper, Gibney, & Holt, 2002, pages 197-206). In this self-guided imagery the person relaxes and imagines being in a special healing place where you felt calm, safe and secure. Then as you relaxed, you become aware of another being (wise one or guide) approaching you (the being can be a person, animal, light, spirit, etc.). The being is wise and knows you well. In your mind, you ask this being or guide questions such as, “What do I need to do to assist in my own healing?” Then you wait and listen for an answer. The answer may take many forms such as in words, a pictures, a sense of knowing, or it may come later in dreams or in other forms. When students are assigned this practice for a week, almost all report experiencing some form of guide and many find the answers meaningful for their self-healing project.
Through this imagery of the inner guide script, she connected with her higher self and the wise one told her to “Wait.” This connecting with the wise one was key in accepting that the project was not as daunting as she initially thought. She realized that pain was not going to be forever in her future. She also interpreted that as reminder to have patience with herself. Change takes practice, time and practice such as she previously experienced while correcting her posture to manage her emotions and edit her negative thoughts into positive ones (Peper, Harvey, Cuellar, & Membrila, 2022). Whenever she would have pain or feel discouraged because of external circumstances, she would remind herself of three things:
A. I need to have patience with myself.
B. I have all the healing tools inside me and I am learning to use them.
C. If I do not make time for my wellness, I’ll be forced to make time for my illness.
5. Practice self-healing imagery as described by Peper, Gibney, & Holt (2002) and adapted from the work by Dr. Martin Rossman (Rossman, 2000). Imagery can be the communication channel between the conscious/voluntary and the unconscious/autonomic/involuntary nervous system (Bressler, 2005; Hadjibalassi et al, 2018; Rossman, 2019). It appears to act as the template and post-hypnotic suggestion to implement behavior change and may offer insight and ways to mobilize the self-healing potential (Battino, 2020). Imagery is dynamic and changeable.
The process of self-healing imagery consists of three parts.
- Inspection the problem and drawing a graphic illustration of the problem as it is experienced at that moment of time.
- Drawing of how that area/problem would look when being completely well/whole or disappeared.
- Creation of a self-healing process by which the problem would become transformed into health (Peper, Gibney & Holt, 2002, pp. 217-236). The process focused on what the person could do for themselves; namely, each time they became aware of, anticipated, or felt the problem, they would focus on the self-healing process. It provideshope; since, the person now focuses on the healing of the problem and becoming well.
The drawings of inspection of the pain and problem she experienced at that moment of time are shown in Figure 1.

Figure 1. Illustration of the problem of the pain. Thorns dug deep, muscles tight, and frozen vertebrates grinding.
The resolution of the problem and being well/whole are illustrated in Figure 2.

Figure 2. Resolution of the problem in which her muscles are warm, full of blood, free of thorns, relaxed and flexible and being whole happy and healthy in which her spine is warm, her muscles are warm, her back is flexible and full of movement.
Although she utilized the first image of the muscles warm, full of blood, free of thorns and the muscles relaxed and flexible, her second image of her fully being healed was inspired through a religious statue of Yemaya that she had in her room (Yemaya is a major water spirit from the Yoruba religion Santeria and Orisha of the seas and protector of women). Each time she saw the statue, she thought of the image of herself fully healed and embodying the spirit Orisha. Therefore, this image remained important to her all the time.
Her healing imagery process by which she transforms the image of inspecting of the problem to being totally well are illustrated in Figure 3.

Figure 3. The healing process: The sun’s warm fingers thaw my muscles, lubricate my vertebra, thorns fall out, and blood returns.
For five weeks as she implemented her self-healing project by creating a self-healing plan, asking questions of her unconscious, drawing her self-healing imagery. She also incorporated previously learned skills from the first part of the semester such diaphragmatic breathing, hand warming, shifting slouching to upright posture, and changing language. Initially she paired hand warming with the self-healing imagery and she could feel an increase in body warmth each time she practiced the imagery. She practiced the self-healing imagery as an in-depth daily practice and throughout the day when she became aware of her back as described in one of her log entries.
I repeated the same steps as the day prior today. I did my practice in the early morning but focused on the details of the slowed down movements of the sun’s hands. I saw them as they stretched out to my back, passed through my skin, wrapped around my muscles, and began to warm them. I focused on this image and tried to see, in realistic detail, my muscles with a little ice still on them, feeling hard through and through, the sun’s glowing yellow-orange fingers wrapped around my muscles. I imaged the thorns still in my muscles, though far fewer than when I started, and then I imaged the yellow-orange glow start to seep out from the sun’s palms and fingers and spread over my muscles. I imaged the tendons developing as the muscle tissue thawed and relaxed, the red of the muscle brightened, the ice on and within my muscles started to melt, and the condensation formed as it ran down into collected droplets at the bottom of my muscles. I imaged the thorns lose their grip and fall out, one at a time, in tandem with the droplets falling. I continued this process and imaged my muscles expanding with warmth and relaxation as they stayed engulfed in the warmth of the sun.
At the end of my practice, I did a small stretch session. I felt extremely refreshed and ready for yet another extremely busy day between internship, graduation, and school. I would say I felt warm and relaxed all the way into the afternoon, about 6 hours after my practice. This was by far the most detailed and impactful imagery practice I have had.
The self-healing imagery practice provided me with the ability to conceptualize more than my problem as it showed me the tools to (and the importance of) conceptualizing my solution, both the tool and end result.
Results
Pain and tightness decreased and she stopped her medication by the third week as shown in Figure 4.

Figure 4. Self-rating of sharp pains and tightness during the self-healing project.
At the 14-week follow-up, she has continued to improve, experiences minimal discomfort, and no longer takes medication. As she stated, I was so incredibly shocked how early on [in the project] I was able to stop taking pain medications that I had already taken every day for over a year.
Discussion
This individual case example provides hope that health can be improved when shifting the focus from pain and discomfort to focusing on actively participating in the self-healing process. As she wrote, The lesson was self- empowerment in regard to my health. I brought comfort to my back. There is metal in my back for the rest of my life and this is something I have accepted. I used to look at that as a horrible thing to have to handle forever. I now look at it as a beautiful contraption that has allowed me to walk across a graduation stage despite having literally shattered a vertebra. I am reintegrating these traumatized parts of my body back into a whole health state of mind and body. Doctors did not do this, surgeries did not, PT didn’t and neither did pain medications. MY body and MY mind did it. I did this.
Besides the self-healing imagery and acting upon the information she received from the asking questions from the unconscious there were many other factors contributed to her healing. These included the semester long self-practices and mastery of different stress management techniques, learning how stress impacts health and what can the person can do to self-regulate, as well as being introduced to the many case examples and research studies that suggested healing could be possible even in cases where it seemed impossible.
The other foundational components that was part of the class teachings included attending the weekly classes session and completing the assign homework practices. These covered discussion about placebo/nocebo, possibilities and examples of self-healing with visualization, the role of nutrition, psychophysiology of stress and factors are associated with healthy aging across cultures. The asynchronous assignments investigated factors that promoted or inhibited health and the role of hope. The discussions pointed out that not everyone may return to health; however, they can always be whole. For example, if a person loses a limb, the limb will not regrow. The healing process includes acceptance and creating new goals to achieve and live a meaningful life.
The possibility that students could benefit by implementing the different skills and concepts taught in the class were illustrated by sharing previous students’ successes in reversing disorders such as hair pulling, anxiety, psoriasis, and pain. In addition, students were assigned to watch and comment on videos of people who had overcome serious illness. These included Janine Shepherd’s 2012 TED talk, A broken body isn’t a broken person, and Dr. Terry Wahl’s 2011 TEDxIowaCity talk, Minding your mitochondria. Janine Shepard shared how she recovered from a very serious accident in which she became paralyzed to becoming an aecrobatic pilot instructor while Dr. Terry Wahl shares how she he used diet to cure her MS and get out of her wheelchair (Shepherd, 2012; Wahl, 2011). Other assignments included watching Madhu Anziani’s presentation, Healing from paralysis-Music (toning) to activate health, in which he discussed his recovery from being a quadriplegic to becoming an inspirational musician (Anziani, & Peper, 2021). The students as read and commented on student case examples of reversing acid reflux, irritable bowel and chronic headaches (Peper, Mason, & Huey, 2017a; Peper, Mason, & Huey, 2017b; Peper, 2018; Peper et al., 2020; Peper, Covell, & Matzembacker, 2021; Peper, 2022).
Although self-healing imagery appears to be the major component that facilitated the healing, it cannot be separated from the many other concepts and practices that may have contributed. For example, the previous practices of learning slow diaphragmatic breathing and hand warming may have allowed the imagery to become a real kinesthetic experience. In addition, by seeing how other students overcame chronic disorders, the class provided a framework to mobilize one’s health.
Lessons extracted from this case example that others may be able use to mobilize health.
- Take action to shifts from being hopeless and powerless to becoming empowered and active agent in the healing process.
- Change personal beliefs through experiential practices and storytelling that provides a framework that healing and improvement are possible.
- Teach the person self-regulation skills such as slower breathing, muscle relaxation, cognitive internal language changes, hand warming by which the person experiences changes.
- Provide believable role models who shared their struggle in overcoming traumatic injury, watch inspirational talks, and share previous clients or students’ self-reports who had previously improved.
- Transform the problem from global description into behavioral specific parts. For example, being depressed is a global statement and too big to work on. Breaking the global concept into specific behaviors such as, my energy is too low to do exercise or I have negative thoughts, would provide specific interventions to work on such as, increasing exercise or changing thoughts. In JC’s case, she changed the general rating of pain into ratings of muscle tightness and sharp pains. This provided the bases for strategies to relax and warm her muscles.
- Focus on what you can do at that moment versus focusing on the past, what happened, who caused it, or blaming yourself and others. Explore and ask what you now can do now to support your healing process and reframe the problem as a new opportunity for growth and development.
- Practice, practice, and practice with a childlike exploratory attitude. Focus on the small positive benefits that occur as a result of the practices. It is not mindless practice; it is practice while being present and being gentle with yourself. Do not discard very small changes. The benefits accrue as you practice more and more, just many people have experienced when learning to play a musical instrument or mastering a sport. Even though many participants think that practicing 15 minutes a day is enough, it usually takes much more time. Reflect on how a baby learns to walk or climb. The toddler practices day-long and takes naps to regenerate and grow. When the toddler is not yet successful in walking or climbing, it does not give up or interpret it as failure or blaming himself that he cannot do it, it just means more practice.
- Have external reminders to evoke the self-healing practices. In JC’s case, the small statue of Yemaya in her room was the reminder. It reminded her to thinks of the image of herself fully healed each time she saw it.
- Guide yourself through the wise one imagery, ask yourself a question and listen and act on the intuitional answers.
- Develop a self-healing imagery process that transforms the dysfunction to health or wholeness. Often the person only perceives the limitations and focusses on describing the problem. Instead, acknowledge, accept what was and is, and focus on developing a process to promote healing. What many people do not realize that if they think/imagine how their injury/illness was caused, it may reactivate and recreate the initial trauma. This can be illustrated through imagery. When we think or imagine something, it changes our physiology. For example, when one imagines eating a lemon, many people will salivate. The image affects physiology. Thus, focus on processes that support healing.
- While practicing the imagery, experience it as if it is real and feel it happening inside yourself. Many people initially find this challenging as they see it outside themselves. One way to increase the “felt sense” is to incorporate more body involvement such as acting out the imagery with hand and body movements.
- When having a relapse, remind yourself to keep going. Every morning is the beginning of a new day, do each practices anew. In addition, reflect of something that was challenging in the past but that you successfully overcame. Focus on that success. As JC wrote, I was also successful in that I gave myself slack and reminded myself that relapses will happen and what matters more is the steps I take to move forward.
- Make your healing a priority that means doing it often during the day. Allow the self-healing imagery and process to run in the back of the head all the time just as a worry can be present in the background. So often people practice for a few minutes (which is great and better than not practicing at all); however, at other times during the day they are captured by their worry, negative thoughts or focus on the limitations of the disorder. When a person focuses on the limitations, it may interrupt the self-healing process. The analogy we often use is that the healing process is similar to healing from a small cut in the skin. Initially a scab forms and eventually the scab falls off and the skin is healed. On the other hand, if you keep moving the skin or pick on the scab, healing is much slower. By focusing on the limitations and past visualization of the injury, self-healing is reduced. This is similar to removing the scab before the skin has healed. As JC stated, “If you don’t make time for your wellness, you’ll be forced to make time for your illness” was 100% a motivating factor in my success.
- Explore resources for providers and people living with pain. See Dr. Rachel Zoffness website which provides a trove of high quality articles, books, videos, apps, and podcasts. https://www.zoffness.com/resources
In summary, we do not know the limits of self-healing; however, this case example illustrates that by implementing self-healing strategies health and recovery occurred. As JC wrote:
To have broken a vertebra in my back and experience all the injuries that came with the accident when I already did not have the strongest mind-body connection was incredibly intense and really heartbreaking and discouraging in my life. And, that made things difficult because I was not able to 100% focus on my healing because I felt so overwhelmed by the feeling of discouragement that I felt. Experiencing this self-healing project, seeing the imagery that helped me not just feel so much better all the time but be able to stop taking all prescription pain medications and eliminate the sharp pains in my back has taught me that I have the skill set needed to be whole and healthy.
Watch the interview will Jillian Cosby inwhich she describes her self-healing process.
References
Anziani, M. & Peper, E. (2021). Healing from paralysis-Music (toning) to activate health. The peperperspective. https://peperperspective.com/2021/11/22/healing-from-paralysis-music-toning-to-activate-health/
Battino, R. (2020). Using Guided Imagery and Hypnosis in Brief Therapy and Palliative Care. New York: Routledge.
Bresler, D. (2005).Physiological Consequences of Guided Imagery. Pract Pain Manag, 5(6). https://www.practicalpainmanagement.com/treatments/complementary/biobehavioral/physiological-consequences-guided-imagery
Eriksen, J., Sjøgren, P., Bruera, E., et al. (2006). Critical issues on opioids in chronic non-cancer pain: An epidemiologic study. Pain, 125,172–179. https://doi.org/10.1016/j.pain.2006.06.009
Green, E. E., Green, A. M., & Walters, E. D. (1970). Voluntary control of internal states: Psychological and physiological. The Journal of Transpersonal Psychology, 2(1), 1. https://atpweb.org/jtparchive/trps-02-70-01-001.pdf
Hadjibalassi, M., Lambrinou, E.., Papastavrou,E., & Papathanassoglou, E. (2018). The effect of guided imagery on physiological and psychological outcomes of adult ICU patients: A systematic literature review and methodological implications, Australian Critical Care, 31(2), 73-86. https://doi.org/10.1016/j.aucc.2017.03.001
Higgins, C, Smith, B.H., & Matthews, K. (2019). Evidence of opioid-induced hyperalgesia in clinical populations after chronic opioid exposure: a systematic review and meta-analysis, British Journal of Anaesthesia, 122(6), e114-e126. https://doi.org/10.1016/j.bja.2018.09.019
IsHak, W.W., Wen, R.Y., Naghdechi, L., Vanle, B., Dang, J., Knosp, M., Dascal, J., Lobsang, Gohar, Y.,; Eskander, L., Yadegar, J., Hanna, S., Sadek, A., Aguilar-Hernandez, L., Danovitch, I., Louy, C. (2018). Pain and Depression: A Systematic Review, Harvard Review of Psychiatry, 11/12, 26(6), 352-363. https://doi.org/10.1097/HRP.0000000000000198
Koob, G.F. (2020). Neurobiology of Opioid Addiction: Opponent Process, Hyperkatifeia, and Negative Reinforcement, Biological Psychiatry, 87(1), 44-53. https://doi.org/10.1016/j.biopsych.2019.05.023
Mullins, P.M., & Bhattacharyya, N. (2022). Prevalence of chronic pain among adults in the United States, Pain, 163(2), e328-e332. https://doi.org/10.1097/j.pain.0000000000002291NIH–
NIDA (2022). Opioid Overdose Crisis. Downloaded June 30, 2022. https://nida.nih.gov/research-topics/opioids/opioid-overdose-crisis
Parisien, M., Lima, L.V., Dagostino, C., El-Hachem, N., Drury, G.L., Grant, A.V., Huising, J., Verma, V…. .(2022). Acute inflammatory response via neutrophil activation protects against the development of chronic pain. Science Translational Medicine, 14(644). https://doi.org/10.1126/scitranslmed.abj99
Peper, E. (2018). Breathing reduces acid reflux and dysmenorrhea discomfort. the peperperspective. https://peperperspective.com/2018/10/04/breathing-reduces-acid-reflux-and-dysmenorrhea-discomfort/
Peper, E. (2022). Resolving a chronic headache with posture feedback and breathing. the peperperspective. https://peperperspective.com/2022/01/04/resolving-a-chronic-headache-with-posture-feedback-and-breathing/
Peper, E., Almedras, M., Heinz, N. & Harvey, R. (in prep). How attending a Holistic Health class reduced symptoms.
Peper, E. Cosby, J. & Amendras, M. Healing chronic back pain. NeuroRegulation, 9I(3), 165-172. https://doi.org/10.15540/nr.9.3.164
Peper, E., Covell, A., & Matzembacker, N. (2021). How a chronic headache condition became resolved with one session of breathing and posture coaching. NeuroRegulation, 8(4), 194–197. https://doi.org/10.15540/nr.8.4.194
Peper, E., Gibney, K.H. & Holt. C. (2002). Make Health Happen: Training Yourself to Create Wellness. Dubuque, IA: Kendall-Hunt.ISBN: 978-0787293314 https://he.kendallhunt.com/make-health-happen
Peper, E., Harvey, R., Cuellar, Y., & Membrila, C. (2022). Reduce anxiety. NeuroRegulation, 9(2), 91–97. https://doi.org/10.15540/nr.9.2.91 https://www.neuroregulation.org/article/view/22815/14575
Peper, E., Lin, I-M., Harvey, r., Gilbert, M. Gubbala, P, Ratkovich, A., & Fletcher, L. (2014). Transforming Chained Behaviors: Case Studies of Overcoming Smoking, Eczema, and Hair Pulling (Trichotillomania), Biofeedback, 42 (4), 154–160. https://doi.org/10.5298/1081-5937-42.4.06
Peper, E., Mason, L, & Huey, C. (2017a). Healing irritable bowel syndrome with diaphragmatic breathing. the peperperspective. https://peperperspective.com/2017/06/23/healing-irritable-bowel-syndrome-with-diaphragmatic-breathing/
Peper, E., Mason, L., Huey, C. (2017b). Healing irritable bowel syndrome with diaphragmatic breathing. Biofeedback. (45-4). https://doi.org/10.5298/1081-5937-45.4.04
Peper, E., Mason, L., Harvey, R., Wolski, L, & Torres, J. (2020). Can acid reflux be reduced by breathing? Townsend Letters-The Examiner of Alternative Medicine, 445/446, 44-47. https://www.townsendletter.com/article/445-6-acid-reflux-reduced-by-breathing/
Peper, E., Miceli, B., & Harvey, R. (2016). Educational Model for Self-healing: Eliminating a Chronic Migraine with Electromyography, Autogenic Training, Posture, and Mindfulness. Biofeedback, 44(3), 130–137. https://doi.org/10.5298/1081-5937-44.3.03
Peper, E., Sato-Perry, K & Gibney, K. H. (2003). Achieving Health: A 14-Session Structured Stress Management Program—Eczema as a Case Illustration. 34rd Annual Meeting of the Association for Applied Psychophysiology and Biofeedback. Abstract in: Applied Psychophysiology and Biofeedback, 28(4), 308. https://biofeedbackhealth.files.wordpress.com/2013/12/2003-aapb-poster-peper-keiko-long1.pdf
Peper, E., Lin, I-M, Harvey, R., Gilbert, M., Gubbala, P., Ratkovich, A., & Fletcher, F. (2014). Transforming chained behaviors: Case studies of overcoming smoking, eczema and hair pulling (trichotillomania). Biofeedback, 42(4), 154-160. https://doi.org/10.5298/1081-5937-42.4.06
Rossman, M. L.(2000). Guided imagery for self-healing. New York: New World Library. https://www.amazon.com/Guided-Imagery-Self-Healing-Martin-Rossman/dp/091581188X/ref=sr_1_3?crid=3M8I1Y1NV3A5N&keywords=martin+rossman&qid=1657649675&s=books&sprefix=rossman%2C+M%2Cstripbooks%2C131&sr=1-3
Rossman, M. L. (2019). Imagine health! Imagery in medical self-care. InSheikh, A.A. (ed). Imagination and healing (pp. 231-258). Routledge. https://www.amazon.com/Imagination-Healing-Imagery-Human-Development-ebook/dp/B07QB4RGSW/ref=sr_1_9?crid=3C7V3E5ZN92R&keywords=Imagination+and+healing&qid=1657818303&s=books&sprefix=imagination+and+healing+%2Cstripbooks%2C105&sr=1-9
Sheng, J., Liu, S., Wang, Y., Cui, R., & Zhang, X. (2017). The link between depression and chronic pain: Neural mechanisms in the brain. Neural Plasticity, 2017, Article 9724371. https://doi.org/10.1155/2017/9724371
Shepherd, Janine. (2012). A broken body isn’t a broken person. TEDxKC. https://www.ted.com/talks/janine_shepherd_a_broken_body_isn_t_a_broken_person
Tan, G., & Jensen, M. P. (2007). Integrating complementary and alternative medicine into multidisciplinary chronic pain treatment. In Chronic Pain Management (pp. 75-99). CRC Press. https://www.taylorfrancis.com/chapters/edit/10.3109/9781420045130-6/integrating-complementary-alternative-medicine-multidisciplinary-chronic-pain-treatment-gabriel-tan-mark-jensen
Treede, R-D., Rief, W., Barke, A., Aziz, Q., Bennett, M.I., Benoliel, R., Cohen, M., Evers, S., Finnerup, N.B., First, M.B., Giamberardino, M.A., Kaasa, S., Korwisi, B., Kosek, E., Lavand’homme, P., ; Nicholas, M., Perrot, S., Scholz, J., Schug, S., Smith, B.H., ; Svensson, P., Vlaeyen, J.S., & Wang, S-J. (2019). Chronic pain as a symptom or a disease: the IASP Classification of Chronic Pain for the International Classification of Diseases (ICD-11), Pain, 160(1), 19-27. https://do.org/10.1097/j.pain.0000000000001384
Von Korff, M. & Simon, G. (1996). The relationship between pain and depression. British Journal of Psychiatry, 168(S30), 101-108. https://doi.org/10.1192/S0007125000298474
Wahl, T. (2011). Minding your mitochondria. TEDzIowaCity. https://www.youtube.com/watch?v=KLjgBLwH3Wc
Warraich, H. (2022). Medicine has failed chronic pain patients. Here’s what they need. Pscyhe, Aeon, https://psyche.co/ideas/medicine-has-failed-chronic-pain-patients-heres-what-they-need
Yong, R. J., Mullins, P. M., & Bhattacharyya, N. (2022). Prevalence of chronic pain among adults in the United States. Pain, 163(2), e328-e332. https://doi.org/10.1097/j.pain.0000000000002291
Relive memory to create healing imagery
Posted: February 15, 2019 Filed under: behavior, health, placebo, relaxation, self-healing, Uncategorized | Tags: conditioning, Imagery, Pavlov, visualization 4 Comments
This blog describes a structured imagery that evokes past memories of joy and health and integrates them into a relaxation practice to support healing. First, a look at the logic for the practice and then the process of creating your own personal imagery script. A sample audio file is included as a model for creating your MP3 file. The blog is adapted from Peper, E., Gibney, K.H. & Holt. C. (2002). Make Health Happen: Training Yourself to Create Wellness. Dubuque, IA: Kendall-Hunt.
“I enjoyed regressing back into my childhood, remembered playing in the rain, making paper sailboats with my brother…. Placing my fingers in a bowl of water and stroking a paper sailboat enabled me to participate in the total experience… I felt tingling sensations all over my body, like tiny bundles of energy exploding inside of me. By the end of the week the simple word “rain” could induce these sensations inside my whole being.”–Student
Daydreaming! We all know how to do it. When we daydream, we feel, sense, hear, and taste our daydream—the image becomes tangible, as if we are living it. A well-developed relaxation image can also include colors, scents, sounds, flavors, temperature, and so forth. Evoking a past memory image of wholeness may contribute significant to healing, as illustrated in Pavlov’s experience with controlled conditioning and with self-healing.
THE POWER OF CONDITIONING
Pavlov’s experience
Most of us are probably familiar with the classical conditioning experiment of the famous Russian physiologist, Ivan Pavlov, who taught dogs to salivate on cue when they heard a bell ring—even when no food was provided. Pavlov accomplished this by giving the dogs food immediately after ringing a bell. Eventually, the dogs became conditioned to expect the food with the bell and simply hearing the bell ring would induce salivation (shown in Figure 1).

Figure 1. The process of classical conditioning. (Figure adapted from: https://opentextbc.ca/introductiontopsychology/chapter/7-1-learning-by-association-classical-conditioning/)
The conditioning effects of imagery can have an effect on health as well as physiology as reflected in an anecdote told by Theodore Melnechuk about Ivan Pavlov. As an old man, he became quite ill with heart disease and his doctors had no hope of curing him. They took his family aside and told them that the end was near. Pavlov himself, however, was not disheartened. He asked the nurse who was caring for him to bring him a bowl of warm water with a little dirt or mud in it. All day, as he lay in bed, he dabbled one hand in the water, with a dreamy, faraway look on his face. His family was quite sure that he had taken leave of his wits and would die soon. However, the next morning he announced that he felt fine, ate a large breakfast, and sat out in the sun awhile. By the end of the day, when the doctor came to check on him, there was no trace of the heart condition. When asked to explain what he had done, he said that he had reasoned that if he could recall a time when he was completely carefree and happy, it might have some healing benefit for him. As a young boy, he used to spend his summers playing with his friends in a shallow swimming hole in a nearby river. The memory of the warm, slightly muddy water was delightful to him. With his knowledge of the power of conditioned stimuli, he reasoned that having a physical reminder of that water might help him evoke that experience and those blissful feelings, and bring some of those memories into the present time. Using this strategy, he harnessed positive memory and the associated emotions that evoked the associated body changes to bring about his healing.
Conditioned Behaviors
We all performs many conditioned behaviors every day. Some of these behaviors can have implications for our health and wellness. There may be aspects of allergic reactions that are conditioned. For example, the literature reports that a woman who was allergic to roses developed a severe allergic reaction to a very realistic-looking paper rose, even though she was not allergic to paper. Her body reacted as if the paper rose was real. (McKenzie, 1886; Vits et al, 2011).
Conditioning can also affect our immune system. When rats were injected with a powerful immune-suppressing drug, while being fed saccharin-flavored water, their immune function showed an immediate drop. After the drug and saccharine water were paired a number of times, the rats were then given just the saccharin water and a harmless injection of salt water. Their immune cells responded exactly as if they had received the drug! The reverse ability, increasing immune cell function, has been shown to be influenced through conditioning (Ader, Cohen & Felten, 1995; Ader and Cohen, 1993).
Belief can also play a role in these scenarios. Bernie Siegel, MD,(2011) has recounted the story of a woman scheduled for chemotherapy who was first given a saline solution, and cautioned that it could cause hair loss. Although this is an unlikely result of a saline injection, given her belief, her hair fell out.
Actions, thoughts, and images affect our physiology.
We often anticipate, react, and form conclusions with incomplete information. Thoughts and images affect our physiology and even our immune system. Re-evoking a positive memory and living in that memory could potentially improve your health. In a remarkable study by a Harvard psychologist, Ellen Langer, eight men in their 70s lived together for one week, recreating aspects of the world that they had experienced more than 20 years earlier. They were instructed to act as they had in 1959, while the control group was instructed to focus entirely on the present time.
In the experimental group, all the physical cues were reminiscent of the culture twenty years earlier. Black and white television and magazines were from 1959. There were no mirrors to remind them of their current age—only photos on the wall of their younger selves. After a week in which the participants acted as if they were younger and the cues around them evoked their younger selves, 63% of the experimental group had improved their cognitive performance as compared with 44% of the control group. Among participants in the experimental group, even their physical health had improved. Independent raters who looked at the before and after pictures of these participants rated their appearance a little younger than the photos taken before the experiment (Langer, 2009; Grierson, 2014; Friedman, 2015). It is possible that by acting and thinking younger, we actually stay younger!
The limits of our belief are the limits of our experience. This concept underlies the remarkable power of placebo. If one believes a drug or a procedure is helpful, that can have a powerful healing effect (Peper & Harvey, 2017; also see the blog, How effective is treatment? The importance of active placebos).
CREATE YOUR OWN VISUALIZATION
Begin by remembering a time when you felt happy, healthy, and whole. Draw inspiration from Pavlov, who evoked happy memories from his childhood, apparently dramatically changing his health. To develop your personal visualization, set aside the time to recreate a healing memory. Remember a time in your life when you felt healthy and joyous (possibly from your childhood). For some, this might be time in nature or with your family or with friends.
Once you remember the event, re-experience it as if you were there right now. Evoke as many senses as possible. Think of the memory and any associations such as an old teddy bear, a shell from the beach, a favorite song, a certain perfume or some other tangible aspect of the experience. The goal is to recreate the experience as if it was current reality. Olfactory and gustatory cues can be especially powerful. If possible include the actual objects and cues associated with that memory—articles, pictures, music, songs, fragrances, or even food.
Sounds, scents, or touching and objects from that era of your life can deepen your ability to recreate and experience the quality of that memory—to actually be in the memory. These sensory reminders will help to evoke the memory and increase the felt experience. You might find it helpful to review Ellen Langer’s experiment, recreating an environment from twenty years earlier. The actual cues will deepen the experience, just as aromas often evoke specific memories and emotions.
The underlying principle is that memories are associated with conditioned stimuli that evoke the physiological state(s) in the body present when the memory was created.
Once you have created a vivid memory that engenders a sense of wholeness, develop a detailed description of your memory to help you evoke that experience. (For some, the memory calls up a timeless setting—relaxing on a warm beach, sitting in front of the fire on a winter evening, or sailing on a calm day. For others, the sense of trust may be associated with a specific person—someone you love—being with your grandmother, helping your mother bake a cake, or going fishing with your dad.). As you recreate the experience, engage all your senses (images, fragrance, tastes, textures, sounds, kinetics). Stay in your image: see it, smell it, taste it, touch it, hear it, be it and allow the experience to deepen.
Begin by writing up your imagery. Then record the introduction the structured relaxation and follow it with a description that evokes the memory as an MP3 audiofile. Use the following three-step process to create the script for your personal relaxation.
- Describe a time in your past when you felt joy, peace, love, or a sense of integration and wholeness.
_________________________________________________________________
_________________________________________________________________
- Identify the specific cues or stimuli associated with that memory.
_________________________________________________________________
_________________________________________________________________
- Write out a detailed description that will evoke your personal memory.
_________________________________________________________________
_________________________________________________________________
_________________________________________________________________
_________________________________________________________________
CREATING YOUR AUDIO FILE
In this approach, there are three components to your script: first, a relaxation practice to ease you into your visualization, then the visualization of your memory, closing with a brief script that brings you back into the present moment.
Begin the recording with progressive relaxation—use your favorite process for relaxing, or apply the script included here.
Generally tense the muscles for about 5 to 8 seconds and let go for 15 to 20 seconds as indicated by the …. inthe script. While tightening and relaxing the muscles, sense the muscle sensations with passive attention. Tense only the muscles that you are instructed to tighten and continue to breathe while tensing and relaxing the muscles. If your attention wanders, gently bring it back to feeling the sensations in the specific muscles that you are instructed to tighten or relax.
First, find a comfortable position for relaxation… To fully relax your face, squeeze your eyes shut tight, press your lips and teeth together, and wrinkle up your nose… feel the tightness in your whole face… Now let it go completely and relax… Allow your face to soften, feel the eyes sinking in their sockets, and your breath to flow effortlessly in and out…
Tense both arms by making fists, and extend them straight ahead, while continuing to breathe deeply… study the tension… Now relax and let your arms drop as if you were a rag doll… To relax your shoulders, hunch them toward your ears and tighten your neck, while keeping the rest of your body loose and relaxed… Continue to breathe easily… Allow your shoulders to drop… Feel the weight of your arms… Feel the relaxation flowing from your shoulders, down your arms into your hands and out your fingers…
Now your stomach. Then let go and relax… Arch your back and feel the tightness in the back. Let go and relax….Allow your body to sink comfortably into the surface on which you are resting… Finally, tighten your butt, thighs, calves, and feet by pressing your heels down into the surface where you are lying, curling your toes and squeezing your knees together… Feel the tension as you continue to breathe, keeping your upper body relaxed… Now let go and relax… Allow relaxation to flow through your legs… Be aware of the sensations of letting go…
Feel the deepening relaxation, the calmness and the serenity… Feel each exhalation flowing down and through your arms, chest, and legs… Let the feelings of relaxation and heaviness deepen as you relax more… Notice the developing sense of inner peace… a calm indifference to external events… Let the feelings of relaxation, calmness, and serenity deepen for a few minutes. After a few minutes, evoke your memory of wholeness.
Insert your imagery script here.
Finish with the brief closing script
Allow yourself to just stay in this special place all your own… and know that you can return to this peaceful sanctuary any time you choose to do so. When you are ready to release the imagery, take a deep breath, gently stretch your body, and open your eyes.
Record these this whole script on your cell phone as an MP3 file.
When you record, it often takes a few tries before the pacing is correct. You may find it helpful to listen to the following audio file as a model for to create your own.
LISTENING TO YOUR VISUALIZATION
Create a sanctuary for yourself by turning off your cellphone, adjusting the heat to a comfortable temperature, and ensuring that you will have uninterrupted quiet time for 20 to 30 minutes. Loosen any constricting clothing or jewelry, your glasses, and so on. Settle into a comfortable chair, bed, or setting where you can easily relax. Enjoy letting yourself drift into and relive the memory experience.
Many participants report that this practice is an exceptionally relaxing and nurturing experience, one that supports regeneration. You’ll probably find that the more you practice, the more the relaxation deepens. You may find it helpful to keep notes and observe how you feel after each practice. Although it may feel strange to listen to your own voice, most people find that after a while it becomes more comfortable. After listening to it for a few times, you may want to rerecord the script. Finally, generalize this practice by smiling and evoking the memory scene as much as you desire during the day.
Additional strategies to enhance the relaxation
- Have a massage or take a warm shower or soak and then do the practice. Compare your level of relaxation afterwards to the result of using the audio alone.
- Practice gentle stretches to loosen tight muscles or “shake out” your arms and legs just before doing your relaxation practice.
- Draw or paint the relaxing image or actually go to the location where your memory occurred (if possible) and do your practice. Or practice outdoors in the most relaxing place you can find. Nature can be a great healer.
- Create an atmosphere that helps to evoke and augment your relaxation image (e.g., play background music or use fragrances that you associated with the image).
Common challenges
- Inability to evoke a memory of wholeness. When this occurs, it is as if one draws a blank. This is common, especially if one has experienced abuse or feels depressed. In that case, use the image presented in the script or make one up and create a totally imaginary peaceful image.
- Positive memories of wholeness evoke a bitter/sweet feeling. This occurs when images of wholeness include a loved one who has passed on or who is no longer in your life. On the one hand, this may call up strongly positive feelings, but it may evoke a sense of loss and sadness. If this occurs, simply chose a different memory or create a different script. Let the memory of loss go. Accept your experience and your feelings as much as possible, and know that at least you have been loved. For your image, it may be easier to focus on a natural setting you love—one you associate with peace and tranquility.
- Lack of experience with places in nature. Some people have only urban experiences and find nature alien. See what comes up for you. Does your favorite memory as a city kid recall a day of freedom on your bike or skateboarding, or an afternoon with your playmates? Perhaps you have treasured memories as a teen or an adult of long walks in the city or time spent with close friends. You also have the option of creating new images such as sitting by a fireplace, in a walled garden, or some other scene of peace and safety.
- Difficulty using progressive relaxation. If you’re having trouble isolating a muscle: touch it, stroke it with your hands, and then tense it fully (without strain) and feel the tension in your hands; feel the difference with your hands as you let go of the tension. Or, you may tighten only as much as is needed to feel the tension.
- The desire to stay in the imagery and not wanting to return to reality. If the imagery is much more pleasant than the present, use this process as a stimulus to reorganize your life and set new goals and priorities.
References
Ader, R. & Cohen, N. (1993). Psychoneuroimmunology, Conditioning,_and_Stress. Annual Review of Psychology, 44(1), 53-85.
Ader, R., Cohen, N. and Felten, D. (1995) Psychoneuroimmunology: Interactions between the Nervous System and the Immune System. The Lancet, 345, 99-103.
https://doi.org/10.1016/S0140-6736(95)90066-7
Friedman, L. F. (2015). A radical experiment tried to make old people young again–and the results were astonishing . https://www.businessinsider.com/ellen-langers-reversing-aging-experiment-2015-4
Grierson, B. (2014). What if age is nothing more than a mind-set? New York Times Magazine. October 22.
Langer, E. (2009). Counterclockwise: Mindful Health and the Power of Possibility . New York: Ballantine Books.
McKenzie, J. (1886). The production of the so-called rose effect by means of an artificial rose, with remarks and historical notes. Am. J. Med. Sci. 91, 45–57
Peper, E., Gibney, K.H. & Holt. C. (2002). Make Health Happen: Training Yourself to Create Wellness . Dubuque, IA: Kendall-Hunt. ISBN-13: 978-0787293314
Peper, E. & Harvey, R. (2017). The fallacy of placebo controlled clinical trials: Are positive outcomes the result of indirect treatment side effects? NeuroRegulation. 4(3–4), 102–113. doi:10.15540/nr.4.3-4.102
Siegel, B. (2011, May). Remarkable recoveries. Retrieved from: http://berniesiegelmd.com/resources/articles/remarkable-recoveries/
Vits, S., Cesko, E., Enck, P., Hillen, U., Schadendorf, D., & Schedlowski, M. (2011). Behavioural conditioning as the mediator of placebo responses in the immune system. Philosophical Transactions: Biological Sciences, 366(1572), 1799–1807. http://www.jstor.org/stable/23035535
Experience how thoughts affect body with lemon imagery*
Posted: July 25, 2018 Filed under: behavior, Breathing/respiration, emotions, relaxation, self-healing, Uncategorized | Tags: autonomic nervous system, Holistic health, Imagery, mind-body, salivation, visualization 2 CommentsMost of us are aware that thoughts affect our body; however, we often overlook the impact of this effect. To demonstrate the power of visualization, participants are guided through a lemon imagery. In a study with 131 college students, 94% report an increase in salivation which is a parasympathetic nervous system response. The participants now know–not believe–that visualization affects physiology. Once salivation has been experienced, participants may apply other visualization techniques to change their physiology and behavior. Through visualization we communicate with our autonomic nervous system which can provide a matrix for self-healing and enhanced performance. In addition, the guided practice shows that almost everyone holds their breath when asked to tighten their muscles and some people have difficulty relaxing after tightening. Once aware, the person can and continue to breathe and relax the muscles. Enjoy the guided exercise, Mindbody connection: Lemon Imagery.
*I thank Paul Godina, Jung Lee and Lena Stampfli for participating in the videos.
Adapted from Peper, E., Gibney, K.H. & Holt. C. (2002). Make Health Happen: Training Yourself to Create Wellness. Dubuque, IA: Kendall-Hunt
Winning the Gold in weight lifting-Using biofeedback, imagery and cognitive change*
Posted: June 12, 2017 Filed under: Uncategorized | Tags: biofeedback, electromyography, Imagery, peak performance, visualization, weight lifting 5 CommentsErik Peper [1], [2] and Jo Aita
“It was the best meet of my life.” -Jo Aita
Setting a personal best and winning the Gold medal is a remarkable feat. Jo Aita, age 46 and weighing 58 kg, set the Masters World Records and Masters Games Records in Snatch, Clean & Jerk and Total Olympic weight lifting at the World Masters Games in Auckland, New Zealand, April 26th, 2017. She lifted 71 kg in the Snatch and 86 kg in the Clean and Jerk Olympic lifts in the 45-49-year-old age group (see video in figure 1). What makes this more remarkable is that her combined lifts were 3 kilograms more than her life-time best in previous competition. She refuted the conventional wisdom that weight lifters peak in their mid to late twenties. There is hope for improvement as aging may not mean we have to decline.
Figure 1. Video of Jo Aita successful lift at the World Masters Games in Auckland, NZ., April 26, 2017.
There are many factors–and many more which we do not know–which contribute to this achievement such as genetics, diligent training and superb coaching at the Max’ Gym in Oakland as a member of Team Juggernauts. In the last three years, Jo Aita also incorporated biofeedback and visualization training to help optimize her performance. This report summarizes how breathing and electromyography feedback combined with imagery may have contributed to achieving her personal best[3]. As Jo Aita stated, “I recommend this to everyone and hope that you can work with athletes in my gym.”
Components of the 30 sessions of biofeedback, internal language and visualization training program
The training was started in September 2014 to reduce anxiety and improve performance. The components embedded in the training are listed sequentially; however, training did not occur sequentially. They were dynamically interwoven throughout the many sessions and augmented with homework practices, as well as storytelling of other people achieving success using similar approaches. The major components included:
1. Mastering effortless slow diaphragmatic breathing in which the abdomen expanded during inhalations and constricted during exhalation. The respiration feedback and training was recorded with BioGraph Infinity respiration sensors and recorded from the abdomen and upper chest. Her homework included monitoring situations where she held her breath and then anticipate breath holding by continuing to breathe. She also practiced slower breathing with heart rate variability feedback from a Stress Eraser. Practicing these allowed her to become centered and regenerate more quickly. As she stated, “It helped me during the day when I am anxious to calm down.” Throughout the training, the focus was to use breathing to rapidly regenerate after exertion especially after training.
2. Learning to relax her shoulder muscles with electromyography (EMG) feedback to regenerate and learn awareness of minimal trapezius muscle tension. She could use this awareness to identify her emotional reactivity (Peper, Booiman, Lin, & Shaffer, 2014). Often emotional reactivity increases muscle tension. She learned to relax here muscles quickly after muscle contractions to allow regeneration
3. Experiencing how cognition affect performance. This was initially demonstrated by arm resistance test. In this experiential practice, she extended her arm and attempted to resist the downward pressure applied to her wrist while she recalled either a hopeless, helpless, powerless or defeated memory or an empowered positive memory (for detailed description see, Gorter and Peper, pp 186-188, 2011). When she recalled the powerless memory she was significantly weaker than when she recalled the empowering memory. This experience demonstrated to her the power of her thoughts.
4. Rewriting failure into success. Each time she missed the lift, she would think, “I should not have done that,” or “I was doubtful or nervous during competition,” she shifted her focus to:
- Accepting what happened by acknowledging she did the best she could have done under the circumstances.
- Exploring how she could have done it differently and imagine herself doing it in the new optimum way.
- Using the trigger of the beginning thought of failure or defeat to evoke the new empowering memory thus interrupting the chained behavior.
The underlying concept was that what we mentally rehearse is what we may become and that our thoughts affect performance which she previously experienced by the arm resistance test. If you keep thinking about a defeat you are training the physiological pattern of defeat. This practice of transforming self-defeating thoughts into empowering thoughts can be applied to all phases of one’s life and was continued throughout the training sessions. The focus was to acknowledge and realize that whatever you did, it was the only thing you could have done because you did not yet have the skills to do it differently. She would then create a new strategy of mental rehearsal that lead to a positive outcome (for detailed description of this practice see Peper, Harvey, Lin, & Duvvuri, 2014).
5. Identifying whether imagery rehearsal is somatically connected. It is our bias that imagery rehearsal is useful if the body responds in a similar pattern when the person images the task as it would during an actual activity (Hall, 2001; Peper et al, 2015). The concurrent physiological activity would indicate that the person is experientially involved in the task and not just observing as a witness/second party.
Her performance is weightlifting and this would involve major muscle activity. Surface EMG was recorded from muscles that would be activated during the actual performance of the task to identify if they would be activated during mental rehearsal. The muscle activity during mental rehearsal is usually at a much smaller amplitude than that occurred during actual physical performance; however, should follow a similar timing sequence. In our experience there are three responses:
- Muscle activity in the appropriate muscles that are in the same timing as in and actual performance. This implies that mental rehearsal is actually training the motor pattern and facilitate performance. Thus continue practicing with mental rehearsal.
- Muscle activity in the appropriate muscles are not generally in the same timing sequence as the actual performance. This may mean that the person was performing too slow or was skipping sequences in the mental rehearsal and mental training may not be useful. The person needs to master and exhibit the same muscle pattern during mental rehearsal as during actual performance of the task.
- No muscle activity or inappropriate muscle activity during the during the mental rehearsal. This implies that during mental rehearsal there is no motor pattern training and the approach would not be useful unless the person learned to activate appropriate motor activity. It is possible that some people who have experienced past traumas may have coped by shutting off feelings and sensations in their bodies.
When Jo Aita initially practiced mental rehearsal while being monitored with surface EMG recorded with Myoscan Pro sensors (filter set narrow 100-200Hz) from the right and left upper trapezius muscles, there was no corresponding muscle activity as shown in Figure 2. Although she imaged, she did not feel/experience the lifting. The training focused upon reconnecting imagery and body experience.

Figure 2. Left and right upper trapezius EMG showed no increase in activity while Jo Aita mentally imaged performing her lift.
6. Integrating imagery and body experience with EMG. After identifying that imagery did not elicit concurrent muscle activity, the training focused on developing the imagery muscle connection. The training consisted of:
- Monitoring EMG activity from her right and left quadriceps and right and left upper trapezius muscle and have her simulate her actually lifting in practice and competition by going through the complete sequence which included standing and waiting till her name was called, caulking her hands, performing a ritual activity to be ready to lift the weights, lifting the weights, and releasing them. The pattern is shown in Figure 3.

Figure 3. Simulating the actual Snatch and Jerk lift (Clean is lifting the weights to the chest and punching Jerk is pushing the weigh upward is labelled).
- Practicing imagery by going through the same procedure and purposely slightly activating the movements which were necessary to lift the weight. As she stated, “I learned to do mental rehearsal in a more structured way and visualized the total sequence from chalking up to doing all six lifts”. This was monitored by the EMG to see that there occurred EMG activation of the muscles. This was repeated numerous times till, the activation occurred in imagery as shown in Figure 4.[1]

Figure 4. EMG activity during mental rehearsal.
She then reported that imagery was a real experience.
7. Training mental rehearsal and imagery for peak performance (Cumming, Hall, & Shambrook, 2004). The major components of the mental rehearsal focused upon performing perfectly, visualizing lifting more weight easily than actually lifted in the gym, performing in the gym as she would during competing, practicing performing when interruptions occurred, and punching the weight through the ceiling.
- Performing perfectly. During the day she would mentally rehearse practicing lifting perfectly. In addition, as part of her readiness routine she would image performing the lift perfectly.
- Practicing recovery and being centered when interruptions would occur. For example, she was asked to role play competition and waiting for the judge to give the signal to start, I delayed giving her the signal to begin and told her the weights had to be adjusted because they had miss-loaded the bar. This way there would be no novelty during actual competition. This concept of coping with the unexpected was illustrated by Michael Phelps swimming the 200-meter butterfly in 2012 Being Olympics when his googles filled up with water when he dove in. Michael still won his 10th gold medal even though he swam part of the race blind (Fanning, E., June 25, 2012). He could do this because numerous time in the past, his coach had purposely trained Michael to swim with leaking googles
- Imagining lifting 10 kg more while competing. The concept of feeling/imagining yourself performing more that you can do at this moment creates the possibility for improvement since the limits of imagination may limit the experience/performance. As she reported, “This was incredibly helpful last year in competition when I needed to lift more than I had done before to qualify for the American Open, so I had mentally done it so often, then I just did it and made the qualifying lift.”
- Feeling your arms extending way up into the ceiling. Extending beyond your mental boundary of the test allows more power because the body tends to stop at the boundary. For example, when running 100 meters you want to see the finish line at least ten meters beyond the actual finish line this way you continue to run at maximum speed through the finish. If you focus on the actual finish line, you often slow down before reaching it. I told her how we used this concept with young male gymnasts to be able to do the iron cross for the first time by thinking of their arms being an iron beam and extending through the rings into the wall. In the case of lifting, you want to feel yourself punching the weight through the ceiling instead of just driving it upward. This portion of the lift when punching up into the ceiling is call the Jerk. This concept was experientially demonstrated by the following Aikido exercise of the iron arm.
Two people pair up and face each other. One stretches his arm straight out and rests the wrist and back of the palm on the shoulder of his partner. The partner put both hands on the elbow and then then pulls down trying to bend the elbow while his partner is try resist the downward force and try not to bend it as shown in Figure 5. 
Figure 5. Testing the effect of imagery on resisting downward pull at the elbow with wrist facing palm up.
Then relax, and repeat the same exercise except the person imagines that his arm is like a metal bar extending from their shoulders out through his hand into the wall. Once the person is imaging this, then the partner again attempts to bend the arm.
In almost all cases, when the person imagines the arm extending like an iron bar into the wall, it is much stronger and much more difficult to bend. Jo integrated this felt imagery in her lifting during practice and she experienced increased strength while imagining/feeling the iron bar and reported that she had the “best Jerks in her life.”
Discussion
Achieving a new world and personal record at age 46 in the master’s competition is a remarkable tribute to the athlete’s dedication and coaching. Although I (EP) may think I contributed, and hopefully what I taught was beneficial, in the end it is the athlete herself who has to perform in the competition–she is alone stands on the platform to lift the weights. When I (EP) asked whether the biofeedback visualization training was useful, Jo inequitably said, “Yes, and I would recommend this approach and training to everyone!” Watch the in-depth interview with Jo Aita in which she describes her experience of integrating imagery techniques and biofeedback to enhance performance on May 26, 2017.
What is interesting to ask is, how come a 46-year-old woman could lift 3 kg more than at any other time during her competitive career of Olympic lifting? It gives hope that loss of strength that commonly occurs as we age may be due less to aging than to learned disuse, injuries and lack of recovery. Most important factors are personal motivation and hope—you want to perform your best and know/believe that it is possible (Wilson and Peper, 2011). As Jo stated, “It helped for me to focus on doing my personal best.” I love Olympic lifting, I like taking care of my body, and I like feeling strong.” Finally, Jo is a recent athlete in her sport. She started lifting when she was 33 and competed one year later. She then took time out to give birth to her son and in a couple of months came back quickly and continued to become stronger. As she stated, “I always wanted to get stronger no matter what my age was.”
From a performance perspective it is interesting that she lifted more than ever before. Would it be possible that she is similar to many performers who achieve maximum performance after about 10 to 15 years of dedicated training? As she gets older, she improves her skills, increases efficiency of here muscles and neural connections. Is a possible that loss of performance as we age less due to aging than loss of motivation after years of practice, competition and achieving your goal. At that point life may offer other challenges and new opportunities.
* This blog was adapted and expanded from: Peper, E. & Aita, J. (2017). Winning the Gold in Weightlifting Using Biofeedback, Imagery and Cognitive Change. Biofeedback, 45(4), 77–82. DOI: 10.5298/1081-5937-45.4.01 https://biofeedbackhealth.files.wordpress.com/2018/02/a-winning-the-gold-in-weightlifting-published.pdf
References
Cumming, J., Hall, C., & Shambrook, C. (2004). The influence of an imagery workshop on athletes’ use of imagery. Athletic insight, 6(1), 52-73.
Fanning, E. (June 25, 2012). 50 stunning Olympic Moments No 42: Michael Phelps goes big in Being. Downloaded May 30, 2017 from https://www.theguardian.com/sport/blog/2012/jun/25/50-stunning-olympic-moments-michael-phelps
Gorter, R. & Peper, E. (2011). Fighting Cancer-A Non Toxic Approach to Treatment. Berkeley: North Atlantic.
Hall, C. (2001). Imagery in sport and exercise. In R. Singer, H. Hausenblas, & C. Janelle (Eds.), Handbook of Sport Psychology (pp. 529 – 549). New York, NY: John Wiley & Sons, Inc.
Peper, E., Harvey, R., Lin, I-M, & Duvvuri, P. (2014). Increase productivity, decrease procrastination and increase energy. Biofeedback, 42(2), 82-87.
Peper, E., Booiman, A., Lin, I-M., & Shaffer, F. (2014). Making the Unaware Aware-Surface Electromyography to Unmask Tension and Teach Awareness. Biofeedback.42(1), 16-23.
Footnotes:
[1] Correspondence: Erik Peper, Ph.D., Institute for Holistic Health Studies, Department of Health Education, San Francisco State University, 1600 Holloway Avenue, San Francisco, CA 94132. email: epeper@sfsu.edu; web: www.biofeedbackhealth.org; blog: www.peperperspective.com
[2] We thank Dr. Sue Wilson for her helpful and constructive feedback.
[3] We purposely use the word “may” because it is a case report and not a controlled study. Coaches, sport psychologist, or anyone who has had contact with an athlete who does extremely well usually claims that their suggestions were the magic ingredient; however, it could be synchronicity and not due to the actual skills taught. It may be due to unidentified factors or covert factors embedded in the coaching or teaching such as transforming hope and belief.
[4] Be aware that when people learn to reconnect with their body or learns slow diaphragmatic breathing and allow their lower abdomen to relax and expand, it is possible that past traumatic memories could be released. This release is a healthy process and we usually adapt an Autogenic Therapy/Training perspective by which the person accepts, allows discharge and continues with the task at hand.
Be a tree and share gratitude
Posted: December 11, 2016 Filed under: Breathing/respiration, self-healing, stress management, Uncategorized | Tags: gratitude, Holistic health, Imagery, relaxation, self-healing, stress management 1 Comment
It was late in the afternoon and I was tired. A knock on my office door. One of my students came in and started to read to me from a card. “I want to thank you for all your help in my self-healing project…I didn’t know the improvements were possible for me in a span of 5 weeks…. I thank you so much for encouraging and supporting me…. I have taken back control of myself and continue to make new discoveries about my identity and find my own happiness and fulfillment… Thank you so much.”
I was deeply touched and my eyes started to fill with tears. At that moment, I felt so appreciated. We hugged. My tiredness disappeared and I felt at peace.
In a world where we are constantly bombarded by negative, fearful stories and images, we forget that our response to these stories impacts our health. When people watch fear eliciting videos, their heart rate increases and their whole body responds with a defense reaction as if they are personally being threatened (Kreibig, Wilhelm, Roth, & Gross, 2007). Afterwards, we may continue to interpret and react to new stimuli as if they are the same as what happened in the video. For example, while watching a horror movie, we may hold our breath, perspire and feel our heart racing; however, when we leave the theatre and walk down the street by ourselves, we continue to be afraid and react to stimuli as if what happened in video will now happen to us.
When we feel threatened, our body responds to defend itself. It reduces the blood flow to the gastrointestinal tract where digestion is taking place and sends it to large muscles so that we can run and fight. When threatened, most of our resources shifted to the processes that promote survival while withdrawing it from processes that do not lead to immediate survival such as digestion or regeneration (Sapolsky, 2004). From an evolutionary perspective, why spent resources to heal yourself, enhance your immune system or digest your food when you will become someone else’s lunch!
The more we feel threatened, the more we will interpret the events around us negatively. We become more stressed, defensive, and pessimistic. If this response occurs frequently, it contributes to increased morbidity and mortality. We may not be in control of external or personal event; however, we may be able to learn how to change our reactions to these events. It is our reactions and interpretations of the event that contributes to our ongoing stress responses. The stressor can be labeled as crisis or opportunity.
Mobilize your own healing when you take charge. When 92 students as part of a class at San Francisco State University practiced self-healing skill, most reported significant improvements in their health as shown in Figure 1.
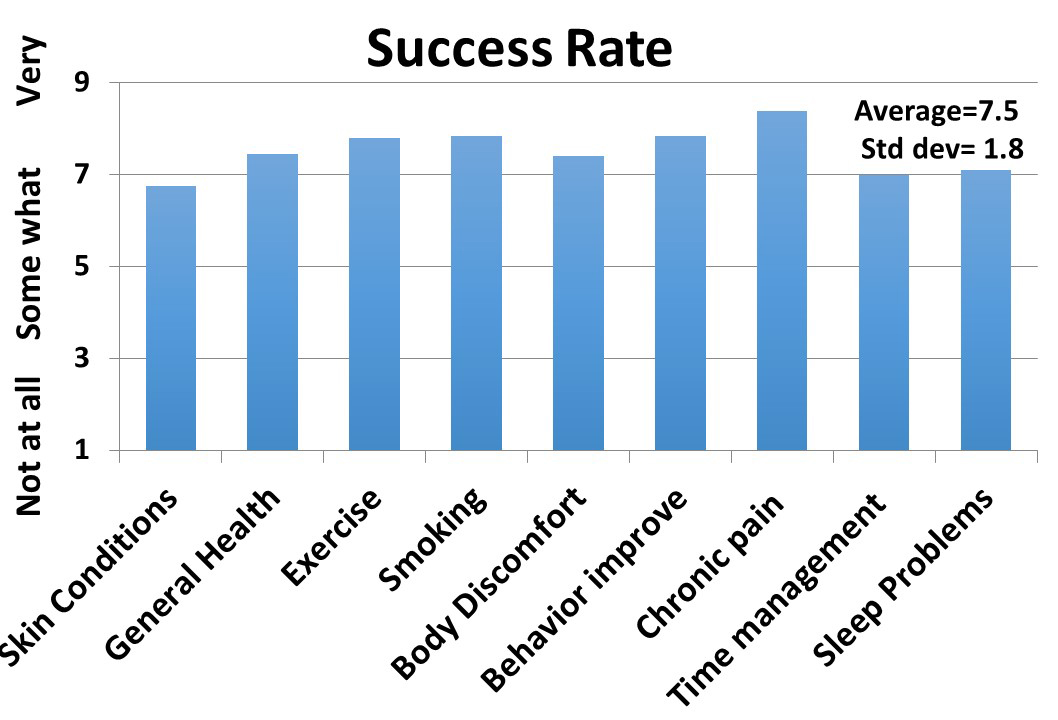
Figure 1. Average self-reported improvement after practicing self-healing skills for at least four weeks. (Reproduced with permission from Tseng, Abili, Peper, & Harvey, 2016).
A strategy that many students used was to interrupt their cascading automatic negative reactions. The moment they became aware of their negative thought and body slumping, they interrupted the process and practiced a very short relaxation or meditation technique.
Implement what the students have done by taking charge of your stress responses and depressive thoughts by 1) beginning the day with a relaxation technique, Relax Body-Mind, 2) interrupting the automatic response to stressors with a rapid stress reduction technique, Breathe and be a Tree, and 3) increasing vitality by the practice, Share Gratitude (Gorter & Peper, 2011).
Relax Body-Mind to start the day*
- Lie down or sit and close your eyes. During the practice if your attention wanders, just bring it back to that part of the body you are asked to tighten or let go.
- Wrinkle your face for ten seconds while continuing to breathe. Let go and relax for ten seconds.
- Bring your hands to your face with the fingers touching the forehead while continuing to breathe. While exhaling, pull your fingers down your face so that you feel your jaw being pulled down and relaxing. Drop your hands to your lap. Feel the sensations in your face and your fingers for ten seconds.
- Make a fist with your hands and lift them slightly up from your lap while continuing to breathe. Feel the sensations of tension in your hands, arms and shoulders for ten seconds. Let go and relax by allowing the arms to drop to your lap and relax. Feel the sensations change in your hands, arms and shoulders for ten seconds.
- Tighten your buttocks and flex your ankles so that the toes are reaching upwards to your knees. Hold for ten seconds while continuing to breathe. Let go and relax for ten seconds.
- Take a big breath while slightly arching your back away from the bed ore chair and expand your stomach while keeping your arms, neck, buttocks and legs relaxed. Hold the breath for twenty seconds. Exhale and let your back relax while allowing the breathing to continue evenly while sensing your body’s contact with the bed or chair for twenty seconds. Repeat three times.
- Gently shake your arms and legs for ten seconds while continuing to breathe. Let go and relax. Feel the tingling sensations in your arms and legs for 20 seconds.
- Evoke a past positive memory where you felt at peace and nurtured.
- Stretch and get up. Know you have done the first self-healing step of the day.
*Be gentle to yourself and stop the tightening or breath holding if it feels uncomfortable.
Breathe and be a Tree to dissipate stress and focus on growth
- Look at a tall tree and realize that you are like a tree that is rooted in the ground and reaching upward to the light. It continues to grow even though it has been buffeted by storms.
- When you become aware of being stressed, exhale slowly and inhale so that your stomach expands, the while slowly exhaling, look upward to the top of a real or imagined tree, admire the upper branches and leaves that are reaching towards the light and smile.
- Remember that even though you started to respond to a stressor, the stressor will pass just like storms battering the tree. By breathing and looking upward, accept what happened and know you are growing just like the tree.
Share Gratitude to increase vitality and health (adapted from Professor Martin Seligman’s 2004 TED presentation, The new era of positive psychology).
- Think of someone who did something for you that impacted your life in a positive direction and whom you never properly thanked. This could be a neighbor, teacher, friend, parent, or other family members.
- Write a 300-word testimonial describing specifically what the person did and how it positively impacted you and changed the course of your life.
- Arrange an actual face-to-face meeting with the person. Tell them you would like to see him/her. If they are far away, arrange a Skype call where you can actually see and hear him/her. Do not do it by email or texting.
- Meet with the person and read the testimonial to her/him.
- It may seem awkward to read the testimonial, after you have done it, you will feel closer and more deeply connected to the person. Moreover, the person to whom you read the testimonial, will usually feel deeply touched. Both your hearts will open.

References:
Gorter, R. & Peper, E. (2011). Fighting cancer: A nontoxic approach to treatment. Berkeley, CA: North Atlantic Books, 205-207.
Kreibig, S. D., Wilhelm, F. H., Roth, W. T., & Gross, J. J. (2007). Cardiovascular, electrodermal, and respiratory response patterns to fear‐and sadness‐inducing films. Psychophysiology, 44(5), 787-806.Kreibig, Sylvia D., Frank H. Wilhelm, Walton T. Roth, and James J. Gross. “Cardiovascular, electrodermal, and respiratory response patterns to fear‐and sadness‐inducing films.” Psychophysiology 44, no. 5 (2007): 787-806.
Sapolsky, R. (2004). Why Zebras Don’t Get Ulcers. New York: Owl Books
Seligman, M. (2014). The new era of positive psychology. Ted Talk. Retrieved, December 10, 2016. https://www.ted.com/talks/martin_seligman_on_the_state_of_psychology
Tseng, C., Abili, R., Peper, E., & Harvey, R. (2016). Reducing Acne-Stress and an integrated self-healing approach. Appl Psychophysiol Biofeedback, 4(4), 445.)
Seeing is believing*
Posted: February 14, 2016 Filed under: Uncategorized | Tags: biofeedback, CBT, cognitive behavior therapy, Imagery, min-body, musle tension, SCL, SEMG, skin conductance, visualization 3 CommentsMy arm did not move and yet the muscle tension from my forearm increased when I mentally rehearsed playing the piano. I did not notice anything. It really made me aware how my thoughts affect my body. –25 year old woman psychologist
*This blog was adapted from: Peper, E., Nemoto, S., Lin, I-M., & Harvey, R. (2015).
Therapists and educators can demonstrate the mind/body interaction with physiological monitoring to change their clients’ illness beliefs and demonstrate how ruminating thoughts may affect mental and physical health (Peper, Shumay, Moss, & Sztembis, 2013). When clients see how their body’s physiological responses are affected by thoughts and emotions, they gain a perspective that allows them to KNOW that thoughts affect body—the objective physiological evidence is indisputable.
The concept that thoughts affect the body has been described by many researchers. For example, Whatmore and Kohli (1975) used the term “Representing efforts,” which are the efforts we bring forth within our self during thinking, remembering, anticipating, daydreaming and worrying. Similarly, Green, Green and Walters (1970, p.3) described a process of thoughts influencing human physiological reactions as the Psycho-physiological principle, where “every change in the physiological state is accompanied by an appropriate change in the mental-emotional state, conscious or unconscious, and conversely, every change in the mental-emotional state, conscious or unconscious, is accompanied by an appropriate change in the physiological state.”
The mind/body connection can be demonstrated through recording physiological signals. For example, when a volunteer had her skin conductance (SC) level monitored, and then another person was asked in the group to give the volunteer a kiss, there was an increase in skin conductance response just after the instruction was given even though the person did not actually kiss the volunteer. The volunteer was responding to the instructions that a kiss might occur, as shown in Figure 1.

Figure 1. The effect on SC level of hearing the instruction that someone will give her a kiss
For educators and psychotherapists, biofeedback can be used to demonstrate the connection between positive or negative mental rehearsal, thoughts or visualization or recalling memories and physiological responses. This process can be demonstrated with surface electromyography (SEMG) recorded from muscles that become activated when the person mentally rehearses a task as illustrated in the following case example.
The participant was a 25 year old female psychologist who had practiced playing the piano for more than 16 years. Muscle activity was recorded from her right forearm extensor muscles and displayed on a large screen so that other group participants could observe. The physiological data and video recording of the volunteer were simultaneously recorded. The volunteer was asked to relax, imagine playing a musical piece, relax, and again imagine playing a musical piece and relax.
Results. Each time she imagined playing the piano, the forearm extensor muscle tension increased, even though there was no observed finger and forearm movements, as shown in Figure 2.

Figure 2. The covert SEMG increase in forearm SEMG as the participant imagined playing the piano.
After the recording, the session was replayed so she could see herself and her movements on the screen simultaneously with the SEMG signal. She reported being totally unaware that she had activated her forearm muscles and, was totally surprised when she saw the recording of the SEMG activity while her forearm appeared to stay in a relaxed position.
Discussion.The physiological monitoring demonstrated that her body responded to here thoughts and imagtes. In the case example, the arm muscle tension increased in tension when she mentally rehearsed playing the piano. This participant like most other people was unaware that her body reacted.If the thought of piano playing increased forearm tension,what would thoughts of anger, resentment, hopelessness, kindness or love do to the body. This concrete physiological demonstration illustrated that changing your thoughts changes your physiology. .
Once the person is aware how thoughts affect their body, it may motivate the person to become aware and change their cognitions. They can now understand that interrupting negative ruminations and behavior patterns and rehearsing new behavior patterns, their health can be improved. We strongly recommend that cognitive behavioral therapists, educators, psychologists, and other therapeutic practitioners include biofeedback monitoring for demonstrating the links between cognitions and physiological reactions.
After such a demonstration, the therapist may point out that what happens in the office setting is likely the identical process that occurs when a person worries, has negative cognitions, continuously reviews personal failures, or makes judgmental statements such as “I should not have done ________.”
When individuals think a negative statement such as “I should not have…………”, they are mentally rehearsing what they should not do and are unintentionally strengthening the negative behavior even more. Instead, whenever people becomes aware of the beginning of the negative cognitions, they can learn to stop and transform their negative cognitions to positive cognitions. In this way they can rehearse what they would want to do instead of what they do not want to do (Peper, Gibney, & Holt, 2002).
The more you rehearse what you want to achieve, the more likely it is to occur. This strategy is useful to change clients’ illness beliefs and motivate them to transform their cognitions from what they do not want to what they want to do. In addition, it offers cognitive behavior therapists documented evidence—the biofeedback recording provides the data which is necessary for evidence based medicine.
Between stimulus and response there is a space. In that space is our power to choose our response. In our response lies our growth and our freedom.
–Victor E. Frankle
References
Green, E.E., Green, A.M., & Walters, E.D. (1970). Voluntary control of internal states: Psychological and physiological. Journal of Transpersonal Psychology, 11, 1-26.
Peper, E., Gibney, K.H., & Holt. C. (2002). Make health happen: Training yourself to create wellness. Dubuque, IA: Kendall-Hunt.
Peper, E., Shumay, D. M., Moss, D. & Sztembis, R. (2013). The Power of Words, Biofeedback, and Somatic Feedback to Impact Illness Beliefs. Somatics .XVII(1), 4-8.
Whatmore, G.B., & Kohli, D. R. (1975). The physiopathology and treatment of functional disorders: Including anxiety states and depression and the role of biofeedback training. New York: Grune and Stratton, Inc.
Mind-Guided Body Scans for Awareness and Healing–Youtube Interview of Erik Peper, PhD by Larry Berkelhammer, PhD
Posted: December 23, 2013 Filed under: Uncategorized | Tags: biofeedback, body scan, body sensations, healing, Imagery, meditation, mind-body, passive attention, visualization 2 CommentsIn this interview psychophysiology expert Dr. Erik Peper explains the ways how a body scan can facilitate awareness and healing. The discussion describes how the mind-guided body scan can be used to improve immune function and hold passive attention (mindfulness) to become centered. It explores the process of passive attentive process that is part of Autogenic Training and self-healing mental imagery. Mind-guided body scanning involves effortlessly observing and attending to body sensations through which we can observe our own physiological processes. Body scanning can be combined with imagery to be in a nonjudgmental state that supports self-healing and improves physiological functioning.
