Will the stock market bubble collapse? Will human fertility decrease to zero?
Posted: July 13, 2026 Filed under: behavior, cancer, Evolutionary perspective, healing, health, lifestyle, Nutrition/diet | Tags: books, cycles, economics, fertility, financial bubble, sperm count, stocks, technology Leave a comment
“Those who cannot remember the past are condemned to repeat it.” – George Santayana (Santayana, 1905)
These two questions may seem totally unrelated, yet they are deeply connected if one takes a long historic view and hypothesizes that present-day trends will continue.
When I drive or commute, I very much enjoy listening to podcasts. They offer an in-depth, nuanced discussions that are missing from today’s soundbite culture. These deep-dive podcasts offer a vital antidote, providing the nuanced, extended discussions necessary for true cognitive synthesis. One of my favorite podcasts is The Diary of a CEO with Steven Bartlett. I found the recent episode, “Billionaire’s WARNING: I’m SELLING. The Crash Is Already Here!”, very eye opening.
The interview was with billionaire investor Jeremy Grantham, the co-founder and long-term investment strategist of GMO. He is also the chairman of the Grantham Foundation for the Preservation of the Environment, and co-author of “The Making of a Permabear: The Perils of Long-term Investing in a Short-term World.”
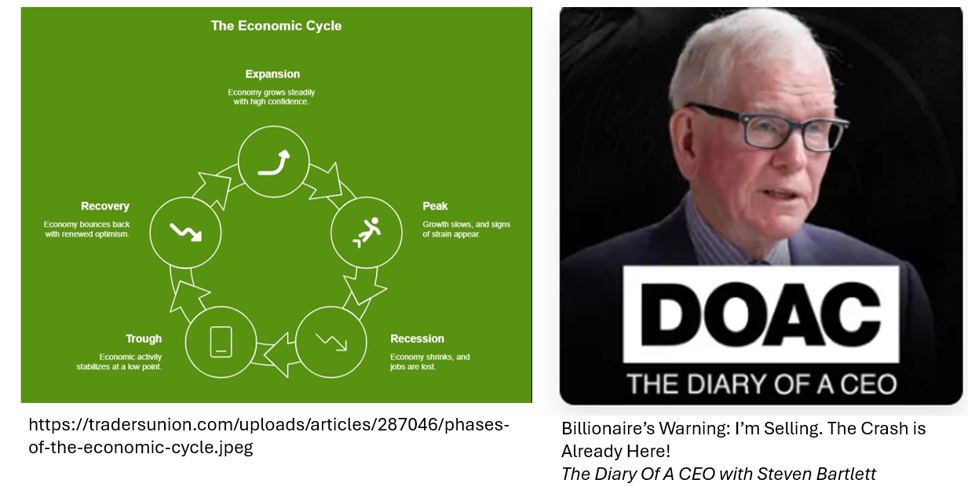
While economics and financial markets fall outside my primary line of research, I deeply appreciated his long-term perspective—an analysis I find to be entirely spot-on. The actual content offered a masterclass in pattern recognition, forcing me to sit back and critically analyze the macroeconomic shifts happening around us rather than just reacting to the daily noise of the market. He persuaded me that the present AI-driven financial bubble will burst; we simply do not know exactly when. I concur with him that it will occur sooner rather than later. Personally, I would not be surprised if it occurred within the next two years. We must simply be prepared to deal with more challenging times.
What surprised and fascinated me even more were the last 40 minutes of the podcast. Grantham shifted entirely away from the financial markets and applied that same rigorous, analytical thinking to what is truly driving the modern “baby bust” (Dilmaghani et al., 2024).
The scientific data is clear: human fertility—both male and female—has been decreasing each decade. This is starkly indicated by a 50% drop in male sperm counts and a rising number of couples struggling to conceive (Ravitsky & Kimmins, 2019; Mann et al., 2020; Inam, 2025). The culprits as for the increase in cancer rates? Ubiquitous modern disruptions like microplastics, pesticides, and pervasive environmental toxins (NIOSH, 2023; Doroftei et al., 2025; Brander et al., 2026).
Although the prognosis can look bleak, Grantham doesn’t just sound the alarm; he offers realistic strategies. He outlines how to protect yourself from the impending financial bubble collapse, as well as what you and your community can do to minimize toxic exposure and enhance fertility.
I smiled as I listened to the podcast, because his systemic analysis and practical recommendations are very similar to what we described in our just-published book, Cancer reconsidered-Why Environment, lifestyle, and immunity matter more than we thought (Peper et al., 2026).
To prepare yourself for the financial future and optimize your health and fertility, listen to Grantham’s insights on the podcast episode, “Billionaire’s WARNING: I’m SELLING. The Crash Is Already Here!”,
See the following blogs for more detailed information:
References
Brander, S.M., Swan, S.H., Mehinto, A.C., & et al. (2026). Impacts of environmental stressors on fertility and fecundity across taxa, with implications for planetary health. npj Emerging Contaminants, 2, Article 12. https://doi.org/10.1038/s44454-026-00032-6
Dilmaghani, D., Ainsworth, A. J., Nath, K. A., & Garovic, V. D. (2024). Decreasing fertility rate in the United States: Demographics, challenges, and consequences. Mayo Clinic Proceedings, 99(11), 1693–1697. https://doi.org/10.1016/j.mayocp.2024.09.004
Doroftei, B., Savuca, A., Cretu, A.-M., Maftei, R., Anton, N., Ilea, C., Doroftei, M., & Puha, B. (2025). Microplastics and human fertility: A comprehensive review of their presence in human samples and reproductive implication. Ecotoxicology and Environmental Safety, 303, Article 118939. https://doi.org/10.1016/j.ecoenv.2025.118939
Inam, Ö. (2025). Impact of microplastics on female reproductive health: Insights from animal and human experimental studies: A systematic review. Archives of Gynecology and Obstetrics, 312(1), 77–92. https://doi.org/10.1007/s00404-024-07929
Mann, U., Shiff, B., & Patel, P. (2020). Reasons for worldwide decline in male fertility. Current Opinion in Urology, 30(3), 296–301. https://doi.org/10.1097/MOU.0000000000000745
NIOSH. (2023, December 15). About pesticides and reproductive health. National Institute for Occupational Safety and Health Centers for Disease Control and Prevention. https://www.cdc.gov/niosh/reproductive-health/prevention/pesticides.html
Peper, E. Gorter, R. & Faass, N. (2026). Cancer Reconsidered: Why Environment, Lifestyle, and Immunity Matter More Than We Thought. BiofeedbackHealth/Regent Press. https://www.amazon.com/Cancer-Reconsidered-Environment-Lifestyle-Immunity/dp/1587907402/
Ravitsky, V. & Kimmins, S. (2019). The forgotten men: rising rates of male infertility urgently require new approaches for its prevention, diagnosis and treatment. Biol Reprod. 101(5), 872-874. https://doi.org/10.1093/biolre/ioz161
Santayana, G. (1905). The Life of Reason: Vol. 1. Reason in Common Sense. Charles Scribner’s Sons. p. 284. https://www.amazon.com/Reason-Phases-Progress-Introduction-Common/dp/B01DF937WU
Can Your Daily Choices Influence Cancer Risk and Recovery?
Posted: June 27, 2026 Filed under: behavior, Breathing/respiration, cancer, emotions, healing, health, lifestyle, Nutrition/diet, Pain/discomfort, self-healing, stress management, Uncategorized | Tags: diet, endocrine disregulators, environmental toxins, glucose monitors, health, Immune function, mental-health, nutrition, pollution, Quality of life, regeneration, resilience, social support, wellness 1 CommentWhat if the way you eat, move, sleep, manage stress, and connect with others could influence your body’s ability to prevent disease and support healing?
Most of us have been taught to think of cancer primarily as a genetic disease. Yet an expanding body of scientific research tells a more hopeful story: while genes matter, they are only part of the picture. Our environment, lifestyle, immune system, and even the quality of our relationships can profoundly influence health.
These are the questions explored in the newly published book Cancer Reconsidered: Why Environment, Lifestyle, and Immunity Matter More than We Thought, by Erik Peper, Robert Gorter, and Nancy Faass.
Written for people living with cancer, their families, healthcare professionals, and anyone interested in optimizing health, the book translates decades of scientific research into practical, evidence-based strategies that readers can use in everyday life.
Rather than viewing cancer through a single lens, Cancer Reconsidered brings together insights from conventional medicine with evidence-based complementary approaches. The authors explore how nutrition, physical activity, stress, sleep, environmental exposures, immune function, and social support interact to influence both cancer risk and the body’s remarkable capacity for repair and resilience.
One of the book’s central messages is both simple and empowering: although we cannot change our genes, we can often change the conditions in which our genes are expressed. Daily choices matter. Healthy habits can strengthen the body’s natural defenses, reduce inflammation, support immune function, and improve quality of life.
A particularly practical chapter explores blood sugar regulation and metabolism. Using continuous glucose monitors (CGMs) together with smartphone apps, readers can observe in real time how different foods, exercise, stress, and sleep affect their glucose levels. Instead of following one-size-fits-all advice, they become active investigators of their own health, discovering what works best for their unique physiology.
Throughout the book, the emphasis is not on fear, but on possibility. Scientific evidence increasingly shows that hope, meaningful social connections, regular movement, nourishing food, restorative sleep, effective stress management, and resilience are not simply “nice ideas”—they are biological factors that can significantly influence health and well-being.
Cancer Reconsidered invites readers to move beyond the question, “What causes cancer?” and instead ask, “What can I do today to create the best possible conditions for health?” It offers a thoughtful, scientifically grounded roadmap for anyone seeking to answer that question.
Cancer Reconsidered: Why Environment, Lifestyle, and Immunity Matter More than We Thought is now available on Amazon in paperback and and affordable ebook Kindle editions. https://www.amazon.com/s?k=cancer+reconsidered
Managing Blood Sugar: Lifestyle Changes for Better Health
Posted: May 25, 2026 Filed under: ADHD, attention, behavior, cancer, Evolutionary perspective, healing, health, lifestyle, Nutrition/diet, self-healing, Uncategorized | Tags: AIC, carbohydrate, continous glucose monitoring, diet, exhaustion, glucose, insulin, metabolic disease, obesity, sugar, ultra-processed foods Leave a comment
It was 4:45 p.m., and I was looking forward to swimming. I briskly walked the eight blocks from my house to the heated outdoor city pool. The pool is unusual—100 feet long instead of the standard 25 yards—and I enjoy the rhythm of swimming lap after lap.
I arrived just as the sign flipped from Closed to Open. I quickly changed into my bathing suit, locked my clothes in a metal locker, took a short shower, and jumped into the lane. The sun was still out, and only one other swimmer shared my lane. I felt energized and expected to complete my usual forty laps.
However, after about eighteen laps, my energy suddenly disappeared. There was nothing left in the tank. I swam to the side, pulled myself slowly onto the pool deck, and even slowly and unsteadily walked to the men’s locker room. I sat down on the bench feeling shaky, weak, and exhausted. This was not ordinary fatigue. After resting for several minutes, I slowly showered, dressed, and walked home with heavy, almost uncoordinated legs.
As I reflected on the experience, I remembered something similar that had happened two weeks earlier. Around 5 p.m, I had taken my son’s dog for a brisk walk. Again, I began energized, walking quickly, and then suddenly felt drained and sweaty. When I returned home, all I could do was sit down and recover.
What happened
Reflecting back, I realized that both cases I had eaten sweets—cake one time and a large chocolate chip cookie the other about two hours earlier Most likely, the rapidly absorbed sugars and refined carbohydrates caused a sharp increase in blood glucose, followed by a significant insulin response (Ludwig & Ebbeling, 2018). During exercise, my muscles then demanded additional glucose, and my blood sugar may have dropped rapidly enough to trigger symptoms of reactive hypoglycemia: shakiness, sweating, weakness, and fatigue (Morales-Brown, 2025, June 12).
The process is more complex than simply “sugar highs” and “crashes.” Carbohydrates are broken .break down into glucose during digestion, which begins in the mouth. Chewing breaks down food physically, while the enzyme amylase in saliva starts the chemical breakdown by splitting starches into sugars (Peyrot des Gachons & Breslin, 2016). This raises blood glucose levels, which stimulates insulin release from the pancreas. Insulin helps move glucose from the bloodstream into cells. In some people—especially those developing insulin resistance or prediabetes—the insulin response may overshoot, leading to a later drop in blood glucose. Exercise can amplify this effect because active muscles rapidly consume glucose for energy (American Diabetes Association, 2024).
This experience was a wake-up call for me because my hemoglobin A1C is 5.7%, the lower threshold for prediabetes. Hemoglobin A1C reflects average blood glucose levels over approximately the previous three months (American Diabetes Association, 2026).
Like many people, I enjoy and am even addicted to bread, potatoes, pastries, and sweets. Looking back, the subtle changes began during COVID. Before the pandemic, I spent much of the day teaching in person, walking across campus, moving, and interacting with students. During lockdown, I sat for hours teaching online. My physical activity during the day dramatically decreased while my eating habits did not significantly change.
When we are inactive, excess sugars and refined carbohydrates are less likely to be immediately used by muscles for fuel. Instead, repeated spikes in blood glucose and insulin can contribute over time to insulin resistance, weight gain, metabolic dysfunction, and increased inflammation (Ludwig & Ebbeling, 2018).
Although my episodes were minor, they reminded me that lifestyle patterns especially eating ultra-processed foods can increase the risk for chronic diseases such as type 2 diabetes, cardiovascular disease, obesity, and some cancers and dementia (Lane et al., 2024; Menegassi & Vinciguerra, 2025). The scientific literature strongly links obesity, insulin resistance, and type 2 diabetes with increased risk for several cancers, including colorectal and postmenopausal breast cancer (Peper et al., 2026; Scully et al., 2021: Lauby-Secretan et al., 2016). Ultra-processed foods and sugar-sweetened beverages are also associated with increased risk for obesity and metabolic disease; moreover, cancer survivors who consume higher amounts of ultra processed foods face a significantly increased risk of both all-cause and cancer-specific mortality (Hall et al., 2019; Bonaccio et al., 2026). However, cancer is multifactorial, and no single food alone “causes” cancer. Rather, long-term dietary patterns, inactivity, obesity, chronic inflammation, genetics, environmental exposures, sleep, and stress all interact together ( Marino et al., 2024; Dalamaga et al., 2026; Peper et al., 2026).
What to do
The encouraging news is that these processes are often reversible.
Weight, hunger, blood sugar fluctuations, and even A1C are not fixed. They can improve significantly through lifestyle changes. Research consistently shows that reducing ultra-processed foods, lowering intake of refined carbohydrates and sugary beverages, increasing fiber-rich vegetables, improving sleep, reducing stress, and exercising regularly can improve insulin sensitivity and metabolic health (Bird & Hawley, 2017; Vaezi et al., 2025; American Diabetes Association, 2024; Peper et al., 2026).
For many people, continuous glucose monitors (CGMs) can provide powerful real-time feedback (Ehrhardt & Zaghal, 2020). Seeing how specific foods affect your glucose levels can increase awareness and motivate healthier choices. Often, we do not realize how dramatically a muffin, fruit juice, or bowl of white rice may affect blood sugar until we see the data on the screen.
The goal is not perfection or rigid dieting. Instead, it is learning to observe how your body responds and gradually shifting toward foods that support stable energy, satiety, and long-term health.
Before making major dietary changes, watch the superb interview with Dr. David Unwin, a British physician known for his work using lower-carbohydrate dietary approaches to help patients improve type 2 diabetes and metabolic health. His clinical work demonstrates that many patients can significantly improve blood sugar control and sometimes reduce medications through lifestyle changes (Unwin et al., 2020). The video, The Sugar Doctor’s Warning: The “Healthy” Foods Quietly Destroying Your Body! – Dr. David Unwin, is from the podcast, The Diary of a CEO with Steven Bartlett.
The Link Between Diet, Lifestyle, and Cancer Risk: Steps You Can Take
Read the new book, Cancer Reconsidered: Why Environment, Lifestyle, and Immunity Matter More than We Thought, by Erik Peper, Robert Gorter, and Nancy Faass. It explore the many of the lifestyle factors that can increase cancer risk—or help protect against it. The book brings together an extraordinary range of scientific research to illuminate how everyday habits and modern lifestyles influence cancer risk and healing. Drawing from both conventional medicine and integrative approaches, the authors thoughtfully examine the many factors involved in cancer causation while offering hopeful, evidence-based strategies for supporting recovery and restoring health.
What makes this book especially compelling is that it goes far beyond reviewing the science. It translates research into practical, everyday actions people can use to support healing and improve quality of life. At its heart is lifestyle medicine—the recognition that stress management, hope, physical activity, nourishing foods, supportive relationships, community, and resilience during times of crisis profoundly affect health and well-being. The book also offers a detailed and highly practical discussion of sugar metabolism and explains how continuous glucose monitoring sensors (CGMS) with the smartphone app can help people directly observe how specific foods and daily habits influence their blood sugar levels. Instead of relying on abstract nutrition advice, readers learn how to become active investigators of their own health.
Throughout the book, the message is empowering: our daily habits, social connections, attitudes, and environment may influence health as much as—if not more than—genetics alone. The book is available from Amazon: https://www.amazon.com/Cancer-Reconsidered-Environment-Lifestyle-Immunity/dp/1587907402
Listen to the in-depth discussion of this blog created with Google NotebookLM
Addition relevant blogs
References
American Diabetes Association. (2026). Blood glucose and exercise. American Diabetes Association. Retrieved May 24, 2026, from https://diabetes.org/health-wellness/fitness/blood-glucose-and-exercise
American Diabetes Association. (2024). Standards of care in diabetes—2024. Diabetes Care, 47(Suppl. 1). https://diabetesjournals.org/care/issue/47/Supplement_1
Bonaccio, M., Di Castelnuovo, A., Costanzo, S., Ruggiero, E., Esposito, S., Panzera, T., Di Costanzo, G., De Curtis, A., Magnacca, S., Cerletti, C., Donati, M. B., de Gaetano, G., & Iacoviello, L., for the Moli-sani Study Group. (2026). Ultra-processed food and mortality among long-term cancer survivors from the Moli-sani Study: Prospective findings and analysis of biological pathways. Cancer Epidemiology, Biomarkers & Prevention, 35(4), 664–674. https://doi.org/10.1158/1055-9965.EPI-25-0808
Dalamaga, M., Rozani, S., & Petropoulou, D. (2026). Why is colorectal cancer occurring earlier? Metabolic dysfunction, underrecognized carcinogens, and emerging controversies. Current Obesity Reports, 15(1), 24. https://doi.org/10.1007/s13679-026-00700-z
Ehrhardt, N., & Al Zaghal, E. (2020). Continuous glucose monitoring as a behavior modification tool. Clinical Diabetes, 38(2), 126–131. https://doi.org/10.2337/cd19-0037
Hall, K. D., Ayuketah, A., Brychta, R., Cai, H., Cassimatis, T., Chen, K. Y., Chung, S. T., Costa, E., Courville, A., Darcey, V., Fletcher, L. A., Forde, C. G., Gharib, A. M., Guo, J., Howard, R., Joseph, P. V., McGehee, S., Ouwerkerk, R., Raisinger, K., … Zhou, M. (2019). Ultra-processed diets cause excess calorie intake and weight gain: An inpatient randomized controlled trial. Cell Metabolism, 30(1), 67–77. https://doi.org/10.1016/j.cmet.2019.05.008
Lane, M. M., Gamage, E., Du, S., Ashtree, D. N., McGuinness, A. J., Gauci, S., Baker, P., Lawrence, M., Rebholz, C. M., Srour, B., Touvier, M., Jacka, F. N., O’Neil, A., Segasby, T., & Marx, W. (2024). Ultra-processed food exposure and adverse health outcomes: Umbrella review of epidemiological meta-analyses. BMJ, 384, e077310. https://doi.org/10.1136/bmj-2023-077310
Lauby-Secretan, B., Scoccianti, C., Loomis, D., Grosse, Y., Bianchini, F., & Straif, K. (2016). Body fatness and cancer—Viewpoint of the IARC Working Group. New England Journal of Medicine, 375(8), 794–798. https://doi.org/10.1056/NEJMsr1606602
Ludwig, D. S., & Ebbeling, C. B. (2018). The carbohydrate-insulin model of obesity: Beyond “calories in, calories out.” JAMA Internal Medicine, 178(8), 1098–1103. https://doi.org/10.1001/jamainternmed.2018.2933
Marino, P., Mininni, M., Deiana, G., Marino, G., Divella, R., Bochicchio, I., Giuliano, A., Lapadula, S., Lettini, A. R., & Sanseverino, F. (2024). Healthy lifestyle and cancer risk: Modifiable risk factors to prevent cancer. Nutrients, 16(6), 800. https://doi.org/10.3390/nu16060800
Menegassi, B., & Vinciguerra, M. (2025). Ultraprocessed food and risk of cancer: Mechanistic pathways and public health implications. Cancers, 17(13), 2064. https://doi.org/10.3390/cancers17132064
Morales-Brown, P. (2025, June 12). What is reactive hypglycemia. Medical News Today. Accessed May 24, 2026. https://www.medicalnewstoday.com/articles/reactive-hypoglycemia
Peper, E., Gorter, R., & Faass, N. (2026). Cancer reconsidered: Why environment, lifestyle, and immunity matter more than we thought. Biofeedback Health. https://www.amazon.com/Cancer-Reconsidered-Environment-Lifestyle-Immunity/dp/1587907402
Peyrot des Gachons, C., & Breslin, P. A. S. (2016). Salivary amylase: Digestion and metabolic syndrome. Current Diabetes Reports, 16, 102. https://doi.org/10.1007/s11892-016-0794-7
Scully, T., Ettela, A., LeRoith, D., & Gallagher, E. J. (2021). Obesity, type 2 diabetes, and cancer risk. Frontiers in Oncology, 10, 615375. https://doi.org/10.3389/fonc.2020.615375
Unwin, D., Khalid, A. A., Unwin, J., Crocombe, D., Delon, C., Martyn, K., Hasan, M., & Tobin, S. D. (2020). Insights from a general practice service evaluation supporting a lower carbohydrate diet in patients with type 2 diabetes mellitus and prediabetes: A secondary analysis of routine clinic data including HbA1c, weight and prescribing over 6 years. BMJ Nutrition, Prevention & Health, 3(2), 285–294. https://doi.org/10.1136/bmjnph-2020-000072
Vaezi, S., Freeling, J. L., de Vargas, B. O., Weidauer, L., Shoemaker, M. E., Sanders, W. M., & Dey, M. (2025). Impacts of minimally-processed omnivorous vs lacto-ovo-vegetarian diets on insulin sensitivity, lipid profile, and adiposity in older adults: Secondary findings from a randomized crossover feeding trial. Clinical Nutrition, 55, 90–103. https://doi.org/10.1016/j.clnu.2025.10.010
Grandmother Therapy: A Common-Sense Approach to Health and Wellness
Posted: July 24, 2024 Filed under: ADHD, attention, behavior, education, Evolutionary perspective, Exercise/movement, Nutrition/diet, Pain/discomfort, relaxation, self-healing | Tags: anxiety, depression, epilepsy, exhaustion, grandmother therapy, health, insomnia, life style change, mental-health, therapy 1 CommentErik Peper, PhD and Angelika Sadar, MA

In today’s fast-paced world, college students and young adults often struggle with various health issues. From anxiety and depression to ADHD and epilepsy, these challenges can significantly impact their daily lives. But what if the solution to many of these problems lies in something as simple as “Grandmother Therapy”?
What is Grandmother Therapy? Grandmother Therapy is all about going back to basics and establishing healthy lifestyle habits. It’s the common-sense approach that our grandmothers might have suggested: regular sleep patterns, balanced nutrition, increased social connections, and regular physical activity.
The Problem: Many college students:
- Skip breakfast before their first class
- Rely on fast food and sugary stimulants
- Have irregular sleep schedules
- Spend excessive time on gaming and social media
The Medical Approach: Often, the quick solution is medication:
- Depression? Take antidepressants.
- Insomnia? Use sleeping pills.
- Anxiety? Try anti-anxiety medication.
- ADHD? Prescribe Ritalin or similar drugs.
While these treatments may help manage symptoms, they often overlook the underlying lifestyle factors contributing to these issues.
The Grandmother Therapy Approach:
- Establish regular sleep patterns
- Adopt healthy eating habits
- Increase social connections
- Incorporate regular physical activity
- Reduce gaming and social media use
Case Study #1: The Power of Sleep
This illustrates the simple intervention of having a bedtime routine. A college student in a holistic health class complained that she was tired most of the time and had difficulty focusing her attention and continuously drifted off in class.
Here is her reported sleep schedule:
- last night I went to bed at 3am and woke up 7;
- the day before, I went to bed at 1pm and woke up at 6,
- two nights before, I went to bed at 4pm and woke up at 10 am.
Holistic treatment approach:
Set a sleep schedule: she was provided with information about the importance of having a regular pattern of sleep and waking. Namely, go to bed at the same time and get up 8 hours later. She agreed to do an experiment for a week to go to bed at 12 and wake up at 8m. To her surprise, she felt so much more energized and could pay attention in class during the week of the experiment.
Case Study #2: Beyond Seizures: A Holistic Approach to Treating Psychogenic Nonepileptic Seizures
This case study highlights the importance of a comprehensive, lifestyle-based approach to treating psychogenic nonepileptic seizures (PNES). It follows a 24-year-old male student initially diagnosed with intractable epilepsy, experiencing over 10 seizures per week that didn’t respond to medication.
Key points:
1. Initial misdiagnosis: Despite normal MRI and EEG results, the client was initially treated for epilepsy.
2. Limited assessment: Traditional medical evaluations focused solely on seizure descriptions and diagnostics, overlooking crucial lifestyle factors.
3. Comprehensive evaluation: A psychophysiological assessment revealed high sympathetic arousal, including rapid breathing, sweaty palms, and muscle tension.
4. Lifestyle factors: The client’s diet consisted of high-glycemic fast foods, excessive caffeine, alcohol, and daily marijuana use. He also had significant student debt and a history of abdominal surgery.
Holistic treatment approach:
– Dietary changes: Switching to unprocessed, low-glycemic foods and increasing vegetable and fruit intake
– Breathing techniques: Learning and practicing slow diaphragmatic breathing
– Stress management: Addressing underlying stressors and practicing relaxation techniques
– Supplements: Adding omega-3 and multivitamins to support brain health
Remarkable results: Within four months, the patient became seizure-free, reduced marijuana use significantly, and decreased medication dosage.
Summary
These cases underscore the potential of integrating lifestyle modifications and stress management techniques in treating attention, anxiety and even psychogenic nonepileptic seizures; offering hope for patients who don’t respond to traditional treatments alone. Before turning to medication or complex treatments, consider the power of Grandmother Therapy. By addressing fundamental lifestyle factors, we can often improve our health and well-being significantly. Remember, sometimes the most effective solutions are the simplest ones.
The Challenges of Simplicity: While Grandmother Therapy may seem straightforward, its simplicity can make it challenging to implement. It requires commitment and a willingness to change long-standing habits.
Implement many Life Style Changes at once: Recommending one change at the time is logical; however, participants will more likely experience rapid benefits and are more motivated to continue when they change multiple lifestyle factors at once.
Call to Action: Are you struggling with health issues? Try implementing some aspects of Grandmother Therapy in your life. Implement changes and see how they impact your overall well-being.
Please let us know your experience with implementing Grandmother Therapy.
See the following blogs for more background information
Reflections on the increase in Autism, ADHD, anxiety and depression: Part 2- Exposure to neurotoxins and ultra-processed foods
Posted: June 30, 2024 Filed under: ADHD, attention, behavior, CBT, digital devices, education, emotions, Evolutionary perspective, health, mindfulness, neurofeedback, Nutrition/diet, Uncategorized | Tags: ADHD, anxiety, depression, diet, glyphosate, herbicide, herbicites, mental-health, neurofeedback, pesticides, supplements', ultraprocessed foods, vitamins 4 CommentsAdapted from: Peper, E. & Shuford, J. (2024). Reflections on the increase in Autism, ADHD, anxiety and depression: Part 2- Exposure to neurotoxins and ultra-processed foods. NeuroRegulation, 11(2), 219–228. https://doi.org/10.15540/nr.11.2.219
Look at your hand and remember that every cell in your body including your brain is constructed out the foods you ingested. If you ingested inferior foods (raw materials to be built your physical structure), then the structure can only be inferior. If you use superior foods, you have the opportunity to create a superior structure which provides the opportunity for superior functioning. -Erik Peper
Summary
Mental health symptoms of attention deficit hyperactivity disorder (ADHD), Autism, anxiety and depression have increased over the last 15 years. An additional risk factor that may affect mental and physical health is the foods we eat. Even though, our food may look and even taste the same as compared to 50 years ago, it contains herbicide and pesticide residues and often consist of ultra-processed foods. These foods (low in fiber, and high in sugar, animal fats and additives) are a significant part of the American diet and correlate with higher levels of inattention and hyperactivity in children with ADHD. Due to affluent malnutrition, many children are deficient in essential vitamins and minerals. We recommend that before beginning neurofeedback and behavioral treatments, diet and lifestyle are assessed (we call this Grandmother therapy assessment). If the diet appears low in organic foods and vegetable, high in ultra-processed foods and drinks, then nutritional deficiencies should be assessed. Then the next intervention step is to reduce the nutritional deficiencies and implement diet changes from ultra-processed foods to organic whole foods. Meta-analysis demonstrates that providing supplements such as Vitamin D, etc. and reducing simple carbohydrates and sugars and eating more vegetables, fruits and healthy fats during regular meals can ameliorate the symptoms and promote health.
The previous article and blog, Reflections on the increase in Autism, ADHD, anxiety and depression: Part 1-bonding, screen time, and circadian rhythms, pointed out how the changes in bonding, screen time and circadian rhythms affected physical and mental health (Peper, 2023a; Peper, 2023b). However, there are many additional factors including genetics that may contribute to the increase is ADHD, autism, anxiety, depression, allergies and autoimmune illnesses (Swatzyna et al., 2018). Genetics contribute to the risk of attention deficit hyperactivity disorder (ADHD); since, family, twin, and adoption studies have reported that ADHD runs in families (Durukan et al., 2018; Faraone & Larsson, 2019). Genetics is in most cases a risk factor that may or may not be expressed. The concept underlying this blog is that genetics loads the gun and environment and behavior pulls the trigger as shown in Figure 1.

Figure 1. Interaction between Genetics and Environment
The pandemic only escalated trends that already was occurring. For example, Bommersbach et al (2023) analyzed the national trends in mental health-related emergency department visits among USA youth, 2011-2021. They observed that in the USA, Over the last 10 years, the proportion of pediatric ED visits for mental health reasons has approximately doubled, including a 5-fold increase in suicide-related visits. The mental health-related emergency department visits increased an average of 8% per year while suicide related visits increased 23.1% per year. Similar trends have reported by Braghieri et al (2022) from the National Survey on Drug Use and Health as shown in Figure 2.

Figure 2. Mental health trends in the United States by age group in 2008–2019. The data come from the National Survey on Drug Use and Health. Reproduced with permission from Braghieri, Luca and Levy, Ro’ee and Makarin, Alexey, Social Media and Mental Health (July 28, 2022) https://ssrn.com/abstract=3919760 or http://dx.doi.org/10.2139/ssrn.3919760
The trends reported from this data shows an increase in mental health illnesses for young people ages 18-23 and 24-29 and no changes for the older groups which could be correlated with the release of the first iPhone 2G on June 29, 2007. Thus, the Covid 19 pandemic and social isolation were not THE CAUSE but an escalation of an ongoing trend. For the younger population, the cellphone has become the vehicle for personal communication and social connections, many young people communicate more with texting than in-person and spent hours on screens which impact sleep (Peper, 2023a). At the same time, there are many other concurrent factors that may contributed to increase of ADHD, autism, anxiety, depression, allergies and autoimmune illnesses.
Without ever signing an informed consent form, we all have participated in lifestyle and environmental changes that differ from that evolved through the process of evolutionary natural selection and promoted survival of the human species. Many of those changes in lifestyle are driven by demand for short-term corporate profits over long-term health of the population. As exemplified by the significant increase in vaping in young people as a covert strategy to increase smoking (CDC, 2023) or the marketing of ultra-processed foods (van Tulleken, 2023).
This post focusses how pesticides and herbicides (exposure to neurotoxins) and changes in our food negatively affects our health and well-being and is may be another contributor to the increase risk for developing ADHD, autism, anxiety and depression. Although our food may look and even taste the same compared to 50 years ago, it is now different–more herbicide and pesticide residues and is often ultra-processed. lt contains lower levels of nutrients and vitamins such as Vitamin C, Vitamin B2, Protein, Iron, Calcium and Phosphorus than 50 years ago (Davis et al, 2004; Fernandez-Cornejo et al., 2014). Non-organic foods as compared to organic foods may reduce longevity, fertility and survival after fasting (Chhabra et al., 2013).
Being poisoned by pesticide and herbicide residues in food
Almost all foods, except those labeled organic, are contaminated with pesticides and herbicides. The United States Department of Agriculture reported that “Pesticide use more than tripled between 1960 and 1981. Herbicide use increased more than tenfold (from 35 to 478 million pounds) as more U.S. farmers began to treat their fields with these chemicals” (Fernandez-Cornejo, et al., 2013, p 11). The increase in herbicides and pesticides is correlated with a significant deterioration of health in the United States (Swanson, et al., 2014 as illustrated in the following Figure 3.


Figure 3. Correlation between Disease Prevalence and Glyphosate Applications (reproduced with permission from Swanson et al., 2014.
Although correlation is not causation and similar relationships could be plotted by correlating consumption of ultra-refined foods, antibiotic use, decrease in physical activity, increase in computer, cellphone and social media use, etc.; nevertheless, it may suggest a causal relationship. Most pesticides and herbicides are neurotoxins and can accumulate in the person over time this could affect physical and mental health (Bjørling-Poulsen et al., 2008; Arab & Mostaflou, 2022). Even though the United States Environmental Protection Agency (EPA) has determined that the residual concentrations in foods are safe, their long-term safety has not been well established (Leoci & Ruberti, 2021). Other countries, especially those in which agribusiness has less power to affect legislation thorough lobbying, and utilize the research findings from studies not funded by agribusiness, have come to different conclusions…
For example, the USA allows much higher residues of pesticides such as, Round-Up, with a toxic ingredient glyphosate (0.7 parts per million) in foods than European countries (0.01 parts per million) (Wahab et al., 2022; EPA, 2023; European Commission, 2023) as is graphically illustrated in figure 4.

Figure 4: Percent of Crops Sprayed with Glyphosate and Allowable Glyphosate Levels in the USA versus the EU
The USA allows this higher exposure than the European Union even though about half of the human gut microbiota are vulnerable to glyphosate exposure (Puigbo et al., 2022). The negative effects most likely would be more harmful in a rapidly growing infant than for an adult. Most likely, some individuals are more vulnerable than others and are the “canary in mine.” They are the early indicators for possible low-level long-term harm. Research has shown that fetal exposure from the mother (gestational exposure) is associated with an increase in behaviors related to attention-deficit/hyperactivity disorders and executive function in the child when they are 7 to 12 years old (Sagiv et al., 2021). Also, organophosphate exposure is correlated with ADHD prevalence in children (Bouchard et al., 2010). We hypothesize this exposure is one of the co-factors that have contributed to the decrease in mental health of adults 18 to 29 years.
At the same time as herbicides and pesticides acreage usage has increased, ultra-processed food have become a major part of the American diet (van Tulleken, 2023). Eating a diet high in ultra-processed foods, low in fiber, high sugar, animal fats and additives has been associated with higher levels of inattention and hyperactivity in children with ADHD; namely, high consumption of sugar, candy, cola beverages, and non-cola soft drinks and low consumption of fatty fish were also associated with a higher prevalence of ADHD diagnosis (Ríos-Hernández et al., 2017).
In international studies, less nutritional eating behaviors were observed in ADHD risk group as compared to the normal group (Ryu et al., 2022). Artificial food colors and additives are also a public health issue and appear to increase the risk of hyperactive behavior (Arnold et al., 2012). In a randomized double-blinded, placebo controlled trial 3 and 8/9 year old children had an increase in hyperactive behavior for those whose diet included extra additives (McCann et al., 2007). The risk may occur during fetal development since poor prenatal maternal is a critical factor in the infants neurodevelopment and is associated with an increased probability of developing ADHD and autism (Zhong et al., 2020; Mengying et al., 2016).
Poor nutrition even affects your unborn grandchild
Poor nutrition not only affects the mother and the developing fetus through epigenetic changes, it also impacts the developing eggs in the ovary of the fetus that can become the future granddaughter (Wilson, 2015). At birth, the baby has all of her eggs. Thus, there is a scientific basis for the old wives tale that curses may skip a generation. Providing maternal support is even more important since it affects the new born and the future grandchild. The risk may even begin a generation earlier since the grandmother’s poor nutrition as well as stress causes epigenetic changes in the fetus eggs. Thus 50% of the chromosomes of the grandchild were impacted epigenetically by the mother’s and grandmother’s dietary and health status .
Highly processed foods
Highly refined foods have been processed to remove many of their nutrients. These foods includes white bread, white rice, pasta, and sugary drinks and almost all the fast foods and snacks. These foods are low in fiber, vitamins, and minerals, and they are high in sugars, unhealthy fats, and calories. In addition, additives may have been added to maximize taste and mouth feel and implicitly encourage addiction to these foods. A diet high in refined sugars and carbohydrates increases the risk of diabetes and can worsen the symptoms of ADHD, autism, depression, anxiety and increase metabolic disease and diabetes (Woo et al., 2014; Lustig, 2021; van Tulleken, 2023). Del-Ponte et al. (2019) noted that a diet high in refined sugar and saturated fat increased the risk of symptoms of ADHD, whereas a healthy diet, characterized by high consumption of fruits and vegetables, would protect against the symptoms.
Most likely, a diet of highly refined foods may cause blood sugar to spike and crash, which can lead to mood swings, irritability, anxiety, depression and cognitive decline and often labeled as “hangryness” (the combination of anger and hunger) (Gomes et al., 2023; Barr et al., 2019). At the same time a Mediterranean diet improves depression significantly more than the befriending control group (Bayles et al., 2022). In addition, refined foods are low in essential vitamins and minerals as well as fiber. Not enough fiber can slow down digestion, affect the human biome, and makes it harder for the body to absorb nutrients. This can lead to nutrient deficiencies, which can contribute to the symptoms of ADHD, autism, depression, and anxiety. Foods do impact our mental and physical health as illustrated by foods that tend to reduce depression (LaChance & Ramsey, 2018; MacInerney et al., 2017). By providing appropriate micronutrients such as minerals (Iron, Magnesium Zinc), vitamins (B6, B12, B9 and D), Omega 3s (Phosphatidylserine) and changing our diet, ADHD symptoms can be ameliorated.
Many children with ADHD, anxiety, depression are low on essential vitamins and minerals. For example, low levels of Omega-3 fatty acids and vitamin D may be caused by eating ultra-refined foods, fast foods, and drinking soft drink. At the same time, the children are sitting more in indoors in front of the screen and thereby have lower sun exposure that is necessary for the vitamin D production.
“Because of lifestyle changes and sunscreen use, about 42% of Americans are deficient in vitamin D. Among children between 1 to 11 years old, an estimated 15% have vitamin D deficiency. And researchers have found that 17% of adolescents and 32% of young adults were deficient in vitamin D.” (Porto and Abu-Alreesh, 2022).
Reduced sun exposure is even more relevant for people of color (and older people); since, their darker skin (increased melanin) protects them from ultraviolet light damage but at the same time reduces the skins production of vitamin D. Northern Europeans were aware of the link between sun exposure and vitamin D production. To prevent rickets (a disease caused by vitamin D deficiency) and reduce upper respiratory tract infections the children were given a tablespoon of cod liver oil to swallow (Linday, 2010). Cod liver oil, although not always liked by children, is more nutritious than just taking a Vitamin D supplements. It is a whole food and a rich source of vitamin A and D as well as containing a variety of Omega 3 fatty acids (eicosapentaenoic acid (EPA) (USDA, 2019).
Research studies suggest that ADHD can be ameliorated with nutrients, and herbs supplements (Henry & CNS, 2023). Table 1 summarizes some of the nutritional deficits observed and the reduction of ADHD symptoms when nutritional supplements were given (adapted from Henry, 2023; Henry & CNS, 2023).
| Nutritional deficits observed in people with ADHD | Decrease in ADHD symptoms with nutritional supplements |
| Vitamin D: In meta-analysis with a total number of 11,324 children, all eight trials reported significantly lower serum concentrations of 25(OH)D in patients diagnosed with ADHD compared to healthy controls. (Kotsi et al, 2019) | After 8 weeks children receiving vitamin D (50,000 IU/week) plus magnesium (6 mg/kg/day) showed a significant reduction in emotional problems as observed in a randomized, double blind, placebo-controlled clinical trial (Hemamy et al., 2021). |
| Iron: In meta-analysis lower serum ferritin was associated with ADHD in children (Wang et al., 2017) and the mean serum ferritin levels are lower in the children with ADHD than in the controls (Konofal et al., 2004). | After 12 weeks of supplementation with Iron (ferrous sulfate) in double-blind, randomized placebo-controlled clinical trial, clinical trials symptoms of in children with ADHD as compared to controls were reduced (Tohidi et al., 2021; Pongpitakdamrong et all, 2022). |
| Omega 3’s: Children with ADHD are more likely to be deficient in omega 3’s than children without ADHD (Chang et al., 2017). | Adding Omega-3 supplements to their diet resulted in an improvement in hyperactivity, impulsivity, learning, reading and short term memory as compared to controls in 16 randomized controlled trials including 1514 children and young adults with ADHD (Derbyshire, 2017) |
| Magnesium: In meta-analysis, subjects with ADHD had lower serum magnesium levels compared with to their healthy controls (Effatpahah et al., 2019) | 8 weeks of supplementation with Vitamin D and magnesium caused a significant decrease in children with conduct problems, social problems, and anxiety/shy scores (Hemamy et al., 2020). |
| Vitamin B2, B6, B9 and B12deficiency has been found in many patients with Attention Deficit and Hyperactivity Disorder (Landaas et al, 2016; Unal et al., 2019). | Vitamin therapy appears to reduce symptoms of ADHD and ASD (Poudineh et al., 2023; Unal et al., 2019). An 8 weeks supplementing with Vitamin B6 and magnesium decreased hyperactivity and hyperemotivity/aggressiveness. When supplementation was stopped, clinical symptoms of the disease reappeared in few weeks (Mousain-Bosc et al., 2006). |
Table 1. Examples of vitamin and mineral deficiencies associated with symptoms of ADHD and supplementation to reduction of ADHD symptoms.
Supplementation of vitamins and minerals in many cases consisted of more than one single vitamin or mineral. For an in-depth analysis and presentation, see the superb webinar by Henry & CNS (2023): https://divcom-events.webex.com/recordingservice/sites/divcom-events/recording/e29cefcae6c1103bb7f3aa780efee435/playback? (Henry & CNS, 2023).
Whole foods are more than the sum of individual parts (the identified individual constituents/nutrients). The process of digestion is much more complicated than ingesting simple foods with added vitamins or minerals. Digestion is the interaction of many food components (many of which we have not identified) which interact and affect the human biome. A simple added nutrient can help; however, eating whole organic foods it most likely be healthier. For example, whole-wheat flour is much more nutritious. Whole wheat is rich in vitamins B-1, B-3, B-5, riboflavin, folate well as fiber while refined white flour has been bleached and stripped of fiber and nutrients to which some added vitamins and iron are added.
Recommendation
When working with clients, follow Talib’s principles as outlined in Part 1 by Peper (2023) which suggests that to improve health first remove the unnatural which in this case are the ultra-processed foods, simple carbohydrates, exposure to pesticides and herbicides (Taleb, 2014). The approach is beneficial for prevention and treatment. This recommendation to optimize health is both very simple and very challenging. The simple recommendation is to eat only organic foods and as much variety as possible as recommended by Professor Michael Pollan in his books, Omnivore’s Dilemma: A Natural History of Four Meals and Food Rules (Pollan, 2006; Pollan, 2011).
Do not eat foods that contain herbicides and pesticide residues or are ultra-processed. Although organic foods especially vegetable and fruits are often much more expensive, you have choice: You can pay more now to optimize health or pay later to treat disease. Be safe and not sorry. This recommendation is similar to the quote, “Let food be thy medicine and medicine be thy food,” that has been attributed falsely since the 1970s to Hippocrates, the Greek founder of western medicine (5th Century, BC) (Cardenas, 2013).
There are many factors that interfere with implementing these suggestions; since, numerous people live in food deserts (no easy access to healthy unprocessed foods ) or food swamps (a plethora of fast food outlets) and 54 million Americans are food insecure (Ney, 2022). In addition, we and our parents have been programmed by the food industry advertising to eat the ultra- processed foods and may no longer know how to prepare healthy foods such as exemplified by a Mediterranean diet. Recent research by Bayles et al (2022) has shown that eating a Mediterranean diet improves depression significantly more than the befriending control group. In addition, highly processed foods and snacks are omnipresent, often addictive and more economical.
Remember that clients are individuals and almost all research findings are based upon group averages. Even when the data implies that a certain intervention is highly successful, there are always some participants for whom it is very beneficial and some for whom it is ineffective or even harmful. Thus, interventions need to be individualized for which there is usually only very limited data. In most cases, the original studies did not identify the characteristics of those who were highly successful or those who were unsuccessful. In addition, when working with specific individuals with ADHD, anxiety, depression, etc. there are multiple possible causes.
Before beginning specific clinical treatment such as neurofeedback and/or medication, we recommend the following:
- “Grandmother assessment” that includes and assessment of screen time, physical activity, outdoor sun exposure, sleep rhythm as outlined in Part 1 by Peper (2023). Then follow-up with a dietary assessment that investigates the prevalence of organic/non organic foods, ingestion of fast foods, ultra-processed foods, soft drinks, high simple carbohydrate and sugar, salty/sugary/fatty snacks, fruits, vegetables, and eating patterns (eating with family or by themselves in front of screens). Be sure to include an assessment of emotional reactivity and frequency of irritability and “hangryness”.
- If the assessment suggest low level of organic whole foods and predominance of ultra- refined foods, it may be possible that the person is deficient in vitamins and minerals. Recommend that the child is tested for the vitamin deficiencies. If vitamin deficiencies identified, recommend to supplement the diet with the necessary vitamins and mineral and encourage eating foods that naturally include these substances (Henry & CNS, 2023). If there is a high level of emotional reactivity and “hangryness,” a possible contributing factor could be hypoglycemic rebound from a high simple carbohydrate (sugar) intake or not eating breakfast combined with hyperventilation (Engel et al., 1947; Barr et al., 2019). Recommend eliminating simple carbohydrate breakfast and fast food snacks and substitute organic foods that include complex carbohydrates, protein, fats, vegetables and fruit. Be sure to eat breakfast.
- Implement “Grandmother Therapy”. Encourage the family and child to change their diet to eating a whide variety of organic foods (vegetables, fruits, some fish, meat and possibly dairy) and eliminate simple carbohydrates and sugars. This diet will tend to reduce nutritional deficits and may eliminate the need for supplements.
- Concurrent with the stabilization of the physiology begin psychophysiological treatment strategies such as neurofeedback biofeedback and cognitive behavior therapy.
Relevant blogs
Author Disclosure
Authors have no grants, financial interests, or conflicts to disclose.
References
Arnold, L, Lofthouse, N., & Hurt, E. (2012). Artificial food colors and attention-deficit/hyperactivity symptoms: conclusions to dye for. Neurotherapeutics, 9(3), 599-609. https://doi.org/10.1007/s13311-012-0133-x
Arab, A. & Mostafalou, S. (2022). Neurotoxicity of pesticides in the context of CNS chronic diseases. International Journal of Environmental Health Research, 32(12), 2718-2755. https://doi.org/10.1080/09603123.2021.1987396
Barr, E.A., Peper, E., & Swatzyna, R.J. (2019). Slouched Posture, Sleep Deprivation, and Mood Disorders: Interconnection and Modulation by Theta Brain Waves. NeuroRegulation, 6(4), 181–189. https://doi.org/10.15540/nr.6.4.181
Bayes. J., Schloss, J., Sibbritt, D. (2022). The effect of a Mediterranean diet on the symptoms of depression in young males (the “AMMEND: A Mediterranean Diet in MEN with Depression” study): a randomized controlled trial. Am J Clin Nutr. 116(2), 572-580. https://doi.org/10.1093/ajcn/nqac106
Bjørling-Poulsen, M., Andersen, H.R. & Grandjean, P. Potential developmental neurotoxicity of pesticides used in Europe. Environ Health 7, 50 (2008). https://doi.org/10.1186/1476-069X-7-50
Bommersbach, T.J., McKean, A.J., Olfson, M., Rhee, T.G. (2023). National Trends in Mental Health–Related Emergency Department Visits Among Youth, 2011-2020. JAMA, 329(17):1469–1477. https://doi.org/10.1001/jama.2023.4809
Bouchard, M.F., Bellinger, D.C., Wright, R.O., & Weisskopf, M.G. (2010). Attention-deficit/hyperactivity disorder and urinary metabolites of organophosphate pesticides. Pediatrics, 125(6), e1270-7. https://doi.org/10.1542/peds.2009-3058
Braghieri, L., Levy, R., & Makarin, A. (2022). Social Media and Mental Health (July 28, 2022). Available at SSRN: https://ssrn.com/abstract=3919760 or http://dx.doi.org/10.2139/ssrn.3919760
Cardenas, D. (2013). Let not thy food be confused with thy medicine: The Hippocratic misquotation. e-Spen Journal, 8(6), 3260-3262. https://doi.org/10.1016/j.clnme.2013.10.002
CDC, (2023). Quick Facts on the Risks of E-cigarettes for Kids, Teens, and Young Adults. CDC. Centers for Disease Control and Prevention. Accessed September 23, 2023. https://www.cdc.gov/tobacco/basic_information/e-cigarettes/Quick-Facts-on-the-Risks-of-E-cigarettes-for-Kids-Teens-and-Young-Adults.html
Chang, J.C., Su, K.P., Mondelli, V. et al. Omega-3 Polyunsaturated Fatty Acids in Youths with Attention Deficit Hyperactivity Disorder: a Systematic Review and Meta-Analysis of Clinical Trials and Biological Studies. Neuropsychopharmacol. 43, 534–545. https://doi.org/10.1038/npp.2017.160
Chhabra, R., Kolli, S., & Bauer, J.H. (2013). Organically Grown Food Provides Health Benefits to Drosophila melanogaster. PLoS ONE, 8(1): e52988. https://doi.org/10.1371/journal.pone.0052988
Davis, D. R., Epp, M. D., & Riordan, H. D. (2004). Changes in USDA food composition data for 43 garden crops, 1950 to 1999. Journal of the American College of Nutrition, 23(6), 669-682. https://doi.org/10.1080/07315724.2004.10719409
Derbyshire, E. (2017). Do Omega-3/6 Fatty Acids Have a Therapeutic Role in Children and Young People with ADHD? J Lipids. 6285218. https://doi.org/10.1155/2017/6285218
Del-Ponte, B., Quinte, G.C., Cruz, S., Grellert, M., & Santos, I. S. Dietary patterns and attention deficit/hyperactivity disorder (ADHD): A systematic review and meta-analysis. Journal of Affective Disorders, 252, 160-173. https://doi.org/10.1016/j.jad.2019.04.061
Durukan, İ., Kara, K., Almbaideen, M., Karaman, D., & Gül, H. (2018). Alexithymia, depression and anxiety in parents of children with neurodevelopmental disorder: Comparative study of autistic disorder, pervasive developmental disorder not otherwise specified and attention deficit-hyperactivity disorder. Pediatrics International, 60(3), 247–253. https://doi.org/10.1111/ped.13510
Effatpanah, M., Rezaei, M., Effatpanah, H., Effatpanah, Z., Varkaneh, H.K., Mousavi. S.M., Fatahi, S., Rinaldi, G., & Hashemi, R. (2019). Magnesium status and attention deficit hyperactivity disorder (ADHD): A meta-analysis. Psychiatry Res, 274, 228-234. https://doi.org/10.1016/j.psychres.2019.02.043
Engel, G.L., Ferris, E.B., & Logan, M. (1947). Hyperventilation; analysis of clinical symptomatology. Ann Intern Med, 27(5), 683-704. https://doi.org/10.7326/0003-4819-27-5-683
EPA. (2023). Glyphosate. United States Environmental Protection Agency. Accessed April 1, 2023. https://www.epa.gov/ingredients-used-pesticide-products/glyphosate
European Commission. (2023). EU legislation on MRLs.Food Safety. Assessed April 1, 2023. https://food.ec.europa.eu/plants/pesticides/maximum-residue-levels/eu-legislation-mrls_en#:~:text=A%20general%20default%20MRL%20of,e.g.%20babies%2C%20children%20and%20vegetarians
Faraone, S.V. & Larsson, H. (2019). Genetics of attention deficit hyperactivity disorder. Mol Psychiatry, 24(4), 562-575. https://doi.org/10.1038/s41380-018-0070-0
Fernandez-Cornejo, J. Nehring, R, Osteen, C., Wechsler, S., Martin, A., & Vialou, A. (2014). Pesticide use in the U.S. Agriculture: 21 Selected Crops, 1960-2008. Economic Information Bulletin Number 123, United State Department of Agriculture. https://www.ers.usda.gov/webdocs/publications/43854/46734_eib124.pdf
Gomes, G. N., Vidal, F. N., Khandpur. N., et al. (2023). Association Between Consumption of Ultraprocessed Foods and Cognitive Decline. JAMA Neurol, 80(2),142–150. https://doi.org/10.1001/jamaneurol.2022.4397
Hemamy, M., Heidari-Beni, M., Askari, G., Karahmadi, M., & Maracy, M. (2020). Effect of Vitamin D and Magnesium Supplementation on Behavior Problems in Children with Attention-Deficit Hyperactivity Disorder. Int J Prev Med, 11(1), 4. https://doi.org/10.4103/ijpvm.IJPVM_546_17
Henry, K. (2023). An Integrative Medicine Approach to ADHD. Rupa Health. Accessed September 30, 2023. https://www.rupahealth.com/post/an-integrative-medicine-approach-to-adhd
Henry, K. & CNS, L.A. (2023). Natural treatments for ADHD. Webinar Presentation by IntegrativePractitioner.com and sponsored by Rupa Health, June 6, 2023 https://divcom-events.webex.com/recordingservice/sites/divcom-events/recording/e29cefcae6c1103bb7f3aa780efee435/playback?
Hemamy, M., Pahlavani, N., Amanollahi, A. et al. (2021). The effect of vitamin D and magnesium supplementation on the mental health status of attention-deficit hyperactive children: a randomized controlled trial. BMC Pediatr, 21, 178. https://doi.org/10.1186/s12887-021-02631-1
Konofal, E., Lecendreux, M., Arnulf, I., & Mouren, M. (2004). Iron Deficiency in Children With Attention-Deficit/Hyperactivity Disorder. Arch Pediatr Adolesc Med, 158(12), 1113–1115. https://doi.org/10.1001/archpedi.158.12.1113
Kotsi, E., Kotsi, E. & Perrea, D.N. (2019). Vitamin D levels in children and adolescents with attention-deficit hyperactivity disorder (ADHD): a meta-analysis. ADHD Atten Def Hyp Disord, 11, 221–232. https://doi.org/10.1007/s12402-018-0276-7
LaChance, L.R. & Ramsey, D. (2018). Antidepressant foods: An evidence-based nutrient profiling system for depression. World J Psychiatr, 8(3): 97-104. World J Psychiatr., 8(3): 97-104. https://doi.org/10.5498/wjp.v8.i3.97
Landaas, E.T., Aarsland, T.I., Ulvik, A., Halmøy, A., Ueland. P.M., & Haavik, J. (20166). Vitamin levels in adults with ADHD. BJPsych Open, 2(6), 377-384. https://doi.org/10.1192/bjpo.bp.116.003491
Linday, L.A. (2010). Cod liver oil, young children, and upper respiratory tract infections. J Am Coll Nutr, 29(6), 559-62. https://doi.org/10.1080/07315724.2010.10719894
Leoci, R. & Ruberti, M. (2021) Pesticides: An Overview of the Current Health Problems of Their Use. Journal of Geoscience and Environment Protection, 9, 1-20. https://doi.org/10.4236/gep.2021.98001
Lustig, R.H. (2021). Metaboical: The lure and the lies of processed food, nutrition, and modern medicine. New York: Harper Wave. https://www.amazon.com/Metabolical-processed-poisons-people-planet/dp/1529350077
MacInerney, E. K., Swatzyna, R. J., Roark, A. J., Gonzalez, B. C., & Kozlowski, G. P. (2017). Breakfast choices influence brainwave activity: Single case study of a 12-year-old female. NeuroRegulation, 4(1), 56–62. https://doi.org/10.15540/nr.4.1.56
McCann, D., Barrett, A., Cooper, A., Crumpler, D., Dalen, L., Grimshaw, K., et al. (2007). Food additives and hyperactive behavior in 3-year old and 8/9-year-old children in the community: a randomized, double-blinded, placebo-controlled trial. Lancet, 370(9598), 1560-1567. https://doi.org/10.1016/S0140-6736(07)61306-3
Mengying, L.I, Fallin, A, D., Riley,A., Landa, R., Walker, S.O., Silverstein, M., Caruso, D., et al. (2016). The Association of Maternal Obesity and Diabetes With Autism and Other Developmental Disabilities. Pediatrics, 137(2), e20152206. https://doi.org/10.1542/peds.2015-2206
Mousain-Bosc, M., Roche, M., Polge, A., Pradal-Prat, D., Rapin, J., & Bali, J.P. (2006). Improvement of neurobehavioral disorders in children supplemented with magnesium-vitamin B6. I. Attention deficit hyperactivity disorders. Magnes Res. 19(1), 46-52. https://pubmed.ncbi.nlm.nih.gov/16846100/#:~:text=In%20almost%20all%20cases%20of,increase%20in%20Erc%2DMg%20values.
Ney, J. (2022). Food Deserts and Inequality. Social Policy Data Lab. Updated: Jan 24, 2022. Accessed September, 23, 2023. https://www.socialpolicylab.org/post/grow-your-blog-community
Peper, E. (2023a). Reflections on the increase in Autism, ADHD, anxiety and depression: Part 1-bonding, screen time, and circadian rhythms. the peperperspective July 2, 2023. Accessed august 8, 2024, https://peperperspective.com/2023/07/04/reflections-on-the-increase-in-autism-adhd-anxiety-and-depression-part-1-bonding-screen-time-and-circadian-rhythms/
Peper, E. (2023b). Reflections on the increase in Autism, ADHD, anxiety and depression: Part 1-bonding, screen time, and circadian rhythms. NeuroRegulation, 10(2), 134-138. https://doi.org/10.15540/nr.10.2.134
Pollan, M. (2006). Omnivore’s Dilemma: A Natural History of Four Meals and Food Rules. New York Penguin Press. https://www.amazon.com/Omnivores-Dilemma-Natural-History-Meals/dp/1594200823/ref=tmm_hrd_swatch_0?_
Pollan, M. (2011). Food rules. New York Penguin Press. https://www.amazon.com/Food-Rules-Eaters-Michael-Pollan/dp/B00VSBILFG/ref=tmm_hrd_swatch_0?
Pongpitakdamrong, A., Chirdkiatgumchai, V., Ruangdaraganon, N., Roongpraiwan, R., Sirachainan, N., Soongprasit, M., & Udomsubpayakul, U. (2022). Effect of Iron Supplementation in Children with Attention-Deficit/Hyperactivity Disorder and Iron Deficiency: A Randomized Controlled Trial. Journal of Developmental & Behavioral Pediatrics, 43(2), 80-86., https://doi.org/10.1097/DBP.0000000000000993
Porto, A. & Abu-Alreesh, S. (2022). Vitamin D for babies, children & adolescents. Health Living. Healthychildren.org. Accessed September 24, 2023. https://www.healthychildren.org/English/healthy-living/nutrition/Pages/vitamin-d-on-the-double.aspx#
Poudineh, M., Parvin, S., Omidali, M., Nikzad, F., Mohammadyari, F., Sadeghi Poor Ranjbar, F., F., Nanbakhsh, S., & Olangian-Tehrani, S. (2023). The Effects of Vitamin Therapy on ASD and ADHD: A Narrative Review. CNS & Neurological Disorders – Drug Targets (Formerly Current Drug Targets – CNS & Neurological Disorders), (22), 5, 2023, 711-735. https://doi.org/10.2174/1871527321666220517205813
Puigbò, P., Leino, L. I., Rainio, M. J., Saikkonen, K., Saloniemi, I., & Helander, M. (2022). Does Glyphosate Affect the Human Microbiota?. Life, 12(5), 707. https://doi.org/10.3390/life12050707
Ríos-Hernández, A., Alda, J.A., Farran-Codina, A., Ferreira-García, E., & Izquierdo-Pulido, M. (2017). The Mediterranean Diet and ADHD in Children and Adolescents. Pediatrics, 139(2):e20162027. https://doi.org/10.1542/peds.2016-2027
Ryu, S.A., Choi, Y.J., An, H., Kwon, H.J., Ha, M., Hong, Y.C., Hong, S.J., & Hwang, H.J. (2022). Associations between Dietary Intake and Attention Deficit Hyperactivity Disorder (ADHD) Scores by Repeated Measurements in School-Age Children. Nutrients, 14(14), 2919. https://doi.org/10.3390/nu14142919
Sagiv, S.K., Kogut, K., Harley, K., Bradman, A., Morga, N., & Eskenazi, B. (2021). Gestational Exposure to Organophosphate Pesticides and Longitudinally Assessed Behaviors Related to Attention-Deficit/Hyperactivity Disorder and Executive Function, American Journal of Epidemiology, 190(11), 2420–2431. https://doi.org/10.1093/aje/kwab173
Swanson, N.L., Leu, A., Abrahamson, J., & Wallet, B. (2014). Genetically engineered crops, glyphosate and the deterioration of health in the United States of America. Journal of Organic Systems, 9(2), 6-17. https://www.organic-systems.org/journal/92/JOS_Volume-9_Number-2_Nov_2014-Swanson-et-al.pdf
Swatzyna, R. J., Boutros, N. N., Genovese, A. C., MacInerney, E. K., Roark, A. J., & Kozlowski, G. P. (2018). Electroencephalogram (EEG) for children with autism spectrum disorder: Evidential considerations for routine screening. European Child & Adolescent Psychiatry, 28(5), 615–624. https://doi.org/10.1007/s00787-018-1225-x
Taleb, N. N. (2014). Antifragile: Things That Gain from Disorder (Incerto). New York: Random House Publishing Group. https://www.amazon.com/Antifragile-Things-That-Disorder-Incerto/dp/0812979680/ref=tmm_pap_swatch_0
Tohidi, S., Bidabadi, E., Khosousi, M.J., Amoukhteh, M., Kousha, M., Mashouf, P., Shahraki, T. (2021). Effects of Iron Supplementation on Attention Deficit Hyperactivity Disorder in Children Treated with Methylphenidate. Clin Psychopharmacol Neurosci, 19(4), 712-720. https://doi.org/10.9758/cpn.2021.19.4.712
Unal, D. Çelebi, F., Bildik,H.N., Koyuncu, A., & Karahan, S. (2019). Vitamin B12 and haemoglobin levels may be related with ADHD symptoms: a study in Turkish children with ADHD, Psychiatry and Clinical Psychopharmacology, 29(4), 515-519. https://doi.org/10.1080/24750573.2018.1459005
USDA. (2019). Fish oil, cod liver. FoodData Central. USDA U.S> Department of Agriculture. Published 4/1/2019. Accessed September 24, 2024. https://fdc.nal.usda.gov/fdc-app.html#/food-details/173577/nutrients
Van Tulleken, C. (2023). Ultra-Processed People. The Science Behind Food That Isn’t Food. New York: W.W. Norton & Company. https://www.amazon.com/Ultra-Processed-People-Science-Behind-Food/dp/1324036729/ref=asc_df_1324036729/?
Wahab, S., Muzammil, K., Nasir, N., Khan, M.S., Ahmad, M.F., Khalid, M., Ahmad, W., Dawria, A., Reddy, L.K.V., & Busayli, A.M. (2022). Advancement and New Trends in Analysis of Pesticide Residues in Food: A Comprehensive Review. Plants (Basel), 11(9), 1106. https://doi.org/10.3390/plants11091106
Wang. Y., Huang, L., Zhang, L., Qu, Y., & Mu, D. (2017). Iron Status in Attention-Deficit/Hyperactivity Disorder: A Systematic Review and Meta-Analysis. PLoS One, 12(1):e0169145. https://doi.org/10.1371/journal.pone.0169145
Wilson, L. (2015). Mothers, beware: Your lifestyle choices will even affect your grandkids.
News Corp Australia Network. Accessed Jun 24, 2024. https://www.news.com.au/lifestyle/parenting/kids/mothers-beware-your-lifestyle-choices-will-even-affect-your-grandkids/news-story/3f326f457546cfb32af5c409f335fb56
Woo, H.D.,; Kim, D.W., Hong, Y.-S., Kim, Y.-M.,Seo, J.-H.,; Choe, B.M., Park, J.H.,; Kang, J.-W., Yoo, J.-H.,; Chueh, H.W., et al. (2014). Dietary Patterns in Children with Attention Deficit/Hyperactivity Disorder (ADHD). Nutrients, 6, 1539-1553. https://doi.org/10.3390/nu6041539
Zhong, C., Tessing, J., Lee, B.K., Lyall, K. Maternal Dietary Factors and the Risk of Autism Spectrum Disorders: A Systematic Review of Existing Evidence. Autism Res,13(10),1634-1658. https://doi.org/10.1002/aur.2402
Reduce the risk for colds and flu and superb science podcasts
Posted: January 24, 2024 Filed under: attention, behavior, education, Evolutionary perspective, Exercise/movement, healing, health, Nutrition/diet, self-healing, stress management, Uncategorized, vision | Tags: colds, darkness, flu, influenza, light 2 Comments
What can we do to reduce the risk of catching a cold or the flu? It is very challenging to make sense out of all the recommendations found on internet and the many different media site such as X(Twitter), Facebook, Instagram, or TikTok. The following podcasts are great sources that examine different topics that can affect health. They are in-depth presentations with superb scientific reasoning.
Huberman Lab podcasts discusses science and science based tools for everyday life. https://www.hubermanlab.com/podcast. Select your episode and they are great to listen to on your cellphone.
THE PODCAST episode, How to prevent and treat cold and flu, is outstanding. Skip the long sponsor introductdion and start listening at the 6 minute point. In this podcast, Professor Andrew Huberman describes behavior, nutrition and supplementation-based tools supported by peer-reviewed research to enhance immune system function and better combat colds and flu. I also dispel common myths about how the cold and flu are transmitted and when you and those around you are contagious. I explain if common preventatives and treatments such as vitamin C, zinc, vitamin D and echinacea work. I also highlight other compounds known to reduce contracting and duration of colds and flu. I discuss how to use exercise and sauna to bolster the immune response. This episode will help listeners understand how to reduce the chances of catching a cold or flu and help people recover more quickly from and prevent the spread of colds and flu.
PODCAST, ScienceVS, is an outstanding podcast series that takes on fads, trends, and opinionated mob to find out what’s fact, what’s not, and what’s somewhere in between. Select your episode and listen.
Link: https://gimletmedia.com/shows/science-vs/episodes#show-tab-picker

PODCAST episode, The Journal club podcast and Youtube, presentation from Huberman Lab is a example of outstanding scientific reasoning. In this presentation, Professor Andrew Huberman and Dr. Peter Attia (author of Outlive: The Science and Art of Longevity) discuss two peer-reviewed scientific papers in-depth. The first discussion explores the role of bright light exposure during the day and dark exposure during the night and its relationship to mental health. The second paper explores a novel class of immunotherapy treatments to combat cancer.
Rethink the monies spent on cancer screening tests
Posted: November 24, 2023 Filed under: behavior, cancer, Evolutionary perspective, healing, health, Nutrition/diet, self-healing | Tags: breast canceer, Cancer screening, environmental toxins, immune competence, Life style, lifestyle modification, mammography, organic foods, overdiagnosis 3 CommentsErik Peper, PhD and Richard Harvey, PhD

Adapted from: Peper, E. & Harvey, R. (2024). Rethinking the monies spent on cancer screening tests. Townsend e-Letter, Townsend Letters. The Examiner of Alternative Medicine, May 18, 2024. https://www.townsendletter.com/e-letter-34-are-we-reducing-cancer-or-just-looking-for-it/
Abstract
While cancer screening tests are commonly promoted for early detection and treatment, evidence increasingly suggests that widespread screening of asymptomatic individuals may not significantly extend lifespan and could contribute to overdiagnosis, overtreatment, and harm. Although billions are spent annually on screenings—$40 billion for colon, $15 billion for breast, and $4 billion for prostate cancer—some of these money might be more effectively invested in lifestyle interventions that reduce cancer risk and improve longevity. Meta-analyses indicate that only sigmoidoscopy for colorectal cancer shows a clear benefit in extending life, while other common screenings (e.g., mammography, PSA, FOBT) show minimal or no effect on overall mortality. Interestingly, breast cancer mortality declines have occurred in similarly European countries that delayed screening implementation as compared to countries that started screen earlier. This suggests that other contributing factors such as improved lifestyle, nutrition, and environmental changes may be the major factor in the reduction of breast cancer. We recommend shifting from profit-driven, generalized screening toward personalized, risk-adjusted methods using multi-omics technology and preventative lifestyle patterns. More critically, the focus should be prevention through diet, physical activity, stress management, sleep hygiene, environmental protections, and social support; since, it is estimated that 70 percent of all cancers are related to diet and environmental factors. Thus, resources need to be allocated toward empowering individuals and communities to adopt health-promoting behaviors and thereby reduce cancer incidence.
Keywords: cancer screening, overdiagnosis, lifestyle modification, preventive health,
immune competence
Cancer screening tests are based upon the rational that early detection of fatal cancers enables earlier and more effective treatments (Kowalski, 2021), however, there is some controversy. Early screening may increase the risk of over diagnosis, treating false positives (people who did not have the cancer but the test indicates they have cancer) and potentially fatal treatment of cancers that would never progress to increase morbidity or mortality (Kowalski, 2021).
Today about $40 billion spent on colon cancer screening, $15 billion spent on breast cancer screening, and $4 billion spent on prostate cancer screening annually (CSPH, 2021). A question is raised whether the billions and billions of dollars spent on screening asymptomatic participants would be more wisely spent on promoting and supporting life style changes that reduce cancer risks and actually extend life span? That cancer screening is expensive does not mean no one should be screened. Instead, the argument is that the majority of healthcare dollars could be spent on health promotion practices and reserving screening for those people who are at highest risk for developing cancers.
What is the evidence that screening prolongs life?
Cancer screening tests appear correlated with preventing deaths since deaths due to cancers in the USA have decreased by about 28% from 1999 to 2020 (CDC, 2023a). Although cancer causes many of the deaths in the USA, overall life expectancy has increased by less than 1% from 1999 to 2020. If cancer screening were more effective, the life expectancy should have increased more because cancer is the second leading cause of death (CDC, 2023b). Consider also that deaths due to cancers may be coincident and or comorbid with other circumstances. For example, during the last four years, overall life expectancy in the USA has precipitously declined in part due to other causes of death such as the COVID pandemic and opioid overdose epidemic (Lewis, 2022). Decline in life expectancy in the USA has many contributing factors, including the ‘harms’ associated with cancer screening procedures. For example, perforations during colon cancer screening can lead to internal bleeding, or complications related to surgeries, radiotherapies or chemotherapies. Bretthauer et al., (2023) commented: “A cancer screening test may reduce cancer-specific mortality but fail to increase longevity if the harms for some individuals outweigh the benefits for others or if cancer-specific deaths are replaced by deaths from competing cause” (p. 1197).
Bretthauer et al. (2023) conducted a systematic review and meta-analysis of 18 long-term randomized clinical trials involving 2.1 million Individuals with more than nine years of follow-up reporting on all-cause mortality. They reported that“…this meta-analysis suggest that current evidence does not substantiate the claim that common cancer screening tests save lives by extending lifetime, except possibly for colorectal cancer screening with sigmoidoscopy.”
Following is a summary of Bretthauer et al. (2023) findings:
- The only cancer screening with a significant lifetime gain (approximately 3 months) was sigmoidoscopy.
- There was no significant difference between harms of screening and benefits of screening for:
- mammography
- prostate cancer screening
- FOBT (fecal occult blood test) screening every year or every other year
- lung cancer screening Pap test cytology for cervical cancer screening, no randomized clinical trials with cancer-specific or all-cause mortality end points and long term follow-up were identified.
Potential for loss or harm (e.g., iatrogenic and nosocomial) versus potential for benefit and extended life
More than 35 years ago a significant decrease in breast cancer mortality was observed after mammography was implemented. The correlation suggested a causal relationship that screening reduced mortality (Fracheboud, 2004). This correlation made logical sense since the breast cancer screening test identified cancers early which could then be treated and thereby would result in a decrease in mortality.
How much money is spent on screening that may correlate with unintended harms?
The annual total expenditure for cancer screening is estimated to be between $40-$50 billion annually (CSPH, 2021). Below are some of the estimated expenditures for common tests other than colorectal cancer screening, which arguably is costly; however, has potential benefits that outweigh potential harms.
- $10.37-13.94 billion for mammography to screen 50% of eligible women (Badal et al, 2023).
- $2-4 billion for prostate cancer (Ma et al., 2014)
- $1-2 billion for lung cancer (Taylor et al., 2022)
What is the correlation between initiation of mammography and decrease in breast cancer mortality?
The conclusion that mammography reduced breast cancer mortality was based upon studies without control groups; however, this relationship could be causal or synchronistic. The ambiguity of correlation or causation was resolved with the use of natural experimental control groups. Some European countries began screening 10 years earlier than other countries. Using statistical techniques such as propensity score matching when comparing the data from countries that initiated mammography screening early (Netherlands, Sweden and Northern Ireland) to countries that started screening 10 year later (Belgium, Norway and Republic of Ireland), the effectiveness of screening could be compared.
The comparisons showed no difference in the decrease of breast cancer mortality in countries that initiated breast cancer screening early or late. For example, there was no difference in the decrease of breast cancer mortality rates of women who lived in the Netherlands that started screening early versus those who lived in Belgium that began screening 10 years later, as is shown Figure 1 (Autier et al, 2011).

Figure 1. No difference in age adjust breast cancer mortality between the two adjacent countries even though breast cancer screening began ten years earlier in the Netherlands than in Belgium (graph reproduced from Autier et al, 2011).
The observations are similar when comparing neighboring countries: Sweden (early screening) to Norway (late screening) as well as Northern Ireland, UK (early screening) compared to the Republic of Ireland (late screening). The systematic comparisons showed that screening did not account for the decrease in breast cancer mortality. To what extent could the decrease in mortality be related to other factors such as better prenatal and early childhood diet and life style, improved nutrition, reduction in environmental pollutants, and other unidentified life style and environmental factors which improve immune competence?
A simplistic model to reduce the risk of cancers is described in the following equation (Gorter & Peper, 2011).

Cancer risk can be reduced, arguably by influencing risk factors that contribute to cancers as well as increasing factors to enhance immune competence. In the simple model above, ‘Cancer burden’ refers to the set of exposures that increase the odds of cancer formations. Categories include exposures to oncoviruses, environmental exposures (e.g., ionizing radiation, carcinogenic chemicals) as well as genetic (e.g., chromosomal aberrations, replication errors) and epigenetic factors (e.g., lifestyle categories related to eating, exercising, sleeping, and relaxing). In the model above, ‘Immune competence’ refers to a set of categories of immune functioning related to DNA repair, orderly cell death (i.e., processes of apoptosis), expected autophagy, as well as ‘metabolic rewiring,’ also called cellular energetics, that would allow the body to be able to reduce manage cancers from progressing (Fouad & Aanei, 2017) .
How do we examine the cancer burden/immune competence relationship?
Schmutzler et al., (2022) have suggested personalized and precision-medicine risk-adjusted cancer screening incorporating “… high-throughput “multi-omics” technologies comprising, among others, genomics, transcriptomics, and proteomics, which have led to the discovery of new molecular risk factors that seem to interact with each other and with non-genetic risk factors in a multiplicative manner.” The argument is that ‘profit-centered’ medicine could incorporate ‘multi-omics’ into risk-adjusted cancer screening as a way to reduce potential loss or harm due to other cancer screening procedures. Rather than simply screening for cancers using currently invasive or toxic procedures which may do more harm than good, consider more nuanced screening tests aimed at the so-called ‘hallmarks of cancer?’ For example, Hanahan (2022) suggests some technical targets for the multi-omics technologies. The following are some of the precision screening tests possible topersonalized medicine of 14 factors or processes related to:
- cells evading growth suppression
- non-mutational epigenetic reprogramming
- avoiding immune destruction
- enabling replicative immortality
- tumor-promoting inflammation
- polymorphic microbiomes
- activating invasion and metastasis
- inducing or accessing vasculature formation/angiogenesis
- cellular senescence
- genome instability and mutation
- resisting cell death
- deregulating cellular metabolism
- unlocking phenotypic plasticity
- sustaining proliferative signaling
Of the listed categories above, ‘phenotypic plasticity’ (cf. Feinberg, 2007; Gupta et al., 2019) suggests that lifestyle behaviors and environmental exposures play a role in cancer progression and regression.
Lifestyle and environmental factors can contribute to the development of cancers.
The 2008-2009 report from the President’s Cancer Panel appraised the National Cancer Program in accordance with the National Cancer Act of 1971 stated (Reuben, 2010):
“We have grossly underestimated the link between environmental toxins, plastics, chemicals, and cancer risk. It is estimated that 70 percent of all cancers were related to diet and environment “
Multiple research studies have shown that a healthy life style pattern is associated with decreased cancer risks and increased longevity. Lifestyle factors that have been documented to increase cancer risks in the United Kingdom (UK) as shown in figure 2.

Figure 2. Percentages of cancer cases in the UK attributable to different exposures. Adapted from Brown et al., 2018 and reproduced by permission from Key et al., 2020.
Similar findings have been reported by Song et al. (2016) from the long term follow-up of 126901 adult health care professionals. People who never smoked, drank no alcohol or moderate alcohol (< 1 drink/d for women; < 2 drinks/d for men}, had a body-mass index (BMI) of at least 18.5 but lower than 27.5, did weekly aerobic physical activity of at least 75 vigorous-intensity minutes or 150 150 moderate-intensity minutes compared to those who smoked, drank, had high BMI and did not exercise had nearly half the cancer death rate. Song et al (2016) concludes:
“…about 20% to 40% of carcinoma cases and about half of carcinoma deaths can be potentially prevented through lifestyle modification. Not surprisingly, these figures increased to 40% to 70% when assessed with regard to the population of US whites which has a much worse lifestyle pattern than other cohorts. Notably, approximately 80% to 90% of lung cancer deaths can be avoided if Americans adopted the lifestyle of the low-risk group, mainly by quitting smoking. For other cancers, a range of 10% to 70% of deaths can be prevented. These results provide strong support for the importance of environmental factors in cancer risk and reinforce the enormous potential of primary prevention for cancer control.”
Said another way, primary prevention should remain a priority for cancer control.
Given that many cancers are related to diet, environment and lifestyle, it is estimated that 50% of all cancers and cancer deaths could be prevented by modifying personal behavior. Thus, the monies spent on screening or even developing new treatments could better be spent on prevention along with implementing programs that promote a healthier environment, diet and personal behavior (AACR, 2011).
What can be done? Addressing systems not symptoms
From a ‘systems perspective,’ the first step is to reduce the cancer burden and carcinogenic agents that occur in our environment such environmental pollution (Turner et al., 2022). In many cases, governmental regulations that reduce cancer risk factors have been weakened, delayed, and contested for years through industry’s lobbying. It often takes more than 30 years after risk factors have been observed and documented before government regulations are successfully implemented, as exemplified in the battle over tobacco or, air pollution regulations related to particulates from burning fossil fuels (Stratton et al, 2001).
Sadly, we cannot depend upon governments or industries to implement regulations known to reduce cancer risks. More within our control is implementing lifestyle changes that enhance immune competence and promote health.
Implement a healthy life style that enhances immune competence and, supports health and well-being
Paraphrasing a trope of what some physicians may state: ‘Take two pills, and call me in the morning. Oh, and eat well, exercise, and get good rest.’ Broadly stated, the following are some controllable lifestyle behaviors that can decrease cancer risks and promotes health. Implementing environmental and lifestyle changes are very challenging because they are highly related to socio economic factors, cultural factors, industry push for profits over health, and self-care challenges since there are no immediate results experienced by behavior and lifestyle changes.
In many cases, the effects of harmful life-style and environment factors are only observed twenty or more years later (e.g., diabetes, lung cancer, cirrhosis of the liver). The individual does not experience immediate benefits of lifestyle changes thus it is more challenging to know that your healthy life style has an effect. The process is even more complex because in most cases it is not a single factor but the interaction of multiple factors (genetics, lifestyle, and environment). The complexity of causality so often conflicts with the simplistic research studies to identify only one isolated risk factor. Instead of waiting for the definitive governmental guidelines and regulations, adopt a ‘precautionary principle’ which means do not take an action when there is uncertainty about its potential harm (Goldstein, 2001). Do not wait for screening; instead, take charge of your health and implement as many of the following behaviors and strategies to enhance immune competence and thereby reduce cancer risks.
Eat organic foods, especially vegetable and fruits.
Many studies have suggested that eating organic foods and in particular more fruits and vegetable such as a Mediterranean diet is associated with increased health and longevity. Similarly, people who eat do not eat highly-processed or ultra-processed foods have better health status (Van Tulleken, 2023). For example, In the large prospective study of 68, 946 participants, adults who consumed the most organic fruits, vegetables, dairy products, meat and other foods had 25% fewer cancers when compared with adults who never ate organic food (Baudry et al., 2018; Rabin, 2018). Similarly, many studies have reported that those who adhere consistently to a Mediterranean diet have a significantly lower incidence of chronic diseases (such as cardiovascular diseases, diabetes, etc.) and cancers compared to those who do not adhere to a Mediterranean diet (Mentella et al., 2019).
Reduce environmental pollution exposure
Air pollution and the exposure to airborne carcinogens are a significant risk factor for cancers as illustrated by the increased cancer rates among smokers. In the USA, the reduction of smoking has significantly decreased the lung cancer deaths (US Department of Health and Human Services, 2014).
Increase movement and exercise
Many studies have documented that people who exercise regularly and are otherwise non–sedentary but are active their entire lives have the lowest risk for breast cancers and colon cancers. Women who exercise 3 hours a week or more have a 30-40% lower risk of developing breast cancer (NIH NCI, 2023). The NIH National Cancer Institute summary concludes that exercises also significantly benefited the following cancer survivors (NIH NCI, 2023):
- Breast cancer: In a 2019 systematic review and meta-analysis of observational studies, breast cancer survivors who were the most physically active had a 42% lower risk of death from any cause and a 40% lower risk of death from breast cancer than those who were the least physically active (Spei et al, 2019).
- Colorectal cancer: Evidence from multiple epidemiologic studies suggests that physical activity after a colorectal cancer diagnosis is associated with a 30% lower risk of death from colorectal cancer and a 38% lower risk of death from any cause (Patel et al., 2019).
- Prostate cancer: Limited evidence from a few epidemiologic studies suggests that physical activity after a prostate cancer diagnosis is associated with a 33% lower risk of death from prostate cancer and a 45% lower risk of death from any cause ((Patel et al., 2019).
- Implement stress management.
Chronic stress may reduce immune competence and increase the risk of cancers as well as hinders healing from cancer treatments (Dai et al., 2020). The results of numerous studies have shown that implementing stress management spractices uch as Cognitive-behavioral stress management (CBSM) improves mood and lowers distress during treatment and, is also associated with longer survival compared to control groups in the 8-15 year follow up (Stagl et al., 2015).
Respect your biological rhythm.
The International Agency for Research on Cancer (IARC) reports that, when the human circadian clock is disrupted, the likelihood of developing cancers, including lung cancers, intestinal cancers, and breast cancers, dramatically increases (Huang, et al., 2023). Go to bed at the same time and, have about 8 hours of sleep. As much as possible avoid night shifts at work along with frequent jet lag as that highly disrupts the circadian rhythm.
Increase social connections and be part of a social community
Absence of social support, feeling lonely and socially isolated tends reduces immune competence and increases cancer mortality risk while having more social support satisfaction is associated with lower mortality risks (Salazaor et al., 2023; Boen et al., 2018). Meta-analysis of 148 studies (308,849 participants) found that that on the average there is a 50% increased likelihood of survival for participants with stronger social relationships (Holt-Lunstad et al., 2010).
Live a life with meaning and purpose
Having meaning and purpose make each moment worth living and may contribute to improving immune function and possible cancer survival (LeShan, 1994; Rosenbaum & Rosenbaum, 2023).
Summary
The research suggests that cancer screening does not extend life span unless specifically performed for certain diagnostic purposes or, with individuals who are at high risk of developing cancers (e.g., have a genetic predisposition). Implementing self-care health behaviors that have been identified to promote health and increase lifespan. Implementing health behaviors is challenging since there is limited governmental and corporate support. Thus, take charge and implement a holistic self-care lifestyle that reduces cancer risk factors and supports health.
See also the following blogs:
References
AACR. (2011). AACR Cancer Progress Report 2011. American Association for Cancer Research. http://www.aacr.org/Uploads/DocumentRepository/2011CPR/2011_AACR_CPR_Text_web.pdf
American Cancer Society. (2021). History of ACS Recommendations for the Early Detection of Cancer in People Without Symptoms. Accessed November 11, 2023. https://www.cancer.org/health-care-professionals/american-cancer-society-prevention-early-detection-guidelines/overview/chronological-history-of-acs-recommendations.html
Autier, P., Boniol, M., Gavin, A,, & Vatten, L.J. (2011) Breast cancer mortality in neighbouring European countries with different levels of screening but similar access to treatment: trend analysis of WHO mortality database. BMJ. 343, d4411. https://doi.org/10.1136/bmj.d4411
Badal., K., Staib, J., Tice,J., Kim, M-O., Eklund, M., DaCosta Byfield, S., Catlett,K., Wilson,L., et al, (2023). Cost of breast cancer screening in the USA: Comparison of current practice, advocated guidelines, and a personalized risk-based approach. Journal of Clinical Oncology, 41: 16_suppl, 3 18917 :16_suppl, e18917. https://doi.org/10.1200/JCO.2023.41.16_suppl.e18917
Baudry, J., Assmann, K.E., Touvier, M., et al. (2018). Association of Frequency of Organic Food Consumption With Cancer Risk: Findings From the NutriNet-Santé Prospective Cohort Study. JAMA Intern Med, 178(12), 1597–1606. https://doi.org/10.1001/jamainternmed.2018.4357
Boen, C.E., Barrow, D..A, Bensen, J.T., Farnan, L., Gerstel, A., Hendrix, L.H., Yang, Y.C. (2018). Social Relationships, Inflammation, and Cancer Survival. Cancer. Epidemiol Biomarkers Prev, 27(5), 541-549. https://doi.org/10.1158/1055-9965.EPI-17-0836
Bretthauer M, Wieszczy P, Løberg M, et al. (2023). Estimated Lifetime Gained With Cancer Screening Tests: A Meta-Analysis of Randomized Clinical Trials. JAMA Intern Med. 183(11),1196–1203. https://doi.org/10.1001/jamainternmed.2023.3798Brown, K.F., Rumgay, H., Dunlop, C. et al. (2018). The fraction of cancer attributable to modifiable risk factors in England, Wales, Scotland, Northern Ireland, and the United Kingdom in 2015. Br J Cancer, 118, 1130–1141. https://doi.org/10.1038/s41416-018-0029-6
CDC. (2023a). U.S. Cancer Statistics Working Group. U.S. Cancer Statistics Data Visualizations Tool, based on 2022 submission data (1999-2020): U.S. Department of Health and Human Services, Centers for Disease Control and Prevention and National Cancer Institute; released in November 2023. https://www.cdc.gov/cancer/dataviz
CDC. (2023b). Leading Causes of Death. National Center for health statistics, Centers for disease control and prevention. Accessed November 20, 2023. https://www.cdc.gov/nchs/fastats/leading-causes-of-death.htm
CSPH. (2021). Estimating annual expenditures for cancer screening in the United States. Center for Surgery and Public Health. Assessed November 14, 2023. https://csph.brighamandwomens.org/wp-content/uploads/2021/12/Estimating-Annual-Expenditures-for-Cancer-Screening-in-the-United-States.pdf
Dai, S., Mo, Y., Wang, Y., Xiang, B., Liao, Q., Zhou, M., Li, X., Li, Y., Xiong. W., Li, G., Guo, C., & Zeng, Z. (2020). Chronic Stress Promotes Cancer Development. Front Oncol. 10, 1492. https://doi.org/10.3389/fonc.2020.01492
Feinberg, A. P. (2007). Phenotypic plasticity and the epigenetics of human disease. Nature, 447(7143), 433-440. https://doi.org/10.1038/nature05919
Fouad, Y. A., & Aanei, C. (2017). Revisiting the hallmarks of cancer. American journal of cancer research, 7(5), 1016. https://pubmed.ncbi.nlm.nih.gov/28560055/
Fracheboud, J. et al. (2004). Decreased rates of advanced breast cancer due to mammography screening in The Netherlands, British Journal of Cancer (2004) 91, 861–867. https://doi,org/10.1038/sj.bjc.6602075
Goldstein, B.D. (2001). The precautionary principle also applies to public health actions. Am J Public Health, 91(9),1358-61. https://doi.org/10.2105/ajph.91.9.1358
Gorter, R. & Peper, E. (2011). Fighting Cancer-A None Toxic Approach to Treatment. Berkeley: North Atlantic/New York: Random House. https://www.amazon.com/Fighting-Cancer-Nontoxic-Approach-Treatment/dp/1583942483
Gupta, P. B., Pastushenko, I., Skibinski, A., Blanpain, C., & Kuperwasser, C. (2019). Phenotypic plasticity: driver of cancer initiation, progression, and therapy resistance. Cell Stem Cell, 24(1), 65-78. https://doi.org/10.1016/j.stem.2018.11.011
Hanahan, Douglas. (2022): Hallmarks of cancer: new dimensions. Cancer discovery, 12(1), 31-46. https://doi.org/10.1158/2159-8290.CD-21-1059
Holt-Lunstad, J., Smith, T.B., & Layton, J.B. (2010). Social Relationships and Mortality Risk: A Meta-analytic Review, PLoS Med 7(7), e1000316. https://doi.org/10.1371/journal.pmed.1000316
Huang, C., Zhang, C,, Cao, Y., Li, J., & Bi, F. (2023). Major roles of the circadian clock in cancer. Cancer Biol Med, 20(1):1–24. https://doi.org/10.20892/j.issn.2095-3941.2022.0474
Kalaf, J.M. (2014). Mammography: a history of success and scientific enthusiasm. Radiol Bras. 47(4):VII-VIII. https://doi.org/10.1590/0100-3984.2014.47.4e2
Key TJ, Bradbury KE, Perez-Cornago A, Sinha R, Tsilidis KK, Tsugane S. Diet, nutrition, and cancer risk: what do we know and what is the way forward? BMJ. 2020 Mar 5;368:m511. https://doi.org/10.1136/bmj.m511
Kowalski, A.E. (2021). Mammograms and mortality: How has the evidence evolved? J Econ Perspect, 35(2), 119-140. https://doi.org/10.1257/jep.35.2.119
LeShan, L. (1994). Cancer as a turning point. New York: Plume. https://www.amazon.com/Cancer-As-Turning-Point-Professionals/dp/0452271371
Lewis, T. (2022). The U.S. just lost 26 years’ worth of progress on life expectancy. Scientific American. October 17, 2022. Accessed November 11, 2023. https://www.scientificamerican.com/article/the-u-s-just-lost-26-years-worth-of-progress-on-life-expectancy/
Ma, X., Wang, R., Long, J.B., Ross, J.S., Soulos, P.R., Yu, J.B., Makarov, D.V., Gold, H.T. and Gross, C.P. (2014), The cost implications of prostate cancer screening in the Medicare population. Cancer, 120: 96-102. https://doi.org/10.1002/cncr.28373
Mentella, M.C., Scaldaferri, F., Ricci, C., Gasbarrini, A., & Miggiano, G.A.D. (2019). Cancer and Mediterranean Diet: A Review. Nutrients,11(9):2059. https://doi.org/10.3390/nu11092059
NIH NCI (2023). Physical Activity and Cancer. National Institutes of Health National Cancer Institute. Accessed November 18, 2023. https://www.cancer.gov/about-cancer/causes-prevention/risk/obesity/physical-activity-fact-sheet
Patel, A,V., Friedenreich, C.M., Moore, S.C, et al. (2019). American College of Sports Medicine Roundtable Report on physical activity, sedentary behavior, and cancer prevention and control. Medicine and Science in Sports and Exercise, 51(11), 2391-2402. https://doi.org/10.1249/MSS.0000000000002117
Rabin, R.C. (2018). Can eating organic food lower your cancer risk? The New York Times. Oct 23, 2018. Accessed November 17, 2023. https://www.nytimes.com/2018/10/23/well/eat/can-eating-organic-food-lower-your-cancer-risk.html
Reuben, S.H. (2010). Reducing environmental cancer risk – What We Can Do Now. The President’s Cancer Panel Report. Washington, D.C: U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES, National Institutes of Health, National Cancer Institute. https://deainfo.nci.nih.gov/advisory/pcp/annualReports/pcp08-09rpt/PCP_Report_08-09_508.pdf
Rosenbaum, E. H. & Rosenbaum, I.R. (2023) The Will to Live. Stanford Center for Integrative Medicine. Surviving Cancer. Accessed November 23, 2023. https://med.stanford.edu/survivingcancer/cancers-existential-questions/cancer-will-to-live.html
Salazar, S.M.D.C., Dino, M.J.S., & Macindo, J.R.B. (2023). Social connectedness and health-related quality of life among patients with cancer undergoing chemotherapy: a mixed method approach using structural equation modelling and photo-elicitation. J Clin Nurs. Published online March 9, 2023. https://doi.org/10.1111/jocn.16675
Schmutzler, R. K., Schmitz-Luhn, B., Borisch, B., Devilee, P., Eccles, D., Hall, P., … & Woopen, C. (2022). Risk-adjusted cancer screening and prevention (RiskAP): complementing screening for early disease detection by a learning screening based on risk factors. Breast Care, 17(2), 208-223. https://doi.org/10.1159/000517182
Song, M., & Giovannucci, E. (2016). Preventable incidence and mortality of carcinoma associated with lifestyle factors among white adults in the United States. JAMA Ooncology, 2(9), 1154-1161. https://doi.org/10.1001/jamaoncol.2016.0843
Spei, M.E., Samoli, E., Bravi, F., et al. (2019). Physical activity in breast cancer survivors: A systematic review and meta-analysis on overall and breast cancer survival. Breast, 44,144-152. https://doi.org/10.1016/j.breast.2019.02.001
Stagl, J.M., Lechner, S.C., Carver, C.S. et al. (2015). A randomized controlled trial of cognitive-behavioral stress management in breast cancer: survival and recurrence at 11-year follow-up. Breast Cancer Res Treat, 154, 319–328. https://doi.org/10.1007/s10549-015-3626-6
Stratton, K., Shetty, P., Wallace, R., et al., eds. (2001). Institute of Medicine (US) Committee to Assess the Science Base for Tobacco Harm Reduction. Washington (DC): National Academies Press (US). https://www.ncbi.nlm.nih.gov/books/NBK222369/
Tailor, T.D,, Bell, S., Fendrick, A.M., & Carlos, R.C. (2022) Total and Out-of-Pocket Costs of Procedures After Lung Cancer Screening in a National Commercially Insured Population: Estimating an Episode of Care. J Am Coll Radiol. 19(1 Pt A), 35-46. https://doi.org/10.1016/j.jacr.2021.09.015
Turner, M.C., Andersen, Z.J., Baccarelli, A., Diver, W.R., Gapstur, S.M., Pope, C.A 3rd, Prada, D., Samet, J., Thurston, G., & Cohen, A. (2020). Outdoor air pollution and cancer: An overview of the current evidence and public health recommendations. CA Cancer J Clin, 10.3322/caac.21632. https://doi.org/10.3322/caac.21632
US Department of Health and Human Services (2014). The Health Consequences of Smoking: 50 Years of Progress. A Report of the Surgeon General. Atlanta, GA: :
US Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health. https://aahb.org/Resources/Pictures/Meetings/2014-Charleston/PPT%20Presentations/Sunday%20Welcome/Abrams.AAHB.3.13.v1.o.pdf
Van Tulleken, C. (2023). Ultra-processed people. The science behind food that isn’t food. New Yoerk: W.W. Norton & Company. https://www.amazon.com/gp/product/1324036729/ref=ox_sc_act_title_1?smid=ATVPDKIKX0DER&psc=1
Be Skeptical: Finding and Evaluating Online Health Resources
Posted: October 22, 2023 Filed under: Evolutionary perspective, healing, health, Nutrition/diet, placebo | Tags: advertising, clinial trialslinical efficacy, critical thinking, efficacy, health information, mobile apps, online resources, research methodology, social media 2 CommentsAdapted from: Peper, E. & Harvey, R. (2023). Be skeptical: Finding and evaluating online health resources. Townsend Letters. The Examiner of Alternative Medicine, October 21, 2023. https://www.townsendletter.com/e-letter-20-evaluate-sources-to-make-informed-choices/
Erik Peper, PhD, BCB and Richard Harvey, PhD

Source: https://live.staticflickr.com/65535/48445803437_726b61e3d1_b.jpg
An unprecedented flood of information is available today at our fingertips in the form of cell phone apps, news stories, blog posts, social media feeds, advertisements, websites, videos, and audio resources. Artificial intelligence (AI) applications such as ChatGPT are also capable of curating health and wellness information all proclaiming to optimize our health or treat our illnesses. This article provides strategies to determine how to trust the information. It offers strategies for assessing information, reasons to have a skeptical perspective, suggestions for finding credible resources and includes a framework to identify beneficial health information, which may be used for improving activities of daily living. The recommendations are based upon an evolutionary perspective in which anything that was not part of our evolutionary past should be viewed with healthy skepticism.
“It is simply no longer possible to believe much of the clinical research that is published, or to rely on the judgment of trusted physicians or authoritative medical guidelines. I take no pleasure in this conclusion, which I reached slowly and reluctantly over my two decades as an editor of The New England Journal of Medicine.” —Dr. Marcia Angell (2009), the first woman editor of the highly respected New England Journal of Medicine.
How to make sense of the flood of health information
An unprecedented flood of health information is available today proclaiming useful information to optimize our health or treat our illnesses, A simple question is, “How do we know which information is accurate?” To what extent do we trust the information in an era of fake news, commercial health apps trying to sell us things, and news stories from publishers and media conglomerates that are dependent on advertising revenues? This article offers strategies for assessing information, reasons to have a skeptical perspective, and suggestions for finding relevant and accurate information.
Skepticism about health information takes many forms including ‘conspiracy theories’ about vaccines such as when people claim a SARS-COVID-19 vaccine will kill you, to when people doubt the efficacy of HIV or similar vaccines. Several authors have suggested political as well as individual personality factors which explain conspiratorial skepticism about health information, most commonly about vaccines (Crescenzi-Lanna, Valente, Cataldi, & Martire, 2023; Koinig, & Kohler, 2021; Putois, & Helms,. 2022). This article takes a broader view of health information skepticism, focusing on perspective building as well as asking relevant, accurate and meaningful questions about health care decisions.
Take a skeptical perspective and ask, “What is the evidence that the product, procedure, or treatment is going to be effective for me compared to others?” The answer could appear obvious: published peer-reviewed systematic meta-analyses of double blind, randomized, controlled trials describing specific products or procedures. However, the answer is more complex. In numerous cases, finding relevant reports can be challenging. In some cases, it may be unethical or impossible to run double blind, randomized, controlled trials to detect the scope of effectiveness or generalize the finding from animal studies to human beings. For example, surgery cannot be evaluated in a double-blind study. (Would you really want your surgeon not to be aware of what he/she was doing?). Although treatment effectiveness can be studied using a matched comparison or a control group receiving mock surgery, in those cases the surgeon would still be aware of the procedure.
The Challenges of Assessing Clinical Efficacy
It is challenging to know what actually contributes to the beneficial outcomes as well as how to measure the outcome. Some of the factors that affect the outcomes include:
Placebo interactions: Intrinsic to all procedures are placebo and nocebo components. In some cases the direct benefit effects of a drug or procedure demonstrated in a randomized controlled trial may still not be due solely to the direct effects of the drug or procedure, but rather due to positive indirect effects triggered by the placebo response to non-specific side effects (Peper and Harvey, 2017).
Lack of evidence is not proof that it does not work. Lack of replicable evidence for some cases implies that a positive response will not occur in all cases. Unfortunately, commercial interests may bias interpretations of research studies when the efforts to replicate a study had limitations in the first place, or the replication efforts did not retain transferable conditions to the next study. In other words, ‘ceteris paribus’ may not apply as all things are not always equal during replication studies. Similarly, individual differences that are outliers or extreme values during a study (e.g. positive benefit from placebo) can be ‘explained away’ with statistics because statistics may also skew the interpretations based on the biases of the researchers.
Clinical trials are very expensive. The average clinical trial for a new therapeutic agent, 2015–2017, was $48 million dollars (Moore et al., 2020). The cost of achieving Food and Drug Administration (FDA) approval is so high that it is often out of reach for small companies. It is no wonder that most clinical trials are funded by the pharmaceutic industry and only for those drugs for which they foresee significant profits. The estimated research and development investment to bring a new medicine to market is estimated to range between $314 million to $2.8 billion (Wouters et al, 2020). To be financially viable, this usually means that drugs must be used by a large consumer base and ideally be taken for the rest of the individual’s life. Non-drug approaches may be less profitable, so without a profit incentive, investigations of non-drug efficacy accumulates less evidence compared to multi-million dollar trials.
Human beings are not rats, mice, or monkeys. The findings from animal studies in numerous studies provide some useful insights into the effects of medications or procedures on living organisms. Unfortunately, many results from animal studies could not be replicated in humans or, the findings may not apply to human beings. The basic assumption that animal studies could mimic human studies may not be valid since almost all test animals are not typical of normal animals, implying test animals are ‘abnormal’ in terms of results. For example, the animals such as rats are usually housed in small cages 24 hours a day which is analogous to a human being held in solitary confinement without social contact or ability to move for a lifetime. Thus, their physiology and their response to interventions are often different from healthy free ranging animals (Shaw, 2023).
Even when animal studies show that the medications are not harmful, they could be harmful for some human beings. For example, thalidomide was approved for use in Germany, so doctors prescribed it to treat morning sickness in pregnant women. However, in humans Thalidomide interfered with embryonic and fetal development in ways not observed in rodent tests (Tantibanchachai & Yang, 2019).
Statistical significance may not indicate meaningful clinical improvement. Many clinical studies demonstrate that the studied interventions have contributed to improvement. However, does the improvement make a quality of life (QOL) difference and/or clinically relevant difference for the person? For example, a successful study that demonstrated lowering of patients’ systolic pressure by 5 mm from 175 mm/Hg to 170mm/Hg may be statistically significant, but is not clinically meaningful, since, a resting systolic blood pressure of 170 mm/Hg is still a cause for concern.
Similarly, in the recent systematic review by Arciero et al. (2021) of approved oncology therapies, 40% of Food and Drug Administration (FDA)-approved as well as 58% of European Medicine Agency (EMA)-approved indications had published QOL evidence. However, only 6% of FDA- and 11% of EMA-approved indications had clinically meaningful improvements in QOL beyond minimally clinically relevant differences. This means that medication therapies are often approved without demonstrating Quality of Life improvement for the long term.
Statistics which describe how large an effect is may be referred to as an ‘effect size estimate, which is a better index of efficacy compared to other statistics such as a difference in statistical mean values. The effect size can be assessed by using various statistics such as Cohen’s d-statistic (Mean A minus Mean B divided by pooled standard deviation; Cohen, 1988)[i].
Number of people need to be treated for one person to benefit. Effect size calculation estimates the average number of people in a trial needing treatment so that one of them experiences benefit. This statistic can be referred to as the number needed to treat (NNT) (Mendes et al., 2017). To calculate the NNT, divide 1 by the control event rate (CER) minus the treatment event rate (TER) or 1/CER-TER. For example, the number patients needed to be treated for five years with cholesterol lowering (e.g., statin drugs) medications to prevent one coronary heart disease event ranges from 53 (high risk group) to 146 (low risk group) (Rossignol et al., 2018). This means that many of the participants could experience negative side effects related to the medications while only one participant benefits from the prevention of a heart attack.
Focus on short-term versus long-term benefits. Many studies measure outcomes under highly controlled conditions of a study and are conducted for a relatively short time period—often for less than 3 months. However, effects that may be beneficial in the short term may not be beneficial or may even be harmful in the long term. For example, opioid medications are very useful in the short term to alleviate intense pain. However, over time, drug dependency may develop, contributing to addiction, inability to function, or death. Shockingly, opioid-related deaths in the U.S. numbered more than 100,000 people in 2022 (CDC, 2022).
Benefits do not enhance quality of life. If the data indicate benefits of treatment, do the interventions improve quality of life and not simply prolong life for a few days, weeks, or months? Does the patient or client value quality of life over quantity of days lived (e.g., ”palliative care with shorter life, but some relief from pain and suffering versus prolonged life with pain and suffering”)?
Results may only apply to a select group. Biochemical individuality means that each person is unique to some degree, differing genetically, biochemically, and physiologically. Similarly, responses vary widely to medical procedures, medications, and other substances. A common example is alcohol sensitivity— the genetic predisposition to metabolizing alcohol breakdown— manifesting in highly visible facial flushing which occurs in 47%-85% of Asians and 3%-29% of Caucasians (Chan, 1986). In the context of medicine, individual differences that influence clinical outcomes include genetic predisposition, as well as age, gender, income, education level, job status, geographic region (e.g., climate and food sources) and other demographic factors, individually or in combination.
Consider that many interventions and medications have only been tested on narrowly defined subgroups such college students (true of most psychological studies), or men (true for most pharmaceuticals since women could be pregnant or in different phases of their menstrual cycle). The promise of personalized or ‘precision’ medicine will likely advance in the coming years, making medications more tailored to individual differences based on age, sex, and other demographic factors.
There is no free lunch. Similar to the concept of short-term versus long-term benefits, when a drug offers a quick improvement, it may be effective, but may cause long-term harm. A representative example is the use of high-dose and multi-doses of anabolic steroids to increase muscle mass and athletic performance. There is a potential cost: “High and multi-doses of anabolic steroids used for athletic enhancement can lead to serious and irreversible organ damage” (Maravelias, et al., 2005).
Risks of hazardous exposures and risks associated with the treatment. Could the procedure or medication result in loss or harm? Given bio-individuality, there can be broad “variability” in response and outcome, which depends on the vulnerability of a given individual (their adaptive capacity) and the risks involved. Additionally, there are sometimes important variables that have not been investigated deliberately because those important variables complicate interpretation, and or, there may be important variables that are missed The most obvious example of omission is when animal studies were or are conducted exclusively on male animals because interpreting results can be more complicated given female reproductive hormones. Beside sex variables other important variables that may be missed include covert illnesses and co-morbidities which are unknown at the time of the study. Taken together, studies which oversimplify variables may make it difficult interpret the results for individuals.
Below is a set of images relevant to climate change and farming, depicting the relationship between the exposure to hazards of systemic climate change and the vulnerabilities, sensitivities, and adaptive capacities of individuals and the community (Wilhelmi and Hayden, 2016).

Use “Uncommon” Sense
The attractive look and feel of a website are not evidence of accuracy or credibility. Rather, good design simply means it was developed by a skilled web designer or that the client paid a great deal of money to have it created. It does not make the content valid. The comments of Yucha (2002) and Yucha and Montgomery (2008) remind readers to increase literacy regarding ”health claims” made on websites, especially a commercial website intended to sell products or services.
Evaluating dietary supplements. If you’re thinking about using a dietary supplement, check the recommendations from reliable sources. Make it a point to purchase a reputable brand, since some supplements contain ingredients not listed on the label. In addition, they may interact with medications or other supplements. Share and discuss all your supplements you are taking with your healthcare provider. For example, vitamin E acts as anticoagulants and may increase clotting time and bleeding especially if one is taking “blood thinners.”
Follow the money. Ask who would financially benefit from the product or service? For example, physicians increase their referrals for lab testing, MRIs (Magnetic Resonance Images), or other diagnostic procedures if they have ownership in those testing centers or, if they receive significant reimbursement for those services, although there is no evidence that patients benefit more (Bishop et al, 2010).
Beware of advertised claims. Most highly advertised drugs are largely no better at treating a disease than generic medication or other options (Patel et al., 2023). Pharmaceutical companies in 2021 spend $6.88 billion for direct to consumer advertising (Faria, 2023). The advertisement suggests that their branded medication is better; however, generics are about 80% cheaper and have the same active ingredient and are similar in their action (AAM, 2020).
If the claims seem unbelievable, they are probably are unbelievable. If it is too good to be true, it probably is not true. Historically, Thomas Lupton (1580) wrote a thoughtful inquiry about religion and utopian societies, introducing a skeptics point of view, describing people and societies that are ”too good to be true.” Modern skeptics consider the preponderance of evidence based on scientific replicability (the replication of findings in subsequent clinical trials) as proof of what they believe to be true.

Source: Indiana University of Pennsylvania, last accessed March 3, 2023 https://www.iup.edu/instructional-design/images/assessment.jpg
Assessing Online Information
What do we know about the accuracy of online health information? A skeptical viewpoint is that bias exists in sources of information from a wide range of commercial, organizational, governmental and educational institutions (identified by ending with .com, .org, .gov and .edu, respectively). Most all institutions set out to prove their own bias; however, people working in educational institutions by and large require their investigators go through a peer-review process, so they tend to be more trusted as sources of information. Commercial, organizational, and governmental institutions all have biased perspectives. However, they are less likely to reveal their biases, simply stating that “a study was conducted” without providing enough information who funded the study or the importance of positive results to achieve academic recognition.
“A lot of what is published is incorrect … much of the scientific literature, perhaps half, may simply be untrue. Afflicted by studies with small sample sizes, tiny effects, invalid exploratory analyses, and flagrant conflicts of interest, together with an obsession for pursuing fashionable trends of dubious importance, science has taken a turn towards darkness.” Dr. Richard Horton (2015), Editor-in-Chief of The Lancet.
Be skeptical of university or published research findings that are directly or indirectly funded/influenced by industry or commercial sources. Government research published in highly respected scientific journals may not be replicable because the investigations were narrowly designed to favor a particular bias. For example, industries that produce pharmaceuticals and medical devices, as well as agribusinesses that produce tobacco and sugar products, have been accused of a ”profit-first” bias (Bruening, 2019; Hill et al., 2019). These industries often support studies conducted by “independent” researchers at universities. However, grant funding quickly disappears if the findings are negative which may affect the career of the researcher because many university faculty positions and promotions depend upon the faculty member’s ability to garner grants.
Compare US safety guidelines to those of the EU. In many cases, the acceptable values are different. The safety limits for herbicide and pesticide residues in foods are often much lower in the EU than in the US (e.g., safer with lower exposure levels). For example, the US allows six times as much residue of the pesticide, Round-Up, with a toxic ingredient, glyphosate, in foods consumed in the American diet (Tano, 2016). The USA allows this higher exposure even though about half of the human gut microbiota are vulnerable to glyphosate exposure (Puigbo et al., 2022). A skeptical view of research could adapt a precautionary principle such as “if you think it could cause harm then do not use it until proven safe.”
Government guidelines and directions may not always be accurate. For example, after 9/11 the CDC initially announced that the particulate dust from the World Trade Center collapse was not harmful The CDC made this claim without any data, in efforts to reassure the public. In fact, the dust was harmful. More recently, some of the politicization of the CDC COVID-19 recommendations have raised questions. For example at the beginning of the pandemic, the CDC publicly recommended “If you are NOT sick: You do not need to wear a facemask unless you are caring for someone who is sick (and they are not able to wear a facemask)” which suggested that masks were not necessary. (McReynolds, 2020). Most likely, the statement was made so that more masks would be available for medical workers. The statement would have engendered more trust if the CDC had stated, Masks are useful; however, please make your own, since the medical-grade n95 masks are in very short supply and needed to protect the frontline health professionals who are most at risk.
The National Personal Protective Technology Laboratory (NPPTL) describes the types of masks needed to protect medical and other types of workers such as fire fighters, where the numbers represent the percentage of particulates filtered (e.g., 95%, 99%, 100%) and the letters represent the types of particles (e.g., N = not resistant to oils, R = resistant to oils and, P = strongly resistant to oils). Other countries have similar mask standards, where a N95 mask in the United States (i.e., N95; NIOSH-42 CRF 84) is equivalent to masks in Europe (FFP2; EN149-2001), China (KN95; GB2626-2019), Australia (P2; AS/NZ 1716-2012), Korea (KF94; KMOEL 2017-64), Japan (DS2; JMIHLW 214-2018) and, Brazil (PFF2; ABNT/NBR 13.698.2011). The reason for including the technical details about masks is to remind the reader that both governments as well as other sources of health information may hide some of the information about potentials for loss or harm behind lots of technical details, so knowing how to compare information becomes relevant when making health decisions.
Patient population in the research study may not represent the average patient (referred to as Berkson’s bias). Research study subjects may have multiple co-morbidities or may all be healthy young males. In either case, they may not be representative of the general patient population nor of individuals (Westreich, 2012).
The data does not discuss or excludes outliers? Positive findings, even in randomized, placebo-controlled studies, mean that the treatment approach is more beneficial than the control condition. In almost all cases, some participants respond extremely well and some very poorly, often referred to as statistical outliers. What is usually not reported are the characteristic of the ‘super responders’ or ‘non-responders.’ Have more trust in studies that provide a full range or a wider range of information about the positive and negative responders, rather than simply reporting about the average response.
The research review is highly selective. Meta-analyses and review articles evaluate the outcomes of multiple research studies. However, typically they include only well designed randomized controlled trials. In many of these studies, 95% of the published articles are excluded because they did not fit the narrow criteria of the randomized selection. Thus, these meta-analyses may exclude conditions under which the treatment approach would be highly beneficial to a specific set of people. When the meta-analyses identify the studies that are excluded and why, it is possible to learn of the biases of the meta-analyses.
Funding for research or clinical trials favors products or technologies which can be patented, commercialized and support industry profits. There is extensive funding for new drug development for the treatment of COVID-19 or hypertension, but limited funding for diet or lifestyle changes that could optimize the immune system. If a product or drug is beneficial however not patentable, it is unlikely that a pharmaceutical company will further develop and market it because competitors could easily produce it. For example, pharmaceutical companies do not advertise vitamin D3 supplements because it is not patent protected even though a preponderance of independent research has clearly demonstrated that the incidence of symptoms following metastatic cancer diagnosis is reduced with vitamin D3 supplements (Chandler et al., 2020).
Be aware of the revolving door. The top administrators of numerous US regulating agencies such as the Food and Drug Administration (FDA) and the US Department of Agriculture (USDA) are often rewarded with well-paying jobs in the pharmaceutical, healthcare, and agribusiness industries after leaving jobs in the US government. For example,
- Scott Gottleib, MD was head of the FDA 2017-2019 before leaving the government in 2019 and then has been a board member of Pfizer pharmaceuticals as independent director. (https://www.pfizer.com/people/leadership/board_of_directors/scott_gottlieb-md).
- Stephen Han was the FDA commissioner under President Trump and approved the emergency use of the Moderna vaccine. Six months later, he quit and joined Flagship Pioneering, the firm behind Moderna. (https://www.fiercebiotech.com/biotech/six-months-after-granting-moderna-covid-19-eua-ex-fda-commish-joins-biotech-s-founding).
- Joby Youn, who served as chief of staff to former U.S. Department of Agriculture Secretary Sonny Perdue, went on to work for the American Farm Bureau Federation. (McVan, 2022).
A skeptical question to be raised is to what extent does the promise of well-paying jobs impact the decisions of administrators who are in charge of regulating industries that may offer a high paying job in the future. Would you avoid antagonizing those companies thereby risk a future financial windfall? Similar conflicts of interest may be at play in other industries. For example, Boeing’s close relationship with the Federal Aviation Administration (FAA) by giving initial approval of Boeing 737 Max airplane that may have contributed to the two fatal airplane crashes (Cassidy, 2020).
Use critical thinking and don’t rely solely on the first internet search results resources when making decisions about your health. Many commercial companies (e.g., internet resources ending with ‘.com’) will pay to be on the first page of an internet search. Consider using more advanced internet search results that access ‘scholarly’ information, often available from ‘.edu’ sources. Consult with your health care provider when you are considering complementary health care approaches if you have a medical condition. Remember that some health providers may have personal biases as well as financial incentives in keeping you as their patient. Request evidence on which the provider is making their judgements and be sure to discuss the following two kinds of questions: (1) What are the risks, costs and benefit as well as potential for loss or harm? (2) Does the product or service interfere with other treatments? If not, then do what you think is useful. At worst, all you will lose is money.

Source: http://library.med.utah.edu/blog/eccles/files/2011/08/logoHealthLiteracy.png
Finding Health Information on the Internet
The following guidelines have been adapted from an online paper from the National Center for Complementary and Integrative Health (NCCIH) entitled, Finding and Evaluating Online Resources. The text in italic is reproduced directly from the online paper (NCCIH, 2023).
“Your search for published and online health information may start at a known, trusted site, but after following several links, you may find yourself on an unfamiliar site. Can you trust this site? Here are some key questions you need to ask.”
When checking online sources of health information, ask the following questions:
Who operates and pays for the website? Can you trust them? Any reliable health-related website should make it easy for you to learn who is responsible for the site. You should be able to find out who runs a website and its purpose on the “About Us” page. For example, on the NCCIH Website, each major page identifies NCCIH and, because NCCIH is part of the NIH, provides a link to the NIH home page.
Does the site sell advertising? Or Why does the site or app exist? Is it sponsored by a company that sells dietary supplements, markets drugs, provides other product, or services? Confirm any information you find on a site that sells products with an independent site that is not a commercial site.
What is the source of the information? Many health or medical sites post information collected from other websites or sources, and that information should be identified. For example, the Health Topics A-Z page on the NCCIH site provides links to documents that NCCIH did not create—but names the sources of the documents.
How do you know if the information is accurate? Is it based on scientific research? The site should describe the evidence (such as articles in medical journals) on which the material is based. Opinions or advice should be clearly set apart from information that is evidence-based (based on research results). For example, if a site discusses health benefits you can expect from a treatment, look for references to scientific research that clearly support what is said. Keep in mind that testimonials, anecdotes, unsupported claims, and opinions are not the same as objective, evidence-based information. [It is important to remember that this does not mean that it is incorrect; it just may mean the appropriate study was not done as there was no funding for it.]
Is the content a sales pitch masquerading as a news report? Some of these reports are reliable, but others are confusing, conflicting, misleading, or missing important information. For insight on how to evaluate news stories about health, wellness, and complementary therapies, visit our interactive module Know the Science: The Facts About Health News Stories.
Has the information been reviewed by experts? You can be more confident in the quality of medical information on a website if health experts reviewed it. Some websites have an editorial board that reviews content. Others put the names and credentials of reviewers in an Acknowledgments section near the end of the page and declare any conflict of interest. [Yet, even this is challenging as stated in the previous quotes by the Lancet journal editor-in-chief Horton. Thus having sign-off by someone with an advanced degree may not guarantee veracity.]
How current is the information? When was the information written or reviewed? Outdated medical information can be misleading or even dangerous. Responsible health websites review and update much of their content on a regular basis. Content such as news reports or meeting summaries that describe an event usually is not updated. To find out whether information is outdated, look for a date on the page (it’s often near the bottom). [However, old information does not mean that it is incorrect. Information from the past may be valid and even fundamental and foundational. Sometimes an older medication may be more effective; however, it is no longer recommended because it has outlasted the time period of its patent protection and, the pharmaceutical company has created a slightly new variation which may or may not be more effective.]
What is the website or smartphone app promising or offering? When claims seem too good to be true, the claims probably are not true.
Useful websites for information resources. Start with one of these organized collections of quality resources suggested by the University of Utah (2023):
- Google Scholar ( https://scholar.google.com/ ) provides access to many peer-reviewed resources.
- MedlinePlus, (https://medlineplus.gov/) sponsored by the National Library of Medicine, which is part of the National Institutes of Health (NIH)
- healthfinder.gov, sponsored by the Office of Disease Prevention and Health Promotion in the U.S. Department of Health and Human Services.
- National Center for Complementary and Integrative Health (NCCIH), (https://www.nccih.nih.gov/) the Federal Government’s lead agency for scientific research on complementary and integrative health approaches. Keep in mind that many integrative health and complementary techniques have not been assessed because of a lack of research and funding, however, the procedures can be highly beneficial. The absence of controlled studies does not mean the absence of benefit.
- Follow NCCIH on Facebook, Twitter, Pinterest, and Instagram. These accounts are updated and managed by NCCIH and provide the latest resources on a variety of complementary health approaches.
- For information on dietary supplements, visit the NIH Office of Dietary Supplements website (https://ods.od.nih.gov/factsheets/list-all/). [Remember that many of the dietary values were initially identified as the minimum value to prevent the develop of the vitamin deficiency disease. This value may only prevent an obvious disease. It may not be the appropriate value for optimum health. Most of the data was based on healthy young Caucasian males and the values may not be accurate for women, other age groups, or genetic phenotypes and most likely need to be significantly higher.]
Finding Health Information on Social Media
Credible sources of health information may be found on some social media websites. One suggestion by Kington et al., (2021) is to apply the ‘CRAP’ test developed originally by librarian Molly Beestrum at Northwestern University using four major considerations labeled: “Currency/Credibility, Reliability, Authority, and Purpose/Point of View.” Also, consider the following:
- Check the sponsor’s website. Health information on social networking sites is often very brief. For more information, go to the sponsoring organization’s website. On Twitter, look for a link to the website in the header; on Facebook, look in the About section.
- Verify that social media accounts are what they claim to be. Some social networking sites have a symbol that an account has been verified. For example, Twitter uses a blue badge but people now pay fee for this badge. Is it really verified or only demonstrates that the person paid a fee. Use the link from the organization’s official website to go to its social networking sites.
Finding Health Information on Mobile Health Apps
The National Academy of Medicine (NAM, 2023) builds on the Kington et al. (2021) article about identifying credible sources of health information. Some of the reminders suggested in the NAM website (cf. https://nam.edu/identifying-credible-sources-of-health-information-in-social-media-principles-and-attributes/) are paraphrased below:
There are thousands of mobile apps (a software program you access using your phone or other mobile device) that provide health information you can read on your mobile devices. Almost 20 percent of smartphone owners had at least one health app on their phones in 2012. Keep these things in mind when using a mobile health app:
- The content of most apps is not written or reviewed by medical experts. The information could be inaccurate and unsafe. In addition, the information you enter when using an app may not be secure in terms of protecting personal or private health information (PHI) . [Even if the content is written by medical experts, remember they most likely got paid for it or received university grants from these companies.]
- There is little research on the benefits, risks, and the impact of apps as a source of health information. For example, the ketogenic diet has been found to improve certain medical conditions such as intractable epilepsy. However, for individuals who tend to put weight on easily with a high fat diet, the sudden versus gradual use of a ketogenic diet may be potentially harmful and could shorten lifespan.
- How secure is the technology?It’s not always easy to know what personal information on an app will accessed by third parties or how personal information will be stored or transferred in an unsecure manner.
- Consider the source. Before you download an app, find out if the store you get the app from says who created it. Don’t trust the app if contact or website information for the creator isn’t available. Health apps created by Government agencies can be found by visiting: Centers for Disease Control and Prevention.
- What is the site’s policy about linking to other sites? Some sites don’t link to any other sites, some link to any site that asks or pays for a link, and others link only to sites that meet certain criteria. You may be able to find information on the site about its linking policy. (For example, NCCIH’s linking policy is available on the NCCIH Website Information and Policies page.) Unless the site’s linking policy is strict, don’t assume that the sites that it links to are reliable. You should evaluate the linked sites just as you would any other site that you’re visiting for the first time.
- How does the site collect and handle personal information? Today, most websites track what pages you’re looking at. They may also ask you to “subscribe” or “become a member.” Any credible site collecting this kind of information should tell you exactly what it will and won’t do with your information.
- Will they sell your data? Many commercial sites sell aggregated data about their users’ demographics to other companies (for example, information such as the percentage of their users that are men over 40 or under 25). In some cases, they may collect and reuse information that’s “personally identifiable,” such as your ZIP Code, gender, and birth date. Read any privacy policy or similar language on the site, and don’t sign up for anything you don’t fully understand. You can find NICCIH’s privacy policy on the NCCIH website.
- Is the site encrypted? See if the address (URL) for the site starts with “https://” instead of “http://.” Sites that use HTTPS (Secure Hyper Text Transfer Protocol) are encrypted, less likely to be hacked, and more likely to protect your privacy.
- Can you communicate with the owner of the website? You should always be able to contact the site owner if you run across problems or have questions or feedback. If the site hosts online discussion forums or message boards, the site should explain the terms of use.
Are You Reading News or Advertising?
The Federal Trade Commission (FTC) has warned the public about fake online news sites. The site may look real, but is actually an advertisement. The site may use the logos of legitimate news organizations or similar names and web addresses. To get you to sign up for whatever they’re selling, they may describe an “investigation” into the effectiveness of the product. But everything is fake: there is no reporter, no news organization, and no investigation. Only the links to a sales site are real. Fake news sites have promoted questionable products, including weight loss products, work-at-home opportunities, and debt reduction plans. You should suspect that a news site may be fake if it:
- Endorses a product. Real news organizations generally don’t do this.
- Only quotes people who say good things about the product (includes only positive reader comments, and you can’t add a comment of your own).
- Presents research findings that seem too good to be true. (If something seems too good to be true, it usually is too good to be true.)
- Contains links to a sales site.
Use common sense and incorporate an Evolutionary Perspective in making decisions
To make sense of the flood of information use critical thinking and ask yourself whether the claims make sense in context of human evolution. Over millions of years of evolution, nature has “performed” ongoing experiments through natural selection to improve reproductive fitness. As (Talib, 2014) stated, “It [is] an insult to Mother Nature to override her programmed reactions unless we [have] a good reason to do so, backed by proper empirical testing to show that we humans can do better; the burden of evidence falls on us humans.”

Source: https://www.publicdomainpictures.net/pictures/130000/velka/darwin-evolution.jpg
How can we improve health with some simple procedures or drugs when nature has experimented for millions of years. Adapt the rules to maintain health as described by Talib (2014) in the book, Antifragile: Things That Gain from Disorder (2014), summarized with the following points:
- Anything that was not part of our evolutionary past should be viewed with healthy skepticism. There is a good possibility that it is harmful, because there has not been sufficient time for humanity to adapt genetically to the new variation. For example, the addition of altered trans fats to commercially available foods, which are not recognized by the human immune system and a result, can promote inflammation, cardiovascular disease, and cancer.
- We do not need evidence of harm to claim that a drug or an unnatural procedure involves potential risk. Take a cautionary approach with a healthy dose of skepticism. If possible then wait until more evidence is discovered. If evidence of harm does not exist, that does not mean harm does not exist.
- Only resort to medical techniques when the health payoff is very large (i.e., to save a life). Does the intervention exceed its potential harm, in cases such as emergency surgery or a lifesaving medicine (e.g., penicillin).
Take charge of your health—talk with your health care providers about any complementary health approaches you use. Together, you can make shared, well-informed decisions.
Key Background Source material for the NCCIH (2023) article, “Finding and Evaluating Online Resources“
- Albrecht, U.V., Von Jan, U., & Praman, O..(2013). Standard reporting for medical apps. Studies in Health Technology and Informatics. 190, 201-203. https://pubmed.ncbi.nlm.nih.gov/23823422/
- Office of Dietary Supplements. How to Evaluate Health Information on the Internet: Questions and Answers. Office of Dietary Supplements website. Accessed July 10, 2023 https://ods.od.nih.gov/HealthInformation/How_To_Evaluate_Health_Information_on_the_Internet_Questions_and_Answers.aspx
- Plaza, I, Demarzo, M.M., Herrera-Mercadal, P., et al. (2013). Mindfulness-based mobile applications: literature review and analysis of current features. JMIR mHealth and uHealth, 1(2), e24. https://doi.org/10.2196/mhealth.2733
- Subhi, Y., Bube, S.H., Rolskov Bojsen, S., et al. (2015). Expert involvement and adherence to medical evidence in medical mobile phone apps: a systematic review. JMIR mHealth and uHealth, 3(3),e79. https://doi.org/10.2196/mhealth.4169
Recommended sources for the NIH (2023) article, “Finding and Evaluating Online Resources“
- Boulos, M.N., Brewer, A.C., Karimkhani, C., et al. (2014). Mobile medical and health apps: state of the art, concerns, regulatory control and certification. Online Journal of Public Health Informatics, 5(3), 229. https://doi.org/10.5210/ojphi.v5i3.4814. eCollection 2014
- Buying health products and services online. Federal Trade Commission website. Accessed July 10, 2023 https://consumer.ftc.gov/articles/0023-buying-health-products-services-online
- Carissoli, C., Villani, D., & Riva. G. (2015). Does a meditation protocol supported by a mobile application help people reduce stress? Suggestions from a controlled pragmatic trial. Cyberpsychology, Behavior and Social Networking, 8(1), :46-53. https://doi.org/10.1089/cyber.2014.0062
- Comprar productos y servicios para la salud en internet. Federal Trade Commission website. Accessed July 10, 2023 https://consumidor.ftc.gov/articulos/s0023-comprar-productos-y-servicios-para-la-salud-en-internet
- How to Spot Fake Online Reviews. Consumer Reports website. Accessed July 10, 2023. https://www.consumerreports.org/money/customer-reviews-ratings/how-to-spot-fake-online-reviews-a1345282053/
- Find quality resources. HealthIT.gov website. Accessed July 10, 2023. https://www.healthit.gov/topic/health-it-resources
- Mani, M., Kavanagh, D.J., Hides, L., et al. (2015). Review and evaluation of mindfulness-based iPhone apps. JMIR mHealth and uHealth, I(3), e82. https://doi.org/10.2196/mhealth.4328
- Marcano Belisario, J.S., Huckvale, K., Greenfield, G., et al. (2016). Smartphone and tablet self management apps for asthma. Cochrane Database of Systematic Reviews. (11) :CD010013. https://doi.org/10.1002/14651858.CD010013.pub2
- Martínez-Pérez, B., de la Torre-Díez, I., & López-Coronado, M. (2015). Privacy and security in mobile health apps: a review and recommendations. Journal of Medical Systems, 39(1), 181. https://doi.org/10.1007/s10916-014-0181-3
- Wallace, L.S. & Dhingra, L.K. (2014). A systematic review of smartphone applications for chronic pain available for download in the United States. Journal of Opioid Management, 10(1), 63-68. https://doi.org/10.5055/jom.2014.0193
References
- AAM (2020). 2020 Report: Generic Drug and Biosimilars Access and Savings in the U.S.,” Association for Accessible Medicines, last accessed March 3, 2023,
https://accessiblemeds.org/2020-Access-Savings-Report - Angell, M. (2009). Drug companies & doctors: A story of corruption. The New York Review of Books, 56(1), 8-12. http://www.nybooks.com/articles/2009/01/15/drug-companies-doctorsa-story-of-corruption/
- Arciero, V., Delos Santos, S., Koshy, L., et al. (2021). Assessment of Food and Drug Administration– and European Medicines Agency–Approved Systemic Oncology Therapies and Clinically Meaningful Improvements in Quality of Life: A Systematic Review. JAMA Netw Open, 4(2):e2033004. https://doi.org/10.1001/jamanetworkopen.2020.33004
- Benbrook, C.M. (2016). Trends in glyphosate herbicide use in the United States and globally. Environ Sci Eur, 28(3). https://doi.org/10.1186/s12302-016-0070-0
- Bishop, T.F., Federman, A.D., Ross, J.S. (2010). Laboratory test ordering at physician offices with and without on-site laboratories. J Gen Intern Med.25(10, 1057-63. https://doi.org/10.1007/s11606-010-1409-7
- Bruening, Z. L. (2019). Profits over People: Flaws in Regulating the Pharmaceutical Industry and Controlled Substances (Doctoral dissertation, Utica College). https://www.proquest.com/openview/ae5178804f2e7a86bd2cf0db62ee2854/1?pq-origsite=gscholar&cbl=18750&diss=y
- Cassidy, J. (2020). How Boeing and the F.A.A. Created the 737 MAX Catastrophe, The New Yorker, September 17, 2020. https://www.newyorker.com/news/our-columnists/how-boeing-and-the-faa-created-the-737-max-catastrophe
- CDC Center for Disease Control and Prevention (May11, 2022). U.S. Overdose Deaths In 2021 Increased Half as Much as in 2020 – But Are Still Up 15%, last accessed 12/12/2022. https://www.cdc.gov/nchs/pressroom/nchs_press_releases/2022/202205.htm
- Chan, A.W. (1986). Racial differences in alcohol sensitivity. Alcohol Alcohol. 21(1), 93-104. https://pubmed.ncbi.nlm.nih.gov/2937417/
- Chandler, P.D., Chen, W.Y., Ajala, O.N., et al. (2020). Effect of Vitamin D3 Supplements on Development of Advanced Cancer: A Secondary Analysis of the VITAL Randomized Clinical Trial. JAMA Netw Open, 3(11):e2025850. https://doi.org/10.1001/jamanetworkopen.2020.25850
- Cohen, J. (1988). Statistical power analysis for the behavioral sciences. 2nd ed. New York: Routledge. https://doi.org/10.4324/9780203771587
- Crescenzi-Lanna, L., Valente, R., Cataldi, S., & Martire, F. (2023). Predictors of young people’s anti-vaccine attitudes in the context of the COVID-19 pandemic. Public Understanding of Science, 09636625231179830. https://doi.org/10.1177/09636625231179830
- Faria, J. (2023). Pharama DTC ad spend in the U.S. 2012-2021. Statista, last accessed March 2, 2023. https://www.statista.com/statistics/686906/pharma-ad-spend-usa/#:~:text=The%20pharmaceutical%20industry%20in%20the,invested%20into%20big%20pharma%20ads.
- Hill, J. A., Agewall, S., Baranchuk, A., Booz, G. W., Borer, J. S., Camici, P. G., … & Vrints, C. (2019). Medical misinformation: Vet the message!. Journal of the American Heart Association, 8(3), e011838. https://doi.org/10.1161/JAHA.118.011838
- Horton, R. (2015). Offline: What is medicine’s 5 sigma? The Lancet, 385(9976), 1380.
https://doi.org/10.1016/S0140-6736(15)60696-1 - Kington, R. S., Arnesen, S., Chou, W. Y. S., Curry, S. J., Lazer, D., & Villarruel, A. M. (2021). Identifying credible sources of health information in social media: Principles and attributes. NAM perspectives, 2021. https://doi.org/10.31478/202107a
- Koinig, I., & Kohler, S. (2021). On the Relationship Between Skepticism Towards and Reactance to Health Messages: The Special Case of Online Communication on Tick-Borne Encephalitis. Frontiers in Communication, 6, 170. https://doi.org/10.3389/fcomm.2021.737800
- Lupton, Thomas (1580). Siuqila too good, to be true : omen : though so at a vewe yet all I tolde you is true, I vpholde you, now cease to aske why? for I can not lye : herein is shewed by way of dialogue, the wonderful maners of the people of Mauqsun, with other talke not friuolous. Printed at London: By H. Bynneman, dwelling in Thames Streate, neere vnto Baynards Castell, 1580. https://www.amazon.com/Siuqila-too-good-true-vpholde/dp/1171274114
- Maravelias, C., Dona, A., Stefanidou, M., & Spiliopoulou, C. (2005). Adverse effects of anabolic steroids in athletes: A constant threat. Toxicology Letters, 158(3), 167-175. https://doi.org/10.1016/j.toxlet.2005.06.005
- McReynolds, T. (2020). CDC: An about face on face masks? Last accessed February 22, 2023. https://www.aaha.org/publications/newstat/articles/2020-03/cdc-an-about-face-on-face-masks/
- Mcvan, M. (2022), In Washington, agricultural policymakers circulate among Farm Bureau, USDA and industry. Missouri Independent, September 6, 2022. https://missouriindependent.com/category/energy-environment/
- Mendes, D., Alves, C., & Batel-Marques, F. (2017). Number needed to treat (NNT) in clinical literature: an appraisal. BMC Med, 15(1), 112. https://doi.org/10.1186/s12916-017-0875-8
- Moore, T.J., Heyward, J., Anderson, G., & Alexander, G.C. (2020). Variation in the estimated costs of pivotal clinical benefit trials supporting the US approval of new therapeutic agents, 2015-2017: a cross-sectional study. BMJ Open. Jun 11;10(6):e038863. https://doi.org/10.1136/bmjopen-2020-038863
- National Academy of Medicine, Identifying Credible Sources of Health Information, last accessed July 5, 2023. https://nam.edu/identifying-credible-sources-of-health-information-in-social-media-principles-and-attributes/
- NCCIH (2023). National Center for Complementary and Integrative Health. Finding and Evaluating Online Resources, Last accessed February 22, 2023. https://www.nccih.nih.gov/health/finding-and-evaluating-online-resources?nav=govd
- Patel, N.G., Hwang , T.J., Woloshin, S., & Kesselheim, A.S. (2023). Therapeutic Value of Drugs Frequently Marketed Using Direct-to-Consumer Television Advertising, 2015 to 2021. JAMA Netw Open, 6(1):e2250991. https://doi.org/10.1001/jamanetworkopen.2022.50991
- Peper, E. & Harvey, R. (2017). The fallacy of the placebo controlled clinical trials: Are positive outcomes the result indirect treatment side effects? NeuroRegulation. 4(3–4,102–113.https://doi.org/10.15540/nr.4.3-4.102
- Perrier, E. T., Armstrong, L. E., Bottin, J. H., Clark, W. F., Dolci, A., Guelinckx, I., … & Péronnet, F. (2021). Hydration for health hypothesis: a narrative review of supporting evidence. European journal of nutrition, 60(3), 1167-1180. https://doi.org/10.1007/s00394-020-02296-z
- Puigbò, P., Leino, L. I., Rainio, M. J., Saikkonen, K., Saloniemi, I., & Helander, M. (2022). Does Glyphosate Affect the Human Microbiota?. Life, 12(5), 707. https://doi.org/10.3390/life12050707
- Putois, O., & Helms, J. (2022). The Role of Denial in Vaccine Skeptics and “Anti-vax” Blame: A Psychodynamic Approach. Frontiers in Psychology, 13, 886368. https://doi.org/10.3389/fpsyg.2022.886368
- Rossignol, M., Labrecque, M., Cauchon, M., Breton, M., & Poirier, P. (2018). Number of patients needed to prescribe statins in primary cardiovascular prevention: mirage and reality, Family Practice, 35(4), 376-382. https://doi.org/10.1093/fampra/cmx124
- Shaw, S. (2023 February 18). The case for free-range lab mice. The New Yorker. Last accessed March 1, 2023. https://www.newyorker.com/culture/annals-of-inquiry/the-case-for-free-range-lab-mice
- Talib, N. N. (2014). Antifragile: Things That Gain from Disorder (Incerto). New York: Random House. https://www.amazon.com/Antifragile-Things-That-Disorder-Incerto/dp/0812979680#:~:text=Antifragile%20is%20a%20standalone%20book,world%20we%20don’t%20understand.
- Tano, B. The Layman’s Guide to Integrative Immunity. Integrative Medical Press; 2016. https://www.amazon.com/Laymans-Guide-Integrative-Immunity-Discover/dp/0983419299
- Tantibanchachai, C, & Yang, J. (2019). Studies of thalidomide’s effects on rodent embryos from 1962-2008. The Embryo Project Encyclopedia. https://embryo.asu.edu/pages/studies-thalidomides-effects-rodent-embryos-1962-2008
- Westreich, D. (2012). Berkson’s bias, selection bias, and missing data. Epidemiology (Cambridge, Mass.), 23(1), 159. https://doi.org/10.1097/EDE.0b013e31823b6296
- Wilhelmi, O. & Hayden, M. (2016). Reducing vulnerability to extreme heat through interdisciplinary research and stakeholder engagement. In Extreme Weather, Health, and Communities (pp. 165-186). Springer, Cham. https://convergence.unc.edu/wp-content/uploads/sites/381/2017/03/wilhelmi-hayden_2016_reducing-vuln-to-extreme-heat-interdiscip-research-stakeholder-engagement.pdf
- Wouters, O. J., McKee, M., & Luyten, J. (2020). Estimated Research and Development Investment Needed to Bring a New Medicine to Market, 2009-2018. JAMA, 323(9), 844-853. https://doi.org/10.1001/jama.2020.1166
- Yucha, C. B. (2002). Problems inherent in assessing biofeedback efficacy studies. Applied psychophysiology and biofeedback, 27(1), 99-106. https://doi.org/10.1023/a:1014528622061
- Yucha, C., & Montgomery, D. (2008). Evidence-based practice in biofeedback and neurofeedback. Wheat Ridge, CO: AAPB. https://www.advantagehcs.com/wp-content/uploads/2018/11/EvidenceBasedYuchaMontgomeryW.pdf
[i]This is a measure of size of the association as measured by as statistic such as Cohen’ d; namely, if it is small–although statistically significant– it probably would not be clinically meaningful. Cohen (1988) suggested a ”d” statistic (e.g. Cohen’s d) comparing the group differences (e.g. treatment group vs. comparison group change scores; [M2 – M1]) divided by the standard deviation of both groups [square root of SD1+SD2]/2], interpreting moderate effects between 0.50 and 0.79 and larger effects above 0.80. Treatment group vs comparison group effects are also estimated by examining percentages. Relative risk ratio or odds ratio is a single number that reflects the increased or decreased risk. For example, a doubled risk would be expressed as a relative risk of 2. Risk decreased by 50% would be expressed as RR 0.5. This number is calculated as the percent of people with clinically meaningful outcomes divided by percent of people without clinically meaningful outcomes. This provides a ‘relative’ estimate of effectiveness, where a ratio close to 1 indicates no difference between treatment and comparison groups, and ratios greater than 3 to 1 (e.g. treatment group was twice as effective as comparison group) are considered moderate effects and 4 to 1 are considered larger effects.
About the Authors
Erik Peper’s teaching and research focuses on self-healing strategies, illness prevention, the effects of posture and respiration, and how to use biofeedback and wearable devices. Each year he mentors undergraduate student researchers to create and complete studies that are presented at scientific meetings. He is an international authority on biofeedback and self-regulation and author of scientific articles and books such as Make Health Happen, Fighting Cancer-A Nontoxic Approach to Treatment, and Biofeedback Mastery. His most recent co-authored book is, TechStress: How Technology is Hijacking Our Lives, Strategies for Coping, and Pragmatic Ergonomics. He publishes the blog, The Peper Perspective–ideas on illness, health and well-being (peperperspective.com). In 2013 was received the Biofeedback Distinguished Scientist Award in recognition of outstanding career & scientific contributions from the Association for Applied Psychophysiology.
Richard Harvey has a Ph.D. for the UC Irvine Social Ecology program. His research includes developing stress-reduction interventions which promote psychological courage and hardiness. Before teaching at SF State, he was a research fellow at the UC Irvine Transdisciplinary Tobacco Use Research Center for five years, developed and ran the UC Irvine Counseling Center Biofeedback and Stress Management Program, and worked as a Maternal, Child and Adolescent Health Research Analyst in Orange County. He is the co-chair of the American Public Health Association, Alternative and Complementary Health Practices Special Interest Group, as well as a board member of the Biofeedback Society of California and the San Francisco Psychological Association. He has published in the areas of biofeedback, stress and computer-related disorders, tobacco cessation, and the psychology of hardiness and courage.
Copyright © 2023 Townsend Letter
Are food companies responsible for the epidemic in diabetes, cancer, dementia and chronic disease and do their products need to be regulated like tobacco? Is it time for a class action suit?
Posted: July 15, 2023 Filed under: behavior, cancer, Evolutionary perspective, health, Nutrition/diet, self-healing | Tags: dementia, diabetes, diet, high fructose corn syrup, mortality, obsity, smoking, sugar, ultra-processed foods, UPF 5 CommentsAdapted from: Peper, E. & Harvey, R. (2024). Are Food Companies Responsible for the Epidemic in Diabetes, Cancer, Dementia and Chronic Disease and Do Their Products Need to Be Regulated Like Tobacco? Is It Time for a Class Action Suit? Thownsend Letter-the examiner of alternative medicine. https://www.townsendletter.com/e-letter-26-ultra-processed-foods-and-health-issues/
Erik Peper, PhD and Richard Harvey, PhD

Why are one third of young Americans becoming obese and at risk for diabetes?
Why are heart disease, cancer, and dementias occurring earlier and earlier? Is it genetics, environment, foods, or lifestyle?
Is it individual responsibility or the result of the quest for profits by agribusiness and the food industry?
Like the tobacco industry that sells products regulated because of their public health dangers, is it time for a class action suit against the processed food industry? The argument relates not only to the regulation of toxic or hazardous food ingredients (e.g., carcinogenic or obesogenic chemicals) but also to the regulation of consumer vulnerabilities. Addressing vulnerabilities to tobacco products include regulations such as how cigarette companies may not advertise their products for sale within a certain distance from school grounds.
Is it time to regulate nationally the installation of vending machines on school grounds selling sugar-sweetened beverages? Students have sensitivity to the enticing nature of advertised, and/or conveniently available consumable products such as ‘fast foods’ that are highly processed (e.g., packaged, preserved and practically imperishable). Whereas ‘processed foods’ have some nutritive value, and may technically pass as ‘nutritious’ food, the quality of processed ‘nutrients’ can be called into question. For the purpose of this blog other important questions to raise relate to ingredients which, alone or in combination, may contribute to the onset of or, the acceleration of a variety of chronic health outcomes related to various kinds of cancers, cardiovascular diseases, and diabetes.
It may be an over statement to suggest that processed food companies are directly responsible for the epidemic in diabetes, cancer, dementia and chronic disease and need to be regulated like tobacco. On the other hand, processed food companies should become much more regulated than they are now.
More than 80 years ago, smoking was identified as a significant factor contributing to lung cancer, heart disease and many other disorders. In 1964 the Surgeon Generals’ report officially linked smoking to deaths of cancer and heart disease (United States Public Health Service, 1964). Another 34 years pased before California prohibited smoking in restaurants in 1998 and, eventually inside all public buildings. The harms of smoking tobacco products were well known, yet many years passed with countless deaths and suffering which could have been prevented before regulation of tobacco products took place. Reviewing historical data there is about a 20 year delay (e.g., a whole generation) before death rates decrease in relation to when regulations became effective and smoking rates decreased, as shown in figure 1.

Figure 1. The relationship between smoking and lung cancer. Reproduced by permission from Roser, M. (2021). Smoking: How large of a global problem is it? And how can we make progress against it? Our world in data.
During those interim years before government actions limited smoking more effectively, tobacco companies hid data regarding the harmful effects of smoking. Arguably, the ‘Big Tobacco’ industry paid researchers to publish data which could confuse readers about tobacco product harm. There is evidence of some published articles suggesting that the harm of cigarette smoking was a hoax– all for the sake of boosting corporate profits (Bero, 2005).
Now we are experiencing a similar problem with the processed food industry. It has been suggested that alongside smoking and vaping, opioid use, a sedentary ‘couch potato’ lifestyle, and lack of exercise, ultra-processed food (UPF) that we eat severely affects our health.
Ultra-processed foods, which for many constitutes a majority of calories ranging from 55% to over 80% of the food they eat, contain chemical additives that trick the tastebuds, mouth and eventually our brain to desire those processed foods and eat more of them (Srour et al., 2022).
What are ultra-processed foods? Any foods that your great grandmother would not recognize as food. This includes all soft drinks, highly processed chips, additives, food coloring, stabilizers, processed proteins, etc. Even oils such as palm oil, canola oil, or soybean are ultra processed since they heated, highly processed with phosphoric acid to remove gums and waxes, neutralized with chemicals, bleached, and deodorized with high pressure steam (van Tulleken, 2023).
The data is clear! Since the 1970s obesity and inflammatory disease have exploded after ultra-processed foods became the constituents of the modern diet as shown in figure 2.
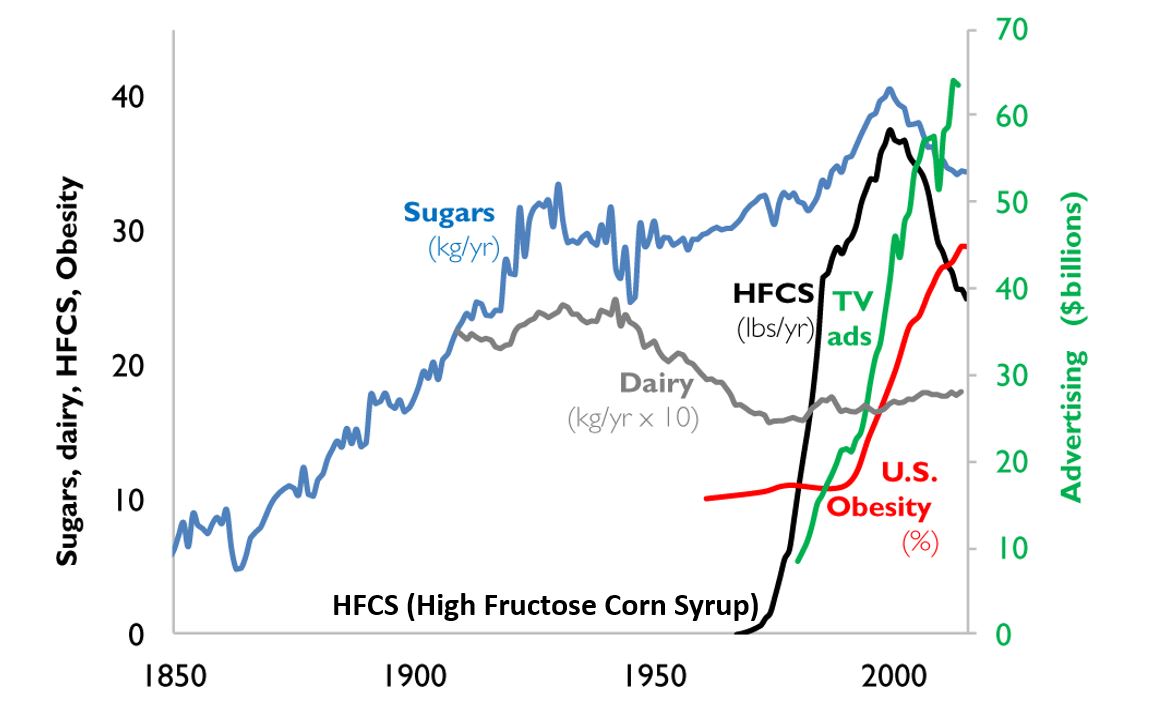
Figure 2. A timeline from 1850 to 2000 reflects the increase in use of refined sugar and high fructose corn syrup (HFCS) to the U.S. diet, together with the increase in U.S. obesity rate. The data for sugar, dairy and HFCS consumption per capita are from USDA Economic Research Service (Johnson et al., 2009) and reflects historical estimates before 1967 (Guyenet et al., 2017). The obesity data (% of U.S. adult population) are from the Robert Wood Johnson Foundation’s Trust for America’s Health. (stateofobesity.org). Total U.S. television advertising data are from the World Advertising Research Center (www.warc.com). The vertical measure (y–axis) for kilograms per year (kg/yr) on the left covers all data except advertising expenditures, which uses the vertical measure for advertising on the right. Reproduced by permission from Bentley et al, 2018.
This graph clearly shows a close association between the years that high fructose corn syrups (HFCS) were introduced into the American diet and an increase in TV advertising with corresponding increase in obesity. HFCS is an ultra-processed food and is a surrogate marker for all other ultra-processed foods. The best interpretation is that ultra-processed foods, which often contain HFCS, are a causal factor of the increase in obesity, and diabetes and in turn are risk factors for heart disease, cancers and dementias.
Ultra-processed foods are novel from an evolutionary perspective.
The human digestive system has only recently encountered sources of calories which are filled with so many unnatural chemicals, textures and flavors. Ultra-processed foods have been engineered, developed and product tested to increase the likelihood they are wanted by consumers and thereby increase sales and profits for the producers. These foods contain the ‘right amount’ processed materials to evoke the taste, flavor and feel of desired foods that ‘trick’ the consumer it eat them because they activate evolutionary preference for survival. Thus, these ultra-processed foods have become an ‘evolutionary trap’ where it is almost impossible not to eat them. We eat the food because it capitalized on our evolutionary preferences even though doing so is ultimately harmful for our health (for a detailed discussion on evolutionary traps, see Peper, Harvey & Faass, 2020).
An example is a young child wanting the candy while waiting with her parents at the supermarket checkout line. The advertised images of sweet foods trigger the cue to eat. Remember, breast milk is sweet and most foods in nature that are sweet in taste, provide calories for growth and survival and are not harmful. Calories are essential of growth. Thus, we have no intrinsic limit on eating sweets unlike foods that taste bitter.
As parents, we wish that our children (and even adults) have self-control and no desire to eat the candy or snacks that is displayed at eye level (eye candy) especially while waiting at the cashier. When reflecting about food advertising and the promotion of foods that are formulated to take advantage of ‘evolutionary traps’, who is responsible? Is it the child, who does not yet have the wisdom and self-control or, is it the food industry that ultra-processes the foods and adds ingredients into foods which can be harmful and then displays them to trigger an evolutionary preference for food that have been highly processed?
Every country that has adapted the USA diet of ultra-processed foods has experienced similar trends in increasing obesity, diabetes, cardiovascular disease, etc. The USA diet is replacing traditional diets as illustrated by the availability of Coca-Cola. It is sold in over 200 countries and territories (Coca-Cola, 2023).
An increase in ultra-processed foods by 10 percent was associated with a 25 percent increase in the risk of dementia and a 14 per cent increase in the risk of Alzheimers’s (Li et al., 2022). More importantly, people who eat the highest proportion of their diet in ultra-processed foods had a 22%-62% increased risk of death compared to the people who ate the lowest proportion of processed foods (van Tulleken, 2023). In the USA, counties with the highest food swamp scores (the availability of fast food outlets in a county) had a 77% increased odds of high obesity-related cancer mortality (Bevel et al., 2023). The increase risk has also been observed for cardiovascular disease, coronary heart disease, cerebrovascular disease and all cause mortality as is shown in figure 3 (Srour et al., 2019; Rico-Campà et al., 2019).

Figure 3. Association between consumption of ultra-processed foods and all cause mortality. Reproduced from Rico-Campà et al, 2019.
The harmful effects of UPF holds up even when correcting for the amount of sugars, carbohydrates or fats in the diet and controlling for socio economic variables.
The logic that underlies this perspective is based upon the writing by Nassim Taleb (2012) in his book, Antifragile: Things That Gain from Disorder (Incerto). He provides an evolutionary perspective and offers broad and simple rules of health as well as recommendations for reducing UPF risk factors:
- Assume that anything that was not part of our evolutionary past is probably harmful.
- Remove the unnatural/unfamiliar (e.g. smoking/ e-cigarettes, added sugars, textured proteins, gums, stabilizers (guar gum, sodium alginate), emulsifiers (mono-and di-glycerides), modified starches, dextrose, palm stearin, and fats, colors and artificial flavoring or other ultra-processed food additives).
What can we do?
The solutions are simple and stated by Michael Pollan in his 2007 New York Times article, “Eat food. Not too much. Mostly Plants.” Eat foods that your great grandmother would recognize as foods (Pollan, 2009). Do not eat any of the processed foods that fill a majority of a supermarket’s space.
- Buy only whole organic natural foods and prepare them yourself.
- Request that food companies only buy and sell non-processed foods.
- Demand government action to tax ultra-processed food and limit access to these foods. In reality, it is almost impossible to expect people to choose healthy, organic foods when they are more expensive and not easily available in the American ‘food swamps and deserts’ (the presence of many fast food outlets or the absence of stores that have fresh produce and non-processed foods). We do have a choice. We can spend more money now for organic, health promoting foods or, pay much more later to treat illness related to UPF.
- It is time to take our cues from the tobacco wars that led to regulating tobacco products. We may even need to start class action suits against producers and merchants of UPF for causing increased illness and premature morbidity.
For more background information and the science behind this blog, read, the book, Ultra-processed people, by Chris van Tulleken.

Look at the following blogs for more background information.
References
Bentley, R.A., Ormerod, P. & Ruck, D.J. (2018). Recent origin and evolution of obesity-income correlation across the United States. Palgrave Commun 4, 146. https://doi.org/10.1057/s41599-018-0201-x
Bero, L. A. (2005). Tobacco Industry Manipulation of Research. Public Health Reports (1974-), 120(2), 200–208. http://www.jstor.org/stable/20056773
Bevel, M.S., Tsai, M., Parham, A., Andrzejak, S.E., Jones, S., & Moore, J.X. (2023). Association of Food Deserts and Food Swamps With Obesity-Related Cancer Mortality in the US. JAMA Oncol. 9(7), 909–916. https://doi.org/10.1001/jamaoncol.2023.0634
Coca-Cola. (2023). More on Coca-Cola. Accessed July 14, 2023. https://www.coca-cola.co.uk/our-business/faqs/how-many-countries-sell-coca-cola-is-there-anywhere-in-the-world-that-doesnt
Johnson, R.K., Appel, L.J., Brands, M., Howard, B.V., Lefevre, M., Lustig, R.H., Sacks, F., Steffen, L.M., & Wylie–Rosett, J. (2009). Dietary sugars intake and cardiovascular health: a scientific statement from the American Heart Association. Circulation, 120(10), 1011–1020. https://doi.org/10.1161/CIRCULATIONAHA.109.192627
Li, H., Li, S., Yang, H., et al, 2022. Association of ultraprocessed food consumption with the risk of dementia: a prospective cohort study. Neurology, 99, e1056-1066. https://doi.org/10.1212/WNL.0000000000200871
Peper, E., Harvey, R. & Faass, N. (2020). TechStress: How Technology is Hijacking Our Lives, Strategies for Coping, and Pragmatic Ergonomics. Berkeley: North Atlantic Books, pp 18-22, 151. https://www.amazon.com/Beyond-Ergonomics-Prevent-Fatigue-Burnout/dp/158394768X/ref=sr_1_1?crid=1U9Y82YO4DKKP&keywords=erik+peper&qid=1689372466&sprefix=erik+peper%2Caps%2C187&sr=8-1
Pollan, M. (2007). Unhappy meals. The New York Times Magazine. https://www.nytimes.com/2007/01/28/magazine/28nutritionism.t.html
Pollan, M. (2009). Food Rules: An Eater’s Manual. New York: Penguin Books. https://www.amazon.com/Food-Rules-Eaters-Michael-Pollan/dp/014311638X/ref=tmm_pap_swatch_0?_encoding=UTF8&qid=1689373484&sr=8-2
Rico-Campà, A., Martínez-González, M. A., Alvarez-Alvarez, I., de Deus Mendonça, R., Carmen de la Fuente-Arrillaga, C., Gómez-Donoso, C., & Bes-Rastrollo, M. (2019). Association between consumption of ultra-processed foods and all cause mortality: SUN prospective cohort study. BMJ; 365: l1949 https://doi.org/10.1136/bmj.l1949
Roser, M. (2021).Smoking: How large of a global problem is it? And how can we make progress against it? Our world in data. Assessed July 13, 2023. https://ourworldindata.org/smoking-big-problem-in-brief
Srour, B., Fezeu, L.K., Kesse-Guyot, E.,Alles, B., Mejean, C…(2019). Ultra-processed food intake and risk of cardiovascular disease: prospective cohort study (NutriNet-Santé) BMJ,365:l1451. https://doi.org/10.1136/bmj.l1451
Srour, B., Kordahi, M. C., Bonazzi, E., Deschasaux-Tanguy, M., Touvier, M., & Chassaing, B. (2022). Ultra-processed foods and human health: from epidemiological evidence to mechanistic insights. The Lancet Gastroenterology & Hepatology. https://doi.org/10.1016/S2468-1253(22)00169-8
Taleb, N. N. (2012). Antifragile: Things That Gain from Disorder (Incerto). New York: Random House Publishing Group. (Kindle Locations 5906-5908). https://www.amazon.com/Antifragile-Things-Disorder-ANTIFRAGILE-Hardcover/dp/B00QOJ6MLC/ref=sr_1_4?crid=3BISYYG0RPGW5&keywords=Antifragile%3A+Things+That+Gain+from+Disorder+%28Incerto%29&qid=1689288744&s=books&sprefix=antifragile+things+that+gain+from+disorder+incerto+%2Cstripbooks%2C158&sr=1-4
Van Tulleken, C. (2023). Ultra-processed people. The science behind food that isn’t food. New Yoerk: W.W. Norton & Company. https://www.amazon.com/gp/product/1324036729/ref=ox_sc_act_title_1?smid=ATVPDKIKX0DER&psc=1
United States Public Health Service. (1964). The 1964 Report on Smoking and Health. United States. Public Health Service. Office of the Surgeon General. https://profiles.nlm.nih.gov/spotlight/nn/catalog?f%5Bexhibit_tags%5D%5B%5D=smoking
Mouth breathing and tongue position: a risk factor for health
Posted: June 8, 2023 Filed under: ADHD, behavior, Breathing/respiration, cognitive behavior therapy, Evolutionary perspective, healing, health, Nutrition/diet, self-healing, Uncategorized | Tags: babies, breastfeedging, development, infants, jaw, mouth breathing, neurocognitive develoment, nose breathing, sleep, tongue-tie Leave a commentErik Peper, PhD, BCB and Ron Swatzyna, PhD, LCSW, BCB, BCN
Adapted from: Peper, E., Swatzyna, R., & Ong, K. (2023). Mouth breathing and tongue position: a risk factor for health. Biofeedback. 51(3), 74–78 https://doi.org/10.5298/912512

Breathing usually occurs without awareness unless there are problems such as asthma, emphysema, allergies, or viral infections. Infant and child development may affect how we breathe as adults. This blog discusses the benefits of nasal breathing, factors that contribute to mouth breathing, how babies’ breastfeeding and chewing decreases the risk of mouth breathing, recommendations that parents may implement to support healthy development of a wider palate, and the embedded video presentation, How the Tongue Informs Healthy (or Unhealthy) Neurocognitive Development, by Karindy Ong, MA, CCC-SLP, CFT, .
Benefits of nasal breathing
Breathing through the nose filters, humidifies, warms, or cools the inhaled air as well as reduces the air turbulence in the upper airways. In addition, the epithelial cells of the nasal cavities produce nitric oxide that are carried into the lungs when inhaling during nasal breathing (Lundberg & Weitzberg, 1999). The nitric oxide contributes to healthy respiratory function by promoting vasodilation, aiding in airway clearance, exerting antimicrobial effects, and regulating inflammation. Breathing through the nose is associated with deeper and slower breathing rate than mouth breathing. This slower breathing also facilitates sympathetic parasympathetic balance and reduces airway irritation.
Mouth breathing
Some people breathe predominantly through their mouth although nose breathing is preferred and health promoting. Mouth breathing negatively impacts the ability to perform during the day as well as affect our cognitions and mood (Nestor, 2020). It contributes to disturbed sleep, snoring, sleep apnea, dry mouth upon waking, fatigue, allergies, ear infections, attention deficit disorders, crowded mis-aligned teeth, and poorer quality of life (Kahn & Ehrlich, 2018). Even the risk of ear infections in children is 2.4 time higher for mouth breathers than nasal breathers (van Bon et al, 1989) and nine and ten year old children who mouth breath have significantly poorer quality of life and have higher use of medications (Leal et al, 2016).
One recommendation to reduce mouth breathing is to tape the mouths closed with mouth tape (McKeown, 2021). Using mouth tape while sleeping bolsters nose breathing and may help people improve sleep, reduce snoring, and improves alertness when awake (Lee et al, 2022).
Experience how mouth breathing affects the throat and upper airway
Inhale quickly, like a gasp, as much air as possible through your open mouth. Exhale letting the air flow out through your mouth. Repeat once more.
Inhale quickly as much air through the nose, then exhale by allow the airflow out through the nose. Repeat once more.
What did you observe? Many people report that rapidly inhaling through the mouth causes the back of the throat and even upper airways to feel drier and irritated. This does not occur when inhaling through the nose. This simple experiment illustrates how habitual mouth breathing may irritate the airways.
Developmental behavior that contributes to mouth breathing
The development of mouth breathing may begin right at birth when the mouth, tongue, jaw and nasal area are still developing. The arch of the upper palate forms the roof of the oral cavity that separates the oral and nasal cavities. When the palate and jaw narrows, the arch of the palate increases and pushes upwards into the nasal area. This reduces space in the nasal cavity for the air to flow and obstructs nasal breathing. The highly vaulted palate is not only genetically predetermined but also by how we use our tongue and jaw from birth. The highly arched palate is only a recent anatomical phenomena since the physical structure of the upper palate and jaw from the pre- industrial era was wider (less arched upper palate) than many of our current skulls (Kahn & Ehrlich, 2018).
The role of the tongue in palate development
After babies are born, they breastfeed by sucking with the appropriate tongue movements that help widen the upper palate and jaw. On the other hand, when babies are bottle fed, the tongue tends to move differently which causes the cheek to pull in and the upper palate to arch which may create a high narrow upper palate and making the jaw narrower. There are many other possible factors that could cause mouth breathing such as tongue-tie (ankyloglossia), septal deviation, congenital malformation, enlarged adenoids and tonsils (Aden tonsillar hyperplasia), inflammatory diseases such as allergic rhinitis (Trabalon et al, 2012). Whatever the reasons, the result of the impoverished tongue movement and jaw increases the risk for having a higher arched upper palate that impedes nasal breathing and contributes to habitual mouth breathing.
The forces that operate on the mouth, jaw and palate during bottle feeding may be similar to when you suck on straw and the cheeks coming in with the face narrowing. The way the infants are fed will change the development of the physical structure that may result in lifelong problems and may contribute to developing a highly arched palate with a narrow jaw and facial abnormalities such as long face syndrome (Tourne, 1990).
To widen the upper palate and jaw, the infant needs to chew, chew and tear the food with their gums and teeth. Before the industrialization of foods, children had to tear food with their teeth, chew fibrous foods or gnaw at the meat on bones. The chewing forces allows the jaw to widen and develop so that when the permanent teeth are erupting, they would more likely be aligned since there would be enough space–eliminating the need for orthodontics. On the other hand, when young children eat puréed and highly processed soft foods (e.g., cereals soaked in milk, soft breads), the chewing forces are not powerful enough to encourage the widening of the palate and jaw.
Although the solution in adults can be the use of mouth tape to keep the mouth closed at night to retrain the breathing pattern, we should not wait until we have symptoms. The focus needs to be on prevention. The first step is an assessment whether the children’s tongue can do its job effectively or limited by tongue-tie and the arch of the palate. These structures are not totally fixed and can change depending on our oral habits. The field of orthodontics is based upon the premise that the physical structure of the jaw and palate can be changed, and teeth can be realigned by applying constant forces with braces.
Support healthy development of the palate and jaw
Breastfeed babies (if possible) for the first year of life and do NOT use bottle feeding. When weaning, provide chewable foods (fruits, vegetable, roots, berries, meats on bone) that was traditionally part of our pre-industrial diet. These foods support in infants’ healthy tongue and jaw development, which helps to support the normal widening of the palate to provide space for nasal breathing.
Provide fresh organic foods that children must tear and chew. Avoid any processed foods which are soft and do not demand chewing. This will have many other beneficial health effects since processed foods are high in simple carbohydrates and usually contain color additives as well as traces of pesticides and herbicides. The highly processed foods increase the risk of developing depression, type 2 diabetes, inflammatory disease, and colon cancer (Srour et al., 2019).
Sadly, the USA allows much higher residues of pesticide and herbicides that act as neurotoxins than are allowed in by the European Union. For example, the acceptable level of the herbicide glyphosate (Round-Up) is 0.7 parts per million in the USA while in the acceptable level is 0.01 parts per million in European countries (Tano, 2016; EPA, 2023; European Commission, 2023). The USA allows this higher exposure even though about half of the human gut microbiota are vulnerable to glyphosate exposure (Puigbò et al., 2022).
The negative effects of herbicides and pesticides are harmful for growing infants. Even fetal exposure from the mother (gestational exposure) is associated with an increase in behaviors related to attention-deficit/hyperactivity disorders and executive function in the child when they are 7 to 12 years old (Sagiv et al., 2021) and organophosphate exposure is correlated with ADHD prevalence in children (Bouchard et al., 2010).
To implement these basic recommendations are very challenging. It means the mother has to breastfeed her infant during the first year of life. This is often not possible because of socioeconomic inequalities; work demands and medical complications. It also goes against the recent cultural norm that fathers should participate in caring for the baby by giving the baby a bottle of stored breast milk or formula.
From our perspective, women who give birth must have a year paid maternity leave to provide their infants with the best opportunity for health (e.g., breast-feeding, emotional bonding, and reduced financial stress). As a society, we have the option to pay the upfront cost now by providing a year- long maternity leave to mothers or later pay much more costs for treating chronic conditions that may have developed because we did not support the natural developmental process of babies.
Relevance to the field of neurofeedback and biofeedback
Clinicians often see clients, especially children with diagnostic labels such as ADHD who have failed to respond to numerous psychotherapies and pharmacotherapies. In the recent umbrella review and meta-analytic evaluation of recent meta-analyses, Leichsenring et al. (2022) found only small benefits overall for both types of intervention. They suggest that a paradigm shift in research seems to be required to achieve further progress in resolving mental health issues. As the past director of National Institute of Health, Dr. Thomas Insel pointed out that the Diagnostic and Statistical Manual of Mental Disorders (DSM) is not a valid instrument and should be a big wake up call for all of us to think outside the box (Insel, 2009). One factor that starts right at birth is the oral cavity development by dysfunctional tongue movements.
We want to make all of you aware of a serious issue in children that you may come across. For those of us who work with children children, we need to ask their parents about the following: tongue-tie, mouth breathing, bedwetting, high-vaulted palate, thumb sucking, abnormal eating issues, apraxia, dysarthria, and hypotonia. Research suggests that the palates of these children are so arched that the tongue cannot do its job effectively, causing multiple issues which may be related.
Please view the webinar from May 17, 2023. Presented by Karindy Ong, MA, CCC-SLP, CFT, How the Tongue Informs Healthy (or Unhealthy) Neurocognitive Development. The presentation explains the developmental process of the role the tongue plays and how it contributes to nasal breathing. Please pass it on to others who may have interest.
References
Bouchard, M.F., Bellinger, D.C., Wright, R.O., & Weisskopf, M.G. (2010). Attention-deficit/hyperactivity disorder and urinary metabolites of organophosphate pesticides. Pediatrics, 125(6), e1270-7. https://doi.org/10.1542/peds.2009-3058
EPA. (2023). Glyphosate. United States Environmental Protection Agency. Accessed April 1, 2023. https://www.epa.gov/ingredients-used-pesticide-products/glyphosate
European Commission. (2023). EU legislation on MRLs.Food Safety. Assessed April 1, 2023. https://food.ec.europa.eu/plants/pesticides/maximum-residue-levels/eu-legislation-mrls_en#:~:text=A%20general%20default%20MRL%20of,e.g.%20babies%2C%20children%20and%20vegetarians.
Insel, T.R. (2009). Translating scientific opportunity into public health impact: a strategic plan for research on mental illness. Arch Gen Psychiatry, 66(2), 128-133. https://doi.org/10.1001/archgenpsychiatry.2008.540
Kahn, S. & Ehrlich, P.R. (2018). Jaws. Stanford, CA: Stanford University Press. https://www.amazon.com/Jaws-Hidden-Epidemic-Sandra-Kahn/dp/1503604136/ref=tmm_hrd_swatch_0?_encoding=UTF8&qid=1685135054&sr=1-1
Leal, R.B., Gomes, M.C., Granville-Garcia, A.F., Goes, P.S.A., & de Menezes, V.A. (2016). Impact of Breathing Patterns on the Quality of Life of 9- to 10-year-old Schoolchildren. American Journal of Rhinology & Allergy, 30(5):e147-e152. https://doi.org/10.2500/ajra.2016.30.4363
Lee, Y.C., Lu, C.T., Cheng, W.N., & Li, H.Y. (2022).The Impact of Mouth-Taping in Mouth-Breathers with Mild Obstructive Sleep Apnea: A Preliminary Study. Healthcare (Basel), 10(9), 1755. https://doi.org/10.3390/healthcare10091755
Leichsenring, F., Steinert, C., Rabung, S. and Ioannidis, J.P.A. (2022), The efficacy of psychotherapies and pharmacotherapies for mental disorders in adults: an umbrella review and meta-analytic evaluation of recent meta-analyses. World Psychiatry, 21: 133-145. https://doi.org/10.1002/wps.20941
Lundberg, J.O. & Weitzberg, E. (1999). Nasal nitric oxide in man. Thorax. (10):947-52. https://doi.org/10.1136/thx.54.10.947
McKeown, P. (2021). The Breathing Cure: Develop New Habits for a Healthier, Happier, and Longer Life. Boca Raton, Fl “Humanix Books. https://www.amazon.com/BREATHING-CURE-Develop-Healthier-Happier/dp/1630061972/
Nestor, J. (2020). Breath: The New Science of a Lost Art. New York: Riverhead Books. https://www.amazon.com/Breath/dp/0593191358/ref=tmm_pap_swatch_0?_encoding=UTF8&qid=1686191995&sr=8-1
Puigbò, P., Leino, L. I., Rainio, M. J., Saikkonen, K., Saloniemi, I., & Helander, M. (2022). Does Glyphosate Affect the Human Microbiota?. Life, 12(5), 707. https://doi.org/10.3390/life12050707
Sagiv, S.K., Kogut, K., Harley, K., Bradman, A., Morga, N., & Eskenazi, B. (2021). Gestational Exposure to Organophosphate Pesticides and Longitudinally Assessed Behaviors Related to Attention-Deficit/Hyperactivity Disorder and Executive Function, American Journal of Epidemiology, 190(11), 2420–2431. https://doi.org/10.1093/aje/kwab173
Srour, B. et al. (2019). Ultra-processed food intake and risk of cardiovascular disease: prospective cohort study (NutriNet-Santé).BMJ, 365. https://doi.org/10.1136/bmj.l1451
Tano, B. (2016). The Layman’s Guide to Integrative Immunity. Integrative Medical Press. https://www.amazon.com/Laymans-Guide-Integrative-Immunity-Discover/dp/0983419299/_
Tourne, L.P. (1990). The long face syndrome and impairment of the nasopharyngeal airway. Angle Orthod, 60(3):167-76. https://doi.org/10.1043/0003
Trabalon, M. & Schaal, B. (2012). It takes a mouth to eat and a nose to breathe: abnormal oral respiration affects neonates’ oral competence and systemic adaptation. Int J Pediatr, 207605. https://doi.org/10.1155/2012/207605
van Bon, M.J., Zielhuis, G.A., Rach, G.H., & van den Broek, P. (1989). Otitis media with effusion and habitual mouth breathing in Dutch preschool children. Int J Pediatr Otorhinolaryngol, (2), 119-25. https://doi.org/10.1016/0165-5876(89)90087-6

{kind=link}
{kind=link}
{kind=link}
{kind=link}