Managing Blood Sugar: Lifestyle Changes for Better Health
Posted: May 25, 2026 Filed under: ADHD, attention, behavior, cancer, Evolutionary perspective, healing, health, lifestyle, Nutrition/diet, self-healing, Uncategorized | Tags: AIC, carbohydrate, continous glucose monitoring, diet, exhaustion, glucose, insulin, metabolic disease, obesity, sugar, ultra-processed foods Leave a comment
It was 4:45 p.m., and I was looking forward to swimming. I briskly walked the eight blocks from my house to the heated outdoor city pool. The pool is unusual—100 feet long instead of the standard 25 yards—and I enjoy the rhythm of swimming lap after lap.
I arrived just as the sign flipped from Closed to Open. I quickly changed into my bathing suit, locked my clothes in a metal locker, took a short shower, and jumped into the lane. The sun was still out, and only one other swimmer shared my lane. I felt energized and expected to complete my usual forty laps.
However, after about eighteen laps, my energy suddenly disappeared. There was nothing left in the tank. I swam to the side, pulled myself slowly onto the pool deck, and even slowly and unsteadily walked to the men’s locker room. I sat down on the bench feeling shaky, weak, and exhausted. This was not ordinary fatigue. After resting for several minutes, I slowly showered, dressed, and walked home with heavy, almost uncoordinated legs.
As I reflected on the experience, I remembered something similar that had happened two weeks earlier. Around 5 p.m, I had taken my son’s dog for a brisk walk. Again, I began energized, walking quickly, and then suddenly felt drained and sweaty. When I returned home, all I could do was sit down and recover.
What happened
Reflecting back, I realized that both cases I had eaten sweets—cake one time and a large chocolate chip cookie the other about two hours earlier Most likely, the rapidly absorbed sugars and refined carbohydrates caused a sharp increase in blood glucose, followed by a significant insulin response (Ludwig & Ebbeling, 2018). During exercise, my muscles then demanded additional glucose, and my blood sugar may have dropped rapidly enough to trigger symptoms of reactive hypoglycemia: shakiness, sweating, weakness, and fatigue (Morales-Brown, 2025, June 12).
The process is more complex than simply “sugar highs” and “crashes.” Carbohydrates are broken .break down into glucose during digestion, which begins in the mouth. Chewing breaks down food physically, while the enzyme amylase in saliva starts the chemical breakdown by splitting starches into sugars (Peyrot des Gachons & Breslin, 2016). This raises blood glucose levels, which stimulates insulin release from the pancreas. Insulin helps move glucose from the bloodstream into cells. In some people—especially those developing insulin resistance or prediabetes—the insulin response may overshoot, leading to a later drop in blood glucose. Exercise can amplify this effect because active muscles rapidly consume glucose for energy (American Diabetes Association, 2024).
This experience was a wake-up call for me because my hemoglobin A1C is 5.7%, the lower threshold for prediabetes. Hemoglobin A1C reflects average blood glucose levels over approximately the previous three months (American Diabetes Association, 2026).
Like many people, I enjoy and am even addicted to bread, potatoes, pastries, and sweets. Looking back, the subtle changes began during COVID. Before the pandemic, I spent much of the day teaching in person, walking across campus, moving, and interacting with students. During lockdown, I sat for hours teaching online. My physical activity during the day dramatically decreased while my eating habits did not significantly change.
When we are inactive, excess sugars and refined carbohydrates are less likely to be immediately used by muscles for fuel. Instead, repeated spikes in blood glucose and insulin can contribute over time to insulin resistance, weight gain, metabolic dysfunction, and increased inflammation (Ludwig & Ebbeling, 2018).
Although my episodes were minor, they reminded me that lifestyle patterns especially eating ultra-processed foods can increase the risk for chronic diseases such as type 2 diabetes, cardiovascular disease, obesity, and some cancers and dementia (Lane et al., 2024; Menegassi & Vinciguerra, 2025). The scientific literature strongly links obesity, insulin resistance, and type 2 diabetes with increased risk for several cancers, including colorectal and postmenopausal breast cancer (Peper et al., 2026; Scully et al., 2021: Lauby-Secretan et al., 2016). Ultra-processed foods and sugar-sweetened beverages are also associated with increased risk for obesity and metabolic disease; moreover, cancer survivors who consume higher amounts of ultra processed foods face a significantly increased risk of both all-cause and cancer-specific mortality (Hall et al., 2019; Bonaccio et al., 2026). However, cancer is multifactorial, and no single food alone “causes” cancer. Rather, long-term dietary patterns, inactivity, obesity, chronic inflammation, genetics, environmental exposures, sleep, and stress all interact together ( Marino et al., 2024; Dalamaga et al., 2026; Peper et al., 2026).
What to do
The encouraging news is that these processes are often reversible.
Weight, hunger, blood sugar fluctuations, and even A1C are not fixed. They can improve significantly through lifestyle changes. Research consistently shows that reducing ultra-processed foods, lowering intake of refined carbohydrates and sugary beverages, increasing fiber-rich vegetables, improving sleep, reducing stress, and exercising regularly can improve insulin sensitivity and metabolic health (Bird & Hawley, 2017; Vaezi et al., 2025; American Diabetes Association, 2024; Peper et al., 2026).
For many people, continuous glucose monitors (CGMs) can provide powerful real-time feedback (Ehrhardt & Zaghal, 2020). Seeing how specific foods affect your glucose levels can increase awareness and motivate healthier choices. Often, we do not realize how dramatically a muffin, fruit juice, or bowl of white rice may affect blood sugar until we see the data on the screen.
The goal is not perfection or rigid dieting. Instead, it is learning to observe how your body responds and gradually shifting toward foods that support stable energy, satiety, and long-term health.
Before making major dietary changes, watch the superb interview with Dr. David Unwin, a British physician known for his work using lower-carbohydrate dietary approaches to help patients improve type 2 diabetes and metabolic health. His clinical work demonstrates that many patients can significantly improve blood sugar control and sometimes reduce medications through lifestyle changes (Unwin et al., 2020). The video, The Sugar Doctor’s Warning: The “Healthy” Foods Quietly Destroying Your Body! – Dr. David Unwin, is from the podcast, The Diary of a CEO with Steven Bartlett.
The Link Between Diet, Lifestyle, and Cancer Risk: Steps You Can Take
Read the new book, Cancer Reconsidered: Why Environment, Lifestyle, and Immunity Matter More than We Thought, by Erik Peper, Robert Gorter, and Nancy Faass. It explore the many of the lifestyle factors that can increase cancer risk—or help protect against it. The book brings together an extraordinary range of scientific research to illuminate how everyday habits and modern lifestyles influence cancer risk and healing. Drawing from both conventional medicine and integrative approaches, the authors thoughtfully examine the many factors involved in cancer causation while offering hopeful, evidence-based strategies for supporting recovery and restoring health.
What makes this book especially compelling is that it goes far beyond reviewing the science. It translates research into practical, everyday actions people can use to support healing and improve quality of life. At its heart is lifestyle medicine—the recognition that stress management, hope, physical activity, nourishing foods, supportive relationships, community, and resilience during times of crisis profoundly affect health and well-being. The book also offers a detailed and highly practical discussion of sugar metabolism and explains how continuous glucose monitoring sensors (CGMS) with the smartphone app can help people directly observe how specific foods and daily habits influence their blood sugar levels. Instead of relying on abstract nutrition advice, readers learn how to become active investigators of their own health.
Throughout the book, the message is empowering: our daily habits, social connections, attitudes, and environment may influence health as much as—if not more than—genetics alone. The book is available from Amazon: https://www.amazon.com/Cancer-Reconsidered-Environment-Lifestyle-Immunity/dp/1587907402
Listen to the in-depth discussion of this blog created with Google NotebookLM
Addition relevant blogs
References
American Diabetes Association. (2026). Blood glucose and exercise. American Diabetes Association. Retrieved May 24, 2026, from https://diabetes.org/health-wellness/fitness/blood-glucose-and-exercise
American Diabetes Association. (2024). Standards of care in diabetes—2024. Diabetes Care, 47(Suppl. 1). https://diabetesjournals.org/care/issue/47/Supplement_1
Bonaccio, M., Di Castelnuovo, A., Costanzo, S., Ruggiero, E., Esposito, S., Panzera, T., Di Costanzo, G., De Curtis, A., Magnacca, S., Cerletti, C., Donati, M. B., de Gaetano, G., & Iacoviello, L., for the Moli-sani Study Group. (2026). Ultra-processed food and mortality among long-term cancer survivors from the Moli-sani Study: Prospective findings and analysis of biological pathways. Cancer Epidemiology, Biomarkers & Prevention, 35(4), 664–674. https://doi.org/10.1158/1055-9965.EPI-25-0808
Dalamaga, M., Rozani, S., & Petropoulou, D. (2026). Why is colorectal cancer occurring earlier? Metabolic dysfunction, underrecognized carcinogens, and emerging controversies. Current Obesity Reports, 15(1), 24. https://doi.org/10.1007/s13679-026-00700-z
Ehrhardt, N., & Al Zaghal, E. (2020). Continuous glucose monitoring as a behavior modification tool. Clinical Diabetes, 38(2), 126–131. https://doi.org/10.2337/cd19-0037
Hall, K. D., Ayuketah, A., Brychta, R., Cai, H., Cassimatis, T., Chen, K. Y., Chung, S. T., Costa, E., Courville, A., Darcey, V., Fletcher, L. A., Forde, C. G., Gharib, A. M., Guo, J., Howard, R., Joseph, P. V., McGehee, S., Ouwerkerk, R., Raisinger, K., … Zhou, M. (2019). Ultra-processed diets cause excess calorie intake and weight gain: An inpatient randomized controlled trial. Cell Metabolism, 30(1), 67–77. https://doi.org/10.1016/j.cmet.2019.05.008
Lane, M. M., Gamage, E., Du, S., Ashtree, D. N., McGuinness, A. J., Gauci, S., Baker, P., Lawrence, M., Rebholz, C. M., Srour, B., Touvier, M., Jacka, F. N., O’Neil, A., Segasby, T., & Marx, W. (2024). Ultra-processed food exposure and adverse health outcomes: Umbrella review of epidemiological meta-analyses. BMJ, 384, e077310. https://doi.org/10.1136/bmj-2023-077310
Lauby-Secretan, B., Scoccianti, C., Loomis, D., Grosse, Y., Bianchini, F., & Straif, K. (2016). Body fatness and cancer—Viewpoint of the IARC Working Group. New England Journal of Medicine, 375(8), 794–798. https://doi.org/10.1056/NEJMsr1606602
Ludwig, D. S., & Ebbeling, C. B. (2018). The carbohydrate-insulin model of obesity: Beyond “calories in, calories out.” JAMA Internal Medicine, 178(8), 1098–1103. https://doi.org/10.1001/jamainternmed.2018.2933
Marino, P., Mininni, M., Deiana, G., Marino, G., Divella, R., Bochicchio, I., Giuliano, A., Lapadula, S., Lettini, A. R., & Sanseverino, F. (2024). Healthy lifestyle and cancer risk: Modifiable risk factors to prevent cancer. Nutrients, 16(6), 800. https://doi.org/10.3390/nu16060800
Menegassi, B., & Vinciguerra, M. (2025). Ultraprocessed food and risk of cancer: Mechanistic pathways and public health implications. Cancers, 17(13), 2064. https://doi.org/10.3390/cancers17132064
Morales-Brown, P. (2025, June 12). What is reactive hypglycemia. Medical News Today. Accessed May 24, 2026. https://www.medicalnewstoday.com/articles/reactive-hypoglycemia
Peper, E., Gorter, R., & Faass, N. (2026). Cancer reconsidered: Why environment, lifestyle, and immunity matter more than we thought. Biofeedback Health. https://www.amazon.com/Cancer-Reconsidered-Environment-Lifestyle-Immunity/dp/1587907402
Peyrot des Gachons, C., & Breslin, P. A. S. (2016). Salivary amylase: Digestion and metabolic syndrome. Current Diabetes Reports, 16, 102. https://doi.org/10.1007/s11892-016-0794-7
Scully, T., Ettela, A., LeRoith, D., & Gallagher, E. J. (2021). Obesity, type 2 diabetes, and cancer risk. Frontiers in Oncology, 10, 615375. https://doi.org/10.3389/fonc.2020.615375
Unwin, D., Khalid, A. A., Unwin, J., Crocombe, D., Delon, C., Martyn, K., Hasan, M., & Tobin, S. D. (2020). Insights from a general practice service evaluation supporting a lower carbohydrate diet in patients with type 2 diabetes mellitus and prediabetes: A secondary analysis of routine clinic data including HbA1c, weight and prescribing over 6 years. BMJ Nutrition, Prevention & Health, 3(2), 285–294. https://doi.org/10.1136/bmjnph-2020-000072
Vaezi, S., Freeling, J. L., de Vargas, B. O., Weidauer, L., Shoemaker, M. E., Sanders, W. M., & Dey, M. (2025). Impacts of minimally-processed omnivorous vs lacto-ovo-vegetarian diets on insulin sensitivity, lipid profile, and adiposity in older adults: Secondary findings from a randomized crossover feeding trial. Clinical Nutrition, 55, 90–103. https://doi.org/10.1016/j.clnu.2025.10.010
Are food companies responsible for the epidemic in diabetes, cancer, dementia and chronic disease and do their products need to be regulated like tobacco? Is it time for a class action suit?
Posted: July 15, 2023 Filed under: behavior, cancer, Evolutionary perspective, health, Nutrition/diet, self-healing | Tags: dementia, diabetes, diet, high fructose corn syrup, mortality, obsity, smoking, sugar, ultra-processed foods, UPF 5 CommentsAdapted from: Peper, E. & Harvey, R. (2024). Are Food Companies Responsible for the Epidemic in Diabetes, Cancer, Dementia and Chronic Disease and Do Their Products Need to Be Regulated Like Tobacco? Is It Time for a Class Action Suit? Thownsend Letter-the examiner of alternative medicine. https://www.townsendletter.com/e-letter-26-ultra-processed-foods-and-health-issues/
Erik Peper, PhD and Richard Harvey, PhD

Why are one third of young Americans becoming obese and at risk for diabetes?
Why are heart disease, cancer, and dementias occurring earlier and earlier? Is it genetics, environment, foods, or lifestyle?
Is it individual responsibility or the result of the quest for profits by agribusiness and the food industry?
Like the tobacco industry that sells products regulated because of their public health dangers, is it time for a class action suit against the processed food industry? The argument relates not only to the regulation of toxic or hazardous food ingredients (e.g., carcinogenic or obesogenic chemicals) but also to the regulation of consumer vulnerabilities. Addressing vulnerabilities to tobacco products include regulations such as how cigarette companies may not advertise their products for sale within a certain distance from school grounds.
Is it time to regulate nationally the installation of vending machines on school grounds selling sugar-sweetened beverages? Students have sensitivity to the enticing nature of advertised, and/or conveniently available consumable products such as ‘fast foods’ that are highly processed (e.g., packaged, preserved and practically imperishable). Whereas ‘processed foods’ have some nutritive value, and may technically pass as ‘nutritious’ food, the quality of processed ‘nutrients’ can be called into question. For the purpose of this blog other important questions to raise relate to ingredients which, alone or in combination, may contribute to the onset of or, the acceleration of a variety of chronic health outcomes related to various kinds of cancers, cardiovascular diseases, and diabetes.
It may be an over statement to suggest that processed food companies are directly responsible for the epidemic in diabetes, cancer, dementia and chronic disease and need to be regulated like tobacco. On the other hand, processed food companies should become much more regulated than they are now.
More than 80 years ago, smoking was identified as a significant factor contributing to lung cancer, heart disease and many other disorders. In 1964 the Surgeon Generals’ report officially linked smoking to deaths of cancer and heart disease (United States Public Health Service, 1964). Another 34 years pased before California prohibited smoking in restaurants in 1998 and, eventually inside all public buildings. The harms of smoking tobacco products were well known, yet many years passed with countless deaths and suffering which could have been prevented before regulation of tobacco products took place. Reviewing historical data there is about a 20 year delay (e.g., a whole generation) before death rates decrease in relation to when regulations became effective and smoking rates decreased, as shown in figure 1.

Figure 1. The relationship between smoking and lung cancer. Reproduced by permission from Roser, M. (2021). Smoking: How large of a global problem is it? And how can we make progress against it? Our world in data.
During those interim years before government actions limited smoking more effectively, tobacco companies hid data regarding the harmful effects of smoking. Arguably, the ‘Big Tobacco’ industry paid researchers to publish data which could confuse readers about tobacco product harm. There is evidence of some published articles suggesting that the harm of cigarette smoking was a hoax– all for the sake of boosting corporate profits (Bero, 2005).
Now we are experiencing a similar problem with the processed food industry. It has been suggested that alongside smoking and vaping, opioid use, a sedentary ‘couch potato’ lifestyle, and lack of exercise, ultra-processed food (UPF) that we eat severely affects our health.
Ultra-processed foods, which for many constitutes a majority of calories ranging from 55% to over 80% of the food they eat, contain chemical additives that trick the tastebuds, mouth and eventually our brain to desire those processed foods and eat more of them (Srour et al., 2022).
What are ultra-processed foods? Any foods that your great grandmother would not recognize as food. This includes all soft drinks, highly processed chips, additives, food coloring, stabilizers, processed proteins, etc. Even oils such as palm oil, canola oil, or soybean are ultra processed since they heated, highly processed with phosphoric acid to remove gums and waxes, neutralized with chemicals, bleached, and deodorized with high pressure steam (van Tulleken, 2023).
The data is clear! Since the 1970s obesity and inflammatory disease have exploded after ultra-processed foods became the constituents of the modern diet as shown in figure 2.
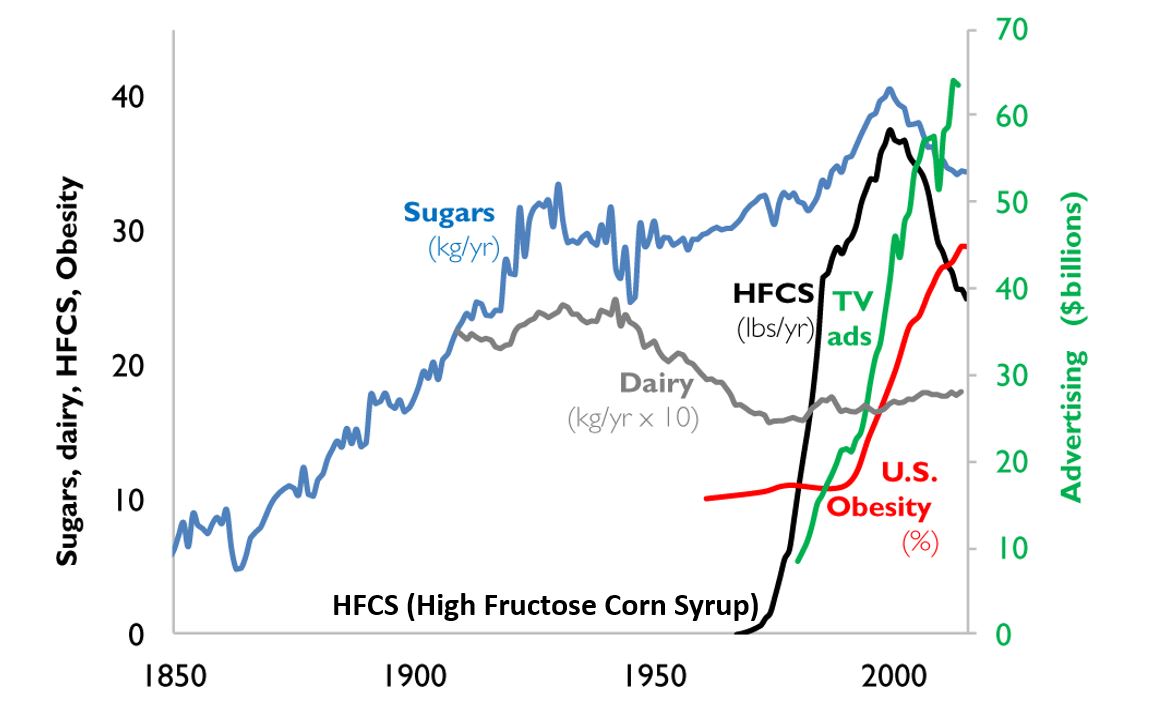
Figure 2. A timeline from 1850 to 2000 reflects the increase in use of refined sugar and high fructose corn syrup (HFCS) to the U.S. diet, together with the increase in U.S. obesity rate. The data for sugar, dairy and HFCS consumption per capita are from USDA Economic Research Service (Johnson et al., 2009) and reflects historical estimates before 1967 (Guyenet et al., 2017). The obesity data (% of U.S. adult population) are from the Robert Wood Johnson Foundation’s Trust for America’s Health. (stateofobesity.org). Total U.S. television advertising data are from the World Advertising Research Center (www.warc.com). The vertical measure (y–axis) for kilograms per year (kg/yr) on the left covers all data except advertising expenditures, which uses the vertical measure for advertising on the right. Reproduced by permission from Bentley et al, 2018.
This graph clearly shows a close association between the years that high fructose corn syrups (HFCS) were introduced into the American diet and an increase in TV advertising with corresponding increase in obesity. HFCS is an ultra-processed food and is a surrogate marker for all other ultra-processed foods. The best interpretation is that ultra-processed foods, which often contain HFCS, are a causal factor of the increase in obesity, and diabetes and in turn are risk factors for heart disease, cancers and dementias.
Ultra-processed foods are novel from an evolutionary perspective.
The human digestive system has only recently encountered sources of calories which are filled with so many unnatural chemicals, textures and flavors. Ultra-processed foods have been engineered, developed and product tested to increase the likelihood they are wanted by consumers and thereby increase sales and profits for the producers. These foods contain the ‘right amount’ processed materials to evoke the taste, flavor and feel of desired foods that ‘trick’ the consumer it eat them because they activate evolutionary preference for survival. Thus, these ultra-processed foods have become an ‘evolutionary trap’ where it is almost impossible not to eat them. We eat the food because it capitalized on our evolutionary preferences even though doing so is ultimately harmful for our health (for a detailed discussion on evolutionary traps, see Peper, Harvey & Faass, 2020).
An example is a young child wanting the candy while waiting with her parents at the supermarket checkout line. The advertised images of sweet foods trigger the cue to eat. Remember, breast milk is sweet and most foods in nature that are sweet in taste, provide calories for growth and survival and are not harmful. Calories are essential of growth. Thus, we have no intrinsic limit on eating sweets unlike foods that taste bitter.
As parents, we wish that our children (and even adults) have self-control and no desire to eat the candy or snacks that is displayed at eye level (eye candy) especially while waiting at the cashier. When reflecting about food advertising and the promotion of foods that are formulated to take advantage of ‘evolutionary traps’, who is responsible? Is it the child, who does not yet have the wisdom and self-control or, is it the food industry that ultra-processes the foods and adds ingredients into foods which can be harmful and then displays them to trigger an evolutionary preference for food that have been highly processed?
Every country that has adapted the USA diet of ultra-processed foods has experienced similar trends in increasing obesity, diabetes, cardiovascular disease, etc. The USA diet is replacing traditional diets as illustrated by the availability of Coca-Cola. It is sold in over 200 countries and territories (Coca-Cola, 2023).
An increase in ultra-processed foods by 10 percent was associated with a 25 percent increase in the risk of dementia and a 14 per cent increase in the risk of Alzheimers’s (Li et al., 2022). More importantly, people who eat the highest proportion of their diet in ultra-processed foods had a 22%-62% increased risk of death compared to the people who ate the lowest proportion of processed foods (van Tulleken, 2023). In the USA, counties with the highest food swamp scores (the availability of fast food outlets in a county) had a 77% increased odds of high obesity-related cancer mortality (Bevel et al., 2023). The increase risk has also been observed for cardiovascular disease, coronary heart disease, cerebrovascular disease and all cause mortality as is shown in figure 3 (Srour et al., 2019; Rico-Campà et al., 2019).

Figure 3. Association between consumption of ultra-processed foods and all cause mortality. Reproduced from Rico-Campà et al, 2019.
The harmful effects of UPF holds up even when correcting for the amount of sugars, carbohydrates or fats in the diet and controlling for socio economic variables.
The logic that underlies this perspective is based upon the writing by Nassim Taleb (2012) in his book, Antifragile: Things That Gain from Disorder (Incerto). He provides an evolutionary perspective and offers broad and simple rules of health as well as recommendations for reducing UPF risk factors:
- Assume that anything that was not part of our evolutionary past is probably harmful.
- Remove the unnatural/unfamiliar (e.g. smoking/ e-cigarettes, added sugars, textured proteins, gums, stabilizers (guar gum, sodium alginate), emulsifiers (mono-and di-glycerides), modified starches, dextrose, palm stearin, and fats, colors and artificial flavoring or other ultra-processed food additives).
What can we do?
The solutions are simple and stated by Michael Pollan in his 2007 New York Times article, “Eat food. Not too much. Mostly Plants.” Eat foods that your great grandmother would recognize as foods (Pollan, 2009). Do not eat any of the processed foods that fill a majority of a supermarket’s space.
- Buy only whole organic natural foods and prepare them yourself.
- Request that food companies only buy and sell non-processed foods.
- Demand government action to tax ultra-processed food and limit access to these foods. In reality, it is almost impossible to expect people to choose healthy, organic foods when they are more expensive and not easily available in the American ‘food swamps and deserts’ (the presence of many fast food outlets or the absence of stores that have fresh produce and non-processed foods). We do have a choice. We can spend more money now for organic, health promoting foods or, pay much more later to treat illness related to UPF.
- It is time to take our cues from the tobacco wars that led to regulating tobacco products. We may even need to start class action suits against producers and merchants of UPF for causing increased illness and premature morbidity.
For more background information and the science behind this blog, read, the book, Ultra-processed people, by Chris van Tulleken.

Look at the following blogs for more background information.
References
Bentley, R.A., Ormerod, P. & Ruck, D.J. (2018). Recent origin and evolution of obesity-income correlation across the United States. Palgrave Commun 4, 146. https://doi.org/10.1057/s41599-018-0201-x
Bero, L. A. (2005). Tobacco Industry Manipulation of Research. Public Health Reports (1974-), 120(2), 200–208. http://www.jstor.org/stable/20056773
Bevel, M.S., Tsai, M., Parham, A., Andrzejak, S.E., Jones, S., & Moore, J.X. (2023). Association of Food Deserts and Food Swamps With Obesity-Related Cancer Mortality in the US. JAMA Oncol. 9(7), 909–916. https://doi.org/10.1001/jamaoncol.2023.0634
Coca-Cola. (2023). More on Coca-Cola. Accessed July 14, 2023. https://www.coca-cola.co.uk/our-business/faqs/how-many-countries-sell-coca-cola-is-there-anywhere-in-the-world-that-doesnt
Johnson, R.K., Appel, L.J., Brands, M., Howard, B.V., Lefevre, M., Lustig, R.H., Sacks, F., Steffen, L.M., & Wylie–Rosett, J. (2009). Dietary sugars intake and cardiovascular health: a scientific statement from the American Heart Association. Circulation, 120(10), 1011–1020. https://doi.org/10.1161/CIRCULATIONAHA.109.192627
Li, H., Li, S., Yang, H., et al, 2022. Association of ultraprocessed food consumption with the risk of dementia: a prospective cohort study. Neurology, 99, e1056-1066. https://doi.org/10.1212/WNL.0000000000200871
Peper, E., Harvey, R. & Faass, N. (2020). TechStress: How Technology is Hijacking Our Lives, Strategies for Coping, and Pragmatic Ergonomics. Berkeley: North Atlantic Books, pp 18-22, 151. https://www.amazon.com/Beyond-Ergonomics-Prevent-Fatigue-Burnout/dp/158394768X/ref=sr_1_1?crid=1U9Y82YO4DKKP&keywords=erik+peper&qid=1689372466&sprefix=erik+peper%2Caps%2C187&sr=8-1
Pollan, M. (2007). Unhappy meals. The New York Times Magazine. https://www.nytimes.com/2007/01/28/magazine/28nutritionism.t.html
Pollan, M. (2009). Food Rules: An Eater’s Manual. New York: Penguin Books. https://www.amazon.com/Food-Rules-Eaters-Michael-Pollan/dp/014311638X/ref=tmm_pap_swatch_0?_encoding=UTF8&qid=1689373484&sr=8-2
Rico-Campà, A., Martínez-González, M. A., Alvarez-Alvarez, I., de Deus Mendonça, R., Carmen de la Fuente-Arrillaga, C., Gómez-Donoso, C., & Bes-Rastrollo, M. (2019). Association between consumption of ultra-processed foods and all cause mortality: SUN prospective cohort study. BMJ; 365: l1949 https://doi.org/10.1136/bmj.l1949
Roser, M. (2021).Smoking: How large of a global problem is it? And how can we make progress against it? Our world in data. Assessed July 13, 2023. https://ourworldindata.org/smoking-big-problem-in-brief
Srour, B., Fezeu, L.K., Kesse-Guyot, E.,Alles, B., Mejean, C…(2019). Ultra-processed food intake and risk of cardiovascular disease: prospective cohort study (NutriNet-Santé) BMJ,365:l1451. https://doi.org/10.1136/bmj.l1451
Srour, B., Kordahi, M. C., Bonazzi, E., Deschasaux-Tanguy, M., Touvier, M., & Chassaing, B. (2022). Ultra-processed foods and human health: from epidemiological evidence to mechanistic insights. The Lancet Gastroenterology & Hepatology. https://doi.org/10.1016/S2468-1253(22)00169-8
Taleb, N. N. (2012). Antifragile: Things That Gain from Disorder (Incerto). New York: Random House Publishing Group. (Kindle Locations 5906-5908). https://www.amazon.com/Antifragile-Things-Disorder-ANTIFRAGILE-Hardcover/dp/B00QOJ6MLC/ref=sr_1_4?crid=3BISYYG0RPGW5&keywords=Antifragile%3A+Things+That+Gain+from+Disorder+%28Incerto%29&qid=1689288744&s=books&sprefix=antifragile+things+that+gain+from+disorder+incerto+%2Cstripbooks%2C158&sr=1-4
Van Tulleken, C. (2023). Ultra-processed people. The science behind food that isn’t food. New Yoerk: W.W. Norton & Company. https://www.amazon.com/gp/product/1324036729/ref=ox_sc_act_title_1?smid=ATVPDKIKX0DER&psc=1
United States Public Health Service. (1964). The 1964 Report on Smoking and Health. United States. Public Health Service. Office of the Surgeon General. https://profiles.nlm.nih.gov/spotlight/nn/catalog?f%5Bexhibit_tags%5D%5B%5D=smoking
Read The case against sugar
Posted: February 18, 2017 Filed under: Nutrition/diet, Uncategorized | Tags: Alzheimer, cancer, carbohydrates, diabetes, heart disease, sugar 11 CommentsAn ounce of prevention is worth a pound of cure.
Albert Schweitzer began working in equatorial lowlands of West Africa in 1913. He was astonished to encounter no cases of cancer among the thousands of native patients he saw each year. However, as the natives [took to] living more and more after the manner of the whites, cancer in his patient population became ever more frequent (Taubes, 2016, pp 257).
Wise elders, grand parents or statesmen have been traditional roles for aging adults. Wisdom transforming into Alzheimer’s disease does not compute (Peper, 2014).
In 1960’s Surgeon Captain T. L. Cleave proposed that common western diseases (diabetes, colon cancer, ischemic heart disease, gallstones, obesity, diverticulosis, and dental carries), to which I would add Alzheimer’s disease, autoimmune diseases and allergies, could not be due primarily to genetic factors but to new factors in the environment to which man had not yet had time to adapt (Cleaves et al, 1969). As he states, “One such factor was the processing of food which resulted in the consumption of large quantities of pure sugar and starch. This led to disease because man was evolutionary adjusted to eating smaller amounts of carbohydrates intimately mixed with fiber and protein.”
Clinicians and epidemiologist have consistently reported that none western cultures, whether the Masai in Africa, the Inuit in Northern Canada, the Japanese in Japan, or the Native American, had very low incidences of these western diseases. Yet, when these people adapted a western diet of highly refined carbohydrates and sugar the prevalence of these diseases increased and approached the incidence in western cultures (Burkitt & Trowell, 1975; Taubes, 2016).
Historically these illness were initially observed in the ruling class. The affluent class was privileged and tended to eat more refined carbohydrates and sugars (white bread, cakes, pastries and sugar in coffee and tea). It is only recently that this class effect is reversed. Lower economic classes tend have a higher prevalence of these western diseases. Affluent people can afford and often eat low processed organic foods while economically disadvantaged people cannot afford low processed foods and instead eat predominantly highly processed carbohydrate and refined foods.
Highly refined processed foods and sugar–not fats–are significant risk factors for the development diabetes and cardiovascular disease and mortality (Imamura et al, 2015; Taubes, 2016; Yang et al, 2014) . What is not as well known is that some cancers and Alzheimer’s disease also correlates with the increase intake of refined carbohydrates and sugar (Das, 2015; Kandimalla et al, 2016; Peper, 2014).
It is highly likely that the increase in beta-amyloid protein plagues in the brain is not the cause of the Alzheimer’s but the brain’s defense mechanism to protect it from the fluctuating high insulin and glucose levels. A high sugar and simple carbohydrate diet are risk factors for inflammatory diseases such as diabetes, heart disease and metabolic syndrome. These inflammatory diseases are recognized as a precursor for Alzheimer’s. Alzheimer’s is sometimes described as Type 3 diabetes (Kandimalla et al, 2016; Steen et al, 2005).
Taking the perspective that foods are significant risk factors for the development of these western diseases, the focus should be on prevention and less on treatment. The research to develop drugs to treat Alzheimer’s have up till now been unsuccessful despite that the billions spent on attempting to develop new drugs. For example, the pharmaceutical company Eli Lilly has spent 3.7 billion dollars over the last decade while the National Institutes of Health spends more than half a billion dollars a year on pursuit of treatment (Coghlan, 2017).
The treatments cost of these western diseases, which at best ameliorate the disorders, is overwhelming. In the USA, we spent $147 billion to treat obesity and $116 billion to treat diabetes. While the medical costs to treat diabetes for a single patient is about $6000/year or $400,000/lifetime (Pollan, 2009).
As a refined carbohydrates and high sugar diet is a risk factor for western diseases, the focus should be on prevention. Thus, reduce sugar and refined carbohydrates intake and increase high fiber vegetable. To implement such a simple preventative measure means:
- Educate the public about the harm of sugars and refined carbohydrate foods.
- Ban advertising of foods that are high in sugar and refined carbohydrates.
- Reward companies to produce foods low in sugar and refined carbohydrates.
- Tax food products high in sugar and refined carbohydrates just as tobacco has been taxed.
I am positive that in the future when we look back at the 20th and early 21st century, we will be appalled that the government allowed people to poison themselves with sugar and highly refined carbohydrates. Just as we now warn against the harm of tobacco, limit the sales to minors, and have ongoing public health stop smoking campaigns.
For much more information, read science writer Gary Taubes superb well researched and engaging book, The case against sugar.

References:
Burkitt, D.P. & Trowell, H.C. (1975). Refined carbohydrate foods and disease: Some implications of dietary fibre. York: Academic Press.
Cleave, T.L., Campbell, G.D., & Painter, N.S. (1969). Diabetes, coronary thrombosis and the saccharine disease, 2nd ed. Bristol, UK: John Wright.
Coghlan, A. 2017). The Alzheimer’s problem. New Scientist, 233(3110), 22-23.
Das, U. N. (2015). Sucrose, fructose, glucose, and their link to metabolic syndrome and cancer. Nutrition, 31(1), 249-257.
Imamura, F., O’Connor, L., Ye, Z., Mursu, J., Hayashino, Y., Bhupathiraju, S. N., & Forouhi, N. G. (2015). Consumption of sugar sweetened beverages, artificially sweetened beverages, and fruit juice and incidence of type 2 diabetes: systematic review, meta-analysis, and estimation of population attributable fraction. Bmj, 351, h3576.
Kandimalla, R., Thirumala, V., & Reddy, P. H. (2016). Is Alzheimer’s disease a Type 3 Diabetes? A critical appraisal. Biochimica et Biophysica Acta (BBA)-Molecular Basis of Disease.
Peper, E. (2014). Affluenza: Transforming Wisdom into Alzheimer’s Disease with Affluent Malnutrition and Immobility. Neuroconnections, 9(2), 32-35.
Pollan, M. (2009). Big food vs. big insurance. New York Times, September 10, A29.
Steen, E., Terry, B.M. Rivera, E.J., Cannon, J.L., Neely, T.R., Tavares, R., Xu, X. J., Wands, J.R., & de al Monte, S. M. (2005). Impaired insulin and insulin-like growth factor expression and signaling mechanisms in Alzheimer’s disease-is this type 3 diabetes? Journal of Alzheimer’s Disease, 7(1), 53-80.
Taubes, G. (2016). The case against sugar. New York: Alfred A. Knopf.
Yang, Q., Zhang, Z., Gregg, E. W., Flanders, W. D., Merritt, R., & Hu, F. B. (2014). Added sugar intake and cardiovascular diseases mortality among US adults. JAMA internal medicine, 174(4), 516-524.
Healthy movement is the new aging
Posted: February 11, 2017 Filed under: Exercise/movement, self-healing, Uncategorized | Tags: aging, diabetes, evolution, exercise, health, interval training, sugar 2 CommentsBorn on 26 November 1911, Mr Robert Marchand and 105 years old, managed cycling 22.55 km (14 miles) at the national velodrome and set a new record for the furthest distance cycled in one hour for riders over 105. (Reynolds, 2017).
Meet 105-year-old Robert Marchand, the centenarian cyclist chasing a new record: https://www.youtube.com/watch?v=Ey48j6dDNEo
As people age there is an increase in Western Diseases such as hypertension, diabetes, gout, cancer, dementia and decreases in physical fitness (Milanović et al, 2013; Tauber, 2016). To assume that the cause of these illnesses is the natural process of aging may be too simplistic. Although aging does affect physiology, there are other factors that contribute to the increase in “Western Diseases” such as diet, lifestyle and genetics.
A significant contributing factor of Western Diseases is diet especially the increase in sugar and simple carbohydrates. Whether you are Pima, Tohono O’odham, and Navajo American Indian Tribes in Arizona, Intuits in Northern Canada, Japanese Americans, or indigenous populations of Kenya, when these people stopped eating their traditional diet and adapted the western high glucose/fructose/simple carbohydrate diet, the degenerative Western Diseases exploded (Bjerregaard et al, 2004; Burkitt & Trowell, 1975; Knowler et al, 1990; Tauber, 2016). Diabetes, hypertension, and cancer which were previously rare skyrocketed within one generation after adapting the Western life style diet. In some of these populations, 30% or more of the adults have diabetes and a significant increase in breast cancer.
The reduction of episodic high intensity physical activity and being sedentary are additional risk factors for the onset of diabetes and cardiovascular disease (Dulloo et al, 2017). As Mensing & Mekel (2015) state, “Sitting is the new smoking.” Sitting encourages more sitting which leads to nonuse of muscles and causes neural and muscle atrophy. Our physiology is efficient and will prune/eliminate what is redundant. This is reflected in the popular phrase, “Use it or lose it.” As we sit for hours in front of digital devices, use escalators, elevators, or drive cars, we are not using the muscles involved in dynamic movement. We are usually unaware of this degenerative process. Instead, we may experience difficulty walking up the stairs which encourages us to take the escalator or elevator. When we do not use the muscles or are limited in movement by discomfort and pain, we move less. As we move less, we become weaker which is often labeled as aging instead of non use.
Just, because most people loose fitness, it may not represent what is possible or optimum. Instead, we may want to emulate the diet and fitness program of Mr. Robert Marchand who at age 103 set a new world record and improved the distance bicycled in one hour from 24.25 km at the age of 101 to 26.92 km at the age of 103. A 11% improvement! As New York Times science writer Gretchen Reynolds reports, “Lifestyle may also matter. Mr. Marchand is “very optimistic and sociable,” The researcher who did the study, Dr. Billat says, “with many friends,” and numerous studies suggest that strong social ties are linked to a longer life. His diet is also simple, focusing on yogurt, soup, cheese, chicken and a glass of red wine at dinner (Reynolds, 2017).
The improvement in bicycling performance and physiological indicators such as ⩒O2max increased (31 to 35 ml.kg-1min-1; +13%), appeared to be due to a change in his training regimen (Billat et al 2016). At age 101 he changed his bicycling training program from riding at a steady speed for one hour to riding 80% at an easy pace and 20% at high intensity. This is a type of interval training and includes enough recovery allows the body the recover and strengthen. This analogous to our evolutionary movement pattern of walking interspersed with short distance high intensity running.
As a hunter and gather we often moved steadily and then had to run very fast to escape a predator or catch an animal. After extreme exertion, we would rest and regenerate (if we did not escape we would be lunch for the predator). Thus episodic high intensity activity with significant rest/regenerative periods is the movement pattern that allowed our species to survive and thrive. Research studies have confirmed that high intensity interval training offers more physiological benefits–increases cardiorespiratory fitness which is a strong determinant of morbidity and mortality– than moderate intensity continuous training (Weston et al, 2014).
Thus when Mr. Marchard changed his exercise pattern from moderate intensity continuous training to high intensity interval training with enough recovery time he set a new world record at age 103. Two years later he set a new world record at age 105.
Exercise improves brain function and interval training appears to improve brain function most. When rats had prolonged exercise, the brain’s stores of energy is significantly lowered in the frontal cortex and hippocampus all areas which area involved in thinking and memory. If on the other hand, the animals had a single intense bout of exercise and were allowed to rest and feed than the brain levels of glycogen was 60% high in the frontal and hippocampus areas. This suggest that the brain can then function better (Matsui et al, 2012).
This perspective is supported by the evolutionary hypothesis discussed by Neuroscientist Daniel Wolpert who points out that brains evolved, not to think or feel, but to direct movement. When movement is no longer needed the brain shrinks and gets reabsorbed which is illustrated by the sea squirt. This animal swims as a juvenile and then anchors on a rock and is passively moved by the currents. Once anchored, it no longer needed to coordinate movement and reabsorb its own nervous system. See Daniel Wolpert’s remarkable TED talk, The real reasons for brains.
The remarkable feat of Mr. Marchand offers suggestions for our own health. Enjoy healthy movement and exercise and incorporate our evolutionary movement patterns: episodic high intensity followed by regeneration. At the same time include a healthy diet by reducing sugars and simple carbohydrates. Finally, it helps to have the right genes.
References:
Billat, V. L., Dhonneur, G., Mille-Hamard, L., Le Moyec, L., Momken, I., Launay, T., & Besse, S. (2016). Case Studies in Physiology: Maximal Oxygen Consumption and Performance in a Centenarian Cyclist. Journal of Applied Physiology, jap-00569. http://jap.physiology.org/content/jap/early/2016/12/29/japplphysiol.00569.2016.full.pdf
Bjerregaard, P., Kue Young, T., Dewailly, E., & Ebbesson, S. O. (2004). Review Article: Indigenous health in the Arctic: an overview of the circumpolar Inuit population. Scandinavian Journal of Social Medicine, 32(5), 390-395. https://www.researchgate.net/publication/51366099_Indigenous_Health_in_the_Arctic_An_Overview_of_the_Circumpolar_Inuit_Population
Burkitt, D.P. & Trowell, H.C. eds. (1975). Refined carbohydrate foods and disease: Some implications of dietary fibre. New York: Academic Press.
Dulloo, A. G., Miles‐Chan, J. L., & Montani, J. P. (2017). Nutrition, movement and sleep behaviours: their interactions in pathways to obesity and cardiometabolic diseases. Obesity Reviews, 18(S1), 3-6.
Knowler, W. C., Pettitt, D. J., Saad, M. F., & Bennett, P. H. (1990). Diabetes mellitus in the Pima Indians: incidence, risk factors and pathogenesis. Diabetes/metabolism reviews, 6(1), 1-27.
Matsui, T., Ishikawa, T., Ito, H., Okamoto, M., Inoue, K., Lee, M. C., … & Soya, H. (2012). Brain glycogen supercompensation following exhaustive exercise. The Journal of physiology, 590(3), 607-616.
Mensing, M., & Mekel, O. C. L. (2015). Sitting is the new smoking-Modelling physical activity interventions in North Rhine-Westphalia. The European Journal of Public Health, 25(suppl 3), ckv171-037.
Milanović, Z., Pantelić, S., Trajković, N., Sporiš, G., Kostić, R., & James, N. (2013). Age-related decrease in physical activity and functional fitness among elderly men and women. Clinical interventions in aging, 8, 549-556.
Reynolds, G. (2017, February 8). Lessons on Aging Well, From a 105-Year-Old Cyclist. Retrieved from: https://www.nytimes.com/2017/02/08/well/move/lessons-on-aging-well-from-a-105-year-old-cyclist.html?rref=collection%2Fsectioncollection%2Fhealth&action=click&contentCollection=health®ion=rank&module=package&version=highlights&contentPlacement=5&pgtype=sectionfront
Taubes, G. (2016). The Case Against Sugar. New York: Alfred A. Knopf.
Weston, K. S., Wisløff, U., & Coombes, J. S. (2014). High-intensity interval training in patients with lifestyle-induced cardiometabolic disease: a systematic review and meta-analysis. British journal of sports medicine, 48(16), 1227-1234. http://www.rcsi.ie/files/facultyofsportsexercise/20141201122758_High-intensity%20interval%20traini.pdf
Wolpert, D. (2011) The Real Reason for Brains. http://www..com/tatedlks/daniel_wolpert_the_real_reason_for_brains.html
Youtube video: Meet 105-year-old Robert Marchand, the centenarian cyclist chasing a new record: https://www.youtube.com/watch?v=Ey48j6dDNEo
Understanding marketing to doctors, food waste and sugar consumption through humor
Posted: August 7, 2015 Filed under: Nutrition/diet, Uncategorized | Tags: diet, drugs, food, marketing, pharmaceutical industry, sugar Leave a commentThe Last Week Tonight Show with John Oliver is a superb presentation of the problems and solutions about our health and food systems. Using humor, John William Oliver hosts the weekly HBO program on Sundays at 11pm and provides superb documentation of the corruption and marketing strategies that often negatively affect our health, diet and budget.
For evidence based–yet humorous–reporting watch the following episodes;
Marketing to Doctors (HBO). Pharmaceutical companies spend billions of dollars marketing drugs to doctors (published on Feb 8, 2015).
Food Waste (HBO). Producers, sellers, and consumers waste tons of food. John Oliver discusses the shocking amount of food we don’t eat (published on Jul 19, 2015).
Sugar (HBO). Sugar. It’s in everything!
Is it good for us? Well, the sugar industry thinks so (published on Oct 26, 2014).
For additional information, see the following blogs:
Be aware of evolutionary/environmental traps
Over diagnosed: Should I have more tests?
Cut out the sugar-it is toxic!
Posted: March 3, 2013 Filed under: Nutrition/diet, Uncategorized | Tags: diabetes, diet, sugar 3 CommentsPutting it simply: Too much sugar in our diet is harmful and when we return to our paleolithic diet, health tends to improve.
Sugar intake in all different forms is the single most important ingredient that contributes to diabetes. In the last one hundred years our sugar intake has radically increased as is shown in figure 1.
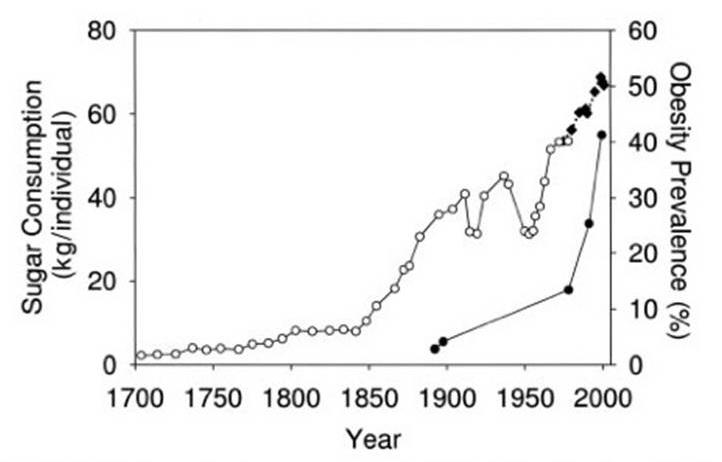
Figure 1. Sugar intake per capita in the United Kingdom from 1700 to 1978 and in the United states from 1975-2000. The line on the right with black dots is the obesity rates in the United States in non-Hispanic white men aged 60-69 y. Values for 1880-1910 are based on studies conducted in male Civil War veterans aged 50-59y. From: Johnson RJ et al, AJCN 2007; 86:899-906; Initial source: http://www.indiana.edu/~oso/Fructose/Fructose.html
Even though research and clinical findings over the last one hundred years have shown that increased sugar and processed simple carbohydrate intake are contributing factors to many illnesses ranging from diabetes, obesity, cancer and even epilepsy, the data is now undisputable. As Mark Bittman wrote in the New York Times on February 27th, “Sugar is indeed toxic. It may not be the only problem with the Standard American Diet, but it’s fast becoming clear that it’s the major one.”
When researchers accounted for poverty, aging, exercise, total food intake, and other factors, increased sugar intake increased diabetes and decreased sugar decreased diabetes. As the authors state, “for every 150 kcal/person/day increase in sugar availability (about one can of soda/day) there was associated with increased diabetes prevalence by 1.1% (p <0.001).” (Basu S, Yoffe P, Hills N, Lustig RH (2013) The Relationship of Sugar to Population-Level Diabetes Prevalence: An Econometric Analysis of Repeated Cross-Sectional Data. PLoS ONE 8(2): e57873. doi:10.1371/journal.pone.0057873)
Presently, the level of proof linking sugar to diabetes is equal to if not better than the level of proof that linked cigarette smoking to lung cancer and other illnesses. Despite the overwhelming scientific data, it will be an uphill battle to change our diet and diet recommendations from the highly processed high glycemic index diet that promotes inflammation and diabetes to a low glycemic index Paleolithic diet that supports health. The major agricultural and food processing businesses have significant influence with the USA Government (for Senate and House members lobbying pays for the election), the FDA and USDA priorities are also highly affected through direct and indirect lobbying efforts or by the financial reward to be offered a job in the agribusiness after working for the FDA or USDA. In the USA lobbying and being rewarded with a highly paid job in industry is the expression of the democratic process–for the rest of the world it is called bribery. Thus, it is likely that agricultural and food processing industries will continue to delay and obstruct any recommendations to reduce sugars and highly processed carbohydrates in our food supply. A preview of this battle has already occurred when Major Michael Bloomberg of New York City intended to restrict sales of sugary soft drinks to no more than 16 ounces a cup in city restaurants, movie theaters, stadiums and arenas. A barrage of negative comments filled the media spaces. For example, Bloomberg News, reported the comments by Kirsten Witt Webb, a Coca-Cola (KO) spokeswoman, who said in an e-mail. “They can make their own choices about the beverages they purchase. We hope New Yorkers loudly voice their disapproval about this arbitrary mandate.”
Soft drinks and soft drinks contain often eight or more table spoons of sugar per drink as shown in Figure 2.
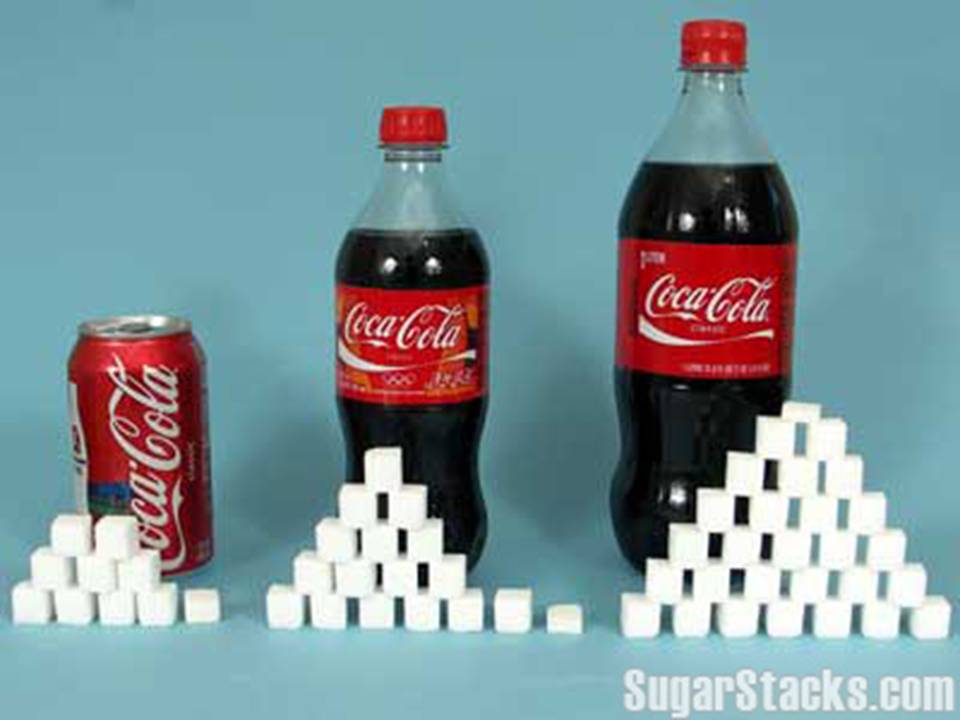 Figure 2. Amount of sugar cubes in soft drinks. Source: http://www.sugarstacks.com/beverages.htm
Figure 2. Amount of sugar cubes in soft drinks. Source: http://www.sugarstacks.com/beverages.htm
The sugar/highly processed foods battle will be similar to the battle the smoking lobby fought for the last 30 years. Just like tobacco subsidies, farmers receive subsidies to grow corn to make more low cost high fructose corn syrup. As recent as 2005 tobacco farmers were still receiving a billion and a half dollars in subsidy while farmers growing corn received more than seven billion dollars in subsidies as shown in Figure 3.
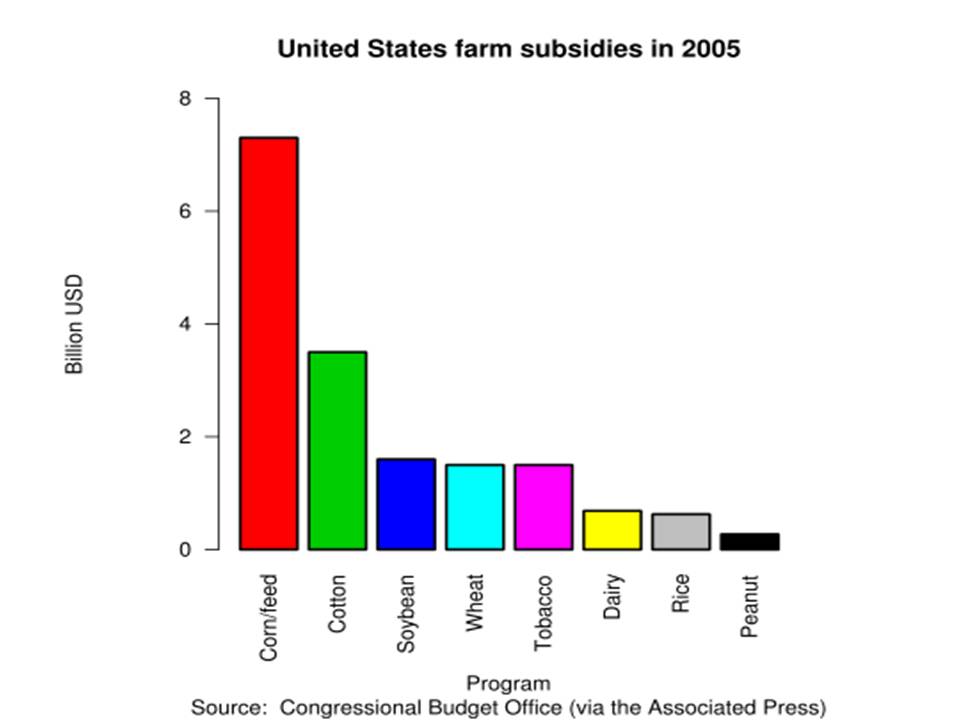
Figure 3. Farm subsidies in 2005. source: http://en.wikipedia.org/wiki/Agricultural_subsidy
At the same time pharmaceutical companies continue to reap a financial bonanza from the sugar diet induced illnesses. They will create more and more drugs to attempt to reduce the illnesses and symptoms.
We cannot expect the US government to promote our health as the lobbying power by agribusiness is overwhelming. We cannot expect published information, whether on the web or in print, to be accurate as advertising dollars significantly affect editorial decisions.
We can start eating differently ourselves and with our families and friends. Begin now. Do an experiment by eating a predominantly Paleolithic diet. For the next two weeks, eat only foods that are real foods which your great grandparents recognized as food. Thus nothing out of box or can. Nothing that has been processed or prepared! Buy only foods in their natural form. Shop at farmers’ markets or only at the periphery of the supermarket: vegetables and fruits, the meat and fish counters. After eating this diet for two weeks, check how you feel. Many people report having more energy, feeling less tired and irritability, and some experience a reduction in arthritic pains, inflammation, headaches and even anxiety. For dietary suggestions see the common sense recommendations in Michael Pollan’s book, In Defense of Food: An Eater’s Manifesto.
