How effective is treatment? The importance of active placebos
Posted: December 16, 2017 Filed under: Pain/discomfort, placebo, self-healing, stress management, Uncategorized | Tags: Active placebo, Clinical trials, expectancy, hope, nocebo, passive placebo, placebo 3 CommentsAdapted by Erik Peper and Richard Harvey from: Peper, E. & Harvey, R. (2017). The fallacy of the placebo-controlled clinical trials: Are positive outcomes the result of “indirect” treatment effects? NeuroRegulation, 4(3–4), 102–113. http://dx.doi.org/10.15540/nr.4.3-4.102
How come some drugs or medical procedures are initially acclaimed to be beneficial and later ineffective or harmful and withdrawn from the market?
How come some patients with a cancer diagnosis experience symptom remission after receiving a placebo medication? Take the case of Mr. Wright. Several decades ago Dr. Klopher (1957) described Mr. Wright as a patient who had a generalized and far advanced malignancy in the form of a lymphosarcoma with an estimated life expectancy of less than two weeks. Following the diagnosis Mr. Wright read a newspaper article about a promising experimental cancer medication called Krebiozen and requested that he receive the latest treatment. Soon after receiving the drug, Mr. Wright had a complete remission of cancer symptoms with no signs of the deadly tumor. For over two months after receiving the new promising drug, Krebiozen, Mr. Wright engaged in a normal life and was even able to fly his own plane at 12,000 feet. After a promising introduction to the medication, Mr. Wright subsequently read another newspaper article which proved the new medication to be a useless, inert preparation. Confused and demoralized, the results of the wonder drug did not last and his symptoms returned. When the final AMA announcement was published “Nationwide tests show Krebiozen to be a worthless drug in treatment of cancer,” his symptoms became acute and he died within two days (Klopher, 1957).
The term placebo loosely translates as ‘I shall please you’ can be contrasted with the term nocebo which loosely translates as ‘I shall harm you’ when referring to exposure to a sham medication, treatment or procedure that results a positive outcome (placebo response), or a negative outcome (nocebo response), respectively. The responses a person has reflect a complex interaction between many processes. For example, when studying a placebo or nocebo response we measure internal psychological processes, measured in terms of a person’s self-reported attitudes, beliefs, cognitions and emotions; behavioral processes, measured overtly by observations of a person’s actions; and, physiological processes, measured more or less directly with instruments such as heart rate monitors, or biochemical analyses. Most relevant is that a person’s beliefs about the placebo (or nocebo) medication, treatment or procedure leads to predictable positive (or negative) behaviors and physiological benefits or harms.
The case of Mr. Wright illustrates that we may underestimate the positive power of the placebo or, the negative power of the nocebo, where Mr. Wright’s belief about the medication’s benefits first interacted in a positive way (placebo) with his behaviors (e.g. engaging in daily activities including flying an airplane) as well as his physiology (e.g. cancer remission) and unfortunately later, in a negative way (nocebo) interacting with his physiology (e.g. cancer return) contributing to his death.
The placebo response can be very powerful and healing. For example, watch the very dramatic demonstration of how the placebo response can be optimized in Derren Brown’s BBC video Fear and Faith Placebo https://www.youtube.com/watch?v=y2XHDLuBZSw).
Placebo and nocebo effects are found in all therapeutic transactions when the communications between therapist and patient reflect embedded beliefs about the treatment. For example, patients have faith in clinician’s knowledge and belief that a prescribed medication is going to be effective at treating their symptoms, which then reinforces the patient’s belief in the medication, increasing indirect, embedded placebo effects, above and beyond any direct effects from the medication. The indirect effects of placebo responses have been most studied with medications; however, placebo effects are also studied in non-drug therapies. The research on placebo effects has demonstrated time and time again that when patients expect that the drug, surgery, or other therapeutic technique to be beneficial, then the patients tend to benefit more from the treatment.
The expectancy that the treatment will be effective at reducing symptoms is overtly, and covertly communicated by the health care professional during patient interactions, as well as by drug companies through direct to consumer advertising, and social media. The implied message is that the drug or procedure will improve symptoms, recovery or improve quality of life. On the other hand, if you do not do take the drug or do the procedure, your health will be compromised. For example, if you have high cholesterol, then take a statin drug to prevent the consequences of high cholesterol such as a heart attack or stroke. The implied message is that if you do not take it, you will die significantly sooner. Statins lower the risk for heart attacks; however, the benefits may be over stated. For people without prior heart disease, 60 people will have to take statins for 5 years to prevent 1 heart attack and 268 people to prevent 1 stroke. During the same time period 1 in 10 will experience muscle damage and 1 in 50 develop diabetes (theNNT, 2017 November).
If placebo and nocebo can have significant effects on medical outcome, how do you know if the treatment benefits are due to the direct effects of a drug or procedure or due to any indirect placebo effects or a combination of both?
The randomized controlled trial (RCT) is considered the gold standard method to determine the effectiveness of a drug or procedure. The ideal study would be a double blind, randomized, placebo controlled clinical trial in which neither the practitioner nor the patient would know who is getting what condition. For example, blinding implies the placebo group would receive a pill that appears identical to a ‘real’ pill, except the placebo has pharmacological ingredients. Similarly, a patient may receive an ‘exploratory’ surgery in which anesthesia is given and the skin is cut however the no further actual internal surgery occurs because the surgeon determined further internal surgery was unnecessary. Although, it is not possible to perform a double blind surgery study, the patient may be totally unaware whether an internal surgery had occurred.
Peper and Harvey (2017) point out that the positive findings of an ‘effective’ treatment are not always the results of the direct effects of medications and may be more attributable to indirect placebo responses. For example, patients may attribute the ‘effectiveness’ of the treatment to their experience of ‘non-directed’ treatment side effects that include: the post-surgical discomfort which signals to the patient that the procedure was successful, or a dry mouth and constipation that were caused by the antidepressant medication, which signals to the person that the trial medication or procedure-related medication is working (Bell, Rear, Cunningham, Dawnay, & Yellon, 2014; Stewart-Williams & Podd, 2004).
Just imagine the how pain can evoke totally different reactions. If you recently had a heart attack and then later experienced pain and cramping in the chest, you automatically may feel terrified as you could interpret the pain as another heart attack. The fear response to the pain may increase pathology and inhibit healing (a nocebo response). On the other hand, after bypass surgery, you may also experience severe pain when you move your chest. In this case, you interpret the pain as a sign that the bypass surgery was successful, which then reduces fear and reinforces the belief that you have survived a life threatening situation and will continue healing (placebo response).
Many research studies employ a placebo control, however what is less typical is a double-blind study using an ‘active’ placebo (Enck, Bingel, Schedlowski, & Rief, 2013). Less than 0.5% of all placebo studies include an active placebo group. (Shader, 2017; Jensen et al, 2017).
Unfortunately, a typical ‘placebo controlled’ study design is problematic for distinguishing the direct from any indirect (covert) placebo effects that occur within the study as shown in Figure 1.
 Figure 1. Normal (passive) placebo control group controls and experimental group. What is not assessed are placebo benefits induced by the medication/treatment induced side effects.
Figure 1. Normal (passive) placebo control group controls and experimental group. What is not assessed are placebo benefits induced by the medication/treatment induced side effects.
With a passive placebo, there is no way to know if the observed benefits are from the medication/medical procedure, or from the placebo/self-healing response triggered by the medication/medical procedure (or both combined, or neither the placebo or medical procedure). The best way to know if the treatment is actually beneficial is to use an ‘active’ placebo instead of a passive placebo.
An active placebo builds on a patient’s attributions about a medication or medical procedure. For example, a patient may be told by a clinician that feeling any side effects such as insomnia, a racing heart or, experiencing a warm flushing feeling will let them know the medication is working, so the patient becomes conditioned to expect the medication is working when they feel or experience side effects. Whereas a passive (inert) placebo such as a sugar pill will have effects that are extremely subtly felt or experienced, an active placebo will have effects that are more overtly felt or experienced. Examples of active placebos include administering low doses of caffeine or niacin that have effects which may be felt internally however which do not have the same effects as the medication. When a patient is told they may have side effects from the medication that include felt changes in heart rate or a flushing feeling, the patient attributes the changes they feel to a medication they believe will bring about benefits, even though the changes are rightfully attributed to the caffeine or niacin in the active placebo.
An active placebo triggers observed and felt body changes which do not affect the actual illness. For surgical procedures, an ‘active’ placebo control would be a sham/mock surgery in which the patient would undergo the same medical procedure (e.g. external surgery incision) without continuing some internal surgical procedure (Jonas et al, 2015). In numerous cases of accepted surgery, such as the Vineberg procedure (Vineburg & Miller, 1951) for angina, or arthroscopic knee surgery for treating osteoarthritis, the clinical benefits of a sham/mock surgery were just as successful as the actual surgery. Similar studies suggest the clinical benefits were solely (or primarily) due directly to the placebo response (Beecher, 1961; Cobb et al, 1959; Moseley et al, 2002).
To persuasively demonstrate that a treatment or therapeutic procedure is effective it should incorporate a study design using an active placebo arm as shown in Figure 2. Figure 2. Active placebo control group controls for the normal placebo benefits plus those placebo benefits induced by the medication/treatment induced side effects.
Figure 2. Active placebo control group controls for the normal placebo benefits plus those placebo benefits induced by the medication/treatment induced side effects.
Some treatments may be less effective then claimed because they were not compared to an active placebo, which could be one of the reasons why so many medical and psychological studies cannot be replicated. The absence of ‘active’ placebo controls may also be a factor explaining why some respected authorities have expressed some doubt about published scientific medical research results. Following are two quotes that illustrate such skepticism.
“Much of the scientific literature, perhaps half, may simply be untrue.” —Richard Horton, editor-in-chief of the Lancet (Horton, 2015).
“It is simply no longer possible to believe much of the clinical research that is published, or to rely on the judgment of trusted physicians or authoritative medical guidelines. I take no pleasure in this conclusion, which I reached slowly and reluctantly over my two decades as an editor of the New England Journal of Medicine” —Dr. Marcia Angell, longtime Editor in Chief of the New England Medical Journal (Angell, 2009).
There are a variety of questions to ask before agreeing on a procedure or before taking medication
A quick way to ask whether a medication or medical treatment effectiveness is the result of placebo components is to ask the following questions:
- Have there been successful self-care or behavioral approaches beyond surgical or pharmaceutical treatments that have demonstrated effectiveness? When successful treatments are reported, then questions are raised whether pharmaceutical or surgical outcomes are also attributable to the result of placebo effects. On the other hand, if there a no successful self-care approaches, then the benefits may be more due to the direct therapeutic effect of a surgical procedure or medication.
- Has the procedure been compared to an active placebo control? If not, then to what extent it is possible that the results of the surgical or pharmaceutical therapy could be attributed to a placebo response instead of directly to the medication or surgery?
- What are the long term benefits and complication rates of the medication, treatment or procedure? When benefits are low and risks of the procedure are high, explore the risks associated with ‘watchful waiting’ (Colloca, Pine, Ernst, Miller & Grillon, 2016; Thomas et al, 2014; Taleb, 2012).
Unfortunately, most clinical studies that includes pharmaceuticals and/or surgery do not test their medication, surgery against an ‘active’ placebo. Whenever possible, enquire whether an active placebo was used to determine the degree of effectiveness of the proposed treatment or procedure. Fortunately, the design of ‘active’ placebo-controlled studies is very possible for anyone interested in comparing the effectiveness of medications, treatments and procedures in various settings, from hospitals and clinics to university classrooms and individual homes.
In summary, the benefits of the treatment must significantly outweigh any risks of negative treatment side effects. Short-term treatment benefits need to be balanced by any long-term benefits. Unfortunately, short-term benefits may lead to significant, long-term harm such as in the use of some medications (e.g. sleep medications, opioid pain killers) that result in chronic dependency and which lead to a significant increase in morbidity and mortality of many kinds. We suggest that more medications and other procedures are tested against an active placebo to investigate whether the medication or procedure is actually effective.
For a detailed analysis and discussion of placebo and the importance of active placebo see our article, Peper, E. & Harvey, R. (2017). The fallacy of the placebo-controlled clinical trials: Are positive outcomes the result of “indirect” treatment effects? NeuroRegulation, 4(3–4), 102–113. http://dx.doi.org/10.15540/nr.4.3-4.102
References:
Angell M. Drug companies and doctors: A story of corruption. January 15, 2009. The New York Review of Books 56. Available: http://www.nybooks.com/articles/archives/2009/jan/15/drug-companies-doctorsa-story-of-corruption/. Accessed 24, November, 2016.
Beecher, H. K. (1961). Surgery as placebo: A quantitative study ofbias. JAMA, 176(13), 1102–1107. http://dx.doi.org/10.1001/jama.1961.63040260007008
Bell, R. M., Rear, R., Cunningham, J., Dawnay, A., & Yellon, D. M. (2014). Effect of remote ischaemic conditioning on contrast-induced nephropathy in patients undergoing elective coronary angiography (ERICCIN): rationale and study design of a randomised single-centre, double-blind placebo-controlled trial. Clinical Research in Cardiology, 103(3), 203-209. http://dx.doi.org/10.1007/s00392-013-0637-3
Cobb, L. A., Thomas, G. I., Dillard, D. H., Merendino, K. A., & Bruce, R. A. (1959). An evaluation of internal-mammary-artery ligation by a double-blind technic. New England Journal of Medicine, 260(22), 1115–1118. http://dx.doi.org/10.1056/NEJM195905282602204
Colloca, L., Pine, D. S., Ernst, M., Miller, F. G., & Grillon, C. (2016). Vasopressin boosts placebo analgesic effects in women: A randomized trial. Biological Psychiatry, 79(10), 794–802. http://dx.doi.org/10.1016/j.biopsych.2015.07.019
Derren Brown’s BBC video Fear and Faith Placebo https://www.youtube.com/watch?v=y2XHDLuBZSw
Enck, P., Bingel, U., Schedlowski, M., & Rief, W. (2013). The placebo response in medicine: minimize, maximize or personalize?. Nature reviews Drug discovery, 12(3), 191-204. http://dx.doi.org/10.1038/nrd3923
Horton, R. (2015). Offline: What is medicine’s 5 sigma. The Lancet, 385(9976), 1380. http://www.thelancet.com/pdfs/journals/lancet/PIIS0140-6736%2815%2960696-1.pdf
Jensen, J. S., Bielefeldt, A. Ø., & Hróbjartsson, A. (2017). Active placebo control groups of pharmacological interventions were rarely used but merited serious consideration: A methodological overview. Journal of Clinical Epidemiology. https://doi.org/10.1016/j.jclinepi.2017.03.001
Jonas, W. B., Crawford, C., Colloca, L., Kaptchuk, T. J., Moseley, B., Miller, F. G., & Meissner, K. (2015). To what extent are surgery and invasive procedures effective beyond a placebo response? A systematic review with meta-analysis of randomised, sham controlled trials. BMJ open, 5(12), e009655. http://dx.doi.org/10.1136/bmjopen-2015-009655
Klopfer, B., (1957). Psychological Variables in Human Cancer, Journal of Projective Techniques, 21(4), 331–340. http://www.tandfonline.com/doi/abs/10.1080/08853126.1957.10380794
Moseley, J. B., O’Malley, K., Petersen, N. J., Menke, T. J., Brody, B. A., Kuykendall, D. H., … Wray, N. P. (2002). A controlled trial of arthroscopic surgery for osteoarthritis of the knee. The New England Journal of Medicine. 347(2), 81–88. http://dx.doi.org/10.1056 /NEJMoa013259
Peper, E. & Harvey, R. (2017). The fallacy of the placebo-controlled clinical trials: Are positive outcomes the result of “indirect” treatment effects? NeuroRegulation, 4(3–4), 102–113. http://dx.doi.org/10.15540/nr.4.3-4.102
Shader, R. I. (2017). Placebos, Active Placebos, and Clinical Trials. Clinical Therapeutics, 39(3), 451–454. http://dx.doi.org/10.1016/j.clinthera.2017.02.001
Stewart-Williams, S., & Podd, J. (2004). The placebo effect: dissolving the expectancy versus conditioning debate. Psychological bulletin, 130(2), 324. http://dx.doi.org/10.1037/0033-2909.130.2.324
Taleb, N. N. (2012). Antifragile: Things that gain from disorder. Random House.
TheNNT (2017, November). http://www.thennt.com/nnt/statins-for-heart-disease-prevention-without-prior-heart-disease/
Thomas, R., Williams, M., Sharma, H., Chaudry, A., & Bellamy, P. (2014). A double-blind, placebo-controlled randomised trial evaluating the effect of a polyphenol-rich whole food supplement on PSA progression in men with prostate cancer—the UK NCRN Pomi-T study. Prostate Cancer and Prostatic Diseases, 17(2), 180–186. http://dx.doi.org/10.1038/pcan.2014.6
Vineberg, A., & Miller, G. (1951). Treatment of coronary insufficiency. Canadian Medical Association Journal, 64(3), 204. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1821866/pdf/canmedaj00654-0019.pdf
First do no harm: Listen to Freakonomics Radio Episodes Bad Medicine
Posted: September 3, 2017 Filed under: Uncategorized | Tags: health, Medicine, pharmaceuticals, placebo, treatment 1 Comment
How come up to 250,000 people a year die of medical errors and is the third leading cause of death in the USA (Makary & Daniel, 2016)?
Why are some drugs recalled after years of use because they did more harm than good?
How come arthroscopic surgery continues to be done for osteoarthritis of the knee even though it is no more beneficial than mock surgery (Moseley et al, 2002)?
How come women have more negative side effects from Ambien and other sleep aids than men?
Is it really true that the average new cancer drug costs about $100,000 for treatment and usually only extends the life of the selected study participants by about two months (Szabo, 2017; Fojo, Mailankody, & Lo, 2014)?
“It is simply no longer possible to believe much of the clinical research that is published, or to rely on the judgment of trusted physicians or authoritative medical guidelines. I take no pleasure in this conclusion, which I reached slowly and reluctantly over my two decades as an editor of the New England Journal of Medicine”—Dr. Marcia Angell, longtime Editor in Chief of the New England Medical Journal (Angell, 2009).
Medical discoveries have made remarkable improvements in our health. The discovery of insulin in 1921 by Canadian physician Frederick Banting and medical student Charles H. Best allowed people with Type 1 Diabetes to live healthy productive lives (Rosenfeld, 2002). Cataract lens replacement surgery is performed more than three million times per year and allows millions of people to see better even though a few patients have serious side negative side effects. And, there appears to be new hope for cancer. The FDA on August 30, 2017, approved a new individualized cancer treatment that uses genetically engineered cells from a patient’s immune system to produce remissions in 83 percent of the children and young adults who have relapsed after undergoing standard treatment for B cell acute lymphoblastic leukemia. (FDA August 30, 2017). The one-time treatment for this breakthrough cancer drug for patients who respond costs $475,000 according to the manufacturer Novartis. Yet, it will be years before we know if there are long term negative side effects.
The cost of this treatment is much more than the average cost of $100,000 for newly developed and approved cancer drugs which at best extend the life of highly selected patients on the average by two months; however, when they used with more typical Medicare patients, these drugs often offer little or no increased benefits (Szabo, 2017; Freakonomics Radio episode Bad Medicine, Part 2: (Drug) Trials and Tribulations).
As the health care industry is promising new screening, diagnostic and treatment approaches especially through direct-to-consumer advertising, they may not always be beneficial and, in some cases, may cause harm. The only way to know if a diagnostic or treatment procedure is beneficial is to do long term follow-up; namely, did the treated patients live longer, have fewer complications and better quality of life than the non-treatment randomized control patients. Just because a surrogate illness markers such as glucose level for type 2 Diabetes or blood pressure for essential hypertension decrease in response to treatment, it does not always mean that the patients will have fewer complications or live longer.
To have a better understanding of the complexity and harm that can occur from medical care, listen to the following three Freakonomics Radio episodes titled Bad Medicine.
Freakonomics Radio episode Bad Medicine, Part 1: The story of 98.6. We tend to think of medicine as a science, but for most of human history it has been scientific-ish at best. In the first episode of a three-part series, we look at the grotesque mistakes produced by centuries of trial-and-error, and ask whether the new era of evidence-based medicine is the solution. http://freakonomics.com/podcast/bad-medicine-part-1-story-98-6/
Freakonomics Radio episode Bad Medicine, Part 2: (Drug) Trials and Tribulations. How do so many ineffective and even dangerous drugs make it to market? One reason is that clinical trials are often run on “dream patients” who aren’t representative of a larger population. On the other hand, sometimes the only thing worse than being excluded from a drug trial is being included. http://freakonomics.com/podcast/bad-medicine-part-2-drug-trials-and-tribulations/
Freakonomics Radio episode, Bad Medicine, Part 3: Death by Diagnosis. By some estimates, medical error is the third-leading cause of death in the U.S. How can that be? And what’s to be done? Our third and final episode in this series offers some encouraging answers. http://freakonomics.com/podcast/bad-medicine-part-3-death-diagnosis/
References
Angell M. Drug companies and doctors: A story of corruption. January 15, 2009. The New York Review of Books 56. Available: http://www.nybooks.com/articles/archives/2009/jan/15/drug-companies-doctorsa-story-of-corruption/. Accessed 24, November, 2016.
FDA approval brings first gene therapy to the United States, August 30, 2017. https://www.fda.gov/newsevents/newsroom/pressannouncements/ucm574058.htm
Makary, M. A., & Daniel, M. (2016). Medical error-the third leading cause of death in the US. BMJ: British Medical Journal (Online), 353. Listen to his BMJ medical talk: https://soundcloud.com/bmjpodcasts/medical-errorthe-third-leading-cause-of-death-in-the-us
Rosenfeld, L. (2002). Insulin: discovery and controversy. Clinical chemistry, 48(12), 2270-2288. http://clinchem.aaccjnls.org/content/48/12/2270
Szabo, L. (201, February 9). Dozens of new cancer drugs do little to improve survival. Kaiser Health News. Downloaded September 3, 2017. https://www.usatoday.com/story/news/nation/2017/02/09/new-cancer-drugs-do-little-improve-survival/97712858/
Evoking your healing potential: You are your placebo
Posted: August 31, 2014 Filed under: Uncategorized | Tags: health, hope, illness beliefs, mind-body, nocebo, placebo 3 CommentsBe careful what you think. You may get what you wish.
The power of the placebo and nocebo are remarkable and often overlooked in medicine. With a placebo, severe chest pain disappears with mock surgery, Parkinson’s tremors stop, knee pain is eliminated following mock arthroscopic knee surgery and even of lymphosarcoma can be affected (Beecher, 1961; Benedeteti, 2007; Moseley et al, 2002; Kirkley et al., 2008; Klopfer, 1957; Moerman & Jonas, 2002). On the other hand, nocebo can increase pain, accelerate cancer growth, and cause death (Cannon, 1942; Klopfer, 1957; Benedeteti, 2007). These are demonstrations of the self-healing and non-healing potential intrinsic within each of us.
The placebo response (from Latin, “I shall please”) is the beneficial physiological or psychological effect that results from the administration of an otherwise ineffective or inert substance, procedure, instruction. and/or environment. An example of placebo on neuron activity is demonstrated with a patient who has Parkinson’s disease (see figure 1).
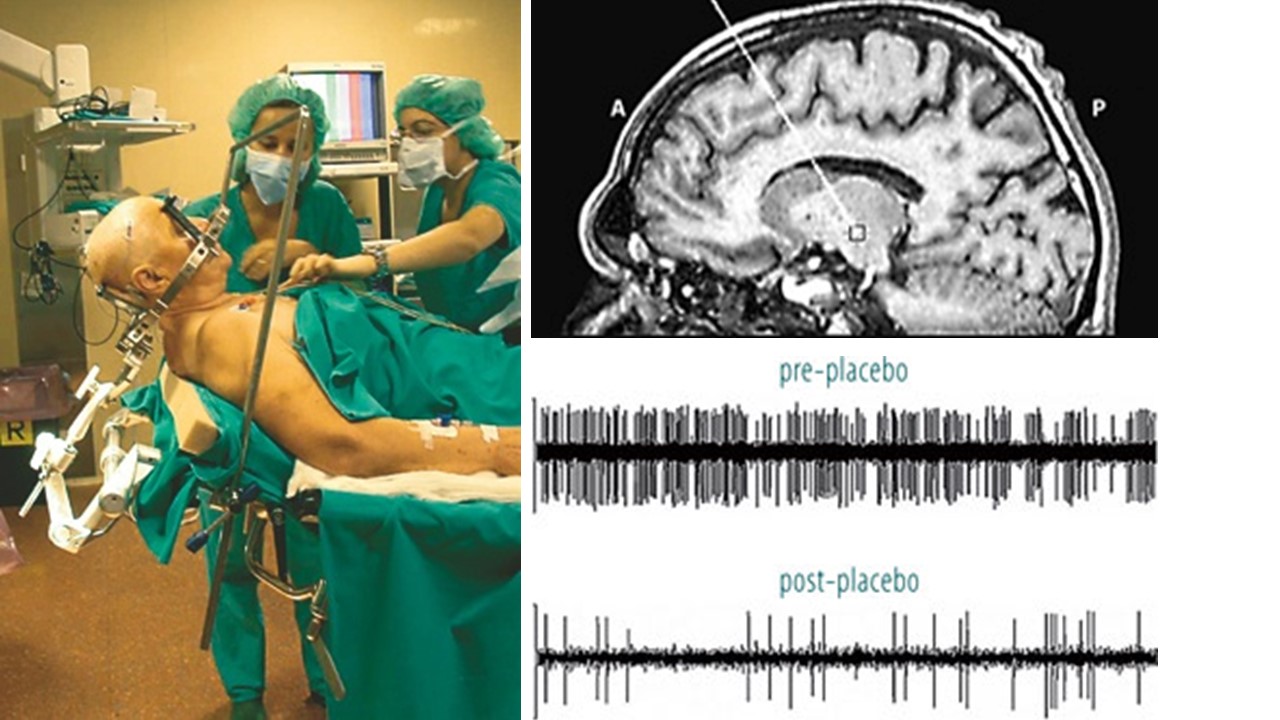 Figure 1. Recording the activity of single neurons from the brain of an awake patient suffering from Parkinson’s disease. Both the recording apparatus (a) and the electrode track (b) can be seen. In (c), the activity of a single neuron in the subthalamic nucleus can be seen before and after placebo administration (reproduced from: Benedeteti, F.(2007). The Placebo and Nocebo Effect: How the Therapist’s Words Act on the Patient’s Brain. Karger Gazette, 69).
Figure 1. Recording the activity of single neurons from the brain of an awake patient suffering from Parkinson’s disease. Both the recording apparatus (a) and the electrode track (b) can be seen. In (c), the activity of a single neuron in the subthalamic nucleus can be seen before and after placebo administration (reproduced from: Benedeteti, F.(2007). The Placebo and Nocebo Effect: How the Therapist’s Words Act on the Patient’s Brain. Karger Gazette, 69).
The nocebo response (from Latin, “I will harm”) may evoke the non-healing process and reactivate symptom/disease producing process and experiences. The nocebo response can be evoked by ineffective or inert substances, procedures, instructions, and internal and external environments which by themselves have no known effects.
The placebo/nocebo response is modulated by our covert cultural, familial and personal beliefs, limitations and expectations. The placebo/nocebo effects are the actual demonstrations that the limits of our beliefs are the limits of our possibilities. This process is well described in the recent published book, You are the Placebo: Making Your Mind Matter, by Chiropractor Joe Dispenza.
 Dr. Dispenza describes the classic studies of placebo, mental processes and possible mechanisms by which placebo effects occur and disappears and how our thoughts and expectancies create our reality. The placebo transforms the inner beliefs and give the person the experience of improved health which transforms beliefs. In many cases we can experience improvement but are pulled back into our previous beliefs and self-images of illness by inner and outer cues which are associated with disease process.
Dr. Dispenza describes the classic studies of placebo, mental processes and possible mechanisms by which placebo effects occur and disappears and how our thoughts and expectancies create our reality. The placebo transforms the inner beliefs and give the person the experience of improved health which transforms beliefs. In many cases we can experience improvement but are pulled back into our previous beliefs and self-images of illness by inner and outer cues which are associated with disease process.
The book describes of the covert conditioning process by which we return to our old self and may maintain illness. It is challenging to maintain new beliefs and act/think in new patterns. The internal mental chatter and doubts flood our awareness. Even the question, “How long will the improvement last?” re-evokes the associative mental conditioned disease patterns. If it is possible to interrupt and transform our thoughts moment by moment, minute by minute, hour by hour, day by day and not just for 15 minutes of practice, remarkable changes are sometimes possible. Every thought that triggers an association of the illness state needs to be interrupted and redirected. When patients somehow transform their thoughts, it may result in reversing and eliminating illnesses such as polyostotic fibrous dysphasia, Hashimot’sthyroiditis or chronic lympocytic thyroiditis, and secondary progressive multiple sclerosis.
I highly recommend this book for its outstanding description of placebo/nocebo and cognitive a model of the conditioning processes that underlie it. The book offers hope and inspiration for many patients who accept “what is/was” and are open to the present and future possibilities without judgement.
The book’s cases show that it is possible to reverse chronic “incurable illnesses.” Patients and health care providers should read the book–it provides hope, empowerment, and possibility. It is an antidote to the feeling that there is nothing one can do except to live with the illness. Medicine needs to explore and study the unusual patient who has reversed the disease process and ask, “How can we understand this process and teach it to other patients.”
The major limitation of the book is the absence of data; namely, what percentage of the patients/participants who have practiced Dispenza’s techniques have actually benefited and transformed their illness? The book would be more useful if it included both successful and the many unsuccessful cases. This would help patients who do the practices and do not improve. These patients sometimes blame themselves and failed at their self-healing—a process that increases depression and hopelessness. We need to realize that many factors affecting our health and illness are beyond our control.
Although I agree with Dr. Dspenza’s basic premise that our beliefs, acceptance of what is and being open to the present and future supports healing. This perspective is only part of the whole picture. Health and illness are multi-factorial and many factors are not within our control.
Read the book and skip chapter 8, The Quantum Mind. This chapter attempts to describe the physics of the healing process using quantum physics. As I did not understand quantum physics and quantum mind, I asked my colleague, James Johnston, PhD, who is an expert in quantum physics, to read it for accuracy. He confirmed my gut reaction when he said, “the quantum physics description of how energy changes is pseudo science, involving an incomplete understanding of quantum theory.”
Beecher, H.K. (1961). Surgery as Placebo. JAMA, 176(13), 1102-1107.
Cannon, W. B. (1942). “Voodoo” death. American Anthropologist, 44(2), 169-181.
Dispenza, J. (2014). You are the Placebo: Making Your Mind Matter. Hay House, Inc.
