This May Save Your Life! Bacteriophage Treatment for Bacterial Diseases*
Posted: September 11, 2025 Filed under: Evolutionary perspective, healing, health, Pain/discomfort, self-healing | Tags: antibiotic resistance, antibiotics, bacteria, bacteriohage, health, Medicine Leave a commentRecently, I listened to a special episode featuring Lina Zeldovich on her book The Living Medicine, from This Podcast Will Kill You. I was totally inspired because it discussesd the healing power of bacteriophages, which apparently treat antibiotic-resistant bacterial infections successfully, reportedly without side effects. (Bacterial phages are viruses that selectively kill specific bacteria and have been used to treat multi-antibiotic-resistant conditions).
This emerging therapy is an aspect of individualized treatment. Zeldovich reports that it can not only be used to treat, but also to prevent the occurrence of bacterial illnesses. I rushed out to buy the book, The Living Medicine: How a lifesaving cure was nearly lost and why it will rescue us when antibiotics fail. Zeldovich is a great science storyteller and the book really captured me. I read it in two evenings and wanted to share this information, since a day may come when it could save your life.
This is a must-read for all of us, particularly for health professionals. It offers hope through a non-toxic strategy in the fight against antibiotic-resistant disease. The book provides a perspective on the challenges of bringing this effective healing strategy to acceptance and implementation when cultural biases and financial disincentives have stood in the way.;

Zeldovich, describes the development and history of bacterial phage medicine and why it has taken so many years to become accepted in the West. Only after several high-profile cases has this approach become of interest. A prime example is the 2016 treatment of Dr. Tom Patterson, a professor at UC San Diego, who contracted a life-threatening Acinetobacter baumannii infection while traveling (Garnett, 2019). The bacteria that caused his infection was resistant to every available antibiotic. After he slipped into a coma, his doctors feared the worst. As a last resort, his wife, Dr. Steffanie Strathdee, worked with scientists to identify phages that could target the infection. Within 48 hours of receiving intravenous phage therapy, Patterson woke up. He went on to make a full recovery, one of the first documented cases in the U.S. in which phages saved a patient’s life.
Pros and cons of antibiotics
Until antibiotics were discovered, bacterial infections were often fatal. This changed with the discovery of penicillin by Alexander Fleming in 1928. During World War II, antibiotics saved countless solders’ lives in the treatment of infected wounds, pneumonia, and blood poisoning. The antibiotic approach was quickly adopted in the United States, beginning in the early 1940’s, since penicillin could be mass-produced and thus was highly profitable for the pharmaceutical companies. Despite the initial success of the drug, bacteria quickly developed antibiotic resistance to penicillin due to the ability of bacteria to produce β-lactamase, an enzyme capable of breaking down the drug.
Antibiotics were and are extraordinary drugs. When a patient is becoming sicker and sicker as a bacterial infection spreads, the infection can be stopped in its tracks with an effective antibiotic. Before the era of antibiotic resistance, patients recovered as if by magic, simple by giving an antibiotic orally or intravenously,
I still remember when our son developed pneumonia at the age of 12, initially with coughing, a high fever, chest pain, and a great deal of congestion. But as the infection progressed, he began to have difficulty breathing and his energy was fading. We were initially hesitant to give the prescribed antibiotic because we hoped his immune system would be able to fight the infection. My hesitancy was based upon the fact that antibiotics do not selectively kill the bacteria causing the illness, but also destroy beneficial bacteria that are part of the human biome.
Millions of women who have taken an antibiotic for an infection subsequently experience chronic vaginal yeast infections. This occurs because antibiotics such as tetracyclines, which are used to treat UTIs, intestinal tract infections, eye infections, sexually transmitted infections, acne, and gum disease, also kill the healthy bacteria of the human biome in the vagina. Since nature abhors a vacuum, yeast then overgrow where healthy bacteria used to predominate, thus allowing a vaginal infection (candidiasis) to occur (Spinillo et al., 1999)
In the case of my son, as it became clear that he was getting weaker and his immune system was not successfully clearing the infection, we followed his doctor’s advice and gave him the antibiotic. Magically, within two days he was better, and we continued with the course of antibiotics to clear his body of all the bacteria that was causing the pneumonia. Treatment is always a decision that involves balancing risk and benefit, getting sicker or getting well, given the possible negative side effects of the treatment. At the same time, it was possible that the antibiotic would not work since there was no time to run a lab test for that specific bacteria. If it had not worked, he would have needed another, different antibiotic, and if that had failed, a third drug.
Today, antibiotic resistance has grown into a worldwide crisis. The World Health Organization estimates that antimicrobial resistance directly caused 1.27 million deaths and contributed to another 5 million deaths globally in 2019. In the United States alone, the CDC reports over 2.8 million antibiotic-resistant infections occur every year, leading to at least 35,000 deaths and more than 3 million cases of infection by Clostridioides difficile (C. diff) occur (CDC, 2019).
Potentially fatal diseases that have become antibiotic resistant include Staphylococcus aureus (such as methicillin-resistant Staph aureus or MRSA) and Streptococcus pneumoniae (strep), as well as Klebsiella pneumoniae, Acinetobacter baumannii, Escherichia coli, and Pseudomonas aeruginosa. These six pathogens alone were responsible for nearly 1 million deaths in 2019. Other dangerous resistant infections include multidrug-resistant tuberculosis (MDR-TB), extensively drug-resistant typhoid fever, and carbapenem-resistant Enterobacteriaceae (CRE), sometimes described as “nightmare bacteria” (Murray, et al., 2022).
Bacterial resistance develops because bacteria, like all living organisms, evolve. Antibiotics, which are typically chemicals produced by molds or other organisms, work by killing or interfering with the life cycle of specific types of bacteria. However, antibiotics are often a blunt instrument: they resemble a form of what has been referred to as carpet bombing in warfare, in which the enemy is destroyed, but the whole neighborhood is also destroyed. While antibiotics may eliminate the bacteria causing the infection, they can also damage or destroy many beneficial bacteria in the gut, on the skin, and other areas of the body.
One in five medication-related visits to the emergency room are from reactions to antibiotics (CDC, 2025). This collateral damage can disrupt the gut microbiome, weaken immunity, and create opportunities for other harmful microbes to flourish. In addition, frequent antibiotic use could possibly contribute to obesity, as evidenced by the fact that low dosages of antibiotics are often given to farm animals, not only to prevent disease, but to increase their weight. Antibiotics appear to alter the gut microbiome to make it more efficient at extracting nutrients and energy from feed (Cox, 2016).
Antibiotics have been one of the major focuses of pharmaceutical drug development; however, they can cause serious side effects and tend to become less effective over time as the bacteria develop antibiotic resistance. Many bacteria can develop antibiotic resistance in less than a 6 month time period (Poku et al., 2023). Once bacteria develop antibiotic resistance to one drug, a new antibiotic drug needs to be discovered, developed, and produced. Even the newer and stronger antibiotics rapidly loose their efficacy as the bacteria develop resistance to it. In the long term, it is a loosing battle, and a totally new approach is needed.
Bacteriophage therapy
One new approach worth closer consideration is bacteriophage therapy. In nature, bacteria and viruses have been locked in a constant evolutionary battle for billions of years. Bacteria are vulnerable to specific viruses, so a bacteriophage, or phage, refers to a virus that specifically infects and kills a particular strain of bacteria. As bacteria change to evade attack, phages evolve to counter them, maintaining an ongoing balance to some degree. The theory is that because phages are very specific and only act on one particular type of bacteria, that potentially makes them a uniquely precise form of medicine.
The challenge involves matching the phage to the pathogenic bacterium, and there are an astonishing number of different phages and bacteria. In two patients with the same symptoms or diagnosis, the causal bacteria could be a slightly different subspecies. When used clinically, bacteriophages work only against specific type of bacterium. This makes phage therapy a useful form of individualized medicine.
To be successful, the bacteria that causes the patient’s infection must first be identified. This is different from the way in which antibiotics are commonly used in primary care. When a patient develops symptoms, often an antibiotic is given before the bacteria has been identified, and if it does not work, another antibiotic is given.
In contrast, phage therapy depends on matching the specific disease-causing bacteria to a specific phage. Phage medicine requires a library of thousands of known phages as an essential prerequisite to treatment. Clinical care involves identifying the phage that can target and destroy that specific bacterium. Then the phage is cultured, purified, and administered in either a liquid preparation, capsule, ointment, intravenously or at a wound site depending on the type of infection.
Unlike antibiotics, which often damage beneficial microbes, phages only target the bacteria they evolved to destroy, leaving the rest of the human biome intact. Because viruses are capable of reproduction, once a phage reaches its bacterial host, it multiplies rapidly and produces hundreds of new phages that continue to attack the specific disease-causing bacteria as shown in Figure 1. According to reports from phage medicine, symptoms improve dramatically within 24 hours. The phages are self-limiting and their numbers naturally decline once the infection is cleared.
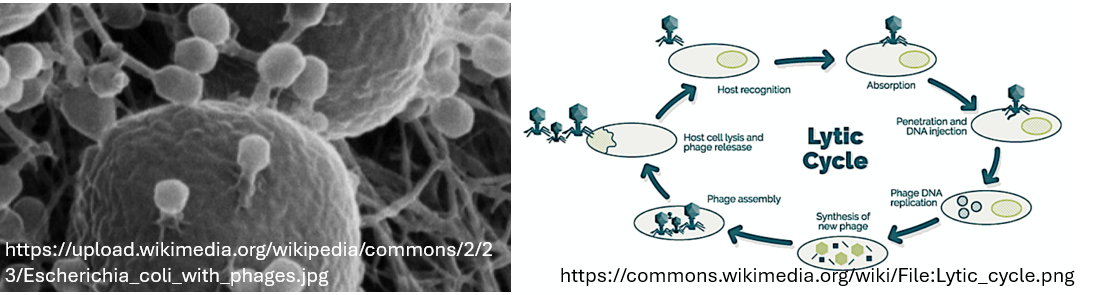
Figure 1. Electron micrograph of a phage attaching and injecting it viral genome into the cell and its life cycle
At present, phage therapy has already shown success against a variety of resistant infections, including methicillin-resistant Staphylococcus aureus (MRSA), Acinetobacter baumannii wound infections (a major problem in military medicine), multidrug-resistant Klebsiella pneumoniae, and even certain cases of tuberculosis. Instead of being the last line of defense, in the future this may become the first line of defense.
The initial research and clinical use has been concentrated in Russia and Eastern Europe. The United States largely abandoned phage therapy after the discovery of antibiotics. Several factors contributed to this trend.
- Funding barriers. Funding agencies in the West have not seen phage therapy as a credible option. In many cases, the review committees that decided which grant applications to approve have tended to fund research that supported their own biases and their interests in antibiotic research. As a result, research money was rarely allocated to study or develop phage therapies. Generally, high- risk, novel research ideas are almost never funded by federal agencies except DARPA which is more open to new concepts when they offer a high potential of success.
- Economic realities discourage investment. Unlike antibiotics, which can be mass-produced as a single chemical and sold at high volume for profit, phage therapy requires maintaining large, evolving phage libraries and tailoring treatments to each patient. This individualized model offered little appeal to large pharmaceutical companies seeking standardized products with a high payout.
- Development is not scalable. A specific bacteriophage must be selected for each specific pathogenic bacteria, and a large phage collection must be maintained to identify the correct phage.
- Scientific and cultural bias. American researchers have tended to dismiss work coming out of Russia and Georgia, failing to recognize the rigor and effectiveness of decades of phage therapy practiced there. Limited scientific exchange was also a factor during the Cold War. A similar bias, for example, has influenced the adoption of psychological treatment strategies developed in Russia. In the U.S., the focus was more on using instrumental learning while neglecting the power of Pavlov’s classical condition.
These scientific prejudices, financial disincentives, and geopolitical divides have meant that phage therapy was almost totally absent in Western medicine although it continued in Eastern Europe, where it has saved countless lives. Phage therapy is currently becoming recognized and desperately needed because of the increase in multi-drug-resistant infections.
Phage treatment challenges
The greatest challenge with phage therapy is that it must be individualized to the pathogen. Each patient’s infection may require a different phage, because phages are exquisitely specific to the bacterium they target. A phage that destroys one strain of E. coli, for example, may have no effect on another subspecies of E. coli. While the same phage can sometimes be used for multiple patients with the same infection, in most cases treatment must be customized to the individual patient.
This requires maintaining vast phage libraries that researchers and clinicians must be able to screen rapidly in order to find the right match. The scale of this challenge is staggering, although AI technology may be part of the solution. Scientists estimate that there are 10³¹ (ten million trillion trillion) specific phages on Earth, making them the most abundant biological entities known. Only a tiny fraction of these have been studied, and only a relatively smaller number are currently catalogued for medical use.
Specialized research institutes, particularly in Georgia, Poland, and Russia (and now in the U.S. and Europe) have developed large collections of phages that can be tested against samples of specific bacterium. Building, maintaining, and updating these libraries is labor-intensive and requires constant monitoring, since both bacteria and phages evolve. Phage therapy does not lend itself easily to large-scale commercialization. Nevertheless, phage therapy represents one of the most promising approaches to resistant infections.
Summary
Unlike antibiotics, which disrupt the human microbiome and can cause significant side effects, phages are naturally occurring, highly targeted, and generally well tolerated. Because they attack only a specific bacterium, without disturbing beneficial microbes, phages have the potential to be used not only as a treatment but also for prevention, helping to control bacterial populations before they cause disease. Harnessing this form of living medicine could mark an evolutionary shift in modern healthcare, offering a sustainable, balanced way to prevent and treat infections. Read the outstanding book by Lina Zeldovich, The Living Medicine: How a lifesaving cure was nearly lost and why it will rescue us when antibiotics fail.
References
admin. (2025, August 28). Special Episode: Lina Zeldovich & The Living Medicine. This Podcast Will Kill You. Accessed September 1, 2025. https://thispodcastwillkillyou.com/2025/08/28/special-episode-lina-zeldovich-the-living-medicine/
CDC. (2019). Antibiotic Resistance Threats in the United States, 2019. Atlanta, GA: U.S. Department of Health and Human Services, CDC. https://www.cdc.gov/antimicrobial-resistance/media/pdfs/2019-ar-threats-report-508.pdf
CDC. (2025). Do antibiotics have side effects. Atlanta, GA: U.S. Department of Health and Human Services, CDC Accessed September 5, 2025. https://www.cdc.gov/antibiotic-use/media/pdfs/Do-Antibiotics-Have-Side-Effects-508.pdf
Cox, L.M. (2016). Antibiotics shape microbiota and weight gain across the animal kingdom, Animal Frontiers, 6(3), 8–14. https://doi.org/10.2527/af.2016-0028
Garnett, C. (2019). Personal quest resurrects phage therapy in infection fight. NIH Record, LXXI(6). https://nihrecord.nih.gov/2019/03/22/personal-quest-resurrects-phage-therapy-infection-fight
Murray, C. J. L. et al. (2022). Global burden of bacterial antimicrobial resistance in 2019: a systematic analysis. The Lancet, 399(103250, 629 – 655. https://doi.org/10.1016/S0140-6736(21)02724-0
Poku, E., Cooper, K., Cantrell, A., Harnan, S., Sin, M.A., Zanuzdana, A., & Hoffmann, A. (2023). Systematic review of time lag between antibiotic use and rise of resistant pathogens among hospitalized adults in Europe. JAC Antimicrob Resist, 5(1), dlad001. https://doi.org/10.1093/jacamr/dlad001
Spinillo, A., Capuzzo, E., Acciano, S., De Santolo, A., & Zara, F. (1999). Effect of antibiotic use on the prevalence of symptomatic vulvovaginal candidiasis. Am J Obstet Gynecol, 180(1 Pt 1),14-7. https://doi.org/10.1016/s0002-9378(99)70141-9
Zeldovich, L. (2024). The Living Medicine: How a lifesaving cure was nearly lost and why it will rescue us when antibiotics fail. New York: St. Martin’s Press. https://www.amazon.com/Living-Medicine-Lifesaving-Lost_and-Antibiotics/dp/1250283388
*Created in part from the information in the book, The Living Medicine-How a lifesaving cure was nearly lost-and why it will rescue Us When Antibiotics Fail, by Linda Zeldovich and with the editorial help of ChatGPT5.
First do no harm: Listen to Freakonomics Radio Episodes Bad Medicine
Posted: September 3, 2017 Filed under: Uncategorized | Tags: health, Medicine, pharmaceuticals, placebo, treatment 1 Comment
How come up to 250,000 people a year die of medical errors and is the third leading cause of death in the USA (Makary & Daniel, 2016)?
Why are some drugs recalled after years of use because they did more harm than good?
How come arthroscopic surgery continues to be done for osteoarthritis of the knee even though it is no more beneficial than mock surgery (Moseley et al, 2002)?
How come women have more negative side effects from Ambien and other sleep aids than men?
Is it really true that the average new cancer drug costs about $100,000 for treatment and usually only extends the life of the selected study participants by about two months (Szabo, 2017; Fojo, Mailankody, & Lo, 2014)?
“It is simply no longer possible to believe much of the clinical research that is published, or to rely on the judgment of trusted physicians or authoritative medical guidelines. I take no pleasure in this conclusion, which I reached slowly and reluctantly over my two decades as an editor of the New England Journal of Medicine”—Dr. Marcia Angell, longtime Editor in Chief of the New England Medical Journal (Angell, 2009).
Medical discoveries have made remarkable improvements in our health. The discovery of insulin in 1921 by Canadian physician Frederick Banting and medical student Charles H. Best allowed people with Type 1 Diabetes to live healthy productive lives (Rosenfeld, 2002). Cataract lens replacement surgery is performed more than three million times per year and allows millions of people to see better even though a few patients have serious side negative side effects. And, there appears to be new hope for cancer. The FDA on August 30, 2017, approved a new individualized cancer treatment that uses genetically engineered cells from a patient’s immune system to produce remissions in 83 percent of the children and young adults who have relapsed after undergoing standard treatment for B cell acute lymphoblastic leukemia. (FDA August 30, 2017). The one-time treatment for this breakthrough cancer drug for patients who respond costs $475,000 according to the manufacturer Novartis. Yet, it will be years before we know if there are long term negative side effects.
The cost of this treatment is much more than the average cost of $100,000 for newly developed and approved cancer drugs which at best extend the life of highly selected patients on the average by two months; however, when they used with more typical Medicare patients, these drugs often offer little or no increased benefits (Szabo, 2017; Freakonomics Radio episode Bad Medicine, Part 2: (Drug) Trials and Tribulations).
As the health care industry is promising new screening, diagnostic and treatment approaches especially through direct-to-consumer advertising, they may not always be beneficial and, in some cases, may cause harm. The only way to know if a diagnostic or treatment procedure is beneficial is to do long term follow-up; namely, did the treated patients live longer, have fewer complications and better quality of life than the non-treatment randomized control patients. Just because a surrogate illness markers such as glucose level for type 2 Diabetes or blood pressure for essential hypertension decrease in response to treatment, it does not always mean that the patients will have fewer complications or live longer.
To have a better understanding of the complexity and harm that can occur from medical care, listen to the following three Freakonomics Radio episodes titled Bad Medicine.
Freakonomics Radio episode Bad Medicine, Part 1: The story of 98.6. We tend to think of medicine as a science, but for most of human history it has been scientific-ish at best. In the first episode of a three-part series, we look at the grotesque mistakes produced by centuries of trial-and-error, and ask whether the new era of evidence-based medicine is the solution. http://freakonomics.com/podcast/bad-medicine-part-1-story-98-6/
Freakonomics Radio episode Bad Medicine, Part 2: (Drug) Trials and Tribulations. How do so many ineffective and even dangerous drugs make it to market? One reason is that clinical trials are often run on “dream patients” who aren’t representative of a larger population. On the other hand, sometimes the only thing worse than being excluded from a drug trial is being included. http://freakonomics.com/podcast/bad-medicine-part-2-drug-trials-and-tribulations/
Freakonomics Radio episode, Bad Medicine, Part 3: Death by Diagnosis. By some estimates, medical error is the third-leading cause of death in the U.S. How can that be? And what’s to be done? Our third and final episode in this series offers some encouraging answers. http://freakonomics.com/podcast/bad-medicine-part-3-death-diagnosis/
References
Angell M. Drug companies and doctors: A story of corruption. January 15, 2009. The New York Review of Books 56. Available: http://www.nybooks.com/articles/archives/2009/jan/15/drug-companies-doctorsa-story-of-corruption/. Accessed 24, November, 2016.
FDA approval brings first gene therapy to the United States, August 30, 2017. https://www.fda.gov/newsevents/newsroom/pressannouncements/ucm574058.htm
Makary, M. A., & Daniel, M. (2016). Medical error-the third leading cause of death in the US. BMJ: British Medical Journal (Online), 353. Listen to his BMJ medical talk: https://soundcloud.com/bmjpodcasts/medical-errorthe-third-leading-cause-of-death-in-the-us
Rosenfeld, L. (2002). Insulin: discovery and controversy. Clinical chemistry, 48(12), 2270-2288. http://clinchem.aaccjnls.org/content/48/12/2270
Szabo, L. (201, February 9). Dozens of new cancer drugs do little to improve survival. Kaiser Health News. Downloaded September 3, 2017. https://www.usatoday.com/story/news/nation/2017/02/09/new-cancer-drugs-do-little-improve-survival/97712858/
Training Compassionate Presence
Posted: November 22, 2015 Filed under: Uncategorized | Tags: compassion, Dora Kunz, Energy healing, healing, Kawakami, Medicine, mindfulness, Muramatsu 3 Comments“Healing is best accomplished when art and science are conjoined, when body and spirit are probed together. Only when doctors can brood for the fate of a fellow human afflicted with fear and pain do they engage the unique individuality of a particular human being…a doctor thereby gains courage to deal with the pervasive uncertainties for which technical skill alone is inadequate. Patient and doctor then enter into a partnership as equals.
I return to my central thesis. Our health care system is breaking down because the medical profession has been shifting its focus away from healing, which begins with listening to the patient. The reasons for this shift include a romance with mindless technology.” Bernard Lown, MD, The Lost Art of Healing: Practicing Compassion in Medicine (1999)
I wanted to study with the healer and she instructed me to sit and observe, nothing more. She did not explain what she was doing, and provided no further instructions. Just observe. I did not understand. Yet, I continued to observe because she knew something, she did something that seemed to be associated with improvement and healing of many patients. A few showed remarkable improvement – at times it seemed miraculous. I felt drawn to understand. It was an unique opportunity and I was prepared to follow her guidance.

Three remarkable healers: Dora Kunz, Mitsumasa Kawakami and Norihiro Muramatsu.
The healer was remarkable. When she put her hands on the patient, I could see the patient’s defenses melt. At that moment, the patient seemed to feel safe, cared for, and totally nurtured. The patient felt accepted for just who she was and all the shame about the disease and past actions appeared to melt away. The healer continued to move her hands here and there and, every so often, she spoke to the client. Tears and slight sobbing erupted from the client. Then, the client became very peaceful and quiet. Eventually, the session was finished and the client expressed gratitude to the healer and reported that her lower back pain and the constriction around her heart had been released, as if a weight had been taken from her body.
How was this possible? I had so many questions to ask the healer: “What were you doing? What did you feel in your hands? What did you think? What did you say so softly to the client?” Yet, she did not help me understand how I could do this. The only instruction the healer kept giving me was to observe. Yes, she did teach me to be aware of the energy fields around the person and taught me how I could practice therapeutic touch (Kreiger, 1979; Kunz & Peper, 1995; Kunz & Krieger, 2004; Denison,2004; van Gelder & Chesley, F, 2015). But she was doing much more.
Sitting at the foot of the healer, observing for months, I often felt frustrated as she continued to insist that I just observe. How could I ever learn from this healer if she did not explain what I should do! Does the learning occur by activating my mirror neurons? Similar instructions are common in spiritual healing and martial arts traditions – the guru or mentor usually tells an apprentice to observe and be there. But how can one gain healing skills or spiritual healing abilities if you are only allowed to observe the process? Shouldn’t the healer be demonstrating actual practices and teaching skills?
After many sessions, I finally realized that the healer’s instruction to observe the healing was an indirect instruction. I began to learn how to be present without judging, to be present with compassion, to be present with total awareness in all senses, and to be present without frustration. The many hours at the foot of this master were not just wasted time. It eventually became clear that those hours of observation were important training and screening strategies used to insure that only those students who were motivated enough to master the discipline of non-judgmental observation, the discipline to be present and open to any experience, would continue to participate in the training process. It was training in compassionate mindfulness. Once apprentices achieved this state, they were ready to begin the work with clients and master the technical aspects of the specific healing art or spiritual practice.
A major component of the healing skill that relies on subtle energies is the ability to be totally present with the client without judgment (Peper, Gibney & Wilson, 2005; Peper, 2015). To be peaceful, caring, and present seems to create an energetic ambiance that sets stage, creates the space, for more subtle aspects of the healing interaction. This energetic ambiance is similar to feeling the love of a grandparent: feeling total acceptance from someone who just knows you are a remarkable human being. In the presence of a healer with such a compassionate presence, you feel safe, accepted, and engaged in a timeless state of mind, a state that promotes healing and regeneration as it dissolves long held defensiveness and fear-based habits of holding others at bay. This state of mind provides an opportunity for worries and unsettled emotions to dissipate. Feeling safe, accepted, and experiencing compassionate love supports the biological processes that nurture regeneration and growth.
How different this is from the more common experience with medical practitioners who sometimes have too little time to listen and to be with a patient. We might experience a medical provider as someone who may see us only as an illness (the cancer patient, the asthma patient) instead of recognizing us as a human being who happens to have an illness (a person with cancer or asthma). At times we can feel as though we are seen only as a series of numbers in a medical chart – yet we know we are more than that. People long to be seen. Often the medical provider interrupts with within the first 90 seconds with questions instead of listening. It becomes clear that the computerized medical record is more important than the human being seated there. Sometimes the patients can feel more fragmented and less safe, when they are not heard, not understood. In this rushed state, based upon “scientific data,” the health care provider may give a diagnosis without being aware of the emotional impact of the diagnosis.
As one 23 year old woman reported after being diagnosed with vulvodynia,”I cried immediately upon leaving the physician’s office. Even though he is an expert on the subject, I felt like I had no psychological support. I was on Gabapentin, and it made me very depressed. I thought to myself: Is my life, as I know it, over?” (Peper, Martinez Aranda, P., & Moss, 2015; Martinez Aranda, P. & Peper, E., 2015)
What was missing for this young woman was compassion and caring. Sometimes, the healthcare providers are unaware of the effect of their rushed behavior and lack of presence. They can issue a diagnosis based on the scientific data without recognizing the emotional impact on the person receiving it.
Sitting at the foot of the master healer is not wasted time when the apprentice learns how to genuinely attend to another with non-judgmental, compassionate presence. However, this requires substantial personal work. Possibly all allied healthcare providers should be required, or at least invited, to learn how to attain the state of mind that can enhance healing. Perhaps the practice of medicine could change if, as Bernard Lown wrote, the focus were once again on healing, “…which begins with listening to the patient.”
References
Denison, B. (2004). Touch the pain away: New research on therapeutic touch and persons with fibromyalgia syndrome. Holistic nursing practice, 18(3), 142-150.
Krieger, D. (1979). The therapeutic touch: How to use your hands to help or to heal. Vol. 15. Englewood Cliffs, NJ: Prentice-Hall.
Kunz, D. & Krieger, K. (2004). The spiritual dimension of therapeutic touch. Rochester, VT: Inner Traditions/Bear & Co.
Kunz, D., & Peper, E. (1995). Fields and their clinical implications. in Kunz, D.,(ed). Spiritual Aspects of the Healing Arts. Wheaton, ILL: Theosophical Pub House, 213-222.
Lown, B. (1999). The lost art of healing: Practicing compassion in medicine. New York, NY: Ballantine Books.
Martinez Aranda, P. & Peper, E. (2015). The healing of vulvodynia from the client’s perspective.
Peper, E. (2015). Towards the end of suffering: The contributions of integrating mind, body and spirit by Mr. Kawakami. In: Kawakami, M., Peper, E., & Kakigi, R. (2015). Cerebral investigation of a Yoga Master during Meditation-Findings from Collaborative Research. Fukuoka, Japan: Showado Publisher, 7-13.
Peper, E., Gibney, K. H. & Wilson, V. E. (2005). Enhancing Therapeutic Success–Some Observations from Mr. Kawakami: Yogi, Teacher, Mentor and Healer. Somatics. XIV (4), 18-21
Peper, E., Martinez Aranda, P., & Moss, E. (2015). Vulvodynia treated successfully with breathing biofeedback and integrated stress reduction: A case report. Biofeedback, 43(2), 103-109.
Van Gelder, K & Chesley, F. (2015). A Most Unusual Life. Wheaton Ill: Theosophical Publishing House.
Notes:
- I thank Peter Parks for his superb editorial support and encouraging me to publish it.
- This blog was adapted the following two published articles, Peper, E. (2015). Compassionate Presence: Covert Training Invites Subtle Energies Insights. Subtle Energies Magazine, 26(2), 22-25; Peper, E. Sitting at the foot of the master-Covert training in compassionate presence. Somatics, 18(3), 46-47.
Less Medicine, More Health?
Posted: October 19, 2015 Filed under: Uncategorized | Tags: decision making, health, iatrogenic disease, medical testing, Medicine 1 CommentShould I get a body scan?
How aggressively should I lower my blood sugar level as I have type 2 diabetes?
I have no symptoms, should I get a routine mammogram?
I feel great, should I follow my doctor’s advice and have my annual physical?
These and hundreds of other questions often imply that the more medical care the better and healthier you will be. We assume that more care, more testing, the newer the drug, the more screening, etc. will prevent illness and promote health. In numerous cases this is not true! Although medical care can be superb for the treatment of acutely ill and injured, excessive use sometimes leads to harm.
In a superb book, Less Medicine, More Health, by Dr. H. Gilbert Welch, professor at Dartmouth Medical School and recognized expert on the effects of medical testing, the following seven basic assumptions underlying too much medical care are described in a readable and personable style.
- All risks can be lowered
- It’s always better to fix the problem
- Sooner is always better
- It never hurts to get more information
- Action is always better than inaction
- Newer is always better
- It’s all about avoiding death
Welch’s book explains the assumptions and the limitations of the assumption. Before assuming that the recommended medical procedures will improve your health—in some cases it will make you sicker—read his book, Less Medicine More Health.

Welch, H.G. (2015). Less Medicine, More Health. Boston: Beacon Press. ISBM 978-0-8070-7164-9
