Resolving pelvic floor pain-A case report
Posted: September 25, 2015 Filed under: Breathing/respiration, Pain/discomfort, self-healing, stress management, Uncategorized | Tags: biofeedback, Breathing, electromyography, pain, posture, self-regulation, vulvodynia 10 CommentsAdapted from: Martinez Aranda, P. & Peper, E. (2015). The healing of vulvodynia from a client’s perspective. https://biofeedbackhealth.files.wordpress.com/2011/01/a-healing-of-vulvodynia-from-the-client-perspective-2015-06-15.pdf
It’s been a little over a year since I began practicing biofeedback and visualization strategies to overcome vulvodynia. Today, I feel whole, healed, and hopeful. I learned that through controlled and conscious breathing, I could unleash the potential to heal myself from chronic pain. Overcoming pain did not happen overnight; but rather, it was a process where I had to create and maintain healthy lifestyle habits and meditation. Not only am I thankful for having learned strategies to overcome chronic pain, but for acquiring skills that will improve my health for the rest of my life. –-24 year old woman who successfully resolved vulvodynia
Pelvic floor pain can be debilitating, and it is surprisingly common, affecting 10 to 25% of American women. Pelvic floor pain has numerous causes and names. It can be labeled as vulvar vestibulitis, an inflammation of vulvar tissue, interstitial cystitis (chronic pain or tenderness in the bladder), or even lingering or episodic hip, back, or abdominal pain. Chronic pain concentrated at the entrance to the vagina (vulva), is known as vulvodynia. It is commonly under-diagnosed, often inadequately treated, and can go on for months and years (Reed et al., 2007; Mayo Clinic, 2014). The discomfort can be so severe that sitting is uncomfortable and intercourse is impossible because of the extreme pain. The pain can be overwhelming and destructive of the patient’s life. As the participant reported,
I visited a vulvar specialist and he gave me drugs, which did not ease the discomfort. He mentioned surgical removal of the affected tissue as the most effective cure (vestibulectomy). I cried immediately upon leaving the physician’s office. Even though he is an expert on the subject, I felt like I had no psychological support. I was on Gabapentin to reduce pain, and it made me very depressed. I thought to myself: Is my life, as I know it, over?
Physically, I was in pain every single day. Sometimes it was a raging burning sensation, while other times it was more of an uncomfortable sensation. I could not wear my skinny jeans anymore or ride a bike. I became very depressed. I cried most days because I felt old and hopeless instead of feeling like a vibrant 23-year-old woman. The physical pain, combined with my negative feelings, affected my relationship with my boyfriend. We were unable to have sex at all, and because of my depressed status, we could not engage in any kind of fun. (For more details, read the published case report,Vulvodynia treated successfully with breathing biofeedback and integrated stress reduction: A case report).
The four-session holistic biofeedback interventions to successfully resolved vulvodynia included teaching diaphragmatic breathing to transform shallow thoracic breathing into slower diaphragmatic breathing, transforming feelings of powerlessness and hopelessness to empowerment and transforming her beliefs that she could reduce her symptoms and optimize her health. The interventions also incorporated self-healing imagery and posture-changing exercises. The posture changes consisted of developing awareness of the onset of moving into a collapsed posture and use this awareness to shift to an erect/empowered postures (Carney, Cuddy, & Yap, 2010; Peper, 2014; Peper, Booiman, Lin, & Harvey, in press). Finally, this case report build upon the seminal of electromyographic feedback protocol developed by Dr. Howard Glazer (Glazer & Hacad, 2015) and the integrated relaxation protocol developed Dr. David Wise (Wise & Anderson, 2007).
Through initial biofeedback monitoring of the lower abdominal muscle activity, chest, and abdomen breathing patterns, the participant observed that when she felt discomfort or was fearful, her lower abdomen muscles tended to tighten. After learning how to sense this tightness, she was able to remind herself to breathe lower and slower, relax the abdominal wall during inhalation and sit or stand in an erect power posture.
The self-mastery approach for healing is based upon a functional as compared to a structural perspective. The structural perspective implies that the problem can only be fixed by changing the physical structure such as with surgery or medications. The functional perspective assumes that if you can learn to change your dysfunctional psychophysiological patterns the disorder may disappear.
The functional approach assumed that an irritation of the vestibular area might have caused the participant to tighten her lower abdomen and pelvic floor muscles reflexively in a covert defense reaction. In addition, ongoing worry and catastrophic thinking (“I must have surgery, it will never go away, I can never have sex again, my boyfriend will leave me”) also triggered the defense reaction—further tightening of her lower abdomen and pelvic area, shallow breathing, and concurrent increases in sympathetic nervous activation—which together activated the trigger points that lead to increased chronic pain (Banks et al, 1998).
When the participant experienced a sensation or thought/worried about the pain, her body responded in a defense reaction by breathing in her chest and tightening the lower abdominal area as monitored with biofeedback. Anticipation of being monitored increased her shoulder tension, recalling the stressful memory increased lower abdominal muscle tension (pulling in the abdomen for protection), and the breathing became shallow and rapid as shown in Figure 1.
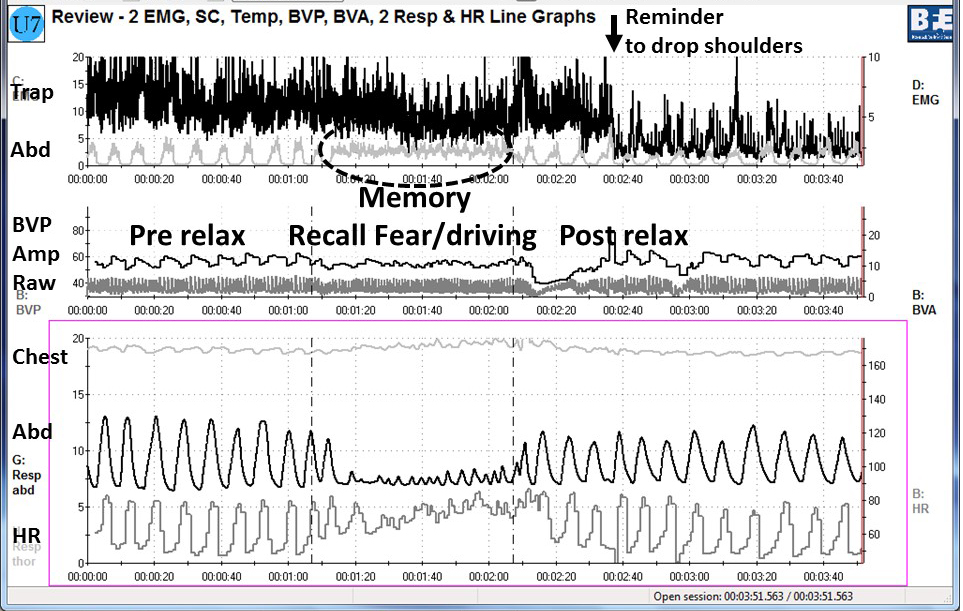
Figure 1. Physiological recording of pre-stressor relaxation, the recall of a fearful driving experience, and a post-stressor relaxation. The scalene to trapezius SEMG increased in anticipation while she recalled the experience, and then initially did not relax (from Peper, Martinez Aranda, & Moss, 2015).
This defense pattern became a conditioned response—initiating intercourse or being touched in the affected area caused the participant to tense and freeze up. She was unaware of these automatic protective patterns, which only worsened her chronic pain.
During the four sessions of training, the participant learned to reverse and interrupt the habitual defense reaction. For example, as she became aware of her breathing patterns she reported,
It was amazing to see on the computer screen the difference between my regular breathing pattern and my diaphragmatic breathing pattern. I could not believe I had been breathing that horribly my whole life, or at least, for who knows how long. My first instinct was to feel sorry for myself. Then, rather than practicing negative patterns and thoughts, I felt happy because I was learning how to breathe properly. My pain decreased from an 8 to alternating between a 0 and 3.
The mastery of slower and lower abdominal breathing within a holistic perspective resulted in the successful resolution of her vulvodynia. An essential component of the training included allowing the participant to feel safe, and creating hope by enabling her to experience a decrease in discomfort while doing a specific practice, and assisting her to master skills to promote self-healing. Instead of feeling powerless and believing that the only resolution was the removal of the affected area (vestibulectomy). The integrated biofeedback protocol offered skill mastery training, to promote self-healing through diaphragmatic breathing, somatic postural changes, reframing internal language, and healing imagery as part of a common sense holistic health approach.
For more details about the case report, download the published study, Peper, E., Martinez Aranda, P., & Moss, E. (2015). Vulvodynia treated successfully with breathing biofeedback and integrated stress reduction: A case report. Biofeedback. 43(2), 103-109.
The participant also wrote up her subjective experience of the integrated biofeedback process in the paper, Martinez Aranda & Peper (2015). Healing of vulvodynia from the client perspective. In this paper she articulated her understanding and experiences in resolving vulvodynia which sheds light on the internal processes that are so often skipped over in published reports.
At the five year follow-up on May 29, 2019, she wrote:
“I am doing very well, and I am very healthy. The vulvodynia symptoms have never come back. It migrated to my stomach a couple of years after, and I still have a sensitive stomach. My stomach has gotten much, much better, though. I don’t really have random pain anymore, now I just have to be watchful and careful of my diet and my exercise, which are all great things!”
References
Banks, S. L., Jacobs, D. W., Gevirtz, R., & Hubbard, D. R. (1998). Effects of autogenic relaxation training on electromyographic activity in active myofascial trigger points. Journal of Musculoskeletal Pain, 6(4), 23-32. https://www.researchgate.net/profile/David_Hubbard/publication/232035243_Effects_of_Autogenic_Relaxation_Training_on_Electromyographic_Activity_in_Active_Myofascial_Trigger_Points/links/5434864a0cf2dc341daf4377.pdf
Carney, D. R., Cuddy, A. J., & Yap, A. J. (2010). Power posing brief nonverbal displays affect neuroendocrine levels and risk tolerance. Psychological Science, 21(10), 1363-1368. Available from: https://www0.gsb.columbia.edu/mygsb/faculty/research/pubfiles/4679/power.poses_.PS_.2010.pdf
Glazer, H. & Hacad, C.R. (2015). The Glazer Protocol: Evidence-Based Medicine Pelvic Floor Muscle (PFM) Surface Electromyography (SEMG). Biofeedback, 40(2), 75-79. http://www.aapb-biofeedback.com/doi/abs/10.5298/1081-5937-40.2.4
Martinez Aranda, P. & Peper, E. (2015). Healing of vulvodynia from the client perspective. Available from: https://biofeedbackhealth.files.wordpress.com/2011/01/a-healing-of-vulvodynia-from-the-client-perspective-2015-06-15.pdf
Mayo Clinic (2014). Diseases and conditions: Vulvodynia. Available at http://www.mayoclinic.org/diseases-conditions/vulvodynia/basics/definition/con-20020326
Peper, E. (2014). Increasing strength and mood by changing posture and sitting habits. Western Edition, pp.10, 12. Available from: http://thewesternedition.com/admin/files/magazines/WE-July-2014.pdf
Peper, E., Booiman, A., Lin, I, M.,& Harvey, R. (in press). Increase strength and mood with posture. Biofeedback.
Peper, E., Martinez Aranda, P., & Moss, E. (2015). Vulvodynia treated successfully with breathing biofeedback and integrated stress reduction: A case report. Biofeedback. 43(2), 103-109. Available from: https://biofeedbackhealth.files.wordpress.com/2011/01/a-vulvodynia-treated-with-biofeedback-published.pdf
Reed, B. D., Haefner, H. K., Sen, A., & Gorenflo, D. W. (2008). Vulvodynia incidence and remission rates among adult women: a 2-year follow-up study. Obstetrics & Gynecology, 112(2, Part 1), 231-237. http://journals.lww.com/greenjournal/Abstract/2008/08000/Vulvodynia_Incidence_and_Remission_Rates_Among.6.aspx
Wise, D., & Anderson, R. U. (2006). A headache in the pelvis: A new understanding and treatment for prostatitis and chronic pelvic pain syndromes. Occidental, CA: National Center for Pelvic Pain Research.http://www.pelvicpainhelp.com/books/
Interrupt Chained Behaviors: Overcome Smoking, Eczema, and Hair Pulling
Posted: March 7, 2015 Filed under: self-healing, stress management, Uncategorized | Tags: chained behavior, eczema, hair pulling, healing, self-monitoring, smoking cessation, stress management, trichotillomania 7 Comments“I am proud to label myself a nonsmoker… diligently performing practices has profoundly helped me eliminate my troublesome craving…The conscious efforts I have made over the past month have helped me regain control of my life.” –L. F., a college student who became a non-smoker after smoking up to two packs a day since age 11. At 18 month follow-up L. F. is still a nonsmoker.
“I have been struggling with eczema for most of my life and until I began this course, I was feeling very hopeless in managing this condition without the use of costly, and potentially dangerous drugs. My self-healing project proved to be empirically successful. My eczema shrunk in size from 72 mm in length and 63 mm in width as measured at baseline to 0 mm in length and 0 mm in width by the final day of this project.” –L. C., a college student who experienced recurring scaly skin patches since childhood.
In our recent published paper, Transforming chained behaviors: Case studies of overcoming smoking, eczema and hair pulling (trichotillomania), we describe an approach by which students learn self-healing techniques which they practice as part of a semester long class project. After four weeks of of self-healing practices many of the students report significant decrease in symptoms and improvement of health as shown in Figure 1. Their success includes smoking cessation, eliminating hair pulling and eczema disappearing.
 Figure 1. Students’ self-rating of success in achieving health benefits after four weeks of practice.
Figure 1. Students’ self-rating of success in achieving health benefits after four weeks of practice.
One component of the self-healing process is interrupting chained behavior. We react automatically and respond instantly with sadness, anger, neck and shoulders tension, eating too much, veg’ing out watching videos, or playing mindless digital games. After a time, we may notice that we are smoking more, experiencing an upset stomach, back pain, headaches, high blood pressure, or even more skin eruptions. The first step is to sense the initial reaction that leads to the symptom development. Then, the person performs an alternative health promoting behavior and interrupts the chained behavior that triggers symptoms as shown in Figure 2.
 Figure 2. Interrupting and transforming the chained behavior. The moment person become aware of the trigger or behavior that is chained to the development of the symptom, he/she interrupts and performs an active new health promoting behavior as illustrated by the dashed lines.
Figure 2. Interrupting and transforming the chained behavior. The moment person become aware of the trigger or behavior that is chained to the development of the symptom, he/she interrupts and performs an active new health promoting behavior as illustrated by the dashed lines.
Overtime these automatic patterns may contribute to the development of autoimmune diseases, increased vulnerability to infections or other chronic diseases. The challenge is to develop an awareness to recognize and interrupt the beginning of the ‘chain of behavior.’ The instant you become aware of the first reaction, do something different, such as,
- Shift your focus of attention to something joyful
- Chang your body position and smile while thinking, This will also pass.
- Practice a quick relaxation technique.
- Imagine a positive self-healing process.
The longer the person waits to interrupt the chain, the more difficult it is to redirect the chained behavior. Awareness and immediate interruption appears to be major factors in achieving success. It means practicing the interruption and new behavior all day long. This is different from from practicing a skill for twenty minutes a day and the rest of the time performing the old dysfunctional behavior.
Mastery of this process consists of three steps:
- Becoming aware of what is happening when the chain reactions.
- Learn a more functional alternative health behavior such as breathing, relaxing, focusing on empowering thought, eating other foods.
- Substitute the alternative behavior the moment you become aware of the triggered dysfunctional behavior.
After having integrated this into daily life, many students report experiencing a significant reduction and even elimination of symptoms and behaviors.
“I will continue to do the practices outlined not only to overcome trichotillomania but also to control my anxiety and, therefore, lead a less stressed and happier life. Knowing I have the power to heal myself is such an inspiring feeling, a feeling that can’t adequately be put into words.” –G. M., a 32 year old student with trichotillomania, who reduced her hair pulling, anxiety, and stress
“I have gained much wisdom from this project…I am ultimately responsible for my own health and well-being…I feel empowered, optimistic, and appreciative of every moment.” –L. C., a college student who experienced recurring scaly skin patches since childhood)
For background, specific techniques and successful case reports, read our published paper, Peper, E., Lin, I-M, Harvey, R., Gilbert, M., Gubbala, P., Ratkovich, A., & Fletcher, F. (2014). Transforming chained behaviors: Case studies of overcoming smoking, eczema and hair pulling (trichotillomania). Biofeedback, 42(4), 154-160.
Reduce hot flashes and premenstrual symptoms with breathing
Posted: February 18, 2015 Filed under: Breathing/respiration, Pain/discomfort, self-healing, stress management, Uncategorized | Tags: biofeedback, Breathing, diaphragmatic breathing, heart rate variability, hormone replacement therapy, hot flashes, HRT, Menopause, respiration, sighs, stress, sympathetic activity 6 CommentsAfter the first week to my astonishment, I have fewer hot flashes and they bother me less. Each time I feel the warmth coming, I breathe out slowly and gently. To my surprise they are less intense and are much less frequent. I keep breathing slowly throughout the day. This is quite a surprise because I was referred for biofeedback training because of headaches that occurred after getting a large electrical shock. After 5 sessions my headaches have decreased and I can control them, and my hot flashes have decreased from 3-4 per day to 1-2 per week. -50 year old client
After students in my Holistic Health class at San Francisco State University practiced slower diaphragmatic breathing and begun to change their dysfunctional shallow breathing, gasping, sighing, and breath holding to diaphragmatic breathing. A number of the older female students students reported that their hot flashes decreased. Some of the younger female students reported that their menstrual cramps and discomfort were reduced by 80 to 90% when they laid down and breathed slower and lower into their abdomen.
 The recent study in JAMA reported that many women continue to experience menopausal triggered hot flashes for up to 14 years. Although the article described the frequency and possible factors that were associated with the prolonged hot flashes, it did not offer helpful solutions.
The recent study in JAMA reported that many women continue to experience menopausal triggered hot flashes for up to 14 years. Although the article described the frequency and possible factors that were associated with the prolonged hot flashes, it did not offer helpful solutions.
Another understanding of the dynamics of hot flashes is that the decrease in estrogen accentuates the sympathetic/ parasympathetic imbalances that probably already existed. Then any increase in sympathetic activation can trigger a hot flash. In many cases the triggers are events and thoughts that trigger a stress response, emotional responses such as anger, anxiety, or worry, increase caffeine intake and especially shallow chest breathing punctuated with sighs. Approximately 80% of American women tend to breathe thoracically often punctuated with sighs and these women are more likely to experience hot flashes. On the other hand, the 20% of women who habitually breathe diaphragmatically tend to have fewer and less intense hot flashes and often go through menopause without any discomfort. In the superb study Drs. Freedman and Woodward (1992), taught women who experience hot flashes to breathe slowly and diaphragmatically which increased their heart rate variability as an indicator of sympathetic/parasympathetic balance and most importantly it reduced the the frequency and intensity of hot flashes by 50%.
Test the breathing connection if you experience hot flashes
Take a breath into your chest and rapidly exhale with a sigh. Repeat this quickly five times. In most cases, one minute later you will experience the beginning sensations of a hot flash. Similarly, when you practice slow diaphragmatic breathing throughout the day and interrupt every gasp, breath holding moment, sigh or shallow chest breathing with slower diaphragmatic breathing, you will experience a significant reduction in hot flashes.
Although this breathing approach has been well documented, many people are unaware of this simple behavioral approach unlike the common recommendation for the hormone replacement therapies (HRT) to ameliorate menopausal symptoms. This is not surprising since pharmaceutical companies spent nearly five billion dollars per year in direct to consumer advertising for drugs and very little money is spent on advertising behavioral treatments. There is no profit for pharmaceutical companies teaching effortless diaphragmatic breathing unlike prescribing HRTs. In addition, teaching and practicing diaphragmatic breathing takes skill training and practice time–time which is not reimbursable by third party payers.
For more information, research data and breathing skills to reduce hot flash intensity, see our article which is reprinted below.
Gibney, H.K. & Peper, E. (2003). Taking control: Strategies to reduce hot flashes and premenstrual mood swings. Biofeedback, 31(3), 20-24.
Taking control: Strategies to reduce hot flashes and premenstrual mood swings*
Erik Peper, Ph.D**., and Katherine H. Gibney
San Francisco State University
After the first week to my astonishment, I have fewer hot flashes and they bother me less. Each time I feel the warmth coming, I breathe out slowly and gently. To my surprise they are less intense and are much less frequent. I keep breathing slowly throughout the day. This is quite a surprise because I was referred for biofeedback training because of headaches that occurred after getting a large electrical shock. After 5 sessions my headaches have decreased and I can control them, and my hot flashes have decreased from 3-4 per day to 1-2 per week. -50 year old client
For the first time in years, I experienced control over my premenstrual mood swings. Each time I could feel myself reacting, I relaxed, did my autogenic training and breathing. I exhaled. It brought me back to center and calmness. -26 year old student
Abstract
Women have been troubled by hot flashes and premenstrual syndrome for ages. Hormone replacement therapy, historically the most common treatment for hot flashes, and other pharmacological approaches for pre-menstrual syndrome (PMS) appear now to be harmful and may not produce significant benefits. This paper reports on a model treatment approach based upon the early research of Freedman & Woodward to reduce hot flashes and PMS using biofeedback training of diaphragmatic breathing, relaxation, and respiratory sinus arrhythmia. Successful symptom reduction is contingent upon lowering sympathetic arousal utilizing slow breathing in response to stressors and somatic changes. We strongly recommend that effortless diaphragmatic breathing be taught as the first step to reduce hot flashes and PMS symptoms.
A long and uncomfortable history
Women have been troubled by hot flashes and premenstrual syndrome for ages. Hot flashes often result in red faces, sweating bodies, and noticeable and embarrassing discomfort. They come in the middle of meetings, in the middle of the night, and in the middle of romantic interludes. Premenstrual syndrome also arrives without notice, bringing such symptoms as severe mood swings, anger, crying, and depression.
Hormone replacement therapy (HRT) was the most common treatment for hot flashes for decades. However, recent randomized controlled trials show that the benefits of HRT are less than previously thought and the risks—especially of invasive breast cancer, coronary artery disease, dementia, stroke and venous thromboembolism—are greater (Humphries & Gill, 2003; Shumaker, et al, 2003; Wassertheil-Smoller, et al, 2003). In addition, there is no evidence of increased quality of life improvements (general health, vitality, mental health, depressive symptoms, or sexual satisfaction) as claimed for HRT (Hays et al, 2003).
“As a result of recent studies, we know that hormone therapy should not be used to prevent heart disease. These studies also report an increased risk of heart attack, stroke, breast cancer, blood clots, and dementia…” -Wyeth Pharmaceuticals (2003)
Because of the increased long-term risk and lack of benefit, many physicians are weaning women off HRT at a time when the largest population of maturing women in history (‘baby boomers’) is entering menopausal years. The desire to find a reliable remedy for hot flashes is on the front burner of many researchers’ minds, not to mention the minds of women suffering from these ‘uncontrollable’ power surges. Yet, many women are becoming increasingly leery of the view that menopause is an illness. There is a rising demand to find a natural remedy for this natural stage in women’s health and development.
For younger women a similar dilemma occurs when they seek treatment of discomfort associated with their menstrual cycle. Is premenstrual syndrome (PMS) just a natural variation in energy and mood levels? Or, are women expected to adapt to a masculine based environment that requires them to override the natural tendency to perform in rhythm with their own psychophysiological states? Instead of perceiving menstruation as a natural occurrence in which one has different moods and/or energy levels, women in our society are required to perform at the status quo, which may contribute to PMS. The feelings and mood changes are quickly labeled as pathology that can only be treated with medication.
Traditionally, premenstrual syndrome is treated with pharmaceuticals, such as birth control pills or Danazol. Although medications may alleviate some symptoms, many women experience unpleasant side effects, such as bloating or acne, and still experience a variety of PMS symptoms. Many cannot tolerate the medications. Thus, millions of women (and families) suffer monthly bouts of ‘uncontrollable’ PMS symptoms
For both hot flashes and PMS the biomedical model tends to frame the symptoms as a “structural biological problem.” Namely, the pathology occurs because the body is either lacking in, or has an excess of, some hormone. All that needs to be done is either augment or suppress hormones/symptoms with some form of drug. Recently, for example, medicine has turned to antidepressant medications to address menopausal hot flashes (Stearns, Beebe, Iyengar, & Dube, 2003).
The biomedical model, however, is only one perspective. The opposite perspective is that the dysfunction occurs because of how we use ourselves. Use in this sense means our thoughts, emotions and body patterns. As we use ourselves, we change our physiology and, thereby, may affect and slowly change the predisposing and maintaining factors that contribute to our dysfunction. By changing our use, we may reduce the constraints that limit the expression of the self-healing potential that is intrinsic in each person.
The intrinsic power of self-healing is easily observed when we cut our finger. Without the individual having to do anything, the small cut bleeds, clotting begin and tissue healing is activated. Obviously, we can interfere with the healing process, such as when we scrape the scab, rub dirt in the wound, reduce blood flow to the tissue or feel anxious or afraid. Conversely, cleaning the wound, increasing blood flow to the area, and feeling “safe” and relaxed can promote healing. Healing is a dynamic process in which both structure and use continuously affect each other. It is highly likely that menopausal hot flashes and PMS mood swings are equally an interaction of the biological structure (hormone levels) and the use factor (sympathetic/parasympathetic activation).
Uncontrollable or overly aroused?
Are the hot flashes and PMS mood swings really ‘uncontrollable?’ From a physiological perspective, hot flashes are increased by sympathetic arousal. When the sympathetic system is activated, whether by medication or by emotions, hot flashes increase and similarly, when sympathetic activity decreases hot flashes decrease. Equally, PMS, with its strong mood swings, is aggravated by sympathetic arousal. There are many self-management approaches that can be mastered to change and reduce sympathetic arousal, such as breathing, meditation, behavioral cognitive therapy, and relaxation.
Breathing patterns are closely associated with hot flashes. During sleep, a sigh generally occurs one minute before a hot flash as reported by Freedman and Woodward (1992). Women who habitually breathe thoracically (in the chest) report much more discomfort and hot flashes than women who habitually breathe diaphragmatically. Freedman, Woodward, Brown, Javaid, and Pandey (1995) and Freedman and Woodward (1992) found that hot flash rates during menopause decreased in women who practiced slower breathing for two weeks. In their studies, the control groups received alpha electroencephalographic feedback and did not benefit from a reduction of hot flashes. Those who received training in paced breathing reduced the frequency of their hot flashes by 50% when they practiced slower breathing. This data suggest that the slower breathing has a significant effect on the sympathetic and parasympathetic balance.
Women with PMS appear similarly able to reduce their discomfort. An early study utilizing Autogenic Training (AT) combined with an emphasis on warming the lower abdomen resulted in women noting improvement in dysfunctional bleeding (Luthe & Schultz, 1969, pp. 144-148). Using a similar approach, Mathew, Claghorn, Largen, and Dobbins (1979) and Dewit (1981) found that biofeedback temperature training was helpful in reducing PMS symptoms.. A later study by Goodale, Domar, and Benson (1990) found that women with severe PMS symptoms who practiced the relaxation response reported a 58% improvement in overall symptomatology as compared to a 27.2% improvement for the reading control group and a 17.0% improvement for the charting group.
Teaching control and achieving results
Teaching women to breathe effortlessly can lead to positive results and an enhanced sense of control. By effortless breathing, the authors refer to their approach to breath training, which involves a slow, comfortable respiration, larger volume of air exchange, and a reliance upon action of the muscles of the diaphragm rather than the chest (Peper, 1990). For more instructions see the recent blog, A breath of fresh air: Improve health with breathing.
Slowing breathing helps to limit the sighs common to rapid thoracic breathing—sighs that often precede menopausal hot flashes. Effortless breathing is associated with stress reduction—stress and mood swings are common concerns of women suffering from PMS. In a pilot study Bier, Kazarian, Peper, and Gibney (2003) at San Francisco State University (SFSU) observed that when the subject practiced diaphragmatic breathing throughout the month, combined with Autogenic Training, her premenstrual psychological symptoms (anger, depressed mood, crying) and premenstrual responses to stressors were significantly reduced as shown in Figure 1.
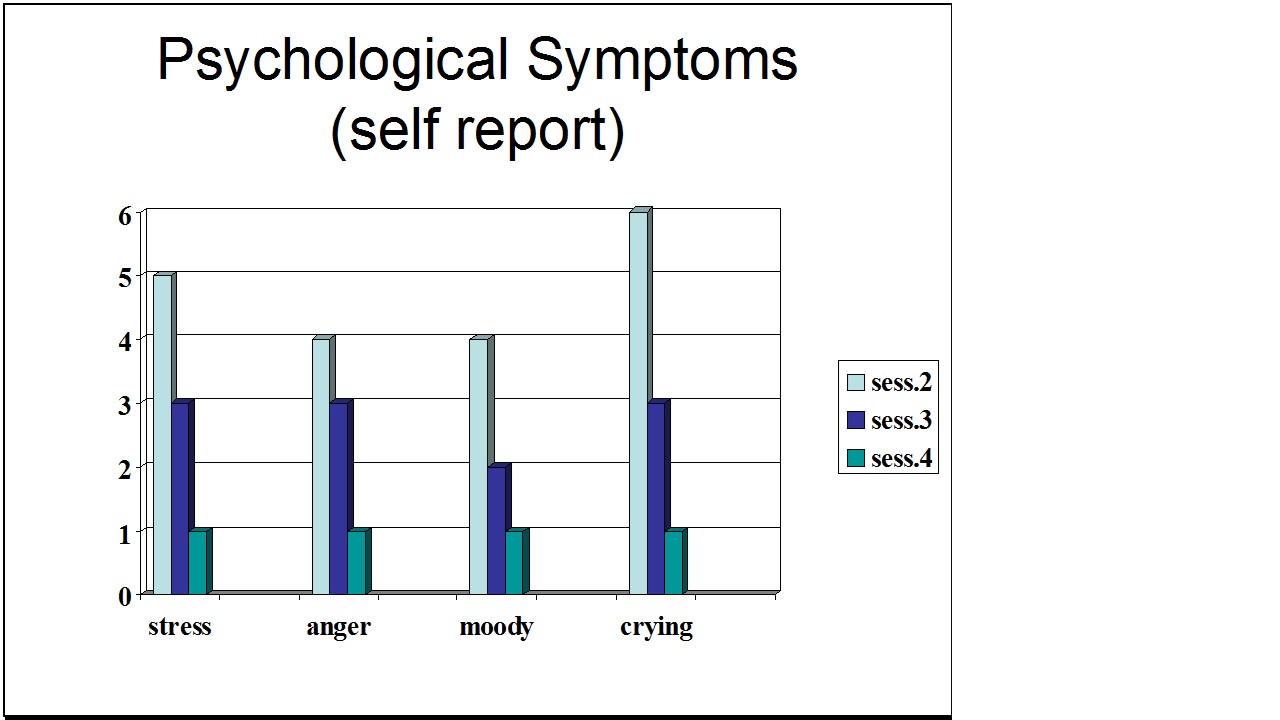
Figure 1. Student’s Individual Subjective Rating in Response to PMS Symptoms.
In another pilot study at SFSU, Frobish, Peper, and Gibney (2003) trained a volunteer who suffered from frequent hot flashes to breathe diaphragmatically. The training goals included modifying breathing patterns, producing a Respiratory Sinus Arrhythmia (RSA), and peripheral hand warming. RSA refers to a pattern of slow, regular breathing during which variations in heart rate enter into a synchrony with the respiration. Each inspiration is accompanied by an increase in heart rate, and each expiration is accompanied by a decrease in heart rate (with some phase differences depending on the rate of breathing). The presence of the RSA pattern is an indication of optimal balance between sympathetic and parasympathetic nervous activity.
During the 11-day study period, the subject charted the occurrence of hot flashes and noted a significant decrease by day 5. However, on the evening of day 7 she sprained her ankle and experienced a dramatic increase in hot flashes on day 8. Once the subject recognized her stress response, she focused more on breathing and was able to reduce the flashes as shown in Figure 2. 
Figure 2. Subjective rating of intensity, frequency and bothersomeness of hot flashes. The increase in hot flashes coincided with increased frustration about an ankle injury.
Our clinical experience confirms the SFSU pilot studies and the previously referenced research by Freedman and Woodward (1992) and Freedman et al. (1995). When arousal is lowered and breathing is effortless, women are better able to cope with stress and report a reduction in symptoms. Habitual rapid thoracic breathing tends to increase arousal while slower breathing, especially slower exhalation, tends to relax and reduce arousal. Learning and then applying effortless breathing reduces excessive sympathetic arousal. It also interrupts the cycle of cognitive activation, anxiety, and somatic arousal. The anticipation and frustration at having hot flashes becomes the cue to shift attention and “breathe slower and lower.” This process stops the cognitively mediated self-activation.
Successful self-regulation and the return to health begin with cognitive reframing: We are not only a genetic biological fixed (deficient) structure but also a dynamic changing system in which all parts (thoughts, emotions, behavior, diet, stress, and physiology) affect and are effected by each other. Within this dynamic changing system, there is an opportunity to implement and practice behaviors and life patterns that promote health.
Learning Diaphragmatic Breathing with and without Biofeedback
Although there are many strategies to modify respiration, biofeedback monitoring combined with respiration training is very useful as it provides real-time feedback. Chest and abdominal movement are recorded with strain gauges and heart rate can be monitored either by an electrocardiogram (EKG) or by a photoplethysmograph sensor on a finger or thumb. Peripheral temperature and electrodermal activity (EDA) biofeedback are also helpful in training. The training focuses on teaching effortless diaphragmatic breathing and encouraging the participant to practice many times during the day, especially when becoming aware of the first sensations of discomfort.
Learning and integrating effortless diaphragmatic breathing into daily life is one of the biofeedback strategies that has been successfully used as a primary or adjunctive/complementary tool for the reversal of disorders such as hypertension, migraine headaches, repetitive strain injury, pain, asthma and anxiety (Schwartz & Andrasik, 2003), as well as hot flashes and PMS.
The biofeedback monitoring provides the trainer with a valuable tool to:
- Observe & identify: Dysfunctional rapid thoracic breathing patterns, especially in response to stressors, are clearly displayed in real-time feedback.
- Demonstrate & train: The physiological feedback display helps the person see that she is breathing rapidly and shallowly in her chest with episodic sighs. Coaching with feedback helps her to change her breathing pattern to one that promotes a more balanced homeostasis.
- Motivate, persuade and change beliefs: The person observes her breathing patterns change concurrently with a felt shift in physiology, such as a decrease in irritability, or an increase in peripheral temperature, or a reduction in the incidence of hot flushes. Thus, she has a confirmation of the importance of breathing diaphragmatically.
In addition, we suggest exercises that integrate verbal and kinesthetic instructions, such as the following: “Exhale gently,” and “Breathe down your leg with a partner.”
Exhale Gently:
Imagine that you are holding a baby. Now with your shoulders relaxed, inhale gently so that your abdomen widens. Then as you exhale, purse your lips and very gently and softly blow over the baby’s hair. Allow your abdomen to narrow when exhaling. Blow so softly that the baby’s hair barely moves. At the same time, imagine that you can allow your breath to flow down and through your legs. Continue imagining that you are gently blowing on the baby’s hair while feeling your breath flowing down your legs. Keep blowing very softly and continuously.
Practice exhaling like this the moment that you feel any sensation associated with hot flashes or PMS symptoms. Smile sweetly as you exhale.
Breathe Down Your Legs with a Partner
Sit or lie comfortably with your feet a shoulder width apart. As you exhale softly whisper the sound “Haaaaa….” Or, very gently press your tongue to your pallet and exhale while making a very soft hissing sound.
Have your partner touch the side of your thighs. As you exhale have your partner stroke down your thighs to your feet and beyond, stroking in rhythm with your exhalation. Do not rush. Apply gentle pressure with the stroking. Do this for four or five breaths.
Now, continue breathing as you imagine your breath flowing through your legs and out your feet.
During the day remember the feeling of your breath flowing downward through your legs and out your feet as you exhale.
Learning Strategies in Biofeedback Assisted Breath Training
Common learning strategies that are associated with the more successful amelioration of hot flashes and PMS include:
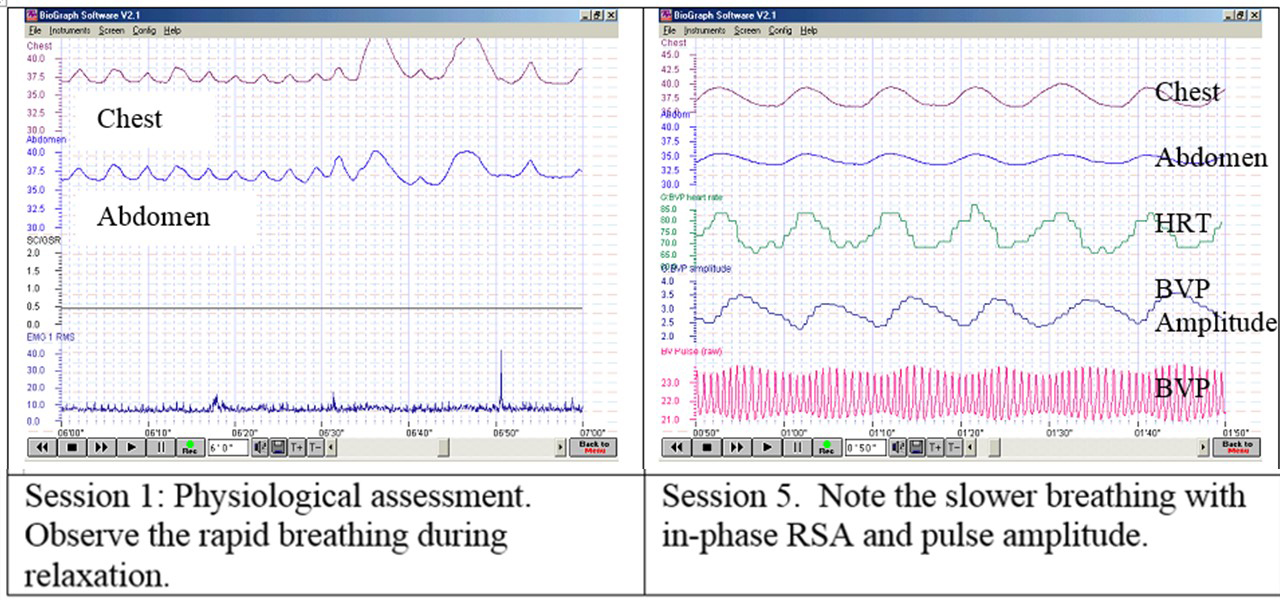
- Master effortless diaphragmatic breathing, and concurrently increase respiratory sinus arrhythmia (RSA). Instead of breathing rapidly, such as at 18 breaths per minute, the person learns to breathe effortlessly and slowly (about 6 to 8 breaths per minute). This slower breathing and increased RSA is an indication of sympathetic-parasympathetic balance as shown in Figure 3.
- Practice slow effortless diaphragmatic breathing many times during the day and, especially in response to stressors.
- Use the physical or emotional sensations of a hot flash or mood alteration as the cue to exhale, let go of anxiety, breathe diaphragmatically and relax.
- Reframe thoughts by accepting the physiological processes of menstruation or menopause, and refocus the mind on positive thoughts, and breathing rhythmically.
- Change one’s lifestyle and allow personal schedules to flow in better balance with individual, dynamic energy levels.
 Figure 3. Physiological Recordings of a Participant with PMS. This subject learned effortless diaphragmatic breathing by the fifth session and experienced a significant decrease in symptoms.
Figure 3. Physiological Recordings of a Participant with PMS. This subject learned effortless diaphragmatic breathing by the fifth session and experienced a significant decrease in symptoms.
Generalizing skills and interrupting the pattern
The limits of self-regulation are unknown, often held back only by the practitioner’s and participant’s beliefs. Biofeedback is a powerful self-regulation tool for individuals to observe and modify their covert physiological reactions. Other skills that augment diaphragmatic breathing are Quieting Reflex (Stroebel, 1982), Autogenic Training (Schultz & Luthe, 1969), and mindfulness training (Kabat-Zinn, 1990). In all skill learning, generalization is a fundamental factor underlying successful training. Integrating the learned psychophysiological skills into daily life can significantly improve health—especially in anticipation of and response to stress. The anticipated stress can be a physical, cognitive or social trigger, or merely the felt onset of a symptom.
As the person learns and applies effortless breathing to daily activities, she becomes more aware of factors that affect her breathing. She also experiences an increased sense of control: She can now take action (a slow effortless breath) in moments when she previously felt powerless. The biofeedback-mastered skill interrupts the evoked frustrations and irritations associated with an embarrassing history of hot flashes or mood swings. Instead of continuing with the automatic self-talk, such as “Damn, I am getting hot, why doesn’t it just stop?” (language fueling sympathetic arousal), she can take a relaxing breath in response to the internal sensations, stop the escalating negative self-talk and allows more acceptance—a process reducing sympathetic arousal.
In summary, effortless breathing appears to be a non-invasive behavioral strategy to reduce hot flashes and PMS symptoms. Practicing effortless diaphragmatic breathing contributes to a sense of control, supports a healthier homeostasis, reduces symptoms, and avoids the negative drug side effects. We strongly recommend that effortless diaphragmatic breathing be taught as the first step to reduce hot flashes and PMS symptoms.
I feel so much cooler. I can’t believe that my hand temperature went up. I actually feel calmer and can’t even feel the threat of a hot flash. Maybe this breathing does work! –Menopausal patient after initial training in diaphragmatic breathing
References
Bier, M., Kazarian, D., Peper, E., & Gibney, K. (2003). Reducing the severity of PMS symptoms with diaphragmatic breathing, autogenic training and biofeedback. Unpublished report.
Freedman, R.R., & Woodward, S. (1992). Behavioral treatment of menopausal hot flushes: Evaluation by ambulatory monitoring. American Journal of Obstetrics and Gynecology, 167 (2), 436-439.
Freedman, R.R., Woodward, S., Brown, B., Javaid, J.I., & Pandey, G.N. (1995). Biochemical and thermoregulatory effects of behavioral treatment for menopausal hot flashes. Menopause: The Journal of the North American Menopause Society, 2 (4), 211-218.
Frobish,C., Peper, E. & Gibney, K. H. (2003). Menopausal Hot Flashes: A Self-Regulation Case Study. Poster presentation at the 35th Annual Meeting of the Association for Applied Psychophysiology and Biofeedback. Abstract in: Applied Psychophysiology and Biofeedback. 29 (4), 302.
Goodale, I.L., Domar, A.D., & Benson, H. (1990). Alleviation of Premenstrual Syndrome symptoms with the relaxation response. Obstetrics and Gynecological Journal, 75 (5), 649-55.
Hays, J., Ockene, J.K., Brunner, R.L., Kotchen, J.M., Manson, J.E., Patterson, R.E., Aragaki, A.K., Shumaker, S.A., Brzyski, R.G., LaCroix, A.Z., Granek, I.A, & Valanis, B.G., Women’s Health Initiative Investigators. (2003). Effects of estrogen plus progestin on health-related quality of life. New England Journal of Medicine, 348, 1839-1854.
Humphries, K.H.., & Gill, s. (2003). Risks and benefits of hormone replacement therapy: the evidence speaks. Canadian Medical Association Journal, 168(8), 1001-10.
Kabat-Zinn, J. (1990). Full catastrophe living. New York: Delacorte Press.
Luthe, W. & Schultz, J.H. (1969). Autogenic therapy: Vol II: Medical applications. New York: Grune & Stratton.
Mathew, R.J.; Claghorn, J.L.; Largen, J.W.; & Dobbins, K. (1979). Skin Temperature control for premenstrual tension syndrome:A pilot study. American Journal of Clinical Biofeedback, 2 (1), 7-10.
Peper, E. (1990). Breathing for health. Montreal: Thought Technology Ltd.
Schultz, J.H., & Luthe, W. (1969). Autogenic therapy: Vol 1. Autogenic methods. New York: Grune and Stratton.
Schwartz, M.S. & Andrasik, F.(2003). Biofeedback: A practitioner’s guide, 3nd edition. New York: Guilford Press.
Shumaker, S.A., Legault, C., Thal, L., Wallace, R.B., Ockene, J., Hendrix, S., Jones III, B., Assaf, A.R., Jackson, R. D., Morley Kotchen, J., Wassertheil-Smoller, S.; & Wactawski-Wende, J. (2003). Estrogen plus progestin and the incidence of dementia and mild cognitive impairment in post menopausal women: The Women’s Health Initiative memory study: A randomized controlled trial. Journal of the American Medical Association, 289 (20), 2651-2662.
Stearns, V., Beebe, K. L., Iyengar, M., & Dube, E. (2003). Paroxetine controlled release in the treatment of menopausal hot flashes. Journal of the American Medical Association, 289 (21), 2827-2834.
Stroebel, C. F. (1982). QR, the quieting reflex. New York: G. P. Putnam’s Sons.
van Dixhoorn, J.J. (1998). Ontspanningsinstructie Principes en Oefeningen (Respiration instructions: Principles and exercises). Maarssen, Netherlands: Elsevier/Bunge.
Wassertheil-Smoller, S., Hendrix, S., Limacher, M., Heiss, G., Kooperberg, C., Baird, A., Kotchen, T., Curb, Dv., Black, H., Rossouw, J.E., Aragaki, A., Safford, M., Stein, E., Laowattana, S., & Mysiw, W.J. (2003). Effect of estrogen plus progestin on stroke in postmenopausal women: The Women’s Health Initiative: A randomized trial. Journal of the American Medical Association, 289 (20), 2673-2684.
Wyeth Pharmaceuticals (2003, June 4). A message from Wyeth: Recent reports on hormone therapy and where we stand today. San Francisco Chronicle, A11.
*We thank Candy Frobish, Mary Bier and Dalainya Kazarian for their helpful contributions to this research.
**For communications contact: Erik Peper, Ph.D., Institute for Holistic Healing Studies, San Francisco State University, 1600 Holloway Avenue, San Francisco, CA 94132; Tel: (415) 338 7683; Email: epeper@sfsu.edu; website: http://www.biofeedbackhealth.org; blog: http://www.peperperspective.come
Great resource: Dr. Mike Evans-The Single Most Important Thing You Can Do for Your Stress
Posted: February 6, 2014 Filed under: self-healing, stress management, Uncategorized | Tags: anxiety, exercise, healing, hypertension, mind-body, stress management 1 CommentA major factor that contributes to illness and health is how we cope with stress. Learning stress management techniques and integrating them into our daily life can significantly reduce illness and discomfort. Patients report significant improvement in numerous disorders such as hypertension, headaches, cancer, pain, or arthritis.
A great health resource are the short YouTube videos by Dr. Mike Evans who is founder of the Health Design Lab at the Li Ka Shing Knowledge Institute, an Associate Professor of Family Medicine and Public Health at the University of Toronto, and a staff physician at St. Michael’s Hospital. His informative short video clips cover a range of medical conditions from concussions to stopping smoking (see his website: http://www.myfavouritemedicine.com).
Watch the following video presentation on The Single Most Important Thing You Can Do for Your Stress.
There is Hope! Interrupt Chained Behavior
Posted: December 28, 2013 Filed under: self-healing, stress management, Uncategorized | Tags: biofeedback, biofeedback breathing, posture, psoriasis, self-talk, stress management 4 Comments“I was able to self-heal myself. I didn’t need anyone else to do it for me.”
“I was surprised that I actually succeeded and had some really great results.”
“How much control I really had over being able to change several of my habits, when I previously thought that it was impossible.”
“That I actually have control.”
Students who have practiced stress management at SFSU
This blog summarizes our recent published article that describes a teaching healing approach that can be used by many clients to mobilize their health. The process is illustrated by a case report student who had suffered from psoriasis for more than five years totally cleared his skin in six weeks and has continued to this benefit (Klein & Peper, 2013). At the recent one year follow-up his skin is still clear.
Low energy, being tired and depressed, having pain, insomnia, itching skin, psoriasis, nervously pulling out hair, hypertension and other are symptoms that affects our lives. In many cases there is no identifiable biological cause. Currently, 74% of patients who visit their health care providers have undiagnosed medical conditions. Most of the symptoms are a culmination of stress, anxiety, and depression. In many cases, health care professionals treat these patients ineffectively with medications instead of offering stress management options. For example, if patients with insomnia visits their physicians, they are most likely prescribed a sleep inducing medication (hypnotics). Patients who take sleeping medication nightly have a fourfold increase in mortality (Kripke et al., 2012). If on the other hand if the healthcare professional takes time to talk to the patient and explores the factors that contribute to the insomnia and teach sleep hygiene methods, 50s% fewer prescriptions are written. Obviously, you may not be able to sleep if you are worried about money, job security, struggles with your partner or problems with your children; however, medication do not solve these problems. Learning problem solving and stress management techniques often does!
When students begin to learn these stress management and self-healing skills as part of a semester long Holistic Health Class at San Francisco State University, 82% reported improvement in achieving benefits such as increasing physical fitness, healthier diets, reducing depression, anxiety, pain and eliminating eczema or reducing hair pulling (one student with Trichotillomania reduced her hair pulling from 855 to 19 minutes per week) (Peper et al., 2003; Bier et al., 2005; Ratkovich et al., 2012). The major factors that contributed to the students’ improvement are:
- Daily monitoring of subjective and objective experiences to facilitates awareness and identify cues that trigger or aggravate the symptoms.
- Ongoing practicing during the day and during activities of the stress management skills as adapted from the book, Make Health Happen (Peper et al, 2003)
- Sharing subjective experiences in small groups which reduces social isolation, normalizes experiences, and encourages hope. Usually, a few students will report rapid benefits such as aborting a headache, falling asleep rapidly, or reducing menstrual cramps, which helps motivate other students to continue their practices.
- Writing an integrative summary paper, which provides a structure to see how emotions, daily practices and change in symptoms are related.
The first step is usually Identifying the trigger that initiates the illness producing patterns. Once identified, the next step is to interrupt the pattern and do something different. This can include transforming internal dialogue, practicing relaxation or modifying body posture. The mental/emotional and physical practices interrupts and diverts the cascading steps that develop the symptoms (Peper et al., 2003).
Interrupting and transforming the chained behavior is illustrated in our article “There Is Hope: Autogenic Biofeedback Training for the Treatment of Psoriasis” published in the recent issue of Biofeedback. We report on the process by which a 23-year-student totally cleared his skin after having had psoriasis for the last five years. Psoriasis causes red, flaky skin and is currently the most common autoimmune disease affecting approximately 2% of the US population. Many people afflicted with this disease use steroids, topical creams, special shampoos, and prescription medication. Unfortunately, the disease can only be suppressed, not cured. Thus many people with psoriasis feel damaged and have a difficult time socially. Stress is often one of the triggers that makes psoriasis worse. In this case study, the 23-year-old student learned how to train his mind/body to transform his feelings of stress, anxiety, self-doubt, and urge to scratch his skin into a positive self-healing process.
Initially, the student was trained in stress management and biofeedback techniques that included relaxation, stress reduction, and desensitization. He learned how to increase his confidence by changing his body posture while sitting and standing. He also took time to stop and refocus his energy when he felt the need to fall back into old habits. What did he really do?
The moment he became aware of skin sensations, he would:
- Stop, take a deep breath into his abdomen and slowly exhale
- Assess how he was thinking-having negative and hopeless thoughts
- Change the negative thoughts into positive affirmative thoughts
- Breathe deeply
- Imagine as he exhaled feeling heaviness and warmth in his arms and feet
- Talk to his body by saying, “My skin is cool, clear, and regenerative.” “I am worthy.”
To become aware of his automatic negative behavior was very challenging. He had to stop focusing on the task in front of him and to put all of his energy into regaining his composure. This is very difficult because people are normally captured by whatever they are doing at that moment. As he stated: “Breaking this chain behavior was by far the hardest things I’ve ever done. It didn’t matter what situation I found myself in, my practice took precedence. The level of self- control I had to maintain was far beyond my norm. I remember taking an exam. I was struggling to recall the answer to the last essay question. All I wanted to do was finish the exam and go home. I knew that I knew it, it was coming to me, I began to write… Yet in that same moment I felt my right elbow start to tingle (the location of one of the psoriasis plagues) and my left hand started to drift towards it. Immediately I had to switch my focus. Despite my desire to finish I dropped my pen. I paused to breathe and focused upon my positive thoughts. Moments like this happened daily, my normal functions were routinely interrupted by urges to scratch. Sometimes I would spend significantly more time doing the practices than the task at hand.
Similarly, whenever he observed his body posture “collapsing” and “hiding” — thus falling into a more powerless posture — he would interrupt the collapse and shift to a power position by expanding and being more erect. He did this while standing, sitting, and talking to other students. As he stated: “I hadn’t realized how my collapsing posture was effecting my self-image until I began practicing a more powerful posture. In class I made myself sit with my butt pushed back against the back of the chair instead of letting myself slide forwarding into a slouch. Just like the urge to itch I had to stay conscious of my posture constantly. At work, at school, even at home on the couch I practiced expanding body posture. The more I was aware of my posture the better my posture became, and the more time I spent in power pose the more natural it began to feel. The more natural it felt the more powerful I felt.”
After three weeks, his skin had cleared and has continued to stay this way for the last year as shown in Figure 1.
 Figure 1. Pre and post photos of the elbow and knee showing the improvement of the skin.
Figure 1. Pre and post photos of the elbow and knee showing the improvement of the skin.
There are many diseases and ailments that require the use of medication for appropriate treatment, but when stress is a factor in any diagnosis, or when a diagnosis cannot be found, it is important for stress management to be offered as a viable option for patients to consider. As shown by the student with psoriasis, learning stress management skills and then actually practicing them during the day can play a major factor in improving the health of an individual. The same process is applicable for numerous symptoms. There is hope=-Just do it.
References:
Bier, M., Peper, E., & Burke, A. (2005). Integrated stress management with ‘Make Health Happen: Measuring the impact through a 5-month follow-up. Presented at the 36th Annual Meeting of the Association for Applied Psychophysiology and Biofeedback. Abstract published in: Applied Psychophysiology and Biofeedback, 30(4), 400. http://biofeedbackhealth.files.wordpress.com/2013/12/2005-aapb-make-health-happen-bier-peper-burke-gibney3-12-05-rev.pdf
Klein, A. & Peper, W. (2013). There is Hope: Autogenic Biofeedback Training for the Treatment of Psoriasis. Biofeedback, 41(4), 194–201. http://biofeedbackhealth.files.wordpress.com/2011/01/published-article-there-is-hope.pdf
Kripke, D.F., Langer, R.D., Kline. L.E. (2012). Hypnotics’association with mortality or cancer: a matched cohort study. BMJOpen, 2:e000850. doi:10.1136/bmjopen-2012-000850 http://bmjopen.bmj.com/content/2/1/e000850.full.pdf+html
Peper, E., Gibney, K.H. & Holt. C. (2002). Make Health Happen: Training Yourself to Create Wellness. Dubuque, IA: Kendall-Hunt. http://www.amazon.com/Make-Health-Happen-Training-Yourself/dp/0787293318
Peper, E., Sato-Perry, K & Gibney, K. H. (2003). Achieving health: A 14-session structured stress management program—Eczema as a case illustration. 34rd Annual Meeting of the Association for Applied Psychophysiology and Biofeedback. Abstract in: Applied Psychophysiology and Biofeedback, 28(4), 308. http://biofeedbackhealth.files.wordpress.com/2013/12/2003-aapb-poster-peper-keiko-long1.pdf
Ratkovich, A., Fletcher, L., Peper, E., & Harvey, R. (2012). Improving College Students’ Health-Including Stopping Smoking and Healing Eczema. Presented at the 43st Annual Meeting of the Association for Applied Psychophysiology and Biofeedback. Baltimore, MD. http://biofeedbackhealth.files.wordpress.com/2011/01/2012-improving-college-student-health-2012-02-28.pdf
From Wisdom to Alzheimer’s: Are we poisoning ourselves with affluent malnutrition and sedentary life style?
Posted: December 14, 2013 Filed under: Exercise/movement, Nutrition/diet, self-healing, Uncategorized | Tags: Alzheimer, diet, evolution, exercise, health 1 CommentWise elders, grand parents or statesmen have been the traditional roles for aging adults. Older people were revered as the repository and sources of wisdom in many traditional cultures. Presently the development of aging into wisdom is being overshadowed by the specter of Alzheimer’s disease. Wisdom transforming into Alzheimer’s disease does not compute. How come that in slightly more than a century after it was first described by the neuropathologist Alois Alzheimer in 1906, the fear of contracting and possible having Alzheimer’s disease with the concurrent loss of cognitive and body functions is becoming a possibility? How could this have occurred?
Today more people are living to older ages; however, in traditional cultures some people also lived to very old age (the major increase in present day longevity is due to the elimination of infant and maternal mortality and medical treatment to survive trauma).
Is it possible that the prevention of Alzheimer’s will not be found in pharmaceutical treatment but in promoting organic food diet and movement? The research data is starting to find that our life style patterns are risk factors for Alzheimer’s. Changing lifestyle factors is a more promising treatment approach than drugs. A significant risk factor may be the confluence of a sedentary lifestyle and affluent malnutrition. Researchers are even reporting that the built up of the beta amyloid plaques in brains of people with Alzheimer’s disease is not the result of aging but the body’s attempt to cope with the influx of environmental and dietary poisons or decreases in essential foods or body activities.
Risk: Sedentary lifestyle-Too little exercise
Over the last hundred years–and rapidly accelerated in the last 30 years–we have transformed work into sitting. By sitting in front of a computer screen, we have created a new disease: Immobilization Syndrome. Lack of exercise is recognize as a major factor in numerous illnesses such as cardiovascular disease, obesity, and diabetes. Movement in many different forms reduces the risk of illness. Older people who exercise have a significant reduction in the risk of developing Alzheimer’s (Larson, 2006; Radak et al, 2010).
Regular movement lowers the risk. Even though there is overwhelming scientific evidence that movement and exercise are required for health, there is a disconnect with the medical and educational practices. Insurances will pay for medical treatment; however, they usually will not pay for prevention or exercise. At the same time physical education in schools is reduced or eliminated to reduce the risk of litigation (an injured child on the playground could sue the school). Children now spend most of their time in front of a screen while exercising their thumb and index fingers instead of playing and moving outdoors.
Risk: Affluent malnutrition-too much sugar and simple carbohydrates
Affluent malnutrition appears to be another risk factor. Recent findings suggests that the beta amyloids plagues, as the marker for Alzheimer’s in the brain, may be a protective response to the modulating insulin levels triggered by affluent malnutrition and sedentary life style. This disease has been labeled as type 3 diabetes by Associate Professor Suzanne de la Monte at Brown University (Steen et al, 2005). Namely, the disease occurs as the brain tissue becomes resistant to insulin.
Rats that are fed high-fructose corn syrup laced water experienced learning and memory problems in less than 6 weeks and became less responsive to insulin. At the same time if the animals were given omega 3 fatty acids, they appear to escape the cognitive decline. In other research rats developed Alzheimer like brain changes and became demented when Suzanne de la Monte interfered with how the rats brains respond to insulin (Trivedi, 2012).
Alois Alzheimer first described these abnormal protein structure in the brains a little more than a hundred years ago. At that time the European diet had increased sugar intake as shown in figure 1. While more recently there has been a significant increase in high fructose corn syrup as shown in figure 2.

Figure 1. Radical increase in sugar consumption in the last 200 years. From: http://blog.zestos.co.nz/2010/09/sugar-consumption-been-high-before.html

Figure 2. Increase in the type of sugar consumption in the last thirty years. From: http://blog.zestos.co.nz/2010/09/sugar-consumption-been-high-before.html
We are now becoming concerned with the Alzheimer’s disease as an upcoming epidemic. It cannot be just sugar; since, its consumption has been high since the beginning of the 20th century. A possible contributor could be the high-fructose corn syrup; however, it is most likely the interaction between reduced exercise and sugar.
Sugar set the stage for pathogenesis to occur in the brain and the absence of movement/exercise promotes and supports the pathogenesis. People continue to decrease movement: from walking or riding horses to sitting cars or standing on escalators and elevators; from doing physical housework to automated washing machines, driers and dishwashers; from preparing foods from raw materials to prepackaged foods; from filing and typing to computer work; from playing family games to watching TV and searching the net; from face to face communication to texting; etc.
We have separated from our biological evolutionary heritage. I am not surprised that Alzheimer’s disease and immobility and sugar are linked. Adopt the precautionary principle and assume that sugar and high-fructose corn syrup in conjunction with reduced movement (immobilization syndrome) is harmful.
As a reader, you will probably have to wait another 20 years before these findings have been scientifically proven against the overt and covert lobbying efforts of agribusiness and pharmaceutical industry. Remember it took 30 years to demonstrate that smoking was harmful. Begin to move and eat in concert with your evolutionary background (See Part III Self-care in Gorter and Peper, 2011).
Begin now!
Eat food not sugars! Eat the foods great grandparents would recognize as food as Michael Pollan (2009) describe in his superb book, In Defense of Food: An Eater’s Manifesto. Eat foods that have not been processed or adulterated by additives. Take charge by eating brain supporting foods such as organic vegetables, roots, fruits, nuts, fish, some organ meat, and eliminate all those sugary, fatty processed highly advertised fast foods.
Move and exercise! Get up and move every hour. Walk up the stairs instead of the escalator. Meet new people and move by going hiking, dancing, Tai Chi or yoga classes or volunteer by helping others.
References
Gorter, R. & Peper, E. (2011). Fighting Cancer-A Non Toxic Approach to Treatment. Berkeley: North Atlantic.
Larson, E.G., Wang, L., Bowen, J.D., McCormick, W. C., Teri, L., Crane, P., & Kukull, W. (2006). Exercise Is Associated with Reduced Risk for Incident Dementia among Persons 65 Years of Age and Older. Ann Intern Med, 144(2), 73-81.
Pollan, M. (2009). In Defense of Food: An Eater’s Manifesto. New York: Penguin Books.
Radak, Z., Hart. N., Sarga, L., Koltai, E., Atalay, M., Ohno, H., & Boldogh, I. (2010). Journal of Alzheimer’s Disease, 20(3), 777-83.
Steen, E., Terry, B.M. Rivera, E.J., Cannon, J.L., Neely, T.R., Tavares, R., Xu, X. J., Wands, J.R., & de al Monte, S. M. (2005). Impaired insulin and insulin-like growth factor expression and signaling mechanisms in Alzheimer’s disease-is this type 3 diabetes? Journal of Alzheimer’s Disease, 7(1), 53-80.
Trivedi, B. (2012). Eat your way to dementia. New Scientist, 215(2880), 32-37.
Simple Ways to Manage Stress- An experiential lecture for people impacted by the March 11, 2011 Great East Japan Earthquake
Posted: November 8, 2013 Filed under: self-healing, stress management, Uncategorized | Tags: anxiety, depression, earthquake, exercise, insomnia, neck pain, stress, stress management, tsunami 6 CommentsStress can be reduced by simple pragmatic exercises. This 99 minute participatory lecture was presented in Sendei, Japan, on July 20, 2013 to people who were impacted by the 2011 Tohoku earthquake and tsunami disaster.* The lecture includes practices that demonstrate 1) how thoughts, emotions and images affect the body, 2) how simple movements can reduce muscle tension, 3) how breathing can be used to reduce stress, 4) how changing posture can change access to positive or negative memories, 5) how acceptance is the beginning step for healing. This approach based upon a holistic evolutionary perspective of stress and health can be used to reduce symptoms caused or increased by stress such as neck, shoulder and back tension, digestive problems, worrying and insomnia. The video lecture is sequentially translated from English to Japanese. Click on the link to watch the video lecture.
http://cat-vnet.tv/movie/medical_health/suimin_02/001_02.html

*The program was organized by Toshihiko Sato, Ph.D., Dept. Health and Social Services, Faculty of Medical Sciences and Welfare Tohoku Bunka Gakuen University, Sendai.
Epilepsy: New (old) treatment without drugs
Posted: March 10, 2013 Filed under: Nutrition/diet, self-healing, Uncategorized | Tags: biofeedback, diet, ketogenic diet, neurofeedback 11 CommentsNothing is so hard as watching a child having a seizure.
–Elizabeth A. Thiele, MD, PhD, professor of neurology at Harvard Medical School
Until recently, when people asked me, “What would I suggest as a non-toxic/non-invasive biofeedback approach for the treatment of epilepsy?” I automatically replied, “A combination of neurofeedback, behavioral analysis treatment, respiration training, a low glycemic diet, and stress management and if these did not work, medications.” I have now changed my mind!
Epilepsy is diagnosed if the person has two or more seizures. About one to two percent of the population is diagnosed with epilepsy and it is the most common neurological illness in children. Medication is usually the initial treatment intervention; however, in about one third of the people, the seizures will still occur despite the medications. In some cases, people -often without the support of their neurologist/healthcare provider–will explore other treatment strategies such as diet, respiration training, neurofeedback, behavioral control, diet, or traditional Chinese medicine.
It is ironic that one of the tools to diagnose epilepsy is recording the electroencephalography (EEG)– brain waves–of the person after fasting while breathing quickly (hyperventilating). For some, the combination of low blood sugar and hyperventilation will evoke epileptic wave forms in their EEG and can trigger seizures (hyperventilation when paired with low sugar levels tends to increase slow wave EEG which would promote seizure activity).
If hyperventilation and fluctuating blood sugar levels are contributing factors in triggering seizures, why not teach breathing control and diet control as the first non-toxic clinical intervention before medications are prescribed. This breathing approach has shown very promising clinical success. (For more details see the book, Fried, R. (1987). The Hyperventilation syndrome-Research and Clinical Treatment. Baltimore: The Johns Hopkins University Press).
Self-management should be the first clinical intervention and not the last. Similarly, neurofeedback– brain wave biofeedback–is another proven approach to reduce seizures. This approach was developed by Professor Maurice B. Sterman at UCLA and was based upon animal studies. He demonstrated that cats who were trained to increase sensory motor rhythm (SMR) in their EEG could postpone seizure onset when exposed to a neurotoxin that induced seizures. He then demonstrated that human beings with epilepsy could equally learn to control their EEG patterns and inhibit seizures. This approach, just as the breathing approach, is non-toxic and reduces seizures.
Underlying both these approaches is the concept of behavioral analysis to identify and interrupt the chained behavior that leads to a seizure. Namely, a stimulus (internal or external) triggers a cascading chain of neurological processes that eventually results in a seizure. Thus, if the person learns to identify and interrupt/divert this cascading chain, the seizure does not occur. From this perspective, respiration training and neurofeedback could be interpreted to interrupt this cascading process. Behavioral analyses includes all behaviors (movement, facial expressions, emotions, etc) which can be identified and then interrupted. As professors Joanne Dahl and Tobias Lundgren from Uppsala University in Sweden state, The behavior technology of seizure control provides low-cost, drug free treatment alternative for individual already suffering from seizures and the stigmatization of epilepsy.
Until recently, I would automatically suggest that people explore these self-control strategies as the first intervention in treatment of epilepsy and only medication for the last resort. Now, I have changed my mind. I suggest the ketogenic diet as the first step for the treatment of epilepsy in conjunction with the self-regulation strategies—medication should only be used if the previous strategies were unsuccessful.
A ketogenic diet has a 90% clinical success rates in children–even in patients with refractory seizures. This diet stabilizes blood sugar levels and is very low on simple carbohydrates, high in fat, some protein, and lots of vegetables (a ratio of 4 grams of fat to 1 gram of carbohydrates and protein). In adults, the success rates drops to about 50%. The lower success rate may be the result of the challenges in implementing these self-regulatory diet approaches. As Elizabeth A. Thiele, MD, PhD, professor of neurology at Harvard Medical School points out, dietary therapy is the most effective known treatment strategy for epilepsy. Even though, ketogenic diet is the most effective therapy, it is less likely to be prescribed than medications—there are no financial incentives; there are, however, many financial incentives for prescribing pharmaceuticals.
These lifestyle changes are very challenging to implement. They need to be taught and socially supported. Just telling people what to do does not often work. It is similar to learning to play a musical instrument. The person needs step by step coaching and social support which is an intensive educational approach. To learn more about the research underlying the ketogenic diet as the first level of intervention for epilepsy, watch Professor Thiele’s presentation from the 2012 Ancentral Health Symposium, Dietary Therapy: Role in Epilepsy and Beyond.
There is hope for neurological recovery: Redirect behaviors of habit
Posted: February 23, 2013 Filed under: self-healing, Uncategorized | Tags: behavior analysis, Cerebral palsy, epilepsy, habit, neurofeedback, rehabilitation, stroke Leave a commentAlthough many neurological disorders appear to be structural and the result of neurological dysfunctioning, recent research suggests that there is much more hope that people can learn to restore function. Even people affected by stroke, cerebral palsy, or epilepsy can regain function. The observed symptoms and dysfunctional movement patterns can be understood as the nervous system’s best strategy to solve a problem at that moment and is the best response the person could perform under the circumstances. For example in the case of stroke, a spastic movement is the best solution that becomes a conditioned habit pattern. It may occur because the person tries to achieve the previous motor behaviors which can no longer be performed because of the neurological damage. With cerebral palsy, the initial damage at birth changed the motor patterns as the child attempted to walk. While in cases of epilepsy, the spreading of the seizure across the brain is not inhibited. Despite the neurological damage, improvement is possible as demonstrated by Jill Bolte Taylor’s presentation of her experience and remarkable recovery from a left hemisphere stroke.
Application to stroke rehabilitation
A useful premise underlying neural regeneration and development is that it healing follows developmental movement sequences which cannot be skipped. Thus after a neurological injury such as a stroke, the movement sequence needs to be re-integrated. It is not relearning what was lost; it is learning the new skills as if the skills are being learned for the first time. This includes an attitude of acceptance, non judgment, fun, play and exploration concurrent with many, many, many training practices until the skills are mastered. Thus stroke patients sitting in wheelchairs may try to repeat movements which were present before the stroke but which are now beyond the biological developmental stage due to the neural damage. The person instead needs to learn anew the movement sequences that a baby mastered (lifting the head, rolling over, cross crawl moment, crawling, etc). This takes lots of practice. Compare the many hours a baby/child practices in order to be able to stand to the limited time people with strokemay spent performing their prescriptive exercises. Thus, children usually show mastery while many people with stroke demonstrate limited improvement. It is practice, practice and practice; it is not mindless practice, it is practice with awareness and intent.
Dysfunctional patterns can be understood as over learned conditioned chained behaviors which occur automatically. A superb explanation of this process is described by Charles Duhigg in his book, The power of habit-Why we do what we do in life and business. Clinical success is to identify these chains and the sequential steps and then teach the person to redirect the behavior.
Application to epilepsy
Some people with epilepsy can learn to identify the initiation of the seizure and then interrupt the cascading sequence by doing something different. In this way the seizure process is interrupted and no seizure will occur. For example, one man hyperventilated before a grand mal seizure. When the therapist taught him to become aware and change his breathing pattern each he began to hyperventilate, his epileptic seizures did not occur. Similarly, a young woman with epilepsy turned her head to the right and slightly lifted her chin upward just before an absence seizure occurred. Teaching her to interrupt her initial head movement and looking straight ahead while slowly exhaling inhibited her seizures. The efficacy of this type of behavioral analysis for the treatment of epilepsy has been described by psychologists, Joanne Dahl, PhD and Tobias Lundgren, PhD in their superb article, Behavior analysis of epilepsy: Conditioning mechanisms, behavior technology and the contribution of ACT.
Another powerful treatment approach to treat seizures was developed by M. B. Sterman, Ph.D. at UCLA who taught people with epilepsy to control their own electrical activity of their brain with neurofeedback. Many people benefited from neurofeedback training and significantly reduced their seizures.
Application to cerebral palsy
To appreciate the power of interrupting the chained behaviors and the possibility that there is hope for people with cerebral palsy. This is illustrated in the remarkable TEDx Winnepeg talk, Baby brains DO recover, but habit hides it, by Karen Pape, MD.
