Yes, fresh organic food is better!
Posted: October 27, 2017 Filed under: Nutrition/diet, self-healing | Tags: farming, Holistic health, longevity, non-organic foods, nutrition, organic foods, pesticides 16 Comments
Is it really worthwhile to spent more money on locally grown organic fruits and vegetables than non-organic fruits and vegetables? The answer is a resounding “YES!” Organic grown foods have significantly more vitamins, antioxidants and secondary metabolites such as phenolic compounds than non-organic foods. These compounds provide protective health benefits and lower the risk of cancer, cardiovascular disease, type two diabetes, hypertension and many other chronic health conditions (Romagnolo & Selmin, 2017; Wilson et al., 2017; Oliveira et al., 2013; Surh & Na, 2008). We are what we eat–we can pay for it now and optimize our health or pay more later when our health has been compromised.
The three reasons why fresh organic food is better are:
- Fresh foods lengthen lifespan.
- Organic foods have more vitamins, minerals, antioxidants and secondary metabolites than non-organic foods.
- Organic foods reduce exposure to harmful neurotoxic and carcinogenic pesticide and herbicides residues.
Background
With the advent of chemical fertilizers farmers increased crop yields while the abundant food became less nutritious. The synthetic fertilizers do not add back all the necessary minerals and other nutrients that the plants extract from the soil while growing. Modern chemical fertilizers only replace three components–Nitrogen, Phosphorus and Potassium–of the hundred of components necessary for nutritious food. Nitrogen (N) which promotes leaf growth; Phosphorus (P which development of roots, flowers, seeds, fruit; and Potassium (K) which promotes strong stem growth, movement of water in plants, promotion of flowering and fruiting. These are great to make the larger and more abundant fruits and vegetables; however, the soil is more and more depleted of the other micro-nutrients and minerals that are necessary for the plants to produce vitamins and anti-oxidants. Our industrial farming is raping the soils for quick growth and profit while reducing the soil fertility for future generations. Organic farms have much better soils and more soil microbial activity than non-organic farm soils which have been poisoned by pesticides, herbicides, insecticides and chemical fertilizers (Mader, 2002; Gomiero et al, 2011). For a superb review of Sustainable Vs. Conventional Agriculture see the web article: https://you.stonybrook.edu/environment/sustainable-vs-conventional-agriculture/
1. Fresh young foods lengthen lifespan. Old foods may be less nutritious than young food. Recent experiments with yeast, flies and mice discovered that when these organisms were fed old versus young food (e.g., mice were diets containing the skeletal muscle of old or young deer), the organisms’ lifespan was shortened by 18% for yeast, 13% for flies, and 13% for mice (Lee et al., 2017). Organic foods such as potatoes, bananas and raisins improves fertility, enhances survival during starvation and decreases long term mortality for fruit flies(Chhabra et al, 2013). See Live longer, enhance fertility and increase stress resistance: Eat organic foods. https://peperperspective.com/2013/04/21/live-longer-enhance-fertility-and-increase-stress-resistance-eat-organic-foods/
In addition, eating lots of fruits and vegetables decreases our risk of dying from cancer and heart disease. In a superb meta-analysis of 95 studies, Dr. Dagfinn Aune from the School of Public Health, Imperial College London, found that people who ate ten portions of fruits and vegetable per day were a third less likely to die than those who ate none (Aune et al, 2017). Thus, eat lots of fresh and organic fruits and vegetables from local sources that is not aged because of transport.
2. Organic foods have more vitamins, minerals, antioxidants and secondary metabolites than non-organic foods. Numerous studies have found that fresh organic fruits and vegetables have more vitamins, minerals, antioxidants, and secondary metabolites than non-organic ones. For example, organic tomatoes contain 57 per cent more vitamin C than non-organic ones (Oliveira et al 2013) or organic milk has more beneficial polyunsaturated fats non-organic milk (Wills, 2017; Butler et al, 2011). Over the last 50 years key nutrients of fruits and vegetables have declined. In a survey of 43 crops of fruits and vegetables, Davis, Epp, & Riordan, (2004) found a significant decrease of vitamins and minerals in foods grown in the 1950s as compared to 1999 as shown in Figure 1 (Lambert, 2015).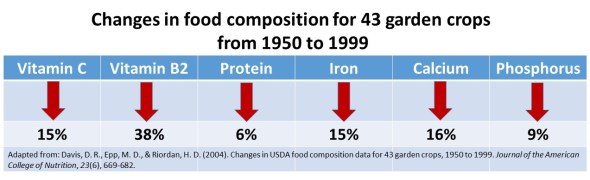
Figure 1. Change in vitamins and minerals from 1950 to 1999. From: Davis, D. R., Epp, M. D., & Riordan, H. D. (2004). Changes in USDA food composition data for 43 garden crops, 1950 to 1999. Journal of the American College of Nutrition, 23(6), 669-682.
3, Organic foods reduce exposure to harmful neurotoxic and carcinogenic pesticide and herbicides residues. Even though, the United States Department of Agriculture (USDA) and the United States Environmental Protection Agency (EPA) state that pesticide residues left in or on food are safe and non-toxic and have no health consequences, I have my doubts! Human beings accumulate pesticides just like tuna fish accumulates mercury—frequent ingesting of very low levels of pesticide and herbicide residue may result in long term harmful effects and these long term risks have not been assessed. Most pesticides are toxic chemicals and were developed to kill agricultural pests — living organisms. Remember human beings are living organisms. The actual risk for chronic low level exposure is probably unknown; since, the EPA pesticide residue limits are the result of a political compromise between scientific findings and lobbying from agricultural and chemical industries (Portney, 1992). Organic diets expose consumers to fewer pesticides associated with human disease (Forman et al, 2012).
Adopt the precautionary principle which states, that if there is a suspected risk of herbicides/pesticides causing harm to the public, or to the environment, in the absence of scientific consensus, the burden of proof that it is not harmful falls on those recommending the use of these substances (Read & O’Riordan, 2017). Thus, eat fresh locally produced organic foods to optimize health.
References
Butler, G. Stergiadis, s., Seal, C., Eyre, M., & Leifert, C. (2011). Fat composition of organic and conventional retail milk in northeast England. Journal of Dairy Science. 94(1), 24-36.http://dx.doi.org/10.3168/jds.2010-3331
Davis, D. R., Epp, M. D., & Riordan, H. D. (2004). Changes in USDA food composition data for 43 garden crops, 1950 to 1999. Journal of the American College of Nutrition, 23(6), 669-682. http://www.chelationmedicalcenter.com/!_articles/Changes%20in%20USDA%20Food%20Composition%20Data%20for%2043%20Garden%20Crops%201950%20to%201999.pdf
Lambert, C. (2015). If Food really better from the farm gate than super market shelf? New Scientist.228(3043), 33-37.
Oliveira, A.B., Moura, C.F.H., Gomes-Filho, E., Marco, C.A., Urban, L., & Miranda, M.R.A. (2013). The Impact of Organic Farming on Quality of Tomatoes Is Associated to Increased Oxidative Stress during Fruit Development. PLoS ONE, 8(2): e56354. https://doi.org/10.1371/journal.pone.0056354
Read, R. and O’Riordan, T. (2017). The Precautionary Principle Under Fire. Environment-Science and policy for sustainable development. September-October. http://www.environmentmagazine.org/Archives/Back%20Issues/2017/September-October%202017/precautionary-principle-full.html
Romagnolo, D. F. & Selmin, O.L. (2017). Mediterranean Diet and Prevention of Chronic Diseases. Nutr Today. 2017 Sep;52(5):208-222. doi: 10.1097/NT.0000000000000228. https://www.ncbi.nlm.nih.gov/pubmed/29051674
Wills, A. (2017). There is evidence organic food is more nutritious. New Scientist,3114, p53.
Wilson, L.F., Antonsson, A., Green, A.C., Jordan, S.J., Kendall, B.J., Nagle, C.M., Neale, R.E., Olsen, C.M., Webb, P.M., & Whiteman, D.C. (2017). How many cancer cases and deaths are potentially preventable? Estimates for Australia in 2013. Int J Cancer. 2017 Oct 6. doi: 10.1002/ijc.31088. https://www.ncbi.nlm.nih.gov/pubmed/28983918
Healing irritable bowel syndrome with diaphragmatic breathing*
Posted: June 23, 2017 Filed under: Breathing/respiration, self-healing | Tags: abdominal pain, diaphragmatic breathing, food intolerances, health, Holistic health, IBS, irritable bowel syndrome, pain, recurrent abdominal pain, self-care, SIBO, stress, thoracic breathing 31 CommentsErik Peper, Lauren Mason and Cindy Huey
This blog was adapted and expanded from: Peper, E., Mason, L., & Huey, C. (2017). Healing irritable bowel syndrome with diaphragmatic breathing. Biofeedback. 45(4), 83-87. DOI: 10.5298/1081-5937-45.4.04 https://biofeedbackhealth.files.wordpress.com/2018/02/a-healing-ibs-published.pdf
After having constant abdominal pain, severe cramps, and losing 15 pounds from IBS, I found myself in the hospital bed where all the doctors could offer me was morphine to reduce the pain. I searched on my smart phone for other options. I saw that abdominal breathing could help. I put my hands on my stomach and tried to expand it while I inhaled. All that happened was that my chest expanded and my stomach did not move. I practiced and practiced and finally, I could breathe lower. Within a few hours, my pain was reduced. I continued breathing this way many times. Now, two years later, I no longer have IBS and have regained 20 pounds.
– 21-year old woman who previously had severe IBS
Irritable bowel syndrome(IBS) affects between 7% to 21% of the general population and is a chronic condition. The symptoms usually include abdominal cramping, discomfort or pain, bloating, loose or frequent stools and constipation and can significantly reduce the quality of life (Chey et al, 2015). A precursor of IBS in children is called recurrent abdominal pain (RAP) which affects between 0.3 to 19% of school children (Chitkara et al, 2005). Both IBS and RAP appear to be functional illnesses, as no organic causes have been identified to explain the symptoms. In the USA, this results in more than 3.1 physician visits and 5.9 million prescriptions written annually. The total direct and indirect cost of these services exceeds $20 billion (Chey et al, 2015). Multiple factors may contribute to IBS, such as genetics, food allergies, previous treatment with antibiotics, severity of infection, psychological status and stress. More recently, changes in the intestinal and colonic microbiome resulting in small intestine bacterial overgrowth are suggested as another risk factor (Dupont, 2014).
Generally, standard medical treatments (reassurance, dietary manipulation and of pharmacological therapy) are often ineffective in reducing abdominal IBS and other abdominal symptoms (Chey et al, 2015), while complementary and alternative approaches such as relaxation and cognitive therapy are more effective than traditional medical treatment (Vlieger et, 2008). More recently, heart rate variability training to enhance sympathetic/ parasympathetic balance appears to be a successful strategy to treat functional abdominal pain (FAB) in children (Sowder et al, 2010). Sympathetic/parasympathetic balance can be enhanced by increasing heart rate variability (HRV), which occurs when a person breathes at their resonant frequency which is usually between 5-7 breaths per minute. For most people, it means breathing much slower, as slow abdominal breathing appears to be a self-control strategy to reduce symptoms of IBS, RAP and FAP.
This article describes how a young woman healed herself from IBS with slow abdominal breathing without any therapeutic coaching, reviews how slower diaphragmatic breathing (abdominal breathing) may reduce symptoms of IBS, explores the possibility that breathing is more than increasing sympathetic/parasympathetic balance, and suggests some self-care strategies to reduce the symptoms of IBS.
Healing IBS-a case report
After being diagnosed with Irritable Bowel Syndrome her Junior year of high school, doctors told Cindy her condition was incurable and could only be managed at best, although she would have it throughout her entire life. With adverse symptoms including excessive weight loss and depression, Cindy underwent monthly hospital visits and countless tests, all which resulted in doctors informing her that her physical and psychological symptoms were due to her untreatable condition known as IBS, of which no one had ever been cured. When doctors offered her what they believed to be the best option: morphine, something Cindy describes now as a “band-aid,” she was left feeling discouraged. Hopeless and alone in her hospital bed, she decided to take matters into her own hands and began to pursue other options. From her cell phone, Cindy discovered something called “diaphragmatic breathing,” a technique which involved breathing through the stomach. This strategy could help to bring warmth to the abdominal region by increasing blood flow throughout abdomen, thereby relieving discomfort of the bowel. Although suspicious of the scientific support behind this method, previous attempts at traditional western treatment had provided no benefit to recovery; therefore, she found no harm in trying. Lying back flat against the hospital bed, she relaxed her body completely, and began to breathe. Immediately, Cindy became aware that she took her breath in her chest, rather than her stomach. Pushing out all of her air, she tried again, this time gasping with inhalation. Delighted, she watched as air flooded into her stomach, causing it to rise beneath her hands, while her chest remained still. Over time, Cindy began to develop more awareness and control over her newfound strategy. While practicing, she could feel her stomach and abdomen becoming warmer. Cindy shares that for the first time in years, she felt relief from pain, causing her to cry from happiness. Later that day, she was released from the hospital, after denying any more pain medication from doctors.
Cindy continues to practice her diaphragmatic breathing as much as she can, anywhere at all, at the sign of pain or discomfort, as well as preventatively prior to what she anticipates will be a stressful situation. Since beginning her practice, Cindy says that her IBS is pretty much non-existent now. She no longer feels depressed about her situation due to her developed ability to manage her condition. Overall, she is much happier. Moreover, since this time two years ago, Cindy has gained approximately 20 pounds, which she attributes to eating a lot more. In regard to her success, she believes it was her drive, motivation, and willingness to dedicate herself fully to the breathing practice which allowed for her to develop skills and prosper. Although it was not natural for her to breathe in her stomach at first, a trait which she says she often recognizes in others, Cindy explains it was due to necessity which caused her to shift her previously-ingrained way of breathing. Upon publicly sharing her story with others for the first time, Cindy reflects on her past, revealing that she experienced shame for a long time as she felt that she had a weird condition, related to abnormal functions, which no one ever talks about. On the experience of speaking out, she affirms that it was very empowering, and hopes to encourage others coping with a situation similar to hers that there is in fact hope for the future. Cindy continues to feel empowered, confident, and happy after taking control of her own body, and acknowledges that her condition is a part of her, something of which she is proud.
Watch the in-depth interview with Cindy Huey in which she describes her experience of discovering diaphragmatic breathing and how she used this to heal herself of IBS
Video 1. Interview with Cindy Huey describing how she healed herself from IBS.
Background perspective
“Why should the body digest food or repair itself, when it will be someone else’s lunch” (paraphrased from Sapolsky (2004), Why zebras do not get ulcers).
From an evolutionary perspective, we were prey and needed to be on guard (vigilant) to the presence of predators. In the long forgotten past, the predators were tigers, snakes, and the carnivore for whom we were food as well as other people. Today, the same physiological response pathways are still operating, except that the pathways are now more likely to be activated by time urgency, work and family conflict, negative mental rehearsal and self-judgment. This is reflected in the common colloquial phrases: “It makes me sick to my stomach,” “I have no stomach for it,” “He is gutless,” “It makes me queasy,” “Butterflies in my stomach,” “Don’t get your bowels in uproar,” “Gut feelings’, or “Scared shitless.”
Whether conscious or unconscious, when threatened, our body reacts with a fight/flight/freeze response in which the blood flow is diverted from the abdomen to deep muscles used for propulsion. This results in peristalsis being reduced. At the same time the abdomen tends to brace to protect it from injury. In almost all cases, the breathing patterns shift to thoracic breathing with limited abdominal movement. As the breathing pattern is predominantly in the chest, the person increases the risk of hyperventilation because the body is ready to run or fight.
In our clinical observations, people with IBS, small intestine bacterial overgrowth (SIBO), abdominal discomfort, anxiety and panic, and abdominal pain tend to breathe more in their chest, and when asked to take breathe, they tend to inhale in their upper chest with little or no abdominal displacement. Almost anyone who experiences abdominal pain tends to hold the abdomen rigid as if the splinting could reduce the pain. A similar phenomenon is observed with female students experiencing menstrual cramps. They tend to curl up to protect themselves and breathe shallowly in their chest instead of slowly in their abdomen, a body pattern which triggers a defense reaction and inhibits regeneration. If instead they breathe slowly and uncurl they report a significant decrease in discomfort (Gibney & Peper, 2003).
Paradoxically, this protective stance of bracing the abdomen and breathing shallowly in the chest increases breathing rate and reduces heart rate variability. It reduces and inhibits blood and lymph flow through the abdomen as the defensive posture evokes the physiology of fight/flight/freeze. The reduction in venous blood and lymph flow occurs because the ongoing compression and expansion in the abdomen is inhibited by the thoracic breathing and, moreover, the inhibition of diaphragmatic breathing. It also inhibits peristalsis and digestion. No wonder so many of the people with IBS report that they are reactive to some foods. If the GI track has reduced blood flow and reduced peristalsis, it may be less able to digest foods which would affect the bacteria in the small intestine and colon. We wonder if a risk factor that contributes to SIBO is chronic lack of abdominal movement and bracing.
Slow diaphragmatic abdominal breathing to establish health
“Digestion and regeneration occurs when the person feels safe.”
Effortless, slow diaphragmatic breathing occurs when the diaphragm descends and pushes the abdominal content downward during inhalation, which causes the abdomen to become bigger. As the abdomen expands, the pelvic floor relaxes and descends. During exhalation, the pelvic floor muscles tighten slightly, lifting the pelvic floor and the transverse and oblique abdominal muscles contract and push the abdominal content upward against the diaphragm, allowing the diaphragm to relax and go upward, pushing the air out. The following video, 3D view of the diaphragm, from www.3D-Yoga.com by illustrates the movement of the diaphragm.
Video 2. 3D view of diaphragm by sohambliss from www.3D-Yoga.com,
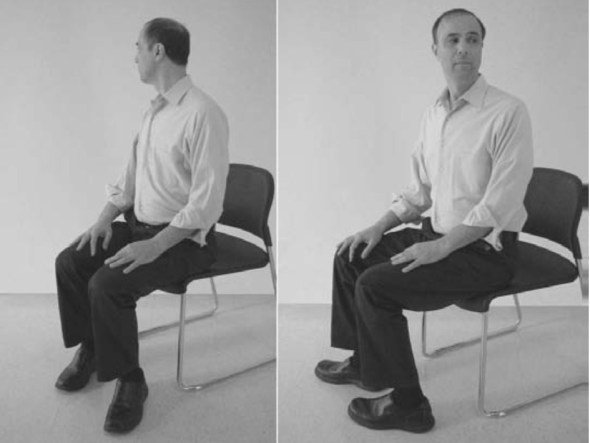
This expansion and constriction of the abdomen occurs most easily if the person is extended, whether sitting or standing erect or lying down, and the waist is not constricted. If the arches forward in a protected pattern and the spine is flexed in a c shape, it would compress the abdomen; instead, the body is long and the abdomen can move and expand during inhalation as the diaphragm descends (see figure 1). If the person holds their abdomen tight or it is constricted by clothing or a belt, it cannot expand during inhalation. Abdominal breathing occurs more easily when the person feels safe and expanded versus unsafe or fearful and collapsed or constricted.
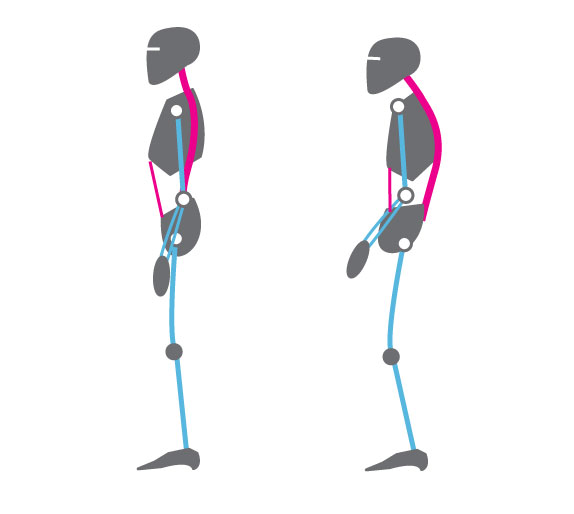
Figure 1. Erect versus collapsed posture note that there is less space for the abdomen to expand in the protective collapsed position. Reproduced by permission from: Clinical Somatics (http://www.clinicalsomatics.ie/
When a person breathes slower and lower it encourages blood and lymph flow through the abdomen. As the person continues to practice slower, lower breathing, it reduces the arousal and vigilance. This is the opposite state of the flight, fight, freeze response so that blood flow is increased in abdomen, and peristalsis re-occurs. When the person practices slow exhalation and breathing and they slightly tighten the oblique and transverse abdominal muscles as well as the pelvic floor and allow these muscles to relax during inhalation. When they breathe in this pattern effortless they, they often will experience an increase in abdominal warmth and an initiation of abdominal sounds (stomach rumble or borborygmus) which indicates that peristalsis has begun to move food through the intestines (Peper et al., 2016). For a detailed description see https://peperperspective.com/2016/04/26/allow-natural-breathing-with-abdominal-muscle-biofeedback-1-2/
What can you do to reduce IBS
There are many factors that cause and effect IBS, some of which we have control over and some which are our out of our control, such as genetics. The purpose of proposed suggestions is to focus on those things over which you have control and reduce risk factors that negatively affect the gastrointestinal track. Generally, begin by integrating self-healing strategies that promote health which have no negative side effects before agreeing to do more aggressive pharmaceutical or even surgical interventions which could have negative side effects. Along the way, work collaboratively with your health care provider. Experiment with the following:
- Avoid food and drinks that may irritate the gastrointestinal tract. These include coffee, hot spices, dairy products, wheat and many others. If you are not sure whether you are reacting to a food or drink, keep a detailed log of what you eat and drink and how you feel. Do self-experimentation by eating or drinking the specific food by itself as the first food in the morning. Then observe how you feel in the next two hours. If possible, eat only organic foods that have not been contaminated by herbicides and pesticides (see: https://peperperspective.com/2015/01/11/are-herbicides-a-cause-for-allergies-immune-incompetence-and-adhd/).
- Identify and resolve stressors, conflicts and problems that negatively affect you and drain your energy. Keep a log to identify situations that drain or increase your subjective energy. Then do problem solving to reduce those situations that drain your energy and increase those situations that increase your energy. For a detailed description of the practice see https://peperperspective.com/2012/12/09/increase-energy-gains-decrease-energy-drains/
Often the most challenging situations that we cannot stomach are those where we feel defeated, helpless, hopeless and powerless or situations where we feel threatened– we do not feel safe. Reach out to other both friends and social services to explore how these situations can be resolved. In some cases, there is nothing that can be done except to accept what is and go on.
- Feel safe. As long as we feel unsafe, we have to be vigilant and are stressed which affects the GI track. Explore the following:
- What does safety mean for you?
- What causes you to feel unsafe from the past or the present?
- What do you need to feel safe?
- Who can offer support that you feel safe?
Reflect on these questions and then explore and implement ways by which you can create feeling more safe.
- Take breaks to regenerate. During the day, at work and at home, monitor yourself. Are you pushing yourself to complete tasks. In a 24/7 world with many ongoing responsibilities, we are unknowingly vigilant and do not allow ourselves to rest and relax to regenerate. Do not wait till you feel tired or exhausted. Stop earlier and take a short break. The break can be a short walk, a cup of tea or soup, or looking outside at a tree. During this break, think about positive events that have happened or people who love you and for whom you feel love. When you smile and think of someone who loves you, such as a grandparent, you may relax and for that moment as you feel safe which allows regeneration to begin.
- Observe how you inhale. Take a deep breath. If you feel you are moving upward and becoming a little bit taller, your breathing is wrong. Put one hand on your lower abdomen and the other on your chest and take a deep breath. If you observe your chest lifted upward and stomach did not expand, your breathing is wrong. You are not breathing diaphragmatically. Watch the following video, The correct way to breathe in, on how to observe your breathing and how to breathe diaphragmatically.
- Learn diaphragmatic breathing. Take time to practice diaphragmatic breathing. Practice while lying down and sitting or standing. Let the breathing rate slow down to about six breaths per minute. Exhale to the count of four and then let it trail off for two more counts, and inhale to the count of three and let it trail for another count. Practice this sitting and lying down (for more details on breathing see: https://peperperspective.com/2014/09/11/a-breath-of-fresh-air-improve-health-with-breathing/.
- Sitting position. Exhale by feeling your abdomen coming inward slightly for the count of four and trailing off for the count of two, then allow the lower ribs to widen, abdomen expand–the whole a trunk expands–as you inhale while the shoulders stay relaxed for a count of three. Allow it to trail off for one more count before you again begin to exhale. Be gentle, do not rush or force yourself. Practice this slower breathing for five minutes. Focus more on the exhalation and allowing the air to just flow in. Give yourself time during the transition between inhalation and exhalation.
- Lying down position. While lying on your back, place a two to five-pound weight such as a bag of rice on your stomach as shown in Figure 2.

Figure 2. Lying down and practicing breathing with two to five-pound weight on stomach (reproduced by permission from Gorter and Peper, 2011.
As you inhale push the weight upward and also feel your lower ribs widen. Then allow exhalation to occur by the weight pushing the abdominal content down which pushes the diaphragm upward. This causing the breath to flow out. As you exhale, imagine the air flowing out through your legs as if there were straws inside your legs. When your attention wanders, smile and bring it back to imagining the air flowing down your legs during exhalation. Practice this for twenty minutes. Many people report that during the practice the gurgling in their abdomen occurs which is a sign that peristalsis and healing is returning.
- Observe and change your breathing during the day. Observe your breathing pattern during the day. Each time you hold your breath, gasp or breathe in your chest, interrupt the pattern and substitute slow diaphragmatic breathing for the next five breaths. Do this the whole day long. Many people observe that when they think of stressor or are worried, they hold their breath or shallow breathe in the chest. If this occurs, acknowledge the worry and focus on changing your breathing. This does not mean that you dismiss the concern, instead for this moment you focus on breathing and then explore ways to solve the problem.
If you observed that under specific circumstance you held your breath or breathed shallowly in your chest, then whenever you anticipate that the same event will occur again, begin to breathe diaphragmatically. To do this consistently is very challenging and most people report that initially they only seem to breathe incorrectly. It takes practice, practice and practice—mindful practice– to change. Yet those who continue to practice often report a decrease in symptoms and feel more energy and improved quality of life.
Summary
Changing habitual health behaviors such as diet and breathing can be remarkably challenging; however, it is possible. Give yourself enough time, and practice it many times until it becomes automatic. It is no different from learning to play a musical instrument or mastering a sport. Initially, it feels impossible, and with lot of practice it becomes more and more automatic. We continue to be impressed that healing is possible. Among our students at San Francisco State University, who practice their self-healing skills for five weeks, approximately 80% report a significant improvement in their health (Peper et al., 2014).
* This blog was adapted and expanded from: Peper, E., Mason, L., & Huey, C. (2017). Healing irritable bowel syndrome with diaphragmatic breathing. Biofeedback. 45(4), 83-87. DOI: 10.5298/1081-5937-45.4.04 https://biofeedbackhealth.files.wordpress.com/2018/02/a-healing-ibs-published.pdf
References
Chey, W. D., Kurlander, J., & Eswaran, S. (2015). Irritable bowel syndrome: a clinical review. Jama, 313(9), 949-958.
Chitkara, D. K., Rawat, D. J., & Talley, N. J. (2005). The epidemiology of childhood recurrent abdominal pain in Western countries: a systematic review. American journal of Gastroenterology, 100(8), 1868-1875.
Dupont, H. L. (2014). Review article: evidence for the role of gut microbiota in irritable bowel syndrome and its potential influence on therapeutic targets. Alimentary pharmacology & therapeutics, 39(10), 1033-1042.
Gibney, H.K. & Peper, E. (2003). Taking control: Strategies to reduce hot flashes and premenstrual mood swings. Biofeedback, 31(3), 20-24.
Gorter, R. & Peper, E. (2011). Fighting Cancer-A NonToxic Approach to Treatment. Berkeley: North Atlantic.
Peper, E., Booiman, A., Lin, I-M, Harvey, R., & Mitose, J. (2016). Abdominal SEMG Feedback for Diaphragmatic Breathing: A Methodological Note. Biofeedback. 44(1), 42-49.
Peper, E., Lin, I-M, Harvey, R., Gilbert, M., Gubbala, P., Ratkovich, A., & Fletcher, F. (2014). Transforming chained behaviors: Case studies of overcoming smoking, eczema and hair pulling (trichotillomania). Biofeedback, 42(4), 154-160.
Sapolsky, R. (2004). Why Zebras Don’t Get Ulcers. New York: Owl Books
Sowder, E., Gevirtz, R., Shapiro, W., & Ebert, C. (2010). Restoration of vagal tone: a possible mechanism for functional abdominal pain. Applied psychophysiology and biofeedback, 35(3), 199-206.
Vlieger, A. M., Blink, M., Tromp, E., & Benninga, M. A. (2008). Use of complementary and alternative medicine by pediatric patients with functional and organic gastrointestinal diseases: results from a multicenter survey. Pediatrics, 122(2), e446-e451.
Freeing the neck and shoulders*
Posted: April 6, 2017 Filed under: Neck and shoulder discomfort, self-healing, Uncategorized | Tags: computer, flexibility, Holistic health, neck pain, relaxation, repetitive strain injurey, shoulder pain, somatic practices, stress 5 CommentsStress, incorrect posture, poor vision and not knowing how to relax may all contribute to neck and shoulder tension. More than 30% of all adults experience neck pain and 45% of girls and 19% of boys 18 year old, report back, neck and shoulder pain (Cohen, 2015; Côté, Cassidy, & Carroll, 2003; Hakala, Rimpelä, Salminen, Virtanen, & Rimpelä, 2002). Shoulder pain affects almost a quarter of adults in the Australian community (Hill et al, 2010). Most employees working at the computer experience neck and shoulder tenderness and pain (Brandt et al, 2014), more than 33% of European workers complained of back-ache (The European Agency for Safety and Health at Work, 2004), more than 25% of Europeans experience work-related neck-shoulder pain, and 15% experience work-related arm pain (Blatter & De Kraker, 2005; Eijckelhof et al, 2013), and more than 90% of college students report some muscular discomfort at the end of the semester especially if they work on the computer (Peper & Harvey, 2008).
The stiffness in the neck and shoulders or the escalating headache at the end of the day may be the result of craning the head more and more forward or concentrating too long on the computer screen. Or, we are unaware that we unknowingly tighten muscles not necessary for the task performance—for example, hunching our shoulders or holding our breath. This misdirected effort is usually unconscious, and unfortunately, can lead to fatigue, soreness, and a buildup of additional muscle tension.
The stiffness in the neck and shoulders or the escalating headache at the end of the day may be the result of craning the head more and more forward or concentrating too long on the computer screen. Poor posture or compromised vision can contribute to discomfort; however, in many cases stress is major factor. Tightening the neck and shoulders is a protective biological response to danger. Danger that for thousands of years ago evoke a biological defense reaction so that we could run from or fight from the predator. The predator is now symbolic, a deadline to meet, having hurry up sickness with too many things to do, anticipating a conflict with your partner or co-worker, worrying how your child is doing in school, or struggling to have enough money to pay for the rent.
Mind-set also plays a role. When we’re anxious, angry, or frustrated most of us tighten the muscles at the back of the neck. We can also experience this when insecure, afraid or worrying about what will happen next. Although this is a normal pattern, anticipating the worst can make us stressed. Thus, implement self-care strategies to prevent the occurrence of discomfort.
What can you do to free up the neck and shoulder?
Become aware what factors precede the neck and shoulder tension. For a week monitor yourself, keep a log during the day and observe what situations occur that precede the neck and should discomfort. If the situation is mainly caused by:
- Immobility while sitting and being captured by the screen. Interrupt sitting every 15 to 20 minutes and move such as walking around while swinging your arms.
- Ergonomic factors such as looking down at the computer or laptop screen while working. Change your work environment to optimize the ergonomics such as using a detached keyboard and raising the laptop screen so that the top of the screen is at eyebrow level.
- Emotional factors. Learn strategies to let go of the negative emotions and do problem solving. Take a slow deep breath and as you exhale imagine the stressor to flow out and away from you. Be willing to explore and change ask yourself: “What do I have to have to lose to change?”, “Who or what is that pain in my neck?”, or “What am I protecting by being so rigid?”
Regardless of the cause, explore the following five relaxation and stretching exercises to free up the neck and shoulders. Be gentle, do not force and stop if your discomfort increases. When moving, continue to breathe.
1. WIGGLE. Wiggle and shake your body many times during the day. The movements can be done surreptitiously such as, moving your feet back and forth in circles or tapping feet to the beat of your favorite music, slightly arching or curling your spine, sifting the weight on your buttock from one to the other, dropping your hands along your side while moving and rotating your fingers and wrists, rotating your head and neck in small unpredictable circles, or gently bouncing your shoulders up and down as if you are giggling. Every ten minutes, wiggle to facilitate blood flow and muscle relaxation.
2. SHAKE AND BOUNCE. Stand up, bend your knees slightly, and let your arms hang along your trunk. Gently bounce your body up and down by bending and straightening your knees. Allow the whole body to shake and move for about one minute like a raggedy Ann doll. Then stop bouncing and alternately reach up with your hand and arm to the ceiling and then let the arm drop. Be sure to continue to breathe.
3. ROTATION MOVEMENT (Adapted from the work by Sue Wilson and reproduced by permission from: Gorter, R. & Peper, E. (2011). Fighting Cancer- A Nontoxic Approach to Treatment).
Pre-assessment: Stand up and give yourself enough space, so that when you lift your arms to shoulder level and rotate, you don’t touch anything. Continue to stand in the same spot during the exercise as shown in figures 1a and 1b.
Lift your arms and hold them out, so that they are at shoulder level, positioned like airplane wings. Gently rotate your arms to the left as far as you can without discomfort. Look along your left arm to your fingertips and beyond to a spot on the wall and remember that spot. Rotate back to center and drop your arms to your sides and relax.
 Figures 1a and 1b. Rotating the arms as far as is comfortable (photos by Jana Asenbrennerova)
Figures 1a and 1b. Rotating the arms as far as is comfortable (photos by Jana Asenbrennerova)
Movement practice. Again, lift your arms to the side so that they are like airplane wings pointing to the left and right. Gently rotate your trunk, keeping your arms fixed at a right angle to your body. Rotate your arms to the right and turn your head to the left. Then reverse the direction and rotate your arms in a fixed position to the left and turn your head to the right. Do not try to stretch or push yourself. Repeat the sequence three times in each direction and then drop your arms to your sides and relax.
With your arms at your sides, lift your shoulders toward your ears while you keep your neck relaxed. Feel the tension in your shoulders, and hold your shoulder up for five seconds. Let your shoulders drop and relax. Then relax even more. Stay relaxed for ten seconds.
Repeat this sequence, lifting, dropping, and relaxing your shoulders two more times. Remember to keep breathing; and each time you drop your shoulders, relax even more after they have dropped.
Repeat the same sequence, but this time, very slowly lift your shoulders so that it takes five seconds to raise them to your ears while you continue to breathe. Keep relaxing your neck and feel the tension just in your shoulders. Then hold the tension for a count of three. Now relax your shoulders very slowly so that it takes five seconds to lower them. Once they are lowered, relax them even more and stay relaxed for five seconds. Repeat this sequence two more times.
Now raise your shoulders quickly toward your ears, feel the tension in your upper shoulders, and hold it for the count of five. Let the tension go and relax. Just let your shoulders drop. Relax, and then relax even more.
Post-assessment. Lift your arms up to the side so that they are at shoulder level and are positioned like airplane wings. Gently rotate without discomfort to the left as far as you can while you look along your left arm to your fingers and beyond to a spot on the wall.
Almost everyone reports that when they rotate the last time, they rotated significantly further than the first time. The increased flexibility is the result of loosening your shoulder muscles.
4. TAPPING FEET (adapted from the work of Servaas Mes)
Diagonal movements underlie human coordination and if your coordination is in sync, this will happen as a reflex without thought. There are many examples of these basic reflexes, all based on diagonal coordination such as arm and leg movement while walking. To restore this coordination, we use exercises that emphasize diagonal movements. This will help you reverse unnecessary tension and use your body more efficiently and thereby reducing “sensory motor amnesia” and dysponesis (Hanna, 2004). Remember to do the practices without straining, with a sense of freedom, while you continue relaxed breathing. If you feel pain, you have gone too far, and you’ll want to ease up a bit. This practice offers brief, simple practices to avoid and reverse dysfunctional patterns of bracing and tension and reduce discomfort. Practicing healthy patterns of movement can reestablish normal tone and reduce tension and pain. This is a light series of movements that involve tapping your feet and turning your head. You’ll be able to do the entire exercise in less than twenty seconds.
Pre-assessment. Sit erect at the edge of the chair with your hands on your lap and your feet shoulders’ width apart, with your heels beneath your knees.
First, notice your flexibility by gently rotating your head to the right as far as you can. Now look at a spot on the wall as a measure of how far you can comfortably turn your head and remember that spot. Then rotate back to the center.
Practicing rotating feet and head. Become familiar with the feet movement, lift the balls of your feet so your feet are resting on your heels. Lightly pivot the balls of your feet to the right, tap the floor, and then stop and relax your feet for just a second. Now lift the balls of your feet, pivot your feet to the left, tap, relax, and pivot back to the right.
Just let your knees follow the movement naturally. This is a series of ten light, quick, relaxed pivoting movements—each pivot and tap takes only about one or two seconds.
Add head rotation. Turn your head in the opposite direction of your feet. This series of movements provides effortless stretches that you can do in less than half a minute as shown in figures 2a and 2b.
 Figures 2a and 2b. Rotating the feet and head in opposite directions (photos by Gary Palmer)
Figures 2a and 2b. Rotating the feet and head in opposite directions (photos by Gary Palmer)
When you’re facing right, move your feet to the left and lightly tap. Then face left and move your feet to the right and tap.
- Continue the tapping movement, but each time pivot your head in the opposite direction. Don’t try to stretch or force the movement.
- Do this sequence ten times. Now stop, face straight head, relax your legs, and just keep breathing.
Post assessment. Rotate your head to the right as far as you can see and look at a spot on the wall. Notice how much more flexibility/rotation you have achieved.
Almost everyone reports being able to rotate significantly farther after the exercise than before. They also report that they have less stiffness in their neck and shoulders.
5. SHOULDER AWARENESS PRACTICE. Sit comfortably with your hands on your lap. Allow your jaw to hang loose and breathe diaphragmatically. Continue to breathe slowly as you do the following:
- Shrug, raising your shoulders towards your ears to 70% of maximum effort and hold them up for about 10 seconds (note the sensations of tension).
- Let your shoulders drop and relax for 10 to 20 seconds
- Shrug, raising your shoulders towards your ears to 50% of maximum effort and hold them up for about 10 seconds (note the sensations of tension).
- Let your shoulders drop and relax for 10 to 20 seconds
- Shrug, raising your shoulders towards your ears to 25% of maximum effort and hold them up for about 10 seconds (note the sensations of tension).
- Let your shoulders drop and relax for 10 to 20 seconds
- Shrug, raising your shoulders towards ears to 5% of maximum effort and hold them up for about 10 seconds (note the sensations of tension).
- Let your shoulders drop and relax for 10 to 20 seconds
- Pull your shoulders down to 25% of maximum effort and hold them up for about 10 seconds (note the sensations of tension).
- Allow your shoulders to come back up and relax for 10 to 20 seconds
Remember to relax your shoulders completely after each incremental tightening. If you tend to hold your breath while raising your shoulders, gently exhale and continue to breathe. When you return to work, check in occasionally with your shoulders and ask yourself if you can feel any of the sensations of tension. If so, drop your shoulders and relax for a few seconds before resuming your tasks.
In summary, when employees and students change their environment and integrate many movements during the day, they report a significant decrease in neck and shoulder discomfort and an increase in energy and health. As one employee reported, after taking many short movement breaks while working at the computer, that he no longer felt tired at the end of the day, “Now, there is life after five”.
To explore how prevent and reverse the automatic somatic stress reactions, read Thomas Hanna‘s book, Somatics: Reawakening The Mind’s Control of Movement, Flexibility, and Health. For easy to do neck and shoulder guided instructions stretches, see the following ebsite: http://greatist.com/move/stretches-for-tight-shoulders
References:
Blatter, B. M., & Kraker, H. D. (2005). Prevalentiecijfers van RSI-klachten en het vóórkomen van risicofactoren in 15 Europese landen. Tijdschrift voor gezondheidswetenschappen, 1, 83, 8-15.
Côté, P., Cassidy, J. D., & Carroll, L. (2003). The epidemiology of neck pain: what we have learned from our population-based studies. The Journal of the Canadian Chiropractic Association, 47(4), 284. http://www.pain-initiative-un.org/doc-
European Agency for Safety and Health at Work (2004). http://europa.eu.int/comm/employment_social/news/2004/nov/musculoskeletaldisorders_en.html
Paoli, P., Merllié, D., & Fundação Europeia para a Melhoria das Condições de Vida e de Trabalho. (2001). Troisième enquête européenne sur les conditions de travail, 2000.
*I thank Sue Wilson and Servaas Mes for teaching me these somatic practices.
Enjoy sex: Breathe away the pain*
Posted: March 19, 2017 Filed under: Breathing/respiration, Pain/discomfort, self-healing, Uncategorized | Tags: Breathing, dyspareunia, intercourse, intimacy, pain, pelvic floor, relaxation, Sexuality, vaginismus 15 CommentsAdapted from: Peper, E. & Cohen, T. (2017). Inhale to breathe away pelvic floor pain and enjoy intercourse. Biofeedback, 45(1), 21–24. https://doi.org/10.5298/1081-5937-45.1.04
“After two and a half years of trying, ups and downs, and a long period of thinking it will never happen, it did happen. I followed your advice by only applying pressure with the cones while inhaling and at the same time relaxing the pelvic floor. We succeeded! we had “real” sex in the first time.”
Millions of women experience involuntary contraction of the musculature of the outer third of the vagina (vaginismus) interfering with intercourse, causing distress and interpersonal difficulty (ter Kuile et, 2010) or pain during intercourse (dyspareunia). It is estimated that 1 to 6% of women have vaginismus (Lewis et al, 2004) and 6.5% to 45.0% in older women and from 14% to 34% in younger women experience dyspareunia (Van Lankveld et al, 2010; Gross & Brubaker, 2022). The most common treatment for vaginismus is sequential dilation of the vaginal opening with progressively larger cones, psychotherapy and medications to reduce the pain and anxiety. At times clients and health care professionals may be unaware of the biological processes that influence the muscle contraction and relaxation of the pelvic floor. Success is more likely if the client works in harmony with the biological processes while practicing self-healing and treatment protocols. These biological processes, described at the end of the blog significantly affects the opening of vestibule and vagina are: 1) feeling safe, 2) inhale during insertion to relax the pelvic floor, 3) stretch very, very slowly to avoid triggering the stretch reflex, and 4) being sexual aroused.
Successful case report: There is hope to resolve pain and vaginismus
Yesterday my husband and I had sex in the first time, after two and a half years of “trying”. Why did it take so long? Well, the doctor said “vaginismus”, the psychologist said “fear”, the physiotherapist said “constricted muscles”, and friends said “just relax, drink some wine and it will happen”.
Sex was always a weird, scary, complicated – and above all, painful – world to me. It may have started in high school: like many other teens, I thought a lot about sex and masturbated almost every night. Masturbation was a good feeling followed by tons of bad feelings – guilt, shame, and feeling disgusting. One of the ideas I had to accept, later in my progress, is that ‘feeling good is a good thing’. It is normal, permitted and even important and healthy.
My first experience, at age 20, was short, very painful, and without any love or even affection. He was…. well, not for me. And I was…. well, naive and with very little knowledge about my body. The experiences that came after that, with other guys, were frustrating. Neither of them knew how to handle the pain that sex caused me, and I didn’t know what to do.
The first gynecologist said that everything is fine and I just need to relax. No need to say I left her clinic very angry and in pain. The second gynecologist was the first one to give it a name: “vaginismus”. He said that there are some solutions to the problem: anesthetic ointment, physiotherapy (“which is rarely helps”, according to his optimistic view..), and if these won’t work “we will start thinking of surgery, which is very painful and you don’t want to go there”. Oh, I certainly didn’t want to go there.
After talking to a friend whose sister had the same problem, I started seeing a great physiotherapist who was an expert in these problems. She used a vaginal biofeedback sensor, that measured muscles’ tonus inside the vagina. My homework were 30 constrictions every day, plus working with “dilators” – plastic cones comes in 6 sizes, starting from a size of a small finger, to a size of a penis.
At this point I was already in a relationship with my husband, who was understanding, calm and most important – very patient. To be honest, we both never thought it would take so long. Practicing was annoying and painful, and I found myself thinking a lot “is it worth it?”. After a while, I felt that the physical practice is not enough, and I need a “psychological breakthrough”. So I stopped practicing and started seeing a psychologist, for about a half a year. We processed my past experiences, examined the thoughts and beliefs I had about sex, and that way we released some of the tension that was shrinking my body.
The next step was to continue practicing with the dilators, but honestly – I had no motivation. My husband and I had great sex without the actual penetration, and I didn’t want the painful practice again. Fortunately, I participated in a short course given by Professor Erik Peper, about biofeedback therapy. In his lecture he described a young woman, who suffered from vulvodynia, a problem that is a bit similar to vaginismus (Peper et al, 2015; See: https://peperperspective.com/2015/09/25/resolving-pelvic-floor-pain-a-case-report/). She learned how to relax her body and deal with the pain, and finally she had sex – and even enjoyed it! I was inspired.
Erik Peper gave me a very important advice: breathing in. Apparently, we can relax the muscles and open the vagina better while inhaling, instead of exhaling – as I tried before. During exhalation the pelvic floor tightens and goes upward while during inhalation the pelvic floor descends and relaxes especially when sitting up (Peper et al, 2016). He advised me to give myself a few minutes with the dilator, and in every inhale – imagine the area opening and insert the dilator a few millimeters. I started practicing again, but in a sitting position, which I found more comfortable and less painful. I advanced to the biggest dilator within a few weeks, and had a just little pain – sometimes without any pain at all. The most important thing I understood was not to be afraid of the pain. The fear is what made me even more tensed, and tension brings pain. Then, my husband and I started practicing with “the real thing”, very slowly and gently, trying to find the best position and angle for us. Finally, we did it. And it was a great feeling.
The biological factors that affect the relaxation/contraction of the pelvic floor and vaginal opening are:
Feeling safe and hopeful. When threatened, scared, anticipate pain, and worry, our body triggers a defense reaction. In this flexor response, labeled by Thomas Hanna as the Red Light Reflex, the body curls up in defense to protect itself which includes the shoulders to round, the chest to be depressed, the legs pressing together, the pelvic floor to tighten and the head to jut forward (Hanna, 2004). This is the natural response of fear, anxiety, prolonged stress or negative depressive thinking.
Before beginning to work on vaginismus, feel safe. This means accepting what is, accepting that it is not your fault, and that there are no demands for performance. It also means not anticipating that it will be again painful because with each anticipation the pelvic floor tends to tightens. Read the chapter on vaginismus in Dr. Lonnie Barbach’s book, For each other: Sharing sexual intimacy (Barbach, 1983).
Inhale during insertion to relax the pelvic floor and vaginal opening. This instruction is seldom taught because in most instances, we have been taught to exhale while relaxing. Exhaling while relaxing is true for most muscles; however, it is different for the pelvic floor. When inhalation occurs, the pelvic floor descends and relaxes. During exhalation the pelvic floor tightens and ascends to support breathing and push the diaphragm upward to exhale the air. Be sure to allow the abdomen to expand during inhalation without lifting the chest and allow the abdomen to constrict during exhalation as if inhalation fills the balloon in the abdomen and exhalation deflates the balloon (for detailed instructions see Peper et al, 2016). Do not inhale by lifting and expanding your chest which often occurs during gasping and and fear. It tends to tighten and lift the pelvic floor.
Experience the connection between diaphragmatic breathing and pelvic floor movement in the following practice.
While sitting upright make a hissing noise as the air escapes with pressure between your lips. As you are exhaling feel, your abdomen and your anus tightening. During the inhalation let your abdomen expand and feel how your anus descends and pelvic floor relaxes. With practice this will become easier.
Stretch very, very slowly to avoid triggering the stretch reflex. When a muscle is rapidly stretched, it triggers an automatic stretch reflex which causes the muscle to contract. This innate response occurs to avoid damaging the muscle by over stretching. The stretch reflex is also triggered by pain and puts a brake on the stretching. Always use a lubricant when practicing by yourself or with a partner. Practice inserting larger and larger diameter dilaters into the vagina. Start with a very small diameter and progress to a larger diameter. These can be different diameter cones, your finger, or other objects. Remember to inhale and feel the pelvic floor descending as you insert the probe or finger. If you feel discomfort/pain, stop pushing, keep breathing, relax your shoulders, relax your hips, legs, and toes and do not push inward and upward again until the discomfort has faded out.
Feel sexually aroused by allowing enough foreplay. When sexually aroused the tissue is more lubricated and may stretch easier. Continue to use a good lubricant.
Putting it all together.
When you feel safe, practice slow diaphragmatic breathing and be aware of the pelvic floor relaxing and descending during inhalation and contracting and going up during exhalation. When practicing stretching the opening with cones or your finger, go very, very slow. Only apply pressure of insertion during the mid-phase of inhalation, then wait during exhalation and then again insert slight more during the next inhalation. When you experience pain, relax your shoulders, keep breathing for four or five breaths till the pain subsides, then push very little during the next inhalation. Go much slower and with more tenderness.
Be patient. Explain to your partner that your body and mind need time to adjust to new feelings. However, don’t stop having sex – you can have great sex without penetration. Practice both alone and with your partner; together find the best angle and rate. Use different lubricants to check out what is best for you. Any little progress is getting you closer to having an enjoyable sex. I recommend watching this TED video of Emily Nagoski explaining the “dual control model” and practicing as she suggests: https://www.youtube.com/watch?v=HILY0wWBlBM
Finally, practice the exercises developed by Dr. Lonnie Barbach, who as one of the first co-directors of clinical training at the University of California San Francisco, Human Sexuality Program, created the women’s pre-orgasmic group treatment program. They are superbly described in her two books, For each other: Sharing sexual intimacy, and For yourself: The fulfillment of female sexuality, and are a must read for anyone desiring to increase sexual fulfillment and joy (Barbach, 2000; 1983).
References:
Barbach, L. (1983). For each other: Sharing sexual intimacy. New York: Anchor
Barbach, L. (2000). For yourself: The fulfillment of female sexuality. New York: Berkley.
BarLewis, R. W., Fugl‐Meyer, K. S., Bosch, R., Fugl‐Meyer, A. R., Laumann, E. O., Lizza, E., & Martin‐Morales, A. (2004). Epidemiology/risk factors of sexual dysfunction. The journal of sexual medicine, 1(1), 35-39. http://www.jsm.jsexmed.org/article/S1743-6095(15)30062-X/fulltext
Gross. E. & Brubaker, L. (2022). Dyspareunia in Women. JAMA. https://doi.org/10.1001/jama.2022.4853
Hanna, T. (2004). Somatics: Reawakening the mind’s control of movement, flexibility, and health. Boston: Da Capo Press.
Martinez Aranda, P. & Peper, E. (2015). The healing of vulvodynia from a client’s perspective. https://biofeedbackhealth.files.wordpress.com/2011/01/a-healing-of-vulvodynia-from-the-client-perspective-2015-06-15.pdf
Peper, E., Booiman, A., Lin, I-M, Harvey, R., & Mitose, J. (2016). Abdominal SEMG Feedback for Diaphragmatic Breathing: A Methodological Note. Biofeedback. 44(1), 42-49. https://biofeedbackhealth.files.wordpress.com/2011/01/1-abdominal-semg-feedback-published.pdf
Peper, E., Martinez Aranda, P., & Moss, E. (2015). Vulvodynia treated successfully with breathing biofeedback and integrated stress reduction: A case report. Biofeedback. 43(2), 103-109. https://biofeedbackhealth.files.wordpress.com/2011/01/a-vulvodynia-treated-with-biofeedback-published.pdf
Ter Kuile, M. M., Both, S., & van Lankveld, J. J. (2010). Cognitive behavioral therapy for sexual dysfunctions in women. Psychiatric Clinics of North America, 33(3), 595-610. https://www.researchgate.net/publication/45090259_Cognitive_Behavioral_Therapy_for_Sexual_Dysfunctions_in_Women
Van Lankveld, J. J., Granot, M., Weijmar Schultz, W., Binik, Y. M., Wesselmann, U., Pukall, C. F., . Achtrari, C. (2010). Women’s sexual pain disorders. The Journal of Sexual Medicine, 7(1pt2), 615-631. http://www.jsm.jsexmed.org/article/S1743-6095(15)32867-8/fulltext
*We thank Dr. Lonnie Barbach for her helpful feedback and support. Written collaboratively with Tal Cohen, biofeedback therapist (Israel) and Erik Peper.
Healthy movement is the new aging
Posted: February 11, 2017 Filed under: Exercise/movement, self-healing, Uncategorized | Tags: aging, diabetes, evolution, exercise, health, interval training, sugar 2 CommentsBorn on 26 November 1911, Mr Robert Marchand and 105 years old, managed cycling 22.55 km (14 miles) at the national velodrome and set a new record for the furthest distance cycled in one hour for riders over 105. (Reynolds, 2017).
Meet 105-year-old Robert Marchand, the centenarian cyclist chasing a new record: https://www.youtube.com/watch?v=Ey48j6dDNEo
As people age there is an increase in Western Diseases such as hypertension, diabetes, gout, cancer, dementia and decreases in physical fitness (Milanović et al, 2013; Tauber, 2016). To assume that the cause of these illnesses is the natural process of aging may be too simplistic. Although aging does affect physiology, there are other factors that contribute to the increase in “Western Diseases” such as diet, lifestyle and genetics.
A significant contributing factor of Western Diseases is diet especially the increase in sugar and simple carbohydrates. Whether you are Pima, Tohono O’odham, and Navajo American Indian Tribes in Arizona, Intuits in Northern Canada, Japanese Americans, or indigenous populations of Kenya, when these people stopped eating their traditional diet and adapted the western high glucose/fructose/simple carbohydrate diet, the degenerative Western Diseases exploded (Bjerregaard et al, 2004; Burkitt & Trowell, 1975; Knowler et al, 1990; Tauber, 2016). Diabetes, hypertension, and cancer which were previously rare skyrocketed within one generation after adapting the Western life style diet. In some of these populations, 30% or more of the adults have diabetes and a significant increase in breast cancer.
The reduction of episodic high intensity physical activity and being sedentary are additional risk factors for the onset of diabetes and cardiovascular disease (Dulloo et al, 2017). As Mensing & Mekel (2015) state, “Sitting is the new smoking.” Sitting encourages more sitting which leads to nonuse of muscles and causes neural and muscle atrophy. Our physiology is efficient and will prune/eliminate what is redundant. This is reflected in the popular phrase, “Use it or lose it.” As we sit for hours in front of digital devices, use escalators, elevators, or drive cars, we are not using the muscles involved in dynamic movement. We are usually unaware of this degenerative process. Instead, we may experience difficulty walking up the stairs which encourages us to take the escalator or elevator. When we do not use the muscles or are limited in movement by discomfort and pain, we move less. As we move less, we become weaker which is often labeled as aging instead of non use.
Just, because most people loose fitness, it may not represent what is possible or optimum. Instead, we may want to emulate the diet and fitness program of Mr. Robert Marchand who at age 103 set a new world record and improved the distance bicycled in one hour from 24.25 km at the age of 101 to 26.92 km at the age of 103. A 11% improvement! As New York Times science writer Gretchen Reynolds reports, “Lifestyle may also matter. Mr. Marchand is “very optimistic and sociable,” The researcher who did the study, Dr. Billat says, “with many friends,” and numerous studies suggest that strong social ties are linked to a longer life. His diet is also simple, focusing on yogurt, soup, cheese, chicken and a glass of red wine at dinner (Reynolds, 2017).
The improvement in bicycling performance and physiological indicators such as ⩒O2max increased (31 to 35 ml.kg-1min-1; +13%), appeared to be due to a change in his training regimen (Billat et al 2016). At age 101 he changed his bicycling training program from riding at a steady speed for one hour to riding 80% at an easy pace and 20% at high intensity. This is a type of interval training and includes enough recovery allows the body the recover and strengthen. This analogous to our evolutionary movement pattern of walking interspersed with short distance high intensity running.
As a hunter and gather we often moved steadily and then had to run very fast to escape a predator or catch an animal. After extreme exertion, we would rest and regenerate (if we did not escape we would be lunch for the predator). Thus episodic high intensity activity with significant rest/regenerative periods is the movement pattern that allowed our species to survive and thrive. Research studies have confirmed that high intensity interval training offers more physiological benefits–increases cardiorespiratory fitness which is a strong determinant of morbidity and mortality– than moderate intensity continuous training (Weston et al, 2014).
Thus when Mr. Marchard changed his exercise pattern from moderate intensity continuous training to high intensity interval training with enough recovery time he set a new world record at age 103. Two years later he set a new world record at age 105.
Exercise improves brain function and interval training appears to improve brain function most. When rats had prolonged exercise, the brain’s stores of energy is significantly lowered in the frontal cortex and hippocampus all areas which area involved in thinking and memory. If on the other hand, the animals had a single intense bout of exercise and were allowed to rest and feed than the brain levels of glycogen was 60% high in the frontal and hippocampus areas. This suggest that the brain can then function better (Matsui et al, 2012).
This perspective is supported by the evolutionary hypothesis discussed by Neuroscientist Daniel Wolpert who points out that brains evolved, not to think or feel, but to direct movement. When movement is no longer needed the brain shrinks and gets reabsorbed which is illustrated by the sea squirt. This animal swims as a juvenile and then anchors on a rock and is passively moved by the currents. Once anchored, it no longer needed to coordinate movement and reabsorb its own nervous system. See Daniel Wolpert’s remarkable TED talk, The real reasons for brains.
The remarkable feat of Mr. Marchand offers suggestions for our own health. Enjoy healthy movement and exercise and incorporate our evolutionary movement patterns: episodic high intensity followed by regeneration. At the same time include a healthy diet by reducing sugars and simple carbohydrates. Finally, it helps to have the right genes.
References:
Billat, V. L., Dhonneur, G., Mille-Hamard, L., Le Moyec, L., Momken, I., Launay, T., & Besse, S. (2016). Case Studies in Physiology: Maximal Oxygen Consumption and Performance in a Centenarian Cyclist. Journal of Applied Physiology, jap-00569. http://jap.physiology.org/content/jap/early/2016/12/29/japplphysiol.00569.2016.full.pdf
Bjerregaard, P., Kue Young, T., Dewailly, E., & Ebbesson, S. O. (2004). Review Article: Indigenous health in the Arctic: an overview of the circumpolar Inuit population. Scandinavian Journal of Social Medicine, 32(5), 390-395. https://www.researchgate.net/publication/51366099_Indigenous_Health_in_the_Arctic_An_Overview_of_the_Circumpolar_Inuit_Population
Burkitt, D.P. & Trowell, H.C. eds. (1975). Refined carbohydrate foods and disease: Some implications of dietary fibre. New York: Academic Press.
Dulloo, A. G., Miles‐Chan, J. L., & Montani, J. P. (2017). Nutrition, movement and sleep behaviours: their interactions in pathways to obesity and cardiometabolic diseases. Obesity Reviews, 18(S1), 3-6.
Knowler, W. C., Pettitt, D. J., Saad, M. F., & Bennett, P. H. (1990). Diabetes mellitus in the Pima Indians: incidence, risk factors and pathogenesis. Diabetes/metabolism reviews, 6(1), 1-27.
Matsui, T., Ishikawa, T., Ito, H., Okamoto, M., Inoue, K., Lee, M. C., … & Soya, H. (2012). Brain glycogen supercompensation following exhaustive exercise. The Journal of physiology, 590(3), 607-616.
Mensing, M., & Mekel, O. C. L. (2015). Sitting is the new smoking-Modelling physical activity interventions in North Rhine-Westphalia. The European Journal of Public Health, 25(suppl 3), ckv171-037.
Milanović, Z., Pantelić, S., Trajković, N., Sporiš, G., Kostić, R., & James, N. (2013). Age-related decrease in physical activity and functional fitness among elderly men and women. Clinical interventions in aging, 8, 549-556.
Reynolds, G. (2017, February 8). Lessons on Aging Well, From a 105-Year-Old Cyclist. Retrieved from: https://www.nytimes.com/2017/02/08/well/move/lessons-on-aging-well-from-a-105-year-old-cyclist.html?rref=collection%2Fsectioncollection%2Fhealth&action=click&contentCollection=health®ion=rank&module=package&version=highlights&contentPlacement=5&pgtype=sectionfront
Taubes, G. (2016). The Case Against Sugar. New York: Alfred A. Knopf.
Weston, K. S., Wisløff, U., & Coombes, J. S. (2014). High-intensity interval training in patients with lifestyle-induced cardiometabolic disease: a systematic review and meta-analysis. British journal of sports medicine, 48(16), 1227-1234. http://www.rcsi.ie/files/facultyofsportsexercise/20141201122758_High-intensity%20interval%20traini.pdf
Wolpert, D. (2011) The Real Reason for Brains. http://www..com/tatedlks/daniel_wolpert_the_real_reason_for_brains.html
Youtube video: Meet 105-year-old Robert Marchand, the centenarian cyclist chasing a new record: https://www.youtube.com/watch?v=Ey48j6dDNEo
Be a tree and share gratitude
Posted: December 11, 2016 Filed under: Breathing/respiration, self-healing, stress management, Uncategorized | Tags: gratitude, Holistic health, Imagery, relaxation, self-healing, stress management 1 Comment
It was late in the afternoon and I was tired. A knock on my office door. One of my students came in and started to read to me from a card. “I want to thank you for all your help in my self-healing project…I didn’t know the improvements were possible for me in a span of 5 weeks…. I thank you so much for encouraging and supporting me…. I have taken back control of myself and continue to make new discoveries about my identity and find my own happiness and fulfillment… Thank you so much.”
I was deeply touched and my eyes started to fill with tears. At that moment, I felt so appreciated. We hugged. My tiredness disappeared and I felt at peace.
In a world where we are constantly bombarded by negative, fearful stories and images, we forget that our response to these stories impacts our health. When people watch fear eliciting videos, their heart rate increases and their whole body responds with a defense reaction as if they are personally being threatened (Kreibig, Wilhelm, Roth, & Gross, 2007). Afterwards, we may continue to interpret and react to new stimuli as if they are the same as what happened in the video. For example, while watching a horror movie, we may hold our breath, perspire and feel our heart racing; however, when we leave the theatre and walk down the street by ourselves, we continue to be afraid and react to stimuli as if what happened in video will now happen to us.
When we feel threatened, our body responds to defend itself. It reduces the blood flow to the gastrointestinal tract where digestion is taking place and sends it to large muscles so that we can run and fight. When threatened, most of our resources shifted to the processes that promote survival while withdrawing it from processes that do not lead to immediate survival such as digestion or regeneration (Sapolsky, 2004). From an evolutionary perspective, why spent resources to heal yourself, enhance your immune system or digest your food when you will become someone else’s lunch!
The more we feel threatened, the more we will interpret the events around us negatively. We become more stressed, defensive, and pessimistic. If this response occurs frequently, it contributes to increased morbidity and mortality. We may not be in control of external or personal event; however, we may be able to learn how to change our reactions to these events. It is our reactions and interpretations of the event that contributes to our ongoing stress responses. The stressor can be labeled as crisis or opportunity.
Mobilize your own healing when you take charge. When 92 students as part of a class at San Francisco State University practiced self-healing skill, most reported significant improvements in their health as shown in Figure 1.

Figure 1. Average self-reported improvement after practicing self-healing skills for at least four weeks. (Reproduced with permission from Tseng, Abili, Peper, & Harvey, 2016).
A strategy that many students used was to interrupt their cascading automatic negative reactions. The moment they became aware of their negative thought and body slumping, they interrupted the process and practiced a very short relaxation or meditation technique.
Implement what the students have done by taking charge of your stress responses and depressive thoughts by 1) beginning the day with a relaxation technique, Relax Body-Mind, 2) interrupting the automatic response to stressors with a rapid stress reduction technique, Breathe and be a Tree, and 3) increasing vitality by the practice, Share Gratitude (Gorter & Peper, 2011).
Relax Body-Mind to start the day*
- Lie down or sit and close your eyes. During the practice if your attention wanders, just bring it back to that part of the body you are asked to tighten or let go.
- Wrinkle your face for ten seconds while continuing to breathe. Let go and relax for ten seconds.
- Bring your hands to your face with the fingers touching the forehead while continuing to breathe. While exhaling, pull your fingers down your face so that you feel your jaw being pulled down and relaxing. Drop your hands to your lap. Feel the sensations in your face and your fingers for ten seconds.
- Make a fist with your hands and lift them slightly up from your lap while continuing to breathe. Feel the sensations of tension in your hands, arms and shoulders for ten seconds. Let go and relax by allowing the arms to drop to your lap and relax. Feel the sensations change in your hands, arms and shoulders for ten seconds.
- Tighten your buttocks and flex your ankles so that the toes are reaching upwards to your knees. Hold for ten seconds while continuing to breathe. Let go and relax for ten seconds.
- Take a big breath while slightly arching your back away from the bed ore chair and expand your stomach while keeping your arms, neck, buttocks and legs relaxed. Hold the breath for twenty seconds. Exhale and let your back relax while allowing the breathing to continue evenly while sensing your body’s contact with the bed or chair for twenty seconds. Repeat three times.
- Gently shake your arms and legs for ten seconds while continuing to breathe. Let go and relax. Feel the tingling sensations in your arms and legs for 20 seconds.
- Evoke a past positive memory where you felt at peace and nurtured.
- Stretch and get up. Know you have done the first self-healing step of the day.
*Be gentle to yourself and stop the tightening or breath holding if it feels uncomfortable.
Breathe and be a Tree to dissipate stress and focus on growth
- Look at a tall tree and realize that you are like a tree that is rooted in the ground and reaching upward to the light. It continues to grow even though it has been buffeted by storms.
- When you become aware of being stressed, exhale slowly and inhale so that your stomach expands, the while slowly exhaling, look upward to the top of a real or imagined tree, admire the upper branches and leaves that are reaching towards the light and smile.
- Remember that even though you started to respond to a stressor, the stressor will pass just like storms battering the tree. By breathing and looking upward, accept what happened and know you are growing just like the tree.
Share Gratitude to increase vitality and health (adapted from Professor Martin Seligman’s 2004 TED presentation, The new era of positive psychology).
- Think of someone who did something for you that impacted your life in a positive direction and whom you never properly thanked. This could be a neighbor, teacher, friend, parent, or other family members.
- Write a 300-word testimonial describing specifically what the person did and how it positively impacted you and changed the course of your life.
- Arrange an actual face-to-face meeting with the person. Tell them you would like to see him/her. If they are far away, arrange a Skype call where you can actually see and hear him/her. Do not do it by email or texting.
- Meet with the person and read the testimonial to her/him.
- It may seem awkward to read the testimonial, after you have done it, you will feel closer and more deeply connected to the person. Moreover, the person to whom you read the testimonial, will usually feel deeply touched. Both your hearts will open.

References:
Gorter, R. & Peper, E. (2011). Fighting cancer: A nontoxic approach to treatment. Berkeley, CA: North Atlantic Books, 205-207.
Kreibig, S. D., Wilhelm, F. H., Roth, W. T., & Gross, J. J. (2007). Cardiovascular, electrodermal, and respiratory response patterns to fear‐and sadness‐inducing films. Psychophysiology, 44(5), 787-806.Kreibig, Sylvia D., Frank H. Wilhelm, Walton T. Roth, and James J. Gross. “Cardiovascular, electrodermal, and respiratory response patterns to fear‐and sadness‐inducing films.” Psychophysiology 44, no. 5 (2007): 787-806.
Sapolsky, R. (2004). Why Zebras Don’t Get Ulcers. New York: Owl Books
Seligman, M. (2014). The new era of positive psychology. Ted Talk. Retrieved, December 10, 2016. https://www.ted.com/talks/martin_seligman_on_the_state_of_psychology
Tseng, C., Abili, R., Peper, E., & Harvey, R. (2016). Reducing Acne-Stress and an integrated self-healing approach. Appl Psychophysiol Biofeedback, 4(4), 445.)
Education versus treatment for self-healing: Eliminating a headache[1]
Posted: November 18, 2016 Filed under: Pain/discomfort, self-healing, stress management, Uncategorized | Tags: autogenic training, biofeedback, education, electromyography, headache, Holistic health, migraine, posture, treatment 3 Comments“I have had headaches for six years, at first occurring almost every day. When I got put on an antidepressant, they slowed to about 3 times a week (sometimes more) and continued this way until I learned relaxation techniques. I am 20 years old and now headache free. Everyone should have this educational opportunity to heal themselves.” -Melinda, a 20 year old student
Health and wellness is a basic right for all people. When students learn stress management skills which include awareness of stress, progressive muscle relaxation, Autogenic phrases, slower breathing, posture change, transforming internal language, self-healing imagery, the role of diet, exercise embedded within an evolutionary perspective as part of a college class their health often improves. When students systematically applied these self-awareness techniques to address a self-selected illness or health behavior (e.g., eczema, diet, exercise, insomnia, or migraine headaches), 80% reported significant improvement in their health during that semester (Peper et al., 2014b; Tseng, et al., 2016). The semester long program is based upon the practices described in the book, Make Health Happen, (Peper, Gibney, & Holt, 2002).
The benefits often last beyond the semester. Numerous students reported remarkable outcomes at follow-up many months after the class had ended because they had mastered the self-regulation skills and continued to implement these skills into their daily lives. The educational model utilized in holistic health courses is often different from the clinical/treatment model.
Educational approach: I am a student and I have an illness (most of me is healthy and only part of me is sick).
Clinical treatment approach: I am a patient and I am sick (all of me is sick)
Some of the concepts underlying the differences between the educational and the clinical approach are shown in Table 1.
| Educational approach | Clinic/treatment approach |
| Focuses on growth and learning | Focuses on remediation |
| Focuses on what is right | Focuses on what is wrong |
| Focuses on what people can do for themselves | Focuses on how the therapist can help patients |
| Assumes students as being competent | Implies patients are damaged and incompetent |
| Students defined as being competent to master the skills | Patients defined as requiring others to help them |
| Encourages active participation in the healing process | Assumes passive participation in the healing process |
| Students keep logs and write integrative and reflective papers, which encourage insight and awareness | Patients usually do not keep logs nor are asked to reflect at the end of treatment to see which factors contributed to success |
| Students meet in small groups, develop social support and perspective | Patients meet only with practitioners and stay isolated |
| Students experience an increased sense of mastery and empowerment | Patients experience no change or possibly a decrease in sense of mastery |
| Students develop skills and become equal or better than the instructor | Patients are healed, but therapist is always seen as more competent than patient |
| Students can become colleagues and friends with their teachers | Patients cannot become friends of the therapist and thus are always distanced |
Table 1. Comparison of an educational versus clinical/treatment approach
The educational approach focuses on mastering skills and empowerment. As part of the course work, students become more mindful of their health behavior patterns and gradually better able to transform their previously covert harm promoting patterns. This educational approach is illustrated in a case report which describes how a student reduced her chronic migraines.
Case Example: Elimination of Chronic Migraines
Melinda, a 20-year-old female student, experienced four to five chronic migraines per week since age 14. A neurologist had prescribed several medications including Imitrex (used to treat migraines) and Topamax (used to prevent seizures as well as migraine headaches), although they were ineffective in treating her migraines. Nortriptyline (a tricyclic antidepressant) and Excedrin Migraine (which contains caffeine, aspirin, and acetaminophen) reduced the frequency of symptoms to three times per week.
She was enrolled in a university biofeedback class that focused on learning self-regulation and biofeedback skills. All these students were taught the fundamentals of biofeedback and practiced Autogenic Training (AT) every day during the semester (Luthe, 1979; Luthe & Schultz, 1969; Peper & Williams, 1980).
In the class, students practiced with surface electromyography (SEMG) feedback to identify the presence of shoulder muscle overexertion (dysponesis), as well as awareness of minimum muscle tension. Additional practices included hand warming, awareness of thoracic and diaphragmatic breathing, and other biofeedback or somatic awareness approaches. In parallel with awareness of physical sensations, students practiced behavioral awareness such as alternating between a slouching body posture (associated with feeling self-critical and powerless) and an upright body posture (associated with feeling powerful and in control). Psychological awareness was focused on transforming negative thoughts and self-judgments to positive empowering thoughts (Harvey and Peper, 2011; Peper et al., 2014a; Peper et al, 2015). Taken together, students systematically increased awareness of physical, behavioral, and psychological aspects of their reactions to stress.
The major determinant for success is to generalize training at school, home and at work. Each time Melinda felt her shoulders tightening, she learned to relax and release the tension in her shoulders, practiced Autogenic Training with the phrase “my neck and shoulders are heavy.” In addition, whenever she felt her body beginning to slouch or noticed a negative self-critical thought arising in her mind, she shifted her body to an upright empowered posture, and substituted positive thoughts to reduce her cortisol level and increase access to positive thoughts (Carney & Cuddy, 2010; Cuddy, 2012; Tsai, et al., 2016). Postural feedback was also informally given by Melinda’s instructor. Every time the instructor noticed her slouching in class or the hallway, he visually changed his own posture to remind her to be erect.
Results
Melinda’s headaches reduced from between three and five per week before enrolling in the class to zero following the course, as shown in Figure 2. She has learned to shift her posture from slouching to upright and relaxed. In addition, she reported feeling empowered, mentally clear, and her acne cleared up. All medications were eliminated. At a two year follow-up, she reported that since she took the class, she had only few headaches which were triggered by excessive stress. 
Figure 2. Frequency of migraine and the implementation of self-practices.
The major factors that contributed to success were:
- Becoming aware of muscle tension through the SEMG feedback. Melinda realized that she had tension when she thought she was relaxed.
- Keeping detailed logs and developing a third person perspective by analyzing her own data and writing a report. A process that encouraged acceptance of self, thereby becoming less judgmental.
- Acquiring a new belief that she could learn to overcome her headaches, facilitated by class lecture and verbal feedback from the instructor.
- Taking active control by becoming aware of the initial negative thoughts or sensations and interrupting the escalating chain of negative thoughts and sensations by shifting the attention to positive empowering thoughts and sensations–a process that integrated mindfulness, acceptance and action. Thus, transforming judgmental thoughts into accepting and positive thoughts.
- Becoming more aware throughout the day, at school and at home, of initial triggers related to body collapse and muscle tension, then changing her body posture and relaxing her shoulders. This awareness was initially developed because the instructor continuously gave feedback whenever she started to slouch in class or when he saw her slouching in the hallways.
- Practicing many, many times during the day. Namely, increasing her ongoing mindfulness of posture, neck, and shoulder tension, and of negative internal dialogue without judgment.
The benefits of this educational approach is captured by Melinda’s summary, “The combined Autogenic biofeedback awareness and skill with the changes in posture helped me remarkably. It improved my self-esteem, empowerment, reduced my stress, and even improved the quality of my skin. It proves the concept that health is a whole system between mind, body, and spirit. When I listen carefully and act on it, my overall well-being is exceptionally improved.”
References:
Carney, D. R., Cuddy, A. J., & Yap, A. J. (2010). Power posing brief nonverbal displays affect neuroendocrine levels and risk tolerance. Psychological Science, 21(10), 1363-1368.
Cuddy, A. (2012). Your body language shapes who you are. Technology, Entertainment, and Design (TED) Talk, available at: http://www.ted.com/talks/amy_cuddy_your_body_language_shapes_who_you_are
Harvey, E. & Peper, E. (2011). I thought I was relaxed: The use of SEMG biofeedback for training awareness and control (pp. 144-159). In W. A. Edmonds, & G. Tenenbaum (Eds.), Case studies in applied psychophysiology: Neurofeedback and biofeedback treatments for advances in human performance. West Sussex, UK: Wiley-Blackwell.
Luthe, W. (1979). About the methods of autogenic therapy (pp. 167-186). In E. Peper, S. Ancoli, & M. Quinn, Mind/body integration. New York: Springer.
Luthe, W., & Schultz, J.H. (1969). Autogenic therapy (Vols. 1-6). New York, NY: Grune and Stratton.
Peper, E., Booiman, A., Lin, I-M., & Shaffer, F. (2014a). Making the unaware aware-Surface electromyography to unmask tension and teach awareness. Biofeedback. 42(1), 16-23.
Peper, E., Gibney, K.H. & Holt. C. (2002). Make health happen: Training yourself to create wellness. Dubuque, IA: Kendall-Hunt. ISBN-13: 978-0787293314
Peper, E., Lin, I-M, Harvey, R., Gilbert, M., Gubbala, P., Ratkovich, A., & Fletcher, F. (2014b). Transforming chained behaviors: Case studies of overcoming smoking, eczema and hair pulling (trichotillomania). Biofeedback, 42(4), 154-160.
Peper, E., Nemoto, S., Lin, I-M., & Harvey, R. (2015). Seeing is believing: Biofeedback a tool to enhance motivation for cognitive therapy. Biofeedback, 43(4), 168-172. doi: 10.5298/1081-5937-43.4.03
Peper, E. & Williams, E.A. (1980). Autogenic therapy (pp. 131-137). In: A. C. Hastings, J. Fadiman, & J. S. Gordon (Eds.). Health for the whole person. Boulder: Westview Press.
Tsai, H. Y., Peper, E., & Lin, I. M. (2016). EEG patterns under positive/negative body postures and emotion recall tasks. NeuroRegulation, 3(1), 23-27.
Tseng, C., Abili, R., Peper, E., & Harvey, R. (2016). Reducing acne-stress and an integrated self-healing approach. Poster presented at the 47th Annual Meeting of the Association for Applied Psychophysiology and Biofeedback, Seattle WA, March 9-12, 2016.
[1] Adapted from: Peper, E., Miceli, B., & Harvey, R. (2016). Educational Model for Self-healing: Eliminating a Chronic Migraine with Electromyography, Autogenic Training, Posture, and Mindfulness. Biofeedback, 44(3), 130–137. https://biofeedbackhealth.files.wordpress.com/2011/01/a-educational-model-for-self-healing-biofeedback.pdf
Allow natural breathing with abdominal muscle biofeedback [1, 2]
Posted: April 26, 2016 Filed under: Breathing/respiration, self-healing, Uncategorized | Tags: abdominal breathing, biofeedback, EMG, Muscle feedback, respiration 7 CommentsWhen I allowed my lower abdomen to expand during inhalation without any striving and slightly constrict during exhalation, breathing was effortless. At the end of exhalation, I just paused and then the air flowed in without any effort. I felt profoundly relaxed and safe. With each effortless breath my hurry-up sickness dissipated.
Effortless breathing from a developmental perspective is a whole body process previously described by the works of Elsa Gindler, Charlotte Selver and Bess M. Mensendieck (Brooks, 1986; Bucholtz, 1994; Gilbert 2016, Mensendieck, 1954). These concepts underlie the the research and therapeutic approach of Jan van Dixhoorn (2008, 2014) and is also part of the treatment processes of Mensendieck/Cesar therapists (Profile Mensendeick) . During inhalation the body expands and during exhalation the body contracts. While sitting or standing, during exhalation the abdominal wall contracts and during inhalation the abdominal wall relaxes. This whole body breathing pattern is often absent in clients who tend to lift their chest and do not expand or sometimes even constrict their abdomen when they inhale . Even if their breathing includes some abdominal movement, often only the upper abdomen above the belly button moves while the lower abdomen shows limited or no movement. This may be associated with physical and emotional discomfort such as breathing difficulty, digestive problems, abdominal and pelvic floor pains, back pain, hyper vigilance, and anxiety. (The background, methodology to monitor and train with muscle biofeedback, and pragmatic exercises are described in detail in our recent published article, Peper, E., Booiman, A.C, Lin, I-M, Harvey, R., & Mitose, J. (2016). Abdominal SEMG Feedback for Diaphragmatic Breathing: A Methodological Note. Biofeedback. 44(1), 42-49.)
Some of the major factors that contribute to the absence of abdominal movement during breathing are (Peper et, 2015):
- ‘Designer jean syndrome’ (the modern girdle): The abdomen is constricted by a waist belt, tight pants or slimming underwear such as Spanx and in former days by the corset as shown in Figure 1 (MacHose & Peper, 1991; Peper & Tibbitts, 1994).
- Self-image: The person tends to pull his or her abdomen inward in an attempt to look slim and attractive.
- Defense reaction: The person unknowingly tenses the abdominal wall –a flexor response-in response to perceived threats (e.g., worry, external threat, loud noises, feeling unsafe). Defense reactions are commonly seen in clients with anxiety, panic or phobias.
- Learned disuse: The person covertly learned to inhibit any movement in the abdominal wall to protect themselves from experiencing pain because of prior abdominal injury or surgery (e.g., hernia or cesarean), abdominal pain (e.g., irritable bowel syndrome, dysmenorrhea, vulvodynia, pelvic floor pain, low back pain).
- Inability to engage abdominal muscles because of the lack of muscle tone.
 Figure 1. How clothing constricts abdominal movement. Previously it was a corset as shown on the left and now it is Spanx or very tight clothing which restricts the waist.
Figure 1. How clothing constricts abdominal movement. Previously it was a corset as shown on the left and now it is Spanx or very tight clothing which restricts the waist.
Whether the lower abdominal muscles are engaged or not (either by chronic tightening or lack of muscle activation), the resultant breathing pattern tends to be more thoracic, shallow, rapid, irregular and punctuated with sighst. Over time participants may not able to activate or relax the lower abdominal muscles during the respiratory cycle. Thus it is no longer involved in whole body movement which can usually be observed in infants and young children.
In our published paper by Peper, E., Booiman, A.C, Lin, I-M, Harvey, R., & Mitose, J. (2016), we describe a methodology to re-establish effortless whole body breathing with the use of surface electromyography (SEMG) recorded from the lower abdominal muscles (external/ internal abdominal oblique and transverse abdominis) and strategies to teach engagement of these lower abdominal muscles. Using this methodology, the participants can once again learn how to activate the lower abdominal muscles to flatten the abdominal wall thereby pushing the diaphragm upward during exhalation. Then, during inhalation they can relax the muscles of the abdominal wall to expand the abdomen and allow the diaphragm to descend as shown in Figure 2.
 Figure 2. Correspondence between respiratory strain gauge changes and SEMG activity during breathing. When the person exhales, the lower abdominal SEMG activity increases and when the person inhales the SEMG decreases.
Figure 2. Correspondence between respiratory strain gauge changes and SEMG activity during breathing. When the person exhales, the lower abdominal SEMG activity increases and when the person inhales the SEMG decreases.
The published article discusses the factors that contribute to the breathing dysregulation and includes guidelines for using SEMG abdominal recording. It describes in detail–with illustrations–numerous practices such as tactile awareness of the lower abdomen, active movements such as pelvic rocking and cats and dogs exercises that people can practice to facilitate lower abdominal breathing. One of these practices, Sensing the lower abdomen during breathing, is developed and described by Annette Booiman, Mensendieck therapist
Sensing the lower abdomen during breathing
The person place their hands below their belly button with the outer edge of hands resting on the groin. During inhalation, they practice bringing their lower abdomen/belly into their hands so that the person can feel the lower abdomen expanding. During exhalation, they pull their lower abdomen inward and away from their palms as shown in Figure 3.

Figure 3. Hands placed below the belly button to sense the movement of the lower abdomen.
Lower abdominal SEMG feedback is useful in retraining breathing for people with depression, rehabilitation after pregnancy, abdomen or chest surgery (e.g., Cesarean surgery, hernia, or appendectomy operations), anxiety, hyperventilation, stress-related disorders, difficulty to become pregnant or maintain pregnancy, pelvic floor problems, headache, low back pain, and lung diseases. As one participant reported:
“Biofeedback might be the single thing that helped me the most. When I began to focus on breathing, I realized that it was almost impossible for me since my body was so tightened. However, I am getting much better at breathing diaphragmatically because I practice every day. This has helped my body and it relaxes my muscles, which in turn help reduce the vulvar pain.”
REFERENCES
Mensendieck, B.M. (1954). Look better, feel better. Pymble, NSW, Australia: HarperCollins.
van Dixhoorn, J. (2008). Whole body breathing. Biofeedback. 3I(2), 54-58
Gilbert, C. (2016). Working with breathing , some early influences. Paper presented at the 47th Annual Meeting of the Association for Applied Psychophysiology and Biofeedback, Seattle WA, March 9-12, 2016.
1. Adapted from: Peper, E., Booiman, A., Lin, I-M, Harvey, R., & Mitose, J. (2016). Abdominal SEMG Feedback for Diaphragmatic Breathing: A Methodological Note. Biofeedback. 44(1), 42-49.
2. .I thank Annette Booiman for her constructive feedback in writing this blog.
Increase energy*
Posted: April 1, 2016 Filed under: self-healing, stress management, Uncategorized | Tags: cognitive therapy, energy level, health, Holistic health, stress management 2 CommentsAre you full of pep and energy, ready to do more? Or do you feel drained and exhausted? After giving at the office, is there nothing left to give at home? Do you feel as if you are on a treadmill that will never stop, that more things feel draining than energizing?
Feeling chronically drained is often a precursor for illness; conversely, feeling energized enhances productivity and encourages health. An important aspect of staying healthy is that one’s daily activities are filled more with activities that contribute to our energy than with tasks and activities that drain our energy. Similarly, Dr. John Gottman and colleagues have discovered that marriages prosper when there are many more positive appreciations communicated by each partner than negative critiques.
Energy is the subjective sense of feeling alive and vibrant. An energy gain is an activity, task, or thought that makes you feel better and slightly more alive—those things we want to or choose to do. An energy drain is the opposite feeling—less alive and almost depressed—those things we have to or must do; often something that we do not want to do. In almost all cases, it is not that we have to, should, or must do, it is a choice. Remember, even though you may say, “I have to study.” It is a choice. You can choose not to study and choose to drop out of school. Similarly, when you say, “I have to do the dishes,” it is still a choice. You can choose to do the dishes or let the dirty dishes pile up and just use paper plates.
Energy drains and gains are always unique to the individual; namely, what is a drain for one can be a gain for another. Energy drains can be doing the dishes and feeling resentful that your partner or children are not doing them, or anticipating seeing a person whom you do not really want to see. An energy gain can be meeting a friend and talking or going for a walk in the woods, or finishing a work project.
When patients with cancer start exploring what they truly would like to do and start acting on their unfulfilled dreams, a few experience that their health improves as documented by Dr. Lawrence LeShan in his remarkable book, Cancer as a Turning Point. So often our lives are filled with things that we should do versus want to do. In some cases, the lives we created are not the ones we wanted but the result of self-doubt and worry, “If I did do this, my family and friends won’t like me”, or “I am not sure I will be successful so I will do something that is safe.” Just ask yourself the question when you woke up this morning and most mornings this week, “How did you feel?” Did you felt happy and looking forward to the day?

Explore strategies to decrease the drains and increase the energy gains. Use the following exercise to increase your energy:
- For one week monitor your energy drains and energy gains. Monitor events, activities, thoughts, or emotions that increase or decrease energy at home and at work. For example some drains can include cleaning bathroom, cooking another meal, or talking to a family member on the phone, while gains can be taking a walk, talking to a friend, completing a work task. Be very honest, just note the events that change your energy level.
- After the week look over your notes and identify at least one activity that drains your energy and one activity that increases your energy
- Develop a strategy to decrease one of the energy drains. Be very specific how, where, when, with whom, and which situations decreasing the tasks that drain your energy. As you think about it, anticipate obstacles that may interfere with reducing your drains and develop new ways to overcome these obstacles such as trading tasks with others (I will cook if you clean the bathroom), setting time limits, giving yourself positive reward after finishing the task (a cup of tea, a text or phone message to a close friend, watching a video in the evening).
- Develop new ways how you can increase energy gains such as doing exercise, completing a task.
- Each day implement the behavior to reduce one less energy drain and increase one energy gain and observe what happens.
Initially it may seem impossible, many students and clients report that the practice made them aware, increased their energy, and they had more control over their lives than they thought. It also encouraged them to explore the question, “What is it that you really want to do?” So often we do energy drains because of convention, habit and fear which makes us feel powerless and suppresses our immune system thereby increasing the risk of illness. In observing the energy drains and energy gains, it may give the person a choice. Sometimes, the choice is not changing the tasks but how we think about it. Many of the things we do are not MUSTs; they are choices. I do the work at my job because I choose to benefits of earning money.
How your internal language impacts your energy**
Sit and think of something that you feel you have to do, should do, or must do. Something you slightly dread such as cleaning the dishes, doing a math assignment. While sitting say to yourself, “I have to do, should do, or must do_______________.” Keep repeating the phrase for a minute.
Then change your internal phrase and instead say one of the following phrases, “I choose to do,” “I look forward to doing,” or “I choose not to do _________.” Keep repeating the phrase for a minute.
Now compare how you felt. Almost all people feel slight less energy and more depressed when they are thinking, “I have to do,” “should do”, or must do”. While when they shifted the phrase to, “I choose to,” “I look forward to doing,” or “I choose not to do it,” they feel lighter, more expanded and more optimistic. When university students practice this change of language during the week, they find it was easier to start and complete their homework tasks.
Watch your thoughts; they become words.
Watch your words; they become actions.
Watch your actions; they become habits.
Watch your habits; they become character.
Watch your character; it becomes your destiny.
– Frank Outlaw
References
Gottman, J.M. & Silver, N. (2015). The Seven Principles for Making Marriage Work. New York: Harmony.
LeShan, L. (1999). Cancer as a Turning Point. New York: Plume
*Adapted from: Peper, E. (2016). Increase energy. Western Edition. April, pp4. http://thewesternedition.com/admin/files/magazines/WE-April-2016.pdf
**Adapted from: Gorter, R. & Peper, E. (2011). Fighting Cancer-A Nontoxic Approach to Treatment. Berkeley: North Atlantic Books, 107-200.
Can abdominal surgery cause epilepsy, panic and anxiety and be reversed with breathing biofeedback?*
Posted: March 5, 2016 Filed under: Breathing/respiration, self-healing, stress management, Uncategorized | Tags: anxiety, biofeedback, Breathing, epilepsy, iatrogenic illness, learned disuse, panic, respiration, surgery 4 Comments“I had colon surgery six months ago. Although I made no connection to my anxiety, it just started to increase and I became fearful and I could not breathe. The asthma medication did not help. Learning effortless diaphragmatic breathing and learning to expand my abdomen during inhalation allowed me to breathe comfortably without panic and anxiety—I could breathe again.” (72 year old woman)
“One year after my appendectomy, I started to have twelve seizures a day. After practicing effortless diaphragmatic breathing and changing my lifestyle, I am now seizure-free.” (24 year old male college student)
One of the hidden long term costs of surgery and injury is covert learned disuse. Learned disuse occurs when a person inhibits using a part of their body to avoid pain and compensates by using other muscle patterns to perform the movements (Taub et al, 2006). This compensation to avoid discomfort creates a new habit pattern. However, the new habit pattern often induces functional impairment and creates the stage for future problems.
Many people have experienced changing their gait while walking after severely twisting their ankle or breaking their leg. While walking, the person will automatically compensate and avoid putting weight on the foot of the injured leg or ankle. These compensations may even leads to shoulder stiffness and pain in the opposite shoulder from the injured leg. Even after the injury has healed, the person may continue to move in the newly learned compensated gait pattern. In most cases, the person is totally unaware that his/her gait has changed. These new patterns may place extra strain on the hip and back and could become a hidden factor in developing hip pain and other chronic symptoms.
Similarly, some women who have given birth develop urinary stress incontinence when older. This occurred because they unknowingly avoided tightening their pelvic floor muscles after delivery because it hurt to tighten the stretched or torn tissue. Even after the tissue was healed, the women may no longer use their pelvic floor muscles appropriately. With the use of pelvic floor muscle biofeedback, many women with stress incontinence can rapidly learn to become aware of the inhibited/forgotten muscle patterns (learned disuse) and regain functional control in nine sessions of training (Burgio et al., 1998; Dannecker et al., 2005). The process of learned disuse is the result of single trial learning to avoid pain. Many of us as children have experienced this process when we touched a hot stove—afterwards we tended to avoid touching the stove even when it was cold.
Often injury will resolve/cure the specific problem. It may not undo the covert newly learned dysfunctional patterns which could contribute to future iatrogenic problems or illnesses (treatment induced illness). These iatrogenic illnesses are treated as a new illness without recognizing that they were the result of functional adaptations to avoid pain and discomfort in the recovery phase of the initial illness.
Surgery creates instability at the incision site and neighboring areas, so our bodies look for the path of least resistance and the best place to stabilize to avoid pain. (Adapted from Evan Osar, DC).
After successful surgical recovery do not assume you are healed!
Yes, you may be cured of the specific illness or injury; however, the seeds for future illness may be sown. Be sure that after injury or surgery, especially if it includes pain, you learn to inhibit the dysfunctional patterns and re-establish the functional patterns once you have recovered from the acute illness. This process is described in the two cases studies in which abdominal surgeries appeared to contribute to the development of anxiety and uncontrolled epilepsy.
How abdominal surgery can have serious, long-term effect on changing breathing patterns and contributing to the development of chronic illness.
When recovering from surgery or injury to the abdomen, it is instinctual for people to protect themselves and reduce pain by reducing the movement around the incision. They tend to breathe more shallowly as not to create discomfort or disrupt the healing process (e.g., open a stitch or staple. Prolonged shallow breathing over the long term may result in people experiencing hyperventilation induced panic symptoms or worse. This process is described in detail in our recent article, Did You Ask about Abdominal Surgery or Injury? A Learned Disuse Risk Factor for Breathing Dysfunction (Peper et al., 2015). The article describes two cases studies in which abdominal surgeries led to breathing dysfunction and ultimately chronic, serious illnesses.
Reducing epileptic seizures from 12 per week to 0 and reducing panic and anxiety
A routine appendectomy caused a 24-year-old male to develop rapid, shallow breathing that initiated a series of up to 12 seizures per week beginning a year after surgery. After four sessions of breathing retraining and incorporating lifestyle changes over a period of three months his uncontrolled seizures decreased to zero and is now seizure free. In the second example, a 39-year-old woman developed anxiety, insomnia, and panic attacks after her second kidney transplant probably due to shallow rapid breathing only in her chest. With biofeedback, she learned to change her breathing patterns from 25 breaths per minute without any abdominal movement to 8 breathes a minute with significant abdominal movement. Through generalization of the learned breathing skills, she was able to achieve control in situations where she normally felt out of control. As she practiced this skill her symptoms were significantly reduced and stated:
“What makes biofeedback so terrific in day-to-day situations is that I can do it at any time as long as I can concentrate. When I feel I can’t concentrate, I focus on counting and working with my diaphragm muscles; then my concentration returns. Because of the repetitive nature of biofeedback, my diaphragm muscles swing into action as soon as I started counting. When I first started, I had to focus on those muscles to get them to react. Getting in the car, I find myself starting these techniques almost immediately. Biofeedback training is wonderful because you learn techniques that can make challenging situations more manageable. For me, the best approach to any situation is to be calm and have peace of mind. I now have one more way to help me achieve this.” (From: Peper et al, 2001).
The commonality between these two participants was that neither realized that they were bracing the abdomen and were breathing rapidly and shallowly in the chest. I highly recommend that anyone who has experienced abdominal insults or surgery observe their breathing patterns and relearn effortless breathing/diaphragmatically breathing instead of shallow, rapid chest breathing often punctuated with breath holding and sighs.
It is important that medical practitioners and post-operative surgery patients recognize the common covert learned disuse patters such as shifting to shallow breathing to avoid pain. The sooner these patterns are identified and unlearned, the less likely will the person develop future iatrogenic illnesses. Biofeedback is an excellent tool to help identify and retrain these patterns and teach patients how to reestablish healthy/natural body patterns.
The full text of the article see: “Did You Ask About Abdominal Surgery or Injury? A Learned Disuse Risk Factor for Breathing Dysfunction,”
*Adapted from: Biofeedback Helps to Control Breathing Dysfunction.http://www.prweb.com/releases/2016/02/prweb13211732.htm
References
Burgio, K. L., Locher, J. L., Goode, P. S., Hardin, J. M., McDowell, B. J., Dombrowski, M., & Candib, D. (1998). Behavioral vs drug treatment for urge urinary incontinence in older women: a randomized controlled trial. Jama, 280(23), 1995-2000.
Dannecker, C., Wolf, V., Raab, R., Hepp, H., & Anthuber, C. (2005). EMG-biofeedback assisted pelvic floor muscle training is an effective therapy of stress urinary or mixed incontinence: a 7-year experience with 390 patients. Archives of Gynecology and Obstetrics, 273(2), 93-97.
Osar, E. (2016). http://www.fitnesseducationseminars.com/
Peper, E., Castillo, J., & Gibney, K. H. (2001, September). Breathing biofeedback to reduce side effects after a kidney transplant. In Applied Psychophysiology and Biofeedback (Vol. 26, No. 3, pp. 241-241). 233 Spring St., New York, NY 10013 USA: Kluwer Academic/Plenum Publ.
Peper, E., Gilbert, C.D., Harvey, R. & Lin, I-M. (2015). Did you ask about abdominal surgery or injury? A learned disuse risk factor for breathing dysfunction. Biofeedback. 34(4), 173-179. DOI: 10.5298/1081-5937-43.4.06
Taub, E., Uswatte, G., Mark, V. W., Morris, D. M. (2006). The learned nonuse phenomenon: Implications for rehabilitation. Europa Medicophysica, 42(3), 241-256.
