A historical perspective of neurofeedback: Video interview by Larrry Berkelhammer of Erik Peper
Posted: January 18, 2015 Filed under: Uncategorized | Tags: biofeedback, cancer, electroencephalography, health, neurofeedback, self-regulation 1 CommentDr. Erik Peper is interviewed by Dr. Larry Berkelhammer about the research he did in the late 60s and early 70s on EEG alpha training. He describes how he learned to turn off alpha brain rhythms in one hemisphere and turn them on in the other.
Neurofeedback equipment allows researchers and clinicians to get extremely useful feedback, allowing people who are hooked up to get very good at identifying their own brain rhythms and to alter them at will. This can potentially allow us to re-train our brains. Dr. Peper talks about how the real gift of science is about being open to explore rather than to assume our beliefs are factual. Science is about curiosity, experimentation, and exploration. In studying people with cancer and other diseases it is vital that we study more than just pathology–we need to study those individuals who are the outliers, that is, those who recovered against all odds–let’s see what they did to mobilize their health.
Cellphone harm: Cervical spine stress and increase risk of brain cancer
Posted: November 20, 2014 Filed under: Uncategorized | Tags: cancer, cell phones, ergonomics, health, microwaves, neck pain, posture, shoulder pain, wireless 6 CommentsIt is impossible to belief that that only a few years ago there were no cell phones.
When I go home, I purposely put the phone away so that I can be present with my children.
I just wonder if the cell phone’s electromagnetic radiation could do harm?
Cell phone use is ubiquitous since information is only a key press or voice command away. Students spend about many hours a day looking and texting on a cell phone and experience exhaustion and neck and shoulder discomfort (Peper et al, 2013). Constant use may also have unexpected consequences: Increased stress on the cervical spine and increased risk for brain cancer.
Increased cervical spine stress
As we look at the screen, text messages or touch the screen for more information, we almost always bend our head down to look down. This head forward position increases cervical compression and stress. The more the head bends down to look, the more the stress in the neck increases as the muscles have to work much harder that hold the head up. In a superb analysis Dr. Kennth Hansraj, Chief of Spine Surgery 0f New York Spine Surgery & Rehabilitation Medicine, showed that stress on the cervical spine increases from 10-12 lbs when the head is in its upright position to 60 lbs when looking down.
 Figure 1. Stress on the cervical spine as related to posture. (From: Hansraj, K. K. (2014). Assessment of stresses in the cervical spine caused by posture and position of the head. Surgical technology international, 25, 277-279.)
Figure 1. Stress on the cervical spine as related to posture. (From: Hansraj, K. K. (2014). Assessment of stresses in the cervical spine caused by posture and position of the head. Surgical technology international, 25, 277-279.)
Looking down for a short time period is no problem; however, many of us look down for extended periods. This slouched collapsed position is becoming the more dominant position. A body posture which tends to decrease energy, and increase hopeless, helpless, powerless thoughts (Wilson & Peper, 2004; Peper & Lin, 2012). The long term effects of this habitual collapsed position are not know–one can expect more neck and back problems and increase in lower energy levels.
increased risk for brain cancer and inactive sperm and lower sperm count
Cell phone use not only affect posture, the cell phone radio-frequency electromagnetic radiation by which the cell phone communicates to the tower may negatively affect biological tissue. It would not be surprising that electromagnetic radiation could be harmful; since, it is identical to the frequencies used in your microwave ovens to cook food. The recent research by Drs Michael Carlberg and Lennart Hardell of the Department of Oncology, University Hospital, Örebro, Sweden, found that long term cell phone use is associated by an increased risk of developing malignant glioma (brain cancers) with the largest risk observed in people who used the cell phone before the age of 20. In addition, men who habitually carry the cell phone in a holster or in their pocket were more likely to have inactive or less mobile sperm as well as a lower sperm count.
What can you do:
Keep an upright posture and when using a cell phone or tablet. Every few minutes stretch, look up and reach upward with your hands to the sky.
Use your speaker phone or ear phones instead of placing the phone against your head.
Enjoy the cartoon video clip, Smartphone Ergonomics – Safe Tips – Mobile or Smart Phone Use while Driving, Traveling on the Move.
References:
Agarwal, A., Singh, A., Hamada, A., & Kesari, K. (2011). Cell phones and male infertility: a review of recent innovations in technology and consequences. International braz j urol, 37(4), 432-454. http://www.isdbweb.org/documents/file/1685_8.pdf
Carlberg, M., & Hardell, L. (2014). Decreased Survival of Glioma Patients with Astrocytoma Grade IV (Glioblastoma Multiforme) Associated with Long-Term Use of Mobile and Cordless Phones. International journal of environmental research and public health, 11(10), 10790-10805. http://www.mdpi.com/1660-4601/11/10/10790/htm
De Iuliis, G. N., Newey, R. J., King, B. V., & Aitken, R. J. (2009). Mobile phone radiation induces reactive oxygen species production and DNA damage in human spermatozoa in vitro. PloS one, 4(7), e6446.
Hansraj, K. K. (2014). Assessment of stresses in the cervical spine caused by posture and position of the head. Surgical technology international, 25, 277-279.
Peper, E. & Lin, I-M. (2012). Increase or decrease depression-How body postures influence your energy level. Biofeedback, 40 (3), 126-130.
Peper, E., Waderich, K., Harvey, R., & Sutter, S. (2013). The Psychophysiology of Contemporary Information Technologies Tablets and Smartphones Can Be a Pain in the Neck. In Applied Psychophysiology and Biofeedback, 38(3), 219.
Wilson, V.E. and Peper, E. (2004). The Effects of upright and slumped postures on the generation of positive and negative thoughts. Applied Psychophysiology and Biofeedback.29 (3), 189-195.
Choices: Creating meaningful days
Posted: October 19, 2014 Filed under: Uncategorized | Tags: cancer, depression, healing, health, hope, palliative care 1 CommentWhen you woke up this morning, how did you feel? Were you looking forward to the day anticipating with joy what would occur or were you dreading the day as if once again you had to step on the treadmill of life?

Whenever I ask this question of college students in their junior or senior year at an urban university about 20% will answer that they are looking forward to the day. The majority answer, “Well not really”, or even “Oh shit, another day”. For many students the burden of living- working 40 hours a week to pay for rent and tuition, worrying about financial debt, and the challenge of commuting, and finding time to do the homework—feels and is overwhelming.
Asking this question about the quality—not quantity—of life is not just a question for students–it is applicable for all of us. The more one chooses to do actively what gives fulfillment and meaning, the higher the quality of life (I do not mean eating more chocolate).
In a remarkable study by Dr. Jennifer Temel and her many colleagues, patients with metastatic non-small-cell lung cancer were given the option of early palliative care versus standard aggressive end-of-life treatment. The patients who were assigned to the early palliative care group had significantly better quality of life, fewer depressive symptoms and lived on the average three months longer than the group who received standard treatment.
Even at the end of life there may be choices. Choosing quality of life and doing what gives meaning may nurture a peaceful transition in death. This process of choice has been tenderly described in the recent New York Times essay, The best possible day. Take a moment and read this article by clicking on the link. http://www.nytimes.com/2014/10/05/opinion/sunday/the-best-possible-day.html?smid=fb-share&_r=0
Then ask yourself each day, “Am I looking forward to my day and my activities?” If the answer tends to be “No,” begin to explore new options. Ask yourself, “What would I like to do and look forward to?” First begin to dream about possible options and then begin to plan how to implement your dreams so that you are on the path to where you want to be.
It is a challenging process; however, each of us can do something that will give meaning and joy to our lives. For suggestions, see the outstanding book by Dr. Lawrence LeShan, Cancer as a Turning Point, or explore the practices in our book by Drs. Robert Gorter and Erik Peper, Fighting Cancer- A Non-Toxic Approach to Treatment.
Reference:
Cartoon ergonomics for working at the computer and laptop
Posted: September 30, 2014 Filed under: Uncategorized | Tags: cell phones, computer, health, Laptop, muscle tension, neck pain, pain, posture, shoulder pain 10 CommentsI finally bought a separate keyboard and a small stand for my laptop so that the screen is at eye level and my shoulders are relaxed while typing at the keyboard. To my surprise, my neck and shoulder tightness and pain disappeared and I am much less exhausted.
How we sit and work at the computer significantly affects our health and productivity. Ergonomics is the science that offers guidelines on how to adjust your workspace and equipment to suit your individual needs. It is just like choosing appropriate shoes–Ever try jogging in high heels? The same process applies to the furniture and equipment you use when computing.
When people arrange their work setting according to good ergonomic principles and incorporate a healthy computing work style numerous disorders (e.g., fatigue, vision discomfort, head, neck, back, shoulder, arm or hand pain) may be prevented (Peper et al, 2004). For pragmatic tips to stay health at the computer see Erik Peper’s Health Computer Email Tips. Enjoy the following superb video cartoons uploaded by Stephen Walker on YouTube that summarize the basic guidelines for computer, laptop and cell phones use at work, home, or while traveling.
Adult or Child Laptop Use at Home, Work or Classroom
Healthy use of laptops anywhere.
Mobile or Smart Phone Use while Driving, Traveling or on the Move.
Evoking your healing potential: You are your placebo
Posted: August 31, 2014 Filed under: Uncategorized | Tags: health, hope, illness beliefs, mind-body, nocebo, placebo 3 CommentsBe careful what you think. You may get what you wish.
The power of the placebo and nocebo are remarkable and often overlooked in medicine. With a placebo, severe chest pain disappears with mock surgery, Parkinson’s tremors stop, knee pain is eliminated following mock arthroscopic knee surgery and even of lymphosarcoma can be affected (Beecher, 1961; Benedeteti, 2007; Moseley et al, 2002; Kirkley et al., 2008; Klopfer, 1957; Moerman & Jonas, 2002). On the other hand, nocebo can increase pain, accelerate cancer growth, and cause death (Cannon, 1942; Klopfer, 1957; Benedeteti, 2007). These are demonstrations of the self-healing and non-healing potential intrinsic within each of us.
The placebo response (from Latin, “I shall please”) is the beneficial physiological or psychological effect that results from the administration of an otherwise ineffective or inert substance, procedure, instruction. and/or environment. An example of placebo on neuron activity is demonstrated with a patient who has Parkinson’s disease (see figure 1).
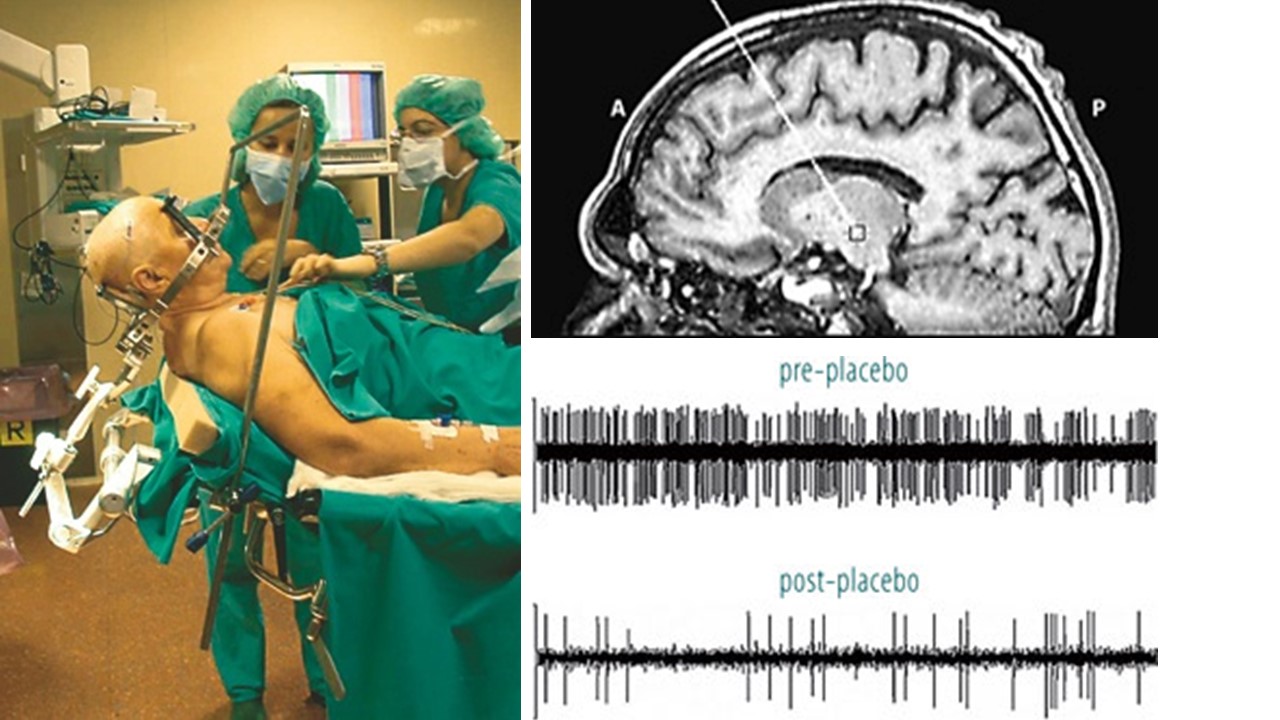 Figure 1. Recording the activity of single neurons from the brain of an awake patient suffering from Parkinson’s disease. Both the recording apparatus (a) and the electrode track (b) can be seen. In (c), the activity of a single neuron in the subthalamic nucleus can be seen before and after placebo administration (reproduced from: Benedeteti, F.(2007). The Placebo and Nocebo Effect: How the Therapist’s Words Act on the Patient’s Brain. Karger Gazette, 69).
Figure 1. Recording the activity of single neurons from the brain of an awake patient suffering from Parkinson’s disease. Both the recording apparatus (a) and the electrode track (b) can be seen. In (c), the activity of a single neuron in the subthalamic nucleus can be seen before and after placebo administration (reproduced from: Benedeteti, F.(2007). The Placebo and Nocebo Effect: How the Therapist’s Words Act on the Patient’s Brain. Karger Gazette, 69).
The nocebo response (from Latin, “I will harm”) may evoke the non-healing process and reactivate symptom/disease producing process and experiences. The nocebo response can be evoked by ineffective or inert substances, procedures, instructions, and internal and external environments which by themselves have no known effects.
The placebo/nocebo response is modulated by our covert cultural, familial and personal beliefs, limitations and expectations. The placebo/nocebo effects are the actual demonstrations that the limits of our beliefs are the limits of our possibilities. This process is well described in the recent published book, You are the Placebo: Making Your Mind Matter, by Chiropractor Joe Dispenza.
 Dr. Dispenza describes the classic studies of placebo, mental processes and possible mechanisms by which placebo effects occur and disappears and how our thoughts and expectancies create our reality. The placebo transforms the inner beliefs and give the person the experience of improved health which transforms beliefs. In many cases we can experience improvement but are pulled back into our previous beliefs and self-images of illness by inner and outer cues which are associated with disease process.
Dr. Dispenza describes the classic studies of placebo, mental processes and possible mechanisms by which placebo effects occur and disappears and how our thoughts and expectancies create our reality. The placebo transforms the inner beliefs and give the person the experience of improved health which transforms beliefs. In many cases we can experience improvement but are pulled back into our previous beliefs and self-images of illness by inner and outer cues which are associated with disease process.
The book describes of the covert conditioning process by which we return to our old self and may maintain illness. It is challenging to maintain new beliefs and act/think in new patterns. The internal mental chatter and doubts flood our awareness. Even the question, “How long will the improvement last?” re-evokes the associative mental conditioned disease patterns. If it is possible to interrupt and transform our thoughts moment by moment, minute by minute, hour by hour, day by day and not just for 15 minutes of practice, remarkable changes are sometimes possible. Every thought that triggers an association of the illness state needs to be interrupted and redirected. When patients somehow transform their thoughts, it may result in reversing and eliminating illnesses such as polyostotic fibrous dysphasia, Hashimot’sthyroiditis or chronic lympocytic thyroiditis, and secondary progressive multiple sclerosis.
I highly recommend this book for its outstanding description of placebo/nocebo and cognitive a model of the conditioning processes that underlie it. The book offers hope and inspiration for many patients who accept “what is/was” and are open to the present and future possibilities without judgement.
The book’s cases show that it is possible to reverse chronic “incurable illnesses.” Patients and health care providers should read the book–it provides hope, empowerment, and possibility. It is an antidote to the feeling that there is nothing one can do except to live with the illness. Medicine needs to explore and study the unusual patient who has reversed the disease process and ask, “How can we understand this process and teach it to other patients.”
The major limitation of the book is the absence of data; namely, what percentage of the patients/participants who have practiced Dispenza’s techniques have actually benefited and transformed their illness? The book would be more useful if it included both successful and the many unsuccessful cases. This would help patients who do the practices and do not improve. These patients sometimes blame themselves and failed at their self-healing—a process that increases depression and hopelessness. We need to realize that many factors affecting our health and illness are beyond our control.
Although I agree with Dr. Dspenza’s basic premise that our beliefs, acceptance of what is and being open to the present and future supports healing. This perspective is only part of the whole picture. Health and illness are multi-factorial and many factors are not within our control.
Read the book and skip chapter 8, The Quantum Mind. This chapter attempts to describe the physics of the healing process using quantum physics. As I did not understand quantum physics and quantum mind, I asked my colleague, James Johnston, PhD, who is an expert in quantum physics, to read it for accuracy. He confirmed my gut reaction when he said, “the quantum physics description of how energy changes is pseudo science, involving an incomplete understanding of quantum theory.”
Beecher, H.K. (1961). Surgery as Placebo. JAMA, 176(13), 1102-1107.
Cannon, W. B. (1942). “Voodoo” death. American Anthropologist, 44(2), 169-181.
Dispenza, J. (2014). You are the Placebo: Making Your Mind Matter. Hay House, Inc.
What to eat? Low fat foods, high fat foods…..?
Posted: July 12, 2014 Filed under: Evolutionary perspective, Nutrition/diet, Uncategorized | Tags: cancer, diet, evolution, health, heart disease, vitamins 4 Comments
Meat for sale (tongue and liver) at a traditional market (photo by Erik Peper).
Should I eat vegetables or meats? Should it be steaks or organ meats such as liver, heart, sweet breads? What foods contributes most to heart disease or cancer? Should I change my diet or take medications to lower my cholesterol?
Despite the many years of research the data is not clear. Many public health dietary guidelines and recommendations were based upon flawed research, researchers’ bias and promoted by agribusiness. Starting in the 1950s there has been a significant change in the dietary habits from eating animal fats to plant based oils and fats. It is so much cheaper to produce plant based polyunsaturated salad or cooking oils (e.g. Wesson and Mazola) and hydrogenated hardened oils (e.g. margarine and Crisco) than animal fats (e.g., butter, beef tallow, and lard). Despite the many claims that lowering animal fat intake would reduce heart disease and possibly cancer, the claims are not supported by research data. It is true that consuming liquid plant based oils lowers the cholesterol, but with the possible exception of olive oil, polyunsaturated oils are associated with an increased cancer and death rates in large population studies (Multiple Risk Factor Intervention Trial Research Group,1982; Shaten, 1997).
 We assume that lowering cholesterol is healthy; however, it is usually a surrogate marker representing a hypothesized improvement in health. A short term apparent reduction in cholesterol levels or other illness markers may mask the long term harm. Only long term outcome studies which measure the total death rate– not just from one disease being studied but from all causes of death–provides the objective results. When looking at the results over a longer time period, there appears to be no correlation between fat intake and heart disease. In fact lowering fat intake seems to be associated with poorer long term health as described in the outstanding book, The Big Fat Surprise–Why Butter, Meat & Cheese Belong in a Healthy Diet, by the science writer, Nina Teichol. Her superb investigative reporting describes in detail the flawed and biased research that underpinned the United States Department of Agriculture (USDA) and the American Heart Association (AHA) recommendations to reduce animal fats and use more plant based oils.
We assume that lowering cholesterol is healthy; however, it is usually a surrogate marker representing a hypothesized improvement in health. A short term apparent reduction in cholesterol levels or other illness markers may mask the long term harm. Only long term outcome studies which measure the total death rate– not just from one disease being studied but from all causes of death–provides the objective results. When looking at the results over a longer time period, there appears to be no correlation between fat intake and heart disease. In fact lowering fat intake seems to be associated with poorer long term health as described in the outstanding book, The Big Fat Surprise–Why Butter, Meat & Cheese Belong in a Healthy Diet, by the science writer, Nina Teichol. Her superb investigative reporting describes in detail the flawed and biased research that underpinned the United States Department of Agriculture (USDA) and the American Heart Association (AHA) recommendations to reduce animal fats and use more plant based oils.
What should I eat now?
Diet recommendations used to be simple: Reduce animal fat intake and eat more plants. Now, there are no simple recommendations because they may depend upon your genetics (e.g., digestion of milk depends whether you are lactose tolerant or intolerant), your epigenetics (e.g., maternal malnutrition during your embryological development is a major risk for developing heart disease in later life), your physical and social activities (e.g., exercise reduces the risk for many diseases), and environment. The recent popularity of the hunter and gatherer diet, often known as the paleo diet, is challenging–it may depends on your ancestors. What hunter and gatherers ate depended upon geography and availability of food sources. The Inuit’s diet in the Arctic consisted of 90% meat/fish diet while the !Kung Bushman’ diet from the Kalahari desert in Africa consisted of less than a 15% meat/fish diet as shown in Figure 1.

Figure 1. The food content of hunter gatherers varied highly depending on geography. From: Jabr, F. (2013). How to Really Eat Like a Hunter-Gatherer: Why the Paleo Diet Is Half-Baked. Scientific American, June 3.
Use common sense to make food choices.
- Eat only those foods which in the course of evolution have been identified as foods. This means eating a variety of plants based foods (fruits, tubers, leaves, stems, nuts, etc.) and more organ meats. Ask yourself what foods did your forefathers/mothers ate that supported survival and reproductive success. Carnivores usually ate the internal organs first and often would leave the muscles for scavengers.
- Eat like your great, great grandparents. They were not yet brainwashed by the profit incentives of agribusiness and pharmaceutical industry. For more information, read the outstanding books by Michael Pollan, The Omnivore’s Dilemma: A Natural History of Four Meals and In Defense of Food: An Eater’s Manifesto.
- If possible eat only organically grown/raised foods. Non organic foods usually contain low levels of pesticides, insecticides, antibiotics and hormones which increases the risk of cancer (Reuben, 2010). They may also also contain fewer nutrients such as essential minerals, vitamins, and antioxidants (Barański et al, 2014). The beneficial effects of organic foods have been challenging to demonstrate because it may take many years to show a difference. Preliminary data strongly suggests that organic foods as compared to non organic foods increases longevity, improves fertility and enhances survival during starvation (Chhabra, Kolli, & Bauer, 2013). For more information, see my blog, Live longer, enhance fertility and increase stress resistance: Eat Organic foods.
- Adapt the precautionary principle and assume that any new and artificially produced additives or chemically processed foods–most of the foods in boxes and cans in the central section of the supermarket–contain novel materials which have not been part of our historical dietary experience. These foods may be harmful over the long term and our bodies not yet know how to appropriately digest such foods such as trans fats (Kummerow, 2009).
- Be doubtful of dietary recommendations especially if you know of counter examples and exceptions. For example, the low fat diet recommendations could not explain the French or Swiss paradox (high butter and cheese intake and low heart disease rates). If examples exist, the popular dogma is incomplete or possibly wrong. Be skeptical about any health food claims. Ask who has funded the research, who decides whether a food can have a label that states “it is heart health” and can prevent a disease, and who would benefit if more of this food is sold.
My final comments on nutrition (source unknown).
- The Japanese eat very little fat and suffer fewer heart attacks than us.
- The Mexicans eat a lot of fat and suffer fewer heart attacks than us.
- The French eat lots of butter and drink alcohol and suffer fewer heart attacks than us.
- The Chinese drink very little red wine and suffer fewer heart attacks than us.
- The Italians drink a lot of red wine and suffer fewer heart attacks than us.
- The Germans drink a lot of beer and eat lots of sausages and fats and suffer fewer heart attacks than us.
Conclusion
Eat and drink what you like especially if you enjoy it with company…speaking English is apparently what kills you!
References:
Jabr, F. (2013). How to Really Eat Like a Hunter-Gatherer: Why the Paleo Diet Is Half-Baked. Scientific American, June 3.http://www.scientificamerican.com/article/why-paleo-diet-half-baked-how-hunter-gatherer-really-eat/
Kummerow, F. A. (2009). The negative effects of hydrogenated trans fats and what to do about them. Atherosclerosis, 205(2), 458-465.http://www.atherosclerosis-journal.com/article/S0021-9150%2809%2900208-1/abstract
Multiple Risk Factor Intervention Trial Research Group. (1982). Multiple risk factor intervention trial. JAMA: The Journal of the American Medical Association, 248(12), 1465-1477. http://jama.jamanetwork.com/article.aspx?articleid=377969
Pollan, M. (2006). The Omnivore’s Dilemma: A Natural History of Four Meals. New York: Penguin Press. ISBN: 1594200823
Pollan, M. (2009). In Defense of Food: An Eater’s Manifesto. New York: Penguin Press. ISBN: 978-0143114963
Reuben, S. H. (2010). Reducing environmental cancer risk: what we can do now. DIANE Publishing. http://deainfo.nci.nih.gov/advisory/pcp/annualReports/pcp08-09rpt/PCP_Report_08-09_508.pdf
Shaten, B. J., Kuller, L. H., Kjelsberg, M. O., Stamler, J., Ockene, J. K., Cutler, J. A., & Cohen, J. D. (1997). Lung cancer mortality after 16 years in MRFIT participants in intervention and usual-care groups. Annals of epidemiology, 7(2), 125-136. http://www.annalsofepidemiology.org/article/S1047-2797%2896%2900123-8/abstract
Teicholz, N. (2014). The big fat surprise-Why butter, meat & cheese belong in a healthy diet. New York: Simon & Schuster. ISBM 978-1-4516-2442-7 http://www.thebigfatsurprise.com/
Look up! Be aware and be open new possibilities
Posted: May 4, 2014 Filed under: Uncategorized | Tags: anxiety, cell phones, health, loneliness 2 CommentsHow is it possible that one is lonely while being connected to hundreds of Facebook friends, networked with even more LinkiedIn colleagues, and continuously sending and receiving Tweets and texts? Are we so captured by the digital devices that we do not notice the actual reality around us? Watch Gary Turk’s remarkable video and then remember to look up and connect with others.
Don’t poison yourself: Avoid foods with high pesticide residues
Posted: May 1, 2014 Filed under: Nutrition/diet, Uncategorized | Tags: diet, health, pesticides Leave a commentIs it worth to pay $3.49 for the organic strawberries while the non-organics are a bargain at $2.49?
Are there foods I should avoid because they have high pesticide residues?
The United States Department of Agriculture (USDA) and the United States Environmental Protection Agency (EPA) state that pesticide residues left in or on food are safe and non-toxic and have no health consequences. I have my doubts! Human beings accumulate pesticides just like tuna fish accumulates mercury—frequent ingesting of very low levels of pesticides residue may result in long term harmful effects and these long term risks have not been assessed. Most pesticides are toxic chemicals and were developed to kill agricultural pests — living organisms. The actual risk for chronic low level exposure is probably unknown; since, the EPA pesticide residue limits are a political compromise between scientific findings and lobbying from agricultural and chemical industries (Portney, 1992).
Organic diets expose consumers to fewer pesticides associated with human disease (Forman et al, 2012). In addition, preliminary studies have shown that GMO foods such as soy, potatoes, bananas and raisins reduces longevity, fertility and starvation tolerance in fruit flies (Chhabra et al, 2013)
Adopt the precautionary principle. As much as possible avoid the following foods that have high levels of residual pesticides as identified by the Environmental Working Group in their 2014 report.
Apples
Strawberries
Grapes
Celery
Peaches
Spinach
Sweet bell peppers
Nectarines-imported
Cucumbers
Cherry tomatoes
Snap peas-imported
Potatoes
Hot peppers
Blueberries-domestic
Lettuce
Kale/collard greens
For more details, see the Environmental Working Group report for the rankings of 48 foods listed from worst to best.
https://www.youtube.com/watch?feature=player_embedded&v=BfNQGd9BTK0
References:
Chhabra R, Kolli S, Bauer JH (2013) Organically Grown Food Provides Health Benefits to Drosophila melanogaster. PLoS ONE 8(1): e52988. doi:10.1371/journal.pone.0052988 http://www.plosone.org/article/info:doi%2F10.1371%2Fjournal.pone.0052988
Portney, P. R. (1992). The determinants of pesticide regulation: A statistical analysis of EPA decision making. The Journal of Political Economy, 100(1), 175-197.
Concered about food and health?
Posted: April 19, 2014 Filed under: Nutrition/diet, Uncategorized | Tags: agriculture, cooking, diabetes, diet, food, health Leave a commentIf you are concerned about food and health, watch Michael Pollan’s presentation, How Cooking Can Change Your Life. It is pragmatic and full of wisdom.
From Wisdom to Alzheimer’s: Are we poisoning ourselves with affluent malnutrition and sedentary life style?
Posted: December 14, 2013 Filed under: Exercise/movement, Nutrition/diet, self-healing, Uncategorized | Tags: Alzheimer, diet, evolution, exercise, health Leave a commentWise elders, grand parents or statesmen have been the traditional roles for aging adults. Older people were revered as the repository and sources of wisdom in many traditional cultures. Presently the development of aging into wisdom is being overshadowed by the specter of Alzheimer’s disease. Wisdom transforming into Alzheimer’s disease does not compute. How come that in slightly more than a century after it was first described by the neuropathologist Alois Alzheimer in 1906, the fear of contracting and possible having Alzheimer’s disease with the concurrent loss of cognitive and body functions is becoming a possibility? How could this have occurred?
Today more people are living to older ages; however, in traditional cultures some people also lived to very old age (the major increase in present day longevity is due to the elimination of infant and maternal mortality and medical treatment to survive trauma).
Is it possible that the prevention of Alzheimer’s will not be found in pharmaceutical treatment but in promoting organic food diet and movement? The research data is starting to find that our life style patterns are risk factors for Alzheimer’s. Changing lifestyle factors is a more promising treatment approach than drugs. A significant risk factor may be the confluence of a sedentary lifestyle and affluent malnutrition. Researchers are even reporting that the built up of the beta amyloid plaques in brains of people with Alzheimer’s disease is not the result of aging but the body’s attempt to cope with the influx of environmental and dietary poisons or decreases in essential foods or body activities.
Risk: Sedentary lifestyle-Too little exercise
Over the last hundred years–and rapidly accelerated in the last 30 years–we have transformed work into sitting. By sitting in front of a computer screen, we have created a new disease: Immobilization Syndrome. Lack of exercise is recognize as a major factor in numerous illnesses such as cardiovascular disease, obesity, and diabetes. Movement in many different forms reduces the risk of illness. Older people who exercise have a significant reduction in the risk of developing Alzheimer’s (Larson, 2006; Radak et al, 2010).
Regular movement lowers the risk. Even though there is overwhelming scientific evidence that movement and exercise are required for health, there is a disconnect with the medical and educational practices. Insurances will pay for medical treatment; however, they usually will not pay for prevention or exercise. At the same time physical education in schools is reduced or eliminated to reduce the risk of litigation (an injured child on the playground could sue the school). Children now spend most of their time in front of a screen while exercising their thumb and index fingers instead of playing and moving outdoors.
Risk: Affluent malnutrition-too much sugar and simple carbohydrates
Affluent malnutrition appears to be another risk factor. Recent findings suggests that the beta amyloids plagues, as the marker for Alzheimer’s in the brain, may be a protective response to the modulating insulin levels triggered by affluent malnutrition and sedentary life style. This disease has been labeled as type 3 diabetes by Associate Professor Suzanne de la Monte at Brown University (Steen et al, 2005). Namely, the disease occurs as the brain tissue becomes resistant to insulin.
Rats that are fed high-fructose corn syrup laced water experienced learning and memory problems in less than 6 weeks and became less responsive to insulin. At the same time if the animals were given omega 3 fatty acids, they appear to escape the cognitive decline. In other research rats developed Alzheimer like brain changes and became demented when Suzanne de la Monte interfered with how the rats brains respond to insulin (Trivedi, 2012).
Alois Alzheimer first described these abnormal protein structure in the brains a little more than a hundred years ago. At that time the European diet had increased sugar intake as shown in figure 1. While more recently there has been a significant increase in high fructose corn syrup as shown in figure 2.

Figure 1. Radical increase in sugar consumption in the last 200 years. From: http://blog.zestos.co.nz/2010/09/sugar-consumption-been-high-before.html

Figure 2. Increase in the type of sugar consumption in the last thirty years. From: http://blog.zestos.co.nz/2010/09/sugar-consumption-been-high-before.html
We are now becoming concerned with the Alzheimer’s disease as an upcoming epidemic. It cannot be just sugar; since, its consumption has been high since the beginning of the 20th century. A possible contributor could be the high-fructose corn syrup; however, it is most likely the interaction between reduced exercise and sugar.
Sugar set the stage for pathogenesis to occur in the brain and the absence of movement/exercise promotes and supports the pathogenesis. People continue to decrease movement: from walking or riding horses to sitting cars or standing on escalators and elevators; from doing physical housework to automated washing machines, driers and dishwashers; from preparing foods from raw materials to prepackaged foods; from filing and typing to computer work; from playing family games to watching TV and searching the net; from face to face communication to texting; etc.
We have separated from our biological evolutionary heritage. I am not surprised that Alzheimer’s disease and immobility and sugar are linked. Adopt the precautionary principle and assume that sugar and high-fructose corn syrup in conjunction with reduced movement (immobilization syndrome) is harmful.
As a reader, you will probably have to wait another 20 years before these findings have been scientifically proven against the overt and covert lobbying efforts of agribusiness and pharmaceutical industry. Remember it took 30 years to demonstrate that smoking was harmful. Begin to move and eat in concert with your evolutionary background (See Part III Self-care in Gorter and Peper, 2011).
Begin now!
Eat food not sugars! Eat the foods great grandparents would recognize as food as Michael Pollan (2009) describe in his superb book, In Defense of Food: An Eater’s Manifesto. Eat foods that have not been processed or adulterated by additives. Take charge by eating brain supporting foods such as organic vegetables, roots, fruits, nuts, fish, some organ meat, and eliminate all those sugary, fatty processed highly advertised fast foods.
Move and exercise! Get up and move every hour. Walk up the stairs instead of the escalator. Meet new people and move by going hiking, dancing, Tai Chi or yoga classes or volunteer by helping others.
References
Gorter, R. & Peper, E. (2011). Fighting Cancer-A Non Toxic Approach to Treatment. Berkeley: North Atlantic.
Larson, E.G., Wang, L., Bowen, J.D., McCormick, W. C., Teri, L., Crane, P., & Kukull, W. (2006). Exercise Is Associated with Reduced Risk for Incident Dementia among Persons 65 Years of Age and Older. Ann Intern Med, 144(2), 73-81.
Pollan, M. (2009). In Defense of Food: An Eater’s Manifesto. New York: Penguin Books.
Radak, Z., Hart. N., Sarga, L., Koltai, E., Atalay, M., Ohno, H., & Boldogh, I. (2010). Journal of Alzheimer’s Disease, 20(3), 777-83.
Steen, E., Terry, B.M. Rivera, E.J., Cannon, J.L., Neely, T.R., Tavares, R., Xu, X. J., Wands, J.R., & de al Monte, S. M. (2005). Impaired insulin and insulin-like growth factor expression and signaling mechanisms in Alzheimer’s disease-is this type 3 diabetes? Journal of Alzheimer’s Disease, 7(1), 53-80.
Trivedi, B. (2012). Eat your way to dementia. New Scientist, 215(2880), 32-37.
