Are you sure what you saw happened?
Posted: April 4, 2015 Filed under: attention, behavior, CBT, cognitive behavior therapy, mindfulness, Uncategorized, vision | Tags: awareness, selective attention, situational awareness 1 CommentWe are often 100 percent sure that what we saw or heard really happened even though another person has a different opinion. The more we are captured or focused on a task the more we may miss what has occurred. Selective attention is the basis of magic tricks by which attention is misdirected so that you do not see what is occurring. This process may affect our daily perceptions and judgements.
Be open to the possibility that your conclusions may be based upon incomplete information or selective attention. For example, when a person has had a car crash and experiences back and neck pain, he is 100 per cent sure that the pain was caused by the car accident. A more healing attitude is to assume that there could be other factors involved. Possibly, the person had a fight with their partner and was still angry and thinking about it when he was hit. The accident anchored the anger and healing may need to include letting go of the anger. Thus, whenever you are 100 per cent sure of your point of view, be open to other possibilities. Observe the power of selective attention in the following video clips.
Interrupt Chained Behaviors: Overcome Smoking, Eczema, and Hair Pulling
Posted: March 7, 2015 Filed under: self-healing, stress management, Uncategorized | Tags: chained behavior, eczema, hair pulling, healing, self-monitoring, smoking cessation, stress management, trichotillomania 7 Comments“I am proud to label myself a nonsmoker… diligently performing practices has profoundly helped me eliminate my troublesome craving…The conscious efforts I have made over the past month have helped me regain control of my life.” –L. F., a college student who became a non-smoker after smoking up to two packs a day since age 11. At 18 month follow-up L. F. is still a nonsmoker.
“I have been struggling with eczema for most of my life and until I began this course, I was feeling very hopeless in managing this condition without the use of costly, and potentially dangerous drugs. My self-healing project proved to be empirically successful. My eczema shrunk in size from 72 mm in length and 63 mm in width as measured at baseline to 0 mm in length and 0 mm in width by the final day of this project.” –L. C., a college student who experienced recurring scaly skin patches since childhood.
In our recent published paper, Transforming chained behaviors: Case studies of overcoming smoking, eczema and hair pulling (trichotillomania), we describe an approach by which students learn self-healing techniques which they practice as part of a semester long class project. After four weeks of of self-healing practices many of the students report significant decrease in symptoms and improvement of health as shown in Figure 1. Their success includes smoking cessation, eliminating hair pulling and eczema disappearing.
 Figure 1. Students’ self-rating of success in achieving health benefits after four weeks of practice.
Figure 1. Students’ self-rating of success in achieving health benefits after four weeks of practice.
One component of the self-healing process is interrupting chained behavior. We react automatically and respond instantly with sadness, anger, neck and shoulders tension, eating too much, veg’ing out watching videos, or playing mindless digital games. After a time, we may notice that we are smoking more, experiencing an upset stomach, back pain, headaches, high blood pressure, or even more skin eruptions. The first step is to sense the initial reaction that leads to the symptom development. Then, the person performs an alternative health promoting behavior and interrupts the chained behavior that triggers symptoms as shown in Figure 2.
 Figure 2. Interrupting and transforming the chained behavior. The moment person become aware of the trigger or behavior that is chained to the development of the symptom, he/she interrupts and performs an active new health promoting behavior as illustrated by the dashed lines.
Figure 2. Interrupting and transforming the chained behavior. The moment person become aware of the trigger or behavior that is chained to the development of the symptom, he/she interrupts and performs an active new health promoting behavior as illustrated by the dashed lines.
Overtime these automatic patterns may contribute to the development of autoimmune diseases, increased vulnerability to infections or other chronic diseases. The challenge is to develop an awareness to recognize and interrupt the beginning of the ‘chain of behavior.’ The instant you become aware of the first reaction, do something different, such as,
- Shift your focus of attention to something joyful
- Chang your body position and smile while thinking, This will also pass.
- Practice a quick relaxation technique.
- Imagine a positive self-healing process.
The longer the person waits to interrupt the chain, the more difficult it is to redirect the chained behavior. Awareness and immediate interruption appears to be major factors in achieving success. It means practicing the interruption and new behavior all day long. This is different from from practicing a skill for twenty minutes a day and the rest of the time performing the old dysfunctional behavior.
Mastery of this process consists of three steps:
- Becoming aware of what is happening when the chain reactions.
- Learn a more functional alternative health behavior such as breathing, relaxing, focusing on empowering thought, eating other foods.
- Substitute the alternative behavior the moment you become aware of the triggered dysfunctional behavior.
After having integrated this into daily life, many students report experiencing a significant reduction and even elimination of symptoms and behaviors.
“I will continue to do the practices outlined not only to overcome trichotillomania but also to control my anxiety and, therefore, lead a less stressed and happier life. Knowing I have the power to heal myself is such an inspiring feeling, a feeling that can’t adequately be put into words.” –G. M., a 32 year old student with trichotillomania, who reduced her hair pulling, anxiety, and stress
“I have gained much wisdom from this project…I am ultimately responsible for my own health and well-being…I feel empowered, optimistic, and appreciative of every moment.” –L. C., a college student who experienced recurring scaly skin patches since childhood)
For background, specific techniques and successful case reports, read our published paper, Peper, E., Lin, I-M, Harvey, R., Gilbert, M., Gubbala, P., Ratkovich, A., & Fletcher, F. (2014). Transforming chained behaviors: Case studies of overcoming smoking, eczema and hair pulling (trichotillomania). Biofeedback, 42(4), 154-160.
What do numbers mean? How much does Walmart’s wage raise affect profits?
Posted: February 22, 2015 Filed under: Uncategorized | Tags: economics, salaries, stress 1 Comment Walmart created news when it announced that it will be paying its 500,000 employees more than the minimum wage. The largest increase would be an increase of the entry-level wage from the US minimum $7.25 to $9 an hour; howver, the overall increase in minimal. As Jody Knauss and Mary Bottari point out, The company forecasts the average hourly wage for full-time workers to rise 15 cents an hour, from $12.85 to $13.00, while the average for part-timers will bump up from $9.48 to $10.00 per hour. This will still still leave most of its workers beneath the poverty level and relying on food stamps to make ends meet.
Walmart created news when it announced that it will be paying its 500,000 employees more than the minimum wage. The largest increase would be an increase of the entry-level wage from the US minimum $7.25 to $9 an hour; howver, the overall increase in minimal. As Jody Knauss and Mary Bottari point out, The company forecasts the average hourly wage for full-time workers to rise 15 cents an hour, from $12.85 to $13.00, while the average for part-timers will bump up from $9.48 to $10.00 per hour. This will still still leave most of its workers beneath the poverty level and relying on food stamps to make ends meet.
The actual cost of this wage raise for Walmart is one billion dollars. This seems impressive; however, this number is not meaningful without knowing the financial state of the company. The company’s estimated profit for 2014 was $16.36 billion on annual sales of $485 Billion. For more details see the Walmart’s financial summary.
The one billion dollars to increase the salaries is an impressive sound bite, but it only a 6.1% decreases the company’s profits. It will still leave more than 15 billion dollar in profit and more than 150 billion dollar wealth for its owners. Given the profits and wealth, Walmart should be ashamed to keep its employees in poverty. It should offer its employees an actually living wage of at least $15 per hour.
Reduce hot flashes and premenstrual symptoms with breathing
Posted: February 18, 2015 Filed under: Breathing/respiration, Pain/discomfort, self-healing, stress management, Uncategorized | Tags: biofeedback, Breathing, diaphragmatic breathing, heart rate variability, hormone replacement therapy, hot flashes, HRT, Menopause, respiration, sighs, stress, sympathetic activity 6 CommentsAfter the first week to my astonishment, I have fewer hot flashes and they bother me less. Each time I feel the warmth coming, I breathe out slowly and gently. To my surprise they are less intense and are much less frequent. I keep breathing slowly throughout the day. This is quite a surprise because I was referred for biofeedback training because of headaches that occurred after getting a large electrical shock. After 5 sessions my headaches have decreased and I can control them, and my hot flashes have decreased from 3-4 per day to 1-2 per week. -50 year old client
After students in my Holistic Health class at San Francisco State University practiced slower diaphragmatic breathing and begun to change their dysfunctional shallow breathing, gasping, sighing, and breath holding to diaphragmatic breathing. A number of the older female students students reported that their hot flashes decreased. Some of the younger female students reported that their menstrual cramps and discomfort were reduced by 80 to 90% when they laid down and breathed slower and lower into their abdomen.
 The recent study in JAMA reported that many women continue to experience menopausal triggered hot flashes for up to 14 years. Although the article described the frequency and possible factors that were associated with the prolonged hot flashes, it did not offer helpful solutions.
The recent study in JAMA reported that many women continue to experience menopausal triggered hot flashes for up to 14 years. Although the article described the frequency and possible factors that were associated with the prolonged hot flashes, it did not offer helpful solutions.
Another understanding of the dynamics of hot flashes is that the decrease in estrogen accentuates the sympathetic/ parasympathetic imbalances that probably already existed. Then any increase in sympathetic activation can trigger a hot flash. In many cases the triggers are events and thoughts that trigger a stress response, emotional responses such as anger, anxiety, or worry, increase caffeine intake and especially shallow chest breathing punctuated with sighs. Approximately 80% of American women tend to breathe thoracically often punctuated with sighs and these women are more likely to experience hot flashes. On the other hand, the 20% of women who habitually breathe diaphragmatically tend to have fewer and less intense hot flashes and often go through menopause without any discomfort. In the superb study Drs. Freedman and Woodward (1992), taught women who experience hot flashes to breathe slowly and diaphragmatically which increased their heart rate variability as an indicator of sympathetic/parasympathetic balance and most importantly it reduced the the frequency and intensity of hot flashes by 50%.
Test the breathing connection if you experience hot flashes
Take a breath into your chest and rapidly exhale with a sigh. Repeat this quickly five times. In most cases, one minute later you will experience the beginning sensations of a hot flash. Similarly, when you practice slow diaphragmatic breathing throughout the day and interrupt every gasp, breath holding moment, sigh or shallow chest breathing with slower diaphragmatic breathing, you will experience a significant reduction in hot flashes.
Although this breathing approach has been well documented, many people are unaware of this simple behavioral approach unlike the common recommendation for the hormone replacement therapies (HRT) to ameliorate menopausal symptoms. This is not surprising since pharmaceutical companies spent nearly five billion dollars per year in direct to consumer advertising for drugs and very little money is spent on advertising behavioral treatments. There is no profit for pharmaceutical companies teaching effortless diaphragmatic breathing unlike prescribing HRTs. In addition, teaching and practicing diaphragmatic breathing takes skill training and practice time–time which is not reimbursable by third party payers.
For more information, research data and breathing skills to reduce hot flash intensity, see our article which is reprinted below.
Gibney, H.K. & Peper, E. (2003). Taking control: Strategies to reduce hot flashes and premenstrual mood swings. Biofeedback, 31(3), 20-24.
Taking control: Strategies to reduce hot flashes and premenstrual mood swings*
Erik Peper, Ph.D**., and Katherine H. Gibney
San Francisco State University
After the first week to my astonishment, I have fewer hot flashes and they bother me less. Each time I feel the warmth coming, I breathe out slowly and gently. To my surprise they are less intense and are much less frequent. I keep breathing slowly throughout the day. This is quite a surprise because I was referred for biofeedback training because of headaches that occurred after getting a large electrical shock. After 5 sessions my headaches have decreased and I can control them, and my hot flashes have decreased from 3-4 per day to 1-2 per week. -50 year old client
For the first time in years, I experienced control over my premenstrual mood swings. Each time I could feel myself reacting, I relaxed, did my autogenic training and breathing. I exhaled. It brought me back to center and calmness. -26 year old student
Abstract
Women have been troubled by hot flashes and premenstrual syndrome for ages. Hormone replacement therapy, historically the most common treatment for hot flashes, and other pharmacological approaches for pre-menstrual syndrome (PMS) appear now to be harmful and may not produce significant benefits. This paper reports on a model treatment approach based upon the early research of Freedman & Woodward to reduce hot flashes and PMS using biofeedback training of diaphragmatic breathing, relaxation, and respiratory sinus arrhythmia. Successful symptom reduction is contingent upon lowering sympathetic arousal utilizing slow breathing in response to stressors and somatic changes. We strongly recommend that effortless diaphragmatic breathing be taught as the first step to reduce hot flashes and PMS symptoms.
A long and uncomfortable history
Women have been troubled by hot flashes and premenstrual syndrome for ages. Hot flashes often result in red faces, sweating bodies, and noticeable and embarrassing discomfort. They come in the middle of meetings, in the middle of the night, and in the middle of romantic interludes. Premenstrual syndrome also arrives without notice, bringing such symptoms as severe mood swings, anger, crying, and depression.
Hormone replacement therapy (HRT) was the most common treatment for hot flashes for decades. However, recent randomized controlled trials show that the benefits of HRT are less than previously thought and the risks—especially of invasive breast cancer, coronary artery disease, dementia, stroke and venous thromboembolism—are greater (Humphries & Gill, 2003; Shumaker, et al, 2003; Wassertheil-Smoller, et al, 2003). In addition, there is no evidence of increased quality of life improvements (general health, vitality, mental health, depressive symptoms, or sexual satisfaction) as claimed for HRT (Hays et al, 2003).
“As a result of recent studies, we know that hormone therapy should not be used to prevent heart disease. These studies also report an increased risk of heart attack, stroke, breast cancer, blood clots, and dementia…” -Wyeth Pharmaceuticals (2003)
Because of the increased long-term risk and lack of benefit, many physicians are weaning women off HRT at a time when the largest population of maturing women in history (‘baby boomers’) is entering menopausal years. The desire to find a reliable remedy for hot flashes is on the front burner of many researchers’ minds, not to mention the minds of women suffering from these ‘uncontrollable’ power surges. Yet, many women are becoming increasingly leery of the view that menopause is an illness. There is a rising demand to find a natural remedy for this natural stage in women’s health and development.
For younger women a similar dilemma occurs when they seek treatment of discomfort associated with their menstrual cycle. Is premenstrual syndrome (PMS) just a natural variation in energy and mood levels? Or, are women expected to adapt to a masculine based environment that requires them to override the natural tendency to perform in rhythm with their own psychophysiological states? Instead of perceiving menstruation as a natural occurrence in which one has different moods and/or energy levels, women in our society are required to perform at the status quo, which may contribute to PMS. The feelings and mood changes are quickly labeled as pathology that can only be treated with medication.
Traditionally, premenstrual syndrome is treated with pharmaceuticals, such as birth control pills or Danazol. Although medications may alleviate some symptoms, many women experience unpleasant side effects, such as bloating or acne, and still experience a variety of PMS symptoms. Many cannot tolerate the medications. Thus, millions of women (and families) suffer monthly bouts of ‘uncontrollable’ PMS symptoms
For both hot flashes and PMS the biomedical model tends to frame the symptoms as a “structural biological problem.” Namely, the pathology occurs because the body is either lacking in, or has an excess of, some hormone. All that needs to be done is either augment or suppress hormones/symptoms with some form of drug. Recently, for example, medicine has turned to antidepressant medications to address menopausal hot flashes (Stearns, Beebe, Iyengar, & Dube, 2003).
The biomedical model, however, is only one perspective. The opposite perspective is that the dysfunction occurs because of how we use ourselves. Use in this sense means our thoughts, emotions and body patterns. As we use ourselves, we change our physiology and, thereby, may affect and slowly change the predisposing and maintaining factors that contribute to our dysfunction. By changing our use, we may reduce the constraints that limit the expression of the self-healing potential that is intrinsic in each person.
The intrinsic power of self-healing is easily observed when we cut our finger. Without the individual having to do anything, the small cut bleeds, clotting begin and tissue healing is activated. Obviously, we can interfere with the healing process, such as when we scrape the scab, rub dirt in the wound, reduce blood flow to the tissue or feel anxious or afraid. Conversely, cleaning the wound, increasing blood flow to the area, and feeling “safe” and relaxed can promote healing. Healing is a dynamic process in which both structure and use continuously affect each other. It is highly likely that menopausal hot flashes and PMS mood swings are equally an interaction of the biological structure (hormone levels) and the use factor (sympathetic/parasympathetic activation).
Uncontrollable or overly aroused?
Are the hot flashes and PMS mood swings really ‘uncontrollable?’ From a physiological perspective, hot flashes are increased by sympathetic arousal. When the sympathetic system is activated, whether by medication or by emotions, hot flashes increase and similarly, when sympathetic activity decreases hot flashes decrease. Equally, PMS, with its strong mood swings, is aggravated by sympathetic arousal. There are many self-management approaches that can be mastered to change and reduce sympathetic arousal, such as breathing, meditation, behavioral cognitive therapy, and relaxation.
Breathing patterns are closely associated with hot flashes. During sleep, a sigh generally occurs one minute before a hot flash as reported by Freedman and Woodward (1992). Women who habitually breathe thoracically (in the chest) report much more discomfort and hot flashes than women who habitually breathe diaphragmatically. Freedman, Woodward, Brown, Javaid, and Pandey (1995) and Freedman and Woodward (1992) found that hot flash rates during menopause decreased in women who practiced slower breathing for two weeks. In their studies, the control groups received alpha electroencephalographic feedback and did not benefit from a reduction of hot flashes. Those who received training in paced breathing reduced the frequency of their hot flashes by 50% when they practiced slower breathing. This data suggest that the slower breathing has a significant effect on the sympathetic and parasympathetic balance.
Women with PMS appear similarly able to reduce their discomfort. An early study utilizing Autogenic Training (AT) combined with an emphasis on warming the lower abdomen resulted in women noting improvement in dysfunctional bleeding (Luthe & Schultz, 1969, pp. 144-148). Using a similar approach, Mathew, Claghorn, Largen, and Dobbins (1979) and Dewit (1981) found that biofeedback temperature training was helpful in reducing PMS symptoms.. A later study by Goodale, Domar, and Benson (1990) found that women with severe PMS symptoms who practiced the relaxation response reported a 58% improvement in overall symptomatology as compared to a 27.2% improvement for the reading control group and a 17.0% improvement for the charting group.
Teaching control and achieving results
Teaching women to breathe effortlessly can lead to positive results and an enhanced sense of control. By effortless breathing, the authors refer to their approach to breath training, which involves a slow, comfortable respiration, larger volume of air exchange, and a reliance upon action of the muscles of the diaphragm rather than the chest (Peper, 1990). For more instructions see the recent blog, A breath of fresh air: Improve health with breathing.
Slowing breathing helps to limit the sighs common to rapid thoracic breathing—sighs that often precede menopausal hot flashes. Effortless breathing is associated with stress reduction—stress and mood swings are common concerns of women suffering from PMS. In a pilot study Bier, Kazarian, Peper, and Gibney (2003) at San Francisco State University (SFSU) observed that when the subject practiced diaphragmatic breathing throughout the month, combined with Autogenic Training, her premenstrual psychological symptoms (anger, depressed mood, crying) and premenstrual responses to stressors were significantly reduced as shown in Figure 1.
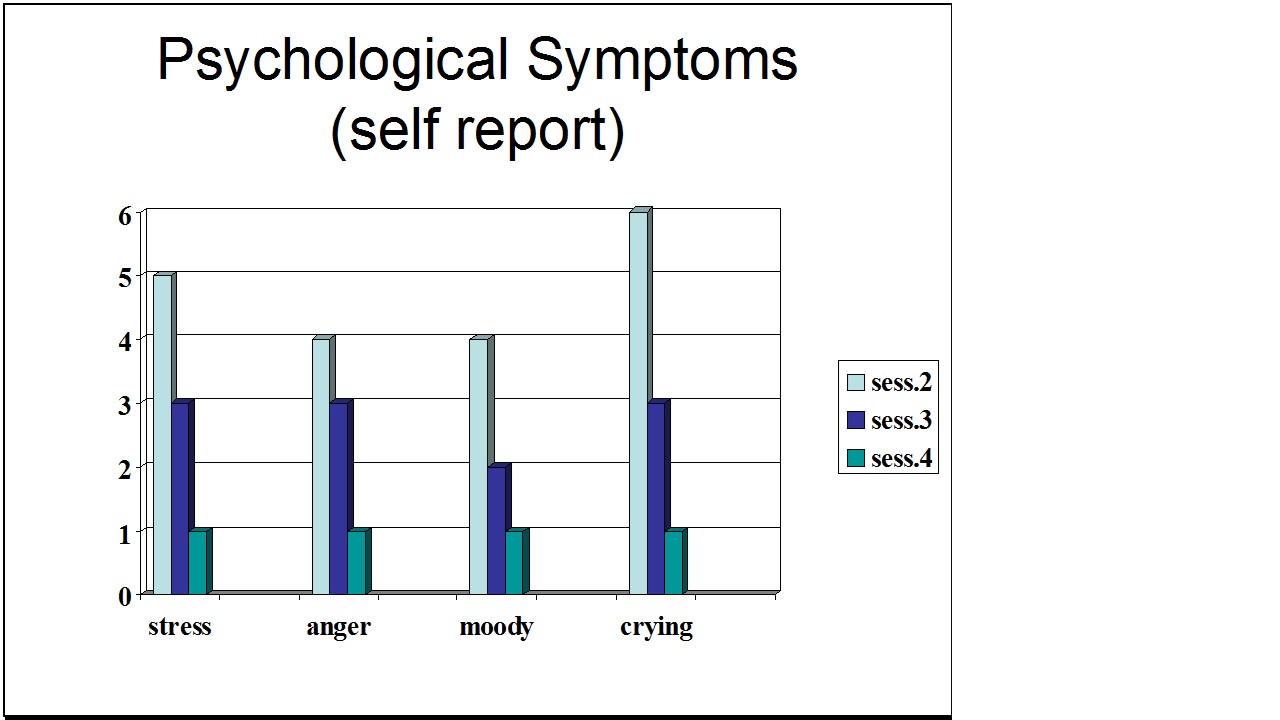
Figure 1. Student’s Individual Subjective Rating in Response to PMS Symptoms.
In another pilot study at SFSU, Frobish, Peper, and Gibney (2003) trained a volunteer who suffered from frequent hot flashes to breathe diaphragmatically. The training goals included modifying breathing patterns, producing a Respiratory Sinus Arrhythmia (RSA), and peripheral hand warming. RSA refers to a pattern of slow, regular breathing during which variations in heart rate enter into a synchrony with the respiration. Each inspiration is accompanied by an increase in heart rate, and each expiration is accompanied by a decrease in heart rate (with some phase differences depending on the rate of breathing). The presence of the RSA pattern is an indication of optimal balance between sympathetic and parasympathetic nervous activity.
During the 11-day study period, the subject charted the occurrence of hot flashes and noted a significant decrease by day 5. However, on the evening of day 7 she sprained her ankle and experienced a dramatic increase in hot flashes on day 8. Once the subject recognized her stress response, she focused more on breathing and was able to reduce the flashes as shown in Figure 2. 
Figure 2. Subjective rating of intensity, frequency and bothersomeness of hot flashes. The increase in hot flashes coincided with increased frustration about an ankle injury.
Our clinical experience confirms the SFSU pilot studies and the previously referenced research by Freedman and Woodward (1992) and Freedman et al. (1995). When arousal is lowered and breathing is effortless, women are better able to cope with stress and report a reduction in symptoms. Habitual rapid thoracic breathing tends to increase arousal while slower breathing, especially slower exhalation, tends to relax and reduce arousal. Learning and then applying effortless breathing reduces excessive sympathetic arousal. It also interrupts the cycle of cognitive activation, anxiety, and somatic arousal. The anticipation and frustration at having hot flashes becomes the cue to shift attention and “breathe slower and lower.” This process stops the cognitively mediated self-activation.
Successful self-regulation and the return to health begin with cognitive reframing: We are not only a genetic biological fixed (deficient) structure but also a dynamic changing system in which all parts (thoughts, emotions, behavior, diet, stress, and physiology) affect and are effected by each other. Within this dynamic changing system, there is an opportunity to implement and practice behaviors and life patterns that promote health.
Learning Diaphragmatic Breathing with and without Biofeedback
Although there are many strategies to modify respiration, biofeedback monitoring combined with respiration training is very useful as it provides real-time feedback. Chest and abdominal movement are recorded with strain gauges and heart rate can be monitored either by an electrocardiogram (EKG) or by a photoplethysmograph sensor on a finger or thumb. Peripheral temperature and electrodermal activity (EDA) biofeedback are also helpful in training. The training focuses on teaching effortless diaphragmatic breathing and encouraging the participant to practice many times during the day, especially when becoming aware of the first sensations of discomfort.
Learning and integrating effortless diaphragmatic breathing into daily life is one of the biofeedback strategies that has been successfully used as a primary or adjunctive/complementary tool for the reversal of disorders such as hypertension, migraine headaches, repetitive strain injury, pain, asthma and anxiety (Schwartz & Andrasik, 2003), as well as hot flashes and PMS.
The biofeedback monitoring provides the trainer with a valuable tool to:
- Observe & identify: Dysfunctional rapid thoracic breathing patterns, especially in response to stressors, are clearly displayed in real-time feedback.
- Demonstrate & train: The physiological feedback display helps the person see that she is breathing rapidly and shallowly in her chest with episodic sighs. Coaching with feedback helps her to change her breathing pattern to one that promotes a more balanced homeostasis.
- Motivate, persuade and change beliefs: The person observes her breathing patterns change concurrently with a felt shift in physiology, such as a decrease in irritability, or an increase in peripheral temperature, or a reduction in the incidence of hot flushes. Thus, she has a confirmation of the importance of breathing diaphragmatically.
In addition, we suggest exercises that integrate verbal and kinesthetic instructions, such as the following: “Exhale gently,” and “Breathe down your leg with a partner.”
Exhale Gently:
Imagine that you are holding a baby. Now with your shoulders relaxed, inhale gently so that your abdomen widens. Then as you exhale, purse your lips and very gently and softly blow over the baby’s hair. Allow your abdomen to narrow when exhaling. Blow so softly that the baby’s hair barely moves. At the same time, imagine that you can allow your breath to flow down and through your legs. Continue imagining that you are gently blowing on the baby’s hair while feeling your breath flowing down your legs. Keep blowing very softly and continuously.
Practice exhaling like this the moment that you feel any sensation associated with hot flashes or PMS symptoms. Smile sweetly as you exhale.
Breathe Down Your Legs with a Partner
Sit or lie comfortably with your feet a shoulder width apart. As you exhale softly whisper the sound “Haaaaa….” Or, very gently press your tongue to your pallet and exhale while making a very soft hissing sound.
Have your partner touch the side of your thighs. As you exhale have your partner stroke down your thighs to your feet and beyond, stroking in rhythm with your exhalation. Do not rush. Apply gentle pressure with the stroking. Do this for four or five breaths.
Now, continue breathing as you imagine your breath flowing through your legs and out your feet.
During the day remember the feeling of your breath flowing downward through your legs and out your feet as you exhale.
Learning Strategies in Biofeedback Assisted Breath Training
Common learning strategies that are associated with the more successful amelioration of hot flashes and PMS include:
- Master effortless diaphragmatic breathing, and concurrently increase respiratory sinus arrhythmia (RSA). Instead of breathing rapidly, such as at 18 breaths per minute, the person learns to breathe effortlessly and slowly (about 6 to 8 breaths per minute). This slower breathing and increased RSA is an indication of sympathetic-parasympathetic balance as shown in Figure 3.
- Practice slow effortless diaphragmatic breathing many times during the day and, especially in response to stressors.
- Use the physical or emotional sensations of a hot flash or mood alteration as the cue to exhale, let go of anxiety, breathe diaphragmatically and relax.
- Reframe thoughts by accepting the physiological processes of menstruation or menopause, and refocus the mind on positive thoughts, and breathing rhythmically.
- Change one’s lifestyle and allow personal schedules to flow in better balance with individual, dynamic energy levels.
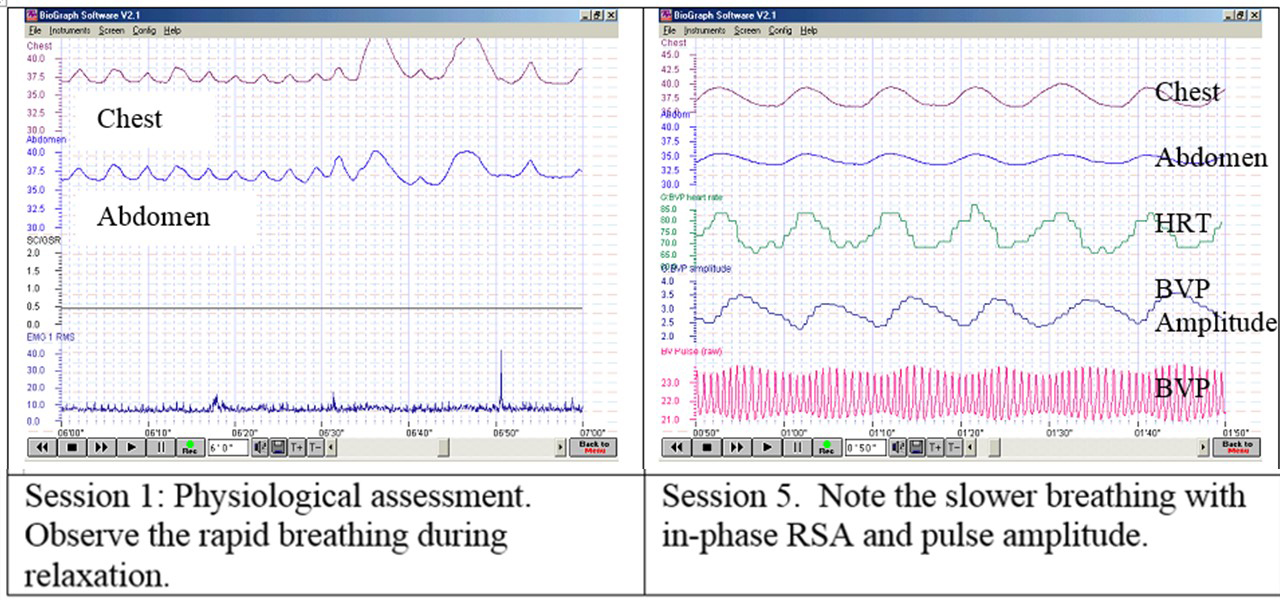 Figure 3. Physiological Recordings of a Participant with PMS. This subject learned effortless diaphragmatic breathing by the fifth session and experienced a significant decrease in symptoms.
Figure 3. Physiological Recordings of a Participant with PMS. This subject learned effortless diaphragmatic breathing by the fifth session and experienced a significant decrease in symptoms.
Generalizing skills and interrupting the pattern
The limits of self-regulation are unknown, often held back only by the practitioner’s and participant’s beliefs. Biofeedback is a powerful self-regulation tool for individuals to observe and modify their covert physiological reactions. Other skills that augment diaphragmatic breathing are Quieting Reflex (Stroebel, 1982), Autogenic Training (Schultz & Luthe, 1969), and mindfulness training (Kabat-Zinn, 1990). In all skill learning, generalization is a fundamental factor underlying successful training. Integrating the learned psychophysiological skills into daily life can significantly improve health—especially in anticipation of and response to stress. The anticipated stress can be a physical, cognitive or social trigger, or merely the felt onset of a symptom.
As the person learns and applies effortless breathing to daily activities, she becomes more aware of factors that affect her breathing. She also experiences an increased sense of control: She can now take action (a slow effortless breath) in moments when she previously felt powerless. The biofeedback-mastered skill interrupts the evoked frustrations and irritations associated with an embarrassing history of hot flashes or mood swings. Instead of continuing with the automatic self-talk, such as “Damn, I am getting hot, why doesn’t it just stop?” (language fueling sympathetic arousal), she can take a relaxing breath in response to the internal sensations, stop the escalating negative self-talk and allows more acceptance—a process reducing sympathetic arousal.
In summary, effortless breathing appears to be a non-invasive behavioral strategy to reduce hot flashes and PMS symptoms. Practicing effortless diaphragmatic breathing contributes to a sense of control, supports a healthier homeostasis, reduces symptoms, and avoids the negative drug side effects. We strongly recommend that effortless diaphragmatic breathing be taught as the first step to reduce hot flashes and PMS symptoms.
I feel so much cooler. I can’t believe that my hand temperature went up. I actually feel calmer and can’t even feel the threat of a hot flash. Maybe this breathing does work! –Menopausal patient after initial training in diaphragmatic breathing
References
Bier, M., Kazarian, D., Peper, E., & Gibney, K. (2003). Reducing the severity of PMS symptoms with diaphragmatic breathing, autogenic training and biofeedback. Unpublished report.
Freedman, R.R., & Woodward, S. (1992). Behavioral treatment of menopausal hot flushes: Evaluation by ambulatory monitoring. American Journal of Obstetrics and Gynecology, 167 (2), 436-439.
Freedman, R.R., Woodward, S., Brown, B., Javaid, J.I., & Pandey, G.N. (1995). Biochemical and thermoregulatory effects of behavioral treatment for menopausal hot flashes. Menopause: The Journal of the North American Menopause Society, 2 (4), 211-218.
Frobish,C., Peper, E. & Gibney, K. H. (2003). Menopausal Hot Flashes: A Self-Regulation Case Study. Poster presentation at the 35th Annual Meeting of the Association for Applied Psychophysiology and Biofeedback. Abstract in: Applied Psychophysiology and Biofeedback. 29 (4), 302.
Goodale, I.L., Domar, A.D., & Benson, H. (1990). Alleviation of Premenstrual Syndrome symptoms with the relaxation response. Obstetrics and Gynecological Journal, 75 (5), 649-55.
Hays, J., Ockene, J.K., Brunner, R.L., Kotchen, J.M., Manson, J.E., Patterson, R.E., Aragaki, A.K., Shumaker, S.A., Brzyski, R.G., LaCroix, A.Z., Granek, I.A, & Valanis, B.G., Women’s Health Initiative Investigators. (2003). Effects of estrogen plus progestin on health-related quality of life. New England Journal of Medicine, 348, 1839-1854.
Humphries, K.H.., & Gill, s. (2003). Risks and benefits of hormone replacement therapy: the evidence speaks. Canadian Medical Association Journal, 168(8), 1001-10.
Kabat-Zinn, J. (1990). Full catastrophe living. New York: Delacorte Press.
Luthe, W. & Schultz, J.H. (1969). Autogenic therapy: Vol II: Medical applications. New York: Grune & Stratton.
Mathew, R.J.; Claghorn, J.L.; Largen, J.W.; & Dobbins, K. (1979). Skin Temperature control for premenstrual tension syndrome:A pilot study. American Journal of Clinical Biofeedback, 2 (1), 7-10.
Peper, E. (1990). Breathing for health. Montreal: Thought Technology Ltd.
Schultz, J.H., & Luthe, W. (1969). Autogenic therapy: Vol 1. Autogenic methods. New York: Grune and Stratton.
Schwartz, M.S. & Andrasik, F.(2003). Biofeedback: A practitioner’s guide, 3nd edition. New York: Guilford Press.
Shumaker, S.A., Legault, C., Thal, L., Wallace, R.B., Ockene, J., Hendrix, S., Jones III, B., Assaf, A.R., Jackson, R. D., Morley Kotchen, J., Wassertheil-Smoller, S.; & Wactawski-Wende, J. (2003). Estrogen plus progestin and the incidence of dementia and mild cognitive impairment in post menopausal women: The Women’s Health Initiative memory study: A randomized controlled trial. Journal of the American Medical Association, 289 (20), 2651-2662.
Stearns, V., Beebe, K. L., Iyengar, M., & Dube, E. (2003). Paroxetine controlled release in the treatment of menopausal hot flashes. Journal of the American Medical Association, 289 (21), 2827-2834.
Stroebel, C. F. (1982). QR, the quieting reflex. New York: G. P. Putnam’s Sons.
van Dixhoorn, J.J. (1998). Ontspanningsinstructie Principes en Oefeningen (Respiration instructions: Principles and exercises). Maarssen, Netherlands: Elsevier/Bunge.
Wassertheil-Smoller, S., Hendrix, S., Limacher, M., Heiss, G., Kooperberg, C., Baird, A., Kotchen, T., Curb, Dv., Black, H., Rossouw, J.E., Aragaki, A., Safford, M., Stein, E., Laowattana, S., & Mysiw, W.J. (2003). Effect of estrogen plus progestin on stroke in postmenopausal women: The Women’s Health Initiative: A randomized trial. Journal of the American Medical Association, 289 (20), 2673-2684.
Wyeth Pharmaceuticals (2003, June 4). A message from Wyeth: Recent reports on hormone therapy and where we stand today. San Francisco Chronicle, A11.
*We thank Candy Frobish, Mary Bier and Dalainya Kazarian for their helpful contributions to this research.
**For communications contact: Erik Peper, Ph.D., Institute for Holistic Healing Studies, San Francisco State University, 1600 Holloway Avenue, San Francisco, CA 94132; Tel: (415) 338 7683; Email: epeper@sfsu.edu; website: http://www.biofeedbackhealth.org; blog: http://www.peperperspective.come
Relax and Relax More*
Posted: February 6, 2015 Filed under: Uncategorized | Tags: awareness, electromyography, muscle biofeedback, relaxation, shoulder pain 4 CommentsAfter raising my shoulders and then relaxing it, I felt relaxed. I was totally surprised that the actual muscle tension recorded with surface electromyographic (SEMG) still showed tension. Only when I gave myself the second instruction, relax even more, that my SEMG activity decreased.
In our experiences, we (Vietta E. Wilson and Erik Peper, 2014) have observed that muscle tension often does not decrease completely after a person is instructed to relax. The complete relaxation only occurs after the second instruction, relax more, let go, drop, or feel the heaviness of gravity. The person is totally unaware that after the first relaxation their muscless have not totally relaxed. Their physiology does not match their perception (Peper et, 2010; Whatmore & Kohli, 1974). The low level of muscle tension appears more prevalent in people who are have a history of muscle stiffness or pain, or in athletes whose coaches report they look ‘tight.’ It is only after the second command, relax and release even more, that the individual notices a change and experiences a deeper relaxation.
The usefulness of giving a second instruction, relax more, after the first instruction, relax, is illustrated below by the surface electromyographic (SEMG) recording from the upper left and right trapezius muscle of a 68 year old male with chronic back pain. While sitting upright without experiencing any pain, he was instructed to lift his shoulders, briefly hold the tension, and then relax (Sella, 1997; Peper et al, 2008). When the SEMG of the trapezius muscles did not decrease to the relaxed state, he was asked to relax more as is shown in Figure 1.

Figure 1. SEMG recordings of the left and right upper trapezius when the client was asked to lift his shoulders, hold, relax, and relax more. Only after the second instruction did the muscle tension decrease to the relaxed baseline level. Reprinted from Wilson and Peper, 2014.
Although the subject felt that he was relaxed after the first relaxation instruction, he continued to hold a low level of muscle tension. We have observed this same process in hundreds of clients and students while teaching SEMG guided relaxation and progressive muscle relaxation.
For numerous people, even the second commands to relax even more is not sufficient for the SEMG to show muscle relaxation and for them to ‘feel’ or know when they are totally relaxed. These individuals may benefit from SEMG biofeedback to identify and quantify the degree of muscle tension. With this information the person can make the invisible muscle contractions ‘ visible,’ the un-felt tension ‘felt,’ and thus develop awareness and control (Peper et al, 2014).
In summary
- Instruct people to relax after tightening and then repeat the instruction to relax even more.
- Use surface electromyography to confirm whether the person’s subjective experience of being muscularly relaxed corresponds to the actual physiological SEMG recording.
- Use the SEMG biofeedback to train the person to increase awareness and learn relaxation (Peper et al, 2014).
- Read the complete article from which this blog was adapted: Wilson, E. & Peper, E. (2014). Clinical Tip: Relax and Relax More. 42(4), 163-164.
References
Peper, E., Booiman, A., Lin, I-M., & Shaffer, F. (2014). Making the Unaware Aware-Surface electromyography to unmask tension and teach awareness. Biofeedback. 42(1), 16-23.
Peper, E., Booiman, A., Tallard, M., & Takebayashi, N. (2010). Surface electromyographic biofeedback to optimize performance in daily life: Improving physical fitness and health at the worksite. Japanese Journal of Biofeedback Research, 37(1), 19-28.
Peper, E., Tylova, H., Gibney, K.H., Harvey, R., & Combatalade, D. (2008). Biofeedback mastery-An experiential teaching and self-training manual. Wheat Ridge, CO: AAPB.
*This blogpost is adapted from, Wilson, E. & Peper, E. (2014). Clinical tip: Relax and relax more. Biofeedback. 42(4), 163-164.
The surprising and powerful links between posture and mood
Posted: February 3, 2015 Filed under: Uncategorized | Tags: anxiety, depression, mind-body, posture, stress, stress management Leave a commentEnjoy Vivian Giang’s superb blog, The surprising and powerful links between posture and mood, published by Fast Company and reprinted with permission. It summarizes in a very readable way how posture affects health and well being.
The Surprising and Powerful Links between Posture and Mood
Why feeling taller tricks your brain into making you feel more confident and why your smartphone addiction might be making you depressed.
The next time you’re feeling sad and depressed, pay close attention to your posture. According to cognitive scientists, you’ll likely be slumped over with your neck and shoulders curved forward and head looking down.
While it’s true that you’re sitting this way because you’re sad, it’s also true that you’re sad because you’re sitting this way. This philosophy, known as embodied cognition, is the idea that the relationship between our mind and body runs both ways, meaning our mind influences the way our body reacts, but the form of our body also triggers our mind.
In large part due to Amy Cuddy’s widly popular 2012 TED talk, most of us know that two minutes of “power poses” a day can change how we feel about ourselves. This isn’t just about displaying confidence to others around; this is about actually changing your hormones—increased levels of testosterone and decreased levels of cortisol, or the stress hormone, in the brain.
“The brain has an area that reflects confidence, but once that area is triggered it doesn’t matter exactly how it’s triggered,” says Richard Petty, professor of psychology at Ohio State University. “It can be difficult to distinguish real confidence from confidence that comes from just standing up straight … these things go both ways just like happiness leads to smiling, but also smiling leads to happiness.”
When it comes to posture, Petty explains that the way we ultimately feel has a lot to do with the associations we have with being taller. For example, if you take two people and you put one on a chair that’s above the other person, the one that’s looking down will feel more powerful because “we have all these associations” with height and power that “gets triggered automatically when certain movements are made,” he says. The function of your body posture tells your brain that you’re powerful, which, in turn, affects your attitude.
In a 2009 study published in the European Journal of Social Psychology, Petty along with other researchers instructed 71 college students to either “sit up straight” and “push out [their] chest” or “sit slouched forward” with their “face looking at [their] knees.” While holding their assigned posture, the students were asked to list either three positive or negative personal traits they thought would contribute to their future job satisfaction and professional performance. Afterward, the students were asked to take a survey where they rated themselves on how well they thought they would perform as a future professional.
The researchers found that how the students rated themselves depended on the posture they kept when they wrote the positive or negative traits. Those who were in the upright position believed in the positive and negative traits they wrote down while those in the slouched over position weren’t convinced of their positive or negative traits. In other words, when the students were in the upright, confident position, they trusted their own thoughts whether those thoughts were positive or negative. On the other hand, when the students sat in a powerless position, they didn’t trust anything they wrote down whether it was positive or negative.
However, those in the upright position likely had an easier time thinking of “empowering, positive” traits about themselves to write down while those in the slouched over position probably had an easier time recalling “hopeless, helpless, powerless, and negative” feelings, according to Erik Peper, professor of Holistic Health at San Francisco State University.
In a series of experiments, Peper found that sitting in a collapsed, helpless position makes it easier for negative thoughts and memories to appear while sitting in an upright, powerful position makes it easier to have empowering thoughts and memories.
“Emotions and thoughts affect our posture and energy levels; conversely, posture and energy affect our emotions and thoughts,” says one of Peper’s studies from 2012, and two minutes of skipping versus walking in a slouched position can make a significant difference on our energy levels. Like Cuddy, Peper’s research finds that it only takes two minutes to change your hormones, meaning you can basically change the chemistry in your brain while waiting for your food to heat up in the microwave.
Since posture affects our mood and thoughts so much, the increase of collapsed sitting and walking—from sitting in front of our computer to looking down at our smartphones—may very much have an effect on the rise of depression in recent years. Peper and his team of researchers suggest that posture is a significant contributor to decreased energy levels and depression. Slouching is also known to result in frequent headaches and neck and shoulder pains.
With so much research proving the influence posture has on our mind, Peper suggests hanging photos of people you love slightly higher on the wall or above your desk so that you have to look up. Also, adjust your rear view mirror slightly higher so that you have to sit up taller while driving. If you need reminders, Petty advises setting reminders on your phone, computer, or even a Post-It note. When you do have negative thoughts, instead of validating them by slumping over or bending your head, Petty says that you should write them down on a piece of paper, then throw that piece of paper away in the trash.
“People who throw those negative thoughts into the trash can are less affected by them then people who had the same thoughts but symbolically put them in their pocket,” he says. “It’s this idea that it’s not what we think that’s important; it’s how much we trust what we think.”
Reprinted by permission from Vivian Giang
Overdiagnosed: Should I have more tests or treatments?
Posted: February 1, 2015 Filed under: Uncategorized | Tags: cancer, diagnosis, health, medication, prevention 2 CommentsOne Computerized tomography (CT) scan of the abdomen and pelvis will expose you to more radiation than the residents of Fukushima, Japan absorbed after the Fukushima Daiichi nuclear power plant accident in 2011. –Consumer Reports, March 2015, Vol.80 No.3, 39.
High-risk patients with heart failure and cardiac arrest hospitalized in teaching hospitals had a significantly lower 30-day mortality when admitted during dates of national cardiology meetings (70% survival when doctors attended meeting as compared to 60% survival when doctors did not attend the meetings). –-Jena et al, 2014.
There are so many questions
I feel healthy but worry that cancer could be lurking in the background, should I do a preventative body scan?
I sometimes have slightly higher blood pressure especially when the doctor measures it. It is probably borderline, should I go on medication?
Should I have my PSA tested?
I am a healthy fifty year old, should I have a mammogram?
Should I have an annual physical?
In the quest to stay healthy or prevent disease, we are bombarded by information that preventative testing would save lives and improve health. Only in the United States and New Zealand allow direct to consumer medical advertising which tends to increase excessive drug use and medical testing (Liang & Mackey, 2011). The messages imply that medical screening and testing (e.g., body scan or stress tests) can identify early stages of a disease and implying that earlier treatment will improve quality of life and survival. Similar messages encourage basically healthy people to take drugs for borderline conditions (e.g., borderline hypertension, osteopenia, increased cholesterol levels. What is not shared is the possible risk of unnecessary medical interventions or the harm caused by drug or treatment side effects especially when they are used for a long time period. When unbiased research such as the Cochran Reviews are done, even the annual physical exam appears to offer no benefits (Krogsbøll et al, 2013). Similarly, mammograms and PSA testing for a healthy population appears to offer no benefits and may increase risks. It is truly difficult to accept that an annual health check up is worthless or that a routine mammogram or PSA test may do more harm than good since for many years the public message has been the opposite: to get more screening and testing. There are many reasons for this approach such as:
- Genuine belief, although not evidence based, that an early intervention and more testing would reduce suffering.
- Financial incentives for the parties that perform testing and preventative screening or encourage increased drugs sales for borderline conditions for which the risk and benefits are not well documented.
- Fear of lawsuits by medical providers. If a patient develops an illness which possibly could have been diagnosed by screening, even though the screening may not have affected the actual outcome, the health professional could be sued.
Become an informed consumer
When you have a symptom and do not feel well, see your doctor and get diagnosed, it may safe your life. At the same time be an educated consumer and when unexpected findings are discovered and not related to your specific symptom/complaint, ask questions before agreeing to have more tests or treatments. Ask your provider some of the following questions which were initially outlined by Dr. Eugene Robins (1984):
- Why are you doing this test or procedure?
- What are the risks and what are the benefits?
- What are the risks of treatment and what are the benefits of treatment?
- How accurate is the test?
- How will the test results change the treatment strategy?
- Are there less invasive strategies that could be used? Be very careful of exposing yourself and especially children to CT scans. It is estimated that for every 1000 children who have an abdominal CT scan, one will develop cancer as a result (2015, Consumer Report, March 16).
To be able to navigate the complexities of diagnosis and to understand the risks and benefits of treatment and testing, read the recent two articles in the New York Times, Can this treatment help me? There is a statistic for that, How to Measure a Medical Treatment’s Potential for Harm and the superb book, Over-diagnosed-Making people sick in the pursuit of health, by Drs. H. Gilbert Welch, Lisa M Schwartz, and Steven Woloshin who are professors at Darthmouth Institute for Health Policy and Clinical Practice. This book is a must read for every patient and health care provider. 
References:
(2015). Overexposed. Consumer Reports, 80(3), 37-41. http://www.consumerreports.org/cro/2015/01/when-to-skip-ct-scans-and-x-rays/index.htm
Carroll, A.E. & Frakt, A. (2015). How to Measure a Medical Treatment’s Potential for Harm. New York Times, February 2.
Frakt, A. & Carroll, A.T. (2015). Can This Treatment Help Me? There’s a Statistic for That, New York Times, January 26.
Jena, A. B., Prasad, V., Goldman, D. P., & Romley, J. (2014). Mortality and Treatment Patterns Among Patients Hospitalized With Acute Cardiovascular Conditions During Dates of National Cardiology Meetings. JAMA internal medicine. doi:10.1001/jamainternmed.2014.6781 http://www.drperlmutter.com/wp-content/uploads/2015/01/Cardiac-outcome.pdf
Krogsbøll, L. T., Jørgensen, K. J., & Gøtzsche, P. C. (2013). General health checks in adults for reducing morbidity and mortality from disease. JAMA, 309(23), 2489-2490. http://drkney.com/pdfs/WAC_A_061913.pdf
Liang, B. A., & Mackey, T. (2011). Direct-to-consumer advertising with interactive internet media: global regulation and public health issues. JAMA, 305(8), 824-825. http://jama.jamanetwork.com/article.aspx?articleid=645713
Robins, E. D. (1984). Matter of Life & Death: Risks vs. Benefits of Medical Care. New York: W.H. Freeman and Company
Welch, H.G., Schwartz, L.M., & Woloshin, S. (2011). Over-diagnosed-Making people sick in the pursuit of health. Boston: Beacon Press.
A historical perspective of neurofeedback: Video interview by Larrry Berkelhammer of Erik Peper
Posted: January 18, 2015 Filed under: Uncategorized | Tags: biofeedback, cancer, electroencephalography, health, neurofeedback, self-regulation 1 CommentDr. Erik Peper is interviewed by Dr. Larry Berkelhammer about the research he did in the late 60s and early 70s on EEG alpha training. He describes how he learned to turn off alpha brain rhythms in one hemisphere and turn them on in the other.
Neurofeedback equipment allows researchers and clinicians to get extremely useful feedback, allowing people who are hooked up to get very good at identifying their own brain rhythms and to alter them at will. This can potentially allow us to re-train our brains. Dr. Peper talks about how the real gift of science is about being open to explore rather than to assume our beliefs are factual. Science is about curiosity, experimentation, and exploration. In studying people with cancer and other diseases it is vital that we study more than just pathology–we need to study those individuals who are the outliers, that is, those who recovered against all odds–let’s see what they did to mobilize their health.
Cell phones and tablets: Health risk and what to do
Posted: January 16, 2015 Filed under: Uncategorized | Tags: cancer, cell phones, microwaves, radiation, wireless 1 CommentCellphones and laptops are part of our world; however, they are also a health risks as described in the previous blogs: Wireless devices may cause harm and Screens will hurt your children. For a superb summary of current research data see Louise Kuo Habakus’s post, An open letter to Apple Inc. It points out the dangers of tablets and smart phones’ radiation.
A poetic summary of risks and what can be done, read Lawrence Klein’s poem, Cell Phone Harm,
Phone Harmful: Poem
Keep mobile phones, tablets or laptops away from your body,
Wireless Devices may cause harm, this research is not shoddy,
Cervical spine stress caused by your communication possession,
Your head forward position increases cervical compression
On top of that there is an increase risk of brain cancer
It is enough to make you pause, before you answer,
Keep your cell phone away from your body and place
it in your purse or outer coat pocket, not near your face!
And use your speaker phone or ear phones instead
of placing the phone directly against your head.
It is impossible to belief that that only a few years ago,
there were no cell phones. So now when you go
home, put the phone away so you can be with your family.
Cell phone use is ubiquitous, sometime you need to get free!
Copyright Lawrence Klein 2015
Are herbicides a cause for allergies, immune incompetence and ADHD?
Posted: January 11, 2015 Filed under: Nutrition/diet, Uncategorized | Tags: ADHD, allergy, celiac disease, glyphosate, herbicide, Immune function, Roundup, Type 2 diabetes 10 CommentsA couple of customers reported that they could eat our baguette even though they were gluten intolerant. –Clerk at a bakery that sells organic baguettes
When I was a little boy, allergies almost never occurred. I remember only one boy in our class of 38 who had asthma and allergies. –71 year old male
Fruit flies fed on organic raisins, bananas, soy, and potatoes, lived significantly longer, had much higher fertility and survived longer after starvation than those fed non-organic foods. —From Chhabraet al, 2013). For more detail see: Live longer-Enhance fertility and increase stress resistance-Eat organic foods.
After a year of practicing stress management and changing to a totally organic food diet, to my own surprise my nut allergy totally disappeared. –-25 young woman (Peper, 2015).
Many people report being allergic to gluten, nuts, cat hair, etc, or have hay fever or some form of autoimmune disorder. In our 2014 survey 36% of 264 students at an urban university (average age 24.5 years) reported having allergies (Peper and Del Dosso, 2015 unpublished). Over the last forty years more and more people are reporting allergies. Allergies are often dismissed because they are not a serious—just uncomfortable and may limit what you eat or where you visit (e.g., I can’t eat a morning bun or I can’t visit my aunt because she has a cat). In rare cases it may trigger life-threatening allergic reactions (anaphylaxis). By injecting a single dose of epinephrine using an EpiPen,® it helps the body override the allergic reaction for a short period of time. This allows people who are suffering anaphylaxis some time to get emergency care. Epinephrine does NOT resolve allergic reaction. Other drugs, such as antihistamine and steroids, are required to suppress the reaction while the body metabolizes the allergen. This usually takes many hours and people typically have to stay in the hospital for 8-24 hours to be monitored for their safety.
Allergies and autoimmune illnesses have become so common that we forget that they may be markers of immune incompetence and may affect the ability of the body to optimize health. The increase in allergies is an early indicator that something harmful is affecting the body. People who have allergies, autoimmune illnesses, diabetes or other disorders are possibly the “canaries in the coal mine” for the rest of the population. In earlier times before carbon monoxide and other poisonous gasses could be measured with instruments, miner used a canary as a poisonous gas meter. If the canary died, the miners would exit the mine before they would die of the poisonous gasses.
There are many factors that contribute to the radical increase in asthma, rhinitis, allergies, Type 2 diabetes and autoimmune disorders. These include excessive hygiene, lack of breast feeding and introducing foreign foods too early in the first year of a baby’s life, ingestion of acetaminophen (Tylenol) by the pregnant mother and during the first year of baby’s life, low Omega 3 levels during pregnancy, increased exposure to plastics and other endocrine disruptors, stress, etc. Many of these factors are outside of our control; however, diet and the ingestion of residual herbicides and pesticides in food appear to be a major risk factors.
In the last thirty years there has been a radical change in our diet. The food may look and even taste the same, yet it is totally different. Almost all grains, corn, soy, processed foods, and meats contain low levels of Monsanta’s herbicide Roundup® and other herbicides and pesticides. Almost all grain, corn, soy and cotton are now genetically modified crops and herbicide tolerant to Roundup®.
Roundup® was first introduced in 1974 by Monsanto and is the most widely used herbicide for farm and urban use. The active ingredient is glyphosate with numerous other inert ingredients which may also be harmful to humans. According to the US Department of Agriculture, as of 2012, 99% of durum wheat, 97% of spring wheat has been treated with herbicides. It is also used on rice, seeds, alfalfa, dried beans and peas, sugar cane and sweet potatoes (Swanson et al, 2014). As Roundup® and equivalent herbicides are used more and more, numerous illnesses including food allergies have increased. For the correlation between celiac disease (gluten intolerance) and glyphosate use see Figure 1.
 Figure 1. The correlation between increase in celiac disease (gluten intolerance) and increase of the use of the herbicide glyphosate (Roundup®) on the genetically modified grain (From: Samsel, A., & Seneff, S. 2013).
Figure 1. The correlation between increase in celiac disease (gluten intolerance) and increase of the use of the herbicide glyphosate (Roundup®) on the genetically modified grain (From: Samsel, A., & Seneff, S. 2013).
Presently, more than 95% of all grain, corn and soy as well as cotton is genetically modified to be herbicide tolerant as shown in Figure 2.
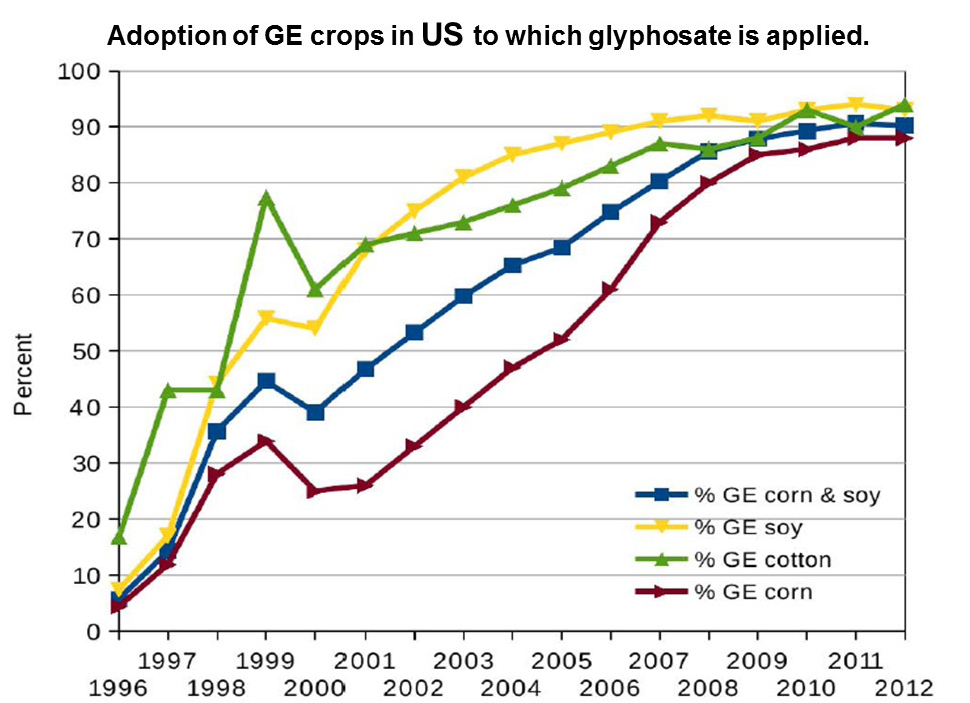
Figure 2. Adoption of GE crops in US to which glyphosate is applied. Reproduce with permission from: Swanson, N. L., Leu, A., Abrahamson, J., & Wallet, B. (2014). Genetically engineered crops, glyphosate and the deterioration of health in the United States of America. Journal of Organic Systems, 9(2), 6-37.
In the USA glyphosate is the most widely used herbicide and about 250 million pounds are applied to U.S farms and even lawns every year. In addition, the common wheat harvest protocol in the United States is to drench the wheat fields with Roundup® several days prior to harvesting. This allow crops to dry down for an earlier, easier and bigger harvest (Swanson et al, 2014; Sarah, 2014). Glyphosate and the many other herbicides and pesticides are in our food, animal fodder and thus in the meat, clothing, water supply and even air. Almost all human and animal food now contains low levels of glyphosate and its inert but poisonous additional ingredients which may impact our health.
The increased application of glyphosate with the increase of chronic diseases over the last 35 years correlates highly (great than 0.9) and is highly significant for obesity (R=0.96), diabetes (R=0.98), end stage renal disease death (R=0.97), Crohn’s disease and ulcerative colitis (R=0.94), death due to intestinal infection (R=0.97), autism in children (6-21 years) (R=0.99), deaths from senile dementia (R=0.99), and death from Alzheimer’s (R=0.93). Figure 3 and 4 shows the relationship between diabetes, autism and glyphosate.
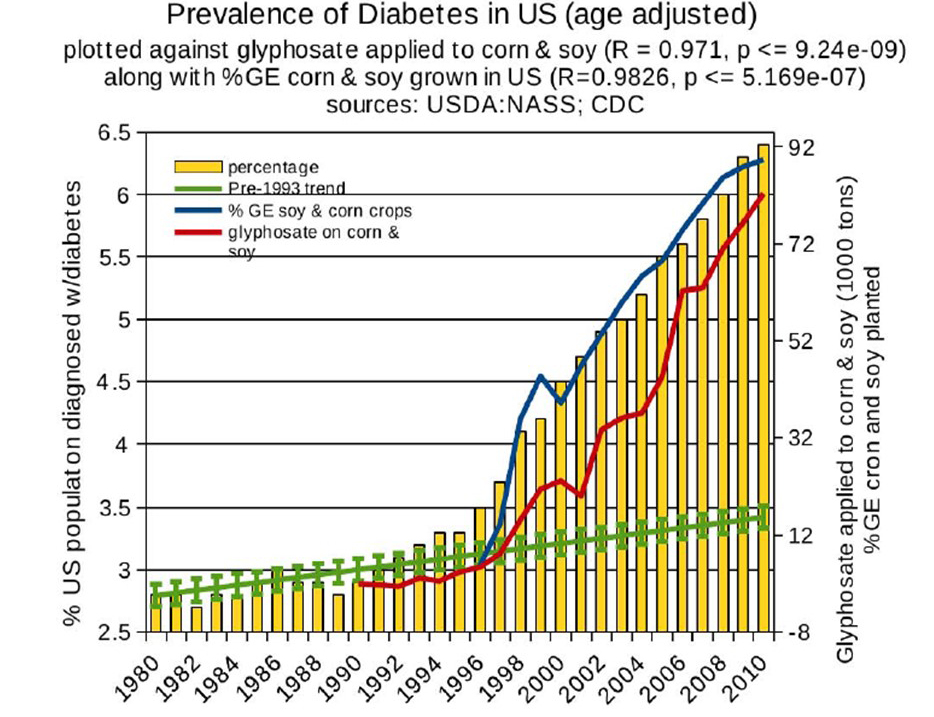
Figure 3. Correlation between age-adjusted diabetes prevalence and glyphosate applications and percentage of US corn and soy crops that are genetically engineered. Reproduce with permission from: Swanson, N. L., Leu, A., Abrahamson, J., & Wallet, B. (2014). Genetically engineered crops, glyphosate and the deterioration of health in the United States of America. Journal of Organic Systems, 9(2), 6-37.
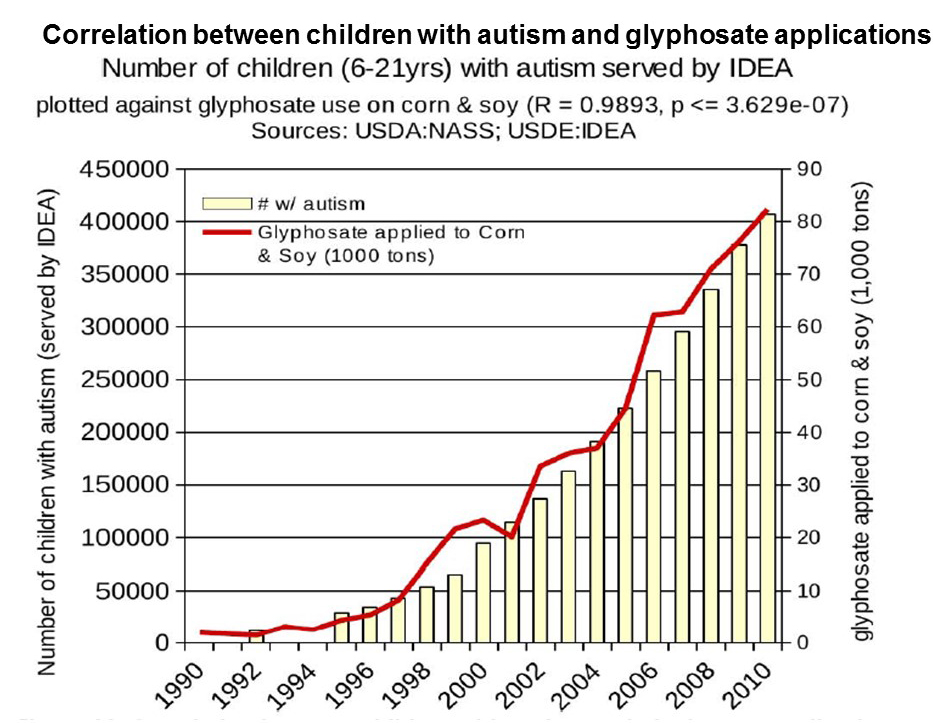 Figure 4. Correlation between children with autism and glyphosate applications. Reproduce with permission from: Swanson, N. L., Leu, A., Abrahamson, J., & Wallet, B. (2014). Genetically engineered crops, glyphosate and the deterioration of health in the United States of America. Journal of Organic Systems, 9(2), 6-37.
Figure 4. Correlation between children with autism and glyphosate applications. Reproduce with permission from: Swanson, N. L., Leu, A., Abrahamson, J., & Wallet, B. (2014). Genetically engineered crops, glyphosate and the deterioration of health in the United States of America. Journal of Organic Systems, 9(2), 6-37.
Correlations are not proof and similar correlations could be plotted between these illnesses and increased production of plastics, intake of high fructose corn syrup, computer use, cell phone use, antidepressant and ADHD medications. Correlations may suggest relationships that should be investigated.
Correlations may suggest possible relationship which should be investigated. It is very difficult to investigate the correlation because most people unknowingly have ingested glyphosate. When using naturalistic observations such as comparing people who eat organic versus non-organic foods, there are many other variables that could account for the differences.
Roundup® residues in food is harmful is from a biological perspective. The purpose of using glyphosate and its inert ingredients is to act as a herbicide and biocide to suppress weed growth and act as a drying agent to improve harvest. As human beings are biological organisms, glyphosate affects our cellular metabolism and especially our bacteria that live in our gut and are necessary for our health. As Samsel & Seneff, (2013) point out, ‘it kills the beneficial bacteria in our gut, leading to the steep rise in intestinal diseases.’ Specifically, Shehata et all (2012) found that “highly pathogenic bacteria as Salmonella Entritidis, Salmonella Gallinarum, Salmonella Typhimurium, Clostridium perfringens and Clostridium botulinum are highly resistant to glyphosate. However, most of beneficial bacteria such as Enterococcus faecalis, Enterococcus faecium, Bacillus badius, Bifidobacterium adolescentis and Lacto-bacillus spp. were found to be moderate to highly susceptible” (Swanson et al, 2014).
Given the very strong correlations of increased disease with increased use of Roundup®, the demonstrated evidence that glyphosate disrupts gut bacteria balance, cellular metabolic processes, kills human embryonic, placental and umbilical cord cells, and acts as endocrine disrupters, the recent decision by the International Agency for Research on Cancer (IARC) which is the specialized cancer agency of the World Health Organization that glyphosate is a possibly carcinogenic to humans (Group 2A), I strongly recommend avoiding glyphosate and other types of herbicide and pesticide contaminated foods. Use the precautionary principle and eat only organic foods.
If the radical increase of allergy and immune incompetence is linked to low level chronic exposure to glyphosate, than avoiding glyphosate and other pesticide and herbicide laced foods may reverse the allergy and immune incompetence. When people adapt an holistic lifestyle which includes stress management and eating organic foods, some report that their immune system became more competent and their allergies disappeared. For example, a 25 year old young woman who successfully reversed cervical dysplasia and eliminated high strains of HPV (her last Paps were normal and the HPV was gone) also found that her nut allergy disappeared (Peper, 2015). As she stated, “I was able to rid myself of a nut allergy that I developed when I was 19. I frequently had trouble breathing therefore I went to an allergist and they told me I had a nut allergy to peanuts (4 out of 4) and tree nuts (2 out of 4). This past July, knowing how truly healthy I had become and after noticing a little to no reaction when I accidentally consumed a nut, I decided to go back to the allergist. I got the test done, and no signs of a nut allergy came up. I believe it was due to this lifestyle change.”
In summary eat only organic foods when possible and follow the wisdom of numerous countries that have banned the use of Roundup®. This year, the Netherlands followed Russia, Tasmania, and Mexico to ban Roundup®. To understand more of the hidden dangers in our food supply from genetic engineering, herbicides and pesticides watch the following impressive videos by Robyn O’Brien presented at TEDxAustin 2011 and MIT researcher Dr. Stephanie Seneff describing in detail the politics and the harmful physiological impact of glyphosate.
References:
Chhabra R, Kolli S & Bauer JH (2013). Organically Grown Food Provides Health Benefits to Drosophila melanogaster. PLoS ONE 8(1): e52988. doi:10.1371/journal.pone.0052988
Peper, E. (2015). Thinking out of the box with biofeedback for the treatment of psychogenic non-epileptic seizures, vulvodynia, and CIN III carcinoma in situ cervical dysplasia. Paper accepted for the 46th Annual Meeting of the Association for Applied Psychophysiology and Biofeedback, Austin, Texas, March 11 – 14, 2015.
Peper, E. & Del Dosso, A. (2015 unpublished). Skipping breakfast a risk for blanking out on exams.
Samsel, A., & Seneff, S. (2013). Glyphosate, pathways to modern diseases II: Celiac sprue and gluten intolerance. Interdisciplinary toxicology, 6(4), 159-184.
Sarah (2014). The real reason wheat is toxic (it’s not the gluten). The Healthy Home Economist, November 13, 2014. Retrieved January 10, 2015 http://www.thehealthyhomeeconomist.com/real-reason-for-toxic-wheat-its-not-gluten/
Saw, L., Shumway, J., & Ruckart, P. (2011). Surveillance Data on Pesticide and Agricultural Chemical Releases and Associated Public Health Consequences in Selected US States, 2003–2007. Journal of medical toxicology, 7(2), 164-171. http://download.springer.com/static/pdf/604/art%253A10.1007%252Fs13181-011-0152-8.pdf?auth66=1421018047_4db65b4e5f0e0349a608560a6c1392e7&ext=.pdf
Shehata, A. A., Schrödl, W., Aldin, A. A., Hafez, H. M., & Krüger, M. (2013). The effect of glyphosate on potential pathogens and beneficial members of poultry microbiota in vitro. Current microbiology, 66(4), 350-358.
Swanson, N. L., Leu, A., Abrahamson, J., & Wallet, B. (2014). Genetically engineered crops, glyphosate and the deterioration of health in the United States of America. Journal of Organic Systems, 9(2), 6-37. http://www.organic-systems.org/journal/92/JOS_Volume-9_Number-2_Nov_2014-Swanson-et-al.pdf
