Reduce TechStress at Home
Posted: March 19, 2020 Filed under: behavior, computer, digital devices, ergonomics, health, laptops, Neck and shoulder discomfort, Pain/discomfort, Uncategorized 8 CommentsAdapted from the book, Peper, E., Harvey, R., & Faass, (2020). Tech Stress: How Technology Is Hijacking Our Lives, Strategies for Coping, and Pragmatic Ergonomics. Berkeley: North Atlantic Books.

Numerous people report that working at the computer at home is more tiring than working in the office. Although there are obvious advantages to working at home, there are also disadvantages (e.g., no space to work, challenging ergonomics, no escape from the family, lack of nonverbal cues used to communicate, less informal sharing at the water cooler, increased multitasking by working and having to take care of the children).
A major challenge is having a comfortable work space in your home. This may mean finding a place to put the computer, keyboard and screen. For some it is the kitchen table, desk in the corner of the bedroom, or coffee table while other it is in a totally separate room.
Incorrect ergonomic arrangement and stressed work style often increases neck, shoulder discomfort and aggravates eye strain and tiredness. Regardless how your digital work space is organized, implement the following life and work style suggestions and ergonomics recommendations to promote health.
LIFE AND WORK STYLE SUGGESTIONS
Take many, many, many breaks. Movement breaks will reduce the covert static tension that builds up as we sit in static positions and work at the computer.
- Every few minutes take a small break such as stand up and wiggle or role your shoulders. When performing the movements, stop looking at the screen and look around the room or out the window.
- Every 30 minutes get up walk around for and move your body. Use timers to notify you every 30 minutes to take a break (e.g., cellphone alarms or personal digital assistants such as Hey Google, Siri, or Alexa).
Improve vision.
- Take vision breaks to reduce eye fatigue.
- Every few minutes look away from the screen and into the far distance and blink. If at all possible look outside at green plants which relaxes the near vision induced tension.
- Blink and blink again. When working at the computer we reduce our blinking rate. Thus, blink each time you click on a new link, finishing entering a column of numbers, etc.
- Close your eyes by letting the eye lids drop down as you also relax your jaw. Imagine a hook on top of your head which is pulling your head upward and at the same time drop your shoulders.
- Reduce glare and bright backgrounds
- Arrange your computer screen at 90 degrees to the brightest light source.
- Have a darker background behind you when participating in video conferencing (e.g., Zoom, Skype, GoToMeeting, WhatsApp, FaceTime). Your face will be visible.
Regenerate
- When stressed remember to breathe. As you inhale let your stomach expand as you exhale let the air flow out slowly.
- Stop watching and listening to the negative news (check the news no more than once a day). Watch positive and humorous movies.
- Get fresh air, go for a walk, and be in the sun
- Reconnect with friends and share positive experiences.
- Remind yourself, that this too shall pass.
ERGONOMIC RECOMMENDATIONS: MAKE THE WORLD YOURS
Good ergonomics means adapting the equipment and environment to you and not the other way around. Optimizes the arrangement of the chair, desk, keyboard, mouse, camera, screen and yourself as shown in Figure 1.

Figure 1. Recommended arrangement for working at the computer.
Arrange the laptop
The laptop is challenging because if your hands are at the right height for data entry on the keyboard, then you must look down to see the screen. If the screen at the right height, then you have to raise your hands to reach the keyboard. There are two solutions for this challenge.
- Use an external keyboard and mouse, then raise the laptop so that the top of the screen is at eye level. Use a laptop stand or a stack of books to raise the lap top.
- Use an external monitor for display, then use the laptop as your keyboard.
If these solutions are not possible, take many, many, many breaks to reduce the neck and shoulder stress.
Arrange the computer workstation
- Adjust the chair so that your forearms can rest on the table without raising your shoulders. This may mean sitting on a pillow. If the chair is then too high and your legs dangle, create a foot stool on which you can rest your feet.
- Adjust the monitor so that the top of the screen is at eye level. If the monitor is too low, raise it by putting some books underneath it.
- If possible, alternate standing and sitting while working.
RESOURCES
Book
Tech Stress: How Technology Is Hijacking Our Lives, Strategies for Coping, and Pragmatic Ergonomics provides insight in how discomfort, symptoms and media addiction develops and what you can do about it. It incorporates the role of evolutionary traps, how biofeedback makes the unaware aware, experiential physical and cognitive practices, and ergonomic recommendations to optimize health and productivity. A must book for anyone using digital devices. Peper, E., Harvey, R., & Faass, (2020). Tech Stress: How Technology Is Hijacking Our Lives, Strategies for Coping, and Pragmatic Ergonomics. Berkeley: North Atlantic Books.
Ergonomic suggestions for working at the computer and laptop.
https://peperperspective.com/2014/09/30/cartoon-ergonomics-for-working-at-the-computer-and-laptop/
11 tips for working at home
How our digital world activates evolutionary response patterns.
https://peperperspective.com/2018/02/10/digital-addiction/
How posture affects health
https://peperperspective.com/2019/07/01/dont-slouch-improves-health-with-posture-feedback/
https://peperperspective.com/2019/05/21/relieve-and-prevent-neck-stiffness-and-pain/
https://peperperspective.com/2019/01/23/head-position-it-matters/
Toning quiets the mind and increases HRV more quickly than mindfulness practice
Posted: September 21, 2019 Filed under: behavior, Breathing/respiration, emotions, health, mindfulness, Pain/discomfort, relaxation, self-healing, stress management, Uncategorized | Tags: heart rate variability, intrusive thoughts, meditation, rumination 6 CommentsDisruptive thoughts, ruminations and worrying are common experiences especially when stressed. Numerous clinical strategies such as cognitive behavioral therapy attempt to teach clients to reduce negative ruminations (Kopelman-Rubin, Omer, & Dar, 2017). Over the last ten years, many people and therapists practice meditative techniques to let go and not be captured by negative ruminations, thoughts, and emotions. However, many people continue to struggle with distracting and wandering thoughts.
Just think back when you’re upset, hurt, angry or frustrated. Attempting just to observe without judgment can be very, very challenging as the mind keeps rehearsing and focusing on what happened. Telling yourself to stop being upset often doesn’t work because your mind is focused on how upset you are. If you can focus on something else or perform physical activity, the thoughts and feelings often subside.
Over the last fifteen years, mindfulness meditation has been integrated and adapted for use in behavioral medicine and psychology (Peper, Harvey, & Lin, 2019). It has also been implemented during bio- and neurofeedback training (Khazan, 2013; Khazan, 2019). Part of the mindfulness instruction is to recognize the thoughts without judging or becoming experientially “fused” with them. A process referred to as “meta-awareness” (Dahl, Lutz, & Davidson, 2015). Mindfulness training combined with bio- and neurofeedback training can improve a wide range of psychological and physical health conditions associated with symptoms of stress, such as anxiety, depression, chronic pain, and addiction (Creswell, 2015, Khazan, 2019).
Mindfulness is an effective technique; however, it may not be more effective than other self-regulations strategies (Peper et al, 2019). Letting go of worrying thoughts and rumination is even more challenging when one is upset, angry, or captured by stressful life circumstances. Is it possible that other strategies beside mindfulness may more rapidly reduce wandering and intrusive thoughts? In 2015, researchers van der Zwan, de Vente, Huiznik, Bogels, & de Bruin found that physical activity, mindfulness meditation and heart rate variability biofeedback were equally effective in reducing stress and its related symptoms when practiced for five weeks.
Our research explored whether other techniques from the ancient wisdom traditions could provide participants tools to reduce rumination and worry. We investigated the physiological effects and subject experiences of mindfulness and toning. Toning is vocalizing long and sustained sounds as a form of mediation. (Watch the video the toning demonstration by sound healer and musician, Madhu Anziani at the end of the blog.)
COMPARING TONING AND MINDFULNESS
The participants were 91 undergraduate college students (35 males, 51 females and 5 unspecified; average age, 22.4 years, (SD = 3.5 years).
After sitting comfortably in class, each student practiced either mindfulness or toning for three minutes each. After each practice, the students rated the extent of mind wandering, occurrence of intrusive thoughts and sensations of vibration on a scale from 0 (not all) to 10 (all the time). They also rated pre and post changes in peacefulness, relaxation, stress, warmth, anxiety and depression. After completing the assessment, they practice the other practice and after three minutes repeated the assessment.
The physiological changes that may occur during mindfulness practice and toning practice was recorded in a separate study with 11 undergraduate students (4 males, 7 females; average age 21.4 years. Heart rate and respiration were monitored with ProComp Infiniti™ system (Thought Technology, Ltd., Montreal, Canada). Respiration was monitored from the abdomen and upper thorax with strain gauges and heartrate was monitored with a blood volume pulse sensor placed on the thumb.
After the sensors were attached, the participants faced away from the screen so they did not receive feedback. They then followed the same procedure as described earlier, with three minutes of mindfulness, or toning practice, counterbalanced. After each condition, they completed a subjective assessment form rating experiences as described above.
RESULTS: SUBJECTIVE FINDINGS
Toning was much more successful in reducing mind wandering and intrusive thoughts than mindfulness. Toning also significantly increased awareness of body vibration as compared to mindfulness as shown in Figure 1.
Figure 1. Differences between mindfulness and toning practice.
There was no significant difference between toning and mindfulness in the increased self-report of peacefulness, warmth, relaxation, and decreased self-report of anxiety and depression as shown in Figure 2.
Figure 2. No significant difference between toning and mindfulness practice in relaxation or stress reports.
RESULTS: PHYSIOLOGICAL FINDINGS
Respiration rate was significantly lower during toning (4.6 br/min) as compared to mindfulness practice (11.6 br/min); heart rate standard deviation (SDNN) was much higher during toning condition (11.6) (SDNN 103.7 ms) than mindfulness (6.4) (SDNN 61.9 ms). Two representative physiological recording are shown in Figure 3.

Figure 3. Representative recordings of breathing and heart rate during mindfulness and toning practice. During toning the respiration rate (chest and abdomen) was much slower than during mindfulness and baseline conditions. Also, during toning heart rate variability was much larger than during mindfulness or baseline conditions.
DISCUSSION
Toning practice is a useful strategy to reduce mind wandering as well as inhibit intrusive thoughts and increase heart rate variability (HRV). Most likely toning uses the same neurological pathways as self-talk and thus inhibits the negative and hopeless thoughts. Toning is a useful meditation alternative because it instructs people to make a sound that vibrates in their body and thus they attend to the sound and not to their thoughts.
Physiologically, toning immediately changed the respiration rate to less than 6 breaths per minute and increases heart rate variability. This increase in heart rate variability occurs without awareness or striving. We recommend that toning is integrated as a strategy to complement bio-neurofeedback protocols. It may be a useful approach to enhance biofeedback-assisted HRV training since toning increases HRV without trying and it may be used as an alternative to mindfulness, or used in tandem for maximum effectiveness.
TAKE HOME MESSAGE
1) When people report feeling worried and anxious and have difficulty interrupting ruminations that they first practice toning before beginning mindfulness meditation or bio-neurofeedback training.
2) When training participants to increase heart rate variability, toning could be a powerful technique to increase HRV without striving
TONING DEMONSTRATION AND INSTRUCTION BY SOUND HEALER MADHU ANZIANI
For the published article see: Peper, E., Pollack, W., Harvey, R., Yoshino, A., Daubenmier, J. & Anziani, M. (2019). Which quiets the mind more quickly and increases HRV: Toning or mindfulness? NeuroRegulation, 6(3), 128-133.
REFERENCES
Creswell, J. D. (2015). Mindfulness Interventions. Annual Review of Psychology, 68, 491-516.
van der Zwan, J. E., de Vente, W., Huizink, A. C., Bogels, S. M., & de Bruin, E. I. (2015). Physical activity, mindfulness meditation, or heart rate variability biofeedback for stress reduction: A randomized controlled trial. Applied Psychophysiology and Biofeedback, 40(4), 257-268. https://doi.org/10.1007/s10484-015-9293-x
Hope for teens with pain
Posted: August 31, 2019 Filed under: behavior, health, Pain/discomfort, relaxation, self-healing, stress management, Uncategorized | Tags: adolescents, teenagers 3 CommentsErik Peper, PhD and Rachel Zoffness, PhD*
KM was 14 years old when he came to my (Zoffness) office for treatment. He’d been diagnosed with migraine and cyclical vomiting syndrome and had been in bed for about 3 years. He had long, unwashed hair; was a sickly, pasty white; and rocked himself back and forth from the pain. He’d seen 15 doctors and had been prescribed 30 medications, including occipital nerve injections and Thorazine. Nothing had worked. Like most teens with chronic pain, KM was depressed, stressed, and terrified he’d never get his life back.
We started Cognitive Behavioral Therapy (CBT), beginning with pain neuroscience education. This involved teaching KM and his family how pain works in the brain, and how thoughts, emotions, physical sensations and behaviors work together to trigger and maintain flares. He then learned a variety of cognitive, behavioral and mind-body techniques to help manage and change pain. His parents received parent-training to support him behind the scenes. After a few weeks of treatment, KM was able to get out of bed and walk to the corner mailbox. After a few more weeks, he was able to walk his dog to the dog park and get a haircut. Within a few months he was jogging around the block, then running. As his functioning increased, his brain desensitized and his body strengthened, his pain started to recede. Gradually he returned to school and social relationships, eventually rejoining his soccer team. I attended his high school graduation a year ago. He got onstage and told the audience that, if you’d told him 4 years ago that he’d graduate high school, he’d never have believed you. He is currently in college, successfully managing his pain, living his important life.
Chronic pain (CP) in teens can be devastating. Teens are already tasked with managing the turbulence of hormone changes, social stress, academic stress, social media, family dynamics, and developing autonomy and independence. CP impacts not only the teen, but also the entire family. Because CP is framed as a biomedical problem, it is frequently treated with opioids and other minimally-helpful (and sometimes harmful) medications. Opioids are ineffective for long-term treatment of chronic pain, and are only useful in acute crises or to control pain at the end of life (Dowell, 2016; King et al, 2011).
Although we typically think of chronic pain as an issue primarily affecting adults coping with issues such as post-surgical pain and arthritis, CP affects up to 1 in 3 youth in the USA – more than 10 million children and teens (Friedrichsdorf, 2016; ). Pain impacts self-esteem, hope, and functioning, relegating teens to their beds and denying them normal educations and healthy social interactions. Like adults, teens often feel powerless and blamed. In a superb workbook, The Chronic Pain & Illness Workbook for Teens, psychologist Rachel Zoffness describes what pain is; how pain is constructed by the brain; how mind, body and emotions interact to affect pain; and offers a sequence of assessments and practices to reduce pain and improve health in language children and teens can easily understand. The approach combines cognitive behavioral therapy (CBT) with imagery, mindfulness, breathing, handwarming with biofeedback, and somatic practices (Turk & Gatchel, 2018; Peper, Gibney, & Holt, 2002).
This simple graphic of the pain cycle is helpful to clients (see Fig. 1).

Fig 1. CBT Pain Cycle
The pragmatic practices in this book offer tools and guided instructions that any child or teen can use for themselves, with parents, or with health providers. Therapists can use and adapt these activities with their clients of all ages. Although these scientifically-supported pain management techniques are written for teens, they can equally be used with adults. Below are two of many different practices described in the book that are useful for chronic pain.
Practice 1: Assessment: What sets off your pain?
The first step is to help youth identify factors that “trigger” – or set off – their pain. It’s helpful to define a trigger as a difficult emotion, situation, or event that causes pain to increase. Difficult situations and events of all kinds – biological, social, etc (situational triggers) can trigger difficult thoughts and emotions (cognitive and emotional triggers), and vice versa. For example, Adam was recovering from back surgery (situational trigger), got into a big fight with his sister about the car (situational trigger), and became angry and frustrated (emotional trigger). He felt the anger in his body, his muscles got hot and tight, and his back started spasming. Gina is an example of the reverse. She believed that nothing could cure her fibromyalgia (cognitive trigger), which made her feel depressed and hopeless (emotional trigger). She stayed home for weeks on end without school, friends, or distractions (situational trigger), and started feeling worse.
We can help youth with pain by asking:
- What emotions trigger your pain?
- Frustration
- Anger
- Stress
- Anxiety
- Loneliness
- Sadness
- What situations trigger your pain?
- Not getting enough sleep
- Arguing with family members
- Inflammation after physical therapy
- Missing fun events because you’re sick
- Thinking about upcoming exams
- Doctor’s appointments and hospital visits
Sometimes, the teen needs to keep a log for a week to identify the situations or triggers related to the pain. Once these have been identified then the teen can explore strategies to reduce the negative reactivity triggered by the emotions or situations.
Practice 2: Changing the voice of pain (Note: this is a summary of a longer activity)
One technique we use in CBT for chronic pain is identifying and tracking cognitive distortions, also known as “thinking traps.” I (Zoffness) call these traps “Pain Voice.” This is the catastrophic, pessimistic, critical, and negative voice that tells us awful, worrisome things, particularly about our pain or health.
For example:
Pain Voice pretends she can predict the future, and says it’s going to be terrible. She says: “You’ll never get better. Nothing will ever help you.” But since she can’t predict the future (who can?), Pain Voice is a liar! Pain Voice is also very bossy about what you can and can’t do: “You can’t see your friends this week,” or “You can’t go for a bike ride, and you definitely can’t have any fun.” Science teaches us that negative thoughts increase pain by turning up the brain’s “pain dial,” so we must make sure not to listen to or believe them. To stop Pain Voice, we first catch negative thoughts.
As soon as you learn how to recognize Pain Voice, you gain the power to change negative thoughts into more helpful “Wise Voice” thoughts. One way to bust Pain Voice is to start tracking your negative thoughts. First, list these critical, self-defeating, catastrophic Pain Voice thoughts. Notice if they’re helpful or harmful. Then check and question them, thoughtfully determining whether they’re the truth or a trap. Next, gather evidence as to why Pain Voice might be wrong by asking yourself, is this thought a fact? What evidence do I have that this thought might not be true? What else might happen other than what I’m predicting? Write out your Wise Voice responses, and use them to fight back every time you hear Pain Voice!
Jason’s example: Jason had terrible, daily back pain and hadn’t gone outside in 6 weeks. His friends texted, inviting him to watch a movie. Immediately he heard the thought, “I can’t go, I’m broken. If I leave my house my pain will spike and I won’t be able to function.” He recognized this as his Pain Voice and knew he had to fight back. He sat down with his worksheet and filled in the answers: yes, the thoughts were harmful, not helpful, and they were trying to trap him! He examined the evidence and wrote the Wise Voice thought, “This negative prediction is not a fact, it’s a trap. I’ve had back pain for 2 years, and sometimes going out and seeing friends actually reduces my pain.” Tuning into his Wise Voice gave him the strength to get the social support and distraction he needed to feel a little better! He went to his friend’s house, watched movies, ate popcorn, giggled, and had a great time. For the first time in 6 weeks, his pain went down. An example of his log is shown in table 1.
|
Situation |
Pain Voice |
Helpful or Harmful? |
Trap or Truth |
Wise Voice |
| Returning to school after missing 3 weeks | If I go back to school, I’ll be so far behind that I won’t understand anything the teacher is talking about. | Harmful | Trap | This negative prediction is not a fact. I’m smart and competent, I’ll probably understand some things. Last time I was behind, I made up the work and everything was fine. |
|
Pain flare-up
|
I can’t handle this! | Harmful | Trap | This negative prediction is not a fact. I’ve had 42 pain flare-ups this year, and I handled all of them. I’ve proven that I’m strong and resilient. There is a 0% chance I can’t handle this. |
Table 1. Example from Jason’s log
Summary: There is hope for youth with chronic pain. Interventions like CBT, mindfulness, biofeedback and other mind-body approaches are scientifically-supported and have evidence of effectiveness. Adhering to the biopsychosocial model – targeting biological, psychological and social factors – is proven to be the most effective treatment for chronic pain across conditions and ages. For more information, see Rachel Zoffness’ book, The chronic pain & illness workbook for teens, for pragmatic treatment practices and user-friendly pain education.

References
*Dr. Rachel Zoffness is a pain psychologist, consultant, writer and educator in Northern California’s East Bay specializing in chronic pain and illness.
Do self-healing first
Posted: May 27, 2019 Filed under: behavior, Breathing/respiration, emotions, Exercise/movement, health, mindfulness, Neck and shoulder discomfort, Nutrition/diet, Pain/discomfort, placebo, relaxation, self-healing, stress management, surgery, Uncategorized 2 Comments
“I am doing very well, and I am very healthy. The vulvodynia symptoms have never come back. Also,my stomach (gastrointestinal discomfort) has gotten much, much better. I don’t really have random pain anymore, now I just have to be watchful and careful of my diet and my exercise, which are all great things!” —A five-year follow-up report from a 28-year-old woman who had previously suffered from severe vulvodynia (pelvic floor pain).
Numerous clients and students have reported that implementing self-healing strategies–common sense suggestions often known as “grandmother’s therapy”—significantly improves their health and find that their symptoms decreased or disappeared (Peper et al, 2014). These educational self-healing approaches are based upon a holistic perspective aimed to reduce physical, emotional and lifestyle patterns that interfere with healing and to increase those life patterns that support healing. This may mean learning diaphragmatic breathing, doing work that give you meaning and energy, alternating between excitation and regeneration, and living a life congruent with our evolutionary past.
If you experience discomfort/symptoms and worry about your health/well-being, do the following:
- See your health professional for diagnosis and treatment suggestions.
- Ask what are the benefits and risks of treatment.
- Ask what would happen if you if you first implemented self-healing strategies before beginning the recommended and sometimes invasive treatment?
- Investigate how you could be affecting your self-healing potential such as:
- Lack of sleep
- Too much sugar, processed foods, coffee, alcohol, etc.
- Lack of exercise
- Limited social support
- Ongoing anger, resentment, frustration, and worry
- Lack of hope and purpose
- Implement self-healing strategies and lifestyle changes to support your healing response. In many cases, you may experience positive changes within three weeks. Obviously, if you feel worse, stop and reassess. Keep a log and monitor what you do so that you can record changes.
This self-healing process has often been labeled or dismissed as the “placebo effect;” however, the placebo effect is the body’s natural self-healing response (Peper & Harvey, 2017). It is impressive that many people report feeling better when they take charge and become active participants in their own healing process. A process that empowers and supports hope and healing. When participants change their life patterns, they often feel better. Their health worries and concerns become reminders/cues to initiate positive action such as:
- Practicing self-healing techniques throughout the day (e.g., diaphragmatic breathing, self-healing imagery, meditation, and relaxation)
- Eating organic foods and eliminating processed foods
- Incorporating daily exercise and movement activities
- Accepting what is and resolving resentment, anger and fear
- Taking time to regenerate
- Resolving stress
- Focusing on what you like to do
- Be loving to yourself and others
For suggestions of what to do, explore some of the following blogs that describe self-healing practices that participants implemented to improve or eliminate their symptoms.
Acid reflux (GERD) https://peperperspective.com/2018/10/04/breathing-reduces-acid-reflux-and-dysmenorrhea-discomfort/
Dyspareunia https://peperperspective.com/2017/03/19/enjoy-sex-breathe-away-the-pain/
Epilepsy https://peperperspective.com/2013/03/10/epilepsy-new-old-treatment-without-drugs/
Irritability/hangry https://peperperspective.com/2017/10/06/are-you-out-of-control-and-reacting-in-anger-the-role-of-food-and-exercise/
Hot flashes and premenstrual symptoms https://peperperspective.com/2015/02/18/reduce-hot-flashes-and-premenstrual-symptoms-with-breathing/
Internet addiction https://peperperspective.com/2018/02/10/digital-addiction/
Irritable bowel syndrome (IBS) https://peperperspective.com/2017/06/23/healing-irritable-bowel-syndrome-with-diaphragmatic-breathing/
Math and test anxiety https://peperperspective.com/2018/07/03/do-better-in-math-dont-slouch-be-tall/
Neck stiffness https://peperperspective.com/2017/04/06/freeing-the-neck-and-shoulders/
Neck tension https://peperperspective.com/2019/05/21/relieve-and-prevent-neck-stiffness-and-pain/
Posture and mood https://peperperspective.com/2017/11/28/posture-and-mood-implications-and-applications-to-health-and-therapy/
Psoriasis https://peperperspective.com/2013/12/28/there-is-hope-interrupt-chained-behavior/
Surgery https://peperperspective.com/2018/03/18/surgery-hope-for-the-best-but-plan-for-the-worst/
Trichotillomania (hair pulling) https://peperperspective.com/2015/03/07/interrupt-chained-behaviors-overcome-smoking-eczema-and-hair-pulling/
Vulvodynia https://peperperspective.com/2015/09/25/resolving-pelvic-floor-pain-a-case-report/
References
Relieve and prevent neck stiffness and pain
Posted: May 21, 2019 Filed under: behavior, Exercise/movement, health, Neck and shoulder discomfort, Pain/discomfort, posture, Uncategorized | Tags: muscle tension, neck pain, neck stiffness, vision 6 CommentsIs your neck stiff, uncomfortable and painful?
When driving is it more difficult to turn your head?
Neck and shoulder pain affect more than 30% of people (Fejer et al, 2006; Cohen, 2015). This blog explores some strategies to reduce or prevent neck stiffness and discomfort and suggests practices to reduce discomfort and increase flexibility if you already are uncomfortable.
Shifts in posture may optimize neck flexibility
In our modern world, we frequently engage in a forward head position while looking at electronic devices or typing on computers. Prolonged smart phone usage has the potential to negatively impact posture and breathing functions (Jung et al., 2016) since we tilt our head down to look at the screen. Holding the head in a forward position, as displayed in Figure 1, can result in muscle tension in the spine, neck, and shoulders.
 Fig 1. Forward head and neck posture in comparison to a neutral spine. Source: https://losethebackpain.com/conditions/forward-head-posture/
Fig 1. Forward head and neck posture in comparison to a neutral spine. Source: https://losethebackpain.com/conditions/forward-head-posture/
Whenever you bring your head forward to look at the screen or tilt it down to look at your cellphone, your neck and shoulder muscles tighten and your breathing pattern become more shallowly. The more the head is forward, the more difficulty is it to rotate your head as is describe in the blog, Head position, it matters! (Harvey et al, 2018). Over time, the head forward position may lead to symptoms such as headaches and backpain. On the other hand, when we shift to an aligned upright position throughout the day, we create an opportunity to relieve this tension as shown in Figure 2.
 Figure 2. EMG and respiration recording from a subject sitting with a forward head position and a neutral, aligned head position. The neck and shoulder muscle tension was recorded from the right trapezius and left scalene muscles (Mason et all, unpublished). .
Figure 2. EMG and respiration recording from a subject sitting with a forward head position and a neutral, aligned head position. The neck and shoulder muscle tension was recorded from the right trapezius and left scalene muscles (Mason et all, unpublished). .
The muscle tension recorded from scalene and trapezius muscles (neck and shoulder) in Figure 2 shows that as the head goes forward or tilts down, the muscle tension significantly increases. In most cases participants are totally unware that their neck tightens. It is only after looking at the screen or focus our eyes until the whole day that we notice discomfort in the late afternoon.
Experience this covert muscle tension pattern in the following video, Sensing neck muscle tension-The eye, head, and neck connection.
Interrupt constant muscle tension
One possible reason why we develop the stiffness and discomfort is that we hold the muscles contracted for long time in static positions. If the muscle can relax frequently, it would significantly reduce the probability of developing discomfort. Experience this concept of interrupting tension practice by practicing the following:
- Sit on a chair and lift your right foot up one inch up from the floor. Keep holding it up? For some people, as soon as five seconds, they will experience tightening and the onset of discomfort and pain in the upper thigh and hip.
How long could you hold your foot slight up from the floor? Obviously, it depends on your motivation, but most people after one minute want to put the foot down as the discomfort become more intense. Put the foot down and relax. Notice the change is sensation and for some it takes a while for the discomfort to fade out.
- The reason for the discomfort is that the function of muscle is to move a joint and then relax. If tightening and relaxation occurs frequently, then there is no problem
- Repeat the same practice except lift the foot, relax and drop it down and repeat and repeat. Many people can easily do this for hours when walking.
What to do to prevent neck and shoulder stiffness.
Interrupt static muscle neck tension by moving your head neck and shoulder frequently while looking at the screen or performing tasks. Explore some of the following:
- Look away from the screen, take a breath and as you exhale, wiggle your head light heartedly as if there is a pencil at reaching from the top of your head to the ceiling and you are drawing random patterns on the ceiling. Keep breathing make the lines in all directions.
- Push the chair back from the desk, roll your right shoulder forward, up and back let it drop down and relax. Then roll you left shoulder forward up and back and drop down and relax. Again, be sure to keep breathing.
- Stand up and skip in place with your hands reaching to the ceiling so that when your right foot goes up you reach upward with your left hand toward the ceiling while looking at your left hand. Then, as your left foot goes up your reach upward to the ceiling with your right hand and look at your right hand. Smile as you are skipping in place.
- Install a break reminder program on your computer such as Stretch Break to remind you to stretch and move.
- Learn how to sit and stand aligned and how to use your body functionally such as with the Gokhale Method or the Alexander Technique (Gokhale, 2013; Peper et al, in press, Vineyard, 2007).
- Learn awareness and control neck and shoulder muscle tension with muscle biofeedback. For practitioners certified in biofeedback BCB, see https://certify.bcia.org/4dcgi/resctr/search.html
- Become aware of your collapsed and slouching wearing a posture feedback device such as UpRight Go on your upper back. This device provides vibratory feedback every time you slouch and reminds you to interrupt slouching and be upright and alighned.
Arrange your computer screen and keyboard so that the screen is at eye level instead of having to reach forward or look down. Similarly, hold your cell phone so that it is at eye level as shown in Figure 3 and 4.
 Figure 3. Slouching forward to see the laptop screen can be avoided by using an external keyboard, mouse and desktop riser. Reproduced by permission from www.backshop.nl
Figure 3. Slouching forward to see the laptop screen can be avoided by using an external keyboard, mouse and desktop riser. Reproduced by permission from www.backshop.nl

Figure 4. Avoid the collapsed while looking down at a cell phone by resting the arms on a backpack or purse and keeping the spine and head alighned. Photo of upright position reproduced with permission from Imogen Ragone, https://imogenragone.com/
Check vision
If you are squinting, bringing your nose to the screen, or if the letters are too small or blurry, have your eyes checked to see if you need computer glasses. Generally do not use bifocals or progressive glasses as they force you to tilt your head up or down to see the material at a specific focal length. Other options included changing the display size on screen by making the text and symbols larger may allow you see the screen without bending forward. Just as your muscle of your neck, your eyes need many vision breaks. Look away from the screen out of the window at a distant tree or for a moment close your eyes and breathe.
What to do if you have stiffness and discomfort
My neck was stiff and it hurt the moment I tried to look to the sides. I was totally surprised that I rapidly increased my flexibility and reduced the discomfort when I implemented the following two practices.
Begin by implementing the previous described preventative strategies. Most important is to interrupt static positions and do many small movement breaks. Get up and wiggle a lot. Look at the blog, Freeing the neck and shoulder, for additional practices.
Then, practice the following exercises numerous times during the day to release neck and shoulder tension and discomfort. While doing these practices exhale gently when you are stretching. If the discomfort increases, stop and see your health professional.
REFERENCES
Cohen, S.P. (2015). Epidemiology, Diagnosis, and Treatment of Neck Pain. Mayo Clinic Proceedings, 90 (2), 284-299. https://doi.org/10.1016/j.mayocp.2014.09.008
Fejer, R., Kyvik, K.Ohm, & Hartvigesen, J. (2006). The prevalence of neck pain in the world population: a systematic critical review of the literature. European Spine Journal, 15(6), 834-848. https://doi.org/10.1007/s00586-004-0864-4
Gokhale, E. (2013). 8 Steps to a Pain-Free Back. Pendo Press.
Harvey, R., Peper, E., Booiman, A., Heredia Cedillo, A., & Villagomez, E. (2018). The effect of head and neck position on head rotation, cervical muscle tension and symptoms. Biofeedback. 46(3), 65–71.
Mason, L., Peper, E., Harvey, R., & Hernandez, W. (unpublished). Healing headaches. Does success sustain over time?
Peper, E., Krüger, B., Gokhale, E., & Harvey, R. (in press). Comparing Muscle Activity and Spine Shape in Various Sitting Styles. Biofeedback.
Vineyar, M. (2007). How You Stand, How You Move, How You Live: Learning the Alexander Technique to Explore Your Mind-Body Connection and Achieve Self-Mastery. Boston: Da Capo Lifelong Books.
Optimize success: Enrich treatment with placebo-the body’s own natural healing response*
Posted: May 2, 2019 Filed under: behavior, health, Pain/discomfort, placebo, surgery, Uncategorized 2 CommentsWhen randomized controlled studies of pharmaceuticals or surgery find that the treatment is no more effective than the placebo, the authors conclude that surgery or drugs have no therapeutic value (Moseley et al, 2002; Jonas et al, 2015). Even though the patients may have gotten better, the researchers often do not explore questions such as, why did some of the patients improve just with the placebo treatment; what are the components of the placebo process; and, how can clinicians integrate placebo components into their practice to enhance the body’s own natural healing response.
To explore these topics further, listen to Shankar Vedantam’s outstanding podcast, A Dramatic Cure, from the NPR program, Hidden Brain-A conversation about life’s unseen patterns. Also, read the background materials on the website https://www.npr.org/2019/04/29/718227789/all-the-worlds-a-stage-including-the-doctor-s-office
 Placebo effects can be a powerful healing strategy as demonstrated by numerous research studies that have persuasively explored the central features of the placebo effect. The research has found that the more dramatic and impressive the procedure, the more powerful the placebo effect. For example, branded medicine with brightly colored packaging is more effective than generic medicine in plain boxes, an injection of a saline or sugar solution is more effective than taking a sugar pill, and placebo surgery is more effective than simply receiving an injection (Branthwaite & Cooper, 1981; Colloca & Benedetti, 2005). For a detailed exploration of placebo, nocebo and the important role of active placebo, see the blog, How effective is treatment? The importance of active placebos.
Placebo effects can be a powerful healing strategy as demonstrated by numerous research studies that have persuasively explored the central features of the placebo effect. The research has found that the more dramatic and impressive the procedure, the more powerful the placebo effect. For example, branded medicine with brightly colored packaging is more effective than generic medicine in plain boxes, an injection of a saline or sugar solution is more effective than taking a sugar pill, and placebo surgery is more effective than simply receiving an injection (Branthwaite & Cooper, 1981; Colloca & Benedetti, 2005). For a detailed exploration of placebo, nocebo and the important role of active placebo, see the blog, How effective is treatment? The importance of active placebos.
To see the effect of the placebo in action, watch the well-known British stage hypnotist and illusionist, Derren Brown’s video, Fear and Faith (https://www.youtube.com/watch?v=hfDlfhHVvTY). He magically weaves together a narrative that addresses the powerful influences of the natural, physical, and clinical environment and language used during a ‘therapeutic’ interaction. He shows how the influences of role modeling, the words that increase hope, trust and social compliance, and other covert factors promote healing. It uses the cover of a drug trial to convince various members of the public to overcome their fears using a placebo medicine called “Rumyodin” (which is a made-up name of a fake pharmaceutical) and demonstrates that the limits of experience are the limits of your belief.
This blog post serves as a reminder to ask ourselves as educators and therapists, ‘what can I do to include placebo enhancing components into my practice so that my clinical and educational outcomes are more effective?’ Explore ways to optimize your clinical environment, language use during ‘therapeutic’ interactions, and role modeling to increase hope, trust and social compliance and thereby optimize your clients’ own natural healing response.
Watch the video: Fear and Faith
References:
*I thank Richard Harvey, PhD., for his constructive feedback and James Fadiman, PhD., for reminding me to reframe the term placebo into “the body’s natural healing response.”
Anxiety, lightheadedness, palpitations, prodromal migraine symptoms? Breathing to the rescue!
Posted: March 24, 2019 Filed under: behavior, Breathing/respiration, emotions, health, Pain/discomfort, relaxation, Uncategorized | Tags: anxiety, aura, diaphragmatic breathing, dizzyness, light headedness, migraine, prodrome, symptom prescription 7 Comments
I quickly gasped twice and a sharp pain radiated up my head and into my eye. I shifted to slow breathing and it faded away.
I felt anxious and became aware of my heart palpitations at the end of practicing 70% exhalation for 30 seconds. I was very surprised how quickly my anxiety was triggered when I changed my breathing pattern.
Breathing is the body/mind/emotion/spirit interface which is reflected in our language with phrases such as a sigh of relief, all choked up, breathless, full of hot air, waiting with bated breath, inspired or expired, all puffed up, breathing room, or it takes my breath away. The colloquial phrases reflect that breathing is more than gas exchange and may have the following effects.
- Changes the lymph and venous blood return from the abdomen (Piller, Leduc, & Ryan, 2006). The downward movement of the diaphragm with the corresponding expansion of the abdomen occurs during inhalation as well as slight relaxation of the pelvic floor. The constriction of the abdomen and slight tightening of the pelvic floor causing the diaphragm to go upward and allows exhalation. This dynamic movement increases and decreases internal abdominal and thoracic pressures and acts a pump to facilitate the venous and lymph return from the abdomen. In many people this dynamic pumping action is reduced because the abdomen does not expand during inhalation as it is constricted by tight clothing (designer jean syndrome), holding the abdomen in to maintain a slim self-image, tightening the abdomen in response to fear, or the result of learned disuse to reduce pain from abdominal surgery, gastrointestinal disorders, or abdominal insults (Peper et al, 2015).
- Increases spinal disk movement. Effortless diaphragmatic breathing is a whole body process and associated with improved functional movement (Bradley, & Esformes, 2014). The spine slightly flexes when we exhale and extends when we inhale which allows dynamic disk movement unless we sit in a chair.
- Communicates our emotional state as our breathing patterns reflect our emotional state. When we are anxious or fearful the breath usually quickens and becomes shallow while when we relax the breath slows and the movement is more in the abdomen (Homma, & Masoka, 2008).
- Evokes, maintains, inhibits symptoms or promotes healing. Breathing changes our physiology, thoughts and emotions. When breathing slowly to about 6 breaths a minute, it may enhance heart rate variability and thereby increase sympathetic and parasympathetic balance (Lehrer & Gevirtz, 2014; Moss & Shaffer, 2017).
Can breathing trigger symptoms?
A fifty-five year old woman asked for suggestions what she could do to prevent the occurrence of episodic prodrome and aura symptoms of visual disturbances and problems in concentration that would signal the onset of a migraine. In the past, she had learned to control her migraines with biofeedback; however, she now experienced these prodromal sensation more and more frequently without experiencing the migraine. As she was talking, I observed that she was slightly gasping before speaking with shallow rapid breathing in her chest.
To explore whether breathing pattern may contribute to evoke, maintain or amplify symptoms, the following two behavioral breathing challenges can suggest whether breathing is a factor: Rapid fearful gasping or 70% exhalation.
Behavioral breathing challenge: Rapid fearful gasping
Take a rapid fearful gasp when inhaling as if your feel scared or fearful. Let the air really quickly come in and repeat two or three times as described in the video. Then describe what you experienced.
If you became aware of the onset of a symptom or that the symptom intensified, then your dysfunctional breathing patterns (e.g., gasping, breath holding or shallow chest breathing) may contribute to development or maintenance of these symptoms. For many people when they gasp–a big rapid inhalation as if they are terrified–it may evoke their specific symptom such as a pain sensation in the back of the eye, slight pain in the neck, blanking out, not being able to think clearly, tightness and stiffness in their back, or even an increase in achiness in their joints (Peper et al, 2016).
To reduce or avoid triggering the symptom, breathe diaphragmatically without effort; namely each time you gasp, hold your breath or breathe shallowly, shift to effortless diaphragmatic breathing.
The above case of the woman with the prodromal migraine symptoms, she experienced visual disturbances and fuzziness in her head after the gasping. This experience allowed her to realize that her breathing style could be a contributing in triggering her symptoms. When she then practiced slow diaphragmatic breathing for a few breaths her symptoms disappeared. Hopefully, if she replaces gasping and shallow breathing with effortless diaphragmatic breathing then there is a possibility that her symptoms may no longer occur.
Behavioral breathing challenge: 70% exhalation
While sitting, breathe normally for a minute. Now change your breathing pattern so that you exhale only 70% or your previous inhaled air. Each time you exhale, exhale only 70% of the inhaled volume. If you need to stop, just stop, and then return to this breathing pattern again by exhaling only 70 percent of the inhaled volume of air. After 30 seconds, let go and breathe normally as guided by the video clip. Observe what happened?
In our research study with 35 volunteers, almost all participants experienced an increase in arousal and symptoms such as lightheadedness, dizziness, anxiety, breathless, neck and shoulder tension after 30 seconds of incomplete exhalation as shown in Figure 1 and Table 1 (Peper and MacHose, 1993).
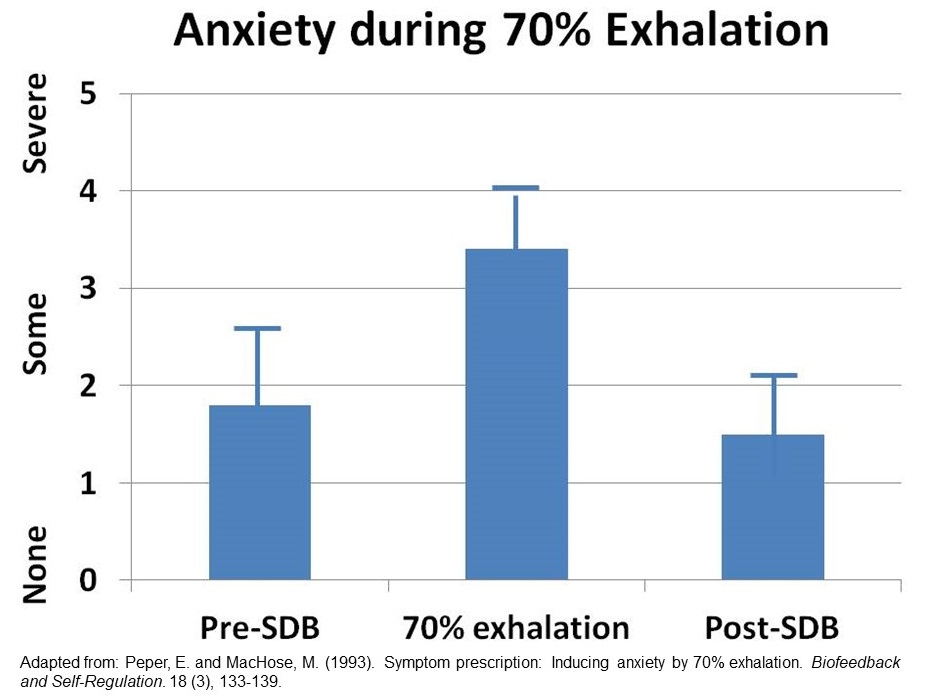
Figure 1. Increase in anxiety evoked by 70% exhalation.

Table 1. Symptoms experienced after exhalation 70%.
Although these symptoms may be similar to those evoked by hyperventilation and overbreathing, they are probably not caused by the reduction of end-tidal carbon dioxide (CO2). The apparent decrease in end-tidal PCO2 is cause by the room air mixing with the exhaled air and not a measure of end-tidal CO2 (Peper and Tibbets, 1992). Most likely the symptoms are associated by the shallow breathing that occurs when we were scared or terrified.
People who have a history of anxiety, panic, nervousness and tension as compared to those who report low anxiety tend to report more symptoms when exhaling 70% of inhaled air for 30 seconds. If this practice evoked symptoms, then changing the breathing patterns to slower diaphragmatic breathing may be a useful self-regulation strategy to optimize health.
These two behavior breathing challenges are useful demonstrations for students and clients that breathing patterns can influence symptoms. By experiencing ON and OFF control over their symptoms with breathing, the person now knows that breathing can affect their health and well being.
BLOGS WITH INSTRUCTIONS FOR LEARNING EFFORTLESS DIAPHRAGMATIC BREATHING
https://peperperspective.com/2017/11/17/breathing-to-improve-well-being/
https://peperperspective.com/2018/10/04/breathing-reduces-acid-reflux-and-dysmenorrhea-discomfort/
https://peperperspective.com/2015/02/18/reduce-hot-flashes-and-premenstrual-symptoms-with-breathing/
https://peperperspective.com/2017/03/19/enjoy-sex-breathe-away-the-pain/
REFERENCES
Lehrer, P.M. & Gevirtz, R. (2014). Heart rate variability biofeedback: how and why does it work? Frontiers in Psychology, 5
Head position, it matters!*
Posted: January 23, 2019 Filed under: behavior, digital devices, Exercise/movement, health, Neck and shoulder discomfort, Pain/discomfort, posture, Uncategorized 5 CommentsThe blog has been adapted from our published article, Harvey, R., Peper, E., Booiman, A., Heredia Cedillo, A., & Villagomez, E. (2018). The effect of head and neck position on head rotation, cervical muscle tension and symptoms. Biofeedback. 46(3), 65–71.

Why is it so difficult to turn your head to see what is behind you?
How come so many people feel pressure in the back of the head or have headaches after working on the computer?
Your mother may have been right when she said, “Sit up straight! Don’t slouch!” Sitting slouched and collapsed is the new norm as digital devices force us to slouch or tilt our head downward. Sometimes we scrunch our neck to look at the laptop screen or cellphone. This collapsed position also contributes to an increased in musculoskeletal dysfunction (Nahar & Sayed, 2018). The more you use a screen for digital tasks, the more you tend to have head-forward posture, especially when the screens are small (Kang, Park, Lee, Kim, Yoon, & Jung, 2012). In addition, the less time children play outside and the more time young children watch the screen, the more likely will they become near sighted and need to have their vision corrected (Sherwin et al, 2012). In addition, the collapsed head forward position unintentionally decreases subjective energy level and may amplify defeated, helpless, hopeless thoughts and memories (Bader, 2015; Peper & Lin, 2012; Tsai, Peper, & Lin, 2016; Peper et al, 2017).
Explore the following two exercises to experience how the head forward position immediately limits head rotation and how neck scrunching can rapidly induce back of the head pressure and headaches.
Exercise 1. Effect of head forward position on neck rotation
Sit at the edge of the chair and bring your head forward, then rotate your head to the right and to the left and observe how far you can rotate. Then sit erect with the crown of the head reaching towards the ceiling and again rotate your head from right to left and observe how far you can rotate as shown in Figure 1.
 Figure 1. Head-erect versus head-forward position.
Figure 1. Head-erect versus head-forward position.
What did you experience?
Most likely your experience is similar to the 87 students (Mean Age = 23.6 years) who participated in this classroom activity designed to bring awareness of the effect of head and neck position on symptoms of muscle tension. 92.0% of the students reported that is was much easier to rotate their head and could rotate further during the head-erect position as compared to the head-forward position (see Figure 2).
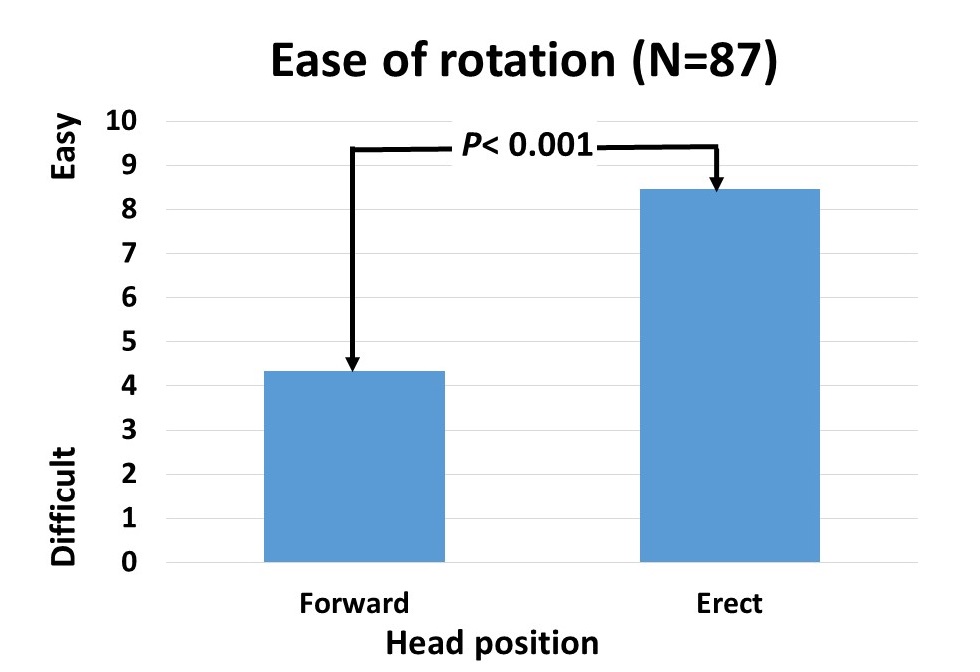 Figure 2. Self-report of ease of head rotation.
Figure 2. Self-report of ease of head rotation.
What does this mean?
Almost all participants were surprised that the head forward position restricted head rotation as well as reduced peripheral awareness (Fernandez-de-Las-Penas et al., 2006). The collapsed head forward may directly affect personal safety; since, it reduces peripheral awareness while walking, biking or driving a car. In addition, when the head is forward, the cervical vertebrae are in a more curved position compared to the erect head with the normal cervical curve (Kang et al., 2012). This means that in the head-forward position, the pressure on the vertebrae and the intervertebral disc is elevated compared to the preferred position with a stretched neck. This increases the risk of damage to the vertebrae and intervertebral disc (Kang et al, 2012). It also means that the muscles that hold the head in the forward position have to work much harder.
Be aware that of factors that contribute to a head-forward position.
- Sitting in a car seat in which the headrest pushes the head forward. Solutions: Tilt the headrest back or put pillow in your back from your shoulders to your pelvis to move your body slightly forward.
- If you wear a bun or ponytail, the headrest (car, airplane seat, or chair) will often push your head forward. This causes a change of the head to a more forward position and it becomes a habit without the person even knowing it. Solution: Place a pillow in your back to move your body forward or loosen the bun or ponytail.
- Difficulty reading the text on the digital screen. The person automatically cranes their head forward to read the text. Solutions: Have your eyes checked and, if necessary, wear computer-reading glasses; alternatively, increase the font size and reduce glare.
- Working on a laptop and looking down on the screen. Solutions: Detachable keyboard and laptop on a stand to raise screen to eye level as shown in Figure 3.
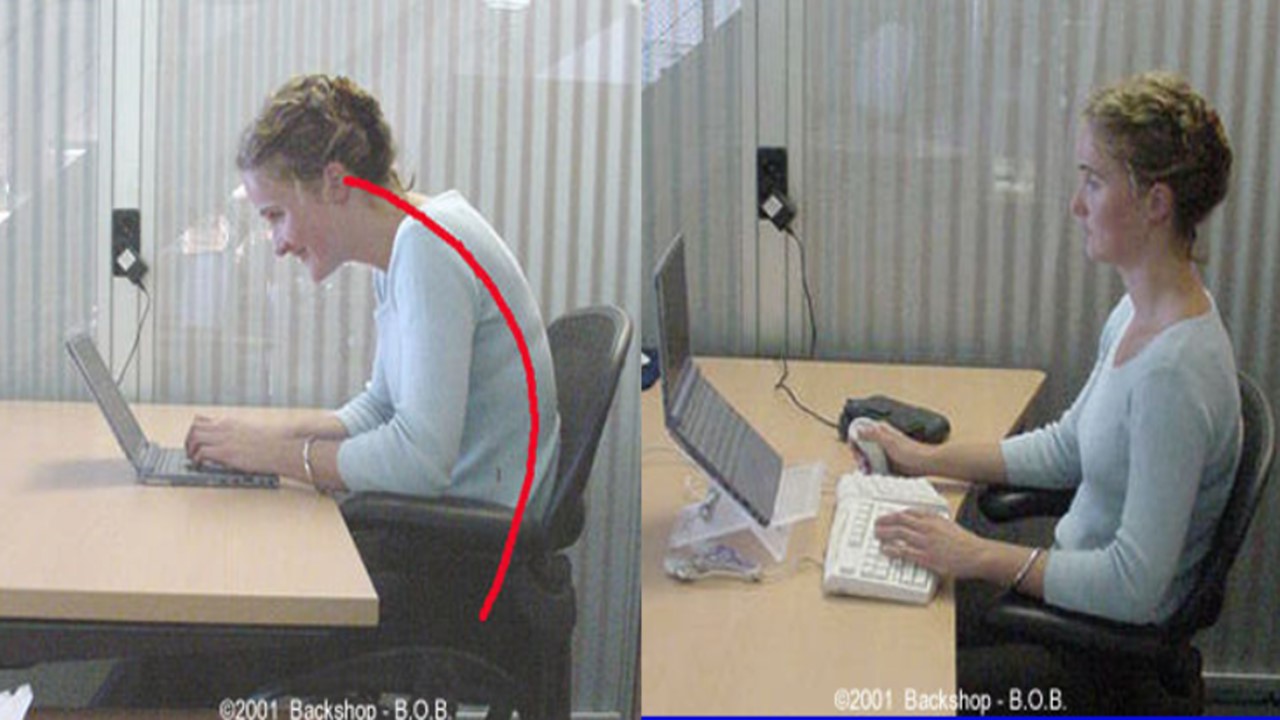
Figure 3. Trying to read the laptop screen, which causes the head to go forward as compared to raising the screen and using an external keyboard. Reproduced by permission from www.backshop.nl
- Being tired or exhausted encourages the body to collapse and slouch and increases the muscle tension in the upper cervical region. You can explore the effect of tiredness that causes slouching and head-forward position during the day by observing the following if you drive a car.
In the morning, adjust your rear mirror and side mirrors. Then at the end of the day when you sit in the car, you may note that you may need to readjust your inside rear mirror. No, the mirror didn’t change of position during the day by itself—you slouched unknowingly. Solutions: Take many breaks during the day to regenerate, install stretch break reminders, or wear an UpRight Go posture feedback device to remind you when you begin to slouch (Peper, Lin & Harvey, 2017).
Exercise 2: Effect of neck scrunching on symptom development
Sit comfortably and your nose forward and slightly. While the head is forward tighten your neck as if your squeezing the back of the head downward into the shoulders and hold this contracted neck position for 20 seconds. Let go and relax.
What did you experience?
Most likely your experience was similar to 98.4% of the 125 college students who reported a rapid increase in discomfort after neck scrunching as shown in Figure 4.
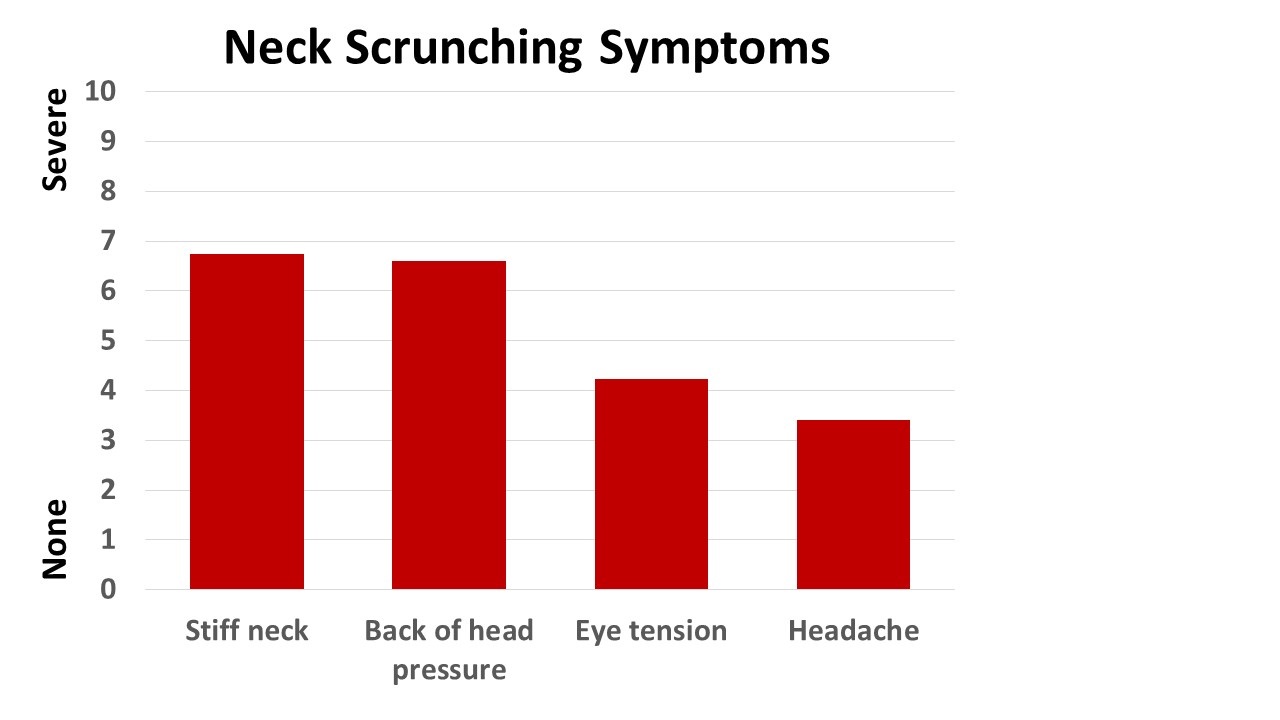 Figure 4. Symptoms induced by 30 seconds of neck scrunching.
Figure 4. Symptoms induced by 30 seconds of neck scrunching.
During scrunching there was a significant increase in the cervical and trapezius sEMG activity recorded from 12 volunteers as shown in Figure 5. Figure 5. Change in cervical and trapezius sEMG during head forward and neck scrunching.
Figure 5. Change in cervical and trapezius sEMG during head forward and neck scrunching.
What does this mean?
Nearly all participants were surprised that 30 seconds of neck scrunching would rapidly increase induce discomfort and cause symptoms. This experience provided motivation to identify situations that evoked neck scrunching and avoid those situations or change the ergonomics that induced the neck scrunching. If you experience headaches or neck discomfort, scrunching could be a contributing factor.
Factors that contribute to neck scrunching and discomfort.
- Bringing your head forward to see the text or graphics more clearly. There may be multiple causes such as blurred vision, tiny text font size, small screen and ergonomic factors. Possible solutions. Have your eyes checked and if appropriate wear computer-reading glasses. Increase the text font size or use a large digital screen. Reduce glare and place the screen at the appropriate height so that the top of the screen is no higher than your eyebrows.
- Immobility and working in static position for too long a time period. Possible solutions. Interrupt your static position with movements every few minutes such as stretching, standing, and wiggling.
Conclusion
These two experiential practices are “symptom prescription practices” that may help you become aware that head position contributes to symptoms development. For example, if you suffer from headaches or neck and backaches from computer work, check your posture and make sure your head is aligned on top of your neck–as if held by an invisible thread from the ceiling and take many movement breaks.The awareness may help you to identify situations that cause these dysfunctional body patterns that could cause symptoms. By inhibiting these head and neck patterns, you may be able to reduce or avoid discomfort. Just as a picture is worth a thousand words, self-experience through feeling and seeing is believing.
REFERENCES
Bader, E. E. (2015). The Psychology and Neurobiology of Mediation. Cardozo J. Conflict Resolution, 17, 363.
Fernandez-de-Las-Penas, C., Alonso-Blanco, C., Cuadrado, M. L., & Pareja, J. A. (2006). Forward head posture and neck mobility in chronic tension-type headache: A blinded, controlled study. Cephalalgia, 26(3), 314-319.
Kang, J. H., Park, R. Y., Lee, S. J., Kim, J. Y., Yoon, S. R., & Jung, K. I. (2012). The effect of the forward head posture on postural balance in long time computer based worker. Annals of rehabilitation medicine, 36(1), 98-104.
Lee, M. Y., Lee, H. Y., & Yong, M. S. (2014). Characteristics of cervical position sense in subjects with forward head posture. Journal of physical therapy science, 26(11), 1741-1743. https://doi.org/10.1589/jpts.26.1741
Nahar, S., & Sayed, A. (2018). Prevalence of musculoskeletal dysfunction in computer science students and analysis of workstation characteristics-an explorative study. International Journal of Advanced Research in Computer Science, 9(2), 21-27. https://doi.org/10.26483/ijarcs.v9i2.5570
Peper, E., & Lin, I. M. (2012). Increase or decrease depression: How body postures influence your energy level. Biofeedback, 40(3), 125-130
Peper, E., Lin, I-M., Harvey, R., & Perez, J. (2017). How posture affects memory recall and mood. Biofeedback.45 (2), 36-41.
Peper, E., Lin, I-M, & Harvey, R. (2017). Posture and mood: Implications and applications to therapy. Biofeedback.35(2), 42-48.
Sherwin, J.C., Reacher, M.H., Keogh, R.H., Khawaja, A.P, Mackey, D.A., & Foster, P.J. (2012). The Association between Time Spent Outdoors and Myopia in Children and Adolescents: A Systematic Review and Meta-analysis. Ophthalmology, 119(10), 2141-2151. https://doi.org/10.1016/j.ophtha.2012.04.020
Tsai, H. Y., Peper, E., & Lin, I. M. (2016). EEG patterns under positive/negative body postures and emotion recall tasks. NeuroRegulation, 3(1), 23-27.
*This blog was adapted from our published article, The blog has been adapted from our research article, Harvey, R., Peper, E., Booiman, A., Heredia Cedillo, A., & Villagomez, E. (2018). The effect of head and neck position on head rotation, cervical muscle tension and symptoms. Biofeedback. 46(3), 65–71.
Today is a new day-a new beginning
Posted: December 31, 2018 Filed under: behavior, health, Pain/discomfort, self-healing, Uncategorized | Tags: dance, hope, joy, pain, regenration, spinal injury 3 CommentsIn a world of turmoil, it is often challenging to think that tomorrow can be different and better. Yet, each day is an opportunity to accept whatever happened in the past and look forward to the unfolding present. So often, we anticipate that the future will be the same or worse especially if we feel depressed, suffer from ongoing pain, chronic illness, family or work stress, etc. At those moments, we forget that yesterday’s memories may contribute to how we experience and interpret the future. Most of us do not know what the future will bring, thus be open to new opportunities for growth and well-being. For the New Year, adapt a daily ritual that I learned from a remarkable healer Dora Kunz.
Each morning when you get out of bed, take a few slow deep breaths. Then think of someone who you feel loved by and makes you smile whether your grandmother, aunt or dog. Then when you get up and put your feet on the ground, say out loud, “Today is a new day- a new beginning.”
Watch the following two videos of people for whom the future appeared hopeless and yet had the courage to transcend their limitations and offer inspiration and joy.
Janine Shepherd: A broken body isn’t a broken person. Cross-country skier Janine Shepherd hoped for an Olympic medal — until she was hit by a truck during a training bike ride. She shares a powerful story about the human potential for recovery. Her message: you are not your body, and giving up old dreams can allow new ones to soar.
Ma Li and Zhai Xiaowei: Hand in Hand. This is a video of a broadcast that originally aired on China’s English-language CCTV channel 9 during a modern dance competition in Beijing, China in 2007. This very unique couple–she without an arm, he without a leg–was one of the finalists among 7000 competitors in the 4th CCTV national dance competition. It is the first time a handicapped couple had ever entered the competition. They won the silver medal and became an instant national hit. The young woman, in her 30’s, was a dancer who had trained since she was a little girl. Later in life, she lost her entire right arm in an automobile accident and fell into a state of depression for a few years. After rebounding, she decided to team with a young man who had lost his leg in a farming accident as a boy and who was completely untrained in dance. After a long and sometimes agonizing training regimen, this is the result. The dance is performed by Ma Li (馬麗) and Zhai Xiaowei (翟孝偉). The music “Holding Hands” is composed by San Bao and choreographed by Zhao Limin.
Breathing reduces acid reflux and dysmenorrhea discomfort
Posted: October 4, 2018 Filed under: Breathing/respiration, Pain/discomfort, posture, relaxation, self-healing, stress management, Uncategorized | Tags: acid reflux, dysmenorrhea, gastroesophageal reflux disease, GERD, menstrual cramps, PMS 14 CommentsPublished as: Peper, E., Mason, L., Harvey, R., Wolski, L, & Torres, J. (2020). Can acid reflux be reduced by breathing? Townsend Letters-The Examiner of Alternative Medicine, 445/446, 44-47. https://www.townsendletter.com/article/445-6-acid-reflux-reduced-by-breathing/
“Although difficult and going against my natural reaction to curl up in the response to my cramps, I stretched out on my back and breathed slowly so that my stomach got bigger with each inhalation. My menstrual pain slowly decreased and disappeared.
“For as long as I remember, I had stomach problems and when I went to doctors, they said, I had acid reflux. I was prescribed medication and nothing worked. The problem of acid reflux got really bad when I went to college and often interfered with my social activities. After learning diaphragmatic breathing so that my stomach expanded instead of my chest, I am free of my symptoms and can even eat the foods that previously triggered the acid reflux.”
In the late 19th earlier part of the 20th century many women were diagnosed with Neurasthenia. The symptoms included fatigue, anxiety, headache, fainting, light headedness, heart palpitation, high blood pressure, neuralgia and depression. It was perceived as a weakness of the nerves. Even though the diagnosis is no longer used, similar symptoms still occur and are aggravated when the abdomen is constricted with a corset or by stylish clothing (see Fig 1).

Figure 1. Wearing a corset squeezes the abdomen.
The constricted waist compromises the functions of digestion and breathing. When the person inhales, the abdomen cannot expand as the diaphragm is flattening and pushing down. Thus, the person is forced to breathe more shallowly by lifting their ribs which increases neck and shoulder tension and the risk of anxiety, heart palpitation, and fatigue. It also can contribute to abdominal discomfort since abdomen is being squeezed by the corset and forcing the abdominal organs upward. It was the reason why the room on top of stairs in the old Victorian houses was call the fainting room (Melissa, 2015).
During inhalation the diaphragm flattens and attempts to descend which increases the pressure of the abdominal content. In some cases this causes the stomach content to be pushed upward into the esophagus which could result in heart burn and acid reflux. To avoid this, health care providers often advice patients with acid reflux to sleep on a slanted bed with the head higher than their feet so that the stomach content flows downward. However, they may not teach the person to wear looser clothing that does not constrict the waist and prevent designer jean syndrome. If the clothing around the waist is loosened, then the abdomen may expand in all directions in response to the downward movement of the diaphragm during inhalation and not squeeze the stomach and thereby pushing its content upward into the esophagus.
Most people have experienced the benefits of loosening the waist when eating a large meal. The moment the stomach is given the room to spread out, you feel more comfortable. If you experienced this, ask yourself, “Could there be a long term cost of keeping my waist constricted?” A constricted waist may be as harmful to our health as having the emergency brake on while driving for a car.
We are usually unaware that shallow rapid breathing in our chest can contribute to symptoms such as anxiety, neck and shoulder tension, heart palpitations, headaches, abdominal discomfort such as heart burn, acid reflux, irritable bowel syndrome, dysmenorrhea and even reduced fertility (Peper, Mason, & Huey, 2017; Domar, Seibel, & Benson, 1990).
Assess whether you are at risk for faulty breathing
Stand up and observe what happens when you take in a big breath and then exhale. Did you feel taller when you inhaled and shorter/smaller when you exhaled?
If the answer is YES, your breathing pattern may compromise your health. Most likely when you inhaled you lifted your chest, slightly arched your back, tightened and raised your shoulders, and lifted your head up while slightly pulling the stomach in. When you exhaled, your body relaxed and collapsed downward and even the stomach may have relaxed and expanded. This is a dysfunctional breathing pattern and the opposite of a breathing pattern that supports health and regeneration as shown in figure 2.

Figure 2. Incorrect and correct breathing. Source unknown.
Observe babies, young children, dogs, and cats when they are peaceful. The abdomen is what moves during breathing. While breathing in, the abdomen expands in all 360 degrees directions and when breathing out, the abdomen constricts and comes in. Similarly when dogs or cats are lying on their sides, their stomach goes up during inhalation and goes down during exhalation.
Many people tend to breathe shallowly in their chest and have forgotten—or cannot– allow their abdomen and lower ribs to widen during inhalation (Peper et al, 2016). These factors include:
- Constriction by the modern corset called “Spanx” to slim the figure or by wearing tight fitting pants. In either case the abdominal content is pushed upward and interferes with normal healthy breathing.
- Maintaining a slim figure by pulling the abdomen (I will look fat when my stomach expands; I will suck it in).
- Avoiding post-surgical abdominal pain by inhibiting abdominal movement. Numerous patients have unknowingly learned to shallowly breathe in their chest to avoid pain at the site of the incision of the abdominal surgery such as for hernia repair or a cesarean operation. This dysfunctional breathing became the new normal unless they actively practice diaphragmatic breathing.
- Slouching as we sit or watch digital screens or look down at our cell phone.
Observe how slouching affects the space in your abdomen.
When you shift from an upright erect position to a slouched or protective position the distance between your pubic bone and the bottom of the sternum (xiphoid process) is significantly reduced.
- Tighten our abdomen to protect ourselves from pain and danger as shown in Figure 3.

Figure 3. Erect versus collapsed posture. There is less space for the abdomen to expand in the protective collapsed position. Reproduced by permission from Clinical Somatics (http://www.clinicalsomatics.ie/).
Regardless why people breathe shallowly in their chest or avoid abdominal and lower rib movement during breathing, by re-establishing normal diaphragmatic breathing many symptoms may be reduced. Numerous students have reported that when they shift to diaphragmatic breathing which means the abdomen and lower ribs expand during inhalation and come in during exhalation as shown in Figure 4, their symptoms such as acid reflux and menstrual cramp significantly decrease.

Figure 4. Diaphragmatic breathing. Reproduced from: www.devang.house/blogs/thejob/belly-breathing-follow-your-gut.
Reduce acid reflux
A 21-year old student, who has had acid reflux (GERD-gastroesophageal reflux diseases) since age 6, observed that she only breathed in her chest and that there were no abdominal movements. When she learned and practiced slower diaphragmatic breathing which allowed her abdomen to expand naturally during inhalation and reduce in size during exhalation her symptoms decreased. The image she used was that her lungs were like a balloon located in her abdomen. To create space for the diaphragm going down, she bought larger size pants so that her abdominal could spread out instead of squeezing her stomach (see Figure 5).

Figure 5. Hydraulic model who inhaling without the abdomen expanding increases pressure on the stomach and possibly cause stomach fluids to be pushed into the esophagus.
She practiced diaphragmatic breathing many times during the day. In addition, the moment she felt stressed and tightened her abdomen, she interrupted this tightening and re-established abdominal breathing. Practicing this was very challenging since she had to accept that she would still be attractive even if her stomach expanded during inhalation. She reported that within two weeks her symptom disappeared and upon a year follow-up she has had no more symptoms. In the video she describes her experiences of integrate breathing and awareness into daily life.
We have also use this similar approach to successfully overcome irritable bowel syndrome see: https://peperperspective.com/2017/06/23/healing-irritable-bowel-syndrome-with-diaphragmatic-breathing/
Take control of menstrual cramps
Numerous college students have reported that when they experience menstrual cramps, their natural impulse is to curl up in a protective cocoon. If instead they interrupted this natural protective pattern and lie relaxed on their back with their legs straight out and breathe diaphragmatically with their abdomen expanding and going upward during inhalation, they report a 50 percent decrease in discomfort (Gibney & Peper, 2003). For some the discomfort totally disappears when they place a warm pad on their lower abdomen and focused on breathing slowly about six breaths per minute so that the abdomen goes up when inhaling and goes down when exhaling. At the same time, they also imagine that the air would flow like a stream from their abdomen through their legs and out their feet while exhaling. They observed that as long as they held their abdomen tight the discomfort including the congestive PMS symptoms remained. Yet, the moment they practice abdominal breathing, the congestion and discomfort is decreased. Most likely the expanding and constricting of the abdomen during the diaphragmatic breathing acts as a pump in the abdomen to increase the lymph and venous blood return and improve circulation.
Conclusion
Breathing is the body-mind bridge and offers hope for numerous disorders. Slower diaphragmatic breathing with the corresponding abdomen movement at about six breaths per minute may reduce autonomic dysregulation. It has profound self-healing effects and may increase calmness and relaxation. At the same time, it may reduce heart palpitations, hypertension, asthma, anxiety, and many other symptoms.
References
DeVault, K.R. & Castell, D.O. (2005). Updated guidelines for the diagnosis and treatment of gastroesophageal reflux disease. The American Journal of Gastroenterology, 100, 190-200.
Domar, A.D., Seibel, M.M., & Benson, H. (1990). The Mind/Body Program for Infertility: a new behavioral treatment approach for women with infertility. Fertility and sterility, 53(2), 246-249.
Gibney, H.K. & Peper, E. (2003). Taking control: Strategies to reduce hot flashes and premenstrual mood swings. Biofeedback, 31(3), 20-24.
Johnson, L.F. & DeMeester, T.R. (1981). Evaluation of elevation of the head of the bed, bethanechol, and antacid foam tablets on gastroesophageal reflux. Digestive Diseases Sciences, 26, 673-680. https://www.ncbi.nlm.nih.gov/pubmed/7261830
Melissa. (2015). Why women fainted so much in the 19th century. May 20, 2015. Donloaded October 2, 1018. http://www.todayifoundout.com/index.php/2015/05/women-fainted-much-19th-century/
Peper, E., Booiman, A., Lin, I-M, Harvey, R., & Mitose, J. (2016). Abdominal SEMG Feedback for Diaphragmatic Breathing: A Methodological Note. Biofeedback. 44(1), 42-49.
Peper, E., Mason, L., Huey, C. (2017). Healing irritable bowel syndrome with diaphragmatic breathing. Biofeedback. (45-4)
Stanciu, C. & Bennett, J.R.. (1977). Effects of posture on gastro-oesophageal reflux. Digestion, 15, 104-109. https://www.karger.com/Article/Abstract/197991
