Hope for teens with pain
Posted: August 31, 2019 Filed under: behavior, health, Pain/discomfort, relaxation, self-healing, stress management, Uncategorized | Tags: adolescents, teenagers 3 CommentsErik Peper, PhD and Rachel Zoffness, PhD*
KM was 14 years old when he came to my (Zoffness) office for treatment. He’d been diagnosed with migraine and cyclical vomiting syndrome and had been in bed for about 3 years. He had long, unwashed hair; was a sickly, pasty white; and rocked himself back and forth from the pain. He’d seen 15 doctors and had been prescribed 30 medications, including occipital nerve injections and Thorazine. Nothing had worked. Like most teens with chronic pain, KM was depressed, stressed, and terrified he’d never get his life back.
We started Cognitive Behavioral Therapy (CBT), beginning with pain neuroscience education. This involved teaching KM and his family how pain works in the brain, and how thoughts, emotions, physical sensations and behaviors work together to trigger and maintain flares. He then learned a variety of cognitive, behavioral and mind-body techniques to help manage and change pain. His parents received parent-training to support him behind the scenes. After a few weeks of treatment, KM was able to get out of bed and walk to the corner mailbox. After a few more weeks, he was able to walk his dog to the dog park and get a haircut. Within a few months he was jogging around the block, then running. As his functioning increased, his brain desensitized and his body strengthened, his pain started to recede. Gradually he returned to school and social relationships, eventually rejoining his soccer team. I attended his high school graduation a year ago. He got onstage and told the audience that, if you’d told him 4 years ago that he’d graduate high school, he’d never have believed you. He is currently in college, successfully managing his pain, living his important life.
Chronic pain (CP) in teens can be devastating. Teens are already tasked with managing the turbulence of hormone changes, social stress, academic stress, social media, family dynamics, and developing autonomy and independence. CP impacts not only the teen, but also the entire family. Because CP is framed as a biomedical problem, it is frequently treated with opioids and other minimally-helpful (and sometimes harmful) medications. Opioids are ineffective for long-term treatment of chronic pain, and are only useful in acute crises or to control pain at the end of life (Dowell, 2016; King et al, 2011).
Although we typically think of chronic pain as an issue primarily affecting adults coping with issues such as post-surgical pain and arthritis, CP affects up to 1 in 3 youth in the USA – more than 10 million children and teens (Friedrichsdorf, 2016; ). Pain impacts self-esteem, hope, and functioning, relegating teens to their beds and denying them normal educations and healthy social interactions. Like adults, teens often feel powerless and blamed. In a superb workbook, The Chronic Pain & Illness Workbook for Teens, psychologist Rachel Zoffness describes what pain is; how pain is constructed by the brain; how mind, body and emotions interact to affect pain; and offers a sequence of assessments and practices to reduce pain and improve health in language children and teens can easily understand. The approach combines cognitive behavioral therapy (CBT) with imagery, mindfulness, breathing, handwarming with biofeedback, and somatic practices (Turk & Gatchel, 2018; Peper, Gibney, & Holt, 2002).
This simple graphic of the pain cycle is helpful to clients (see Fig. 1).

Fig 1. CBT Pain Cycle
The pragmatic practices in this book offer tools and guided instructions that any child or teen can use for themselves, with parents, or with health providers. Therapists can use and adapt these activities with their clients of all ages. Although these scientifically-supported pain management techniques are written for teens, they can equally be used with adults. Below are two of many different practices described in the book that are useful for chronic pain.
Practice 1: Assessment: What sets off your pain?
The first step is to help youth identify factors that “trigger” – or set off – their pain. It’s helpful to define a trigger as a difficult emotion, situation, or event that causes pain to increase. Difficult situations and events of all kinds – biological, social, etc (situational triggers) can trigger difficult thoughts and emotions (cognitive and emotional triggers), and vice versa. For example, Adam was recovering from back surgery (situational trigger), got into a big fight with his sister about the car (situational trigger), and became angry and frustrated (emotional trigger). He felt the anger in his body, his muscles got hot and tight, and his back started spasming. Gina is an example of the reverse. She believed that nothing could cure her fibromyalgia (cognitive trigger), which made her feel depressed and hopeless (emotional trigger). She stayed home for weeks on end without school, friends, or distractions (situational trigger), and started feeling worse.
We can help youth with pain by asking:
- What emotions trigger your pain?
- Frustration
- Anger
- Stress
- Anxiety
- Loneliness
- Sadness
- What situations trigger your pain?
- Not getting enough sleep
- Arguing with family members
- Inflammation after physical therapy
- Missing fun events because you’re sick
- Thinking about upcoming exams
- Doctor’s appointments and hospital visits
Sometimes, the teen needs to keep a log for a week to identify the situations or triggers related to the pain. Once these have been identified then the teen can explore strategies to reduce the negative reactivity triggered by the emotions or situations.
Practice 2: Changing the voice of pain (Note: this is a summary of a longer activity)
One technique we use in CBT for chronic pain is identifying and tracking cognitive distortions, also known as “thinking traps.” I (Zoffness) call these traps “Pain Voice.” This is the catastrophic, pessimistic, critical, and negative voice that tells us awful, worrisome things, particularly about our pain or health.
For example:
Pain Voice pretends she can predict the future, and says it’s going to be terrible. She says: “You’ll never get better. Nothing will ever help you.” But since she can’t predict the future (who can?), Pain Voice is a liar! Pain Voice is also very bossy about what you can and can’t do: “You can’t see your friends this week,” or “You can’t go for a bike ride, and you definitely can’t have any fun.” Science teaches us that negative thoughts increase pain by turning up the brain’s “pain dial,” so we must make sure not to listen to or believe them. To stop Pain Voice, we first catch negative thoughts.
As soon as you learn how to recognize Pain Voice, you gain the power to change negative thoughts into more helpful “Wise Voice” thoughts. One way to bust Pain Voice is to start tracking your negative thoughts. First, list these critical, self-defeating, catastrophic Pain Voice thoughts. Notice if they’re helpful or harmful. Then check and question them, thoughtfully determining whether they’re the truth or a trap. Next, gather evidence as to why Pain Voice might be wrong by asking yourself, is this thought a fact? What evidence do I have that this thought might not be true? What else might happen other than what I’m predicting? Write out your Wise Voice responses, and use them to fight back every time you hear Pain Voice!
Jason’s example: Jason had terrible, daily back pain and hadn’t gone outside in 6 weeks. His friends texted, inviting him to watch a movie. Immediately he heard the thought, “I can’t go, I’m broken. If I leave my house my pain will spike and I won’t be able to function.” He recognized this as his Pain Voice and knew he had to fight back. He sat down with his worksheet and filled in the answers: yes, the thoughts were harmful, not helpful, and they were trying to trap him! He examined the evidence and wrote the Wise Voice thought, “This negative prediction is not a fact, it’s a trap. I’ve had back pain for 2 years, and sometimes going out and seeing friends actually reduces my pain.” Tuning into his Wise Voice gave him the strength to get the social support and distraction he needed to feel a little better! He went to his friend’s house, watched movies, ate popcorn, giggled, and had a great time. For the first time in 6 weeks, his pain went down. An example of his log is shown in table 1.
|
Situation |
Pain Voice |
Helpful or Harmful? |
Trap or Truth |
Wise Voice |
| Returning to school after missing 3 weeks | If I go back to school, I’ll be so far behind that I won’t understand anything the teacher is talking about. | Harmful | Trap | This negative prediction is not a fact. I’m smart and competent, I’ll probably understand some things. Last time I was behind, I made up the work and everything was fine. |
|
Pain flare-up
|
I can’t handle this! | Harmful | Trap | This negative prediction is not a fact. I’ve had 42 pain flare-ups this year, and I handled all of them. I’ve proven that I’m strong and resilient. There is a 0% chance I can’t handle this. |
Table 1. Example from Jason’s log
Summary: There is hope for youth with chronic pain. Interventions like CBT, mindfulness, biofeedback and other mind-body approaches are scientifically-supported and have evidence of effectiveness. Adhering to the biopsychosocial model – targeting biological, psychological and social factors – is proven to be the most effective treatment for chronic pain across conditions and ages. For more information, see Rachel Zoffness’ book, The chronic pain & illness workbook for teens, for pragmatic treatment practices and user-friendly pain education.

References
*Dr. Rachel Zoffness is a pain psychologist, consultant, writer and educator in Northern California’s East Bay specializing in chronic pain and illness.
“Don’t slouch!” Improve health with posture feedback
Posted: July 1, 2019 Filed under: behavior, digital devices, ergonomics, health, Neck and shoulder discomfort, posture, self-healing, Uncategorized | Tags: cellphone, eye strain, Laptop 9 Comments“Although I knew I slouched and often corrected myself, I never realized how often and how long I slouched until the vibratory posture feedback from the UpRight Go 2™ cued me to sit up (see Figure 1).” -Erik Peper
 Figure 1. Wearing an UpRight Go 2™ to increase awareness of slouching and as a reminder to change position.
Figure 1. Wearing an UpRight Go 2™ to increase awareness of slouching and as a reminder to change position.
For thousands of years we sat and stood erect. In those earlier times, we looked down to identify specific plants or animal track and then looked up and around to search for possible food sources, identify friends, and avoid predators. The upright, not slouched posture body posture, is innate and optimizes body movement as illustrated in Figure 2 (for more information, see Gokhale, 2013).
 Figure 2. The normal aligned spine of a toddler and the aligned posture of a man carrying a heavy load.
Figure 2. The normal aligned spine of a toddler and the aligned posture of a man carrying a heavy load.
Being tall and erect allows the head to freely rotate. Head rotation is reduced when we look down at our cell phones, tablets or laptops (Harvey, Peper, Booiman, Heredia Cedillo, & Villagomez, 2018). Our digital world captures us as illustrated in Figure 3.
 Figure 3. Captured by the screen with a head forward positions.
Figure 3. Captured by the screen with a head forward positions.
Looking down and focusing on the screen for long time periods is the opposite of what supported us to survive and thrive when we lived as hunters and gatherers. When we look down, we become more oblivious to our surroundings and unaware of the possible predators that would have been hunting us for food.
This slouched position increases back, neck, head and eye tension as well as affecting respiration and digestion (Devi, Lakshmi, & Devi, 2018; Peper, Lin, & Harvey, 2017). After looking at the screens for a long time, we may feel tired or exhausted and lack initiative to do something else. Our mood may turn more negative since it is easier to evoke hopeless, helpless and powerless thoughts and memories when looking down than when looking up (Wilson, & Peper, 2004; Peper, Lin, Harvey, & Perez, 2017). In the down position, our brain has to work harder to evoke positive thoughts and memories or perform cognitive tasks as compared to when the head is erect (Tsai, Peper, & Lin, 2016; Peper, Harvey, Mason, & Lin, 2018). By looking down and focusing at the screen, our eyes may begin to strain. To be able to see objects near us, the extraocular muscles of the eyes contract to converge the eyes and the cilia muscles around the lens contract to increase the curvature of the lens so that the reading material is in focus.
Become aware how nearby vision increases eye strain.
Hold your arm straight ahead of you at eye level with your thumb up. While focusing on your thumb, slowly bring your thumb closer and closer to your nose. Observe the increase in eyestrain as you bring your thumb closer to your nose.
Eyestrain tends to develop when we do not relax the eyes by periodically looking away from the screen. When we look at the horizon or trees in the far distance the ciliary muscles and the extraocular muscles relax (Schneider, 2016).
Head forward posture increases neck and back tension
When we look down and concentrate, our head moves significantly forward. The neck and back muscles have to work much harder to hold the head up when the neck is in this flexed position. As Dr. Kenneth Hansraj, Chief of Spine Surgery New York Spine Surgery & Rehabilitation Medicine reported, “The weight seen by the spine dramatically increases when flexing the head forward at varying degrees. An adult head weighs 10-12 pounds in the neutral position. As the head tilts forward the forces seen by the neck surges to 27 pounds at 15 degrees, 40 pounds at 30 degrees, 49 pounds at 45 degrees and 60 pounds at 60 degrees.” (Hansraj, 2014). Our head tends to tilt down when we look at the text, videos, emails, photos, or games and stay in this position for long time periods. We are captured by the digital display and are unaware of our tight overused neck and back muscles. Straightening up so that the back of the head is re-positioned over the spine and looking into the distance may help relax those muscles.
To reduce discomfort caused by slouching, we need to reintegrate our prehistoric life style pattern of alternating between looking down to being tall and looking at the distant scenery or across the room. The first step is awareness of knowing when slouching begins. Yet, we tend to be unaware until we experience discomfort or are reminded by others (e.g, “Don’t slouch! Sit up straight!”). If we could have immediate posture feedback when we begin to slouch, our awareness would increase and remind us to change our posture.
Posture feedback with UpRight Go
Simple posture feedback device such as an UpRight Go 2™ can provide vibratory feedback each time slouching starts as the neck as the head goes forward. The wearable feedback device consists of a small sensor that is attached to the back of the neck or back (see Figure 1). After being paired with a cellphone and calibrated for the upright position, the software algorithm detects changes in tilt and provides vibratory feedback each time the neck/back tilts forward.
In our initial exploration, employees, students and clients used the UpRight feedback devices at work, at school, at home, while driving, walking and other activities to identify situations that caused them to slouch. The most common triggers were:
- Ergonomic caused movement such as bring the head closer to the screen or looking down at their cell phone (for suggestions to improve ergonomics see recommendations at the end of the article)
- Tiredness
- Negative self-critical/depressive thoughts
- Crossing the legs protectively, shallow breathing, and other factors
After having identified some of the factors that were associated with slouching, we compared the health outcome of students who used the device for a minimum for 15 minutes a day for four weeks as compared to a control group who did not use the device. The students who received the UpRight feedback were also encouraged to use the feedback to change their posture and behavior and implemented some of the following strategies.
- Head down when looking at their laptop, tablet or cellphone.
- Change the ergonomics such as using a laptop stand and an external keyboard so that they could be upright while looking at the screen.
- Take many movement breaks to interrupt the static tension.
- Feeling tired.
- Take a break or nap to regenerate.
- Do fun physical activity especially activities where you look upward to re-energize.
- Negative self-critical, powerless, self-critical and depressive thoughts and feelings.
- Reframe internal language to empowering thoughts.
- Change posture by wiggling and looking up to have a different point of view.
- Crossing the legs.
- Sit in power position and breathe diaphragmatically.
- Get up and do a few movements such as shoulder rolls, skipping, or arm swings.
- Other causes.
- Identify the trigger and explore strategies so that you can sit erect without effort.
- Wiggle, move and get up to interrupt static muscle tension.
- Stand up and look out of the window and the far distance while breathing slowly
Posture feedback improves health
After four weeks of using the feedback device and changing behavior, the treatment group reported significant improvements in physical and mental health as shown in Figure 4 & 5.
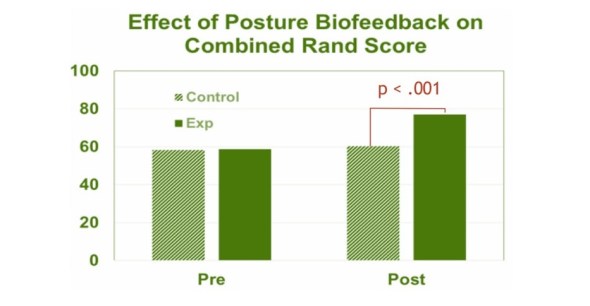
Figure 4. Using the posture feedback significantly improved the Physical Health and Mental Health Composite Scores for the treatment group as compared to the control group (reproduced from Mason, L., Joy, Peper, & Harvey, 2018).

Figure 5. Pre to post changes after using posture feedback (reproduced from Colombo, Joy, Mason, L., Peper, Harvey, & Booiman, 2017).
Summary
Slouched posture and head forward and down position usually occurs without awareness and often results in long-term discomfort. We recommend that practitioners integrate wearable biofeedback devices to facilitate home practice especially for people with neck, shoulder, back and eye discomfort as well as for those with low energy and depression (Mason et al., 2018). We observed that a small wearable posture feedback device helped participants improve posture and decreased symptoms. The vibratory posture feedback provided the person with the opportunity to identify the triggers associated with slouching and the option to change their posture, behavior and environment.
As one participant reported, “I have been using the Upright device for a few weeks now. I mostly use the device while studying at my desk and during class. I have found that it helps me stay focused at my desk for longer time. Knowing there is something monitoring my posture helps to keep me sitting longer because I want to see how long I can keep an upright posture. While studying, I have found whenever I become frustrated, tired, or when my mind begins to wander I slouch. The Upright then vibrates and I become aware of these feelings and thoughts, and can quickly correct them. This device has improved my posture, created awareness, and increased my overall study time.”
Suggestions to reduce slouching and improve ergonomics
How to arrange your computer and laptop: https://peperperspective.com/2014/09/30/cartoon-ergonomics-for-working-at-the-computer-and-laptop/
Relieve neck and shoulder stiffness: https://peperperspective.com/2019/05/21/relieve-and-prevent-neck-stiffness-and-pain/
Cellphone health: https://peperperspective.com/2014/11/20/cellphone-harm-cervical-spine-stress-and-increase-risk-of-brain-cancer/
References
Colombo, S., Joy, M., Mason, L., Peper, E., Harvey, R., & Booiman, A. (2017). Posture Change Feedback Training and its Effect on Health. Poster presented at the 48th Annual Meeting of the Association for Applied Psychophysiology and Biofeedback, Chicago, IL March, 2017. Abstract published in Applied Psychophysiology and Biofeedback.42(2), 147.
Gokhale, E. (2013). 8 Steps to a Pain-Free Back. Pendo Press.
Schneider, M. (2016). Vision for Life. Berkeley, CA: North Atlantic.
Do self-healing first
Posted: May 27, 2019 Filed under: behavior, Breathing/respiration, emotions, Exercise/movement, health, mindfulness, Neck and shoulder discomfort, Nutrition/diet, Pain/discomfort, placebo, relaxation, self-healing, stress management, surgery, Uncategorized 2 Comments
“I am doing very well, and I am very healthy. The vulvodynia symptoms have never come back. Also,my stomach (gastrointestinal discomfort) has gotten much, much better. I don’t really have random pain anymore, now I just have to be watchful and careful of my diet and my exercise, which are all great things!” —A five-year follow-up report from a 28-year-old woman who had previously suffered from severe vulvodynia (pelvic floor pain).
Numerous clients and students have reported that implementing self-healing strategies–common sense suggestions often known as “grandmother’s therapy”—significantly improves their health and find that their symptoms decreased or disappeared (Peper et al, 2014). These educational self-healing approaches are based upon a holistic perspective aimed to reduce physical, emotional and lifestyle patterns that interfere with healing and to increase those life patterns that support healing. This may mean learning diaphragmatic breathing, doing work that give you meaning and energy, alternating between excitation and regeneration, and living a life congruent with our evolutionary past.
If you experience discomfort/symptoms and worry about your health/well-being, do the following:
- See your health professional for diagnosis and treatment suggestions.
- Ask what are the benefits and risks of treatment.
- Ask what would happen if you if you first implemented self-healing strategies before beginning the recommended and sometimes invasive treatment?
- Investigate how you could be affecting your self-healing potential such as:
- Lack of sleep
- Too much sugar, processed foods, coffee, alcohol, etc.
- Lack of exercise
- Limited social support
- Ongoing anger, resentment, frustration, and worry
- Lack of hope and purpose
- Implement self-healing strategies and lifestyle changes to support your healing response. In many cases, you may experience positive changes within three weeks. Obviously, if you feel worse, stop and reassess. Keep a log and monitor what you do so that you can record changes.
This self-healing process has often been labeled or dismissed as the “placebo effect;” however, the placebo effect is the body’s natural self-healing response (Peper & Harvey, 2017). It is impressive that many people report feeling better when they take charge and become active participants in their own healing process. A process that empowers and supports hope and healing. When participants change their life patterns, they often feel better. Their health worries and concerns become reminders/cues to initiate positive action such as:
- Practicing self-healing techniques throughout the day (e.g., diaphragmatic breathing, self-healing imagery, meditation, and relaxation)
- Eating organic foods and eliminating processed foods
- Incorporating daily exercise and movement activities
- Accepting what is and resolving resentment, anger and fear
- Taking time to regenerate
- Resolving stress
- Focusing on what you like to do
- Be loving to yourself and others
For suggestions of what to do, explore some of the following blogs that describe self-healing practices that participants implemented to improve or eliminate their symptoms.
Acid reflux (GERD) https://peperperspective.com/2018/10/04/breathing-reduces-acid-reflux-and-dysmenorrhea-discomfort/
Dyspareunia https://peperperspective.com/2017/03/19/enjoy-sex-breathe-away-the-pain/
Epilepsy https://peperperspective.com/2013/03/10/epilepsy-new-old-treatment-without-drugs/
Irritability/hangry https://peperperspective.com/2017/10/06/are-you-out-of-control-and-reacting-in-anger-the-role-of-food-and-exercise/
Hot flashes and premenstrual symptoms https://peperperspective.com/2015/02/18/reduce-hot-flashes-and-premenstrual-symptoms-with-breathing/
Internet addiction https://peperperspective.com/2018/02/10/digital-addiction/
Irritable bowel syndrome (IBS) https://peperperspective.com/2017/06/23/healing-irritable-bowel-syndrome-with-diaphragmatic-breathing/
Math and test anxiety https://peperperspective.com/2018/07/03/do-better-in-math-dont-slouch-be-tall/
Neck stiffness https://peperperspective.com/2017/04/06/freeing-the-neck-and-shoulders/
Neck tension https://peperperspective.com/2019/05/21/relieve-and-prevent-neck-stiffness-and-pain/
Posture and mood https://peperperspective.com/2017/11/28/posture-and-mood-implications-and-applications-to-health-and-therapy/
Psoriasis https://peperperspective.com/2013/12/28/there-is-hope-interrupt-chained-behavior/
Surgery https://peperperspective.com/2018/03/18/surgery-hope-for-the-best-but-plan-for-the-worst/
Trichotillomania (hair pulling) https://peperperspective.com/2015/03/07/interrupt-chained-behaviors-overcome-smoking-eczema-and-hair-pulling/
Vulvodynia https://peperperspective.com/2015/09/25/resolving-pelvic-floor-pain-a-case-report/
References
Relive memory to create healing imagery
Posted: February 15, 2019 Filed under: behavior, health, placebo, relaxation, self-healing, Uncategorized | Tags: conditioning, Imagery, Pavlov, visualization 4 Comments
This blog describes a structured imagery that evokes past memories of joy and health and integrates them into a relaxation practice to support healing. First, a look at the logic for the practice and then the process of creating your own personal imagery script. A sample audio file is included as a model for creating your MP3 file. The blog is adapted from Peper, E., Gibney, K.H. & Holt. C. (2002). Make Health Happen: Training Yourself to Create Wellness. Dubuque, IA: Kendall-Hunt.
“I enjoyed regressing back into my childhood, remembered playing in the rain, making paper sailboats with my brother…. Placing my fingers in a bowl of water and stroking a paper sailboat enabled me to participate in the total experience… I felt tingling sensations all over my body, like tiny bundles of energy exploding inside of me. By the end of the week the simple word “rain” could induce these sensations inside my whole being.”–Student
Daydreaming! We all know how to do it. When we daydream, we feel, sense, hear, and taste our daydream—the image becomes tangible, as if we are living it. A well-developed relaxation image can also include colors, scents, sounds, flavors, temperature, and so forth. Evoking a past memory image of wholeness may contribute significant to healing, as illustrated in Pavlov’s experience with controlled conditioning and with self-healing.
THE POWER OF CONDITIONING
Pavlov’s experience
Most of us are probably familiar with the classical conditioning experiment of the famous Russian physiologist, Ivan Pavlov, who taught dogs to salivate on cue when they heard a bell ring—even when no food was provided. Pavlov accomplished this by giving the dogs food immediately after ringing a bell. Eventually, the dogs became conditioned to expect the food with the bell and simply hearing the bell ring would induce salivation (shown in Figure 1).

Figure 1. The process of classical conditioning. (Figure adapted from: https://opentextbc.ca/introductiontopsychology/chapter/7-1-learning-by-association-classical-conditioning/)
The conditioning effects of imagery can have an effect on health as well as physiology as reflected in an anecdote told by Theodore Melnechuk about Ivan Pavlov. As an old man, he became quite ill with heart disease and his doctors had no hope of curing him. They took his family aside and told them that the end was near. Pavlov himself, however, was not disheartened. He asked the nurse who was caring for him to bring him a bowl of warm water with a little dirt or mud in it. All day, as he lay in bed, he dabbled one hand in the water, with a dreamy, faraway look on his face. His family was quite sure that he had taken leave of his wits and would die soon. However, the next morning he announced that he felt fine, ate a large breakfast, and sat out in the sun awhile. By the end of the day, when the doctor came to check on him, there was no trace of the heart condition. When asked to explain what he had done, he said that he had reasoned that if he could recall a time when he was completely carefree and happy, it might have some healing benefit for him. As a young boy, he used to spend his summers playing with his friends in a shallow swimming hole in a nearby river. The memory of the warm, slightly muddy water was delightful to him. With his knowledge of the power of conditioned stimuli, he reasoned that having a physical reminder of that water might help him evoke that experience and those blissful feelings, and bring some of those memories into the present time. Using this strategy, he harnessed positive memory and the associated emotions that evoked the associated body changes to bring about his healing.
Conditioned Behaviors
We all performs many conditioned behaviors every day. Some of these behaviors can have implications for our health and wellness. There may be aspects of allergic reactions that are conditioned. For example, the literature reports that a woman who was allergic to roses developed a severe allergic reaction to a very realistic-looking paper rose, even though she was not allergic to paper. Her body reacted as if the paper rose was real. (McKenzie, 1886; Vits et al, 2011).
Conditioning can also affect our immune system. When rats were injected with a powerful immune-suppressing drug, while being fed saccharin-flavored water, their immune function showed an immediate drop. After the drug and saccharine water were paired a number of times, the rats were then given just the saccharin water and a harmless injection of salt water. Their immune cells responded exactly as if they had received the drug! The reverse ability, increasing immune cell function, has been shown to be influenced through conditioning (Ader, Cohen & Felten, 1995; Ader and Cohen, 1993).
Belief can also play a role in these scenarios. Bernie Siegel, MD,(2011) has recounted the story of a woman scheduled for chemotherapy who was first given a saline solution, and cautioned that it could cause hair loss. Although this is an unlikely result of a saline injection, given her belief, her hair fell out.
Actions, thoughts, and images affect our physiology.
We often anticipate, react, and form conclusions with incomplete information. Thoughts and images affect our physiology and even our immune system. Re-evoking a positive memory and living in that memory could potentially improve your health. In a remarkable study by a Harvard psychologist, Ellen Langer, eight men in their 70s lived together for one week, recreating aspects of the world that they had experienced more than 20 years earlier. They were instructed to act as they had in 1959, while the control group was instructed to focus entirely on the present time.
In the experimental group, all the physical cues were reminiscent of the culture twenty years earlier. Black and white television and magazines were from 1959. There were no mirrors to remind them of their current age—only photos on the wall of their younger selves. After a week in which the participants acted as if they were younger and the cues around them evoked their younger selves, 63% of the experimental group had improved their cognitive performance as compared with 44% of the control group. Among participants in the experimental group, even their physical health had improved. Independent raters who looked at the before and after pictures of these participants rated their appearance a little younger than the photos taken before the experiment (Langer, 2009; Grierson, 2014; Friedman, 2015). It is possible that by acting and thinking younger, we actually stay younger!
The limits of our belief are the limits of our experience. This concept underlies the remarkable power of placebo. If one believes a drug or a procedure is helpful, that can have a powerful healing effect (Peper & Harvey, 2017; also see the blog, How effective is treatment? The importance of active placebos).
CREATE YOUR OWN VISUALIZATION
Begin by remembering a time when you felt happy, healthy, and whole. Draw inspiration from Pavlov, who evoked happy memories from his childhood, apparently dramatically changing his health. To develop your personal visualization, set aside the time to recreate a healing memory. Remember a time in your life when you felt healthy and joyous (possibly from your childhood). For some, this might be time in nature or with your family or with friends.
Once you remember the event, re-experience it as if you were there right now. Evoke as many senses as possible. Think of the memory and any associations such as an old teddy bear, a shell from the beach, a favorite song, a certain perfume or some other tangible aspect of the experience. The goal is to recreate the experience as if it was current reality. Olfactory and gustatory cues can be especially powerful. If possible include the actual objects and cues associated with that memory—articles, pictures, music, songs, fragrances, or even food.
Sounds, scents, or touching and objects from that era of your life can deepen your ability to recreate and experience the quality of that memory—to actually be in the memory. These sensory reminders will help to evoke the memory and increase the felt experience. You might find it helpful to review Ellen Langer’s experiment, recreating an environment from twenty years earlier. The actual cues will deepen the experience, just as aromas often evoke specific memories and emotions.
The underlying principle is that memories are associated with conditioned stimuli that evoke the physiological state(s) in the body present when the memory was created.
Once you have created a vivid memory that engenders a sense of wholeness, develop a detailed description of your memory to help you evoke that experience. (For some, the memory calls up a timeless setting—relaxing on a warm beach, sitting in front of the fire on a winter evening, or sailing on a calm day. For others, the sense of trust may be associated with a specific person—someone you love—being with your grandmother, helping your mother bake a cake, or going fishing with your dad.). As you recreate the experience, engage all your senses (images, fragrance, tastes, textures, sounds, kinetics). Stay in your image: see it, smell it, taste it, touch it, hear it, be it and allow the experience to deepen.
Begin by writing up your imagery. Then record the introduction the structured relaxation and follow it with a description that evokes the memory as an MP3 audiofile. Use the following three-step process to create the script for your personal relaxation.
- Describe a time in your past when you felt joy, peace, love, or a sense of integration and wholeness.
_________________________________________________________________
_________________________________________________________________
- Identify the specific cues or stimuli associated with that memory.
_________________________________________________________________
_________________________________________________________________
- Write out a detailed description that will evoke your personal memory.
_________________________________________________________________
_________________________________________________________________
_________________________________________________________________
_________________________________________________________________
CREATING YOUR AUDIO FILE
In this approach, there are three components to your script: first, a relaxation practice to ease you into your visualization, then the visualization of your memory, closing with a brief script that brings you back into the present moment.
Begin the recording with progressive relaxation—use your favorite process for relaxing, or apply the script included here.
Generally tense the muscles for about 5 to 8 seconds and let go for 15 to 20 seconds as indicated by the …. inthe script. While tightening and relaxing the muscles, sense the muscle sensations with passive attention. Tense only the muscles that you are instructed to tighten and continue to breathe while tensing and relaxing the muscles. If your attention wanders, gently bring it back to feeling the sensations in the specific muscles that you are instructed to tighten or relax.
First, find a comfortable position for relaxation… To fully relax your face, squeeze your eyes shut tight, press your lips and teeth together, and wrinkle up your nose… feel the tightness in your whole face… Now let it go completely and relax… Allow your face to soften, feel the eyes sinking in their sockets, and your breath to flow effortlessly in and out…
Tense both arms by making fists, and extend them straight ahead, while continuing to breathe deeply… study the tension… Now relax and let your arms drop as if you were a rag doll… To relax your shoulders, hunch them toward your ears and tighten your neck, while keeping the rest of your body loose and relaxed… Continue to breathe easily… Allow your shoulders to drop… Feel the weight of your arms… Feel the relaxation flowing from your shoulders, down your arms into your hands and out your fingers…
Now your stomach. Then let go and relax… Arch your back and feel the tightness in the back. Let go and relax….Allow your body to sink comfortably into the surface on which you are resting… Finally, tighten your butt, thighs, calves, and feet by pressing your heels down into the surface where you are lying, curling your toes and squeezing your knees together… Feel the tension as you continue to breathe, keeping your upper body relaxed… Now let go and relax… Allow relaxation to flow through your legs… Be aware of the sensations of letting go…
Feel the deepening relaxation, the calmness and the serenity… Feel each exhalation flowing down and through your arms, chest, and legs… Let the feelings of relaxation and heaviness deepen as you relax more… Notice the developing sense of inner peace… a calm indifference to external events… Let the feelings of relaxation, calmness, and serenity deepen for a few minutes. After a few minutes, evoke your memory of wholeness.
Insert your imagery script here.
Finish with the brief closing script
Allow yourself to just stay in this special place all your own… and know that you can return to this peaceful sanctuary any time you choose to do so. When you are ready to release the imagery, take a deep breath, gently stretch your body, and open your eyes.
Record these this whole script on your cell phone as an MP3 file.
When you record, it often takes a few tries before the pacing is correct. You may find it helpful to listen to the following audio file as a model for to create your own.
LISTENING TO YOUR VISUALIZATION
Create a sanctuary for yourself by turning off your cellphone, adjusting the heat to a comfortable temperature, and ensuring that you will have uninterrupted quiet time for 20 to 30 minutes. Loosen any constricting clothing or jewelry, your glasses, and so on. Settle into a comfortable chair, bed, or setting where you can easily relax. Enjoy letting yourself drift into and relive the memory experience.
Many participants report that this practice is an exceptionally relaxing and nurturing experience, one that supports regeneration. You’ll probably find that the more you practice, the more the relaxation deepens. You may find it helpful to keep notes and observe how you feel after each practice. Although it may feel strange to listen to your own voice, most people find that after a while it becomes more comfortable. After listening to it for a few times, you may want to rerecord the script. Finally, generalize this practice by smiling and evoking the memory scene as much as you desire during the day.
Additional strategies to enhance the relaxation
- Have a massage or take a warm shower or soak and then do the practice. Compare your level of relaxation afterwards to the result of using the audio alone.
- Practice gentle stretches to loosen tight muscles or “shake out” your arms and legs just before doing your relaxation practice.
- Draw or paint the relaxing image or actually go to the location where your memory occurred (if possible) and do your practice. Or practice outdoors in the most relaxing place you can find. Nature can be a great healer.
- Create an atmosphere that helps to evoke and augment your relaxation image (e.g., play background music or use fragrances that you associated with the image).
Common challenges
- Inability to evoke a memory of wholeness. When this occurs, it is as if one draws a blank. This is common, especially if one has experienced abuse or feels depressed. In that case, use the image presented in the script or make one up and create a totally imaginary peaceful image.
- Positive memories of wholeness evoke a bitter/sweet feeling. This occurs when images of wholeness include a loved one who has passed on or who is no longer in your life. On the one hand, this may call up strongly positive feelings, but it may evoke a sense of loss and sadness. If this occurs, simply chose a different memory or create a different script. Let the memory of loss go. Accept your experience and your feelings as much as possible, and know that at least you have been loved. For your image, it may be easier to focus on a natural setting you love—one you associate with peace and tranquility.
- Lack of experience with places in nature. Some people have only urban experiences and find nature alien. See what comes up for you. Does your favorite memory as a city kid recall a day of freedom on your bike or skateboarding, or an afternoon with your playmates? Perhaps you have treasured memories as a teen or an adult of long walks in the city or time spent with close friends. You also have the option of creating new images such as sitting by a fireplace, in a walled garden, or some other scene of peace and safety.
- Difficulty using progressive relaxation. If you’re having trouble isolating a muscle: touch it, stroke it with your hands, and then tense it fully (without strain) and feel the tension in your hands; feel the difference with your hands as you let go of the tension. Or, you may tighten only as much as is needed to feel the tension.
- The desire to stay in the imagery and not wanting to return to reality. If the imagery is much more pleasant than the present, use this process as a stimulus to reorganize your life and set new goals and priorities.
References
Ader, R. & Cohen, N. (1993). Psychoneuroimmunology, Conditioning,_and_Stress. Annual Review of Psychology, 44(1), 53-85.
Ader, R., Cohen, N. and Felten, D. (1995) Psychoneuroimmunology: Interactions between the Nervous System and the Immune System. The Lancet, 345, 99-103.
https://doi.org/10.1016/S0140-6736(95)90066-7
Friedman, L. F. (2015). A radical experiment tried to make old people young again–and the results were astonishing . https://www.businessinsider.com/ellen-langers-reversing-aging-experiment-2015-4
Grierson, B. (2014). What if age is nothing more than a mind-set? New York Times Magazine. October 22.
Langer, E. (2009). Counterclockwise: Mindful Health and the Power of Possibility . New York: Ballantine Books.
McKenzie, J. (1886). The production of the so-called rose effect by means of an artificial rose, with remarks and historical notes. Am. J. Med. Sci. 91, 45–57
Peper, E., Gibney, K.H. & Holt. C. (2002). Make Health Happen: Training Yourself to Create Wellness . Dubuque, IA: Kendall-Hunt. ISBN-13: 978-0787293314
Peper, E. & Harvey, R. (2017). The fallacy of placebo controlled clinical trials: Are positive outcomes the result of indirect treatment side effects? NeuroRegulation. 4(3–4), 102–113. doi:10.15540/nr.4.3-4.102
Siegel, B. (2011, May). Remarkable recoveries. Retrieved from: http://berniesiegelmd.com/resources/articles/remarkable-recoveries/
Vits, S., Cesko, E., Enck, P., Hillen, U., Schadendorf, D., & Schedlowski, M. (2011). Behavioural conditioning as the mediator of placebo responses in the immune system. Philosophical Transactions: Biological Sciences, 366(1572), 1799–1807. http://www.jstor.org/stable/23035535
Today is a new day-a new beginning
Posted: December 31, 2018 Filed under: behavior, health, Pain/discomfort, self-healing, Uncategorized | Tags: dance, hope, joy, pain, regenration, spinal injury 3 CommentsIn a world of turmoil, it is often challenging to think that tomorrow can be different and better. Yet, each day is an opportunity to accept whatever happened in the past and look forward to the unfolding present. So often, we anticipate that the future will be the same or worse especially if we feel depressed, suffer from ongoing pain, chronic illness, family or work stress, etc. At those moments, we forget that yesterday’s memories may contribute to how we experience and interpret the future. Most of us do not know what the future will bring, thus be open to new opportunities for growth and well-being. For the New Year, adapt a daily ritual that I learned from a remarkable healer Dora Kunz.
Each morning when you get out of bed, take a few slow deep breaths. Then think of someone who you feel loved by and makes you smile whether your grandmother, aunt or dog. Then when you get up and put your feet on the ground, say out loud, “Today is a new day- a new beginning.”
Watch the following two videos of people for whom the future appeared hopeless and yet had the courage to transcend their limitations and offer inspiration and joy.
Janine Shepherd: A broken body isn’t a broken person. Cross-country skier Janine Shepherd hoped for an Olympic medal — until she was hit by a truck during a training bike ride. She shares a powerful story about the human potential for recovery. Her message: you are not your body, and giving up old dreams can allow new ones to soar.
Ma Li and Zhai Xiaowei: Hand in Hand. This is a video of a broadcast that originally aired on China’s English-language CCTV channel 9 during a modern dance competition in Beijing, China in 2007. This very unique couple–she without an arm, he without a leg–was one of the finalists among 7000 competitors in the 4th CCTV national dance competition. It is the first time a handicapped couple had ever entered the competition. They won the silver medal and became an instant national hit. The young woman, in her 30’s, was a dancer who had trained since she was a little girl. Later in life, she lost her entire right arm in an automobile accident and fell into a state of depression for a few years. After rebounding, she decided to team with a young man who had lost his leg in a farming accident as a boy and who was completely untrained in dance. After a long and sometimes agonizing training regimen, this is the result. The dance is performed by Ma Li (馬麗) and Zhai Xiaowei (翟孝偉). The music “Holding Hands” is composed by San Bao and choreographed by Zhao Limin.
Cell phone radio frequency radiation increases cancer risk*
Posted: November 12, 2018 Filed under: cancer, digital devices, self-healing, Uncategorized | Tags: cellphones, digital devices, Radio frequency radiation, technology 3 Comments
Be safe rather than sorry. Cellphone radio frequency radiation is harmful!
The National Toxicology Program (NTP) released on October 31, 2018 their final report on rat and mouse studies of radio frequency radiation like that used with cellphones. The $30 million NTP studies took more than 10 years to complete and are the most comprehensive assessments to date of health effects in animals exposed to Radio Frequency Radiation (RFR) with modulations used in 2G and 3G cell phones. 2G and 3G networks were standard when the studies were designed and are still used for phone calls and texting.
The report concluded there is clear evidence that male rats exposed to high levels of radio frequency radiation (RFR) like that used in 2G and 3G cell phones developed cancerous heart tumors, according to final reports. There was also some evidence of tumors in the brain and adrenal gland of exposed male rats. For female rats, and male and female mice, the evidence was equivocal as to whether cancers observed were associated with exposure to RFR.
“The exposures used in the studies cannot be compared directly to the exposure that humans experience when using a cell phone,” said John Bucher, Ph.D., NTP senior scientist. “In our studies, rats and mice received radio frequency radiation across their whole bodies. By contrast, people are mostly exposed in specific local tissues close to where they hold the phone. In addition, the exposure levels and durations in our studies were greater than what people experience.”
In the NTP study, the lowest exposure level used in the studies was equal to the maximum local tissue exposure currently allowed for cell phone users. This power level rarely occurs with typical cell phone use. The highest exposure level in the studies was four times higher than the maximum power level permitted. Butcher state, “We believe that the link between radio frequency radiation and tumors in male rats is real, and the external experts agreed.”
I interpret that their results support the previous–often contested–observations that brain cancers were more prevalent in high cell phone users especially on the side of the head they held the cellphone.
More some women who have habitually stashed their cell phone in their bra have been diagnosed with a rare breast cancer located beneath the area of the breast where they stored their cell phone. Watch the heart breaking TV interview with Tiffany. She was 21 years old when she developed breast cancer which was located right beneath the breast were she had kept her cell phone against her bare skin for the last 6 years.
While these rare cases could have occurred by chance, they could also be an early indicator of risk. Previously, most research studies were based upon older adults who have tended to use their mobile phone much less than most young people today. The average age a person acquires a mobile phone is ten years old (this data was from 2016 and many children now have cellphones even earlier). Often infants and toddlers are entertained by smartphones and tablets–the new technological babysitter. The possible risk may be much greater for a young people since their bodies and brains are still growing rapidly. I wonder if the antenna radiation may be one of the many initiators or promoters of later onset cancers. We will not know the answer; since, most cancer take twenty or more years to develop.
What can you do to reduce risk?
Act now and reduce the exposure to the antenna radiation by implementing the following suggestions:
- Keep your phone, tablet or laptop in your purse, backpack or briefcase. Do not keep it on or close to your body.
- Use the speakerphone or earphones with microphone while talking. Do not hold it against the side of your head, close to your breast or on your lap.
- Text while the phone is on a book or on a table away from your body.
- Put the tablet and laptop on a table and away from the genitals.
- Set the phone to airplane mode.
- Be old fashioned and use a cable to connect to your home router instead of relying on the WiFi connection.
- Keep your calls short and enjoy the people in person.
- Support legislation to label wireless devices with a legible statement of possible risk and the specific absorption rate (SAR) value. Generally, higher the SAR value, the higher the exposure to antenna radiation.
- Support the work by the Environmental Health Trust.
For an radio interview on this topic, listen to my interview on Deborah Quilter’s radio show. http://www.blogtalkradio.com/rsihelp/2018/11/20/why-you-should-keep-your-cell-phone-away-from-your-body-with-dr-erik-peper
For more information on NTP study see:
*The blog is adapted in part from the November 1, 2018 news release from the National Toxicology Program (NTP)1, National Institute of Environmental Health Sciences2, National Institute of Health (NIH)3.
- About the National Toxicology Program (NTP):NTP is a federal, interagency program headquartered at NIEHS, whose goal is to safeguard the public by identifying substances in the environment that may affect human health. For more information about NTP and its programs, visit niehs.nih.gov.
- About the National Institute of Environmental Health Sciences (NIEHS): NIEHS supports research to understand the effects of the environment on human health and is part of NIH. For more information on environmental health topics, visit niehs.nih.gov. Subscribe to one or more of the NIEHS news lists (www.niehs.nih.gov/news/newsroom/newslist/index.cfm) to stay current on NIEHS news, press releases, grant opportunities, training, events, and publications.
- About the National Institutes of Health (NIH):NIH, the nation’s medical research agency, includes 27 Institutes and Centers and is a component of the U.S. Department of Health and Human Services. NIH is the primary federal agency conducting and supporting basic, clinical, and translational medical research, and is investigating the causes, treatments, and cures for both common and rare diseases. For more information about NIH and its programs, visit nih.gov.
Breathing reduces acid reflux and dysmenorrhea discomfort
Posted: October 4, 2018 Filed under: Breathing/respiration, Pain/discomfort, posture, relaxation, self-healing, stress management, Uncategorized | Tags: acid reflux, dysmenorrhea, gastroesophageal reflux disease, GERD, menstrual cramps, PMS 14 CommentsPublished as: Peper, E., Mason, L., Harvey, R., Wolski, L, & Torres, J. (2020). Can acid reflux be reduced by breathing? Townsend Letters-The Examiner of Alternative Medicine, 445/446, 44-47. https://www.townsendletter.com/article/445-6-acid-reflux-reduced-by-breathing/
“Although difficult and going against my natural reaction to curl up in the response to my cramps, I stretched out on my back and breathed slowly so that my stomach got bigger with each inhalation. My menstrual pain slowly decreased and disappeared.
“For as long as I remember, I had stomach problems and when I went to doctors, they said, I had acid reflux. I was prescribed medication and nothing worked. The problem of acid reflux got really bad when I went to college and often interfered with my social activities. After learning diaphragmatic breathing so that my stomach expanded instead of my chest, I am free of my symptoms and can even eat the foods that previously triggered the acid reflux.”
In the late 19th earlier part of the 20th century many women were diagnosed with Neurasthenia. The symptoms included fatigue, anxiety, headache, fainting, light headedness, heart palpitation, high blood pressure, neuralgia and depression. It was perceived as a weakness of the nerves. Even though the diagnosis is no longer used, similar symptoms still occur and are aggravated when the abdomen is constricted with a corset or by stylish clothing (see Fig 1).

Figure 1. Wearing a corset squeezes the abdomen.
The constricted waist compromises the functions of digestion and breathing. When the person inhales, the abdomen cannot expand as the diaphragm is flattening and pushing down. Thus, the person is forced to breathe more shallowly by lifting their ribs which increases neck and shoulder tension and the risk of anxiety, heart palpitation, and fatigue. It also can contribute to abdominal discomfort since abdomen is being squeezed by the corset and forcing the abdominal organs upward. It was the reason why the room on top of stairs in the old Victorian houses was call the fainting room (Melissa, 2015).
During inhalation the diaphragm flattens and attempts to descend which increases the pressure of the abdominal content. In some cases this causes the stomach content to be pushed upward into the esophagus which could result in heart burn and acid reflux. To avoid this, health care providers often advice patients with acid reflux to sleep on a slanted bed with the head higher than their feet so that the stomach content flows downward. However, they may not teach the person to wear looser clothing that does not constrict the waist and prevent designer jean syndrome. If the clothing around the waist is loosened, then the abdomen may expand in all directions in response to the downward movement of the diaphragm during inhalation and not squeeze the stomach and thereby pushing its content upward into the esophagus.
Most people have experienced the benefits of loosening the waist when eating a large meal. The moment the stomach is given the room to spread out, you feel more comfortable. If you experienced this, ask yourself, “Could there be a long term cost of keeping my waist constricted?” A constricted waist may be as harmful to our health as having the emergency brake on while driving for a car.
We are usually unaware that shallow rapid breathing in our chest can contribute to symptoms such as anxiety, neck and shoulder tension, heart palpitations, headaches, abdominal discomfort such as heart burn, acid reflux, irritable bowel syndrome, dysmenorrhea and even reduced fertility (Peper, Mason, & Huey, 2017; Domar, Seibel, & Benson, 1990).
Assess whether you are at risk for faulty breathing
Stand up and observe what happens when you take in a big breath and then exhale. Did you feel taller when you inhaled and shorter/smaller when you exhaled?
If the answer is YES, your breathing pattern may compromise your health. Most likely when you inhaled you lifted your chest, slightly arched your back, tightened and raised your shoulders, and lifted your head up while slightly pulling the stomach in. When you exhaled, your body relaxed and collapsed downward and even the stomach may have relaxed and expanded. This is a dysfunctional breathing pattern and the opposite of a breathing pattern that supports health and regeneration as shown in figure 2.
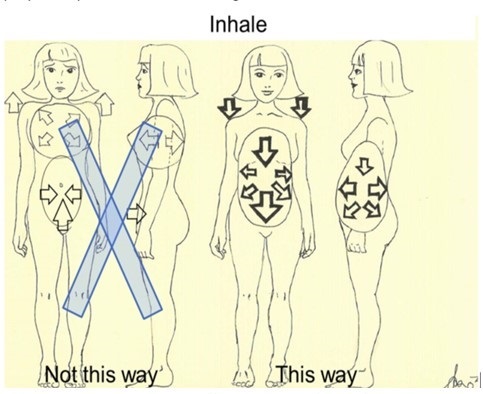
Figure 2. Incorrect and correct breathing. Source unknown.
Observe babies, young children, dogs, and cats when they are peaceful. The abdomen is what moves during breathing. While breathing in, the abdomen expands in all 360 degrees directions and when breathing out, the abdomen constricts and comes in. Similarly when dogs or cats are lying on their sides, their stomach goes up during inhalation and goes down during exhalation.
Many people tend to breathe shallowly in their chest and have forgotten—or cannot– allow their abdomen and lower ribs to widen during inhalation (Peper et al, 2016). These factors include:
- Constriction by the modern corset called “Spanx” to slim the figure or by wearing tight fitting pants. In either case the abdominal content is pushed upward and interferes with normal healthy breathing.
- Maintaining a slim figure by pulling the abdomen (I will look fat when my stomach expands; I will suck it in).
- Avoiding post-surgical abdominal pain by inhibiting abdominal movement. Numerous patients have unknowingly learned to shallowly breathe in their chest to avoid pain at the site of the incision of the abdominal surgery such as for hernia repair or a cesarean operation. This dysfunctional breathing became the new normal unless they actively practice diaphragmatic breathing.
- Slouching as we sit or watch digital screens or look down at our cell phone.
Observe how slouching affects the space in your abdomen.
When you shift from an upright erect position to a slouched or protective position the distance between your pubic bone and the bottom of the sternum (xiphoid process) is significantly reduced.
- Tighten our abdomen to protect ourselves from pain and danger as shown in Figure 3.

Figure 3. Erect versus collapsed posture. There is less space for the abdomen to expand in the protective collapsed position. Reproduced by permission from Clinical Somatics (http://www.clinicalsomatics.ie/).
Regardless why people breathe shallowly in their chest or avoid abdominal and lower rib movement during breathing, by re-establishing normal diaphragmatic breathing many symptoms may be reduced. Numerous students have reported that when they shift to diaphragmatic breathing which means the abdomen and lower ribs expand during inhalation and come in during exhalation as shown in Figure 4, their symptoms such as acid reflux and menstrual cramp significantly decrease.
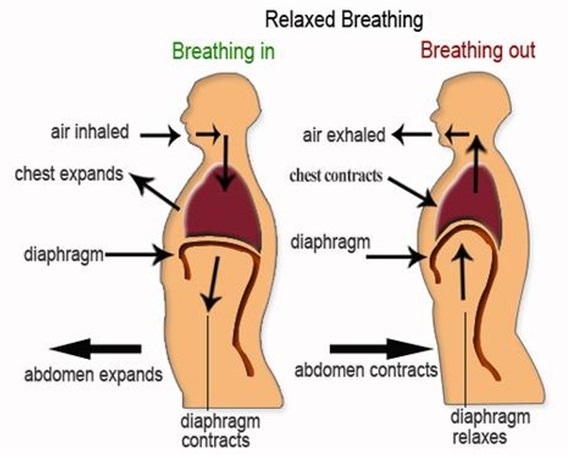
Figure 4. Diaphragmatic breathing. Reproduced from: www.devang.house/blogs/thejob/belly-breathing-follow-your-gut.
Reduce acid reflux
A 21-year old student, who has had acid reflux (GERD-gastroesophageal reflux diseases) since age 6, observed that she only breathed in her chest and that there were no abdominal movements. When she learned and practiced slower diaphragmatic breathing which allowed her abdomen to expand naturally during inhalation and reduce in size during exhalation her symptoms decreased. The image she used was that her lungs were like a balloon located in her abdomen. To create space for the diaphragm going down, she bought larger size pants so that her abdominal could spread out instead of squeezing her stomach (see Figure 5).
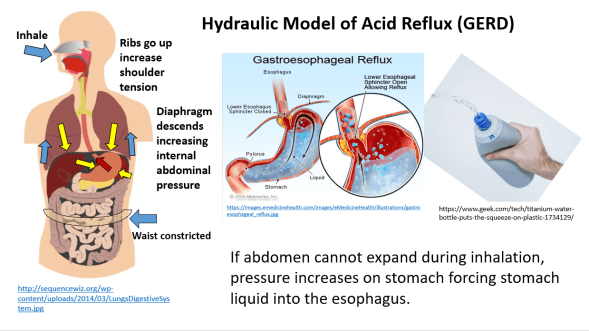
Figure 5. Hydraulic model who inhaling without the abdomen expanding increases pressure on the stomach and possibly cause stomach fluids to be pushed into the esophagus.
She practiced diaphragmatic breathing many times during the day. In addition, the moment she felt stressed and tightened her abdomen, she interrupted this tightening and re-established abdominal breathing. Practicing this was very challenging since she had to accept that she would still be attractive even if her stomach expanded during inhalation. She reported that within two weeks her symptom disappeared and upon a year follow-up she has had no more symptoms. In the video she describes her experiences of integrate breathing and awareness into daily life.
We have also use this similar approach to successfully overcome irritable bowel syndrome see: https://peperperspective.com/2017/06/23/healing-irritable-bowel-syndrome-with-diaphragmatic-breathing/
Take control of menstrual cramps
Numerous college students have reported that when they experience menstrual cramps, their natural impulse is to curl up in a protective cocoon. If instead they interrupted this natural protective pattern and lie relaxed on their back with their legs straight out and breathe diaphragmatically with their abdomen expanding and going upward during inhalation, they report a 50 percent decrease in discomfort (Gibney & Peper, 2003). For some the discomfort totally disappears when they place a warm pad on their lower abdomen and focused on breathing slowly about six breaths per minute so that the abdomen goes up when inhaling and goes down when exhaling. At the same time, they also imagine that the air would flow like a stream from their abdomen through their legs and out their feet while exhaling. They observed that as long as they held their abdomen tight the discomfort including the congestive PMS symptoms remained. Yet, the moment they practice abdominal breathing, the congestion and discomfort is decreased. Most likely the expanding and constricting of the abdomen during the diaphragmatic breathing acts as a pump in the abdomen to increase the lymph and venous blood return and improve circulation.
Conclusion
Breathing is the body-mind bridge and offers hope for numerous disorders. Slower diaphragmatic breathing with the corresponding abdomen movement at about six breaths per minute may reduce autonomic dysregulation. It has profound self-healing effects and may increase calmness and relaxation. At the same time, it may reduce heart palpitations, hypertension, asthma, anxiety, and many other symptoms.
References
DeVault, K.R. & Castell, D.O. (2005). Updated guidelines for the diagnosis and treatment of gastroesophageal reflux disease. The American Journal of Gastroenterology, 100, 190-200.
Domar, A.D., Seibel, M.M., & Benson, H. (1990). The Mind/Body Program for Infertility: a new behavioral treatment approach for women with infertility. Fertility and sterility, 53(2), 246-249.
Gibney, H.K. & Peper, E. (2003). Taking control: Strategies to reduce hot flashes and premenstrual mood swings. Biofeedback, 31(3), 20-24.
Johnson, L.F. & DeMeester, T.R. (1981). Evaluation of elevation of the head of the bed, bethanechol, and antacid foam tablets on gastroesophageal reflux. Digestive Diseases Sciences, 26, 673-680. https://www.ncbi.nlm.nih.gov/pubmed/7261830
Melissa. (2015). Why women fainted so much in the 19th century. May 20, 2015. Donloaded October 2, 1018. http://www.todayifoundout.com/index.php/2015/05/women-fainted-much-19th-century/
Peper, E., Booiman, A., Lin, I-M, Harvey, R., & Mitose, J. (2016). Abdominal SEMG Feedback for Diaphragmatic Breathing: A Methodological Note. Biofeedback. 44(1), 42-49.
Peper, E., Mason, L., Huey, C. (2017). Healing irritable bowel syndrome with diaphragmatic breathing. Biofeedback. (45-4)
Stanciu, C. & Bennett, J.R.. (1977). Effects of posture on gastro-oesophageal reflux. Digestion, 15, 104-109. https://www.karger.com/Article/Abstract/197991
Experience how thoughts affect body with lemon imagery*
Posted: July 25, 2018 Filed under: behavior, Breathing/respiration, emotions, relaxation, self-healing, Uncategorized | Tags: autonomic nervous system, Holistic health, Imagery, mind-body, salivation, visualization 2 CommentsMost of us are aware that thoughts affect our body; however, we often overlook the impact of this effect. To demonstrate the power of visualization, participants are guided through a lemon imagery. In a study with 131 college students, 94% report an increase in salivation which is a parasympathetic nervous system response. The participants now know–not believe–that visualization affects physiology. Once salivation has been experienced, participants may apply other visualization techniques to change their physiology and behavior. Through visualization we communicate with our autonomic nervous system which can provide a matrix for self-healing and enhanced performance. In addition, the guided practice shows that almost everyone holds their breath when asked to tighten their muscles and some people have difficulty relaxing after tightening. Once aware, the person can and continue to breathe and relax the muscles. Enjoy the guided exercise, Mindbody connection: Lemon Imagery.
*I thank Paul Godina, Jung Lee and Lena Stampfli for participating in the videos.
Adapted from Peper, E., Gibney, K.H. & Holt. C. (2002). Make Health Happen: Training Yourself to Create Wellness. Dubuque, IA: Kendall-Hunt
Be careful what you think*
Posted: July 23, 2018 Filed under: behavior, Exercise/movement, self-healing, stress management, Uncategorized | Tags: CBT, cognitive therapy, Mind body connection, muscle testing, performance, psyching out, somatic practices Leave a comment“I couldn’t belief it. I thought that I was strong and yet, I could not resist the downward pressure when I recalled a hopeless and helpless memory. Yet a minute later, I could easily resist the downward pressure on my arm when I thought of a positive and empower memory. I now understand how thoughts affect me.”
Thoughts/emotions affect body and body affects thoughts and emotions is the basis of the psychophysiological principle formulated by the biofeedback pioneers Elmer and Alice Green. The language we use, the thoughts we contemplate, the worries and ruminations that preoccupy us may impact our health.
Changing thoughts is the basis of cognitive behavior therapy and practitioners often teach clients to become aware of their negative thoughts and transform the internal language from hopeless, helpless, or powerless to empowered and positive. Think and visualize what you want and not what you do not want. For example, state, “I have studied and I will perform as best as I can” or “I choose to be a non-smoker instead of stating, “I hope I do not fail the exam” or “I want to stop smoking.” The more you imagine what you what in graphic detail, the more likely will it occur.
Most people rationally accept that thoughts may affect their body; however, it is abstract and not a felt experience. Also, some people have less awareness of the mind-body connection unless it causes discomfort. Our attention tends to be captured by visual and auditory stimuli that constantly bombard us so that we are d less aware of the subtle somatic changes.
This guided practice explores what happens when you recall helpless, hopeless, powerless or defeated memories as compared to recalling empowering positive memories. It allows a person to experience–instead of believing—how thoughts impact the body. 98% of participants felt significantly weaker after recalling the helpless, hopeless, powerless or defeated memories. Once the participants have experienced the effect, they realize how thoughts effect their body.
The loss of strength is metaphor of what may happen to our immune system and health. Do you want to be stronger or weaker? The challenge in transforming thoughts is that they occur automatically and we often doubt that we can change them. The key is to become aware of the onset of the thought and transform the thought. Thoughts are habit patterns and the more you practice a habit, the more it becomes automatic. Enjoy the experiential exercise, Mind-body/Bodymind-connection: Muscle testing.
*I thank Paul Godina, Jung Lee and Lena Stampfli for participating in the videos.
The practice was adapted from, Gorter, R. & Peper, E. (2011). Fighting Cancer-A Non Toxic Approach to Treatment. Berkeley: North Atlantic.
Cancer: What you can do to prevent and support healing
Posted: April 22, 2018 Filed under: cancer, self-healing, Uncategorized | Tags: cancer, healing, Holistic health, prevention, self-care, stress Leave a commentAre you curious to know if there is anything you can do to help prevent cancer?
Are you searching for ways to support your healing process and your immune system?
If yes, watch the invited lecture presented October 14, 2017, at the Caribbean Active Aging Congress, Oranjestad, Aruba, http://www.caacaruba.com
