How effective is treatment? The importance of active placebos
Posted: December 16, 2017 Filed under: Pain/discomfort, placebo, self-healing, stress management, Uncategorized | Tags: Active placebo, Clinical trials, expectancy, hope, nocebo, passive placebo, placebo 3 CommentsAdapted by Erik Peper and Richard Harvey from: Peper, E. & Harvey, R. (2017). The fallacy of the placebo-controlled clinical trials: Are positive outcomes the result of “indirect” treatment effects? NeuroRegulation, 4(3–4), 102–113. http://dx.doi.org/10.15540/nr.4.3-4.102
How come some drugs or medical procedures are initially acclaimed to be beneficial and later ineffective or harmful and withdrawn from the market?
How come some patients with a cancer diagnosis experience symptom remission after receiving a placebo medication? Take the case of Mr. Wright. Several decades ago Dr. Klopher (1957) described Mr. Wright as a patient who had a generalized and far advanced malignancy in the form of a lymphosarcoma with an estimated life expectancy of less than two weeks. Following the diagnosis Mr. Wright read a newspaper article about a promising experimental cancer medication called Krebiozen and requested that he receive the latest treatment. Soon after receiving the drug, Mr. Wright had a complete remission of cancer symptoms with no signs of the deadly tumor. For over two months after receiving the new promising drug, Krebiozen, Mr. Wright engaged in a normal life and was even able to fly his own plane at 12,000 feet. After a promising introduction to the medication, Mr. Wright subsequently read another newspaper article which proved the new medication to be a useless, inert preparation. Confused and demoralized, the results of the wonder drug did not last and his symptoms returned. When the final AMA announcement was published “Nationwide tests show Krebiozen to be a worthless drug in treatment of cancer,” his symptoms became acute and he died within two days (Klopher, 1957).
The term placebo loosely translates as ‘I shall please you’ can be contrasted with the term nocebo which loosely translates as ‘I shall harm you’ when referring to exposure to a sham medication, treatment or procedure that results a positive outcome (placebo response), or a negative outcome (nocebo response), respectively. The responses a person has reflect a complex interaction between many processes. For example, when studying a placebo or nocebo response we measure internal psychological processes, measured in terms of a person’s self-reported attitudes, beliefs, cognitions and emotions; behavioral processes, measured overtly by observations of a person’s actions; and, physiological processes, measured more or less directly with instruments such as heart rate monitors, or biochemical analyses. Most relevant is that a person’s beliefs about the placebo (or nocebo) medication, treatment or procedure leads to predictable positive (or negative) behaviors and physiological benefits or harms.
The case of Mr. Wright illustrates that we may underestimate the positive power of the placebo or, the negative power of the nocebo, where Mr. Wright’s belief about the medication’s benefits first interacted in a positive way (placebo) with his behaviors (e.g. engaging in daily activities including flying an airplane) as well as his physiology (e.g. cancer remission) and unfortunately later, in a negative way (nocebo) interacting with his physiology (e.g. cancer return) contributing to his death.
The placebo response can be very powerful and healing. For example, watch the very dramatic demonstration of how the placebo response can be optimized in Derren Brown’s BBC video Fear and Faith Placebo https://www.youtube.com/watch?v=y2XHDLuBZSw).
Placebo and nocebo effects are found in all therapeutic transactions when the communications between therapist and patient reflect embedded beliefs about the treatment. For example, patients have faith in clinician’s knowledge and belief that a prescribed medication is going to be effective at treating their symptoms, which then reinforces the patient’s belief in the medication, increasing indirect, embedded placebo effects, above and beyond any direct effects from the medication. The indirect effects of placebo responses have been most studied with medications; however, placebo effects are also studied in non-drug therapies. The research on placebo effects has demonstrated time and time again that when patients expect that the drug, surgery, or other therapeutic technique to be beneficial, then the patients tend to benefit more from the treatment.
The expectancy that the treatment will be effective at reducing symptoms is overtly, and covertly communicated by the health care professional during patient interactions, as well as by drug companies through direct to consumer advertising, and social media. The implied message is that the drug or procedure will improve symptoms, recovery or improve quality of life. On the other hand, if you do not do take the drug or do the procedure, your health will be compromised. For example, if you have high cholesterol, then take a statin drug to prevent the consequences of high cholesterol such as a heart attack or stroke. The implied message is that if you do not take it, you will die significantly sooner. Statins lower the risk for heart attacks; however, the benefits may be over stated. For people without prior heart disease, 60 people will have to take statins for 5 years to prevent 1 heart attack and 268 people to prevent 1 stroke. During the same time period 1 in 10 will experience muscle damage and 1 in 50 develop diabetes (theNNT, 2017 November).
If placebo and nocebo can have significant effects on medical outcome, how do you know if the treatment benefits are due to the direct effects of a drug or procedure or due to any indirect placebo effects or a combination of both?
The randomized controlled trial (RCT) is considered the gold standard method to determine the effectiveness of a drug or procedure. The ideal study would be a double blind, randomized, placebo controlled clinical trial in which neither the practitioner nor the patient would know who is getting what condition. For example, blinding implies the placebo group would receive a pill that appears identical to a ‘real’ pill, except the placebo has pharmacological ingredients. Similarly, a patient may receive an ‘exploratory’ surgery in which anesthesia is given and the skin is cut however the no further actual internal surgery occurs because the surgeon determined further internal surgery was unnecessary. Although, it is not possible to perform a double blind surgery study, the patient may be totally unaware whether an internal surgery had occurred.
Peper and Harvey (2017) point out that the positive findings of an ‘effective’ treatment are not always the results of the direct effects of medications and may be more attributable to indirect placebo responses. For example, patients may attribute the ‘effectiveness’ of the treatment to their experience of ‘non-directed’ treatment side effects that include: the post-surgical discomfort which signals to the patient that the procedure was successful, or a dry mouth and constipation that were caused by the antidepressant medication, which signals to the person that the trial medication or procedure-related medication is working (Bell, Rear, Cunningham, Dawnay, & Yellon, 2014; Stewart-Williams & Podd, 2004).
Just imagine the how pain can evoke totally different reactions. If you recently had a heart attack and then later experienced pain and cramping in the chest, you automatically may feel terrified as you could interpret the pain as another heart attack. The fear response to the pain may increase pathology and inhibit healing (a nocebo response). On the other hand, after bypass surgery, you may also experience severe pain when you move your chest. In this case, you interpret the pain as a sign that the bypass surgery was successful, which then reduces fear and reinforces the belief that you have survived a life threatening situation and will continue healing (placebo response).
Many research studies employ a placebo control, however what is less typical is a double-blind study using an ‘active’ placebo (Enck, Bingel, Schedlowski, & Rief, 2013). Less than 0.5% of all placebo studies include an active placebo group. (Shader, 2017; Jensen et al, 2017).
Unfortunately, a typical ‘placebo controlled’ study design is problematic for distinguishing the direct from any indirect (covert) placebo effects that occur within the study as shown in Figure 1.
 Figure 1. Normal (passive) placebo control group controls and experimental group. What is not assessed are placebo benefits induced by the medication/treatment induced side effects.
Figure 1. Normal (passive) placebo control group controls and experimental group. What is not assessed are placebo benefits induced by the medication/treatment induced side effects.
With a passive placebo, there is no way to know if the observed benefits are from the medication/medical procedure, or from the placebo/self-healing response triggered by the medication/medical procedure (or both combined, or neither the placebo or medical procedure). The best way to know if the treatment is actually beneficial is to use an ‘active’ placebo instead of a passive placebo.
An active placebo builds on a patient’s attributions about a medication or medical procedure. For example, a patient may be told by a clinician that feeling any side effects such as insomnia, a racing heart or, experiencing a warm flushing feeling will let them know the medication is working, so the patient becomes conditioned to expect the medication is working when they feel or experience side effects. Whereas a passive (inert) placebo such as a sugar pill will have effects that are extremely subtly felt or experienced, an active placebo will have effects that are more overtly felt or experienced. Examples of active placebos include administering low doses of caffeine or niacin that have effects which may be felt internally however which do not have the same effects as the medication. When a patient is told they may have side effects from the medication that include felt changes in heart rate or a flushing feeling, the patient attributes the changes they feel to a medication they believe will bring about benefits, even though the changes are rightfully attributed to the caffeine or niacin in the active placebo.
An active placebo triggers observed and felt body changes which do not affect the actual illness. For surgical procedures, an ‘active’ placebo control would be a sham/mock surgery in which the patient would undergo the same medical procedure (e.g. external surgery incision) without continuing some internal surgical procedure (Jonas et al, 2015). In numerous cases of accepted surgery, such as the Vineberg procedure (Vineburg & Miller, 1951) for angina, or arthroscopic knee surgery for treating osteoarthritis, the clinical benefits of a sham/mock surgery were just as successful as the actual surgery. Similar studies suggest the clinical benefits were solely (or primarily) due directly to the placebo response (Beecher, 1961; Cobb et al, 1959; Moseley et al, 2002).
To persuasively demonstrate that a treatment or therapeutic procedure is effective it should incorporate a study design using an active placebo arm as shown in Figure 2. Figure 2. Active placebo control group controls for the normal placebo benefits plus those placebo benefits induced by the medication/treatment induced side effects.
Figure 2. Active placebo control group controls for the normal placebo benefits plus those placebo benefits induced by the medication/treatment induced side effects.
Some treatments may be less effective then claimed because they were not compared to an active placebo, which could be one of the reasons why so many medical and psychological studies cannot be replicated. The absence of ‘active’ placebo controls may also be a factor explaining why some respected authorities have expressed some doubt about published scientific medical research results. Following are two quotes that illustrate such skepticism.
“Much of the scientific literature, perhaps half, may simply be untrue.” —Richard Horton, editor-in-chief of the Lancet (Horton, 2015).
“It is simply no longer possible to believe much of the clinical research that is published, or to rely on the judgment of trusted physicians or authoritative medical guidelines. I take no pleasure in this conclusion, which I reached slowly and reluctantly over my two decades as an editor of the New England Journal of Medicine” —Dr. Marcia Angell, longtime Editor in Chief of the New England Medical Journal (Angell, 2009).
There are a variety of questions to ask before agreeing on a procedure or before taking medication
A quick way to ask whether a medication or medical treatment effectiveness is the result of placebo components is to ask the following questions:
- Have there been successful self-care or behavioral approaches beyond surgical or pharmaceutical treatments that have demonstrated effectiveness? When successful treatments are reported, then questions are raised whether pharmaceutical or surgical outcomes are also attributable to the result of placebo effects. On the other hand, if there a no successful self-care approaches, then the benefits may be more due to the direct therapeutic effect of a surgical procedure or medication.
- Has the procedure been compared to an active placebo control? If not, then to what extent it is possible that the results of the surgical or pharmaceutical therapy could be attributed to a placebo response instead of directly to the medication or surgery?
- What are the long term benefits and complication rates of the medication, treatment or procedure? When benefits are low and risks of the procedure are high, explore the risks associated with ‘watchful waiting’ (Colloca, Pine, Ernst, Miller & Grillon, 2016; Thomas et al, 2014; Taleb, 2012).
Unfortunately, most clinical studies that includes pharmaceuticals and/or surgery do not test their medication, surgery against an ‘active’ placebo. Whenever possible, enquire whether an active placebo was used to determine the degree of effectiveness of the proposed treatment or procedure. Fortunately, the design of ‘active’ placebo-controlled studies is very possible for anyone interested in comparing the effectiveness of medications, treatments and procedures in various settings, from hospitals and clinics to university classrooms and individual homes.
In summary, the benefits of the treatment must significantly outweigh any risks of negative treatment side effects. Short-term treatment benefits need to be balanced by any long-term benefits. Unfortunately, short-term benefits may lead to significant, long-term harm such as in the use of some medications (e.g. sleep medications, opioid pain killers) that result in chronic dependency and which lead to a significant increase in morbidity and mortality of many kinds. We suggest that more medications and other procedures are tested against an active placebo to investigate whether the medication or procedure is actually effective.
For a detailed analysis and discussion of placebo and the importance of active placebo see our article, Peper, E. & Harvey, R. (2017). The fallacy of the placebo-controlled clinical trials: Are positive outcomes the result of “indirect” treatment effects? NeuroRegulation, 4(3–4), 102–113. http://dx.doi.org/10.15540/nr.4.3-4.102
References:
Angell M. Drug companies and doctors: A story of corruption. January 15, 2009. The New York Review of Books 56. Available: http://www.nybooks.com/articles/archives/2009/jan/15/drug-companies-doctorsa-story-of-corruption/. Accessed 24, November, 2016.
Beecher, H. K. (1961). Surgery as placebo: A quantitative study ofbias. JAMA, 176(13), 1102–1107. http://dx.doi.org/10.1001/jama.1961.63040260007008
Bell, R. M., Rear, R., Cunningham, J., Dawnay, A., & Yellon, D. M. (2014). Effect of remote ischaemic conditioning on contrast-induced nephropathy in patients undergoing elective coronary angiography (ERICCIN): rationale and study design of a randomised single-centre, double-blind placebo-controlled trial. Clinical Research in Cardiology, 103(3), 203-209. http://dx.doi.org/10.1007/s00392-013-0637-3
Cobb, L. A., Thomas, G. I., Dillard, D. H., Merendino, K. A., & Bruce, R. A. (1959). An evaluation of internal-mammary-artery ligation by a double-blind technic. New England Journal of Medicine, 260(22), 1115–1118. http://dx.doi.org/10.1056/NEJM195905282602204
Colloca, L., Pine, D. S., Ernst, M., Miller, F. G., & Grillon, C. (2016). Vasopressin boosts placebo analgesic effects in women: A randomized trial. Biological Psychiatry, 79(10), 794–802. http://dx.doi.org/10.1016/j.biopsych.2015.07.019
Derren Brown’s BBC video Fear and Faith Placebo https://www.youtube.com/watch?v=y2XHDLuBZSw
Enck, P., Bingel, U., Schedlowski, M., & Rief, W. (2013). The placebo response in medicine: minimize, maximize or personalize?. Nature reviews Drug discovery, 12(3), 191-204. http://dx.doi.org/10.1038/nrd3923
Horton, R. (2015). Offline: What is medicine’s 5 sigma. The Lancet, 385(9976), 1380. http://www.thelancet.com/pdfs/journals/lancet/PIIS0140-6736%2815%2960696-1.pdf
Jensen, J. S., Bielefeldt, A. Ø., & Hróbjartsson, A. (2017). Active placebo control groups of pharmacological interventions were rarely used but merited serious consideration: A methodological overview. Journal of Clinical Epidemiology. https://doi.org/10.1016/j.jclinepi.2017.03.001
Jonas, W. B., Crawford, C., Colloca, L., Kaptchuk, T. J., Moseley, B., Miller, F. G., & Meissner, K. (2015). To what extent are surgery and invasive procedures effective beyond a placebo response? A systematic review with meta-analysis of randomised, sham controlled trials. BMJ open, 5(12), e009655. http://dx.doi.org/10.1136/bmjopen-2015-009655
Klopfer, B., (1957). Psychological Variables in Human Cancer, Journal of Projective Techniques, 21(4), 331–340. http://www.tandfonline.com/doi/abs/10.1080/08853126.1957.10380794
Moseley, J. B., O’Malley, K., Petersen, N. J., Menke, T. J., Brody, B. A., Kuykendall, D. H., … Wray, N. P. (2002). A controlled trial of arthroscopic surgery for osteoarthritis of the knee. The New England Journal of Medicine. 347(2), 81–88. http://dx.doi.org/10.1056 /NEJMoa013259
Peper, E. & Harvey, R. (2017). The fallacy of the placebo-controlled clinical trials: Are positive outcomes the result of “indirect” treatment effects? NeuroRegulation, 4(3–4), 102–113. http://dx.doi.org/10.15540/nr.4.3-4.102
Shader, R. I. (2017). Placebos, Active Placebos, and Clinical Trials. Clinical Therapeutics, 39(3), 451–454. http://dx.doi.org/10.1016/j.clinthera.2017.02.001
Stewart-Williams, S., & Podd, J. (2004). The placebo effect: dissolving the expectancy versus conditioning debate. Psychological bulletin, 130(2), 324. http://dx.doi.org/10.1037/0033-2909.130.2.324
Taleb, N. N. (2012). Antifragile: Things that gain from disorder. Random House.
TheNNT (2017, November). http://www.thennt.com/nnt/statins-for-heart-disease-prevention-without-prior-heart-disease/
Thomas, R., Williams, M., Sharma, H., Chaudry, A., & Bellamy, P. (2014). A double-blind, placebo-controlled randomised trial evaluating the effect of a polyphenol-rich whole food supplement on PSA progression in men with prostate cancer—the UK NCRN Pomi-T study. Prostate Cancer and Prostatic Diseases, 17(2), 180–186. http://dx.doi.org/10.1038/pcan.2014.6
Vineberg, A., & Miller, G. (1951). Treatment of coronary insufficiency. Canadian Medical Association Journal, 64(3), 204. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1821866/pdf/canmedaj00654-0019.pdf
Overcoming obstacles
Posted: December 8, 2017 Filed under: self-healing, stress management, Uncategorized | Tags: deaf, healing, Inspiration, paraplegia, public speaking, singing 1 CommentIn a world with so much violence, inequalities and overwhelming negative news, it is easy to feel discouraged and forget that people can overcome trauma. Take charge of the news and images that surround us since the sounds and images impact our brain. Instead of watching disheartening and violent news before going to sleep, inspire yourself by watching the following two videos.
Muniba Mazari who at age 21 sustained spinal cord damage which left her paraplegic. She is an activist, motivational speaker and television host. https://www.youtube.com/watch?v=btb9wLkiKPE
Mandy Harvey who at age nineteen lost her hearing and is an outstanding American pop singer and songwriter. Even though she is deaf, she received Simon’s Golden Buzzer in America’s Got Talent 2017 while singing her original song. https://www.youtube.com/watch?v=ZKSWXzAnVe0
Posture affects memory recall and mood
Posted: November 25, 2017 Filed under: Exercise/movement, self-healing, stress management, Uncategorized | Tags: cognitive therapy, depression, empowerment, energy, helplessness, memory, mood, posture, power posture, somatics 5 CommentsThis blog has been reprinted from: Peper, E., Lin, I-M., Harvey, R., & Perez, J. (2017). How posture affects memory recall and mood. Biofeedback, 45 (2), 36-41.
When I sat collapsed looking down, negative memories flooded me and I found it difficult to shift and think of positive memories. While sitting erect, I found it easier to think of positive memories. -Student participant
 The link between posture and mood is embedded in idiomatic phrases such as walking tall, standing proud, and an upstanding citizen, versus collapsed, defeated, or in a slump–Language suggests that posture and mood/emotions are connected. Slumped posture is commonly observed in depression (Canales et al., 2010; Michalak et al., 2009) and adapting an upright posture increases positive affect, reduces fatigue, and increases energy in people with mild to moderate depression (Wilkes et al., 2017; Peper & Lin, 2012).
The link between posture and mood is embedded in idiomatic phrases such as walking tall, standing proud, and an upstanding citizen, versus collapsed, defeated, or in a slump–Language suggests that posture and mood/emotions are connected. Slumped posture is commonly observed in depression (Canales et al., 2010; Michalak et al., 2009) and adapting an upright posture increases positive affect, reduces fatigue, and increases energy in people with mild to moderate depression (Wilkes et al., 2017; Peper & Lin, 2012).
This blog describes in detail our research study that demonstrated how posture affects memory recall (Peper et al, 2017). Our findings may explain why depression is increasing the more people use cell phones. More importantly, learning posture awareness and siting more upright at home and in the office may be an effective somatic self-healing strategy to increase positive affect and decrease depression.
Background
Most psychotherapies tend to focus on the mind component of the body-mind relationship. On the other hand, exercise and posture focus on the body component of the mind/emotion/body relationship. Physical activity in general has been demonstrated to improve mood and exercise has been successfully used to treat depression with lower recidivism rates than pharmaceuticals such as sertraline (Zoloft) (Babyak et al., 2000). Although the role of exercise as a treatment strategy for depression has been accepted, the role of posture is not commonly included in cognitive behavior therapy (CBT) or biofeedback or neurofeedback therapy.
The link between posture, emotions and cognition to counter symptoms of depression and low energy have been suggested by Wilkes et al. (2017) and Peper and Lin (2012), . Peper and Lin (2012) demonstrated that if people tried skipping rather than walking in a slouched posture, subjective energy after the exercise was significantly higher. Among the participants who had reported the highest level of depression during the last two years, there was a significant decrease of subjective energy when they walked in slouched position as compared to those who reported a low level of depression. Earlier, Wilson and Peper (2004) demonstrated that in a collapsed posture, students more easily accessed hopeless, powerless, defeated and other negative memories as compared to memories accessed in an upright position. More recently, Tsai, Peper, and Lin (2016) showed that when participants sat in a collapsed position, evoking positive thoughts required more “brain activation” (i.e. greater mental effort) compared to that required when walking in an upright position.
Even hormone levels also appear to change in a collapsed posture (Carney, Cuddy, & Yap, 2010). For example, two minutes of standing in a collapsed position significantly decreased testosterone and increased cortisol as compared to a ‘power posture,’ which significantly increased testosterone and decreased cortisol while standing. As Professor Amy Cuddy pointed out in herTechnology, Entertainment and Design (TED) talk, “By changing posture, you not only present yourself differently to the world around you, you actually change your hormones” (Cuddy, 2012). Although there appears to be controversy about the results of this study, the overall findings match mammalian behavior of dominance and submission. From my perspective, the concepts underlying Cuddy’s TED talk are correct and are reconfirmed in our research on the effect of posture. For more detail about the controversy, see the article by Susan Dominusin in the New York Times, “When the revolution came for Amy Cuddy,”, and Amy Cuddy’s response (Dominus, 2017;Singal and Dahl, 2016).
The purpose of our study is to expand on our observations with more than 3,000 students and workshop participants. We observed that body posture and position affects recall of emotional memory. Moreover, a history of self-described depression appears to affect the recall of either positive or negative memories.
Method
Subjects: 216 college students (65 males; 142 females; 9 undeclared), average age: 24.6 years (SD = 7.6) participated in a regularly planned classroom demonstration regarding the relationship between posture and mood. As an evaluation of a classroom activity, this report of findings was exempted from Institutional Review Board oversight.
Procedure
While sitting in a class, students filled out a short, anonymous questionnaire, which asked them to rate their history of depression over the last two years, their level of depression and energy at this moment, and how easy it was for them to change their moods and energy level (on a scale from 1–10). The students also rated the extent they became emotionally absorbed or “captured” by their positive or negative memory recall. Half of the students were asked to rate how they sat in front of their computer, tablet, or mobile device on a scale from 1 (sitting upright) to 10 (completely slouched).
Two different sitting postures were clearly defined for participants: slouched/collapsed and erect/upright as shown in Figure 1. To assume the collapsed position, they were asked to slouch and look down while slightly rounding the back. For the erect position, they were asked to sit upright with a slight arch in their back, while looking upward.
 Figure 1. Sitting in a collapsed position and upright position (photo by Jana Asenbrennerova). Reprinted by permission from Gorter and Peper (2011).
Figure 1. Sitting in a collapsed position and upright position (photo by Jana Asenbrennerova). Reprinted by permission from Gorter and Peper (2011).
After experiencing both postures, half the students sat in the collapsed position while the other half sat in the upright position. While in this position, they were asked to recall/evoke as many hopeless, helpless, powerless, or defeated memories as possible, one after the other, for 30 seconds.
After 30 seconds they were reminded to keep their same position and let go of thinking negative memories. They were then asked to recall/evoke only positive, optimistic, or empowering memories for 30 seconds.
They were then asked to switch positions. Those who were collapsed switched to sitting erect, and those who were erect switched to sitting collapsed. Then they were again asked to recall/evoke as many hopeless, helpless, powerless, or defeated memories as possible one after the other for 30 seconds. After 30 seconds they were reminded to keep their same position and again let go of thinking of negative memories. They were then asked to recall/evoke only positive, optimistic, or empowering memories for 30 seconds, while still retaining the second posture.
They then rated their subjective experience in recalling negative or positive memories and the degree to which they were absorbed or captured by the memories in each position, and in which position it was easier to recall positive or negative experiences.
Results
86% of the participants reported that it was easier to recall/access negative memories in the collapsed position than in the erect position, which was significantly different as determined by one-way ANOVA (F(1,430)=110.193, p < 0.01) and 87% of participants reported that it was easier to recall/access positive images in the erect position than in the collapsed position, which was significantly different as determined by one-way ANOVA (F(1,430)=173.861, p < 0.01) as shown in Figure 2.
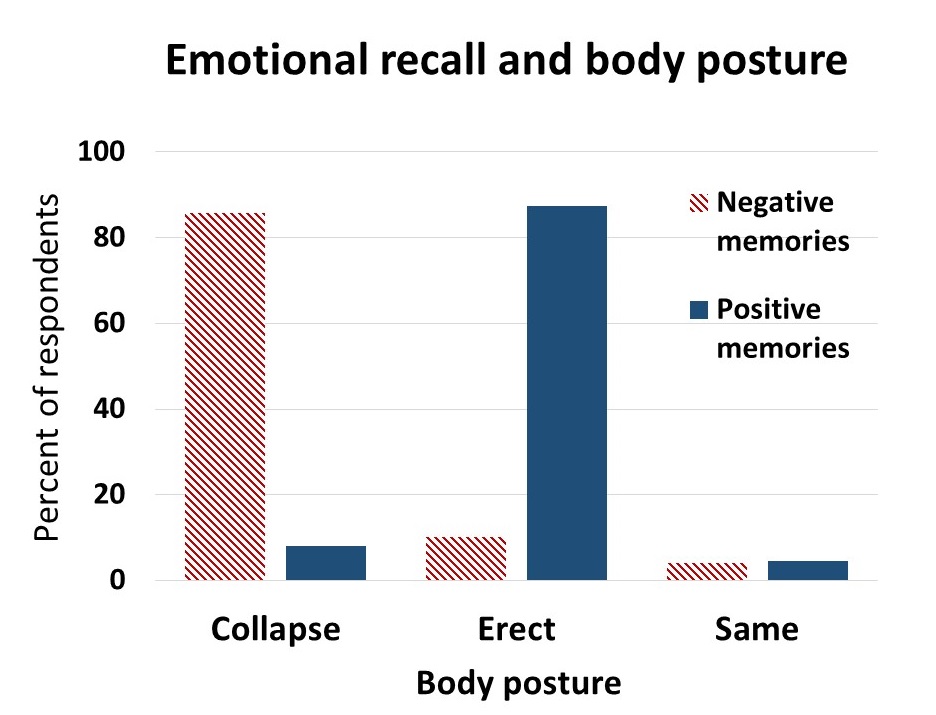 Figure 2. Percent of respondents who reported that it was easier to recall positive or negative memories in an upright or slouched posture.
Figure 2. Percent of respondents who reported that it was easier to recall positive or negative memories in an upright or slouched posture.
The difficulty or ease of recalling negative or positive memories varied depending on position as shown in Figure 3.
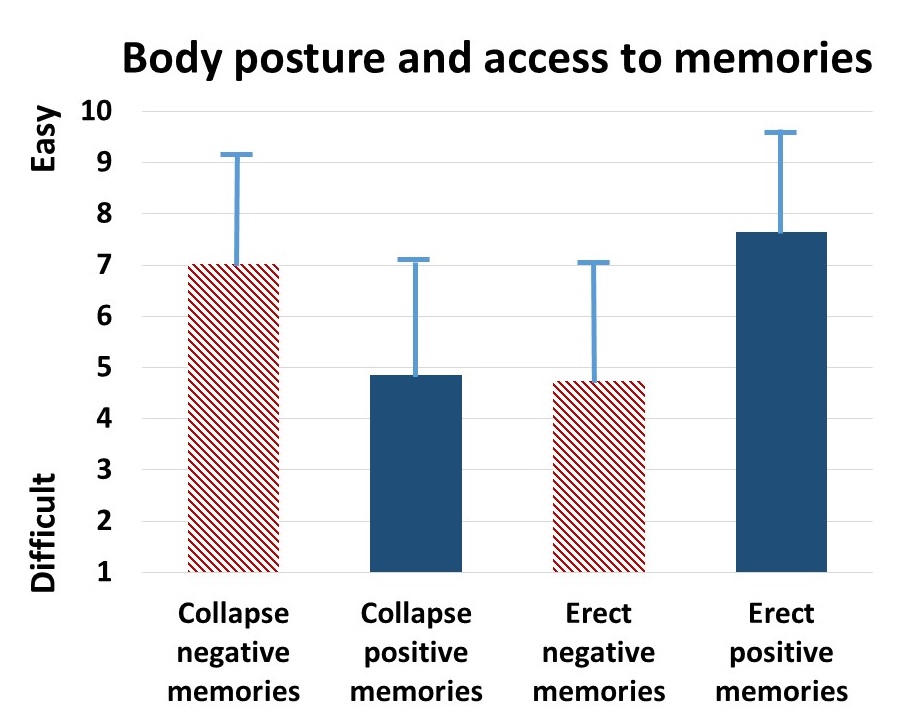 Figure 3. The relative subjective rating in the ease or difficulty of recalling negative and positive memories in collapsed and upright positions.
Figure 3. The relative subjective rating in the ease or difficulty of recalling negative and positive memories in collapsed and upright positions.
The participants with a high level of depression over the last two years (top 23% of participants who scored 7 or higher on the scale of 1–10) reported that it was significantly more difficult to change their mood from negative to positive (t(110) = 4.08, p < 0.01) than was reported by those with a low level of depression (lowest 29% of the participants who scored 3 or less on the scale of 1–10). It was significantly easier for more depressed students to recall/evoke negative memories in the collapsed posture (t(109) = 2.55, p = 0.01) and in the upright posture (t(110) = 2.41, p ≦0.05 he) and no significant difference in recalling positive memories in either posture, as shown in Figure 4.
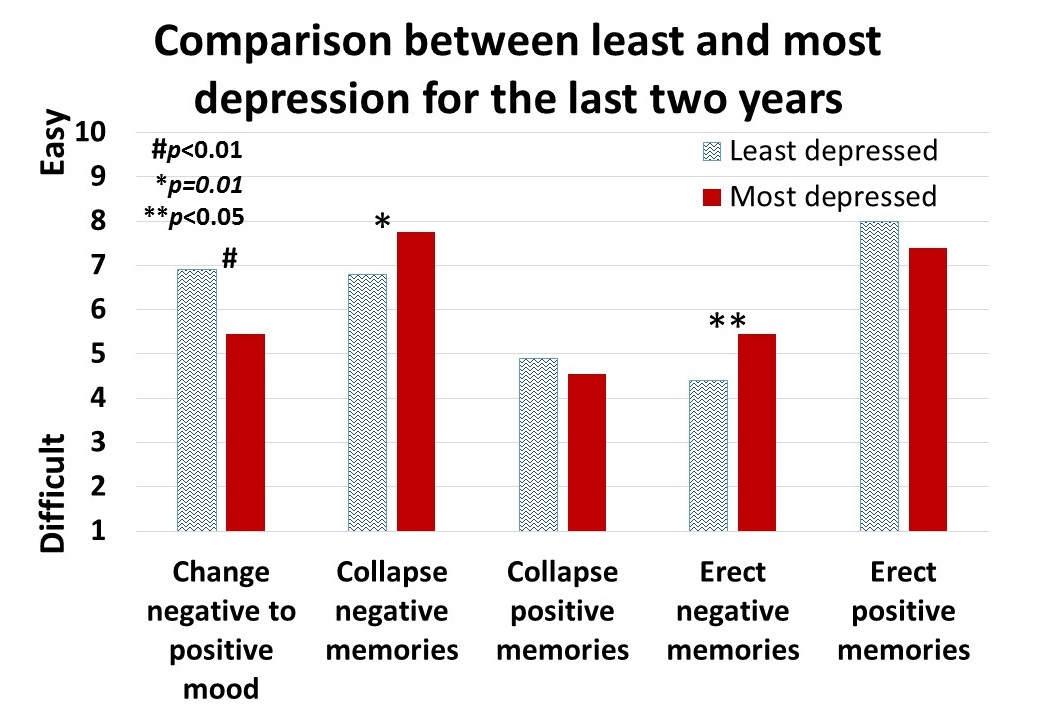 Figure 4. Differences is in memory access for participants with a history of least or most depression.
Figure 4. Differences is in memory access for participants with a history of least or most depression.
For all participants, there was a significant correlation (r = 0.4) between subjective energy level and ease with which they could change from negative to positive mood. There were no significance differences for gender in all measures except that males reported a significantly higher energy level than females (M = 5.5, SD = 3.0 and M = 4.7, SD = 3.8, respectively; t(203) = 2.78, p < 0.01).
A subset of students also had rated their posture when sitting in front of a computer or using a digital device (tablet or cell phone) on a scale from 1 (upright) to 10 (completely slouched). The students with the highest levels of depression over the last two years reporting slouching significantly more than those with the lowest level of depression over the last two years (M = 6.4, SD = 3.5 and M = 4.6, SD = 2.6; t(46) = 3.5, p < 0.01).
There were no other order effects except of accessing fewer negative memories in the collapsed posture after accessing positive memories in the erect posture (t(159)=2.7, p < 0.01). Approximately half of the students who also rated being “captured” by their positive or negative memories were significantly more captured by the negative memories in the collapsed posture than in the erect posture (t(197) = 6.8, p < 0.01) and were significantly more captured by positive memories in the erect posture than the collapsed posture (t(197) = 7.6, p < 0.01), as shown in Figure 5.
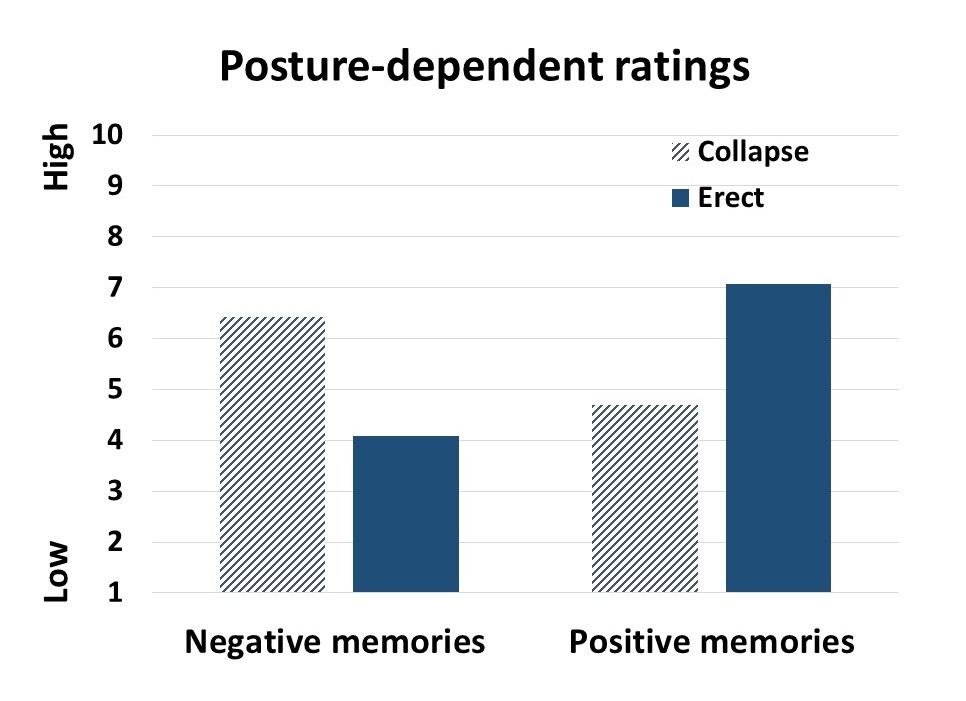 Figure 5. Subjective rating of being captured by negative and positive memories depending upon position.
Figure 5. Subjective rating of being captured by negative and positive memories depending upon position.
Discussion
Posture significantly influenced access to negative and positive memory recall and confirms the report by Wilson and Peper (2004). The collapsed/slouched position was associated with significantly easier access to negative memories. This is a useful clinical observation because ruminating on negative memories tends to decrease subjective energy and increase depressive feelings (Michi et al., 2015). When working with clients to change their cognition, especially in the treatment of depression, the posture may affect the outcome. Thus, therapists should consider posture retraining as a clinical intervention. This would include teaching clients to change their posture in the office and at home as a strategy to optimize access to positive memories and thereby reduce access or fixation on negative memories. Thus if one is in a negative mood, then slouching could maintain this negative mood while changing body posture to an erect posture, would make it easier to shift moods.
Physiologically, an erect body posture allows participants to breathe more diaphragmatically because the diaphragm has more space for descent. It is easier for participants to learn slower breathing and increased heart rate variability while sitting erect as compared to collapsed, as shown in Figure 6 (Mason et al., 2017).
 Figure 6. Effect of posture on respiratory breathing pattern and heart rate variability.
Figure 6. Effect of posture on respiratory breathing pattern and heart rate variability.
The collapsed position also tends to increase neck and shoulder symptoms This position is often observed in people who work at the computer or are constantly looking at their cell phone—a position sometimes labeled as the i-Neck.
Implication for therapy
In most biofeedback and neurofeedback training sessions, posture is not assessed and clients sit in a comfortable chair, which automatically causes a slouched position. Similarly, at home, most clients sit on an easy chair or couch, which lets them slouch as they watch TV or surf the web. Finally, most people slouch when looking at their cellphone, tablet, or the computer screen (Guan et al., 2016). They usually only become aware of slouching when they experience neck, shoulder, or back discomfort.
Clients and therapists are usually not aware that a slouched posture may decrease the client’s energy level and increase the prevalence of a negative mood. Thus, we recommend that therapists incorporate posture awareness and training to optimize access to positive imagery and increase energy.
References
Singal, J. and Dahl, M. (2016, Sept 30 ) Here Is Amy Cuddy’s Response to Critiques of Her Power-Posing Research. https://www.thecut.com/2016/09/read-amy-cuddys-response-to-power-posing-critiques.html
We thank Frank Andrasik for his constructive comments.
Breathing to improve well-being
Posted: November 17, 2017 Filed under: Breathing/respiration, Exercise/movement, Neck and shoulder discomfort, Pain/discomfort, self-healing, stress management, Uncategorized | Tags: anxiety, Breathing, health, mindfulness, pain, respiration, stress 9 CommentsBreathing affects all aspects of your life. This invited keynote, Breathing and posture: Mind-body interventions to improve health, reduce pain and discomfort, was presented at the Caribbean Active Aging Congress, October 14, Oranjestad, Aruba. www.caacaruba.com
The presentation includes numerous practices that can be rapidly adapted into daily life to improve health and well-being.
Be a tree and share gratitude
Posted: December 11, 2016 Filed under: Breathing/respiration, self-healing, stress management, Uncategorized | Tags: gratitude, Holistic health, Imagery, relaxation, self-healing, stress management 1 Comment
It was late in the afternoon and I was tired. A knock on my office door. One of my students came in and started to read to me from a card. “I want to thank you for all your help in my self-healing project…I didn’t know the improvements were possible for me in a span of 5 weeks…. I thank you so much for encouraging and supporting me…. I have taken back control of myself and continue to make new discoveries about my identity and find my own happiness and fulfillment… Thank you so much.”
I was deeply touched and my eyes started to fill with tears. At that moment, I felt so appreciated. We hugged. My tiredness disappeared and I felt at peace.
In a world where we are constantly bombarded by negative, fearful stories and images, we forget that our response to these stories impacts our health. When people watch fear eliciting videos, their heart rate increases and their whole body responds with a defense reaction as if they are personally being threatened (Kreibig, Wilhelm, Roth, & Gross, 2007). Afterwards, we may continue to interpret and react to new stimuli as if they are the same as what happened in the video. For example, while watching a horror movie, we may hold our breath, perspire and feel our heart racing; however, when we leave the theatre and walk down the street by ourselves, we continue to be afraid and react to stimuli as if what happened in video will now happen to us.
When we feel threatened, our body responds to defend itself. It reduces the blood flow to the gastrointestinal tract where digestion is taking place and sends it to large muscles so that we can run and fight. When threatened, most of our resources shifted to the processes that promote survival while withdrawing it from processes that do not lead to immediate survival such as digestion or regeneration (Sapolsky, 2004). From an evolutionary perspective, why spent resources to heal yourself, enhance your immune system or digest your food when you will become someone else’s lunch!
The more we feel threatened, the more we will interpret the events around us negatively. We become more stressed, defensive, and pessimistic. If this response occurs frequently, it contributes to increased morbidity and mortality. We may not be in control of external or personal event; however, we may be able to learn how to change our reactions to these events. It is our reactions and interpretations of the event that contributes to our ongoing stress responses. The stressor can be labeled as crisis or opportunity.
Mobilize your own healing when you take charge. When 92 students as part of a class at San Francisco State University practiced self-healing skill, most reported significant improvements in their health as shown in Figure 1.
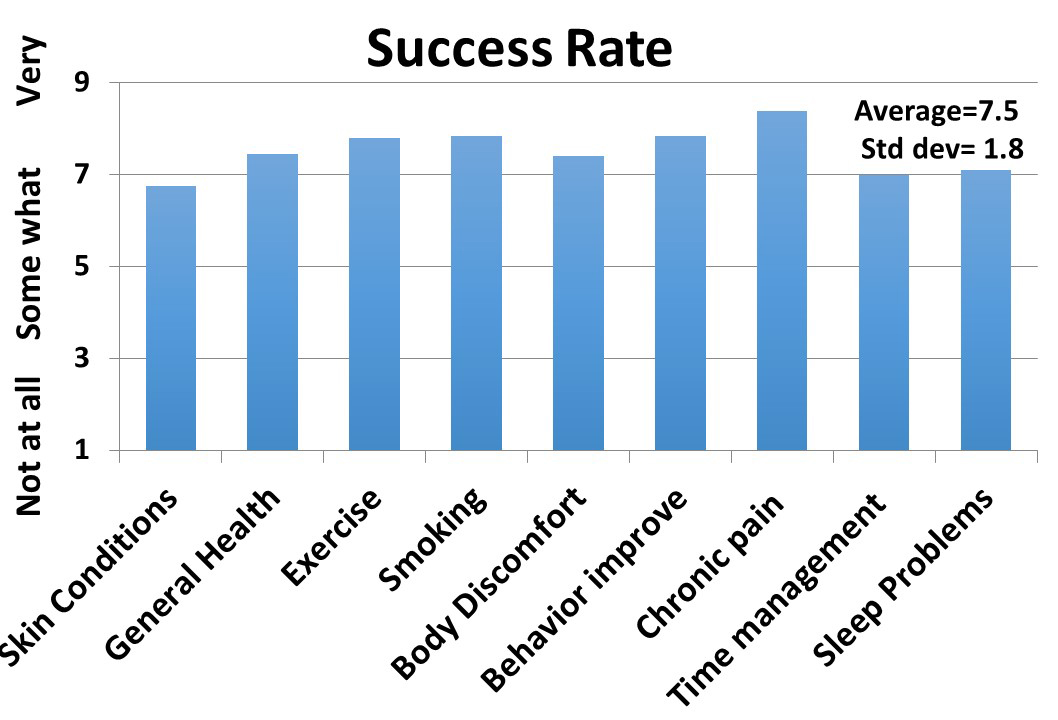
Figure 1. Average self-reported improvement after practicing self-healing skills for at least four weeks. (Reproduced with permission from Tseng, Abili, Peper, & Harvey, 2016).
A strategy that many students used was to interrupt their cascading automatic negative reactions. The moment they became aware of their negative thought and body slumping, they interrupted the process and practiced a very short relaxation or meditation technique.
Implement what the students have done by taking charge of your stress responses and depressive thoughts by 1) beginning the day with a relaxation technique, Relax Body-Mind, 2) interrupting the automatic response to stressors with a rapid stress reduction technique, Breathe and be a Tree, and 3) increasing vitality by the practice, Share Gratitude (Gorter & Peper, 2011).
Relax Body-Mind to start the day*
- Lie down or sit and close your eyes. During the practice if your attention wanders, just bring it back to that part of the body you are asked to tighten or let go.
- Wrinkle your face for ten seconds while continuing to breathe. Let go and relax for ten seconds.
- Bring your hands to your face with the fingers touching the forehead while continuing to breathe. While exhaling, pull your fingers down your face so that you feel your jaw being pulled down and relaxing. Drop your hands to your lap. Feel the sensations in your face and your fingers for ten seconds.
- Make a fist with your hands and lift them slightly up from your lap while continuing to breathe. Feel the sensations of tension in your hands, arms and shoulders for ten seconds. Let go and relax by allowing the arms to drop to your lap and relax. Feel the sensations change in your hands, arms and shoulders for ten seconds.
- Tighten your buttocks and flex your ankles so that the toes are reaching upwards to your knees. Hold for ten seconds while continuing to breathe. Let go and relax for ten seconds.
- Take a big breath while slightly arching your back away from the bed ore chair and expand your stomach while keeping your arms, neck, buttocks and legs relaxed. Hold the breath for twenty seconds. Exhale and let your back relax while allowing the breathing to continue evenly while sensing your body’s contact with the bed or chair for twenty seconds. Repeat three times.
- Gently shake your arms and legs for ten seconds while continuing to breathe. Let go and relax. Feel the tingling sensations in your arms and legs for 20 seconds.
- Evoke a past positive memory where you felt at peace and nurtured.
- Stretch and get up. Know you have done the first self-healing step of the day.
*Be gentle to yourself and stop the tightening or breath holding if it feels uncomfortable.
Breathe and be a Tree to dissipate stress and focus on growth
- Look at a tall tree and realize that you are like a tree that is rooted in the ground and reaching upward to the light. It continues to grow even though it has been buffeted by storms.
- When you become aware of being stressed, exhale slowly and inhale so that your stomach expands, the while slowly exhaling, look upward to the top of a real or imagined tree, admire the upper branches and leaves that are reaching towards the light and smile.
- Remember that even though you started to respond to a stressor, the stressor will pass just like storms battering the tree. By breathing and looking upward, accept what happened and know you are growing just like the tree.
Share Gratitude to increase vitality and health (adapted from Professor Martin Seligman’s 2004 TED presentation, The new era of positive psychology).
- Think of someone who did something for you that impacted your life in a positive direction and whom you never properly thanked. This could be a neighbor, teacher, friend, parent, or other family members.
- Write a 300-word testimonial describing specifically what the person did and how it positively impacted you and changed the course of your life.
- Arrange an actual face-to-face meeting with the person. Tell them you would like to see him/her. If they are far away, arrange a Skype call where you can actually see and hear him/her. Do not do it by email or texting.
- Meet with the person and read the testimonial to her/him.
- It may seem awkward to read the testimonial, after you have done it, you will feel closer and more deeply connected to the person. Moreover, the person to whom you read the testimonial, will usually feel deeply touched. Both your hearts will open.

References:
Gorter, R. & Peper, E. (2011). Fighting cancer: A nontoxic approach to treatment. Berkeley, CA: North Atlantic Books, 205-207.
Kreibig, S. D., Wilhelm, F. H., Roth, W. T., & Gross, J. J. (2007). Cardiovascular, electrodermal, and respiratory response patterns to fear‐and sadness‐inducing films. Psychophysiology, 44(5), 787-806.Kreibig, Sylvia D., Frank H. Wilhelm, Walton T. Roth, and James J. Gross. “Cardiovascular, electrodermal, and respiratory response patterns to fear‐and sadness‐inducing films.” Psychophysiology 44, no. 5 (2007): 787-806.
Sapolsky, R. (2004). Why Zebras Don’t Get Ulcers. New York: Owl Books
Seligman, M. (2014). The new era of positive psychology. Ted Talk. Retrieved, December 10, 2016. https://www.ted.com/talks/martin_seligman_on_the_state_of_psychology
Tseng, C., Abili, R., Peper, E., & Harvey, R. (2016). Reducing Acne-Stress and an integrated self-healing approach. Appl Psychophysiol Biofeedback, 4(4), 445.)
Education versus treatment for self-healing: Eliminating a headache[1]
Posted: November 18, 2016 Filed under: Pain/discomfort, self-healing, stress management, Uncategorized | Tags: autogenic training, biofeedback, education, electromyography, headache, Holistic health, migraine, posture, treatment 3 Comments“I have had headaches for six years, at first occurring almost every day. When I got put on an antidepressant, they slowed to about 3 times a week (sometimes more) and continued this way until I learned relaxation techniques. I am 20 years old and now headache free. Everyone should have this educational opportunity to heal themselves.” -Melinda, a 20 year old student
Health and wellness is a basic right for all people. When students learn stress management skills which include awareness of stress, progressive muscle relaxation, Autogenic phrases, slower breathing, posture change, transforming internal language, self-healing imagery, the role of diet, exercise embedded within an evolutionary perspective as part of a college class their health often improves. When students systematically applied these self-awareness techniques to address a self-selected illness or health behavior (e.g., eczema, diet, exercise, insomnia, or migraine headaches), 80% reported significant improvement in their health during that semester (Peper et al., 2014b; Tseng, et al., 2016). The semester long program is based upon the practices described in the book, Make Health Happen, (Peper, Gibney, & Holt, 2002).
The benefits often last beyond the semester. Numerous students reported remarkable outcomes at follow-up many months after the class had ended because they had mastered the self-regulation skills and continued to implement these skills into their daily lives. The educational model utilized in holistic health courses is often different from the clinical/treatment model.
Educational approach: I am a student and I have an illness (most of me is healthy and only part of me is sick).
Clinical treatment approach: I am a patient and I am sick (all of me is sick)
Some of the concepts underlying the differences between the educational and the clinical approach are shown in Table 1.
| Educational approach | Clinic/treatment approach |
| Focuses on growth and learning | Focuses on remediation |
| Focuses on what is right | Focuses on what is wrong |
| Focuses on what people can do for themselves | Focuses on how the therapist can help patients |
| Assumes students as being competent | Implies patients are damaged and incompetent |
| Students defined as being competent to master the skills | Patients defined as requiring others to help them |
| Encourages active participation in the healing process | Assumes passive participation in the healing process |
| Students keep logs and write integrative and reflective papers, which encourage insight and awareness | Patients usually do not keep logs nor are asked to reflect at the end of treatment to see which factors contributed to success |
| Students meet in small groups, develop social support and perspective | Patients meet only with practitioners and stay isolated |
| Students experience an increased sense of mastery and empowerment | Patients experience no change or possibly a decrease in sense of mastery |
| Students develop skills and become equal or better than the instructor | Patients are healed, but therapist is always seen as more competent than patient |
| Students can become colleagues and friends with their teachers | Patients cannot become friends of the therapist and thus are always distanced |
Table 1. Comparison of an educational versus clinical/treatment approach
The educational approach focuses on mastering skills and empowerment. As part of the course work, students become more mindful of their health behavior patterns and gradually better able to transform their previously covert harm promoting patterns. This educational approach is illustrated in a case report which describes how a student reduced her chronic migraines.
Case Example: Elimination of Chronic Migraines
Melinda, a 20-year-old female student, experienced four to five chronic migraines per week since age 14. A neurologist had prescribed several medications including Imitrex (used to treat migraines) and Topamax (used to prevent seizures as well as migraine headaches), although they were ineffective in treating her migraines. Nortriptyline (a tricyclic antidepressant) and Excedrin Migraine (which contains caffeine, aspirin, and acetaminophen) reduced the frequency of symptoms to three times per week.
She was enrolled in a university biofeedback class that focused on learning self-regulation and biofeedback skills. All these students were taught the fundamentals of biofeedback and practiced Autogenic Training (AT) every day during the semester (Luthe, 1979; Luthe & Schultz, 1969; Peper & Williams, 1980).
In the class, students practiced with surface electromyography (SEMG) feedback to identify the presence of shoulder muscle overexertion (dysponesis), as well as awareness of minimum muscle tension. Additional practices included hand warming, awareness of thoracic and diaphragmatic breathing, and other biofeedback or somatic awareness approaches. In parallel with awareness of physical sensations, students practiced behavioral awareness such as alternating between a slouching body posture (associated with feeling self-critical and powerless) and an upright body posture (associated with feeling powerful and in control). Psychological awareness was focused on transforming negative thoughts and self-judgments to positive empowering thoughts (Harvey and Peper, 2011; Peper et al., 2014a; Peper et al, 2015). Taken together, students systematically increased awareness of physical, behavioral, and psychological aspects of their reactions to stress.
The major determinant for success is to generalize training at school, home and at work. Each time Melinda felt her shoulders tightening, she learned to relax and release the tension in her shoulders, practiced Autogenic Training with the phrase “my neck and shoulders are heavy.” In addition, whenever she felt her body beginning to slouch or noticed a negative self-critical thought arising in her mind, she shifted her body to an upright empowered posture, and substituted positive thoughts to reduce her cortisol level and increase access to positive thoughts (Carney & Cuddy, 2010; Cuddy, 2012; Tsai, et al., 2016). Postural feedback was also informally given by Melinda’s instructor. Every time the instructor noticed her slouching in class or the hallway, he visually changed his own posture to remind her to be erect.
Results
Melinda’s headaches reduced from between three and five per week before enrolling in the class to zero following the course, as shown in Figure 2. She has learned to shift her posture from slouching to upright and relaxed. In addition, she reported feeling empowered, mentally clear, and her acne cleared up. All medications were eliminated. At a two year follow-up, she reported that since she took the class, she had only few headaches which were triggered by excessive stress. 
Figure 2. Frequency of migraine and the implementation of self-practices.
The major factors that contributed to success were:
- Becoming aware of muscle tension through the SEMG feedback. Melinda realized that she had tension when she thought she was relaxed.
- Keeping detailed logs and developing a third person perspective by analyzing her own data and writing a report. A process that encouraged acceptance of self, thereby becoming less judgmental.
- Acquiring a new belief that she could learn to overcome her headaches, facilitated by class lecture and verbal feedback from the instructor.
- Taking active control by becoming aware of the initial negative thoughts or sensations and interrupting the escalating chain of negative thoughts and sensations by shifting the attention to positive empowering thoughts and sensations–a process that integrated mindfulness, acceptance and action. Thus, transforming judgmental thoughts into accepting and positive thoughts.
- Becoming more aware throughout the day, at school and at home, of initial triggers related to body collapse and muscle tension, then changing her body posture and relaxing her shoulders. This awareness was initially developed because the instructor continuously gave feedback whenever she started to slouch in class or when he saw her slouching in the hallways.
- Practicing many, many times during the day. Namely, increasing her ongoing mindfulness of posture, neck, and shoulder tension, and of negative internal dialogue without judgment.
The benefits of this educational approach is captured by Melinda’s summary, “The combined Autogenic biofeedback awareness and skill with the changes in posture helped me remarkably. It improved my self-esteem, empowerment, reduced my stress, and even improved the quality of my skin. It proves the concept that health is a whole system between mind, body, and spirit. When I listen carefully and act on it, my overall well-being is exceptionally improved.”
References:
Carney, D. R., Cuddy, A. J., & Yap, A. J. (2010). Power posing brief nonverbal displays affect neuroendocrine levels and risk tolerance. Psychological Science, 21(10), 1363-1368.
Cuddy, A. (2012). Your body language shapes who you are. Technology, Entertainment, and Design (TED) Talk, available at: http://www.ted.com/talks/amy_cuddy_your_body_language_shapes_who_you_are
Harvey, E. & Peper, E. (2011). I thought I was relaxed: The use of SEMG biofeedback for training awareness and control (pp. 144-159). In W. A. Edmonds, & G. Tenenbaum (Eds.), Case studies in applied psychophysiology: Neurofeedback and biofeedback treatments for advances in human performance. West Sussex, UK: Wiley-Blackwell.
Luthe, W. (1979). About the methods of autogenic therapy (pp. 167-186). In E. Peper, S. Ancoli, & M. Quinn, Mind/body integration. New York: Springer.
Luthe, W., & Schultz, J.H. (1969). Autogenic therapy (Vols. 1-6). New York, NY: Grune and Stratton.
Peper, E., Booiman, A., Lin, I-M., & Shaffer, F. (2014a). Making the unaware aware-Surface electromyography to unmask tension and teach awareness. Biofeedback. 42(1), 16-23.
Peper, E., Gibney, K.H. & Holt. C. (2002). Make health happen: Training yourself to create wellness. Dubuque, IA: Kendall-Hunt. ISBN-13: 978-0787293314
Peper, E., Lin, I-M, Harvey, R., Gilbert, M., Gubbala, P., Ratkovich, A., & Fletcher, F. (2014b). Transforming chained behaviors: Case studies of overcoming smoking, eczema and hair pulling (trichotillomania). Biofeedback, 42(4), 154-160.
Peper, E., Nemoto, S., Lin, I-M., & Harvey, R. (2015). Seeing is believing: Biofeedback a tool to enhance motivation for cognitive therapy. Biofeedback, 43(4), 168-172. doi: 10.5298/1081-5937-43.4.03
Peper, E. & Williams, E.A. (1980). Autogenic therapy (pp. 131-137). In: A. C. Hastings, J. Fadiman, & J. S. Gordon (Eds.). Health for the whole person. Boulder: Westview Press.
Tsai, H. Y., Peper, E., & Lin, I. M. (2016). EEG patterns under positive/negative body postures and emotion recall tasks. NeuroRegulation, 3(1), 23-27.
Tseng, C., Abili, R., Peper, E., & Harvey, R. (2016). Reducing acne-stress and an integrated self-healing approach. Poster presented at the 47th Annual Meeting of the Association for Applied Psychophysiology and Biofeedback, Seattle WA, March 9-12, 2016.
[1] Adapted from: Peper, E., Miceli, B., & Harvey, R. (2016). Educational Model for Self-healing: Eliminating a Chronic Migraine with Electromyography, Autogenic Training, Posture, and Mindfulness. Biofeedback, 44(3), 130–137. https://biofeedbackhealth.files.wordpress.com/2011/01/a-educational-model-for-self-healing-biofeedback.pdf
Do you blank out on exams? Improve school performance with breathing* **
Posted: September 18, 2016 Filed under: Breathing/respiration, stress management, Uncategorized | Tags: anxiety, fear, gasping, math, memory, performance, respiration 3 Comments “I opened the exam booklet and I went blank.”
“I opened the exam booklet and I went blank.”
“When I got anxious, I took a slow breath, reminded myself that I would remember the material. I successfully passed the exam.”
“I was shocked, when I gasped, I could not remember my girlfriend’s name and then I could not remember my mother’s name. When breathed slowly, I had no problem and easily remembered both”
Blanking out the memorized information that you have studied on an exam is a common experiences of students even if they worked hard (Arnsten, Mazure, & Sinha, 2012). Fear and poor study habits often contribute to forgetting the material (Fitkov-Norris, & Yeghiazarian, 2013). Most students study while listening to music, responding to text message, or monitoring social network sites such as, Facebook, twitter, Instagram, or Pinterest (David et al., 2015).. Other students study the material for one class then immediately shift and study material from another class. While at home they study while sitting or lying on their bed. Numerous students have internalized the cultural or familial beliefs that math is difficult and you do not have the aptitude for the material—your mother and father were also poor in math (Cherif, Movahedzadeh, Adams, & Dunning, 2013). These beliefs and dysfunctional study habits limit learning (Neal, Wood, & Drolet, 2013).
Blanking out on an exam or class presentation is usually caused by fear or performance anxiety which triggers a stress response (Hodges, 2015; Spielberger, Anton, & Bedell, 2015). At that moment, the brain is flooded with thoughts such as, I can’t do it,” “I will fail,” “I used to know this, but…”, or “What will people think?” The body responds with a defense reaction as if you are being threatened and your survival is at stake. The emotional reactivity and anxiety overwhelms cognition, resulting in an automatic ‘freeze’ response of breath holding or very shallow breathing. At that moment, you blank out (Hagenaars, Oitzl, & Roelofs, 2014; Sink et al., 2013; Von Der Embse, Barterian, & Segool, 2013).
Experience how your thinking is affected by your breathing pattern. Do the following practice with another person.
Have the person ask you a question and the moment you hear the beginning of the question, gasp as if you are shocked or surprised. React just as quickly and automatically as you would if you see a car speeding towards you. At that moment of shock or surprise, you do not think, you don’t spend time identifying the car or look at who is driving. You reflexively and automatically jump out of the way. Similarly in this exercise, when you are asked to answer a question, act as if you are as shocked or surprised to see a car racing towards you.
Practice gasping at the onset of hearing the beginning of a question such as, “What day was it yesterday?” At the onset of the sound, gasp as if startled or afraid. During the first few practices, many people wait until they have heard the whole phrase before gasping. This would be similar to seeing a car racing towards you and first thinking about the car, at that point you would be hit. Repeat this a few times till it is automatic.
Now change the breathing pattern from gasping to slow breathing and practice this for a few times.
When you hear the beginning of the question breathe slowly and then exhale.” Inhale slowly for about 4 seconds while allowing your abdomen to expand and then exhale softly for about 5 or six seconds. Repeat practicing slow breathing in response to hearing the onset of the question until it is automatic.
Now repeat the two breathing patterns (gasping and slow breathing) while the person asks you a subtraction or math questions such as, “Subtract 7 from 93.”
In research with more than 100 college students, we found that students had significantly more self-reported anxiety and difficulty in solving math problems when gasping as compared to slow breathing as shown Figure 1 (Lee et al, 2016; Peper, Lee, Harvey & Lin, 2016).
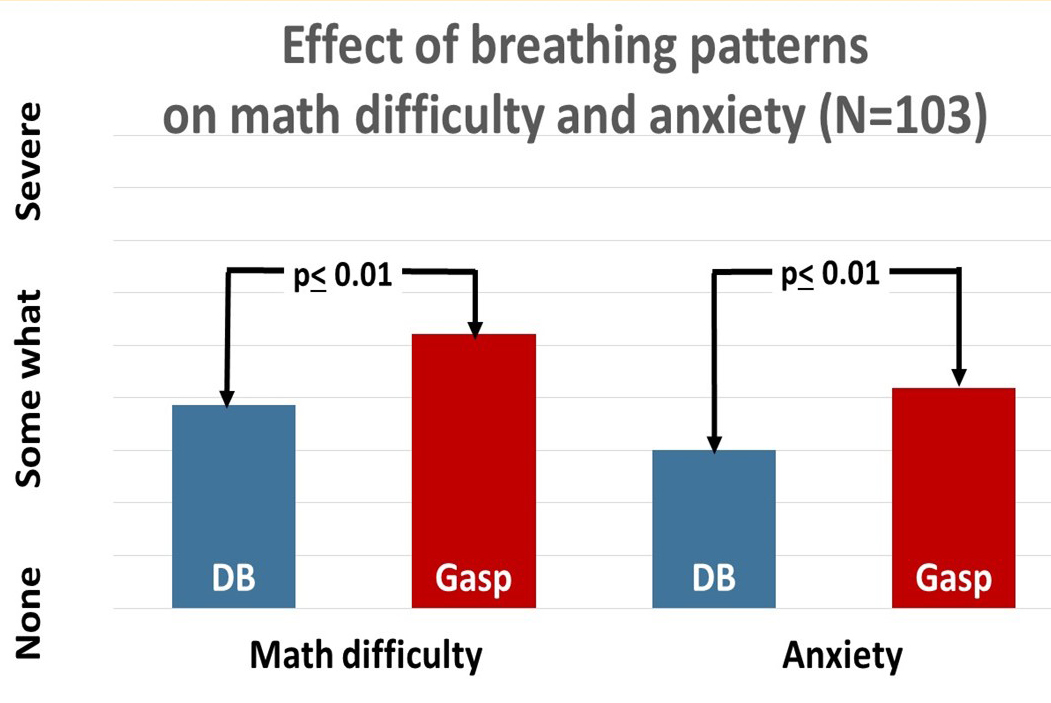
Fig 1. The effect of breathing style on math performance. Diaphragmatic breathing significantly increased math performance and decreased anxiety (from: Peper, Lee, Harvey & Lin, 2016).
As one 20 year old college student said, “When I gasped, my mind went blank and I could not do the subtraction. When I breathed slowly, I had no problem doing the subtractions. I never realized that breathing had such a big effect upon my performance.”
When you are stressed and blank out, take a slow diaphragmatic breath to improve performance; however, it is only effective if you have previously studied the materials effectively. To improve effective learning incorporate the following concepts when studying.
- Approached learning with a question. When you begin to study the material or attend a class, ask yourself a question that you would like to be answered. When you have a purpose, it is easier to stay emotionally present and remember the material (Osman, & Hannafin, 1994).
- Process what you are learning with as many sensory cues as possible. Take hand written notes when reading the text or listening to your teacher. Afterwards meet with your friends in person, on Skype and again discuss and review the materials. As you discuss the materials, add comments to your notes. Do not take notes on your computer because people can often type almost as quickly as someone speaks. The computer notes are much less processed and are similar to the experience of a court or medical transcriptionist where the information flows from the ears to the fingers without staying in between. College students who take notes in class on a computer or tablets perform worse on exams than students who write notes. When you write your notes you have to process the material and extract and synthesis relevant concepts.
- Review the notes and material before going to sleep. Research has demonstrated that whatever material is in temporary memory before going to sleep will be more likely be stored in long term memory (Gais et al., 2006; Diekelmann et al., 2009). When you study material is stored in temporary memory, and then when you study something else, the first material tends to displaced by the more recent material. The last studied material is more likely stored in long term memory. When you watch a movie after studying, the movie content is preferentially stored in permanent memory during sleep. In addition, what is emotionally most important to you is usually stored first. Thus, instead of watching movies and chatting on social media, discuss and review the materials just before you go to sleep.
- Learning is state dependent. Study and review the materials under similar conditions as you will be tested. Without awareness the learned content is covertly associated with environmental, emotional, social and kinesthetic cues. Thus when you study in bed, the material is most easily accessed while lying down. When you study with music, the music become retrieval trigger. Without awareness the materials are encoded with the cues of lying down or the music played in the background. When you come to the exam room, none of those cues are there, thus it is more difficult to recall the material (Eich, 2014).
- Avoid interruptions. When studying each time you become distracted by answering a text message or responding to social media, your concentration is disrupted (Swingle, 2016). Imagine that learning is like scuba diving and the learning occurs mainly at the bottom. Each interruption forces you to go to the surface and it takes time to dive down again. Thus you learn much less than if you stayed at the bottom for the whole time period.
- Develop study rituals. Incorporate a ritual before beginning studying and repeat it during studying such as three slow breaths. The ritual can become the structure cue associated with the learned material. When you come to exam and you do not remember or are anxious, perform the same ritual which will allow easier access to the memory.
- Change your internal language. What we overtly or covertly say and believe is what we become. When you say, “I am stupid”, “I can’t do math,” or “It is too difficult to learn,” you become powerless which increases your stress and inhibits cognitive function. Instead, change your internal language so that it implies that you can master the materials such as, “I need more time to study and to practice the material,” “Learning just takes time and at this moment it may take a bit longer than for someone else,” or “I need a better tutor,”
When you take charge of your study habits and practice slower breathing during studying and test taking, you may experience a significant improvement in learning, remembering, accessing, and processing information.
References
Arnsten, A., Mazure, C. M., & Sinha, R. (2012). This is your brain in meltdown. Scientific American, 306(4), 48-53.
Cherif, A. H., Movahedzadeh, F., Adams, G. E., & Dunning, J. (2013). Why Do Students Fail?. Higher Learning, 227, 228.
David, P., Kim, J. H., Brickman, J. S., Ran, W., & Curtis, C. M. (2015). Mobile phone distraction while studying. new media & society, 17(10), 1661-1679.
Diekelmann, S., Wilhelm, I., & Born, J. (2009). The whats and whens of sleep-dependent memory consolidation. Sleep medicine reviews, 13(5), 309-321.
Eich, J. E. (2014). State-dependent retrieval of information in human episodic memory. Alcohol and Human Memory (PLE: Memory), 2, 141.
Fitkov-Norris, E. D., & Yeghiazarian, A. (2013). Measuring study habits in higher education: the way forward?. In Journal of Physics: Conference Series (Vol. 459, No. 1, p. 012022). IOP Publishing.
Gais, S., Lucas, B., & Born, J. (2006). Sleep after learning aids memory recall. Learning & Memory, 13(3), 259-262.
Hagenaars, M. A., Oitzl, M., & Roelofs, K. (2014). Updating freeze: aligning animal and human research. Neuroscience & Biobehavioral Reviews, 47, 165-176.
Hodges, W. F. (2015). The psychophysiology of anxiety. Emotions and Anxiety (PLE: Emotion): New Concepts, Methods, and Applications, 12, 175.
Lee, S., Sanchez, J., Peper, E., & Harvey, R. (2016). Effect of Breathing Style on Math Problem Solving. Presented at the 47th Annual Meeting of the Association for Applied Psychophysiology and Biofeedback, Seattle WA, March 9-12, 2016
Neal, D. T., Wood, W., & Drolet, A. (2013). How do people adhere to goals when willpower is low? The profits (and pitfalls) of strong habits. Journal of Personality and Social Psychology, 104(6), 959.
Osman, M. E., & Hannafin, M. J. (1994). Effects of advance questioning and prior knowledge on science learning. The Journal of Educational Research,88(1), 5-13.
Peper, E., Lee, S., Harvey, R., & Lin, I-M. (2016). Breathing and math performance: Implication for performance and neurotherapy. NeuroRegulation, 3(4),142–149.
Spielberger, C. D., Anton, W. D., & Bedell, J. (2015). The nature and treatment of test anxiety. Emotions and anxiety: New concepts, methods, and applications, 317-344.
Sink, K. S., Walker, D. L., Freeman, S. M., Flandreau, E. I., Ressler, K. J., & Davis, M. (2013). Effects of continuously enhanced corticotropin releasing factor expression within the bed nucleus of the stria terminalis on conditioned and unconditioned anxiety. Molecular psychiatry, 18(3), 308-319.
Swingle, M. (2016). i-Minds: How cell phones, computers, gaming and social media are changing our brains, our behavior, and the evolution of our species. Gabriola Island, BC, Canada: New Society Publishers.
Von Der Embse, N., Barterian, J., & Segool, N. (2013). Test anxiety interventions for children and adolescents: A systematic review of treatment studies from 2000–2010. Psychology in the Schools, 50(1), 57-71.
*I thank Richard Harvey, PhD. for his constructive feedback and comments and Shannon Lee for her superb research.
** This blog was adapted from: Lee, S., Sanchez, J., Peper, E., & Harvey, R. (2016). Effect of Breathing Style on Math Problem Solving. Presented at the 47th Annual Meeting of the Association for Applied Psychophysiology and Biofeedback, Seattle WA, March 9-12, 2016
Increase energy*
Posted: April 1, 2016 Filed under: self-healing, stress management, Uncategorized | Tags: cognitive therapy, energy level, health, Holistic health, stress management 2 CommentsAre you full of pep and energy, ready to do more? Or do you feel drained and exhausted? After giving at the office, is there nothing left to give at home? Do you feel as if you are on a treadmill that will never stop, that more things feel draining than energizing?
Feeling chronically drained is often a precursor for illness; conversely, feeling energized enhances productivity and encourages health. An important aspect of staying healthy is that one’s daily activities are filled more with activities that contribute to our energy than with tasks and activities that drain our energy. Similarly, Dr. John Gottman and colleagues have discovered that marriages prosper when there are many more positive appreciations communicated by each partner than negative critiques.
Energy is the subjective sense of feeling alive and vibrant. An energy gain is an activity, task, or thought that makes you feel better and slightly more alive—those things we want to or choose to do. An energy drain is the opposite feeling—less alive and almost depressed—those things we have to or must do; often something that we do not want to do. In almost all cases, it is not that we have to, should, or must do, it is a choice. Remember, even though you may say, “I have to study.” It is a choice. You can choose not to study and choose to drop out of school. Similarly, when you say, “I have to do the dishes,” it is still a choice. You can choose to do the dishes or let the dirty dishes pile up and just use paper plates.
Energy drains and gains are always unique to the individual; namely, what is a drain for one can be a gain for another. Energy drains can be doing the dishes and feeling resentful that your partner or children are not doing them, or anticipating seeing a person whom you do not really want to see. An energy gain can be meeting a friend and talking or going for a walk in the woods, or finishing a work project.
When patients with cancer start exploring what they truly would like to do and start acting on their unfulfilled dreams, a few experience that their health improves as documented by Dr. Lawrence LeShan in his remarkable book, Cancer as a Turning Point. So often our lives are filled with things that we should do versus want to do. In some cases, the lives we created are not the ones we wanted but the result of self-doubt and worry, “If I did do this, my family and friends won’t like me”, or “I am not sure I will be successful so I will do something that is safe.” Just ask yourself the question when you woke up this morning and most mornings this week, “How did you feel?” Did you felt happy and looking forward to the day?

Explore strategies to decrease the drains and increase the energy gains. Use the following exercise to increase your energy:
- For one week monitor your energy drains and energy gains. Monitor events, activities, thoughts, or emotions that increase or decrease energy at home and at work. For example some drains can include cleaning bathroom, cooking another meal, or talking to a family member on the phone, while gains can be taking a walk, talking to a friend, completing a work task. Be very honest, just note the events that change your energy level.
- After the week look over your notes and identify at least one activity that drains your energy and one activity that increases your energy
- Develop a strategy to decrease one of the energy drains. Be very specific how, where, when, with whom, and which situations decreasing the tasks that drain your energy. As you think about it, anticipate obstacles that may interfere with reducing your drains and develop new ways to overcome these obstacles such as trading tasks with others (I will cook if you clean the bathroom), setting time limits, giving yourself positive reward after finishing the task (a cup of tea, a text or phone message to a close friend, watching a video in the evening).
- Develop new ways how you can increase energy gains such as doing exercise, completing a task.
- Each day implement the behavior to reduce one less energy drain and increase one energy gain and observe what happens.
Initially it may seem impossible, many students and clients report that the practice made them aware, increased their energy, and they had more control over their lives than they thought. It also encouraged them to explore the question, “What is it that you really want to do?” So often we do energy drains because of convention, habit and fear which makes us feel powerless and suppresses our immune system thereby increasing the risk of illness. In observing the energy drains and energy gains, it may give the person a choice. Sometimes, the choice is not changing the tasks but how we think about it. Many of the things we do are not MUSTs; they are choices. I do the work at my job because I choose to benefits of earning money.
How your internal language impacts your energy**
Sit and think of something that you feel you have to do, should do, or must do. Something you slightly dread such as cleaning the dishes, doing a math assignment. While sitting say to yourself, “I have to do, should do, or must do_______________.” Keep repeating the phrase for a minute.
Then change your internal phrase and instead say one of the following phrases, “I choose to do,” “I look forward to doing,” or “I choose not to do _________.” Keep repeating the phrase for a minute.
Now compare how you felt. Almost all people feel slight less energy and more depressed when they are thinking, “I have to do,” “should do”, or must do”. While when they shifted the phrase to, “I choose to,” “I look forward to doing,” or “I choose not to do it,” they feel lighter, more expanded and more optimistic. When university students practice this change of language during the week, they find it was easier to start and complete their homework tasks.
Watch your thoughts; they become words.
Watch your words; they become actions.
Watch your actions; they become habits.
Watch your habits; they become character.
Watch your character; it becomes your destiny.
– Frank Outlaw
References
Gottman, J.M. & Silver, N. (2015). The Seven Principles for Making Marriage Work. New York: Harmony.
LeShan, L. (1999). Cancer as a Turning Point. New York: Plume
*Adapted from: Peper, E. (2016). Increase energy. Western Edition. April, pp4. http://thewesternedition.com/admin/files/magazines/WE-April-2016.pdf
**Adapted from: Gorter, R. & Peper, E. (2011). Fighting Cancer-A Nontoxic Approach to Treatment. Berkeley: North Atlantic Books, 107-200.
Can abdominal surgery cause epilepsy, panic and anxiety and be reversed with breathing biofeedback?*
Posted: March 5, 2016 Filed under: Breathing/respiration, self-healing, stress management, Uncategorized | Tags: anxiety, biofeedback, Breathing, epilepsy, iatrogenic illness, learned disuse, panic, respiration, surgery 4 Comments“I had colon surgery six months ago. Although I made no connection to my anxiety, it just started to increase and I became fearful and I could not breathe. The asthma medication did not help. Learning effortless diaphragmatic breathing and learning to expand my abdomen during inhalation allowed me to breathe comfortably without panic and anxiety—I could breathe again.” (72 year old woman)
“One year after my appendectomy, I started to have twelve seizures a day. After practicing effortless diaphragmatic breathing and changing my lifestyle, I am now seizure-free.” (24 year old male college student)
One of the hidden long term costs of surgery and injury is covert learned disuse. Learned disuse occurs when a person inhibits using a part of their body to avoid pain and compensates by using other muscle patterns to perform the movements (Taub et al, 2006). This compensation to avoid discomfort creates a new habit pattern. However, the new habit pattern often induces functional impairment and creates the stage for future problems.
Many people have experienced changing their gait while walking after severely twisting their ankle or breaking their leg. While walking, the person will automatically compensate and avoid putting weight on the foot of the injured leg or ankle. These compensations may even leads to shoulder stiffness and pain in the opposite shoulder from the injured leg. Even after the injury has healed, the person may continue to move in the newly learned compensated gait pattern. In most cases, the person is totally unaware that his/her gait has changed. These new patterns may place extra strain on the hip and back and could become a hidden factor in developing hip pain and other chronic symptoms.
Similarly, some women who have given birth develop urinary stress incontinence when older. This occurred because they unknowingly avoided tightening their pelvic floor muscles after delivery because it hurt to tighten the stretched or torn tissue. Even after the tissue was healed, the women may no longer use their pelvic floor muscles appropriately. With the use of pelvic floor muscle biofeedback, many women with stress incontinence can rapidly learn to become aware of the inhibited/forgotten muscle patterns (learned disuse) and regain functional control in nine sessions of training (Burgio et al., 1998; Dannecker et al., 2005). The process of learned disuse is the result of single trial learning to avoid pain. Many of us as children have experienced this process when we touched a hot stove—afterwards we tended to avoid touching the stove even when it was cold.
Often injury will resolve/cure the specific problem. It may not undo the covert newly learned dysfunctional patterns which could contribute to future iatrogenic problems or illnesses (treatment induced illness). These iatrogenic illnesses are treated as a new illness without recognizing that they were the result of functional adaptations to avoid pain and discomfort in the recovery phase of the initial illness.
Surgery creates instability at the incision site and neighboring areas, so our bodies look for the path of least resistance and the best place to stabilize to avoid pain. (Adapted from Evan Osar, DC).
After successful surgical recovery do not assume you are healed!
Yes, you may be cured of the specific illness or injury; however, the seeds for future illness may be sown. Be sure that after injury or surgery, especially if it includes pain, you learn to inhibit the dysfunctional patterns and re-establish the functional patterns once you have recovered from the acute illness. This process is described in the two cases studies in which abdominal surgeries appeared to contribute to the development of anxiety and uncontrolled epilepsy.
How abdominal surgery can have serious, long-term effect on changing breathing patterns and contributing to the development of chronic illness.
When recovering from surgery or injury to the abdomen, it is instinctual for people to protect themselves and reduce pain by reducing the movement around the incision. They tend to breathe more shallowly as not to create discomfort or disrupt the healing process (e.g., open a stitch or staple. Prolonged shallow breathing over the long term may result in people experiencing hyperventilation induced panic symptoms or worse. This process is described in detail in our recent article, Did You Ask about Abdominal Surgery or Injury? A Learned Disuse Risk Factor for Breathing Dysfunction (Peper et al., 2015). The article describes two cases studies in which abdominal surgeries led to breathing dysfunction and ultimately chronic, serious illnesses.
Reducing epileptic seizures from 12 per week to 0 and reducing panic and anxiety
A routine appendectomy caused a 24-year-old male to develop rapid, shallow breathing that initiated a series of up to 12 seizures per week beginning a year after surgery. After four sessions of breathing retraining and incorporating lifestyle changes over a period of three months his uncontrolled seizures decreased to zero and is now seizure free. In the second example, a 39-year-old woman developed anxiety, insomnia, and panic attacks after her second kidney transplant probably due to shallow rapid breathing only in her chest. With biofeedback, she learned to change her breathing patterns from 25 breaths per minute without any abdominal movement to 8 breathes a minute with significant abdominal movement. Through generalization of the learned breathing skills, she was able to achieve control in situations where she normally felt out of control. As she practiced this skill her symptoms were significantly reduced and stated:
“What makes biofeedback so terrific in day-to-day situations is that I can do it at any time as long as I can concentrate. When I feel I can’t concentrate, I focus on counting and working with my diaphragm muscles; then my concentration returns. Because of the repetitive nature of biofeedback, my diaphragm muscles swing into action as soon as I started counting. When I first started, I had to focus on those muscles to get them to react. Getting in the car, I find myself starting these techniques almost immediately. Biofeedback training is wonderful because you learn techniques that can make challenging situations more manageable. For me, the best approach to any situation is to be calm and have peace of mind. I now have one more way to help me achieve this.” (From: Peper et al, 2001).
The commonality between these two participants was that neither realized that they were bracing the abdomen and were breathing rapidly and shallowly in the chest. I highly recommend that anyone who has experienced abdominal insults or surgery observe their breathing patterns and relearn effortless breathing/diaphragmatically breathing instead of shallow, rapid chest breathing often punctuated with breath holding and sighs.
It is important that medical practitioners and post-operative surgery patients recognize the common covert learned disuse patters such as shifting to shallow breathing to avoid pain. The sooner these patterns are identified and unlearned, the less likely will the person develop future iatrogenic illnesses. Biofeedback is an excellent tool to help identify and retrain these patterns and teach patients how to reestablish healthy/natural body patterns.
The full text of the article see: “Did You Ask About Abdominal Surgery or Injury? A Learned Disuse Risk Factor for Breathing Dysfunction,”
*Adapted from: Biofeedback Helps to Control Breathing Dysfunction.http://www.prweb.com/releases/2016/02/prweb13211732.htm
References
Burgio, K. L., Locher, J. L., Goode, P. S., Hardin, J. M., McDowell, B. J., Dombrowski, M., & Candib, D. (1998). Behavioral vs drug treatment for urge urinary incontinence in older women: a randomized controlled trial. Jama, 280(23), 1995-2000.
Dannecker, C., Wolf, V., Raab, R., Hepp, H., & Anthuber, C. (2005). EMG-biofeedback assisted pelvic floor muscle training is an effective therapy of stress urinary or mixed incontinence: a 7-year experience with 390 patients. Archives of Gynecology and Obstetrics, 273(2), 93-97.
Osar, E. (2016). http://www.fitnesseducationseminars.com/
Peper, E., Castillo, J., & Gibney, K. H. (2001, September). Breathing biofeedback to reduce side effects after a kidney transplant. In Applied Psychophysiology and Biofeedback (Vol. 26, No. 3, pp. 241-241). 233 Spring St., New York, NY 10013 USA: Kluwer Academic/Plenum Publ.
Peper, E., Gilbert, C.D., Harvey, R. & Lin, I-M. (2015). Did you ask about abdominal surgery or injury? A learned disuse risk factor for breathing dysfunction. Biofeedback. 34(4), 173-179. DOI: 10.5298/1081-5937-43.4.06
Taub, E., Uswatte, G., Mark, V. W., Morris, D. M. (2006). The learned nonuse phenomenon: Implications for rehabilitation. Europa Medicophysica, 42(3), 241-256.
Resolving pelvic floor pain-A case report
Posted: September 25, 2015 Filed under: Breathing/respiration, Pain/discomfort, self-healing, stress management, Uncategorized | Tags: biofeedback, Breathing, electromyography, pain, posture, self-regulation, vulvodynia 10 CommentsAdapted from: Martinez Aranda, P. & Peper, E. (2015). The healing of vulvodynia from a client’s perspective. https://biofeedbackhealth.files.wordpress.com/2011/01/a-healing-of-vulvodynia-from-the-client-perspective-2015-06-15.pdf
It’s been a little over a year since I began practicing biofeedback and visualization strategies to overcome vulvodynia. Today, I feel whole, healed, and hopeful. I learned that through controlled and conscious breathing, I could unleash the potential to heal myself from chronic pain. Overcoming pain did not happen overnight; but rather, it was a process where I had to create and maintain healthy lifestyle habits and meditation. Not only am I thankful for having learned strategies to overcome chronic pain, but for acquiring skills that will improve my health for the rest of my life. –-24 year old woman who successfully resolved vulvodynia
Pelvic floor pain can be debilitating, and it is surprisingly common, affecting 10 to 25% of American women. Pelvic floor pain has numerous causes and names. It can be labeled as vulvar vestibulitis, an inflammation of vulvar tissue, interstitial cystitis (chronic pain or tenderness in the bladder), or even lingering or episodic hip, back, or abdominal pain. Chronic pain concentrated at the entrance to the vagina (vulva), is known as vulvodynia. It is commonly under-diagnosed, often inadequately treated, and can go on for months and years (Reed et al., 2007; Mayo Clinic, 2014). The discomfort can be so severe that sitting is uncomfortable and intercourse is impossible because of the extreme pain. The pain can be overwhelming and destructive of the patient’s life. As the participant reported,
I visited a vulvar specialist and he gave me drugs, which did not ease the discomfort. He mentioned surgical removal of the affected tissue as the most effective cure (vestibulectomy). I cried immediately upon leaving the physician’s office. Even though he is an expert on the subject, I felt like I had no psychological support. I was on Gabapentin to reduce pain, and it made me very depressed. I thought to myself: Is my life, as I know it, over?
Physically, I was in pain every single day. Sometimes it was a raging burning sensation, while other times it was more of an uncomfortable sensation. I could not wear my skinny jeans anymore or ride a bike. I became very depressed. I cried most days because I felt old and hopeless instead of feeling like a vibrant 23-year-old woman. The physical pain, combined with my negative feelings, affected my relationship with my boyfriend. We were unable to have sex at all, and because of my depressed status, we could not engage in any kind of fun. (For more details, read the published case report,Vulvodynia treated successfully with breathing biofeedback and integrated stress reduction: A case report).
The four-session holistic biofeedback interventions to successfully resolved vulvodynia included teaching diaphragmatic breathing to transform shallow thoracic breathing into slower diaphragmatic breathing, transforming feelings of powerlessness and hopelessness to empowerment and transforming her beliefs that she could reduce her symptoms and optimize her health. The interventions also incorporated self-healing imagery and posture-changing exercises. The posture changes consisted of developing awareness of the onset of moving into a collapsed posture and use this awareness to shift to an erect/empowered postures (Carney, Cuddy, & Yap, 2010; Peper, 2014; Peper, Booiman, Lin, & Harvey, in press). Finally, this case report build upon the seminal of electromyographic feedback protocol developed by Dr. Howard Glazer (Glazer & Hacad, 2015) and the integrated relaxation protocol developed Dr. David Wise (Wise & Anderson, 2007).
Through initial biofeedback monitoring of the lower abdominal muscle activity, chest, and abdomen breathing patterns, the participant observed that when she felt discomfort or was fearful, her lower abdomen muscles tended to tighten. After learning how to sense this tightness, she was able to remind herself to breathe lower and slower, relax the abdominal wall during inhalation and sit or stand in an erect power posture.
The self-mastery approach for healing is based upon a functional as compared to a structural perspective. The structural perspective implies that the problem can only be fixed by changing the physical structure such as with surgery or medications. The functional perspective assumes that if you can learn to change your dysfunctional psychophysiological patterns the disorder may disappear.
The functional approach assumed that an irritation of the vestibular area might have caused the participant to tighten her lower abdomen and pelvic floor muscles reflexively in a covert defense reaction. In addition, ongoing worry and catastrophic thinking (“I must have surgery, it will never go away, I can never have sex again, my boyfriend will leave me”) also triggered the defense reaction—further tightening of her lower abdomen and pelvic area, shallow breathing, and concurrent increases in sympathetic nervous activation—which together activated the trigger points that lead to increased chronic pain (Banks et al, 1998).
When the participant experienced a sensation or thought/worried about the pain, her body responded in a defense reaction by breathing in her chest and tightening the lower abdominal area as monitored with biofeedback. Anticipation of being monitored increased her shoulder tension, recalling the stressful memory increased lower abdominal muscle tension (pulling in the abdomen for protection), and the breathing became shallow and rapid as shown in Figure 1.
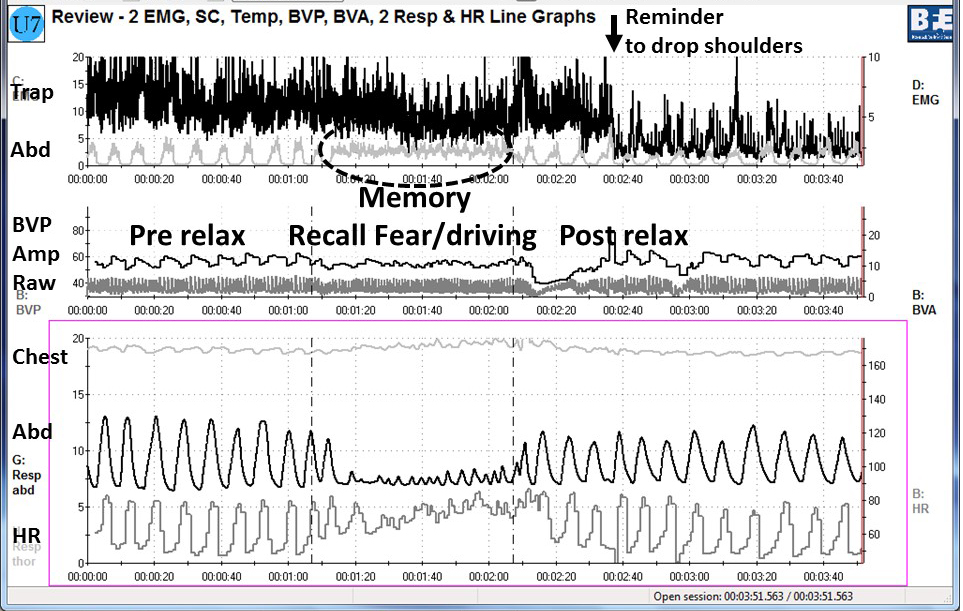
Figure 1. Physiological recording of pre-stressor relaxation, the recall of a fearful driving experience, and a post-stressor relaxation. The scalene to trapezius SEMG increased in anticipation while she recalled the experience, and then initially did not relax (from Peper, Martinez Aranda, & Moss, 2015).
This defense pattern became a conditioned response—initiating intercourse or being touched in the affected area caused the participant to tense and freeze up. She was unaware of these automatic protective patterns, which only worsened her chronic pain.
During the four sessions of training, the participant learned to reverse and interrupt the habitual defense reaction. For example, as she became aware of her breathing patterns she reported,
It was amazing to see on the computer screen the difference between my regular breathing pattern and my diaphragmatic breathing pattern. I could not believe I had been breathing that horribly my whole life, or at least, for who knows how long. My first instinct was to feel sorry for myself. Then, rather than practicing negative patterns and thoughts, I felt happy because I was learning how to breathe properly. My pain decreased from an 8 to alternating between a 0 and 3.
The mastery of slower and lower abdominal breathing within a holistic perspective resulted in the successful resolution of her vulvodynia. An essential component of the training included allowing the participant to feel safe, and creating hope by enabling her to experience a decrease in discomfort while doing a specific practice, and assisting her to master skills to promote self-healing. Instead of feeling powerless and believing that the only resolution was the removal of the affected area (vestibulectomy). The integrated biofeedback protocol offered skill mastery training, to promote self-healing through diaphragmatic breathing, somatic postural changes, reframing internal language, and healing imagery as part of a common sense holistic health approach.
For more details about the case report, download the published study, Peper, E., Martinez Aranda, P., & Moss, E. (2015). Vulvodynia treated successfully with breathing biofeedback and integrated stress reduction: A case report. Biofeedback. 43(2), 103-109.
The participant also wrote up her subjective experience of the integrated biofeedback process in the paper, Martinez Aranda & Peper (2015). Healing of vulvodynia from the client perspective. In this paper she articulated her understanding and experiences in resolving vulvodynia which sheds light on the internal processes that are so often skipped over in published reports.
At the five year follow-up on May 29, 2019, she wrote:
“I am doing very well, and I am very healthy. The vulvodynia symptoms have never come back. It migrated to my stomach a couple of years after, and I still have a sensitive stomach. My stomach has gotten much, much better, though. I don’t really have random pain anymore, now I just have to be watchful and careful of my diet and my exercise, which are all great things!”
References
Banks, S. L., Jacobs, D. W., Gevirtz, R., & Hubbard, D. R. (1998). Effects of autogenic relaxation training on electromyographic activity in active myofascial trigger points. Journal of Musculoskeletal Pain, 6(4), 23-32. https://www.researchgate.net/profile/David_Hubbard/publication/232035243_Effects_of_Autogenic_Relaxation_Training_on_Electromyographic_Activity_in_Active_Myofascial_Trigger_Points/links/5434864a0cf2dc341daf4377.pdf
Carney, D. R., Cuddy, A. J., & Yap, A. J. (2010). Power posing brief nonverbal displays affect neuroendocrine levels and risk tolerance. Psychological Science, 21(10), 1363-1368. Available from: https://www0.gsb.columbia.edu/mygsb/faculty/research/pubfiles/4679/power.poses_.PS_.2010.pdf
Glazer, H. & Hacad, C.R. (2015). The Glazer Protocol: Evidence-Based Medicine Pelvic Floor Muscle (PFM) Surface Electromyography (SEMG). Biofeedback, 40(2), 75-79. http://www.aapb-biofeedback.com/doi/abs/10.5298/1081-5937-40.2.4
Martinez Aranda, P. & Peper, E. (2015). Healing of vulvodynia from the client perspective. Available from: https://biofeedbackhealth.files.wordpress.com/2011/01/a-healing-of-vulvodynia-from-the-client-perspective-2015-06-15.pdf
Mayo Clinic (2014). Diseases and conditions: Vulvodynia. Available at http://www.mayoclinic.org/diseases-conditions/vulvodynia/basics/definition/con-20020326
Peper, E. (2014). Increasing strength and mood by changing posture and sitting habits. Western Edition, pp.10, 12. Available from: http://thewesternedition.com/admin/files/magazines/WE-July-2014.pdf
Peper, E., Booiman, A., Lin, I, M.,& Harvey, R. (in press). Increase strength and mood with posture. Biofeedback.
Peper, E., Martinez Aranda, P., & Moss, E. (2015). Vulvodynia treated successfully with breathing biofeedback and integrated stress reduction: A case report. Biofeedback. 43(2), 103-109. Available from: https://biofeedbackhealth.files.wordpress.com/2011/01/a-vulvodynia-treated-with-biofeedback-published.pdf
Reed, B. D., Haefner, H. K., Sen, A., & Gorenflo, D. W. (2008). Vulvodynia incidence and remission rates among adult women: a 2-year follow-up study. Obstetrics & Gynecology, 112(2, Part 1), 231-237. http://journals.lww.com/greenjournal/Abstract/2008/08000/Vulvodynia_Incidence_and_Remission_Rates_Among.6.aspx
Wise, D., & Anderson, R. U. (2006). A headache in the pelvis: A new understanding and treatment for prostatitis and chronic pelvic pain syndromes. Occidental, CA: National Center for Pelvic Pain Research.http://www.pelvicpainhelp.com/books/
