Family or work? The importance of value clarification
Posted: May 4, 2018 Filed under: Breathing/respiration, mindfulness, Neck and shoulder discomfort, Pain/discomfort, relaxation, stress management, Uncategorized | Tags: meaning, regeneration, relaxation, respiration, stress management, values clarification 1 CommentRichard Harvey, PhD and Erik Peper, PhD

In a technologically modern world, many people have the option of spending 24 hours a day/ 7 days a week continuously interacting via telephone, text, work and personal emails or internet websites and various social media platforms such as Facebook, What’s App, Instagram, Twitter, LinkedIn and Snapchat. How many people do we know who work too many hours, watch too many episodes on digital screens, commute too many hours, or fill loneliness with online versions of retail therapy? In the rush of work-a-day survival as well as being nudged and bombarded with social media notifications, or advertisements for material goods, we forget to nurture meaningful friendships and family relationships (Peper and Harvey, 2018). The following ‘values clarification’ practice may help us identify what is most important to us and help keep sight of those things that are most relevant in our lives (Hofmann, 2008; Knott, Ribar, & Duson, 1989; Twohig & Crosby, 2009;. Peper, 2014).
Give yourself about 12 minutes of uninterrupted time to do this practice. Do this practice by yourself, in a group, or with family and friends. Have a piece of paper ready. Be guided by the two video clips at the end of the blog. Begin with the Touch Relaxation and Regeneration Practice to relax and let go of thoughts and worries, then follow it with the Value Clarification Practice.
Touch Relaxation and Regeneration Practice
Turn off your cell phone and let other know not to interrupt for the next 12 minutes, then engage in the following six-minute relaxation exercise. If your attention wanders during the practice, then bring your attention back to the various sensations in your body.
- Sit comfortably, then lift your arms from your lap, holding them parallel to the floor and tighten your arms while making a fist in each hand. While holding your fists tightly closed, keep breathing for a total of 10 seconds before dropping the arms to your lap while you relax all of your muscles. Attend for 20 seconds to the changing sensations in arms and hands as they relax. If your attention wanders bring it back to the sensations in your arm and hands.
- Tighten your buttock muscles and bend your ankles so that the toes move upwards in a direction towards your knees. Keep breathing and hold your toes upwards for 10 seconds and then let the toes move down to the floor, letting go and relaxing all the muscles of the lower trunk and legs. Feel your knees widening and feel your buttock muscles relaxing. Continue attending to the body and muscle sensations for the next 20 seconds. If your attention wanders bring it back to the sensations in your body.
- Tighten your whole body by pressing your knees together, lifting your arms up from your lap, making a fist and wrinkling your face. Hold the tension while continuing to breath for 10 seconds. Let go and relax and feel the whole body sinking and relaxing and being supported by the chair for the next 20 seconds.
- Bring your right hand to your left shoulder. Over the next 10 seconds, inhale for three or four seconds and as you exhale for five or six seconds, with your right hand stroke down your left arm from your shoulder to past your hand. Imagine that the exhaled air is flowing through your arm and out your hand. Repeat at least once more.
- Bring your left hand to your right shoulder. Inhale for three or four seconds and as you exhale for five or six seconds with your left hand stroke down your right arm from your shoulder to past your hand. Imagine that the exhaled air is flowing through your arm and out your hand. Repeat at least once more.
- Bring both hands to the sides of your hips. Inhale for three or four seconds and as you exhale for five or six seconds stroke your legs with your hands from the hips to the ankles. Imagine that the exhaled air is flowing through your legs and out your feet. Repeat a least once more.
- Close your eyes and inhale for three or four seconds, then hold your breath for seven seconds slowly exhale for eight seconds. Imagine as you exhale the air flowing through your arms and out your hands and through your legs and out your feet. Continue breathing easily and slowly such as inhaling for three or four seconds, and out for five to seven seconds. If your attention wanders just bring it back to the sensations going down your arms and legs. Feel the relaxation and peacefulness.
- Take another deep breath and then stretch and continue with the Value Clarification
Value Clarification Practice
Get the paper and pen and do the following Value Clarification Practice.
- Quickly (e.g. 30-60 seconds) list the 10 most important things in your life. For the activity to work, the list must contain 10 important things that may be concrete or abstract, ranging from material things such as a smart phone or a car to immaterial things such as family, love, god, health… If you need to, break up a larger category into smaller pieces. For example, if one item on the list is family, and you only have seven items on the list, assuming you have a family of four, then identify separate family members in order to complete a list of 10 important things.
- To start off, in only 10 seconds, please cross off three items from the list, then explain why you removed those three. If done in a group of people turn to the person explain why you made these choices.
- Next, in only 10 seconds, please cross off three more, then explain why you kept what you kept. If done in a group of people turn to the person explain why you made these choices.
- Finally, in only 10 seconds, please cross off three more, then reveal the one most important thing on your list. Share your choice for the item you kept and how you felt while crossing items from the list or keeping them.
- When engaging with this type of values clarification practice, please remind yourself and others that the items on the list were never gone, they are always in your life to the extent that you can honor the presence of those things in your life.
We have done these exercises with thousands of student and adults. The most common final item on the list is family or an individual family member. Sometimes, categories such as health or god appear, however it is extremely rare that material items make it to the final round. For example, no one would report that their last item is their job, their bank account, their house, or their smart phone. It is common that people have difficulty choosing the last item on their list, often taking more than 10 seconds to choose. For example, they find that they cannot choose between eliminating individual family members. For those who find the activity too difficult, remind them that the exercise is voluntary and meant as a ‘thought experiment’ which they may stop at any time.
Reflect how much of your time is spent nurturing what is most important to you? In many cases we feel compelled to finish some employment priorities instead of making time for nurturing our family relationship. And when we become overwhelmed with work demands, we retreat to sooth our difficulties by checking our email or browsing social media rather than supporting the family connections that are so important to us.
Organize an action plan to honor and support your commitment to the items on your list that you value the most. If possible let other people know what you are doing.
- Describe in detail what you will do in real life and in real time in service to honor and support your relationships with the things that you value.
- Describe in detail what you will do, when you will do it, with whom you will do it, at what time you will do it, and anticipate what will get in the way of doing it. For example, how will you resolve any conflicts between what you plan and what you actually do when there is not enough time to carry out your plans?
- Schedule a time during the following week for feedback about your plans to honor and support the things you value.
Summary
Many people experience that it is challenging to make time to honor and support their primary values given the ongoing demands of daily living. To be congruent with our values means making ongoing choices such as listening and sharing experiences with your partner versus binging on videos or, using your smartphone for answering email or texting instead of watching your child play ball.
The values you previously identified are similar to those identified by patients who are in hospice and dying. For them as they look back on their lives, the five most common regret are (Ware, 2009; Ware, 2012):
- I wish I’d the courage to live a life true to myself, not the life others expected of me.
- I wish I hadn’t worked so hard.
- I wish I had the courage to express my feelings.
- I wish I had stayed in touch with my friends.
- I wish I had let myself be happier.
Take the time to plan actions that support your identified values. Feel free to watch the following videos that guide you through the activities described here.
References
Hofmann, S.G. (2008). Acceptance and commitment therapy: New wave or Morita therapy?. Clinical Psychology: Science and Practice, 15(4), 280-285. https://doi.org/10.1111/j.1468-2850.2008.00138.x
Knott, J.E., Ribar, M.C. & Duson, B.M. (1989). Thanatopics: Activities and Exercises for Confronting Death, Lexington Books: Lexington, MA. https://www.amazon.com/Thanatopics-Activities-Exercise-Confronting-Death/dp/066920871X
Peper, E. (October 19, 2014). Choices-Creating meaningful days. https://peperperspective.com/2014/10/19/choices-creating-meaningful-days/
Peper, E. & Harvey, R. (2018). Digital addiction: increased loneliness, depression, and anxiety. NeuroRegulation. 5(1),3–8. doi:10.15540/nr.5.1.3 http://www.neuroregulation.org/article/view/18189/11842
Twohig, M.P. & Crosby, J.M. (2009). Values clarification. In: O’Donohue & W.T., Fisher, J.E., Eds. Cognitive behavior therapy: applying empirically supported techniques in your practice. Wiley: Hoeboken, N.J., p. 681-686.
Ware, B. (2009). Regrets of the dying. https://bronnieware.com/blog/regrets-of-the-dying/
Ware, B. (2012). The top five regrets of dying: A life transformed by the dearly departing. Hay House. ISBN: 978-1401940652
Surgery: Hope for the best and plan for the worst!
Posted: March 18, 2018 Filed under: Pain/discomfort, placebo, self-healing, stress management, surgery, Uncategorized | Tags: anesthesia, hernia, iatrogenic illness, technology, urinary retention 20 CommentsAdapted from: Peper, E. Surviving and preventing medical errors. (2019). Townsend Letter-The Examiner of Alternative Medicine. 429, 63-69. https://townsendletter.com/surviving-and-preventing-medical-errors-peper/
The purpose of this blog is to share what I have learned from a cascade of medical errors that happen much more commonly than surgeons, hospitals, or health care providers acknowledge and is the third leading cause of death in the US (Makary, M.A. & Daniel, M., 2016). My goal here is to provide a few simple recommendations to reduce these errors.

It is now two years since my own surgery—double hernia repair by laparoscopy. The recovery predicted by my surgeon, “In a week you can go swimming again,” turned out to be totally incorrect.
Six weeks after the surgery, I was still lugging a Foley catheter with a leg collection bag that drained my bladder. I had swelling due to blood clots in the abdominal area around my belly button, severe abdominal cramping, and at times, overwhelming spasms. For six weeks my throat was hoarse following the intubation. Instead of swimming, hiking, walking, working, and making love with my wife, I was totally incapacitated, unable to work, travel, or exercise. I had to lie down every few hours to reduce the pain and the spasms.
Instead of going to Japan for a research project, I had to cancel my trip. Rather than teaching my class at the University, I had another faculty member teach for me. I am a fairly athletic guy—I swim several times a week, bike the Berkeley hills, and hiked. Yet after the surgery, I avoided even walking in order to minimize the pain. I moved about as if I were crippled. Now two years later, I finally feel healthy again.
How come my experiences were not what the surgeon promised?
All those who cared for me during this journey were compassionate individuals, committed to doing their best, including the emergency staff, the nurses, my two primary physicians, my surgeon, and my urologist. However, given the personal, professional, and economic cost to me and my family, I feel it is important to assess where things went wrong. The research literature makes it clear that my experience was by no means unique, so I have summarized some of the most important factors that contributed to these unexpected complications, following “simple arthroscopic surgery.”
- Underestimating the risk. Although the surgeon suggested that the operation would be very low risk with no complications, the published research data does not support his optimistic statement and misrepresented the actual risk. Complications for laparoscopic surgery range from 15% to as high as 38% or higher, depending on the age of the patient and how well they do with general anesthesia (Vigneswaran et al, 2015; Neumayer et al, 2004; Perugini & Callery, 2001). Experienced surgeons who have done more than 250 laparoscopic surgeries have a lower complication rate. However, a 2011 Cochran review points out that there is theoretically a higher risk that intra-abdominal organs will be injured during a laparoscopic procedure (Sauerland, 2011). In addition, bilateral laparoscopic hernia repair has significantly higher risk than single sided laparoscopic hernia repair for post-operative urinary retention (Blair et al, 2016). My experience is not an outlier–it is more common.
- Inappropriate post-operative procedures. In my case I was released directly after waking up from general anesthesia without checking to determine whether I could urinate or not. The medical staff and facility should never have released me, since older males have a 30% or higher probability that urinary retention will occur after general anesthesia. However, it was a Friday afternoon and the staff probably wanted to go home since the facility closes at 5:30 pm. This landed me in the Emergency Room.
- Medical negligence. In my case the surgeon recommended that I have my bladder in the emergency room emptied and then go home. That was not sufficient, and my body still was not working properly, requiring a second visit to the ER and the insertion of a Foley catheter. Following the second ER visit, the surgeon removed the catheter in his office in the late afternoon and did not check to determine whether I could urinate or not. This resulted in a third ER visit.
- Medical error. On my third visit to the emergency room, the nurse made the error of inflating the Foley catheter balloon when it was in the urethra (rather than the bladder) which caused tearing and bleeding of the urethra and possible irritation to the prostate.
- Drawbacks of the ER as the primary resource for post-surgical care. Care is not scheduled for the patient’s needs, but rather based on a triage system. In my case I had to wait sometimes two hours or more until a catheter could be inserted. The wait kept increasing the urine volume which expanded and irritated the bladder further.
- A medical system that does not track treatment outcomes. Without good follow-up and long-term data, no one is accountable or responsible.
- A reimbursement system that rewards lower up-front costs. The system favors quick outpatient surgeries without factoring in the long-term costs and harm of the type I experienced.
Assuming the best and not planning for the worst.
Can I trust the health care provider’s statement that the procedure is low risk and that the recovery will go smoothly?
The typical outcome of a medical procedure or surgery may be significantly worse than generally reported by hospitals or medical staff. In many cases there is no systematic follow-up nor data on outcomes and complications, thus no one knows the actual risks.
In the United States medical error results in at least 98,000 unnecessary deaths each year and 1,000,000 excess injuries (Weingart et al, 2000; Khon et al, 2000). The Institute of Medicine reported in 2012 that one-third of hospitalized patients are harmed during their stay (Ferguson, 2012; Institute of Medicine, 2012).
One should also be intelligently skeptical about positive claims for any specific study—it is important to know whether the study has been replicated with other populations and not just a particular group of patients.
To quote Dr. Marcia Angell (2009), the first woman editor of the highly respected New England Journal of Medicine, “It is simply no longer possible to believe much of the clinical research that is published, or to rely on the judgment of trusted physicians or authoritative medical guidelines. I take no pleasure in this conclusion, which I reached slowly and reluctantly over my two decades as an editor of The New England Journal of Medicine.”
The evidence for many procedures and medications is surprisingly limited
- Research studies frequently select specific subsets of patients. They may exclude many patients who have other co-morbidities.
- Clinical trials may demonstrate statistical significance without providing clinically meaningful results. For example, between 2009 and 2013 all most all cancer drugs that were approved for treatment in Europe showed upon follow-up no clear evidence that they improved survival or quality of life for patients (Davis et al, 2017; Kim & Prasad, 2015).
- Pharmaceuticals are tested only against a passive placebo. In some cases, the patient’s positive response may actually be the placebo effect, due to physical sensations induced by the medication or its side effects, thus inspiring hope that the drug is working (Peper and Harvey, 2017).
- Negative side effects are significantly underreported. The data depend on self-report by both the patient and the health care provider.
Many published studies on the positive clinical outcome of pharmaceuticals are suspect. As Dr. Richard Horton (2015), Editor-in-Chief of The Lancet, wrote in 2015, “A lot of what is published is incorrect … much of the scientific literature, perhaps half, may simply be untrue. Afflicted by studies with small sample sizes, tiny effects, invalid exploratory analyses, and flagrant conflicts of interest, together with an obsession for pursuing fashionable trends of dubious importance, science has taken a turn towards darkness.”
Most studies, including those on surgery, lack long-term follow-up.
The apparent short-term benefits may be not beneficial in the long term or may even be harmful. For example, doctors and patients are convinced that SSRIs (serotonin re-uptake inhibitors—antidepressants such as Paxil and Prozac) are beneficial, with resulting global sales in 2011 of $11.9 billion. However, when all the research data were pooled, metanalysis showed that these drugs are no more effective than placebo for the treatment of mild to moderate depression and increase suicides significantly among young adults (Fournier et all, 2010; Kirsch, 2014).
Consider long-term follow-up in my case: the surgeon will report a successful surgery, despite the fact that it took me almost two years to recover fully. (I did not die during surgery and left in seemingly good shape.). Although I called him numerous times for medical guidance during my complications, the outpatient surgical facility will report no complications since I was not transferred from that facility during the surgery to a hospital for continuing care. My insurance carrier that paid the majority of the medical bills recorded the invoices as separate unrelated events: one surgery/one bill, but three separate bills for the emergency room, an additional visit to my primary care physician to check my abdomen when my surgeon did not return my call, and the ongoing invoices from the urologist. They all reported success because the iatrogenic events were not linked to the initial procedure in the data base.
In my case, following surgery, I had to go to the emergency room on three separate occasions due to post-operative urinary retention, placing me at risk of permanent detrusor muscle damage. For more than 18 months, I was under the care of a urologist.
Over the past two years, my symptoms have included gastrointestinal inflammation, spasms, and abdominal bulging, which are only now disappearing. Even my posture has changed. I am now working to reverse the automatic flexing at the hips and leaning forward which I covertly learned to reduce the abdominal discomfort. This level of discomfort and dysfunction are new to me. Reading the research on laparoscopy, I realized that excessive internal bruising, large hematomas, and internal adhesions are fairly common with this type of surgery. However, soft tissue injuries are difficult to confirm with imaging techniques.
My complications were also a direct result of inappropriate post-surgical recommendations and treatment. The symptoms were further compounded by faulty patient discharge procedures performed by the outpatient surgical facility. Since this was my first general anesthesia, I had no idea that I would be one of the people whose outcome were not what the surgeon had predicted. Thus, hope for the best, but plan for the worst.
SCHEDULING MEDICAL PROCEDURES
The following are recommendations may help reduce post-surgical or medical procedure complications.
- Schedule elective medical procedures or surgery early the morning and in the middle of the week. Do not schedule procedures on Mondays, Fridays, or in the afternoon. Procedures performed in the afternoon have significant increase in complications and errors. Anesthesia complications, for example, are four times higher in the afternoon than in the morning (Wright et al, 2006). Our biological rhythms affect our ability to attend and focus. In the morning most people are able to concentrate better than in the afternoon (Pink, 2018).
- Avoid weekends. Procedures performed on weekends (as compared to those done in the middle of the week) increase the risk of complications or dying. For example, babies born on the weekend have a 9.2% higher infant mortality than those born during the week, while those born on Tuesdays have the lowest death rate (Palmer et al, 2015). It is possible that on Mondays medical staff are recovering from weekend binging, while on Fridays they are tired and looking forward to the weekend? If elective procedures are done on a Friday and complications arise, the emergency room is the only option, as the medical staff may not be available over the weekend. In my case the procedure was done on a Friday, and I left the surgical outpatient facility at 2 pm. When complications occurred, it was after 5:30 pm—phone support from the advice nurse and the surgeon on call were my only option until the following Monday. Thus, I had to go the emergency room late Friday evening and again the next evening because of urinary retention, with a long delay in a busy waiting room. Since, I wasn’t bleeding or having a heart attack, that meant I had to wait, wait and wait, which significantly aggravated my specific problem.
- Schedule medical procedures at least one or two weeks before any holiday. Do not schedule surgery just before or during holidays. Medical staff also take holidays and may not available. In my case, I scheduled the procedure the Friday before Thanksgiving because I thought I would have a week of recovery during my Thanksgiving break from teaching. This meant that medical staff were less available and more involved in their holiday planning.
- Schedule procedures so that you are released early in the day. This can allow you to return to the facility in case complications arise. I was released at 2 pm and the complications did not occur until early evening. The facility was closed, so the only option was the ER. When possible, schedule medical procedures or surgery in a facility that is able to provide post-operative care after 5 pm.
- Do not schedule elective procedures during the month of July in an academic teaching hospital. During this month mortality increases and efficiency of care decreases because of the end of the academic year and subsequent changeover to new personnel (Young et al, 2011). Medical school graduates with limited clinical experience begin their residencies and experienced house staff are replaced with new trainees. This is known as the July effect in the U.S. and Killing season in the United Kingdom. During the month of July in any given year, fatal medication errors, for example, increase by 10% at teaching hospitals, but not at neighboring hospitals which do not experience this turnover in medical personnel (Phillips & Barker, 2010).
- Have procedures performed at a medical facility in which the health care professional has no financial interest—take economics out of the equation. When health care practitioners have financial interest in a facility, they tend to order more tests and procedures than health care providers who have no financial interests (Bishop et al, 2010). In my case the surgeon had a financial interest in the outpatient surgical facility where I received surgery. Had I had the operation across the street in the hospital where the surgeon also operates, I probably would not have been released early, avoiding the problems in follow-up care.
STRATEGIES TO OPTIMIZE OUTCOMES AND HEALTH
Organize your support system. Assume that recovery could be more difficult then promised.
Before your procedure, ask family members, friends, and neighbors to be prepared to help. If you did not need them, thank them for their willingness to help. In my case I did not plan for complications, thus my wife was my entire support system, especially for the first three weeks when I was unable to do anything except rest and cope. I was very fortunate to have numerous family, friends, and colleagues who offered their expertise to help me understand what was going on and who assumed my responsibilities when needed.[1]
- Bring an advocate to your appointments. Have your advocate/friend keep notes and ask questions, especially if the health care provider is a respected authority and you are suffering, exhausted, and/or anxious. Record any detailed instructions you must follow at home as a video or audio file on your cell phone or write them down (be sure to ask the health provider for permission). Under stress one may not be able to fully process instructions from the health care provider.
- Make a list of questions and concerns before seeing your health care provider. Talk to your partner and close friends and ask them if there are questions or concerns that you should raise with your provider.
- Ask for more information when tests or procedures are proposed (Robin, 1984).
- Why do you recommend this particular test/procedure/intervention for me and what are the major benefits?
- What are the risks and how often do they occur, in your experience and in the research literature?
- What will you do if the treatment is not successful?
- Ask your provider if there is anything that you should or should not do to promote healing. As much as possible, ask for advice on specific efforts you can make. General statements without instructions such as, “Relax” or “Don’t worry,” are not helpful unless the practitioner teaches you specific skills to relax or to interrupt worrisome thoughts. Many health professionals do not have the time to teach you these types of skills. In many cases the provider may not be able to recommend documented peer-reviewed self-care strategies. Often they imply—and they can be correct—that the specific medical treatment is the only thing that will make you better. In my case I did not find any alternative procedures that would reverse a hernia, although there may be habitual postural and movement patterns that could possibly prevent the occurrence of a hernia (Bowman, 2016). Being totally dependent upon the medical procedure may leave you feeling powerless, helpless, and prone to worry. In most cases there are things you can do to optimize self- healing.
- Think outside the box. Explore other forms of self-care that could enhance your healing. Initiate self-care action instead of waiting passively. By taking the initiative, you gain a sense of control, which tends to enhance your immune system and healing potential. Do anything that may be helpful, as long as it is not harmful. In my case, future medical options to resolve urinary retention could include additional medications or even surgery. Researching the medical literature, there were a number of studies showing that certain herbs in traditional Chinese medicine and Ayurveda medicine could help to reduce prostate inflammation and possibly promote healing. Thus, I began taking three different herbal substances for which there was documented scientific literature. I also was prescribed herbal tea to sooth the bladder. Additionally, I reduced my sugar and caffeine intake to lower the risk of bladder irritation and infection.
- Collaborate with your health care provider. Let your provider know the other approaches you are using. Report any interventions such as vitamins, herbs, Chinese medicine. Ask if they know of any harm that could occur. In most cases there is no harm. The health care professional may just think it is a waste of time and money. However, if you find it helpful, if it gives you control, if it makes you less anxious, and if it is not harmful, it may be beneficial. What do you have to lose?
- Assume that all the health care professionals are committed to improving your health to the best of their ability. Yet at times professionals are now so specialized that they focus only on their own discipline and not the whole person. In their quest to treat the specific problem, they may lose sight of other important aspects of care. Thus, hope for the best, but plan for the worst.
PREPARING FOR SURGERY
Assume that the clinical staff will predict a more positive outcome than that reported in the medical literature. In most cases, especially in the United States, there is no systematic follow-up data since many post-surgical complications are resolved at another location. In addition, many studies are funded by medical companies which have a vested interest and report only the positive outcomes. The companies tend not to investigate for negative side-affects, especially if the iatrogenic effects occur weeks, months, or years after the procedure. This has also been observed in the pharmaceutical companies sponsoring studies for new medications.
Generally, when independent researchers investigated medical procedures they found the complication rate three-fold higher than the medical staff reported. For example, for endoscopic procedures such colonoscopies, doctors reported only 31 complications from 6,383 outpatient upper endoscopies and 11,632 outpatient colonoscopies. The actual rate was 134 trips to the emergency room and 76 hospitalizations. This discrepancy occurred because the only incidents reported involved patients who went back to their own doctors. It did not capture those patients who sought help at other locations or hospitals (Leffler et al, 2010).
The data are even worse for patients who are hospitalized; in the U.S. 20% of patients who leave the hospital return within a month while in England, 7% of those leaving the hospital return within a month (Krumholz, 2013).
- Ask about possible complications that could arise, the symptoms, and what the physician would do if they occurred. Do not assume the health professional will have the time to explain or know all the possible complications. In my case when the surgeon removed the catheter at 4 pm during my second emergency room visit, I had to ask, “What would happen if I still cannot urinate?” Again, the emergency room was the only answer. However, I know now that he could have taught me simple self-catherization which would have eliminated the long waiting in the emergency room, the excessive stretching of the bladder and the subsequent emergency room medical error on my third visit to the ER. It would also have reduced the medical costs by a thousand-fold.
- Get a second opinion. In my case, the surgeon came highly recommended, is very experienced, and has done many hernia repairs. I trusted his judgement that I needed a bilateral hernia repair although I only felt the bulging in the right inguinal area and did not feel bulging or sensations in the left inguinal area. Despite my feeling of trust, I should have asked for a second independent opinion just to be sure. In many moments of despair when suffering the significant complications, I even started to wonder if the bilateral laparoscopic surgical repair was really necessary or just done to increase the income of the surgeon and the outpatient surgical facility in which he had a financial interest. My surgery resulted in large hematomas, irritation of internal organs, and possible damage to the GI track. This type of complication did not occur for a close friend who had a single-sided hernia repair by the same surgeon in a hospital where the surgeon had no financial interests.
- Request medical personnel who are highly experienced in the intervention. Mortality and complications rates are significantly lower for practitioners who have done the procedure at least 250 times.
- Don’t assume the worst but be prepared for the worst. Ask your health care provider about the various side effects of surgery, including the worst things that could happen, and then develop a pre-emptive plan.
The most common problems associated with surgery and general anesthesia include:
- Urinary retention. Following general anesthesia, neural enervation to the bladder and gastrointestinal tract are often affected. The general risk for postoperative urinary retention (POUR) for all types of surgeries ranges from 7% to 52% (Tammela et al, 1986; Petros et al, 1990; Petros et al, 1991; Gonullu et al, 1993; Tammela, 1995). For patients who have surgery for hernia repair 24.4% will experience postoperative urinary retention (Keita et al, 2005)—one in four. The risk for older males is even higher (Blair et al, 2017). Do not leave the medical unit until you have urinated or have a Foley catheter inserted with a leg bag and appropriate follow-up managed by a urologist. In my case, neither the surgeon nor the outpatient hospital checked to determine whether I could urinate—they just discharged me the moment I was conscious. Discharging a patient who has had general anesthesia without checking to determine whether they can urinate goes against all medical guidelines and standard hospital policies and constitutes malpractice. As this was my first surgery, I had no idea that urinary retention could occur. Thus, I did not recognize the symptoms nor did the advice nurse or the surgeon when called for advice before I checked into the emergency room.
- Expect constipation and plan to eat a high roughage diet that supports bowel movements. In case bowel function is slow in resuming, you may want to have on hand simple over-the-counter supplements such as magnesium capsules, psyllium husks, and aloe vera juice or gel, all available at any health food store. Liquid magnesium citrate (GoLytely® solution available at drug stores), can be useful, but tends to be a little stressful to take. Check these over-the-counter supplements with your provider to avoid supplement-drug interaction.
- Infection. Many patients pickup hospital-induced infections (nosocomial infections). In my case, I after four weeks with a Foley catheter, I got a mild bladder infection and had to control it with antibiotics. While in the hospital, avoid direct physical contact with other patients and staff, wash and rewash your hands. Remember medical staff tend are less attentive and wash their hands 10% less in the afternoons than in morning. Ask the medical staff to thoroughly wash their hands before they examine you. If you do get an infection, contact your medical provider immediately.
ACTION STEPS
- Pace yourself. Assume that recovery could be slower than promised. Although your body may appear to be healed, in many cases your vitality could be significantly reduced for a number of months, and you will probably feel much more fatigued in the evening. The recovery from general anesthesia has been compared to recovery from a head-on car collision.
- Identify your support system in case you cannot take care of yourself initially. Organize family and friends to help you. In my case, for the first two weeks I did not have the energy to do anything for myself—the overwhelming abdominal spasms and the three episodes in the ER had drained my energy. I was very lucky that I had my family and friends to help me. For the first few weeks I was so distracted by the pain and discomfort that I did not drive or take care of myself.
- Have a plan in case you need to go to the Emergency Room in the evening. Know its location and have someone who can take you.
- Assume that you will probably have an extensive wait in the ER unless you are desperately ill. Do not try to “tough it out.” Be totally honest about your level of pain, so you can get the best possible care. In my case, I had horrible abdominal pain and spasms with urinary retention, but still acted as if I were okay. When the admitting nurse asked me how I felt, I rated my discomfort as a 5 on a scale from 0 to 10. In my mind I compared the pain with that I had experienced after a skiing accident, which was much worse. What I had forgotten was that the ER is triage system, so I had to wait and wait and wait, which was phenomenally uncomfortable.
- In the ER, ask which medical specialist can follow up with you if further issues develop. A general hospital usually has specialists on call. In my case, if I had requested care from a specialist, I would have been treated directly by a urologist. I would not have had to follow the advice of the surgeon who said, “When you go to Emergency Room, have them empty the bladder and then go home.” Almost all urologists would have recommended keeping the Foley catheter in for a few days to allow the side effects of the anesthesia and the trauma caused by the bladder expansion to ameliorate and then test whether urination was possible.
- Have a medical advocate with you at all times who can observe that the procedures are done correctly. There is a four-fold increase in errors during the evenings and nights as compared to the morning. The more medical staff is multi-tasking, the more likely they will make errors. Have the medical personnel explain any procedure before they perform it—why and how they will do the procedure and what you will experience. You also need to know if they are experienced in that particular procedure? If the answers do not make sense, stop them and ask for another staff member.
- In the ER, record the instructions on your phone. Have medical staff explain and demonstrate to you and your support person what you will need to do at home. Then repeat the instructions back to them to be certain you have it right.
- Remind yourself that errors can occur. In my case, during the third ER visit for urinary retention, the nurse delayed the anchoring of the catheter and it had slipped down into the urethra. As she began to pump, I could feel my urethra tearing and I alerted her to stop. This was immediately followed by another procedural error on her part, so I had to again alert her to stop, which she finally did. All this occurred at 1 am in the morning. As the patient, I had to take charge at a time when I was totally exhausted. As the nurse retreated, I was left sitting on the gurney waiting for someone to come and follow-up. I waited and waited and when I finally stood up, the catheter dropped out and I began bleeding.
Lesson learned: hope for the best but prepare for the worst. In my situation, after eight weeks and numerous visits to the urologist, he removed the catheter. He did this at 8:30 in the morning. This way I could go home and in case something happened, I could go back to his office for further care. Before leaving the office, I planned for the worst. I asked what would happen if I could not urinate later in the evening and requested that he give me a few catheters, so if problems developed, I could catheterize myself.
The urologist gave me the catheters and explained how to use them, although I did not actually practice on myself. Still, I felt better prepared. During the day, I become more and more optimistic because I had no problems; however, at 2 am I woke up unable to urinate. For the next hour, I felt very anxious about inserting the catheter, since I had never done it myself. Finally, my discomfort overcame my anxiety. To my surprise, it was easy. After waiting a few minutes, I removed the catheter and went to bed feeling much more comfortable. The next morning after breakfast and a cup of coffee, I found that my body was working fine without the catheter.
Had I not planned for the worst, I would have once again gone to the Emergency Room and probably waited for hours, risking a repeat of tremendous discomfort and irritation. This simple planning reduced my medical cost more than a thousand-fold from $1700 for the emergency room to $2 for some single-use catheters.
References
Angell, M. (2009). Drug companies & doctors: A story of corruption. The New York Review of Books, 56(1), 8-12. http://www.nybooks.com/articles/2009/01/15/drug-companies-doctorsa-story-of-corruption/
Bishop, T.F., Federman, A.D., & Ross, J.S. (2010). Laboratory test ordering at physician offices with and without on-site laboratories, Journal of Gen Intern Med, 25(10)m 1057-1063. doi: 10.1007/s11606-010-1409-7
Blair, A.B., Dwarakanath, A., Mehta, A., Liang, H., Hui, X., Wyman, C., Ouanes, J.P.P., & Nguyen, H.T. (2017). Postoperative urinary retention after inguinal hernia repair: a single institution experience. Hernia, 21(6), 895-900.
Bowman, K. (2016). Diastasis Recti: The whole-body solution to abdominal weakness and separation. Propriometrics Press: Carlsborg, WA 98324
Davis, C., Naci, N., Gurpinar, E., Poplavska, E., Pinto, A., Aggarwal, A. (2017). Availability of evidence of benefits on overall survival and quality of life of cancer drugs approved by European Medicines Agency: retrospective cohort study of drug approvals 2009-13. BMJ, 2017; j4530 DOI: 10.1136/bmj.j4530
Ferguson, T. B. (2012). The Institute of Medicine Committee report “best care at lower cost: the path to continuously learning health care”. Circulation: Cardiovascular Quality and Outcomes, 5(6), e93-e94. http://jama.jamanetwork.com/article.aspx?articleid=185157
Fournier, J. C., DeRubeis, R. J., Hollon, S. D., Dimidjian, S., Amsterdam, J. D., Shelton, R. C., & Fawcett, J. (2010). Antidepressant drug effects and depression severity: a patient-level meta-analysis. JAMA, 303(1), 47-53.
Gönüllü, N. N., Gönüllü, M., Utkan, N. Z., Dülger, M., Gökgöz, S., & Karsli, B. (1993). Postoperative retention of urine in general surgical patients. The European journal of surgery= Acta chirurgica, 159(3), 145-147.
Horton, R. (2015). Offline: What is medicine’s 5 sigma? The Lancet, 385(9976), 1380. http://www.thelancet.com/journals/lancet/article/PIIS0140-6736%2815%2960696-1/fulltext?rss%3Dyes
Institute of Medicine’s Infographic, accompanying their 2012 report, Best Care at Lower Cost, at http://www.iom.edu/Reports/2012/Best-Care-at-Lower-Cost-The-Path-to-Continuously-Learning-Health-Care-in-America/Infographic.aspx
Keita, H., Diouf, E., Tubach, F., Brouwer, T., Dahmani, S., Mantz, J., & Desmonts, J. M. (2005). Predictive factors of early postoperative urinary retention in the postanesthesia care unit. Anesthesia & Analgesia, 101(2), 592-596.
Kim, C. & Prasad, V. (2015). Cancer drugs approved on the basis of a surrogate end point and subsequent overall survival-An analysis of 5 Years of US Food and Drug Administration approvals. JAMA Intern Med,175(12):1992-1994. doi:10.1001/jamainternmed.2015.5868
Kirsch, I. (2014). The emperor’s new drugs: medication and placebo in the treatment of depression. In Placebo (pp. 291-303). Springer Berlin Heidelberg.
Kohn, L. T., Corrigan, J. M., & Donaldson, M. S. (Eds.). (2000). To err is human: building a safer health system (Vol. 6). National Academies Press. http://www.ncbi.nlm.nih.gov/books/NBK221671/
Krumholz, H. M. (2013). Post-hospital syndrome—an acquired, transient condition of generalized risk. New England Journal of Medicine, 368(2), 100-102. http://www.nejm.org/doi/full/10.1056/NEJMp1212324
Leffler, D.A, Kheraj, R., Garud, S., Neeman, N., Nathanson, L.A., Kelly, C.P., Sawhney, M., Landon, B., Doyle, R., Rosenberg, S., & Aronson, M. (2010). The incidence and cost of unexpected hospital use after scheduled outpatient endoscopy. Arch Intern Medicine, 170(19), 1752-1757. http://archinte.jamanetwork.com/article.aspx?articleid=226125
Makary, M.A. & Daniel, M. (2016). Medical error–the third leading cause of death in the US. British Medical Journal, 353:i2139
Neumayer, L., Giobbie-Hurder, A., Jonasson, O., Fitzgibbons Jr, R., Dunlop, D., Gibbs, J., & Henderson, W. (2004). Open mesh versus laparoscopic mesh repair of inguinal hernia. New England Journal of Medicine, 350(18), 1819-1827. http://academicdepartments.musc.edu/surgery/education/resident_info/journal_club/09-10/April-inguinal.pdf
Palmer, W. L., Bottle, A., & Aylin, P. (2015). Association between day of delivery and obstetric outcomes: observational study. BMJ, 351, h5774. http://www.bmj.com/content/bmj/351/bmj.h5774.full.pdf
Peper, E. & Harvey, R. (2017). The fallacy of the placebo controlled clinical trials: Are positive outcomes the result indirect treatment side effects? NeuroRegulation. 4(3–4):102–113 2017 doi:10.15540/nr.4.3-4.102
Perugini, R. A., & Callery, M. P. (2001). Complications of laparoscopic surgery. http://www.ncbi.nlm.nih.gov/books/NBK6923/?report=reader
Petros, J. G., & Bradley, T. M. (1990). Factors influencing postoperative urinary retention in patients undergoing surgery for benign anorectal disease. The American Journal of Surgery, 159(4), 374-376.
Petros, J. G., Rimm, E. B., Robillard, R. J., & Argy, O. (1991). Factors influencing postoperative urinary retention in patients undergoing elective inguinal herniorrhaphy. The American Journal of Surgery, 161(4), 431-433.
Phillips, D. P., & Barker, G. E. (2010). A July spike in fatal medication errors: a possible effect of new medical residents. Journal of General Internal Medicine, 25(8), 774-779. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2896592/
Pink, D.H. (2018). When: The Scientific Secrets of Perfect Timing. New York: Riverhead Books, ISBN-13: 978-0735210622
Robins, E.D. (1984). Matter of Life & Death: Risks vs. Benefits of Medical Care. New York: W.H. Freeman and Company.
Sauerland, S., Walgenbach, M., Habermalz, B., Seiler, C. M., & Miserez, M. (2011). Laparoscopic versus open surgical techniques for ventral or incisional hernia repair. The Cochrane Library.
Tammela, T. (1994). Postoperative urinary retention–why the patient cannot void. Scandinavian Journal of Urology and Nephrology. Supplementum, 175, 75-77.
Tammela, T., Kontturi, M., & Lukkarinen, O. (1986). Postoperative urinary retention: I. Incidence and predisposing factors. Scandinavian Journal of Urology and Nephrology. 20(3), 197-201.
Vigneswaran, Y., Gitelis, M., Lapin, B., Denham, W., Linn, J., Carbray, J., & Ujiki, M. (2015). Elderly and octogenarian cohort: Comparable outcomes with nonelderly cohort after open or laparoscopic inguinal hernia repairs. Surgery, 158(4), 1137-1144.
Weingart, S. N., Wilson, R. M., Gibberd, R. W., & Harrison, B. (2000). Epidemiology of medical error. BMJ: British Medical Journal, 320(7237), 774. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1117772/
Wright, M.D., Philips-Bute, B., Mark, J.B., Stafford-Smith, M., Grichnik, K.P., Andregg, B.C., & Taekman, J.M. (2006). Time of day effects on the incidence of anesthetic adverse events. Quality and Safety in Health Care. 15(4): 258–263.doi: 10.1136/qshc.2005.017566
Young, J. Q., Ranji, S. R., Wachter, R. M., Lee, C. M., Niehaus, B., & Auerbach, A. D. (2011). “July effect”: impact of the academic year-end changeover on patient outcomes: a systematic review. Annals of Internal Medicine, 155(5), 309-315. http://www.girardslaw.com/library/July_Effect_Annals_of_Internal_Medicine.pdf
[1] I think my family, friends and colleagues (Karen Peper, Norihiro Muramatsu, Richard Harvey, David Wise, Annette Booiman, Lance Nagel and many others) who generously supported me during this journey.
Behave: The biology of humans at our best and worst
Posted: February 24, 2018 Filed under: behavior, emotions, Evolutionary perspective, Pain/discomfort, Uncategorized | Tags: compassion, evil, goodness 2 CommentsHow can people be so caring and sometimes cruel? What are the evolutionary, genetic, epigenetic, developmental, familial, tribal, community and cultural determinants that allow human beings to be heroic and give their own life for others or be killers and unbelievably cruel. Stanford biology professor Robert Sapolsky‘s book, Behave: The Biology of Humans at Our Best and Worst, explores what drives human behavior. It is a remarkable tour de force to explore and explain why we do as we do. Watch his February 6, 2018 lecture at the Jewish Community Center of San Francisco.
https://www.jccsf.org/arts-ideas/ondemand/2017-2018-season/robert-sapolsky/

How effective is treatment? The importance of active placebos
Posted: December 16, 2017 Filed under: Pain/discomfort, placebo, self-healing, stress management, Uncategorized | Tags: Active placebo, Clinical trials, expectancy, hope, nocebo, passive placebo, placebo 3 CommentsAdapted by Erik Peper and Richard Harvey from: Peper, E. & Harvey, R. (2017). The fallacy of the placebo-controlled clinical trials: Are positive outcomes the result of “indirect” treatment effects? NeuroRegulation, 4(3–4), 102–113. http://dx.doi.org/10.15540/nr.4.3-4.102
How come some drugs or medical procedures are initially acclaimed to be beneficial and later ineffective or harmful and withdrawn from the market?
How come some patients with a cancer diagnosis experience symptom remission after receiving a placebo medication? Take the case of Mr. Wright. Several decades ago Dr. Klopher (1957) described Mr. Wright as a patient who had a generalized and far advanced malignancy in the form of a lymphosarcoma with an estimated life expectancy of less than two weeks. Following the diagnosis Mr. Wright read a newspaper article about a promising experimental cancer medication called Krebiozen and requested that he receive the latest treatment. Soon after receiving the drug, Mr. Wright had a complete remission of cancer symptoms with no signs of the deadly tumor. For over two months after receiving the new promising drug, Krebiozen, Mr. Wright engaged in a normal life and was even able to fly his own plane at 12,000 feet. After a promising introduction to the medication, Mr. Wright subsequently read another newspaper article which proved the new medication to be a useless, inert preparation. Confused and demoralized, the results of the wonder drug did not last and his symptoms returned. When the final AMA announcement was published “Nationwide tests show Krebiozen to be a worthless drug in treatment of cancer,” his symptoms became acute and he died within two days (Klopher, 1957).
The term placebo loosely translates as ‘I shall please you’ can be contrasted with the term nocebo which loosely translates as ‘I shall harm you’ when referring to exposure to a sham medication, treatment or procedure that results a positive outcome (placebo response), or a negative outcome (nocebo response), respectively. The responses a person has reflect a complex interaction between many processes. For example, when studying a placebo or nocebo response we measure internal psychological processes, measured in terms of a person’s self-reported attitudes, beliefs, cognitions and emotions; behavioral processes, measured overtly by observations of a person’s actions; and, physiological processes, measured more or less directly with instruments such as heart rate monitors, or biochemical analyses. Most relevant is that a person’s beliefs about the placebo (or nocebo) medication, treatment or procedure leads to predictable positive (or negative) behaviors and physiological benefits or harms.
The case of Mr. Wright illustrates that we may underestimate the positive power of the placebo or, the negative power of the nocebo, where Mr. Wright’s belief about the medication’s benefits first interacted in a positive way (placebo) with his behaviors (e.g. engaging in daily activities including flying an airplane) as well as his physiology (e.g. cancer remission) and unfortunately later, in a negative way (nocebo) interacting with his physiology (e.g. cancer return) contributing to his death.
The placebo response can be very powerful and healing. For example, watch the very dramatic demonstration of how the placebo response can be optimized in Derren Brown’s BBC video Fear and Faith Placebo https://www.youtube.com/watch?v=y2XHDLuBZSw).
Placebo and nocebo effects are found in all therapeutic transactions when the communications between therapist and patient reflect embedded beliefs about the treatment. For example, patients have faith in clinician’s knowledge and belief that a prescribed medication is going to be effective at treating their symptoms, which then reinforces the patient’s belief in the medication, increasing indirect, embedded placebo effects, above and beyond any direct effects from the medication. The indirect effects of placebo responses have been most studied with medications; however, placebo effects are also studied in non-drug therapies. The research on placebo effects has demonstrated time and time again that when patients expect that the drug, surgery, or other therapeutic technique to be beneficial, then the patients tend to benefit more from the treatment.
The expectancy that the treatment will be effective at reducing symptoms is overtly, and covertly communicated by the health care professional during patient interactions, as well as by drug companies through direct to consumer advertising, and social media. The implied message is that the drug or procedure will improve symptoms, recovery or improve quality of life. On the other hand, if you do not do take the drug or do the procedure, your health will be compromised. For example, if you have high cholesterol, then take a statin drug to prevent the consequences of high cholesterol such as a heart attack or stroke. The implied message is that if you do not take it, you will die significantly sooner. Statins lower the risk for heart attacks; however, the benefits may be over stated. For people without prior heart disease, 60 people will have to take statins for 5 years to prevent 1 heart attack and 268 people to prevent 1 stroke. During the same time period 1 in 10 will experience muscle damage and 1 in 50 develop diabetes (theNNT, 2017 November).
If placebo and nocebo can have significant effects on medical outcome, how do you know if the treatment benefits are due to the direct effects of a drug or procedure or due to any indirect placebo effects or a combination of both?
The randomized controlled trial (RCT) is considered the gold standard method to determine the effectiveness of a drug or procedure. The ideal study would be a double blind, randomized, placebo controlled clinical trial in which neither the practitioner nor the patient would know who is getting what condition. For example, blinding implies the placebo group would receive a pill that appears identical to a ‘real’ pill, except the placebo has pharmacological ingredients. Similarly, a patient may receive an ‘exploratory’ surgery in which anesthesia is given and the skin is cut however the no further actual internal surgery occurs because the surgeon determined further internal surgery was unnecessary. Although, it is not possible to perform a double blind surgery study, the patient may be totally unaware whether an internal surgery had occurred.
Peper and Harvey (2017) point out that the positive findings of an ‘effective’ treatment are not always the results of the direct effects of medications and may be more attributable to indirect placebo responses. For example, patients may attribute the ‘effectiveness’ of the treatment to their experience of ‘non-directed’ treatment side effects that include: the post-surgical discomfort which signals to the patient that the procedure was successful, or a dry mouth and constipation that were caused by the antidepressant medication, which signals to the person that the trial medication or procedure-related medication is working (Bell, Rear, Cunningham, Dawnay, & Yellon, 2014; Stewart-Williams & Podd, 2004).
Just imagine the how pain can evoke totally different reactions. If you recently had a heart attack and then later experienced pain and cramping in the chest, you automatically may feel terrified as you could interpret the pain as another heart attack. The fear response to the pain may increase pathology and inhibit healing (a nocebo response). On the other hand, after bypass surgery, you may also experience severe pain when you move your chest. In this case, you interpret the pain as a sign that the bypass surgery was successful, which then reduces fear and reinforces the belief that you have survived a life threatening situation and will continue healing (placebo response).
Many research studies employ a placebo control, however what is less typical is a double-blind study using an ‘active’ placebo (Enck, Bingel, Schedlowski, & Rief, 2013). Less than 0.5% of all placebo studies include an active placebo group. (Shader, 2017; Jensen et al, 2017).
Unfortunately, a typical ‘placebo controlled’ study design is problematic for distinguishing the direct from any indirect (covert) placebo effects that occur within the study as shown in Figure 1.
 Figure 1. Normal (passive) placebo control group controls and experimental group. What is not assessed are placebo benefits induced by the medication/treatment induced side effects.
Figure 1. Normal (passive) placebo control group controls and experimental group. What is not assessed are placebo benefits induced by the medication/treatment induced side effects.
With a passive placebo, there is no way to know if the observed benefits are from the medication/medical procedure, or from the placebo/self-healing response triggered by the medication/medical procedure (or both combined, or neither the placebo or medical procedure). The best way to know if the treatment is actually beneficial is to use an ‘active’ placebo instead of a passive placebo.
An active placebo builds on a patient’s attributions about a medication or medical procedure. For example, a patient may be told by a clinician that feeling any side effects such as insomnia, a racing heart or, experiencing a warm flushing feeling will let them know the medication is working, so the patient becomes conditioned to expect the medication is working when they feel or experience side effects. Whereas a passive (inert) placebo such as a sugar pill will have effects that are extremely subtly felt or experienced, an active placebo will have effects that are more overtly felt or experienced. Examples of active placebos include administering low doses of caffeine or niacin that have effects which may be felt internally however which do not have the same effects as the medication. When a patient is told they may have side effects from the medication that include felt changes in heart rate or a flushing feeling, the patient attributes the changes they feel to a medication they believe will bring about benefits, even though the changes are rightfully attributed to the caffeine or niacin in the active placebo.
An active placebo triggers observed and felt body changes which do not affect the actual illness. For surgical procedures, an ‘active’ placebo control would be a sham/mock surgery in which the patient would undergo the same medical procedure (e.g. external surgery incision) without continuing some internal surgical procedure (Jonas et al, 2015). In numerous cases of accepted surgery, such as the Vineberg procedure (Vineburg & Miller, 1951) for angina, or arthroscopic knee surgery for treating osteoarthritis, the clinical benefits of a sham/mock surgery were just as successful as the actual surgery. Similar studies suggest the clinical benefits were solely (or primarily) due directly to the placebo response (Beecher, 1961; Cobb et al, 1959; Moseley et al, 2002).
To persuasively demonstrate that a treatment or therapeutic procedure is effective it should incorporate a study design using an active placebo arm as shown in Figure 2. Figure 2. Active placebo control group controls for the normal placebo benefits plus those placebo benefits induced by the medication/treatment induced side effects.
Figure 2. Active placebo control group controls for the normal placebo benefits plus those placebo benefits induced by the medication/treatment induced side effects.
Some treatments may be less effective then claimed because they were not compared to an active placebo, which could be one of the reasons why so many medical and psychological studies cannot be replicated. The absence of ‘active’ placebo controls may also be a factor explaining why some respected authorities have expressed some doubt about published scientific medical research results. Following are two quotes that illustrate such skepticism.
“Much of the scientific literature, perhaps half, may simply be untrue.” —Richard Horton, editor-in-chief of the Lancet (Horton, 2015).
“It is simply no longer possible to believe much of the clinical research that is published, or to rely on the judgment of trusted physicians or authoritative medical guidelines. I take no pleasure in this conclusion, which I reached slowly and reluctantly over my two decades as an editor of the New England Journal of Medicine” —Dr. Marcia Angell, longtime Editor in Chief of the New England Medical Journal (Angell, 2009).
There are a variety of questions to ask before agreeing on a procedure or before taking medication
A quick way to ask whether a medication or medical treatment effectiveness is the result of placebo components is to ask the following questions:
- Have there been successful self-care or behavioral approaches beyond surgical or pharmaceutical treatments that have demonstrated effectiveness? When successful treatments are reported, then questions are raised whether pharmaceutical or surgical outcomes are also attributable to the result of placebo effects. On the other hand, if there a no successful self-care approaches, then the benefits may be more due to the direct therapeutic effect of a surgical procedure or medication.
- Has the procedure been compared to an active placebo control? If not, then to what extent it is possible that the results of the surgical or pharmaceutical therapy could be attributed to a placebo response instead of directly to the medication or surgery?
- What are the long term benefits and complication rates of the medication, treatment or procedure? When benefits are low and risks of the procedure are high, explore the risks associated with ‘watchful waiting’ (Colloca, Pine, Ernst, Miller & Grillon, 2016; Thomas et al, 2014; Taleb, 2012).
Unfortunately, most clinical studies that includes pharmaceuticals and/or surgery do not test their medication, surgery against an ‘active’ placebo. Whenever possible, enquire whether an active placebo was used to determine the degree of effectiveness of the proposed treatment or procedure. Fortunately, the design of ‘active’ placebo-controlled studies is very possible for anyone interested in comparing the effectiveness of medications, treatments and procedures in various settings, from hospitals and clinics to university classrooms and individual homes.
In summary, the benefits of the treatment must significantly outweigh any risks of negative treatment side effects. Short-term treatment benefits need to be balanced by any long-term benefits. Unfortunately, short-term benefits may lead to significant, long-term harm such as in the use of some medications (e.g. sleep medications, opioid pain killers) that result in chronic dependency and which lead to a significant increase in morbidity and mortality of many kinds. We suggest that more medications and other procedures are tested against an active placebo to investigate whether the medication or procedure is actually effective.
For a detailed analysis and discussion of placebo and the importance of active placebo see our article, Peper, E. & Harvey, R. (2017). The fallacy of the placebo-controlled clinical trials: Are positive outcomes the result of “indirect” treatment effects? NeuroRegulation, 4(3–4), 102–113. http://dx.doi.org/10.15540/nr.4.3-4.102
References:
Angell M. Drug companies and doctors: A story of corruption. January 15, 2009. The New York Review of Books 56. Available: http://www.nybooks.com/articles/archives/2009/jan/15/drug-companies-doctorsa-story-of-corruption/. Accessed 24, November, 2016.
Beecher, H. K. (1961). Surgery as placebo: A quantitative study ofbias. JAMA, 176(13), 1102–1107. http://dx.doi.org/10.1001/jama.1961.63040260007008
Bell, R. M., Rear, R., Cunningham, J., Dawnay, A., & Yellon, D. M. (2014). Effect of remote ischaemic conditioning on contrast-induced nephropathy in patients undergoing elective coronary angiography (ERICCIN): rationale and study design of a randomised single-centre, double-blind placebo-controlled trial. Clinical Research in Cardiology, 103(3), 203-209. http://dx.doi.org/10.1007/s00392-013-0637-3
Cobb, L. A., Thomas, G. I., Dillard, D. H., Merendino, K. A., & Bruce, R. A. (1959). An evaluation of internal-mammary-artery ligation by a double-blind technic. New England Journal of Medicine, 260(22), 1115–1118. http://dx.doi.org/10.1056/NEJM195905282602204
Colloca, L., Pine, D. S., Ernst, M., Miller, F. G., & Grillon, C. (2016). Vasopressin boosts placebo analgesic effects in women: A randomized trial. Biological Psychiatry, 79(10), 794–802. http://dx.doi.org/10.1016/j.biopsych.2015.07.019
Derren Brown’s BBC video Fear and Faith Placebo https://www.youtube.com/watch?v=y2XHDLuBZSw
Enck, P., Bingel, U., Schedlowski, M., & Rief, W. (2013). The placebo response in medicine: minimize, maximize or personalize?. Nature reviews Drug discovery, 12(3), 191-204. http://dx.doi.org/10.1038/nrd3923
Horton, R. (2015). Offline: What is medicine’s 5 sigma. The Lancet, 385(9976), 1380. http://www.thelancet.com/pdfs/journals/lancet/PIIS0140-6736%2815%2960696-1.pdf
Jensen, J. S., Bielefeldt, A. Ø., & Hróbjartsson, A. (2017). Active placebo control groups of pharmacological interventions were rarely used but merited serious consideration: A methodological overview. Journal of Clinical Epidemiology. https://doi.org/10.1016/j.jclinepi.2017.03.001
Jonas, W. B., Crawford, C., Colloca, L., Kaptchuk, T. J., Moseley, B., Miller, F. G., & Meissner, K. (2015). To what extent are surgery and invasive procedures effective beyond a placebo response? A systematic review with meta-analysis of randomised, sham controlled trials. BMJ open, 5(12), e009655. http://dx.doi.org/10.1136/bmjopen-2015-009655
Klopfer, B., (1957). Psychological Variables in Human Cancer, Journal of Projective Techniques, 21(4), 331–340. http://www.tandfonline.com/doi/abs/10.1080/08853126.1957.10380794
Moseley, J. B., O’Malley, K., Petersen, N. J., Menke, T. J., Brody, B. A., Kuykendall, D. H., … Wray, N. P. (2002). A controlled trial of arthroscopic surgery for osteoarthritis of the knee. The New England Journal of Medicine. 347(2), 81–88. http://dx.doi.org/10.1056 /NEJMoa013259
Peper, E. & Harvey, R. (2017). The fallacy of the placebo-controlled clinical trials: Are positive outcomes the result of “indirect” treatment effects? NeuroRegulation, 4(3–4), 102–113. http://dx.doi.org/10.15540/nr.4.3-4.102
Shader, R. I. (2017). Placebos, Active Placebos, and Clinical Trials. Clinical Therapeutics, 39(3), 451–454. http://dx.doi.org/10.1016/j.clinthera.2017.02.001
Stewart-Williams, S., & Podd, J. (2004). The placebo effect: dissolving the expectancy versus conditioning debate. Psychological bulletin, 130(2), 324. http://dx.doi.org/10.1037/0033-2909.130.2.324
Taleb, N. N. (2012). Antifragile: Things that gain from disorder. Random House.
TheNNT (2017, November). http://www.thennt.com/nnt/statins-for-heart-disease-prevention-without-prior-heart-disease/
Thomas, R., Williams, M., Sharma, H., Chaudry, A., & Bellamy, P. (2014). A double-blind, placebo-controlled randomised trial evaluating the effect of a polyphenol-rich whole food supplement on PSA progression in men with prostate cancer—the UK NCRN Pomi-T study. Prostate Cancer and Prostatic Diseases, 17(2), 180–186. http://dx.doi.org/10.1038/pcan.2014.6
Vineberg, A., & Miller, G. (1951). Treatment of coronary insufficiency. Canadian Medical Association Journal, 64(3), 204. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1821866/pdf/canmedaj00654-0019.pdf
Breathing to improve well-being
Posted: November 17, 2017 Filed under: Breathing/respiration, Exercise/movement, Neck and shoulder discomfort, Pain/discomfort, self-healing, stress management, Uncategorized | Tags: anxiety, Breathing, health, mindfulness, pain, respiration, stress 9 CommentsBreathing affects all aspects of your life. This invited keynote, Breathing and posture: Mind-body interventions to improve health, reduce pain and discomfort, was presented at the Caribbean Active Aging Congress, October 14, Oranjestad, Aruba. www.caacaruba.com
The presentation includes numerous practices that can be rapidly adapted into daily life to improve health and well-being.
Enjoy sex: Breathe away the pain*
Posted: March 19, 2017 Filed under: Breathing/respiration, Pain/discomfort, self-healing, Uncategorized | Tags: Breathing, dyspareunia, intercourse, intimacy, pain, pelvic floor, relaxation, Sexuality, vaginismus 15 CommentsAdapted from: Peper, E. & Cohen, T. (2017). Inhale to breathe away pelvic floor pain and enjoy intercourse. Biofeedback, 45(1), 21–24. https://doi.org/10.5298/1081-5937-45.1.04
“After two and a half years of trying, ups and downs, and a long period of thinking it will never happen, it did happen. I followed your advice by only applying pressure with the cones while inhaling and at the same time relaxing the pelvic floor. We succeeded! we had “real” sex in the first time.”
Millions of women experience involuntary contraction of the musculature of the outer third of the vagina (vaginismus) interfering with intercourse, causing distress and interpersonal difficulty (ter Kuile et, 2010) or pain during intercourse (dyspareunia). It is estimated that 1 to 6% of women have vaginismus (Lewis et al, 2004) and 6.5% to 45.0% in older women and from 14% to 34% in younger women experience dyspareunia (Van Lankveld et al, 2010; Gross & Brubaker, 2022). The most common treatment for vaginismus is sequential dilation of the vaginal opening with progressively larger cones, psychotherapy and medications to reduce the pain and anxiety. At times clients and health care professionals may be unaware of the biological processes that influence the muscle contraction and relaxation of the pelvic floor. Success is more likely if the client works in harmony with the biological processes while practicing self-healing and treatment protocols. These biological processes, described at the end of the blog significantly affects the opening of vestibule and vagina are: 1) feeling safe, 2) inhale during insertion to relax the pelvic floor, 3) stretch very, very slowly to avoid triggering the stretch reflex, and 4) being sexual aroused.
Successful case report: There is hope to resolve pain and vaginismus
Yesterday my husband and I had sex in the first time, after two and a half years of “trying”. Why did it take so long? Well, the doctor said “vaginismus”, the psychologist said “fear”, the physiotherapist said “constricted muscles”, and friends said “just relax, drink some wine and it will happen”.
Sex was always a weird, scary, complicated – and above all, painful – world to me. It may have started in high school: like many other teens, I thought a lot about sex and masturbated almost every night. Masturbation was a good feeling followed by tons of bad feelings – guilt, shame, and feeling disgusting. One of the ideas I had to accept, later in my progress, is that ‘feeling good is a good thing’. It is normal, permitted and even important and healthy.
My first experience, at age 20, was short, very painful, and without any love or even affection. He was…. well, not for me. And I was…. well, naive and with very little knowledge about my body. The experiences that came after that, with other guys, were frustrating. Neither of them knew how to handle the pain that sex caused me, and I didn’t know what to do.
The first gynecologist said that everything is fine and I just need to relax. No need to say I left her clinic very angry and in pain. The second gynecologist was the first one to give it a name: “vaginismus”. He said that there are some solutions to the problem: anesthetic ointment, physiotherapy (“which is rarely helps”, according to his optimistic view..), and if these won’t work “we will start thinking of surgery, which is very painful and you don’t want to go there”. Oh, I certainly didn’t want to go there.
After talking to a friend whose sister had the same problem, I started seeing a great physiotherapist who was an expert in these problems. She used a vaginal biofeedback sensor, that measured muscles’ tonus inside the vagina. My homework were 30 constrictions every day, plus working with “dilators” – plastic cones comes in 6 sizes, starting from a size of a small finger, to a size of a penis.
At this point I was already in a relationship with my husband, who was understanding, calm and most important – very patient. To be honest, we both never thought it would take so long. Practicing was annoying and painful, and I found myself thinking a lot “is it worth it?”. After a while, I felt that the physical practice is not enough, and I need a “psychological breakthrough”. So I stopped practicing and started seeing a psychologist, for about a half a year. We processed my past experiences, examined the thoughts and beliefs I had about sex, and that way we released some of the tension that was shrinking my body.
The next step was to continue practicing with the dilators, but honestly – I had no motivation. My husband and I had great sex without the actual penetration, and I didn’t want the painful practice again. Fortunately, I participated in a short course given by Professor Erik Peper, about biofeedback therapy. In his lecture he described a young woman, who suffered from vulvodynia, a problem that is a bit similar to vaginismus (Peper et al, 2015; See: https://peperperspective.com/2015/09/25/resolving-pelvic-floor-pain-a-case-report/). She learned how to relax her body and deal with the pain, and finally she had sex – and even enjoyed it! I was inspired.
Erik Peper gave me a very important advice: breathing in. Apparently, we can relax the muscles and open the vagina better while inhaling, instead of exhaling – as I tried before. During exhalation the pelvic floor tightens and goes upward while during inhalation the pelvic floor descends and relaxes especially when sitting up (Peper et al, 2016). He advised me to give myself a few minutes with the dilator, and in every inhale – imagine the area opening and insert the dilator a few millimeters. I started practicing again, but in a sitting position, which I found more comfortable and less painful. I advanced to the biggest dilator within a few weeks, and had a just little pain – sometimes without any pain at all. The most important thing I understood was not to be afraid of the pain. The fear is what made me even more tensed, and tension brings pain. Then, my husband and I started practicing with “the real thing”, very slowly and gently, trying to find the best position and angle for us. Finally, we did it. And it was a great feeling.
The biological factors that affect the relaxation/contraction of the pelvic floor and vaginal opening are:
Feeling safe and hopeful. When threatened, scared, anticipate pain, and worry, our body triggers a defense reaction. In this flexor response, labeled by Thomas Hanna as the Red Light Reflex, the body curls up in defense to protect itself which includes the shoulders to round, the chest to be depressed, the legs pressing together, the pelvic floor to tighten and the head to jut forward (Hanna, 2004). This is the natural response of fear, anxiety, prolonged stress or negative depressive thinking.
Before beginning to work on vaginismus, feel safe. This means accepting what is, accepting that it is not your fault, and that there are no demands for performance. It also means not anticipating that it will be again painful because with each anticipation the pelvic floor tends to tightens. Read the chapter on vaginismus in Dr. Lonnie Barbach’s book, For each other: Sharing sexual intimacy (Barbach, 1983).
Inhale during insertion to relax the pelvic floor and vaginal opening. This instruction is seldom taught because in most instances, we have been taught to exhale while relaxing. Exhaling while relaxing is true for most muscles; however, it is different for the pelvic floor. When inhalation occurs, the pelvic floor descends and relaxes. During exhalation the pelvic floor tightens and ascends to support breathing and push the diaphragm upward to exhale the air. Be sure to allow the abdomen to expand during inhalation without lifting the chest and allow the abdomen to constrict during exhalation as if inhalation fills the balloon in the abdomen and exhalation deflates the balloon (for detailed instructions see Peper et al, 2016). Do not inhale by lifting and expanding your chest which often occurs during gasping and and fear. It tends to tighten and lift the pelvic floor.
Experience the connection between diaphragmatic breathing and pelvic floor movement in the following practice.
While sitting upright make a hissing noise as the air escapes with pressure between your lips. As you are exhaling feel, your abdomen and your anus tightening. During the inhalation let your abdomen expand and feel how your anus descends and pelvic floor relaxes. With practice this will become easier.
Stretch very, very slowly to avoid triggering the stretch reflex. When a muscle is rapidly stretched, it triggers an automatic stretch reflex which causes the muscle to contract. This innate response occurs to avoid damaging the muscle by over stretching. The stretch reflex is also triggered by pain and puts a brake on the stretching. Always use a lubricant when practicing by yourself or with a partner. Practice inserting larger and larger diameter dilaters into the vagina. Start with a very small diameter and progress to a larger diameter. These can be different diameter cones, your finger, or other objects. Remember to inhale and feel the pelvic floor descending as you insert the probe or finger. If you feel discomfort/pain, stop pushing, keep breathing, relax your shoulders, relax your hips, legs, and toes and do not push inward and upward again until the discomfort has faded out.
Feel sexually aroused by allowing enough foreplay. When sexually aroused the tissue is more lubricated and may stretch easier. Continue to use a good lubricant.
Putting it all together.
When you feel safe, practice slow diaphragmatic breathing and be aware of the pelvic floor relaxing and descending during inhalation and contracting and going up during exhalation. When practicing stretching the opening with cones or your finger, go very, very slow. Only apply pressure of insertion during the mid-phase of inhalation, then wait during exhalation and then again insert slight more during the next inhalation. When you experience pain, relax your shoulders, keep breathing for four or five breaths till the pain subsides, then push very little during the next inhalation. Go much slower and with more tenderness.
Be patient. Explain to your partner that your body and mind need time to adjust to new feelings. However, don’t stop having sex – you can have great sex without penetration. Practice both alone and with your partner; together find the best angle and rate. Use different lubricants to check out what is best for you. Any little progress is getting you closer to having an enjoyable sex. I recommend watching this TED video of Emily Nagoski explaining the “dual control model” and practicing as she suggests: https://www.youtube.com/watch?v=HILY0wWBlBM
Finally, practice the exercises developed by Dr. Lonnie Barbach, who as one of the first co-directors of clinical training at the University of California San Francisco, Human Sexuality Program, created the women’s pre-orgasmic group treatment program. They are superbly described in her two books, For each other: Sharing sexual intimacy, and For yourself: The fulfillment of female sexuality, and are a must read for anyone desiring to increase sexual fulfillment and joy (Barbach, 2000; 1983).
References:
Barbach, L. (1983). For each other: Sharing sexual intimacy. New York: Anchor
Barbach, L. (2000). For yourself: The fulfillment of female sexuality. New York: Berkley.
BarLewis, R. W., Fugl‐Meyer, K. S., Bosch, R., Fugl‐Meyer, A. R., Laumann, E. O., Lizza, E., & Martin‐Morales, A. (2004). Epidemiology/risk factors of sexual dysfunction. The journal of sexual medicine, 1(1), 35-39. http://www.jsm.jsexmed.org/article/S1743-6095(15)30062-X/fulltext
Gross. E. & Brubaker, L. (2022). Dyspareunia in Women. JAMA. https://doi.org/10.1001/jama.2022.4853
Hanna, T. (2004). Somatics: Reawakening the mind’s control of movement, flexibility, and health. Boston: Da Capo Press.
Martinez Aranda, P. & Peper, E. (2015). The healing of vulvodynia from a client’s perspective. https://biofeedbackhealth.files.wordpress.com/2011/01/a-healing-of-vulvodynia-from-the-client-perspective-2015-06-15.pdf
Peper, E., Booiman, A., Lin, I-M, Harvey, R., & Mitose, J. (2016). Abdominal SEMG Feedback for Diaphragmatic Breathing: A Methodological Note. Biofeedback. 44(1), 42-49. https://biofeedbackhealth.files.wordpress.com/2011/01/1-abdominal-semg-feedback-published.pdf
Peper, E., Martinez Aranda, P., & Moss, E. (2015). Vulvodynia treated successfully with breathing biofeedback and integrated stress reduction: A case report. Biofeedback. 43(2), 103-109. https://biofeedbackhealth.files.wordpress.com/2011/01/a-vulvodynia-treated-with-biofeedback-published.pdf
Ter Kuile, M. M., Both, S., & van Lankveld, J. J. (2010). Cognitive behavioral therapy for sexual dysfunctions in women. Psychiatric Clinics of North America, 33(3), 595-610. https://www.researchgate.net/publication/45090259_Cognitive_Behavioral_Therapy_for_Sexual_Dysfunctions_in_Women
Van Lankveld, J. J., Granot, M., Weijmar Schultz, W., Binik, Y. M., Wesselmann, U., Pukall, C. F., . Achtrari, C. (2010). Women’s sexual pain disorders. The Journal of Sexual Medicine, 7(1pt2), 615-631. http://www.jsm.jsexmed.org/article/S1743-6095(15)32867-8/fulltext
*We thank Dr. Lonnie Barbach for her helpful feedback and support. Written collaboratively with Tal Cohen, biofeedback therapist (Israel) and Erik Peper.
Education versus treatment for self-healing: Eliminating a headache[1]
Posted: November 18, 2016 Filed under: Pain/discomfort, self-healing, stress management, Uncategorized | Tags: autogenic training, biofeedback, education, electromyography, headache, Holistic health, migraine, posture, treatment 3 Comments“I have had headaches for six years, at first occurring almost every day. When I got put on an antidepressant, they slowed to about 3 times a week (sometimes more) and continued this way until I learned relaxation techniques. I am 20 years old and now headache free. Everyone should have this educational opportunity to heal themselves.” -Melinda, a 20 year old student
Health and wellness is a basic right for all people. When students learn stress management skills which include awareness of stress, progressive muscle relaxation, Autogenic phrases, slower breathing, posture change, transforming internal language, self-healing imagery, the role of diet, exercise embedded within an evolutionary perspective as part of a college class their health often improves. When students systematically applied these self-awareness techniques to address a self-selected illness or health behavior (e.g., eczema, diet, exercise, insomnia, or migraine headaches), 80% reported significant improvement in their health during that semester (Peper et al., 2014b; Tseng, et al., 2016). The semester long program is based upon the practices described in the book, Make Health Happen, (Peper, Gibney, & Holt, 2002).
The benefits often last beyond the semester. Numerous students reported remarkable outcomes at follow-up many months after the class had ended because they had mastered the self-regulation skills and continued to implement these skills into their daily lives. The educational model utilized in holistic health courses is often different from the clinical/treatment model.
Educational approach: I am a student and I have an illness (most of me is healthy and only part of me is sick).
Clinical treatment approach: I am a patient and I am sick (all of me is sick)
Some of the concepts underlying the differences between the educational and the clinical approach are shown in Table 1.
| Educational approach | Clinic/treatment approach |
| Focuses on growth and learning | Focuses on remediation |
| Focuses on what is right | Focuses on what is wrong |
| Focuses on what people can do for themselves | Focuses on how the therapist can help patients |
| Assumes students as being competent | Implies patients are damaged and incompetent |
| Students defined as being competent to master the skills | Patients defined as requiring others to help them |
| Encourages active participation in the healing process | Assumes passive participation in the healing process |
| Students keep logs and write integrative and reflective papers, which encourage insight and awareness | Patients usually do not keep logs nor are asked to reflect at the end of treatment to see which factors contributed to success |
| Students meet in small groups, develop social support and perspective | Patients meet only with practitioners and stay isolated |
| Students experience an increased sense of mastery and empowerment | Patients experience no change or possibly a decrease in sense of mastery |
| Students develop skills and become equal or better than the instructor | Patients are healed, but therapist is always seen as more competent than patient |
| Students can become colleagues and friends with their teachers | Patients cannot become friends of the therapist and thus are always distanced |
Table 1. Comparison of an educational versus clinical/treatment approach
The educational approach focuses on mastering skills and empowerment. As part of the course work, students become more mindful of their health behavior patterns and gradually better able to transform their previously covert harm promoting patterns. This educational approach is illustrated in a case report which describes how a student reduced her chronic migraines.
Case Example: Elimination of Chronic Migraines
Melinda, a 20-year-old female student, experienced four to five chronic migraines per week since age 14. A neurologist had prescribed several medications including Imitrex (used to treat migraines) and Topamax (used to prevent seizures as well as migraine headaches), although they were ineffective in treating her migraines. Nortriptyline (a tricyclic antidepressant) and Excedrin Migraine (which contains caffeine, aspirin, and acetaminophen) reduced the frequency of symptoms to three times per week.
She was enrolled in a university biofeedback class that focused on learning self-regulation and biofeedback skills. All these students were taught the fundamentals of biofeedback and practiced Autogenic Training (AT) every day during the semester (Luthe, 1979; Luthe & Schultz, 1969; Peper & Williams, 1980).
In the class, students practiced with surface electromyography (SEMG) feedback to identify the presence of shoulder muscle overexertion (dysponesis), as well as awareness of minimum muscle tension. Additional practices included hand warming, awareness of thoracic and diaphragmatic breathing, and other biofeedback or somatic awareness approaches. In parallel with awareness of physical sensations, students practiced behavioral awareness such as alternating between a slouching body posture (associated with feeling self-critical and powerless) and an upright body posture (associated with feeling powerful and in control). Psychological awareness was focused on transforming negative thoughts and self-judgments to positive empowering thoughts (Harvey and Peper, 2011; Peper et al., 2014a; Peper et al, 2015). Taken together, students systematically increased awareness of physical, behavioral, and psychological aspects of their reactions to stress.
The major determinant for success is to generalize training at school, home and at work. Each time Melinda felt her shoulders tightening, she learned to relax and release the tension in her shoulders, practiced Autogenic Training with the phrase “my neck and shoulders are heavy.” In addition, whenever she felt her body beginning to slouch or noticed a negative self-critical thought arising in her mind, she shifted her body to an upright empowered posture, and substituted positive thoughts to reduce her cortisol level and increase access to positive thoughts (Carney & Cuddy, 2010; Cuddy, 2012; Tsai, et al., 2016). Postural feedback was also informally given by Melinda’s instructor. Every time the instructor noticed her slouching in class or the hallway, he visually changed his own posture to remind her to be erect.
Results
Melinda’s headaches reduced from between three and five per week before enrolling in the class to zero following the course, as shown in Figure 2. She has learned to shift her posture from slouching to upright and relaxed. In addition, she reported feeling empowered, mentally clear, and her acne cleared up. All medications were eliminated. At a two year follow-up, she reported that since she took the class, she had only few headaches which were triggered by excessive stress. 
Figure 2. Frequency of migraine and the implementation of self-practices.
The major factors that contributed to success were:
- Becoming aware of muscle tension through the SEMG feedback. Melinda realized that she had tension when she thought she was relaxed.
- Keeping detailed logs and developing a third person perspective by analyzing her own data and writing a report. A process that encouraged acceptance of self, thereby becoming less judgmental.
- Acquiring a new belief that she could learn to overcome her headaches, facilitated by class lecture and verbal feedback from the instructor.
- Taking active control by becoming aware of the initial negative thoughts or sensations and interrupting the escalating chain of negative thoughts and sensations by shifting the attention to positive empowering thoughts and sensations–a process that integrated mindfulness, acceptance and action. Thus, transforming judgmental thoughts into accepting and positive thoughts.
- Becoming more aware throughout the day, at school and at home, of initial triggers related to body collapse and muscle tension, then changing her body posture and relaxing her shoulders. This awareness was initially developed because the instructor continuously gave feedback whenever she started to slouch in class or when he saw her slouching in the hallways.
- Practicing many, many times during the day. Namely, increasing her ongoing mindfulness of posture, neck, and shoulder tension, and of negative internal dialogue without judgment.
The benefits of this educational approach is captured by Melinda’s summary, “The combined Autogenic biofeedback awareness and skill with the changes in posture helped me remarkably. It improved my self-esteem, empowerment, reduced my stress, and even improved the quality of my skin. It proves the concept that health is a whole system between mind, body, and spirit. When I listen carefully and act on it, my overall well-being is exceptionally improved.”
References:
Carney, D. R., Cuddy, A. J., & Yap, A. J. (2010). Power posing brief nonverbal displays affect neuroendocrine levels and risk tolerance. Psychological Science, 21(10), 1363-1368.
Cuddy, A. (2012). Your body language shapes who you are. Technology, Entertainment, and Design (TED) Talk, available at: http://www.ted.com/talks/amy_cuddy_your_body_language_shapes_who_you_are
Harvey, E. & Peper, E. (2011). I thought I was relaxed: The use of SEMG biofeedback for training awareness and control (pp. 144-159). In W. A. Edmonds, & G. Tenenbaum (Eds.), Case studies in applied psychophysiology: Neurofeedback and biofeedback treatments for advances in human performance. West Sussex, UK: Wiley-Blackwell.
Luthe, W. (1979). About the methods of autogenic therapy (pp. 167-186). In E. Peper, S. Ancoli, & M. Quinn, Mind/body integration. New York: Springer.
Luthe, W., & Schultz, J.H. (1969). Autogenic therapy (Vols. 1-6). New York, NY: Grune and Stratton.
Peper, E., Booiman, A., Lin, I-M., & Shaffer, F. (2014a). Making the unaware aware-Surface electromyography to unmask tension and teach awareness. Biofeedback. 42(1), 16-23.
Peper, E., Gibney, K.H. & Holt. C. (2002). Make health happen: Training yourself to create wellness. Dubuque, IA: Kendall-Hunt. ISBN-13: 978-0787293314
Peper, E., Lin, I-M, Harvey, R., Gilbert, M., Gubbala, P., Ratkovich, A., & Fletcher, F. (2014b). Transforming chained behaviors: Case studies of overcoming smoking, eczema and hair pulling (trichotillomania). Biofeedback, 42(4), 154-160.
Peper, E., Nemoto, S., Lin, I-M., & Harvey, R. (2015). Seeing is believing: Biofeedback a tool to enhance motivation for cognitive therapy. Biofeedback, 43(4), 168-172. doi: 10.5298/1081-5937-43.4.03
Peper, E. & Williams, E.A. (1980). Autogenic therapy (pp. 131-137). In: A. C. Hastings, J. Fadiman, & J. S. Gordon (Eds.). Health for the whole person. Boulder: Westview Press.
Tsai, H. Y., Peper, E., & Lin, I. M. (2016). EEG patterns under positive/negative body postures and emotion recall tasks. NeuroRegulation, 3(1), 23-27.
Tseng, C., Abili, R., Peper, E., & Harvey, R. (2016). Reducing acne-stress and an integrated self-healing approach. Poster presented at the 47th Annual Meeting of the Association for Applied Psychophysiology and Biofeedback, Seattle WA, March 9-12, 2016.
[1] Adapted from: Peper, E., Miceli, B., & Harvey, R. (2016). Educational Model for Self-healing: Eliminating a Chronic Migraine with Electromyography, Autogenic Training, Posture, and Mindfulness. Biofeedback, 44(3), 130–137. https://biofeedbackhealth.files.wordpress.com/2011/01/a-educational-model-for-self-healing-biofeedback.pdf
Resolving pelvic floor pain-A case report
Posted: September 25, 2015 Filed under: Breathing/respiration, Pain/discomfort, self-healing, stress management, Uncategorized | Tags: biofeedback, Breathing, electromyography, pain, posture, self-regulation, vulvodynia 10 CommentsAdapted from: Martinez Aranda, P. & Peper, E. (2015). The healing of vulvodynia from a client’s perspective. https://biofeedbackhealth.files.wordpress.com/2011/01/a-healing-of-vulvodynia-from-the-client-perspective-2015-06-15.pdf
It’s been a little over a year since I began practicing biofeedback and visualization strategies to overcome vulvodynia. Today, I feel whole, healed, and hopeful. I learned that through controlled and conscious breathing, I could unleash the potential to heal myself from chronic pain. Overcoming pain did not happen overnight; but rather, it was a process where I had to create and maintain healthy lifestyle habits and meditation. Not only am I thankful for having learned strategies to overcome chronic pain, but for acquiring skills that will improve my health for the rest of my life. –-24 year old woman who successfully resolved vulvodynia
Pelvic floor pain can be debilitating, and it is surprisingly common, affecting 10 to 25% of American women. Pelvic floor pain has numerous causes and names. It can be labeled as vulvar vestibulitis, an inflammation of vulvar tissue, interstitial cystitis (chronic pain or tenderness in the bladder), or even lingering or episodic hip, back, or abdominal pain. Chronic pain concentrated at the entrance to the vagina (vulva), is known as vulvodynia. It is commonly under-diagnosed, often inadequately treated, and can go on for months and years (Reed et al., 2007; Mayo Clinic, 2014). The discomfort can be so severe that sitting is uncomfortable and intercourse is impossible because of the extreme pain. The pain can be overwhelming and destructive of the patient’s life. As the participant reported,
I visited a vulvar specialist and he gave me drugs, which did not ease the discomfort. He mentioned surgical removal of the affected tissue as the most effective cure (vestibulectomy). I cried immediately upon leaving the physician’s office. Even though he is an expert on the subject, I felt like I had no psychological support. I was on Gabapentin to reduce pain, and it made me very depressed. I thought to myself: Is my life, as I know it, over?
Physically, I was in pain every single day. Sometimes it was a raging burning sensation, while other times it was more of an uncomfortable sensation. I could not wear my skinny jeans anymore or ride a bike. I became very depressed. I cried most days because I felt old and hopeless instead of feeling like a vibrant 23-year-old woman. The physical pain, combined with my negative feelings, affected my relationship with my boyfriend. We were unable to have sex at all, and because of my depressed status, we could not engage in any kind of fun. (For more details, read the published case report,Vulvodynia treated successfully with breathing biofeedback and integrated stress reduction: A case report).
The four-session holistic biofeedback interventions to successfully resolved vulvodynia included teaching diaphragmatic breathing to transform shallow thoracic breathing into slower diaphragmatic breathing, transforming feelings of powerlessness and hopelessness to empowerment and transforming her beliefs that she could reduce her symptoms and optimize her health. The interventions also incorporated self-healing imagery and posture-changing exercises. The posture changes consisted of developing awareness of the onset of moving into a collapsed posture and use this awareness to shift to an erect/empowered postures (Carney, Cuddy, & Yap, 2010; Peper, 2014; Peper, Booiman, Lin, & Harvey, in press). Finally, this case report build upon the seminal of electromyographic feedback protocol developed by Dr. Howard Glazer (Glazer & Hacad, 2015) and the integrated relaxation protocol developed Dr. David Wise (Wise & Anderson, 2007).
Through initial biofeedback monitoring of the lower abdominal muscle activity, chest, and abdomen breathing patterns, the participant observed that when she felt discomfort or was fearful, her lower abdomen muscles tended to tighten. After learning how to sense this tightness, she was able to remind herself to breathe lower and slower, relax the abdominal wall during inhalation and sit or stand in an erect power posture.
The self-mastery approach for healing is based upon a functional as compared to a structural perspective. The structural perspective implies that the problem can only be fixed by changing the physical structure such as with surgery or medications. The functional perspective assumes that if you can learn to change your dysfunctional psychophysiological patterns the disorder may disappear.
The functional approach assumed that an irritation of the vestibular area might have caused the participant to tighten her lower abdomen and pelvic floor muscles reflexively in a covert defense reaction. In addition, ongoing worry and catastrophic thinking (“I must have surgery, it will never go away, I can never have sex again, my boyfriend will leave me”) also triggered the defense reaction—further tightening of her lower abdomen and pelvic area, shallow breathing, and concurrent increases in sympathetic nervous activation—which together activated the trigger points that lead to increased chronic pain (Banks et al, 1998).
When the participant experienced a sensation or thought/worried about the pain, her body responded in a defense reaction by breathing in her chest and tightening the lower abdominal area as monitored with biofeedback. Anticipation of being monitored increased her shoulder tension, recalling the stressful memory increased lower abdominal muscle tension (pulling in the abdomen for protection), and the breathing became shallow and rapid as shown in Figure 1.
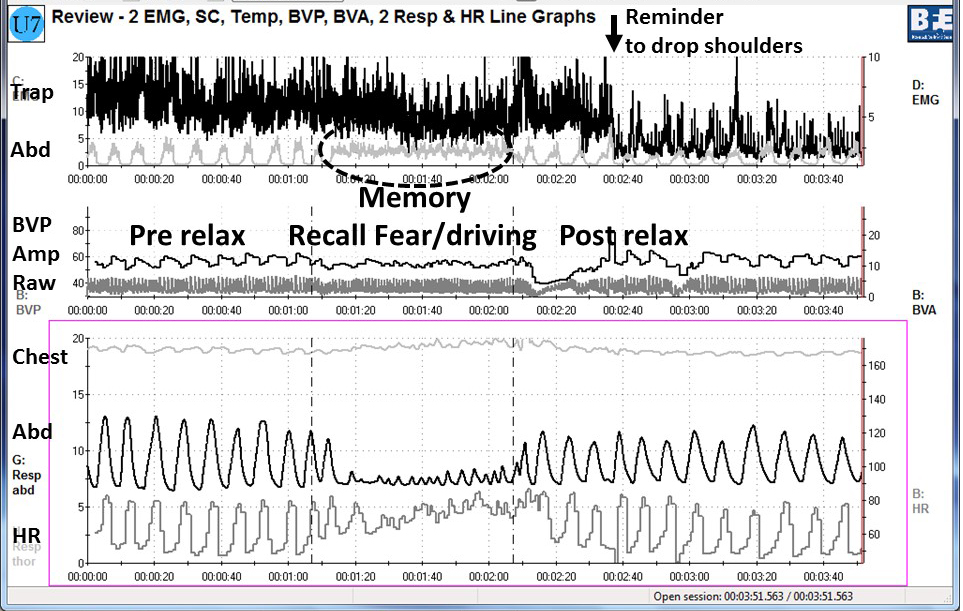
Figure 1. Physiological recording of pre-stressor relaxation, the recall of a fearful driving experience, and a post-stressor relaxation. The scalene to trapezius SEMG increased in anticipation while she recalled the experience, and then initially did not relax (from Peper, Martinez Aranda, & Moss, 2015).
This defense pattern became a conditioned response—initiating intercourse or being touched in the affected area caused the participant to tense and freeze up. She was unaware of these automatic protective patterns, which only worsened her chronic pain.
During the four sessions of training, the participant learned to reverse and interrupt the habitual defense reaction. For example, as she became aware of her breathing patterns she reported,
It was amazing to see on the computer screen the difference between my regular breathing pattern and my diaphragmatic breathing pattern. I could not believe I had been breathing that horribly my whole life, or at least, for who knows how long. My first instinct was to feel sorry for myself. Then, rather than practicing negative patterns and thoughts, I felt happy because I was learning how to breathe properly. My pain decreased from an 8 to alternating between a 0 and 3.
The mastery of slower and lower abdominal breathing within a holistic perspective resulted in the successful resolution of her vulvodynia. An essential component of the training included allowing the participant to feel safe, and creating hope by enabling her to experience a decrease in discomfort while doing a specific practice, and assisting her to master skills to promote self-healing. Instead of feeling powerless and believing that the only resolution was the removal of the affected area (vestibulectomy). The integrated biofeedback protocol offered skill mastery training, to promote self-healing through diaphragmatic breathing, somatic postural changes, reframing internal language, and healing imagery as part of a common sense holistic health approach.
For more details about the case report, download the published study, Peper, E., Martinez Aranda, P., & Moss, E. (2015). Vulvodynia treated successfully with breathing biofeedback and integrated stress reduction: A case report. Biofeedback. 43(2), 103-109.
The participant also wrote up her subjective experience of the integrated biofeedback process in the paper, Martinez Aranda & Peper (2015). Healing of vulvodynia from the client perspective. In this paper she articulated her understanding and experiences in resolving vulvodynia which sheds light on the internal processes that are so often skipped over in published reports.
At the five year follow-up on May 29, 2019, she wrote:
“I am doing very well, and I am very healthy. The vulvodynia symptoms have never come back. It migrated to my stomach a couple of years after, and I still have a sensitive stomach. My stomach has gotten much, much better, though. I don’t really have random pain anymore, now I just have to be watchful and careful of my diet and my exercise, which are all great things!”
References
Banks, S. L., Jacobs, D. W., Gevirtz, R., & Hubbard, D. R. (1998). Effects of autogenic relaxation training on electromyographic activity in active myofascial trigger points. Journal of Musculoskeletal Pain, 6(4), 23-32. https://www.researchgate.net/profile/David_Hubbard/publication/232035243_Effects_of_Autogenic_Relaxation_Training_on_Electromyographic_Activity_in_Active_Myofascial_Trigger_Points/links/5434864a0cf2dc341daf4377.pdf
Carney, D. R., Cuddy, A. J., & Yap, A. J. (2010). Power posing brief nonverbal displays affect neuroendocrine levels and risk tolerance. Psychological Science, 21(10), 1363-1368. Available from: https://www0.gsb.columbia.edu/mygsb/faculty/research/pubfiles/4679/power.poses_.PS_.2010.pdf
Glazer, H. & Hacad, C.R. (2015). The Glazer Protocol: Evidence-Based Medicine Pelvic Floor Muscle (PFM) Surface Electromyography (SEMG). Biofeedback, 40(2), 75-79. http://www.aapb-biofeedback.com/doi/abs/10.5298/1081-5937-40.2.4
Martinez Aranda, P. & Peper, E. (2015). Healing of vulvodynia from the client perspective. Available from: https://biofeedbackhealth.files.wordpress.com/2011/01/a-healing-of-vulvodynia-from-the-client-perspective-2015-06-15.pdf
Mayo Clinic (2014). Diseases and conditions: Vulvodynia. Available at http://www.mayoclinic.org/diseases-conditions/vulvodynia/basics/definition/con-20020326
Peper, E. (2014). Increasing strength and mood by changing posture and sitting habits. Western Edition, pp.10, 12. Available from: http://thewesternedition.com/admin/files/magazines/WE-July-2014.pdf
Peper, E., Booiman, A., Lin, I, M.,& Harvey, R. (in press). Increase strength and mood with posture. Biofeedback.
Peper, E., Martinez Aranda, P., & Moss, E. (2015). Vulvodynia treated successfully with breathing biofeedback and integrated stress reduction: A case report. Biofeedback. 43(2), 103-109. Available from: https://biofeedbackhealth.files.wordpress.com/2011/01/a-vulvodynia-treated-with-biofeedback-published.pdf
Reed, B. D., Haefner, H. K., Sen, A., & Gorenflo, D. W. (2008). Vulvodynia incidence and remission rates among adult women: a 2-year follow-up study. Obstetrics & Gynecology, 112(2, Part 1), 231-237. http://journals.lww.com/greenjournal/Abstract/2008/08000/Vulvodynia_Incidence_and_Remission_Rates_Among.6.aspx
Wise, D., & Anderson, R. U. (2006). A headache in the pelvis: A new understanding and treatment for prostatitis and chronic pelvic pain syndromes. Occidental, CA: National Center for Pelvic Pain Research.http://www.pelvicpainhelp.com/books/
Reduce hot flashes and premenstrual symptoms with breathing
Posted: February 18, 2015 Filed under: Breathing/respiration, Pain/discomfort, self-healing, stress management, Uncategorized | Tags: biofeedback, Breathing, diaphragmatic breathing, heart rate variability, hormone replacement therapy, hot flashes, HRT, Menopause, respiration, sighs, stress, sympathetic activity 6 CommentsAfter the first week to my astonishment, I have fewer hot flashes and they bother me less. Each time I feel the warmth coming, I breathe out slowly and gently. To my surprise they are less intense and are much less frequent. I keep breathing slowly throughout the day. This is quite a surprise because I was referred for biofeedback training because of headaches that occurred after getting a large electrical shock. After 5 sessions my headaches have decreased and I can control them, and my hot flashes have decreased from 3-4 per day to 1-2 per week. -50 year old client
After students in my Holistic Health class at San Francisco State University practiced slower diaphragmatic breathing and begun to change their dysfunctional shallow breathing, gasping, sighing, and breath holding to diaphragmatic breathing. A number of the older female students students reported that their hot flashes decreased. Some of the younger female students reported that their menstrual cramps and discomfort were reduced by 80 to 90% when they laid down and breathed slower and lower into their abdomen.
 The recent study in JAMA reported that many women continue to experience menopausal triggered hot flashes for up to 14 years. Although the article described the frequency and possible factors that were associated with the prolonged hot flashes, it did not offer helpful solutions.
The recent study in JAMA reported that many women continue to experience menopausal triggered hot flashes for up to 14 years. Although the article described the frequency and possible factors that were associated with the prolonged hot flashes, it did not offer helpful solutions.
Another understanding of the dynamics of hot flashes is that the decrease in estrogen accentuates the sympathetic/ parasympathetic imbalances that probably already existed. Then any increase in sympathetic activation can trigger a hot flash. In many cases the triggers are events and thoughts that trigger a stress response, emotional responses such as anger, anxiety, or worry, increase caffeine intake and especially shallow chest breathing punctuated with sighs. Approximately 80% of American women tend to breathe thoracically often punctuated with sighs and these women are more likely to experience hot flashes. On the other hand, the 20% of women who habitually breathe diaphragmatically tend to have fewer and less intense hot flashes and often go through menopause without any discomfort. In the superb study Drs. Freedman and Woodward (1992), taught women who experience hot flashes to breathe slowly and diaphragmatically which increased their heart rate variability as an indicator of sympathetic/parasympathetic balance and most importantly it reduced the the frequency and intensity of hot flashes by 50%.
Test the breathing connection if you experience hot flashes
Take a breath into your chest and rapidly exhale with a sigh. Repeat this quickly five times. In most cases, one minute later you will experience the beginning sensations of a hot flash. Similarly, when you practice slow diaphragmatic breathing throughout the day and interrupt every gasp, breath holding moment, sigh or shallow chest breathing with slower diaphragmatic breathing, you will experience a significant reduction in hot flashes.
Although this breathing approach has been well documented, many people are unaware of this simple behavioral approach unlike the common recommendation for the hormone replacement therapies (HRT) to ameliorate menopausal symptoms. This is not surprising since pharmaceutical companies spent nearly five billion dollars per year in direct to consumer advertising for drugs and very little money is spent on advertising behavioral treatments. There is no profit for pharmaceutical companies teaching effortless diaphragmatic breathing unlike prescribing HRTs. In addition, teaching and practicing diaphragmatic breathing takes skill training and practice time–time which is not reimbursable by third party payers.
For more information, research data and breathing skills to reduce hot flash intensity, see our article which is reprinted below.
Gibney, H.K. & Peper, E. (2003). Taking control: Strategies to reduce hot flashes and premenstrual mood swings. Biofeedback, 31(3), 20-24.
Taking control: Strategies to reduce hot flashes and premenstrual mood swings*
Erik Peper, Ph.D**., and Katherine H. Gibney
San Francisco State University
After the first week to my astonishment, I have fewer hot flashes and they bother me less. Each time I feel the warmth coming, I breathe out slowly and gently. To my surprise they are less intense and are much less frequent. I keep breathing slowly throughout the day. This is quite a surprise because I was referred for biofeedback training because of headaches that occurred after getting a large electrical shock. After 5 sessions my headaches have decreased and I can control them, and my hot flashes have decreased from 3-4 per day to 1-2 per week. -50 year old client
For the first time in years, I experienced control over my premenstrual mood swings. Each time I could feel myself reacting, I relaxed, did my autogenic training and breathing. I exhaled. It brought me back to center and calmness. -26 year old student
Abstract
Women have been troubled by hot flashes and premenstrual syndrome for ages. Hormone replacement therapy, historically the most common treatment for hot flashes, and other pharmacological approaches for pre-menstrual syndrome (PMS) appear now to be harmful and may not produce significant benefits. This paper reports on a model treatment approach based upon the early research of Freedman & Woodward to reduce hot flashes and PMS using biofeedback training of diaphragmatic breathing, relaxation, and respiratory sinus arrhythmia. Successful symptom reduction is contingent upon lowering sympathetic arousal utilizing slow breathing in response to stressors and somatic changes. We strongly recommend that effortless diaphragmatic breathing be taught as the first step to reduce hot flashes and PMS symptoms.
A long and uncomfortable history
Women have been troubled by hot flashes and premenstrual syndrome for ages. Hot flashes often result in red faces, sweating bodies, and noticeable and embarrassing discomfort. They come in the middle of meetings, in the middle of the night, and in the middle of romantic interludes. Premenstrual syndrome also arrives without notice, bringing such symptoms as severe mood swings, anger, crying, and depression.
Hormone replacement therapy (HRT) was the most common treatment for hot flashes for decades. However, recent randomized controlled trials show that the benefits of HRT are less than previously thought and the risks—especially of invasive breast cancer, coronary artery disease, dementia, stroke and venous thromboembolism—are greater (Humphries & Gill, 2003; Shumaker, et al, 2003; Wassertheil-Smoller, et al, 2003). In addition, there is no evidence of increased quality of life improvements (general health, vitality, mental health, depressive symptoms, or sexual satisfaction) as claimed for HRT (Hays et al, 2003).
“As a result of recent studies, we know that hormone therapy should not be used to prevent heart disease. These studies also report an increased risk of heart attack, stroke, breast cancer, blood clots, and dementia…” -Wyeth Pharmaceuticals (2003)
Because of the increased long-term risk and lack of benefit, many physicians are weaning women off HRT at a time when the largest population of maturing women in history (‘baby boomers’) is entering menopausal years. The desire to find a reliable remedy for hot flashes is on the front burner of many researchers’ minds, not to mention the minds of women suffering from these ‘uncontrollable’ power surges. Yet, many women are becoming increasingly leery of the view that menopause is an illness. There is a rising demand to find a natural remedy for this natural stage in women’s health and development.
For younger women a similar dilemma occurs when they seek treatment of discomfort associated with their menstrual cycle. Is premenstrual syndrome (PMS) just a natural variation in energy and mood levels? Or, are women expected to adapt to a masculine based environment that requires them to override the natural tendency to perform in rhythm with their own psychophysiological states? Instead of perceiving menstruation as a natural occurrence in which one has different moods and/or energy levels, women in our society are required to perform at the status quo, which may contribute to PMS. The feelings and mood changes are quickly labeled as pathology that can only be treated with medication.
Traditionally, premenstrual syndrome is treated with pharmaceuticals, such as birth control pills or Danazol. Although medications may alleviate some symptoms, many women experience unpleasant side effects, such as bloating or acne, and still experience a variety of PMS symptoms. Many cannot tolerate the medications. Thus, millions of women (and families) suffer monthly bouts of ‘uncontrollable’ PMS symptoms
For both hot flashes and PMS the biomedical model tends to frame the symptoms as a “structural biological problem.” Namely, the pathology occurs because the body is either lacking in, or has an excess of, some hormone. All that needs to be done is either augment or suppress hormones/symptoms with some form of drug. Recently, for example, medicine has turned to antidepressant medications to address menopausal hot flashes (Stearns, Beebe, Iyengar, & Dube, 2003).
The biomedical model, however, is only one perspective. The opposite perspective is that the dysfunction occurs because of how we use ourselves. Use in this sense means our thoughts, emotions and body patterns. As we use ourselves, we change our physiology and, thereby, may affect and slowly change the predisposing and maintaining factors that contribute to our dysfunction. By changing our use, we may reduce the constraints that limit the expression of the self-healing potential that is intrinsic in each person.
The intrinsic power of self-healing is easily observed when we cut our finger. Without the individual having to do anything, the small cut bleeds, clotting begin and tissue healing is activated. Obviously, we can interfere with the healing process, such as when we scrape the scab, rub dirt in the wound, reduce blood flow to the tissue or feel anxious or afraid. Conversely, cleaning the wound, increasing blood flow to the area, and feeling “safe” and relaxed can promote healing. Healing is a dynamic process in which both structure and use continuously affect each other. It is highly likely that menopausal hot flashes and PMS mood swings are equally an interaction of the biological structure (hormone levels) and the use factor (sympathetic/parasympathetic activation).
Uncontrollable or overly aroused?
Are the hot flashes and PMS mood swings really ‘uncontrollable?’ From a physiological perspective, hot flashes are increased by sympathetic arousal. When the sympathetic system is activated, whether by medication or by emotions, hot flashes increase and similarly, when sympathetic activity decreases hot flashes decrease. Equally, PMS, with its strong mood swings, is aggravated by sympathetic arousal. There are many self-management approaches that can be mastered to change and reduce sympathetic arousal, such as breathing, meditation, behavioral cognitive therapy, and relaxation.
Breathing patterns are closely associated with hot flashes. During sleep, a sigh generally occurs one minute before a hot flash as reported by Freedman and Woodward (1992). Women who habitually breathe thoracically (in the chest) report much more discomfort and hot flashes than women who habitually breathe diaphragmatically. Freedman, Woodward, Brown, Javaid, and Pandey (1995) and Freedman and Woodward (1992) found that hot flash rates during menopause decreased in women who practiced slower breathing for two weeks. In their studies, the control groups received alpha electroencephalographic feedback and did not benefit from a reduction of hot flashes. Those who received training in paced breathing reduced the frequency of their hot flashes by 50% when they practiced slower breathing. This data suggest that the slower breathing has a significant effect on the sympathetic and parasympathetic balance.
Women with PMS appear similarly able to reduce their discomfort. An early study utilizing Autogenic Training (AT) combined with an emphasis on warming the lower abdomen resulted in women noting improvement in dysfunctional bleeding (Luthe & Schultz, 1969, pp. 144-148). Using a similar approach, Mathew, Claghorn, Largen, and Dobbins (1979) and Dewit (1981) found that biofeedback temperature training was helpful in reducing PMS symptoms.. A later study by Goodale, Domar, and Benson (1990) found that women with severe PMS symptoms who practiced the relaxation response reported a 58% improvement in overall symptomatology as compared to a 27.2% improvement for the reading control group and a 17.0% improvement for the charting group.
Teaching control and achieving results
Teaching women to breathe effortlessly can lead to positive results and an enhanced sense of control. By effortless breathing, the authors refer to their approach to breath training, which involves a slow, comfortable respiration, larger volume of air exchange, and a reliance upon action of the muscles of the diaphragm rather than the chest (Peper, 1990). For more instructions see the recent blog, A breath of fresh air: Improve health with breathing.
Slowing breathing helps to limit the sighs common to rapid thoracic breathing—sighs that often precede menopausal hot flashes. Effortless breathing is associated with stress reduction—stress and mood swings are common concerns of women suffering from PMS. In a pilot study Bier, Kazarian, Peper, and Gibney (2003) at San Francisco State University (SFSU) observed that when the subject practiced diaphragmatic breathing throughout the month, combined with Autogenic Training, her premenstrual psychological symptoms (anger, depressed mood, crying) and premenstrual responses to stressors were significantly reduced as shown in Figure 1.
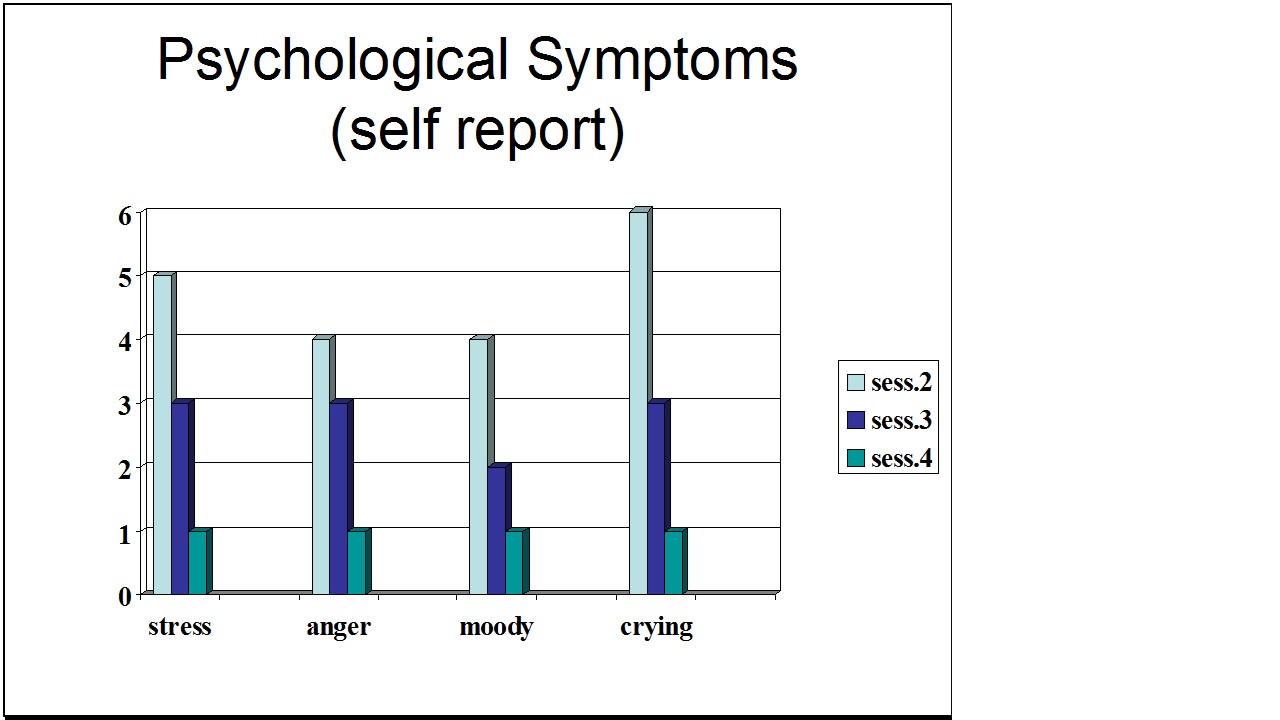
Figure 1. Student’s Individual Subjective Rating in Response to PMS Symptoms.
In another pilot study at SFSU, Frobish, Peper, and Gibney (2003) trained a volunteer who suffered from frequent hot flashes to breathe diaphragmatically. The training goals included modifying breathing patterns, producing a Respiratory Sinus Arrhythmia (RSA), and peripheral hand warming. RSA refers to a pattern of slow, regular breathing during which variations in heart rate enter into a synchrony with the respiration. Each inspiration is accompanied by an increase in heart rate, and each expiration is accompanied by a decrease in heart rate (with some phase differences depending on the rate of breathing). The presence of the RSA pattern is an indication of optimal balance between sympathetic and parasympathetic nervous activity.
During the 11-day study period, the subject charted the occurrence of hot flashes and noted a significant decrease by day 5. However, on the evening of day 7 she sprained her ankle and experienced a dramatic increase in hot flashes on day 8. Once the subject recognized her stress response, she focused more on breathing and was able to reduce the flashes as shown in Figure 2. 
Figure 2. Subjective rating of intensity, frequency and bothersomeness of hot flashes. The increase in hot flashes coincided with increased frustration about an ankle injury.
Our clinical experience confirms the SFSU pilot studies and the previously referenced research by Freedman and Woodward (1992) and Freedman et al. (1995). When arousal is lowered and breathing is effortless, women are better able to cope with stress and report a reduction in symptoms. Habitual rapid thoracic breathing tends to increase arousal while slower breathing, especially slower exhalation, tends to relax and reduce arousal. Learning and then applying effortless breathing reduces excessive sympathetic arousal. It also interrupts the cycle of cognitive activation, anxiety, and somatic arousal. The anticipation and frustration at having hot flashes becomes the cue to shift attention and “breathe slower and lower.” This process stops the cognitively mediated self-activation.
Successful self-regulation and the return to health begin with cognitive reframing: We are not only a genetic biological fixed (deficient) structure but also a dynamic changing system in which all parts (thoughts, emotions, behavior, diet, stress, and physiology) affect and are effected by each other. Within this dynamic changing system, there is an opportunity to implement and practice behaviors and life patterns that promote health.
Learning Diaphragmatic Breathing with and without Biofeedback
Although there are many strategies to modify respiration, biofeedback monitoring combined with respiration training is very useful as it provides real-time feedback. Chest and abdominal movement are recorded with strain gauges and heart rate can be monitored either by an electrocardiogram (EKG) or by a photoplethysmograph sensor on a finger or thumb. Peripheral temperature and electrodermal activity (EDA) biofeedback are also helpful in training. The training focuses on teaching effortless diaphragmatic breathing and encouraging the participant to practice many times during the day, especially when becoming aware of the first sensations of discomfort.
Learning and integrating effortless diaphragmatic breathing into daily life is one of the biofeedback strategies that has been successfully used as a primary or adjunctive/complementary tool for the reversal of disorders such as hypertension, migraine headaches, repetitive strain injury, pain, asthma and anxiety (Schwartz & Andrasik, 2003), as well as hot flashes and PMS.
The biofeedback monitoring provides the trainer with a valuable tool to:
- Observe & identify: Dysfunctional rapid thoracic breathing patterns, especially in response to stressors, are clearly displayed in real-time feedback.
- Demonstrate & train: The physiological feedback display helps the person see that she is breathing rapidly and shallowly in her chest with episodic sighs. Coaching with feedback helps her to change her breathing pattern to one that promotes a more balanced homeostasis.
- Motivate, persuade and change beliefs: The person observes her breathing patterns change concurrently with a felt shift in physiology, such as a decrease in irritability, or an increase in peripheral temperature, or a reduction in the incidence of hot flushes. Thus, she has a confirmation of the importance of breathing diaphragmatically.
In addition, we suggest exercises that integrate verbal and kinesthetic instructions, such as the following: “Exhale gently,” and “Breathe down your leg with a partner.”
Exhale Gently:
Imagine that you are holding a baby. Now with your shoulders relaxed, inhale gently so that your abdomen widens. Then as you exhale, purse your lips and very gently and softly blow over the baby’s hair. Allow your abdomen to narrow when exhaling. Blow so softly that the baby’s hair barely moves. At the same time, imagine that you can allow your breath to flow down and through your legs. Continue imagining that you are gently blowing on the baby’s hair while feeling your breath flowing down your legs. Keep blowing very softly and continuously.
Practice exhaling like this the moment that you feel any sensation associated with hot flashes or PMS symptoms. Smile sweetly as you exhale.
Breathe Down Your Legs with a Partner
Sit or lie comfortably with your feet a shoulder width apart. As you exhale softly whisper the sound “Haaaaa….” Or, very gently press your tongue to your pallet and exhale while making a very soft hissing sound.
Have your partner touch the side of your thighs. As you exhale have your partner stroke down your thighs to your feet and beyond, stroking in rhythm with your exhalation. Do not rush. Apply gentle pressure with the stroking. Do this for four or five breaths.
Now, continue breathing as you imagine your breath flowing through your legs and out your feet.
During the day remember the feeling of your breath flowing downward through your legs and out your feet as you exhale.
Learning Strategies in Biofeedback Assisted Breath Training
Common learning strategies that are associated with the more successful amelioration of hot flashes and PMS include:
- Master effortless diaphragmatic breathing, and concurrently increase respiratory sinus arrhythmia (RSA). Instead of breathing rapidly, such as at 18 breaths per minute, the person learns to breathe effortlessly and slowly (about 6 to 8 breaths per minute). This slower breathing and increased RSA is an indication of sympathetic-parasympathetic balance as shown in Figure 3.
- Practice slow effortless diaphragmatic breathing many times during the day and, especially in response to stressors.
- Use the physical or emotional sensations of a hot flash or mood alteration as the cue to exhale, let go of anxiety, breathe diaphragmatically and relax.
- Reframe thoughts by accepting the physiological processes of menstruation or menopause, and refocus the mind on positive thoughts, and breathing rhythmically.
- Change one’s lifestyle and allow personal schedules to flow in better balance with individual, dynamic energy levels.
 Figure 3. Physiological Recordings of a Participant with PMS. This subject learned effortless diaphragmatic breathing by the fifth session and experienced a significant decrease in symptoms.
Figure 3. Physiological Recordings of a Participant with PMS. This subject learned effortless diaphragmatic breathing by the fifth session and experienced a significant decrease in symptoms.
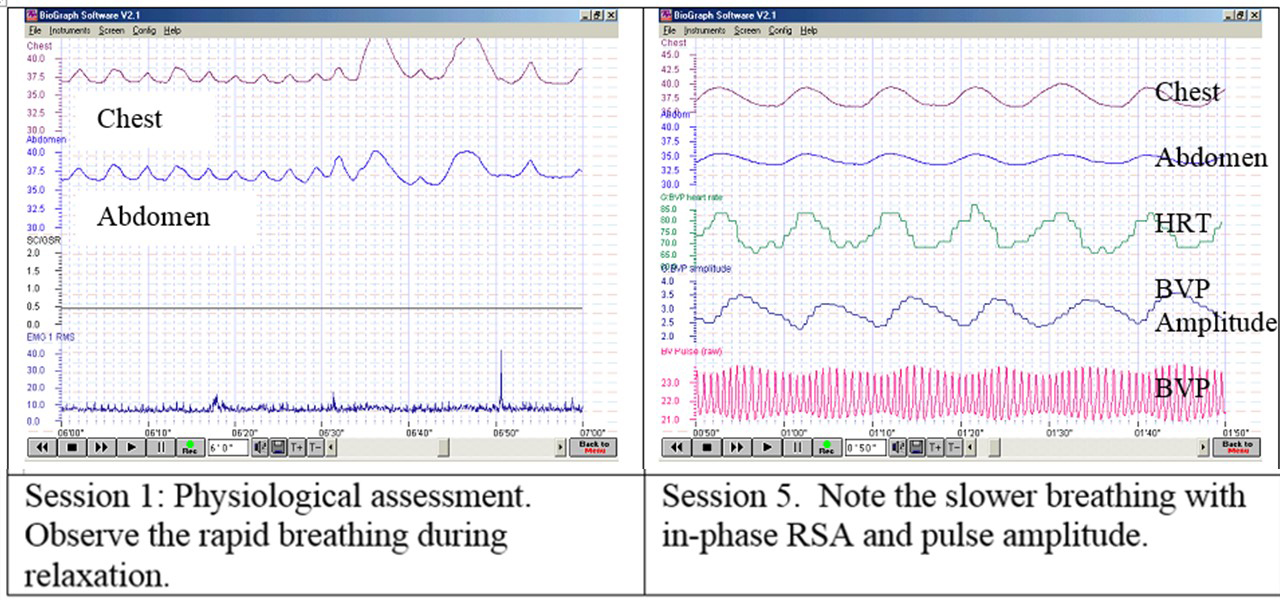
Generalizing skills and interrupting the pattern
The limits of self-regulation are unknown, often held back only by the practitioner’s and participant’s beliefs. Biofeedback is a powerful self-regulation tool for individuals to observe and modify their covert physiological reactions. Other skills that augment diaphragmatic breathing are Quieting Reflex (Stroebel, 1982), Autogenic Training (Schultz & Luthe, 1969), and mindfulness training (Kabat-Zinn, 1990). In all skill learning, generalization is a fundamental factor underlying successful training. Integrating the learned psychophysiological skills into daily life can significantly improve health—especially in anticipation of and response to stress. The anticipated stress can be a physical, cognitive or social trigger, or merely the felt onset of a symptom.
As the person learns and applies effortless breathing to daily activities, she becomes more aware of factors that affect her breathing. She also experiences an increased sense of control: She can now take action (a slow effortless breath) in moments when she previously felt powerless. The biofeedback-mastered skill interrupts the evoked frustrations and irritations associated with an embarrassing history of hot flashes or mood swings. Instead of continuing with the automatic self-talk, such as “Damn, I am getting hot, why doesn’t it just stop?” (language fueling sympathetic arousal), she can take a relaxing breath in response to the internal sensations, stop the escalating negative self-talk and allows more acceptance—a process reducing sympathetic arousal.
In summary, effortless breathing appears to be a non-invasive behavioral strategy to reduce hot flashes and PMS symptoms. Practicing effortless diaphragmatic breathing contributes to a sense of control, supports a healthier homeostasis, reduces symptoms, and avoids the negative drug side effects. We strongly recommend that effortless diaphragmatic breathing be taught as the first step to reduce hot flashes and PMS symptoms.
I feel so much cooler. I can’t believe that my hand temperature went up. I actually feel calmer and can’t even feel the threat of a hot flash. Maybe this breathing does work! –Menopausal patient after initial training in diaphragmatic breathing
References
Bier, M., Kazarian, D., Peper, E., & Gibney, K. (2003). Reducing the severity of PMS symptoms with diaphragmatic breathing, autogenic training and biofeedback. Unpublished report.
Freedman, R.R., & Woodward, S. (1992). Behavioral treatment of menopausal hot flushes: Evaluation by ambulatory monitoring. American Journal of Obstetrics and Gynecology, 167 (2), 436-439.
Freedman, R.R., Woodward, S., Brown, B., Javaid, J.I., & Pandey, G.N. (1995). Biochemical and thermoregulatory effects of behavioral treatment for menopausal hot flashes. Menopause: The Journal of the North American Menopause Society, 2 (4), 211-218.
Frobish,C., Peper, E. & Gibney, K. H. (2003). Menopausal Hot Flashes: A Self-Regulation Case Study. Poster presentation at the 35th Annual Meeting of the Association for Applied Psychophysiology and Biofeedback. Abstract in: Applied Psychophysiology and Biofeedback. 29 (4), 302.
Goodale, I.L., Domar, A.D., & Benson, H. (1990). Alleviation of Premenstrual Syndrome symptoms with the relaxation response. Obstetrics and Gynecological Journal, 75 (5), 649-55.
Hays, J., Ockene, J.K., Brunner, R.L., Kotchen, J.M., Manson, J.E., Patterson, R.E., Aragaki, A.K., Shumaker, S.A., Brzyski, R.G., LaCroix, A.Z., Granek, I.A, & Valanis, B.G., Women’s Health Initiative Investigators. (2003). Effects of estrogen plus progestin on health-related quality of life. New England Journal of Medicine, 348, 1839-1854.
Humphries, K.H.., & Gill, s. (2003). Risks and benefits of hormone replacement therapy: the evidence speaks. Canadian Medical Association Journal, 168(8), 1001-10.
Kabat-Zinn, J. (1990). Full catastrophe living. New York: Delacorte Press.
Luthe, W. & Schultz, J.H. (1969). Autogenic therapy: Vol II: Medical applications. New York: Grune & Stratton.
Mathew, R.J.; Claghorn, J.L.; Largen, J.W.; & Dobbins, K. (1979). Skin Temperature control for premenstrual tension syndrome:A pilot study. American Journal of Clinical Biofeedback, 2 (1), 7-10.
Peper, E. (1990). Breathing for health. Montreal: Thought Technology Ltd.
Schultz, J.H., & Luthe, W. (1969). Autogenic therapy: Vol 1. Autogenic methods. New York: Grune and Stratton.
Schwartz, M.S. & Andrasik, F.(2003). Biofeedback: A practitioner’s guide, 3nd edition. New York: Guilford Press.
Shumaker, S.A., Legault, C., Thal, L., Wallace, R.B., Ockene, J., Hendrix, S., Jones III, B., Assaf, A.R., Jackson, R. D., Morley Kotchen, J., Wassertheil-Smoller, S.; & Wactawski-Wende, J. (2003). Estrogen plus progestin and the incidence of dementia and mild cognitive impairment in post menopausal women: The Women’s Health Initiative memory study: A randomized controlled trial. Journal of the American Medical Association, 289 (20), 2651-2662.
Stearns, V., Beebe, K. L., Iyengar, M., & Dube, E. (2003). Paroxetine controlled release in the treatment of menopausal hot flashes. Journal of the American Medical Association, 289 (21), 2827-2834.
Stroebel, C. F. (1982). QR, the quieting reflex. New York: G. P. Putnam’s Sons.
van Dixhoorn, J.J. (1998). Ontspanningsinstructie Principes en Oefeningen (Respiration instructions: Principles and exercises). Maarssen, Netherlands: Elsevier/Bunge.
Wassertheil-Smoller, S., Hendrix, S., Limacher, M., Heiss, G., Kooperberg, C., Baird, A., Kotchen, T., Curb, Dv., Black, H., Rossouw, J.E., Aragaki, A., Safford, M., Stein, E., Laowattana, S., & Mysiw, W.J. (2003). Effect of estrogen plus progestin on stroke in postmenopausal women: The Women’s Health Initiative: A randomized trial. Journal of the American Medical Association, 289 (20), 2673-2684.
Wyeth Pharmaceuticals (2003, June 4). A message from Wyeth: Recent reports on hormone therapy and where we stand today. San Francisco Chronicle, A11.
*We thank Candy Frobish, Mary Bier and Dalainya Kazarian for their helpful contributions to this research.
**For communications contact: Erik Peper, Ph.D., Institute for Holistic Healing Studies, San Francisco State University, 1600 Holloway Avenue, San Francisco, CA 94132; Tel: (415) 338 7683; Email: epeper@sfsu.edu; website: http://www.biofeedbackhealth.org; blog: http://www.peperperspective.come
A breath of fresh air-Improve health with breathing
Posted: September 11, 2014 Filed under: Breathing/respiration, Pain/discomfort, stress management, Uncategorized | Tags: asthma, Breathing, pain, regeneration, relaxation, respiration, stress management, yoga 12 Comments“My breathing was something that took me a long time to adjust. I had been breathing almost entirely from my chest and my stomach was hardly moving when I breathed. I made a conscious effort all throughout the day to breathe slowly and with my stomach relaxed. I’ve noticed that my mood is much better when I am breathing this way, and I am much more relaxed. Immediately before I feel like I would have a seizure, if I would change my breathing technique and make sure I was breathing slowly and with my stomach. It would avoid the seizure from developing… This is a huge improvement for me.” –24 year old student who previously experienced 10 epileptic seizures per week
“I blanked out and could not remember the test material. I then reminded myself to breathe lower and slower while imagining the air slowly flowing down my legs. After three breaths, I could again process the information and continue to take the exam. A week later I got my grade back– an A-. Better than I had expected.” –21 year old student
Breathing occurs without awareness unless there are specific problems such as asthma, emphysema or when we run out of air while exercising. Breathing is more than just the air moving in and out. It is the boundary between the conscious and the unconscious—the voluntary and involuntary nervous system— and affects the sympathetic and parasympathetic activity of our body. The way we breathe, such as chronic low level hyperventilation, may contribute to increasing or decreasing anxiety, pain, epileptic seizure, exhaustion, abdominal pain, urinary incontinence or fertility.
We usually think of breathing occurring in our chest. Thus, during inhalation, we puff-up our chest so the lungs will expand. Observe that many people breathe this way and call it normal. Experience how you breathe:
Put your right and on your stomach and your left hand of your chest. Now take a quick big breath. Observe what happened. In most cases, your chest went up and your abdomen tightened and even pulled in.
This breathing pattern evokes a state of arousal and vigilance and activates your sympathetic nervous system. You tend to automatically tighten or pull in your stomach wall to protect your body. When we’re in pain, afraid, anticipate danger or have negative and fearful thoughts, “Do I have enough money for the rent,” or “Feeling rushed and waiting for a delayed Muni bus,” we instinctively hold our breath, slightly tense our muscles and breathe shallowly. Unfortunately, this makes the situation worse—symptoms such as pain, anxiety or abdominal discomfort will increase. This type of breathing is the part of the freeze response—a primal survival reflex. It may even affect our ability to think. Experience how dysfunctional breathing effects us by doing the following exercise (Peper & MacHose, 1993; Gorter & Peper, 2011).
Sit comfortably and breathe normally.
Now inhale normally, but exhale only 70 percent of the air you just inhaled.
Inhale again, and again only exhale 70 percent of the previously inhaled volume of air. If you need to sigh, just do it, and then return to this breathing pattern again by exhaling only 70 percent of the inhaled volume of air.
Continue to breathe in this pattern of 70 percent exhalation for about forty-five seconds, each time exhaling only 70 percent of the air you breathe in. Then stop, and observe what happened.
What did you notice? Within forty-five seconds, more than 98 percent of people report uncomfortable sensations such as lightheadedness, dizziness, anxiety or panic, tension in their neck, back, shoulders, or face, nervousness, an increased heart rate or palpitations, agitation or jitteriness, feeling flushed, tingling, breathlessness, chest pressure, gasping for air, or even a sensation of starving for air. This exercise may also aggravate symptoms that already exist, such as headaches, joint pain, or pain from an injury. If you’re feeling exhausted or stressed, the effects seem even worse.
On the other hand, if you breathed like a happy baby, or more like a peaceful dog lying on its side, the breathing movement occured mainly in the abdomen and the chest stays relaxed. This effortless diaphragmatic breathing promotes regeneration by allowing the abdomen to expand during inhalation and becoming smaller during exhalation as shown in Figure 1.

Figure 1. Illustration of diaphragmatic breathing in which the abdomen expands during inhalation and contracts during exhalation (reproduced by permission from Gorter, R. & Peper, E. (2011). Fighting Cancer-A Non Toxic Approach to Treatment. Berkeley: North Atlantic).
The abdominal movement created by the breathing improves blood and lymph circulation in the abdomen and normalizes gastrointestinal function and enhances regeneration. It supports sympathetic and parasympathetic balance especially when the breathing rate slows to about six breaths per minute. When breathing slower, exhaling takes about twice as long as the inhalation. When you inhale, the abdomen and lower ribs expand to allow the air to flow in and during exhalation the abdomen decreases in diameter and the breath slowly trails off. It is as if there is an upside down umbrella above the pelvic floor opening during inhalation and closing during exhalation.
Most people do not breathe this way . They suffer from “designer’s jean syndrome”. The clothing is too constricting to allow the abdomen to expand during inhalation (Remember how good it felt when you loosened your belt when eating a big meal?). Or, you are self-conscious of your stomach, “What would people thinks if my stomach hung out?” Yet, to regenerate, allow yourself to breathe like peaceful baby with the breathing movements occurring in the belly. Effortless diaphragmatic breathing is the cheapest way to improve your health. Thus observe yourself and transform your breathing patterns.
Interrupt breath holding and continue to breathe to enhance health. Observe situations where you hold your breath and then continue to breathe. If you expect pain during movement or a procedure, remember to allow your abdomen to expand during inhalation and then begin to exhaling whispering “Shhhhhhhhh.” Start exhaling and then begin your movement while continuing to exhale. In almost all cases the movement is less painful and easier. We observed this identical breathing pattern in our studies of Mr. Kawakami, a yogi who insert unsterilized skewers through his neck and tongue while exhaling—he did not experience any pain or bleeding as shown in Fig 2.

Figure 2. Demonstration by Mr. Kawakami, a yogi, who inserted non-sterile skewers while exhaling and reported no pain. When he removed the skewers there was no bleeding and the tissue healed rapidly (by permission from Peper, E., Kawakami, M., Sata, M. & Wilson, V.S. (2005). The physiological correlates of body piercing by a yoga master: Control of pain and bleeding. Subtle Energies & Energy Medicine Journal. 14(3), 223-237).
Shift shallow chest breathing to slower diaphragmatic breathing. Each time you catch yourself breathing higher in your chest. Stop. Focus on allowing your abdomen to expand during inhalation and become smaller during exhalation as if it was a balloon. Allow the air to flow smoothly during exhalation and allow the exhalation to be twice as long as the inhalation. Over time allow yourself to inhale to the count of three and exhale to the count of 6 or 7 without effort. Imagine that when you exhale the air flows down and through your legs and out your feet. As you continue to breathe this way, your heart rate will slightly increase during inhalation and decrease during exhalation which is an indication of sympathetic and parasympathetic restorative balance. A state that supports regeneration (for more information see, Peper, E. & Vicci Tibbetts, Effortless diaphragmatic breathing).
For many people when they practice these simple breathing skills during the day their blood pressure, anxiety and even pain decreases. While for other, it allows clarity of thought.
