Surgery: Hope for the best and plan for the worst!
Posted: March 18, 2018 Filed under: Pain/discomfort, placebo, self-healing, stress management, surgery, Uncategorized | Tags: anesthesia, hernia, iatrogenic illness, technology, urinary retention 20 CommentsAdapted from: Peper, E. Surviving and preventing medical errors. (2019). Townsend Letter-The Examiner of Alternative Medicine. 429, 63-69. https://townsendletter.com/surviving-and-preventing-medical-errors-peper/
The purpose of this blog is to share what I have learned from a cascade of medical errors that happen much more commonly than surgeons, hospitals, or health care providers acknowledge and is the third leading cause of death in the US (Makary, M.A. & Daniel, M., 2016). My goal here is to provide a few simple recommendations to reduce these errors.

It is now two years since my own surgery—double hernia repair by laparoscopy. The recovery predicted by my surgeon, “In a week you can go swimming again,” turned out to be totally incorrect.
Six weeks after the surgery, I was still lugging a Foley catheter with a leg collection bag that drained my bladder. I had swelling due to blood clots in the abdominal area around my belly button, severe abdominal cramping, and at times, overwhelming spasms. For six weeks my throat was hoarse following the intubation. Instead of swimming, hiking, walking, working, and making love with my wife, I was totally incapacitated, unable to work, travel, or exercise. I had to lie down every few hours to reduce the pain and the spasms.
Instead of going to Japan for a research project, I had to cancel my trip. Rather than teaching my class at the University, I had another faculty member teach for me. I am a fairly athletic guy—I swim several times a week, bike the Berkeley hills, and hiked. Yet after the surgery, I avoided even walking in order to minimize the pain. I moved about as if I were crippled. Now two years later, I finally feel healthy again.
How come my experiences were not what the surgeon promised?
All those who cared for me during this journey were compassionate individuals, committed to doing their best, including the emergency staff, the nurses, my two primary physicians, my surgeon, and my urologist. However, given the personal, professional, and economic cost to me and my family, I feel it is important to assess where things went wrong. The research literature makes it clear that my experience was by no means unique, so I have summarized some of the most important factors that contributed to these unexpected complications, following “simple arthroscopic surgery.”
- Underestimating the risk. Although the surgeon suggested that the operation would be very low risk with no complications, the published research data does not support his optimistic statement and misrepresented the actual risk. Complications for laparoscopic surgery range from 15% to as high as 38% or higher, depending on the age of the patient and how well they do with general anesthesia (Vigneswaran et al, 2015; Neumayer et al, 2004; Perugini & Callery, 2001). Experienced surgeons who have done more than 250 laparoscopic surgeries have a lower complication rate. However, a 2011 Cochran review points out that there is theoretically a higher risk that intra-abdominal organs will be injured during a laparoscopic procedure (Sauerland, 2011). In addition, bilateral laparoscopic hernia repair has significantly higher risk than single sided laparoscopic hernia repair for post-operative urinary retention (Blair et al, 2016). My experience is not an outlier–it is more common.
- Inappropriate post-operative procedures. In my case I was released directly after waking up from general anesthesia without checking to determine whether I could urinate or not. The medical staff and facility should never have released me, since older males have a 30% or higher probability that urinary retention will occur after general anesthesia. However, it was a Friday afternoon and the staff probably wanted to go home since the facility closes at 5:30 pm. This landed me in the Emergency Room.
- Medical negligence. In my case the surgeon recommended that I have my bladder in the emergency room emptied and then go home. That was not sufficient, and my body still was not working properly, requiring a second visit to the ER and the insertion of a Foley catheter. Following the second ER visit, the surgeon removed the catheter in his office in the late afternoon and did not check to determine whether I could urinate or not. This resulted in a third ER visit.
- Medical error. On my third visit to the emergency room, the nurse made the error of inflating the Foley catheter balloon when it was in the urethra (rather than the bladder) which caused tearing and bleeding of the urethra and possible irritation to the prostate.
- Drawbacks of the ER as the primary resource for post-surgical care. Care is not scheduled for the patient’s needs, but rather based on a triage system. In my case I had to wait sometimes two hours or more until a catheter could be inserted. The wait kept increasing the urine volume which expanded and irritated the bladder further.
- A medical system that does not track treatment outcomes. Without good follow-up and long-term data, no one is accountable or responsible.
- A reimbursement system that rewards lower up-front costs. The system favors quick outpatient surgeries without factoring in the long-term costs and harm of the type I experienced.
Assuming the best and not planning for the worst.
Can I trust the health care provider’s statement that the procedure is low risk and that the recovery will go smoothly?
The typical outcome of a medical procedure or surgery may be significantly worse than generally reported by hospitals or medical staff. In many cases there is no systematic follow-up nor data on outcomes and complications, thus no one knows the actual risks.
In the United States medical error results in at least 98,000 unnecessary deaths each year and 1,000,000 excess injuries (Weingart et al, 2000; Khon et al, 2000). The Institute of Medicine reported in 2012 that one-third of hospitalized patients are harmed during their stay (Ferguson, 2012; Institute of Medicine, 2012).
One should also be intelligently skeptical about positive claims for any specific study—it is important to know whether the study has been replicated with other populations and not just a particular group of patients.
To quote Dr. Marcia Angell (2009), the first woman editor of the highly respected New England Journal of Medicine, “It is simply no longer possible to believe much of the clinical research that is published, or to rely on the judgment of trusted physicians or authoritative medical guidelines. I take no pleasure in this conclusion, which I reached slowly and reluctantly over my two decades as an editor of The New England Journal of Medicine.”
The evidence for many procedures and medications is surprisingly limited
- Research studies frequently select specific subsets of patients. They may exclude many patients who have other co-morbidities.
- Clinical trials may demonstrate statistical significance without providing clinically meaningful results. For example, between 2009 and 2013 all most all cancer drugs that were approved for treatment in Europe showed upon follow-up no clear evidence that they improved survival or quality of life for patients (Davis et al, 2017; Kim & Prasad, 2015).
- Pharmaceuticals are tested only against a passive placebo. In some cases, the patient’s positive response may actually be the placebo effect, due to physical sensations induced by the medication or its side effects, thus inspiring hope that the drug is working (Peper and Harvey, 2017).
- Negative side effects are significantly underreported. The data depend on self-report by both the patient and the health care provider.
Many published studies on the positive clinical outcome of pharmaceuticals are suspect. As Dr. Richard Horton (2015), Editor-in-Chief of The Lancet, wrote in 2015, “A lot of what is published is incorrect … much of the scientific literature, perhaps half, may simply be untrue. Afflicted by studies with small sample sizes, tiny effects, invalid exploratory analyses, and flagrant conflicts of interest, together with an obsession for pursuing fashionable trends of dubious importance, science has taken a turn towards darkness.”
Most studies, including those on surgery, lack long-term follow-up.
The apparent short-term benefits may be not beneficial in the long term or may even be harmful. For example, doctors and patients are convinced that SSRIs (serotonin re-uptake inhibitors—antidepressants such as Paxil and Prozac) are beneficial, with resulting global sales in 2011 of $11.9 billion. However, when all the research data were pooled, metanalysis showed that these drugs are no more effective than placebo for the treatment of mild to moderate depression and increase suicides significantly among young adults (Fournier et all, 2010; Kirsch, 2014).
Consider long-term follow-up in my case: the surgeon will report a successful surgery, despite the fact that it took me almost two years to recover fully. (I did not die during surgery and left in seemingly good shape.). Although I called him numerous times for medical guidance during my complications, the outpatient surgical facility will report no complications since I was not transferred from that facility during the surgery to a hospital for continuing care. My insurance carrier that paid the majority of the medical bills recorded the invoices as separate unrelated events: one surgery/one bill, but three separate bills for the emergency room, an additional visit to my primary care physician to check my abdomen when my surgeon did not return my call, and the ongoing invoices from the urologist. They all reported success because the iatrogenic events were not linked to the initial procedure in the data base.
In my case, following surgery, I had to go to the emergency room on three separate occasions due to post-operative urinary retention, placing me at risk of permanent detrusor muscle damage. For more than 18 months, I was under the care of a urologist.
Over the past two years, my symptoms have included gastrointestinal inflammation, spasms, and abdominal bulging, which are only now disappearing. Even my posture has changed. I am now working to reverse the automatic flexing at the hips and leaning forward which I covertly learned to reduce the abdominal discomfort. This level of discomfort and dysfunction are new to me. Reading the research on laparoscopy, I realized that excessive internal bruising, large hematomas, and internal adhesions are fairly common with this type of surgery. However, soft tissue injuries are difficult to confirm with imaging techniques.
My complications were also a direct result of inappropriate post-surgical recommendations and treatment. The symptoms were further compounded by faulty patient discharge procedures performed by the outpatient surgical facility. Since this was my first general anesthesia, I had no idea that I would be one of the people whose outcome were not what the surgeon had predicted. Thus, hope for the best, but plan for the worst.
SCHEDULING MEDICAL PROCEDURES
The following are recommendations may help reduce post-surgical or medical procedure complications.
- Schedule elective medical procedures or surgery early the morning and in the middle of the week. Do not schedule procedures on Mondays, Fridays, or in the afternoon. Procedures performed in the afternoon have significant increase in complications and errors. Anesthesia complications, for example, are four times higher in the afternoon than in the morning (Wright et al, 2006). Our biological rhythms affect our ability to attend and focus. In the morning most people are able to concentrate better than in the afternoon (Pink, 2018).
- Avoid weekends. Procedures performed on weekends (as compared to those done in the middle of the week) increase the risk of complications or dying. For example, babies born on the weekend have a 9.2% higher infant mortality than those born during the week, while those born on Tuesdays have the lowest death rate (Palmer et al, 2015). It is possible that on Mondays medical staff are recovering from weekend binging, while on Fridays they are tired and looking forward to the weekend? If elective procedures are done on a Friday and complications arise, the emergency room is the only option, as the medical staff may not be available over the weekend. In my case the procedure was done on a Friday, and I left the surgical outpatient facility at 2 pm. When complications occurred, it was after 5:30 pm—phone support from the advice nurse and the surgeon on call were my only option until the following Monday. Thus, I had to go the emergency room late Friday evening and again the next evening because of urinary retention, with a long delay in a busy waiting room. Since, I wasn’t bleeding or having a heart attack, that meant I had to wait, wait and wait, which significantly aggravated my specific problem.
- Schedule medical procedures at least one or two weeks before any holiday. Do not schedule surgery just before or during holidays. Medical staff also take holidays and may not available. In my case, I scheduled the procedure the Friday before Thanksgiving because I thought I would have a week of recovery during my Thanksgiving break from teaching. This meant that medical staff were less available and more involved in their holiday planning.
- Schedule procedures so that you are released early in the day. This can allow you to return to the facility in case complications arise. I was released at 2 pm and the complications did not occur until early evening. The facility was closed, so the only option was the ER. When possible, schedule medical procedures or surgery in a facility that is able to provide post-operative care after 5 pm.
- Do not schedule elective procedures during the month of July in an academic teaching hospital. During this month mortality increases and efficiency of care decreases because of the end of the academic year and subsequent changeover to new personnel (Young et al, 2011). Medical school graduates with limited clinical experience begin their residencies and experienced house staff are replaced with new trainees. This is known as the July effect in the U.S. and Killing season in the United Kingdom. During the month of July in any given year, fatal medication errors, for example, increase by 10% at teaching hospitals, but not at neighboring hospitals which do not experience this turnover in medical personnel (Phillips & Barker, 2010).
- Have procedures performed at a medical facility in which the health care professional has no financial interest—take economics out of the equation. When health care practitioners have financial interest in a facility, they tend to order more tests and procedures than health care providers who have no financial interests (Bishop et al, 2010). In my case the surgeon had a financial interest in the outpatient surgical facility where I received surgery. Had I had the operation across the street in the hospital where the surgeon also operates, I probably would not have been released early, avoiding the problems in follow-up care.
STRATEGIES TO OPTIMIZE OUTCOMES AND HEALTH
Organize your support system. Assume that recovery could be more difficult then promised.
Before your procedure, ask family members, friends, and neighbors to be prepared to help. If you did not need them, thank them for their willingness to help. In my case I did not plan for complications, thus my wife was my entire support system, especially for the first three weeks when I was unable to do anything except rest and cope. I was very fortunate to have numerous family, friends, and colleagues who offered their expertise to help me understand what was going on and who assumed my responsibilities when needed.[1]
- Bring an advocate to your appointments. Have your advocate/friend keep notes and ask questions, especially if the health care provider is a respected authority and you are suffering, exhausted, and/or anxious. Record any detailed instructions you must follow at home as a video or audio file on your cell phone or write them down (be sure to ask the health provider for permission). Under stress one may not be able to fully process instructions from the health care provider.
- Make a list of questions and concerns before seeing your health care provider. Talk to your partner and close friends and ask them if there are questions or concerns that you should raise with your provider.
- Ask for more information when tests or procedures are proposed (Robin, 1984).
- Why do you recommend this particular test/procedure/intervention for me and what are the major benefits?
- What are the risks and how often do they occur, in your experience and in the research literature?
- What will you do if the treatment is not successful?
- Ask your provider if there is anything that you should or should not do to promote healing. As much as possible, ask for advice on specific efforts you can make. General statements without instructions such as, “Relax” or “Don’t worry,” are not helpful unless the practitioner teaches you specific skills to relax or to interrupt worrisome thoughts. Many health professionals do not have the time to teach you these types of skills. In many cases the provider may not be able to recommend documented peer-reviewed self-care strategies. Often they imply—and they can be correct—that the specific medical treatment is the only thing that will make you better. In my case I did not find any alternative procedures that would reverse a hernia, although there may be habitual postural and movement patterns that could possibly prevent the occurrence of a hernia (Bowman, 2016). Being totally dependent upon the medical procedure may leave you feeling powerless, helpless, and prone to worry. In most cases there are things you can do to optimize self- healing.
- Think outside the box. Explore other forms of self-care that could enhance your healing. Initiate self-care action instead of waiting passively. By taking the initiative, you gain a sense of control, which tends to enhance your immune system and healing potential. Do anything that may be helpful, as long as it is not harmful. In my case, future medical options to resolve urinary retention could include additional medications or even surgery. Researching the medical literature, there were a number of studies showing that certain herbs in traditional Chinese medicine and Ayurveda medicine could help to reduce prostate inflammation and possibly promote healing. Thus, I began taking three different herbal substances for which there was documented scientific literature. I also was prescribed herbal tea to sooth the bladder. Additionally, I reduced my sugar and caffeine intake to lower the risk of bladder irritation and infection.
- Collaborate with your health care provider. Let your provider know the other approaches you are using. Report any interventions such as vitamins, herbs, Chinese medicine. Ask if they know of any harm that could occur. In most cases there is no harm. The health care professional may just think it is a waste of time and money. However, if you find it helpful, if it gives you control, if it makes you less anxious, and if it is not harmful, it may be beneficial. What do you have to lose?
- Assume that all the health care professionals are committed to improving your health to the best of their ability. Yet at times professionals are now so specialized that they focus only on their own discipline and not the whole person. In their quest to treat the specific problem, they may lose sight of other important aspects of care. Thus, hope for the best, but plan for the worst.
PREPARING FOR SURGERY
Assume that the clinical staff will predict a more positive outcome than that reported in the medical literature. In most cases, especially in the United States, there is no systematic follow-up data since many post-surgical complications are resolved at another location. In addition, many studies are funded by medical companies which have a vested interest and report only the positive outcomes. The companies tend not to investigate for negative side-affects, especially if the iatrogenic effects occur weeks, months, or years after the procedure. This has also been observed in the pharmaceutical companies sponsoring studies for new medications.
Generally, when independent researchers investigated medical procedures they found the complication rate three-fold higher than the medical staff reported. For example, for endoscopic procedures such colonoscopies, doctors reported only 31 complications from 6,383 outpatient upper endoscopies and 11,632 outpatient colonoscopies. The actual rate was 134 trips to the emergency room and 76 hospitalizations. This discrepancy occurred because the only incidents reported involved patients who went back to their own doctors. It did not capture those patients who sought help at other locations or hospitals (Leffler et al, 2010).
The data are even worse for patients who are hospitalized; in the U.S. 20% of patients who leave the hospital return within a month while in England, 7% of those leaving the hospital return within a month (Krumholz, 2013).
- Ask about possible complications that could arise, the symptoms, and what the physician would do if they occurred. Do not assume the health professional will have the time to explain or know all the possible complications. In my case when the surgeon removed the catheter at 4 pm during my second emergency room visit, I had to ask, “What would happen if I still cannot urinate?” Again, the emergency room was the only answer. However, I know now that he could have taught me simple self-catherization which would have eliminated the long waiting in the emergency room, the excessive stretching of the bladder and the subsequent emergency room medical error on my third visit to the ER. It would also have reduced the medical costs by a thousand-fold.
- Get a second opinion. In my case, the surgeon came highly recommended, is very experienced, and has done many hernia repairs. I trusted his judgement that I needed a bilateral hernia repair although I only felt the bulging in the right inguinal area and did not feel bulging or sensations in the left inguinal area. Despite my feeling of trust, I should have asked for a second independent opinion just to be sure. In many moments of despair when suffering the significant complications, I even started to wonder if the bilateral laparoscopic surgical repair was really necessary or just done to increase the income of the surgeon and the outpatient surgical facility in which he had a financial interest. My surgery resulted in large hematomas, irritation of internal organs, and possible damage to the GI track. This type of complication did not occur for a close friend who had a single-sided hernia repair by the same surgeon in a hospital where the surgeon had no financial interests.
- Request medical personnel who are highly experienced in the intervention. Mortality and complications rates are significantly lower for practitioners who have done the procedure at least 250 times.
- Don’t assume the worst but be prepared for the worst. Ask your health care provider about the various side effects of surgery, including the worst things that could happen, and then develop a pre-emptive plan.
The most common problems associated with surgery and general anesthesia include:
- Urinary retention. Following general anesthesia, neural enervation to the bladder and gastrointestinal tract are often affected. The general risk for postoperative urinary retention (POUR) for all types of surgeries ranges from 7% to 52% (Tammela et al, 1986; Petros et al, 1990; Petros et al, 1991; Gonullu et al, 1993; Tammela, 1995). For patients who have surgery for hernia repair 24.4% will experience postoperative urinary retention (Keita et al, 2005)—one in four. The risk for older males is even higher (Blair et al, 2017). Do not leave the medical unit until you have urinated or have a Foley catheter inserted with a leg bag and appropriate follow-up managed by a urologist. In my case, neither the surgeon nor the outpatient hospital checked to determine whether I could urinate—they just discharged me the moment I was conscious. Discharging a patient who has had general anesthesia without checking to determine whether they can urinate goes against all medical guidelines and standard hospital policies and constitutes malpractice. As this was my first surgery, I had no idea that urinary retention could occur. Thus, I did not recognize the symptoms nor did the advice nurse or the surgeon when called for advice before I checked into the emergency room.
- Expect constipation and plan to eat a high roughage diet that supports bowel movements. In case bowel function is slow in resuming, you may want to have on hand simple over-the-counter supplements such as magnesium capsules, psyllium husks, and aloe vera juice or gel, all available at any health food store. Liquid magnesium citrate (GoLytely® solution available at drug stores), can be useful, but tends to be a little stressful to take. Check these over-the-counter supplements with your provider to avoid supplement-drug interaction.
- Infection. Many patients pickup hospital-induced infections (nosocomial infections). In my case, I after four weeks with a Foley catheter, I got a mild bladder infection and had to control it with antibiotics. While in the hospital, avoid direct physical contact with other patients and staff, wash and rewash your hands. Remember medical staff tend are less attentive and wash their hands 10% less in the afternoons than in morning. Ask the medical staff to thoroughly wash their hands before they examine you. If you do get an infection, contact your medical provider immediately.
ACTION STEPS
- Pace yourself. Assume that recovery could be slower than promised. Although your body may appear to be healed, in many cases your vitality could be significantly reduced for a number of months, and you will probably feel much more fatigued in the evening. The recovery from general anesthesia has been compared to recovery from a head-on car collision.
- Identify your support system in case you cannot take care of yourself initially. Organize family and friends to help you. In my case, for the first two weeks I did not have the energy to do anything for myself—the overwhelming abdominal spasms and the three episodes in the ER had drained my energy. I was very lucky that I had my family and friends to help me. For the first few weeks I was so distracted by the pain and discomfort that I did not drive or take care of myself.
- Have a plan in case you need to go to the Emergency Room in the evening. Know its location and have someone who can take you.
- Assume that you will probably have an extensive wait in the ER unless you are desperately ill. Do not try to “tough it out.” Be totally honest about your level of pain, so you can get the best possible care. In my case, I had horrible abdominal pain and spasms with urinary retention, but still acted as if I were okay. When the admitting nurse asked me how I felt, I rated my discomfort as a 5 on a scale from 0 to 10. In my mind I compared the pain with that I had experienced after a skiing accident, which was much worse. What I had forgotten was that the ER is triage system, so I had to wait and wait and wait, which was phenomenally uncomfortable.
- In the ER, ask which medical specialist can follow up with you if further issues develop. A general hospital usually has specialists on call. In my case, if I had requested care from a specialist, I would have been treated directly by a urologist. I would not have had to follow the advice of the surgeon who said, “When you go to Emergency Room, have them empty the bladder and then go home.” Almost all urologists would have recommended keeping the Foley catheter in for a few days to allow the side effects of the anesthesia and the trauma caused by the bladder expansion to ameliorate and then test whether urination was possible.
- Have a medical advocate with you at all times who can observe that the procedures are done correctly. There is a four-fold increase in errors during the evenings and nights as compared to the morning. The more medical staff is multi-tasking, the more likely they will make errors. Have the medical personnel explain any procedure before they perform it—why and how they will do the procedure and what you will experience. You also need to know if they are experienced in that particular procedure? If the answers do not make sense, stop them and ask for another staff member.
- In the ER, record the instructions on your phone. Have medical staff explain and demonstrate to you and your support person what you will need to do at home. Then repeat the instructions back to them to be certain you have it right.
- Remind yourself that errors can occur. In my case, during the third ER visit for urinary retention, the nurse delayed the anchoring of the catheter and it had slipped down into the urethra. As she began to pump, I could feel my urethra tearing and I alerted her to stop. This was immediately followed by another procedural error on her part, so I had to again alert her to stop, which she finally did. All this occurred at 1 am in the morning. As the patient, I had to take charge at a time when I was totally exhausted. As the nurse retreated, I was left sitting on the gurney waiting for someone to come and follow-up. I waited and waited and when I finally stood up, the catheter dropped out and I began bleeding.
Lesson learned: hope for the best but prepare for the worst. In my situation, after eight weeks and numerous visits to the urologist, he removed the catheter. He did this at 8:30 in the morning. This way I could go home and in case something happened, I could go back to his office for further care. Before leaving the office, I planned for the worst. I asked what would happen if I could not urinate later in the evening and requested that he give me a few catheters, so if problems developed, I could catheterize myself.
The urologist gave me the catheters and explained how to use them, although I did not actually practice on myself. Still, I felt better prepared. During the day, I become more and more optimistic because I had no problems; however, at 2 am I woke up unable to urinate. For the next hour, I felt very anxious about inserting the catheter, since I had never done it myself. Finally, my discomfort overcame my anxiety. To my surprise, it was easy. After waiting a few minutes, I removed the catheter and went to bed feeling much more comfortable. The next morning after breakfast and a cup of coffee, I found that my body was working fine without the catheter.
Had I not planned for the worst, I would have once again gone to the Emergency Room and probably waited for hours, risking a repeat of tremendous discomfort and irritation. This simple planning reduced my medical cost more than a thousand-fold from $1700 for the emergency room to $2 for some single-use catheters.
References
Angell, M. (2009). Drug companies & doctors: A story of corruption. The New York Review of Books, 56(1), 8-12. http://www.nybooks.com/articles/2009/01/15/drug-companies-doctorsa-story-of-corruption/
Bishop, T.F., Federman, A.D., & Ross, J.S. (2010). Laboratory test ordering at physician offices with and without on-site laboratories, Journal of Gen Intern Med, 25(10)m 1057-1063. doi: 10.1007/s11606-010-1409-7
Blair, A.B., Dwarakanath, A., Mehta, A., Liang, H., Hui, X., Wyman, C., Ouanes, J.P.P., & Nguyen, H.T. (2017). Postoperative urinary retention after inguinal hernia repair: a single institution experience. Hernia, 21(6), 895-900.
Bowman, K. (2016). Diastasis Recti: The whole-body solution to abdominal weakness and separation. Propriometrics Press: Carlsborg, WA 98324
Davis, C., Naci, N., Gurpinar, E., Poplavska, E., Pinto, A., Aggarwal, A. (2017). Availability of evidence of benefits on overall survival and quality of life of cancer drugs approved by European Medicines Agency: retrospective cohort study of drug approvals 2009-13. BMJ, 2017; j4530 DOI: 10.1136/bmj.j4530
Ferguson, T. B. (2012). The Institute of Medicine Committee report “best care at lower cost: the path to continuously learning health care”. Circulation: Cardiovascular Quality and Outcomes, 5(6), e93-e94. http://jama.jamanetwork.com/article.aspx?articleid=185157
Fournier, J. C., DeRubeis, R. J., Hollon, S. D., Dimidjian, S., Amsterdam, J. D., Shelton, R. C., & Fawcett, J. (2010). Antidepressant drug effects and depression severity: a patient-level meta-analysis. JAMA, 303(1), 47-53.
Gönüllü, N. N., Gönüllü, M., Utkan, N. Z., Dülger, M., Gökgöz, S., & Karsli, B. (1993). Postoperative retention of urine in general surgical patients. The European journal of surgery= Acta chirurgica, 159(3), 145-147.
Horton, R. (2015). Offline: What is medicine’s 5 sigma? The Lancet, 385(9976), 1380. http://www.thelancet.com/journals/lancet/article/PIIS0140-6736%2815%2960696-1/fulltext?rss%3Dyes
Institute of Medicine’s Infographic, accompanying their 2012 report, Best Care at Lower Cost, at http://www.iom.edu/Reports/2012/Best-Care-at-Lower-Cost-The-Path-to-Continuously-Learning-Health-Care-in-America/Infographic.aspx
Keita, H., Diouf, E., Tubach, F., Brouwer, T., Dahmani, S., Mantz, J., & Desmonts, J. M. (2005). Predictive factors of early postoperative urinary retention in the postanesthesia care unit. Anesthesia & Analgesia, 101(2), 592-596.
Kim, C. & Prasad, V. (2015). Cancer drugs approved on the basis of a surrogate end point and subsequent overall survival-An analysis of 5 Years of US Food and Drug Administration approvals. JAMA Intern Med,175(12):1992-1994. doi:10.1001/jamainternmed.2015.5868
Kirsch, I. (2014). The emperor’s new drugs: medication and placebo in the treatment of depression. In Placebo (pp. 291-303). Springer Berlin Heidelberg.
Kohn, L. T., Corrigan, J. M., & Donaldson, M. S. (Eds.). (2000). To err is human: building a safer health system (Vol. 6). National Academies Press. http://www.ncbi.nlm.nih.gov/books/NBK221671/
Krumholz, H. M. (2013). Post-hospital syndrome—an acquired, transient condition of generalized risk. New England Journal of Medicine, 368(2), 100-102. http://www.nejm.org/doi/full/10.1056/NEJMp1212324
Leffler, D.A, Kheraj, R., Garud, S., Neeman, N., Nathanson, L.A., Kelly, C.P., Sawhney, M., Landon, B., Doyle, R., Rosenberg, S., & Aronson, M. (2010). The incidence and cost of unexpected hospital use after scheduled outpatient endoscopy. Arch Intern Medicine, 170(19), 1752-1757. http://archinte.jamanetwork.com/article.aspx?articleid=226125
Makary, M.A. & Daniel, M. (2016). Medical error–the third leading cause of death in the US. British Medical Journal, 353:i2139
Neumayer, L., Giobbie-Hurder, A., Jonasson, O., Fitzgibbons Jr, R., Dunlop, D., Gibbs, J., & Henderson, W. (2004). Open mesh versus laparoscopic mesh repair of inguinal hernia. New England Journal of Medicine, 350(18), 1819-1827. http://academicdepartments.musc.edu/surgery/education/resident_info/journal_club/09-10/April-inguinal.pdf
Palmer, W. L., Bottle, A., & Aylin, P. (2015). Association between day of delivery and obstetric outcomes: observational study. BMJ, 351, h5774. http://www.bmj.com/content/bmj/351/bmj.h5774.full.pdf
Peper, E. & Harvey, R. (2017). The fallacy of the placebo controlled clinical trials: Are positive outcomes the result indirect treatment side effects? NeuroRegulation. 4(3–4):102–113 2017 doi:10.15540/nr.4.3-4.102
Perugini, R. A., & Callery, M. P. (2001). Complications of laparoscopic surgery. http://www.ncbi.nlm.nih.gov/books/NBK6923/?report=reader
Petros, J. G., & Bradley, T. M. (1990). Factors influencing postoperative urinary retention in patients undergoing surgery for benign anorectal disease. The American Journal of Surgery, 159(4), 374-376.
Petros, J. G., Rimm, E. B., Robillard, R. J., & Argy, O. (1991). Factors influencing postoperative urinary retention in patients undergoing elective inguinal herniorrhaphy. The American Journal of Surgery, 161(4), 431-433.
Phillips, D. P., & Barker, G. E. (2010). A July spike in fatal medication errors: a possible effect of new medical residents. Journal of General Internal Medicine, 25(8), 774-779. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2896592/
Pink, D.H. (2018). When: The Scientific Secrets of Perfect Timing. New York: Riverhead Books, ISBN-13: 978-0735210622
Robins, E.D. (1984). Matter of Life & Death: Risks vs. Benefits of Medical Care. New York: W.H. Freeman and Company.
Sauerland, S., Walgenbach, M., Habermalz, B., Seiler, C. M., & Miserez, M. (2011). Laparoscopic versus open surgical techniques for ventral or incisional hernia repair. The Cochrane Library.
Tammela, T. (1994). Postoperative urinary retention–why the patient cannot void. Scandinavian Journal of Urology and Nephrology. Supplementum, 175, 75-77.
Tammela, T., Kontturi, M., & Lukkarinen, O. (1986). Postoperative urinary retention: I. Incidence and predisposing factors. Scandinavian Journal of Urology and Nephrology. 20(3), 197-201.
Vigneswaran, Y., Gitelis, M., Lapin, B., Denham, W., Linn, J., Carbray, J., & Ujiki, M. (2015). Elderly and octogenarian cohort: Comparable outcomes with nonelderly cohort after open or laparoscopic inguinal hernia repairs. Surgery, 158(4), 1137-1144.
Weingart, S. N., Wilson, R. M., Gibberd, R. W., & Harrison, B. (2000). Epidemiology of medical error. BMJ: British Medical Journal, 320(7237), 774. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1117772/
Wright, M.D., Philips-Bute, B., Mark, J.B., Stafford-Smith, M., Grichnik, K.P., Andregg, B.C., & Taekman, J.M. (2006). Time of day effects on the incidence of anesthetic adverse events. Quality and Safety in Health Care. 15(4): 258–263.doi: 10.1136/qshc.2005.017566
Young, J. Q., Ranji, S. R., Wachter, R. M., Lee, C. M., Niehaus, B., & Auerbach, A. D. (2011). “July effect”: impact of the academic year-end changeover on patient outcomes: a systematic review. Annals of Internal Medicine, 155(5), 309-315. http://www.girardslaw.com/library/July_Effect_Annals_of_Internal_Medicine.pdf
[1] I think my family, friends and colleagues (Karen Peper, Norihiro Muramatsu, Richard Harvey, David Wise, Annette Booiman, Lance Nagel and many others) who generously supported me during this journey.
Improve your health: Lower your carbs
Posted: January 25, 2018 Filed under: Evolutionary perspective, Exercise/movement, Nutrition/diet, self-healing, Uncategorized | Tags: diet, metabolic syndrome, obesity, Type 2 diabetes 8 Comments
How come there is no disease caused by the absence of carbohydrates? This simple observation suggests that carbohydrates are not necessary for health and are not an essential food in our evolutionary history. This is different from vitamin C or other essential nutrients whose absence will cause scurvy and eventually death.
From an evolutionary perspective, simple carbohydrates, especially sugars and high-fructose corn syrup, are significant contributing factors to the increasing epidemic of obesity, type 2 diabetes, metabolic syndrome, coronary heart disease and many autoimmune disorders. The recommended nutritional guideline of the last forty years to reduce fats and increase carbohydrates were not based upon good science but on ideology influenced by agribusiness and the sugar industry (La Berge, 2008). The recommendations were WRONG AND HARMFUL (Taubes, 2016; see also: https://peperperspective.com/2017/02/18/read-the-case-against-sugar/). It may explains why the obesity epidemic is not caused by eating or drinking too many calories but the eating the wrong type of calories; namely, those found in simple carbohydrates and overly processed foods. The increase in obesity appears highly correlated with the US low-fat diet recommendations published in 1977 as shown in figure 1.
 Figure 1. Increase in U.S. obesity begins after the publication of the U.S. recommendations to eat a low-fat diet. Reproduced from National Center for Health Statistics (US). Health, United States, 2008: With Special Feature on the Health of Young Adults. Hyattsville (MD): National Center for Health Statistics (US); 2009 Mar. Chartbook
Figure 1. Increase in U.S. obesity begins after the publication of the U.S. recommendations to eat a low-fat diet. Reproduced from National Center for Health Statistics (US). Health, United States, 2008: With Special Feature on the Health of Young Adults. Hyattsville (MD): National Center for Health Statistics (US); 2009 Mar. Chartbook
The harmful effects of the simple high carbohydrate diet amplified with a decrease in physical activity interacts with your genetics. People, with a family risk factors of metabolic syndrome (type 2 diabetes) can improve their health by eating a low carbohydrate diet with lots of vegetables, fruit and fats.
Watch the superb video lectures by Professor Timothy Noakes, an emeritus professor of exercise and sports science at the University of Cape Town and by Gary Taubes, science writer and author of The case against sugar. It may shift your perspective and improve your health.
Reference:
La Berge, A. F. (2008). How the ideology of low fat conquered America. Journal of the History of Medicine and Allied Sciences, Volume 63, Issue 2, 1 April 2008, Pages 139–177, https://doi.org/10.1093/jhmas/jrn001
National Center for Health Statistics (US). Health, United States, 2008: With Special Feature on the Health of Young Adults. Hyattsville (MD): National Center for Health Statistics (US); 2009 Mar. Chartbook
Taubes, G. (2016). The Case Against Sugar. Portobello Books. ISBN 978-0-307-70164-0
How effective is treatment? The importance of active placebos
Posted: December 16, 2017 Filed under: Pain/discomfort, placebo, self-healing, stress management, Uncategorized | Tags: Active placebo, Clinical trials, expectancy, hope, nocebo, passive placebo, placebo 3 CommentsAdapted by Erik Peper and Richard Harvey from: Peper, E. & Harvey, R. (2017). The fallacy of the placebo-controlled clinical trials: Are positive outcomes the result of “indirect” treatment effects? NeuroRegulation, 4(3–4), 102–113. http://dx.doi.org/10.15540/nr.4.3-4.102
How come some drugs or medical procedures are initially acclaimed to be beneficial and later ineffective or harmful and withdrawn from the market?
How come some patients with a cancer diagnosis experience symptom remission after receiving a placebo medication? Take the case of Mr. Wright. Several decades ago Dr. Klopher (1957) described Mr. Wright as a patient who had a generalized and far advanced malignancy in the form of a lymphosarcoma with an estimated life expectancy of less than two weeks. Following the diagnosis Mr. Wright read a newspaper article about a promising experimental cancer medication called Krebiozen and requested that he receive the latest treatment. Soon after receiving the drug, Mr. Wright had a complete remission of cancer symptoms with no signs of the deadly tumor. For over two months after receiving the new promising drug, Krebiozen, Mr. Wright engaged in a normal life and was even able to fly his own plane at 12,000 feet. After a promising introduction to the medication, Mr. Wright subsequently read another newspaper article which proved the new medication to be a useless, inert preparation. Confused and demoralized, the results of the wonder drug did not last and his symptoms returned. When the final AMA announcement was published “Nationwide tests show Krebiozen to be a worthless drug in treatment of cancer,” his symptoms became acute and he died within two days (Klopher, 1957).
The term placebo loosely translates as ‘I shall please you’ can be contrasted with the term nocebo which loosely translates as ‘I shall harm you’ when referring to exposure to a sham medication, treatment or procedure that results a positive outcome (placebo response), or a negative outcome (nocebo response), respectively. The responses a person has reflect a complex interaction between many processes. For example, when studying a placebo or nocebo response we measure internal psychological processes, measured in terms of a person’s self-reported attitudes, beliefs, cognitions and emotions; behavioral processes, measured overtly by observations of a person’s actions; and, physiological processes, measured more or less directly with instruments such as heart rate monitors, or biochemical analyses. Most relevant is that a person’s beliefs about the placebo (or nocebo) medication, treatment or procedure leads to predictable positive (or negative) behaviors and physiological benefits or harms.
The case of Mr. Wright illustrates that we may underestimate the positive power of the placebo or, the negative power of the nocebo, where Mr. Wright’s belief about the medication’s benefits first interacted in a positive way (placebo) with his behaviors (e.g. engaging in daily activities including flying an airplane) as well as his physiology (e.g. cancer remission) and unfortunately later, in a negative way (nocebo) interacting with his physiology (e.g. cancer return) contributing to his death.
The placebo response can be very powerful and healing. For example, watch the very dramatic demonstration of how the placebo response can be optimized in Derren Brown’s BBC video Fear and Faith Placebo https://www.youtube.com/watch?v=y2XHDLuBZSw).
Placebo and nocebo effects are found in all therapeutic transactions when the communications between therapist and patient reflect embedded beliefs about the treatment. For example, patients have faith in clinician’s knowledge and belief that a prescribed medication is going to be effective at treating their symptoms, which then reinforces the patient’s belief in the medication, increasing indirect, embedded placebo effects, above and beyond any direct effects from the medication. The indirect effects of placebo responses have been most studied with medications; however, placebo effects are also studied in non-drug therapies. The research on placebo effects has demonstrated time and time again that when patients expect that the drug, surgery, or other therapeutic technique to be beneficial, then the patients tend to benefit more from the treatment.
The expectancy that the treatment will be effective at reducing symptoms is overtly, and covertly communicated by the health care professional during patient interactions, as well as by drug companies through direct to consumer advertising, and social media. The implied message is that the drug or procedure will improve symptoms, recovery or improve quality of life. On the other hand, if you do not do take the drug or do the procedure, your health will be compromised. For example, if you have high cholesterol, then take a statin drug to prevent the consequences of high cholesterol such as a heart attack or stroke. The implied message is that if you do not take it, you will die significantly sooner. Statins lower the risk for heart attacks; however, the benefits may be over stated. For people without prior heart disease, 60 people will have to take statins for 5 years to prevent 1 heart attack and 268 people to prevent 1 stroke. During the same time period 1 in 10 will experience muscle damage and 1 in 50 develop diabetes (theNNT, 2017 November).
If placebo and nocebo can have significant effects on medical outcome, how do you know if the treatment benefits are due to the direct effects of a drug or procedure or due to any indirect placebo effects or a combination of both?
The randomized controlled trial (RCT) is considered the gold standard method to determine the effectiveness of a drug or procedure. The ideal study would be a double blind, randomized, placebo controlled clinical trial in which neither the practitioner nor the patient would know who is getting what condition. For example, blinding implies the placebo group would receive a pill that appears identical to a ‘real’ pill, except the placebo has pharmacological ingredients. Similarly, a patient may receive an ‘exploratory’ surgery in which anesthesia is given and the skin is cut however the no further actual internal surgery occurs because the surgeon determined further internal surgery was unnecessary. Although, it is not possible to perform a double blind surgery study, the patient may be totally unaware whether an internal surgery had occurred.
Peper and Harvey (2017) point out that the positive findings of an ‘effective’ treatment are not always the results of the direct effects of medications and may be more attributable to indirect placebo responses. For example, patients may attribute the ‘effectiveness’ of the treatment to their experience of ‘non-directed’ treatment side effects that include: the post-surgical discomfort which signals to the patient that the procedure was successful, or a dry mouth and constipation that were caused by the antidepressant medication, which signals to the person that the trial medication or procedure-related medication is working (Bell, Rear, Cunningham, Dawnay, & Yellon, 2014; Stewart-Williams & Podd, 2004).
Just imagine the how pain can evoke totally different reactions. If you recently had a heart attack and then later experienced pain and cramping in the chest, you automatically may feel terrified as you could interpret the pain as another heart attack. The fear response to the pain may increase pathology and inhibit healing (a nocebo response). On the other hand, after bypass surgery, you may also experience severe pain when you move your chest. In this case, you interpret the pain as a sign that the bypass surgery was successful, which then reduces fear and reinforces the belief that you have survived a life threatening situation and will continue healing (placebo response).
Many research studies employ a placebo control, however what is less typical is a double-blind study using an ‘active’ placebo (Enck, Bingel, Schedlowski, & Rief, 2013). Less than 0.5% of all placebo studies include an active placebo group. (Shader, 2017; Jensen et al, 2017).
Unfortunately, a typical ‘placebo controlled’ study design is problematic for distinguishing the direct from any indirect (covert) placebo effects that occur within the study as shown in Figure 1.
 Figure 1. Normal (passive) placebo control group controls and experimental group. What is not assessed are placebo benefits induced by the medication/treatment induced side effects.
Figure 1. Normal (passive) placebo control group controls and experimental group. What is not assessed are placebo benefits induced by the medication/treatment induced side effects.
With a passive placebo, there is no way to know if the observed benefits are from the medication/medical procedure, or from the placebo/self-healing response triggered by the medication/medical procedure (or both combined, or neither the placebo or medical procedure). The best way to know if the treatment is actually beneficial is to use an ‘active’ placebo instead of a passive placebo.
An active placebo builds on a patient’s attributions about a medication or medical procedure. For example, a patient may be told by a clinician that feeling any side effects such as insomnia, a racing heart or, experiencing a warm flushing feeling will let them know the medication is working, so the patient becomes conditioned to expect the medication is working when they feel or experience side effects. Whereas a passive (inert) placebo such as a sugar pill will have effects that are extremely subtly felt or experienced, an active placebo will have effects that are more overtly felt or experienced. Examples of active placebos include administering low doses of caffeine or niacin that have effects which may be felt internally however which do not have the same effects as the medication. When a patient is told they may have side effects from the medication that include felt changes in heart rate or a flushing feeling, the patient attributes the changes they feel to a medication they believe will bring about benefits, even though the changes are rightfully attributed to the caffeine or niacin in the active placebo.
An active placebo triggers observed and felt body changes which do not affect the actual illness. For surgical procedures, an ‘active’ placebo control would be a sham/mock surgery in which the patient would undergo the same medical procedure (e.g. external surgery incision) without continuing some internal surgical procedure (Jonas et al, 2015). In numerous cases of accepted surgery, such as the Vineberg procedure (Vineburg & Miller, 1951) for angina, or arthroscopic knee surgery for treating osteoarthritis, the clinical benefits of a sham/mock surgery were just as successful as the actual surgery. Similar studies suggest the clinical benefits were solely (or primarily) due directly to the placebo response (Beecher, 1961; Cobb et al, 1959; Moseley et al, 2002).
To persuasively demonstrate that a treatment or therapeutic procedure is effective it should incorporate a study design using an active placebo arm as shown in Figure 2. Figure 2. Active placebo control group controls for the normal placebo benefits plus those placebo benefits induced by the medication/treatment induced side effects.
Figure 2. Active placebo control group controls for the normal placebo benefits plus those placebo benefits induced by the medication/treatment induced side effects.
Some treatments may be less effective then claimed because they were not compared to an active placebo, which could be one of the reasons why so many medical and psychological studies cannot be replicated. The absence of ‘active’ placebo controls may also be a factor explaining why some respected authorities have expressed some doubt about published scientific medical research results. Following are two quotes that illustrate such skepticism.
“Much of the scientific literature, perhaps half, may simply be untrue.” —Richard Horton, editor-in-chief of the Lancet (Horton, 2015).
“It is simply no longer possible to believe much of the clinical research that is published, or to rely on the judgment of trusted physicians or authoritative medical guidelines. I take no pleasure in this conclusion, which I reached slowly and reluctantly over my two decades as an editor of the New England Journal of Medicine” —Dr. Marcia Angell, longtime Editor in Chief of the New England Medical Journal (Angell, 2009).
There are a variety of questions to ask before agreeing on a procedure or before taking medication
A quick way to ask whether a medication or medical treatment effectiveness is the result of placebo components is to ask the following questions:
- Have there been successful self-care or behavioral approaches beyond surgical or pharmaceutical treatments that have demonstrated effectiveness? When successful treatments are reported, then questions are raised whether pharmaceutical or surgical outcomes are also attributable to the result of placebo effects. On the other hand, if there a no successful self-care approaches, then the benefits may be more due to the direct therapeutic effect of a surgical procedure or medication.
- Has the procedure been compared to an active placebo control? If not, then to what extent it is possible that the results of the surgical or pharmaceutical therapy could be attributed to a placebo response instead of directly to the medication or surgery?
- What are the long term benefits and complication rates of the medication, treatment or procedure? When benefits are low and risks of the procedure are high, explore the risks associated with ‘watchful waiting’ (Colloca, Pine, Ernst, Miller & Grillon, 2016; Thomas et al, 2014; Taleb, 2012).
Unfortunately, most clinical studies that includes pharmaceuticals and/or surgery do not test their medication, surgery against an ‘active’ placebo. Whenever possible, enquire whether an active placebo was used to determine the degree of effectiveness of the proposed treatment or procedure. Fortunately, the design of ‘active’ placebo-controlled studies is very possible for anyone interested in comparing the effectiveness of medications, treatments and procedures in various settings, from hospitals and clinics to university classrooms and individual homes.
In summary, the benefits of the treatment must significantly outweigh any risks of negative treatment side effects. Short-term treatment benefits need to be balanced by any long-term benefits. Unfortunately, short-term benefits may lead to significant, long-term harm such as in the use of some medications (e.g. sleep medications, opioid pain killers) that result in chronic dependency and which lead to a significant increase in morbidity and mortality of many kinds. We suggest that more medications and other procedures are tested against an active placebo to investigate whether the medication or procedure is actually effective.
For a detailed analysis and discussion of placebo and the importance of active placebo see our article, Peper, E. & Harvey, R. (2017). The fallacy of the placebo-controlled clinical trials: Are positive outcomes the result of “indirect” treatment effects? NeuroRegulation, 4(3–4), 102–113. http://dx.doi.org/10.15540/nr.4.3-4.102
References:
Angell M. Drug companies and doctors: A story of corruption. January 15, 2009. The New York Review of Books 56. Available: http://www.nybooks.com/articles/archives/2009/jan/15/drug-companies-doctorsa-story-of-corruption/. Accessed 24, November, 2016.
Beecher, H. K. (1961). Surgery as placebo: A quantitative study ofbias. JAMA, 176(13), 1102–1107. http://dx.doi.org/10.1001/jama.1961.63040260007008
Bell, R. M., Rear, R., Cunningham, J., Dawnay, A., & Yellon, D. M. (2014). Effect of remote ischaemic conditioning on contrast-induced nephropathy in patients undergoing elective coronary angiography (ERICCIN): rationale and study design of a randomised single-centre, double-blind placebo-controlled trial. Clinical Research in Cardiology, 103(3), 203-209. http://dx.doi.org/10.1007/s00392-013-0637-3
Cobb, L. A., Thomas, G. I., Dillard, D. H., Merendino, K. A., & Bruce, R. A. (1959). An evaluation of internal-mammary-artery ligation by a double-blind technic. New England Journal of Medicine, 260(22), 1115–1118. http://dx.doi.org/10.1056/NEJM195905282602204
Colloca, L., Pine, D. S., Ernst, M., Miller, F. G., & Grillon, C. (2016). Vasopressin boosts placebo analgesic effects in women: A randomized trial. Biological Psychiatry, 79(10), 794–802. http://dx.doi.org/10.1016/j.biopsych.2015.07.019
Derren Brown’s BBC video Fear and Faith Placebo https://www.youtube.com/watch?v=y2XHDLuBZSw
Enck, P., Bingel, U., Schedlowski, M., & Rief, W. (2013). The placebo response in medicine: minimize, maximize or personalize?. Nature reviews Drug discovery, 12(3), 191-204. http://dx.doi.org/10.1038/nrd3923
Horton, R. (2015). Offline: What is medicine’s 5 sigma. The Lancet, 385(9976), 1380. http://www.thelancet.com/pdfs/journals/lancet/PIIS0140-6736%2815%2960696-1.pdf
Jensen, J. S., Bielefeldt, A. Ø., & Hróbjartsson, A. (2017). Active placebo control groups of pharmacological interventions were rarely used but merited serious consideration: A methodological overview. Journal of Clinical Epidemiology. https://doi.org/10.1016/j.jclinepi.2017.03.001
Jonas, W. B., Crawford, C., Colloca, L., Kaptchuk, T. J., Moseley, B., Miller, F. G., & Meissner, K. (2015). To what extent are surgery and invasive procedures effective beyond a placebo response? A systematic review with meta-analysis of randomised, sham controlled trials. BMJ open, 5(12), e009655. http://dx.doi.org/10.1136/bmjopen-2015-009655
Klopfer, B., (1957). Psychological Variables in Human Cancer, Journal of Projective Techniques, 21(4), 331–340. http://www.tandfonline.com/doi/abs/10.1080/08853126.1957.10380794
Moseley, J. B., O’Malley, K., Petersen, N. J., Menke, T. J., Brody, B. A., Kuykendall, D. H., … Wray, N. P. (2002). A controlled trial of arthroscopic surgery for osteoarthritis of the knee. The New England Journal of Medicine. 347(2), 81–88. http://dx.doi.org/10.1056 /NEJMoa013259
Peper, E. & Harvey, R. (2017). The fallacy of the placebo-controlled clinical trials: Are positive outcomes the result of “indirect” treatment effects? NeuroRegulation, 4(3–4), 102–113. http://dx.doi.org/10.15540/nr.4.3-4.102
Shader, R. I. (2017). Placebos, Active Placebos, and Clinical Trials. Clinical Therapeutics, 39(3), 451–454. http://dx.doi.org/10.1016/j.clinthera.2017.02.001
Stewart-Williams, S., & Podd, J. (2004). The placebo effect: dissolving the expectancy versus conditioning debate. Psychological bulletin, 130(2), 324. http://dx.doi.org/10.1037/0033-2909.130.2.324
Taleb, N. N. (2012). Antifragile: Things that gain from disorder. Random House.
TheNNT (2017, November). http://www.thennt.com/nnt/statins-for-heart-disease-prevention-without-prior-heart-disease/
Thomas, R., Williams, M., Sharma, H., Chaudry, A., & Bellamy, P. (2014). A double-blind, placebo-controlled randomised trial evaluating the effect of a polyphenol-rich whole food supplement on PSA progression in men with prostate cancer—the UK NCRN Pomi-T study. Prostate Cancer and Prostatic Diseases, 17(2), 180–186. http://dx.doi.org/10.1038/pcan.2014.6
Vineberg, A., & Miller, G. (1951). Treatment of coronary insufficiency. Canadian Medical Association Journal, 64(3), 204. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1821866/pdf/canmedaj00654-0019.pdf
Overcoming obstacles
Posted: December 8, 2017 Filed under: self-healing, stress management, Uncategorized | Tags: deaf, healing, Inspiration, paraplegia, public speaking, singing 1 CommentIn a world with so much violence, inequalities and overwhelming negative news, it is easy to feel discouraged and forget that people can overcome trauma. Take charge of the news and images that surround us since the sounds and images impact our brain. Instead of watching disheartening and violent news before going to sleep, inspire yourself by watching the following two videos.
Muniba Mazari who at age 21 sustained spinal cord damage which left her paraplegic. She is an activist, motivational speaker and television host. https://www.youtube.com/watch?v=btb9wLkiKPE
Mandy Harvey who at age nineteen lost her hearing and is an outstanding American pop singer and songwriter. Even though she is deaf, she received Simon’s Golden Buzzer in America’s Got Talent 2017 while singing her original song. https://www.youtube.com/watch?v=ZKSWXzAnVe0
Posture and mood: implications and applications to health and therapy
Posted: November 28, 2017 Filed under: Neck and shoulder discomfort, posture, self-healing, Uncategorized | Tags: back pain, electromyography, ergonomics, neck and shoulder tension, posture, spinal alignment, stress management 7 CommentsThis blog has been reprinted from: Peper, E., Lin, I-M, & Harvey, R. (2017). Posture and mood: Implications and applications to therapy. Biofeedback.35(2), 42-48.
Slouched posture is very common and tends to increase access to helpless, hopeless, powerless and depressive thoughts as well as increased head, neck and shoulder pain. Described are five educational and clinical strategies that therapists can incorporate in their practice to encourage an upright/erect posture. These include practices to experience the negative effects of a collapsed posture as compared to an erect posture, watching YouTube video to enhance motivation, electromyography to demonstrate the effect of posture on muscle activity, ergonomic suggestions to optimize posture, the use of a wearable posture biofeedback device, and strategies to keep looking upward. When clients implement these changes, they report a more positive outlook and reduced neck and shoulder discomfort.
Background
Most people slouch without awareness when looking at their cellphone, tablet, or the computer screen (Guan et al., 2016) as shown in Figure 1. Many clients in psychotherapy and in biofeedback or neurofeedback training experience concurrent rumination and depressive thoughts with their physical symptoms. In most therapeutic sessions, clients sit in a comfortable chair, which automatically creates a posterior pelvic tilt and encourages the spine to curve so that the client sits in a slouched position. While at home, they sit on an easy chair or couch, which lets them slouch as they watch TV or surf the web.
Figure 1. (A). Employee working on his laptop. (B). Boy with ADHD being trained with neurofeedback in a clinic. (C). Student looking at cell phone. When people slouch and look at the screen, they tend to slouch and scrunch their neck.
In many cases, the collapsed position also causes people to scrunch their necks, which puts pressure on their necks that may contribute to developing headache or becoming exhausted. Repetitive strain on the neck and cervical spine may trigger a cervical neuromuscular syndrome that involves chronic neck pain, autonomic imbalance and concomitant depression and anxiety (Matsui & Fujimoto, 2011), and may contribute to vertebrobasilar insufficiency –a reduction in the blood supply to the hindbrain through the left and right vertebral arteries and basilar arteries (Kerry, Taylor, Mitchell, McCarthy, & Brew, 2008). From a biomechanical perspective, slouching also places more stress is on the cervical spine, as shown in Figure 2. When the neck compression is relieved, the symptoms decrease (Matsui & Fujimoto, 2011).
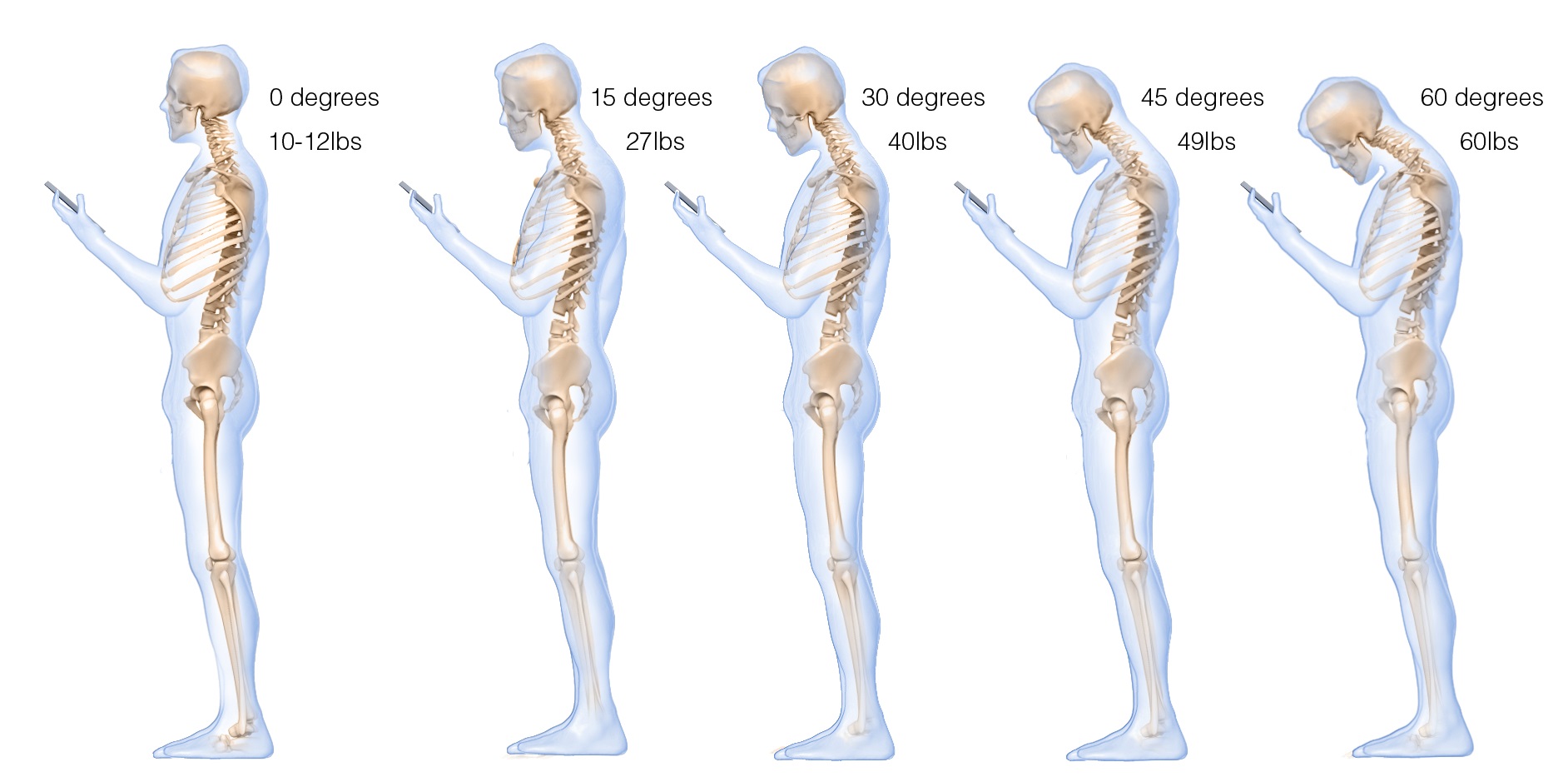 Figure 2. The more the head tilts forward, the more stress is placed on the cervical spine. Reproduced by permission from: Hansraj, K. K. (2014). Assessment of stresses in the cervical spine caused by posture and position of the head. Surgical Technology International, 25, 277–279.
Figure 2. The more the head tilts forward, the more stress is placed on the cervical spine. Reproduced by permission from: Hansraj, K. K. (2014). Assessment of stresses in the cervical spine caused by posture and position of the head. Surgical Technology International, 25, 277–279.
Most people are totally unaware of slouching positions and postures until they experience neck, shoulder, and/or back discomfort. Neither clients nor therapists are typically aware that slouching may decrease energy levels and increase the prevalence of negative (hopeless, helpless, powerless, or defeated) memories and thoughts (Peper & Lin, 2012; Peper et al, 2017)
Recommendations for posture awareness and training in treatment/education
The first step in biofeedback training and therapy is to systematically increase awareness and training of posture before attempting further bio/neurofeedback training and/or cognitive behavior therapy. If the client is sitting in a collapsed position in therapy, then it will be much more difficult for them to access positive thoughts, which interferes with further training and effective therapy. For example, research by Tsai, Peper, & Lin (2016) showed that engaging in positive thinking while slouched requires greater mental effort then when sitting erect. Sitting erect and tall contributes to elevated mood and positive thinking. An upright posture supports positive outcomes that may be akin to the beneficial effects of exercise for the treatment of depression (Schuch, Vancampfort, Richards, Rosenbaum, Ward, & Stubbs., 2016).
Most people know that posture affects health; however, they are unaware of how rapidly a slouching posture can impact their physical and mental health. We recommend the following educational and clinical strategies to teach this awareness.
- Practicing activities that raise awareness about a collapsed posture as compared to an erect posture
Guide clients through the practices so that they experience how posture can affect memory recall, physical strength, energy level, and possible triggering of headaches.
A. The effect of collapsed and erect posture on memory recall. Participants reported that it is much easier evoke powerless, hopeless, helpless, and defeated memories when sitting in a collapsed position than when sitting upright. Guide the client through the procedure described in the article, How posture affects memory recall and mood (Peper, Lin, Harvey, and Perez, 2017) and in the blog Posture affects memory recall and mood.
B. The effects of collapsed and erect posture on perceived physical strength. Participants experience much more difficulty in resisting downward pressure at the wrist of an outstretched arm when slouched rather than upright. Guide the client through the exercise described in the article, Increase strength and mood with posture (Peper, Booiman, Lin, & Harvey, 2016) and the blog, Increase strength and mood with posture.
C. The effect of slouching versus skipping on perceived energy levels. Participants experience a significant increase in subjective energy after skipping than walking slouched. Guide the client through the exercises as described in the article, Increase or decrease depression—How body postures influence your energy level (Peper & Lin, 2012).
D. The effect of neck compression to evoke head pressure and headache sensations. In our unpublished study with students and workshop participants, almost all participants who are asked to bring their head forward, then tilt the chin up and at the same time compress the neck (scrunching the neck), report that within thirty seconds they feel a pressure building up in the back of the head or the beginning of a headache. To their surprise, it may take up to 5 to 20 minutes for the discomfort to disappear. Practicing similar awareness activities can be a useful demonstration for clients with dizziness or headaches to experience how posture can increase their symptoms.
- Watching a Youtube video to enhance motivation.
Have clients watch Professor Amy Cuddy’s 2012 TED (Technology, Entertainment, and Design) Talk, Your body language shape who you are, which describes the hormonal changes that occur when adapting a upright power versus collapsed defeated posture.
- Electromyographic (EMG) feedback to demonstrate how posture affects muscle activity.
Record EMG from muscles such as around the cervical spine, trapezius, frontalis, and masseters or beneath the chin (submental lead) to demonstrate that having the head is forward and/or the neck compressed will increase EMG activity, as shown in Figure 3.

Figure 3. Electromyographic recording of the muscle under the chin while alternating between bringing the head forward or holding it back, feeling erect and tall.
The client can then learn awareness of the head and neck position. For example, one client with severe concussion experienced significant increase in head pressure and dizziness when she slouched or looked at a computer screen as well as feeling she would never get better. She then practiced the exercise of alternating her awareness by bringing her head forward and then back, and then bringing her neck back while her chin was down, thereby elongating the neck while she continued to breathe. With her head forward, she would feel her molars touching and with her neck back she felt an increase in space between the molars. When she elongated her neck in an erect position, she felt the pressure draining out of her head and her dizziness and tinnitus significantly decrease.
- Assessing ergonomics to optimize posture.
Change the seated posture of both the therapist and the client during treatment and training. Although people may be aware of their posture, it is much easier to change the external environment so that they automatically sit in a more erect power posture. Possible options include:
A. Seat insert or cushions. Sit in upright chairs that encourage an anterior pelvic tilt by having the seat pan slightly lower in the front than in the back or using a seat insert to facilitate a more erect posture (Schwanbeck, Peper, Booiman, Harvey, & Lin, 2015) as shown in Figure 4.

Figure 4. An example of how posture can be impacted covertly when one sits on a seat insert that rotates the pelvis anteriorly (The seat insert shown in the diagram and used in research is produced by BackJoy™).
B. Back cushion. Place a small pillow or rolled up towel at the kidney level so that the spine is slight arched, instead of sitting collapsed, as shown in Figure 5.
 Figure 5. An example of how a small pillow, placed between the back of the chair and the lower back, changes posture from collapsed to erect.
Figure 5. An example of how a small pillow, placed between the back of the chair and the lower back, changes posture from collapsed to erect.
C. Check ergonomic and work site computer use to ensure that the client can sit upright while working at the computer. For some, that means checking their vision if they tend to crane forward and crunch their neck to read the text. For those who work on laptops, it means using either an external keyboard, a monitor, or a laptop stand so the screen is at eye level, as shown in Figure 6.
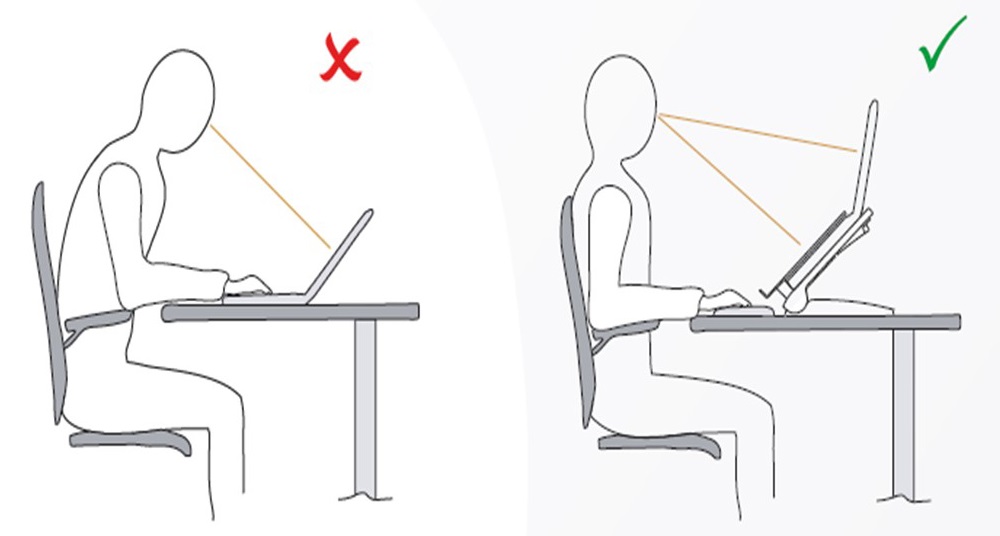 Figure 6. Posture is collapsed when working on a laptop and can be improved by using an external keyboard and monitor. Reproduced by permission from: Bakker Elkhuizen. (n.d.). Office employees are like professional athletes! (2017).
Figure 6. Posture is collapsed when working on a laptop and can be improved by using an external keyboard and monitor. Reproduced by permission from: Bakker Elkhuizen. (n.d.). Office employees are like professional athletes! (2017).
- Wearable posture biofeedback training device
The wearable biofeedback device, UpRight™, consists of a small sensor placed on the spine and works as an app on the cell phone. After calibration the erect and slouched positions, the posture device gives vibratory feedback each time the participant slouches, as shown in Figure 7.
Figure 7. Illustration of a posture feedback device, UpRight™. It provides vibratory feedback to the wearer to indicate that they are beginning to slouch.
Clinically, we have observed that clients can learn to identify conditions that are associated with slouching, such as feeling tired, thinking depressive/hopeless thoughts or other situations that evoke slouching. When people wear a posture feedback device during the day, they rapidly become aware of these subjective experiences whenever they slouch. The feedback reminds them to sit in an erect position, and they subsequently report an improvement in health (Colombo et al., 2017). For example, a 26-year-old man who works more than 8 hours a day on computer reported, “I have an improved awareness of my posture throughout my day. I also notice that I had less back pain at the end of the day.”
- Integrating posture awareness and position changes throughout the day
After clients have become aware of their posture, additional training included having them observe their posture as well and negative changes in mood, energy level or tension in their neck and head. When they become aware of these changes, they use it as a cue to slightly arch their back and look upward. If possible have the clients look outside at the tops of trees and notice details such as how the leaves and branches move. Looking at the details interrupts any ongoing rumination. At the same time, have them think of an uplifting positive memory. Then have them take another breath, wiggling, and return to the task at hand. Recommend to clients to go outside during breaks and lunchtime to look upward at the trees, the hills, or the clouds. Each time one is distracted, return to appreciate the natural patterns. This mental break concludes by reminding oneself that humans are like trees.
Trees are rooted in the earth and reach upward to the light. Despite the trauma of being buffeted by the storms, they continue to reach upward. Similarly, clouds reflect the natural beauty of the world, and are often visible in the densest city environment. The upward movement reflects our intrinsic resilience and growth. –Erik Peper
Have clients place family photos and art slightly higher on the wall at home so they automatically look upward to see the pictures. A similar strategy can be employed in the office, using art to evoke positive feelings. When clients integrate an erect posture into their daily lives, they experience a more positive outlook and reduced neck and shoulder discomfort.
Compliance with Ethical Standards:
Conflict of Interest: Author Erik Peper has received donations of 15 UpRight posture feedback devices from UpRight (http://www.uprightpose.com/) and 12 BackJoy seat inserts from Backjoy (https://www.backjoy.com) for use in research. Co-authors I-Mei Lin and Richard Harvey declare that they have no conflict of interest.
This report evaluated a convenience sample of a student classroom activity related to posture and the information was anonymous collected. As an evaluation of a classroom activity, this report of findings was exempted from Institutional Review Board oversight
References:
Bakker Elkhuizen. (n.d.). Office employees are like professional athletes! (2017). Retrieved from https://www.bakkerelkhuizen.com/knowledge-center/whitepaper-improving-work-performance-with-insights-from-pro-sports/
Cuddy, A. (2012). Your body language shapes who you are. Technology, Entertainment, and Design (TED) Talk, available at: www.ted.com/talks/amy_cuddy_your_body_language_shapes_who_you_are
We thank Frank Andrasik for his constructive comments.
Posture affects memory recall and mood
Posted: November 25, 2017 Filed under: Exercise/movement, self-healing, stress management, Uncategorized | Tags: cognitive therapy, depression, empowerment, energy, helplessness, memory, mood, posture, power posture, somatics 5 CommentsThis blog has been reprinted from: Peper, E., Lin, I-M., Harvey, R., & Perez, J. (2017). How posture affects memory recall and mood. Biofeedback, 45 (2), 36-41.
When I sat collapsed looking down, negative memories flooded me and I found it difficult to shift and think of positive memories. While sitting erect, I found it easier to think of positive memories. -Student participant
 The link between posture and mood is embedded in idiomatic phrases such as walking tall, standing proud, and an upstanding citizen, versus collapsed, defeated, or in a slump–Language suggests that posture and mood/emotions are connected. Slumped posture is commonly observed in depression (Canales et al., 2010; Michalak et al., 2009) and adapting an upright posture increases positive affect, reduces fatigue, and increases energy in people with mild to moderate depression (Wilkes et al., 2017; Peper & Lin, 2012).
The link between posture and mood is embedded in idiomatic phrases such as walking tall, standing proud, and an upstanding citizen, versus collapsed, defeated, or in a slump–Language suggests that posture and mood/emotions are connected. Slumped posture is commonly observed in depression (Canales et al., 2010; Michalak et al., 2009) and adapting an upright posture increases positive affect, reduces fatigue, and increases energy in people with mild to moderate depression (Wilkes et al., 2017; Peper & Lin, 2012).
This blog describes in detail our research study that demonstrated how posture affects memory recall (Peper et al, 2017). Our findings may explain why depression is increasing the more people use cell phones. More importantly, learning posture awareness and siting more upright at home and in the office may be an effective somatic self-healing strategy to increase positive affect and decrease depression.
Background
Most psychotherapies tend to focus on the mind component of the body-mind relationship. On the other hand, exercise and posture focus on the body component of the mind/emotion/body relationship. Physical activity in general has been demonstrated to improve mood and exercise has been successfully used to treat depression with lower recidivism rates than pharmaceuticals such as sertraline (Zoloft) (Babyak et al., 2000). Although the role of exercise as a treatment strategy for depression has been accepted, the role of posture is not commonly included in cognitive behavior therapy (CBT) or biofeedback or neurofeedback therapy.
The link between posture, emotions and cognition to counter symptoms of depression and low energy have been suggested by Wilkes et al. (2017) and Peper and Lin (2012), . Peper and Lin (2012) demonstrated that if people tried skipping rather than walking in a slouched posture, subjective energy after the exercise was significantly higher. Among the participants who had reported the highest level of depression during the last two years, there was a significant decrease of subjective energy when they walked in slouched position as compared to those who reported a low level of depression. Earlier, Wilson and Peper (2004) demonstrated that in a collapsed posture, students more easily accessed hopeless, powerless, defeated and other negative memories as compared to memories accessed in an upright position. More recently, Tsai, Peper, and Lin (2016) showed that when participants sat in a collapsed position, evoking positive thoughts required more “brain activation” (i.e. greater mental effort) compared to that required when walking in an upright position.
Even hormone levels also appear to change in a collapsed posture (Carney, Cuddy, & Yap, 2010). For example, two minutes of standing in a collapsed position significantly decreased testosterone and increased cortisol as compared to a ‘power posture,’ which significantly increased testosterone and decreased cortisol while standing. As Professor Amy Cuddy pointed out in herTechnology, Entertainment and Design (TED) talk, “By changing posture, you not only present yourself differently to the world around you, you actually change your hormones” (Cuddy, 2012). Although there appears to be controversy about the results of this study, the overall findings match mammalian behavior of dominance and submission. From my perspective, the concepts underlying Cuddy’s TED talk are correct and are reconfirmed in our research on the effect of posture. For more detail about the controversy, see the article by Susan Dominusin in the New York Times, “When the revolution came for Amy Cuddy,”, and Amy Cuddy’s response (Dominus, 2017;Singal and Dahl, 2016).
The purpose of our study is to expand on our observations with more than 3,000 students and workshop participants. We observed that body posture and position affects recall of emotional memory. Moreover, a history of self-described depression appears to affect the recall of either positive or negative memories.
Method
Subjects: 216 college students (65 males; 142 females; 9 undeclared), average age: 24.6 years (SD = 7.6) participated in a regularly planned classroom demonstration regarding the relationship between posture and mood. As an evaluation of a classroom activity, this report of findings was exempted from Institutional Review Board oversight.
Procedure
While sitting in a class, students filled out a short, anonymous questionnaire, which asked them to rate their history of depression over the last two years, their level of depression and energy at this moment, and how easy it was for them to change their moods and energy level (on a scale from 1–10). The students also rated the extent they became emotionally absorbed or “captured” by their positive or negative memory recall. Half of the students were asked to rate how they sat in front of their computer, tablet, or mobile device on a scale from 1 (sitting upright) to 10 (completely slouched).
Two different sitting postures were clearly defined for participants: slouched/collapsed and erect/upright as shown in Figure 1. To assume the collapsed position, they were asked to slouch and look down while slightly rounding the back. For the erect position, they were asked to sit upright with a slight arch in their back, while looking upward.
 Figure 1. Sitting in a collapsed position and upright position (photo by Jana Asenbrennerova). Reprinted by permission from Gorter and Peper (2011).
Figure 1. Sitting in a collapsed position and upright position (photo by Jana Asenbrennerova). Reprinted by permission from Gorter and Peper (2011).
After experiencing both postures, half the students sat in the collapsed position while the other half sat in the upright position. While in this position, they were asked to recall/evoke as many hopeless, helpless, powerless, or defeated memories as possible, one after the other, for 30 seconds.
After 30 seconds they were reminded to keep their same position and let go of thinking negative memories. They were then asked to recall/evoke only positive, optimistic, or empowering memories for 30 seconds.
They were then asked to switch positions. Those who were collapsed switched to sitting erect, and those who were erect switched to sitting collapsed. Then they were again asked to recall/evoke as many hopeless, helpless, powerless, or defeated memories as possible one after the other for 30 seconds. After 30 seconds they were reminded to keep their same position and again let go of thinking of negative memories. They were then asked to recall/evoke only positive, optimistic, or empowering memories for 30 seconds, while still retaining the second posture.
They then rated their subjective experience in recalling negative or positive memories and the degree to which they were absorbed or captured by the memories in each position, and in which position it was easier to recall positive or negative experiences.
Results
86% of the participants reported that it was easier to recall/access negative memories in the collapsed position than in the erect position, which was significantly different as determined by one-way ANOVA (F(1,430)=110.193, p < 0.01) and 87% of participants reported that it was easier to recall/access positive images in the erect position than in the collapsed position, which was significantly different as determined by one-way ANOVA (F(1,430)=173.861, p < 0.01) as shown in Figure 2.
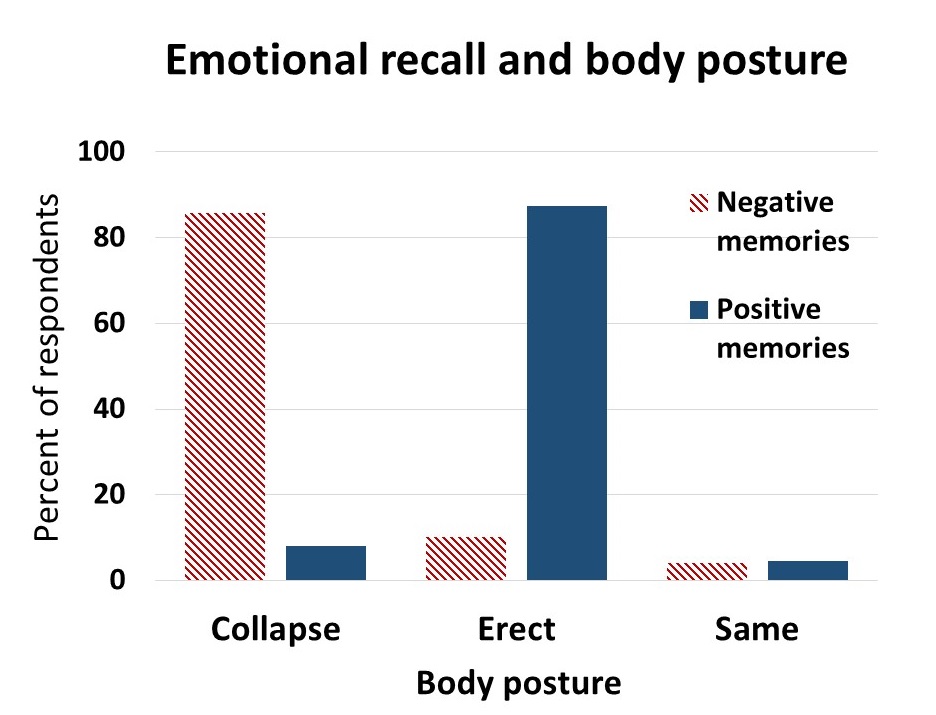 Figure 2. Percent of respondents who reported that it was easier to recall positive or negative memories in an upright or slouched posture.
Figure 2. Percent of respondents who reported that it was easier to recall positive or negative memories in an upright or slouched posture.
The difficulty or ease of recalling negative or positive memories varied depending on position as shown in Figure 3.
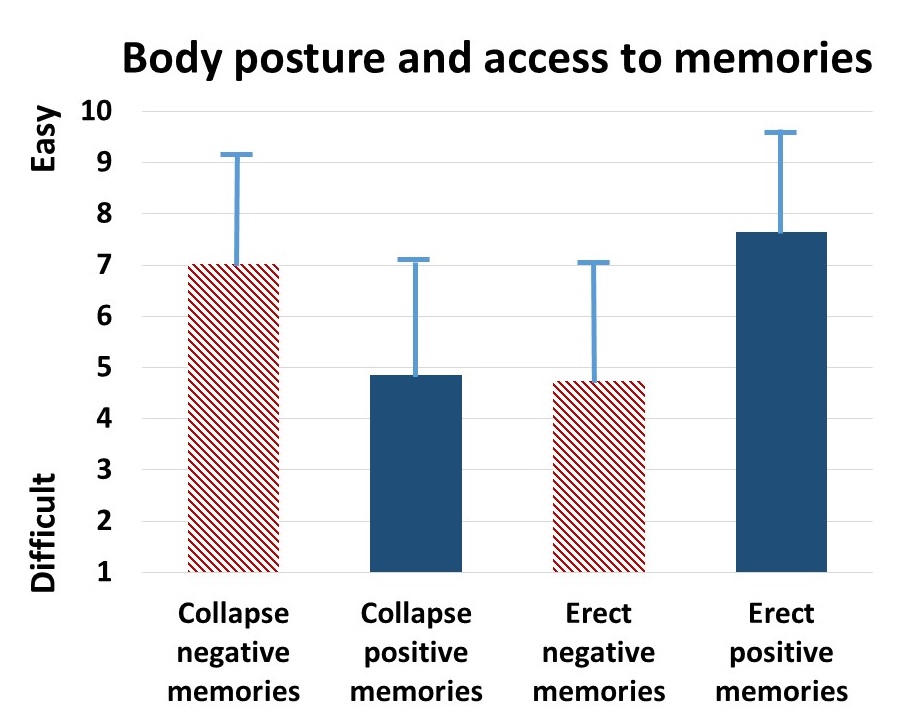 Figure 3. The relative subjective rating in the ease or difficulty of recalling negative and positive memories in collapsed and upright positions.
Figure 3. The relative subjective rating in the ease or difficulty of recalling negative and positive memories in collapsed and upright positions.
The participants with a high level of depression over the last two years (top 23% of participants who scored 7 or higher on the scale of 1–10) reported that it was significantly more difficult to change their mood from negative to positive (t(110) = 4.08, p < 0.01) than was reported by those with a low level of depression (lowest 29% of the participants who scored 3 or less on the scale of 1–10). It was significantly easier for more depressed students to recall/evoke negative memories in the collapsed posture (t(109) = 2.55, p = 0.01) and in the upright posture (t(110) = 2.41, p ≦0.05 he) and no significant difference in recalling positive memories in either posture, as shown in Figure 4.
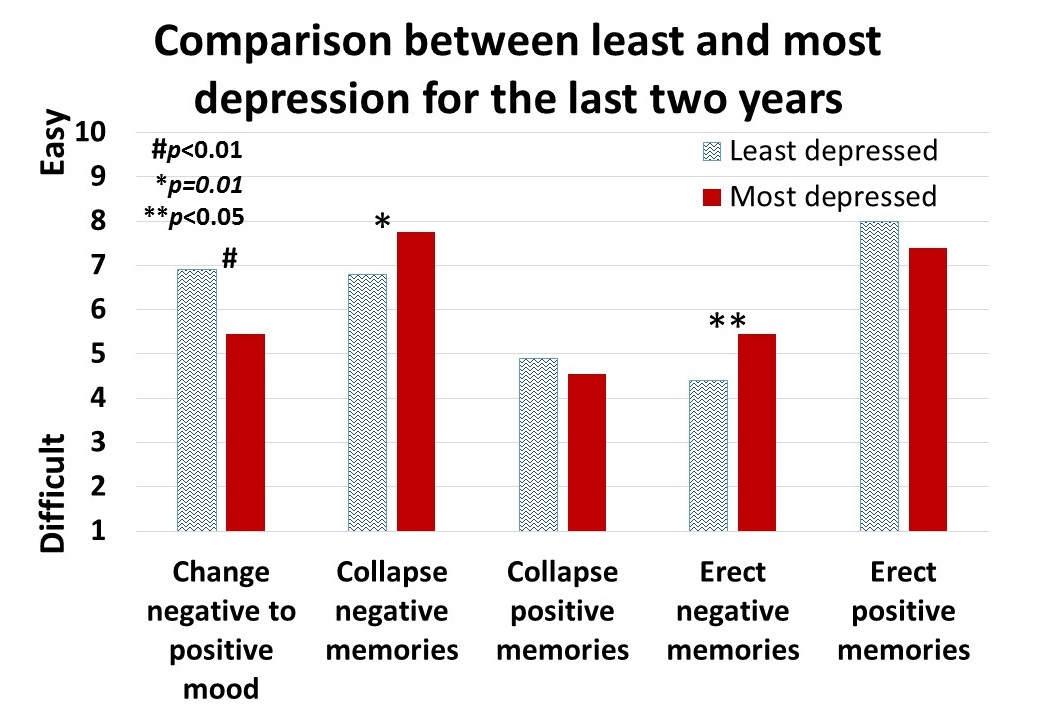 Figure 4. Differences is in memory access for participants with a history of least or most depression.
Figure 4. Differences is in memory access for participants with a history of least or most depression.
For all participants, there was a significant correlation (r = 0.4) between subjective energy level and ease with which they could change from negative to positive mood. There were no significance differences for gender in all measures except that males reported a significantly higher energy level than females (M = 5.5, SD = 3.0 and M = 4.7, SD = 3.8, respectively; t(203) = 2.78, p < 0.01).
A subset of students also had rated their posture when sitting in front of a computer or using a digital device (tablet or cell phone) on a scale from 1 (upright) to 10 (completely slouched). The students with the highest levels of depression over the last two years reporting slouching significantly more than those with the lowest level of depression over the last two years (M = 6.4, SD = 3.5 and M = 4.6, SD = 2.6; t(46) = 3.5, p < 0.01).
There were no other order effects except of accessing fewer negative memories in the collapsed posture after accessing positive memories in the erect posture (t(159)=2.7, p < 0.01). Approximately half of the students who also rated being “captured” by their positive or negative memories were significantly more captured by the negative memories in the collapsed posture than in the erect posture (t(197) = 6.8, p < 0.01) and were significantly more captured by positive memories in the erect posture than the collapsed posture (t(197) = 7.6, p < 0.01), as shown in Figure 5.
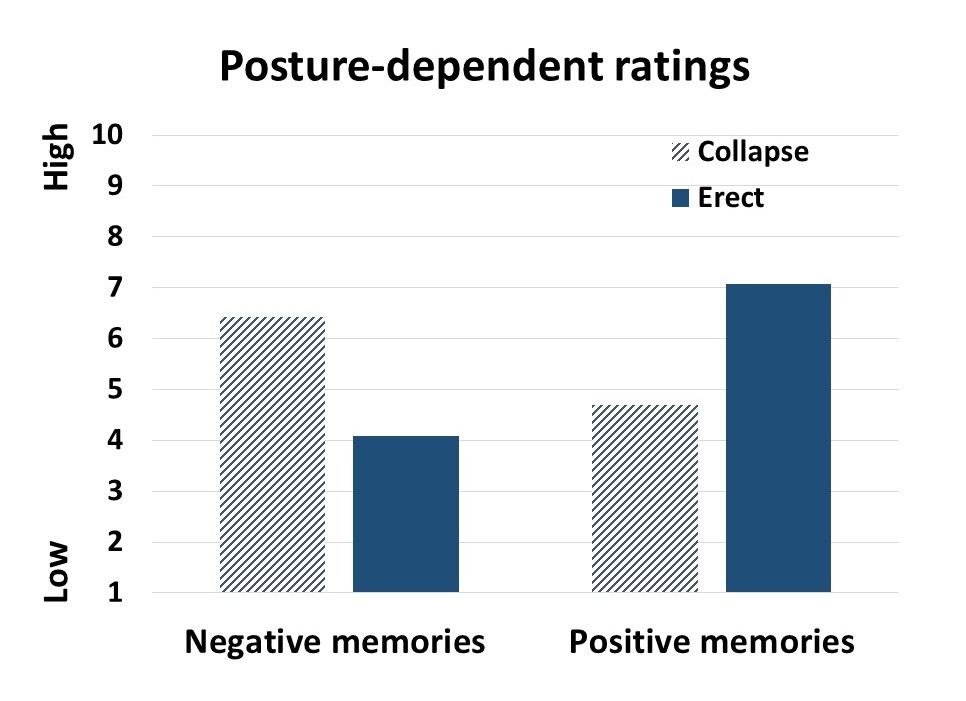 Figure 5. Subjective rating of being captured by negative and positive memories depending upon position.
Figure 5. Subjective rating of being captured by negative and positive memories depending upon position.
Discussion
Posture significantly influenced access to negative and positive memory recall and confirms the report by Wilson and Peper (2004). The collapsed/slouched position was associated with significantly easier access to negative memories. This is a useful clinical observation because ruminating on negative memories tends to decrease subjective energy and increase depressive feelings (Michi et al., 2015). When working with clients to change their cognition, especially in the treatment of depression, the posture may affect the outcome. Thus, therapists should consider posture retraining as a clinical intervention. This would include teaching clients to change their posture in the office and at home as a strategy to optimize access to positive memories and thereby reduce access or fixation on negative memories. Thus if one is in a negative mood, then slouching could maintain this negative mood while changing body posture to an erect posture, would make it easier to shift moods.
Physiologically, an erect body posture allows participants to breathe more diaphragmatically because the diaphragm has more space for descent. It is easier for participants to learn slower breathing and increased heart rate variability while sitting erect as compared to collapsed, as shown in Figure 6 (Mason et al., 2017).
 Figure 6. Effect of posture on respiratory breathing pattern and heart rate variability.
Figure 6. Effect of posture on respiratory breathing pattern and heart rate variability.
The collapsed position also tends to increase neck and shoulder symptoms This position is often observed in people who work at the computer or are constantly looking at their cell phone—a position sometimes labeled as the i-Neck.
Implication for therapy
In most biofeedback and neurofeedback training sessions, posture is not assessed and clients sit in a comfortable chair, which automatically causes a slouched position. Similarly, at home, most clients sit on an easy chair or couch, which lets them slouch as they watch TV or surf the web. Finally, most people slouch when looking at their cellphone, tablet, or the computer screen (Guan et al., 2016). They usually only become aware of slouching when they experience neck, shoulder, or back discomfort.
Clients and therapists are usually not aware that a slouched posture may decrease the client’s energy level and increase the prevalence of a negative mood. Thus, we recommend that therapists incorporate posture awareness and training to optimize access to positive imagery and increase energy.
References
Singal, J. and Dahl, M. (2016, Sept 30 ) Here Is Amy Cuddy’s Response to Critiques of Her Power-Posing Research. https://www.thecut.com/2016/09/read-amy-cuddys-response-to-power-posing-critiques.html
We thank Frank Andrasik for his constructive comments.
Breathing to improve well-being
Posted: November 17, 2017 Filed under: Breathing/respiration, Exercise/movement, Neck and shoulder discomfort, Pain/discomfort, self-healing, stress management, Uncategorized | Tags: anxiety, Breathing, health, mindfulness, pain, respiration, stress 9 CommentsBreathing affects all aspects of your life. This invited keynote, Breathing and posture: Mind-body interventions to improve health, reduce pain and discomfort, was presented at the Caribbean Active Aging Congress, October 14, Oranjestad, Aruba. www.caacaruba.com
The presentation includes numerous practices that can be rapidly adapted into daily life to improve health and well-being.
Yes, fresh organic food is better!
Posted: October 27, 2017 Filed under: Nutrition/diet, self-healing | Tags: farming, Holistic health, longevity, non-organic foods, nutrition, organic foods, pesticides 16 Comments
Is it really worthwhile to spent more money on locally grown organic fruits and vegetables than non-organic fruits and vegetables? The answer is a resounding “YES!” Organic grown foods have significantly more vitamins, antioxidants and secondary metabolites such as phenolic compounds than non-organic foods. These compounds provide protective health benefits and lower the risk of cancer, cardiovascular disease, type two diabetes, hypertension and many other chronic health conditions (Romagnolo & Selmin, 2017; Wilson et al., 2017; Oliveira et al., 2013; Surh & Na, 2008). We are what we eat–we can pay for it now and optimize our health or pay more later when our health has been compromised.
The three reasons why fresh organic food is better are:
- Fresh foods lengthen lifespan.
- Organic foods have more vitamins, minerals, antioxidants and secondary metabolites than non-organic foods.
- Organic foods reduce exposure to harmful neurotoxic and carcinogenic pesticide and herbicides residues.
Background
With the advent of chemical fertilizers farmers increased crop yields while the abundant food became less nutritious. The synthetic fertilizers do not add back all the necessary minerals and other nutrients that the plants extract from the soil while growing. Modern chemical fertilizers only replace three components–Nitrogen, Phosphorus and Potassium–of the hundred of components necessary for nutritious food. Nitrogen (N) which promotes leaf growth; Phosphorus (P which development of roots, flowers, seeds, fruit; and Potassium (K) which promotes strong stem growth, movement of water in plants, promotion of flowering and fruiting. These are great to make the larger and more abundant fruits and vegetables; however, the soil is more and more depleted of the other micro-nutrients and minerals that are necessary for the plants to produce vitamins and anti-oxidants. Our industrial farming is raping the soils for quick growth and profit while reducing the soil fertility for future generations. Organic farms have much better soils and more soil microbial activity than non-organic farm soils which have been poisoned by pesticides, herbicides, insecticides and chemical fertilizers (Mader, 2002; Gomiero et al, 2011). For a superb review of Sustainable Vs. Conventional Agriculture see the web article: https://you.stonybrook.edu/environment/sustainable-vs-conventional-agriculture/
1. Fresh young foods lengthen lifespan. Old foods may be less nutritious than young food. Recent experiments with yeast, flies and mice discovered that when these organisms were fed old versus young food (e.g., mice were diets containing the skeletal muscle of old or young deer), the organisms’ lifespan was shortened by 18% for yeast, 13% for flies, and 13% for mice (Lee et al., 2017). Organic foods such as potatoes, bananas and raisins improves fertility, enhances survival during starvation and decreases long term mortality for fruit flies(Chhabra et al, 2013). See Live longer, enhance fertility and increase stress resistance: Eat organic foods. https://peperperspective.com/2013/04/21/live-longer-enhance-fertility-and-increase-stress-resistance-eat-organic-foods/
In addition, eating lots of fruits and vegetables decreases our risk of dying from cancer and heart disease. In a superb meta-analysis of 95 studies, Dr. Dagfinn Aune from the School of Public Health, Imperial College London, found that people who ate ten portions of fruits and vegetable per day were a third less likely to die than those who ate none (Aune et al, 2017). Thus, eat lots of fresh and organic fruits and vegetables from local sources that is not aged because of transport.
2. Organic foods have more vitamins, minerals, antioxidants and secondary metabolites than non-organic foods. Numerous studies have found that fresh organic fruits and vegetables have more vitamins, minerals, antioxidants, and secondary metabolites than non-organic ones. For example, organic tomatoes contain 57 per cent more vitamin C than non-organic ones (Oliveira et al 2013) or organic milk has more beneficial polyunsaturated fats non-organic milk (Wills, 2017; Butler et al, 2011). Over the last 50 years key nutrients of fruits and vegetables have declined. In a survey of 43 crops of fruits and vegetables, Davis, Epp, & Riordan, (2004) found a significant decrease of vitamins and minerals in foods grown in the 1950s as compared to 1999 as shown in Figure 1 (Lambert, 2015).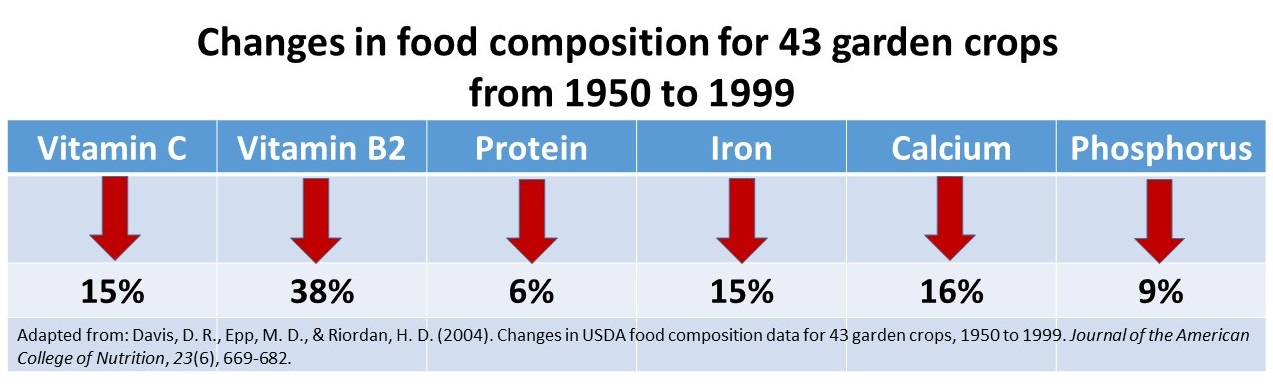
Figure 1. Change in vitamins and minerals from 1950 to 1999. From: Davis, D. R., Epp, M. D., & Riordan, H. D. (2004). Changes in USDA food composition data for 43 garden crops, 1950 to 1999. Journal of the American College of Nutrition, 23(6), 669-682.
3, Organic foods reduce exposure to harmful neurotoxic and carcinogenic pesticide and herbicides residues. Even though, the United States Department of Agriculture (USDA) and the United States Environmental Protection Agency (EPA) state that pesticide residues left in or on food are safe and non-toxic and have no health consequences, I have my doubts! Human beings accumulate pesticides just like tuna fish accumulates mercury—frequent ingesting of very low levels of pesticide and herbicide residue may result in long term harmful effects and these long term risks have not been assessed. Most pesticides are toxic chemicals and were developed to kill agricultural pests — living organisms. Remember human beings are living organisms. The actual risk for chronic low level exposure is probably unknown; since, the EPA pesticide residue limits are the result of a political compromise between scientific findings and lobbying from agricultural and chemical industries (Portney, 1992). Organic diets expose consumers to fewer pesticides associated with human disease (Forman et al, 2012).
Adopt the precautionary principle which states, that if there is a suspected risk of herbicides/pesticides causing harm to the public, or to the environment, in the absence of scientific consensus, the burden of proof that it is not harmful falls on those recommending the use of these substances (Read & O’Riordan, 2017). Thus, eat fresh locally produced organic foods to optimize health.
References
Butler, G. Stergiadis, s., Seal, C., Eyre, M., & Leifert, C. (2011). Fat composition of organic and conventional retail milk in northeast England. Journal of Dairy Science. 94(1), 24-36.http://dx.doi.org/10.3168/jds.2010-3331
Davis, D. R., Epp, M. D., & Riordan, H. D. (2004). Changes in USDA food composition data for 43 garden crops, 1950 to 1999. Journal of the American College of Nutrition, 23(6), 669-682. http://www.chelationmedicalcenter.com/!_articles/Changes%20in%20USDA%20Food%20Composition%20Data%20for%2043%20Garden%20Crops%201950%20to%201999.pdf
Lambert, C. (2015). If Food really better from the farm gate than super market shelf? New Scientist.228(3043), 33-37.
Oliveira, A.B., Moura, C.F.H., Gomes-Filho, E., Marco, C.A., Urban, L., & Miranda, M.R.A. (2013). The Impact of Organic Farming on Quality of Tomatoes Is Associated to Increased Oxidative Stress during Fruit Development. PLoS ONE, 8(2): e56354. https://doi.org/10.1371/journal.pone.0056354
Read, R. and O’Riordan, T. (2017). The Precautionary Principle Under Fire. Environment-Science and policy for sustainable development. September-October. http://www.environmentmagazine.org/Archives/Back%20Issues/2017/September-October%202017/precautionary-principle-full.html
Romagnolo, D. F. & Selmin, O.L. (2017). Mediterranean Diet and Prevention of Chronic Diseases. Nutr Today. 2017 Sep;52(5):208-222. doi: 10.1097/NT.0000000000000228. https://www.ncbi.nlm.nih.gov/pubmed/29051674
Wills, A. (2017). There is evidence organic food is more nutritious. New Scientist,3114, p53.
Wilson, L.F., Antonsson, A., Green, A.C., Jordan, S.J., Kendall, B.J., Nagle, C.M., Neale, R.E., Olsen, C.M., Webb, P.M., & Whiteman, D.C. (2017). How many cancer cases and deaths are potentially preventable? Estimates for Australia in 2013. Int J Cancer. 2017 Oct 6. doi: 10.1002/ijc.31088. https://www.ncbi.nlm.nih.gov/pubmed/28983918
Healing irritable bowel syndrome with diaphragmatic breathing*
Posted: June 23, 2017 Filed under: Breathing/respiration, self-healing | Tags: abdominal pain, diaphragmatic breathing, food intolerances, health, Holistic health, IBS, irritable bowel syndrome, pain, recurrent abdominal pain, self-care, SIBO, stress, thoracic breathing 30 CommentsErik Peper, Lauren Mason and Cindy Huey
This blog was adapted and expanded from: Peper, E., Mason, L., & Huey, C. (2017). Healing irritable bowel syndrome with diaphragmatic breathing. Biofeedback. 45(4), 83-87. DOI: 10.5298/1081-5937-45.4.04 https://biofeedbackhealth.files.wordpress.com/2018/02/a-healing-ibs-published.pdf
After having constant abdominal pain, severe cramps, and losing 15 pounds from IBS, I found myself in the hospital bed where all the doctors could offer me was morphine to reduce the pain. I searched on my smart phone for other options. I saw that abdominal breathing could help. I put my hands on my stomach and tried to expand it while I inhaled. All that happened was that my chest expanded and my stomach did not move. I practiced and practiced and finally, I could breathe lower. Within a few hours, my pain was reduced. I continued breathing this way many times. Now, two years later, I no longer have IBS and have regained 20 pounds.
– 21-year old woman who previously had severe IBS
Irritable bowel syndrome(IBS) affects between 7% to 21% of the general population and is a chronic condition. The symptoms usually include abdominal cramping, discomfort or pain, bloating, loose or frequent stools and constipation and can significantly reduce the quality of life (Chey et al, 2015). A precursor of IBS in children is called recurrent abdominal pain (RAP) which affects between 0.3 to 19% of school children (Chitkara et al, 2005). Both IBS and RAP appear to be functional illnesses, as no organic causes have been identified to explain the symptoms. In the USA, this results in more than 3.1 physician visits and 5.9 million prescriptions written annually. The total direct and indirect cost of these services exceeds $20 billion (Chey et al, 2015). Multiple factors may contribute to IBS, such as genetics, food allergies, previous treatment with antibiotics, severity of infection, psychological status and stress. More recently, changes in the intestinal and colonic microbiome resulting in small intestine bacterial overgrowth are suggested as another risk factor (Dupont, 2014).
Generally, standard medical treatments (reassurance, dietary manipulation and of pharmacological therapy) are often ineffective in reducing abdominal IBS and other abdominal symptoms (Chey et al, 2015), while complementary and alternative approaches such as relaxation and cognitive therapy are more effective than traditional medical treatment (Vlieger et, 2008). More recently, heart rate variability training to enhance sympathetic/ parasympathetic balance appears to be a successful strategy to treat functional abdominal pain (FAB) in children (Sowder et al, 2010). Sympathetic/parasympathetic balance can be enhanced by increasing heart rate variability (HRV), which occurs when a person breathes at their resonant frequency which is usually between 5-7 breaths per minute. For most people, it means breathing much slower, as slow abdominal breathing appears to be a self-control strategy to reduce symptoms of IBS, RAP and FAP.
This article describes how a young woman healed herself from IBS with slow abdominal breathing without any therapeutic coaching, reviews how slower diaphragmatic breathing (abdominal breathing) may reduce symptoms of IBS, explores the possibility that breathing is more than increasing sympathetic/parasympathetic balance, and suggests some self-care strategies to reduce the symptoms of IBS.
Healing IBS-a case report
After being diagnosed with Irritable Bowel Syndrome her Junior year of high school, doctors told Cindy her condition was incurable and could only be managed at best, although she would have it throughout her entire life. With adverse symptoms including excessive weight loss and depression, Cindy underwent monthly hospital visits and countless tests, all which resulted in doctors informing her that her physical and psychological symptoms were due to her untreatable condition known as IBS, of which no one had ever been cured. When doctors offered her what they believed to be the best option: morphine, something Cindy describes now as a “band-aid,” she was left feeling discouraged. Hopeless and alone in her hospital bed, she decided to take matters into her own hands and began to pursue other options. From her cell phone, Cindy discovered something called “diaphragmatic breathing,” a technique which involved breathing through the stomach. This strategy could help to bring warmth to the abdominal region by increasing blood flow throughout abdomen, thereby relieving discomfort of the bowel. Although suspicious of the scientific support behind this method, previous attempts at traditional western treatment had provided no benefit to recovery; therefore, she found no harm in trying. Lying back flat against the hospital bed, she relaxed her body completely, and began to breathe. Immediately, Cindy became aware that she took her breath in her chest, rather than her stomach. Pushing out all of her air, she tried again, this time gasping with inhalation. Delighted, she watched as air flooded into her stomach, causing it to rise beneath her hands, while her chest remained still. Over time, Cindy began to develop more awareness and control over her newfound strategy. While practicing, she could feel her stomach and abdomen becoming warmer. Cindy shares that for the first time in years, she felt relief from pain, causing her to cry from happiness. Later that day, she was released from the hospital, after denying any more pain medication from doctors.
Cindy continues to practice her diaphragmatic breathing as much as she can, anywhere at all, at the sign of pain or discomfort, as well as preventatively prior to what she anticipates will be a stressful situation. Since beginning her practice, Cindy says that her IBS is pretty much non-existent now. She no longer feels depressed about her situation due to her developed ability to manage her condition. Overall, she is much happier. Moreover, since this time two years ago, Cindy has gained approximately 20 pounds, which she attributes to eating a lot more. In regard to her success, she believes it was her drive, motivation, and willingness to dedicate herself fully to the breathing practice which allowed for her to develop skills and prosper. Although it was not natural for her to breathe in her stomach at first, a trait which she says she often recognizes in others, Cindy explains it was due to necessity which caused her to shift her previously-ingrained way of breathing. Upon publicly sharing her story with others for the first time, Cindy reflects on her past, revealing that she experienced shame for a long time as she felt that she had a weird condition, related to abnormal functions, which no one ever talks about. On the experience of speaking out, she affirms that it was very empowering, and hopes to encourage others coping with a situation similar to hers that there is in fact hope for the future. Cindy continues to feel empowered, confident, and happy after taking control of her own body, and acknowledges that her condition is a part of her, something of which she is proud.
Watch the in-depth interview with Cindy Huey in which she describes her experience of discovering diaphragmatic breathing and how she used this to heal herself of IBS
Video 1. Interview with Cindy Huey describing how she healed herself from IBS.
Background perspective
“Why should the body digest food or repair itself, when it will be someone else’s lunch” (paraphrased from Sapolsky (2004), Why zebras do not get ulcers).
From an evolutionary perspective, we were prey and needed to be on guard (vigilant) to the presence of predators. In the long forgotten past, the predators were tigers, snakes, and the carnivore for whom we were food as well as other people. Today, the same physiological response pathways are still operating, except that the pathways are now more likely to be activated by time urgency, work and family conflict, negative mental rehearsal and self-judgment. This is reflected in the common colloquial phrases: “It makes me sick to my stomach,” “I have no stomach for it,” “He is gutless,” “It makes me queasy,” “Butterflies in my stomach,” “Don’t get your bowels in uproar,” “Gut feelings’, or “Scared shitless.”
Whether conscious or unconscious, when threatened, our body reacts with a fight/flight/freeze response in which the blood flow is diverted from the abdomen to deep muscles used for propulsion. This results in peristalsis being reduced. At the same time the abdomen tends to brace to protect it from injury. In almost all cases, the breathing patterns shift to thoracic breathing with limited abdominal movement. As the breathing pattern is predominantly in the chest, the person increases the risk of hyperventilation because the body is ready to run or fight.
In our clinical observations, people with IBS, small intestine bacterial overgrowth (SIBO), abdominal discomfort, anxiety and panic, and abdominal pain tend to breathe more in their chest, and when asked to take breathe, they tend to inhale in their upper chest with little or no abdominal displacement. Almost anyone who experiences abdominal pain tends to hold the abdomen rigid as if the splinting could reduce the pain. A similar phenomenon is observed with female students experiencing menstrual cramps. They tend to curl up to protect themselves and breathe shallowly in their chest instead of slowly in their abdomen, a body pattern which triggers a defense reaction and inhibits regeneration. If instead they breathe slowly and uncurl they report a significant decrease in discomfort (Gibney & Peper, 2003).
Paradoxically, this protective stance of bracing the abdomen and breathing shallowly in the chest increases breathing rate and reduces heart rate variability. It reduces and inhibits blood and lymph flow through the abdomen as the defensive posture evokes the physiology of fight/flight/freeze. The reduction in venous blood and lymph flow occurs because the ongoing compression and expansion in the abdomen is inhibited by the thoracic breathing and, moreover, the inhibition of diaphragmatic breathing. It also inhibits peristalsis and digestion. No wonder so many of the people with IBS report that they are reactive to some foods. If the GI track has reduced blood flow and reduced peristalsis, it may be less able to digest foods which would affect the bacteria in the small intestine and colon. We wonder if a risk factor that contributes to SIBO is chronic lack of abdominal movement and bracing.
Slow diaphragmatic abdominal breathing to establish health
“Digestion and regeneration occurs when the person feels safe.”
Effortless, slow diaphragmatic breathing occurs when the diaphragm descends and pushes the abdominal content downward during inhalation, which causes the abdomen to become bigger. As the abdomen expands, the pelvic floor relaxes and descends. During exhalation, the pelvic floor muscles tighten slightly, lifting the pelvic floor and the transverse and oblique abdominal muscles contract and push the abdominal content upward against the diaphragm, allowing the diaphragm to relax and go upward, pushing the air out. The following video, 3D view of the diaphragm, from www.3D-Yoga.com by illustrates the movement of the diaphragm.
Video 2. 3D view of diaphragm by sohambliss from www.3D-Yoga.com,
This expansion and constriction of the abdomen occurs most easily if the person is extended, whether sitting or standing erect or lying down, and the waist is not constricted. If the arches forward in a protected pattern and the spine is flexed in a c shape, it would compress the abdomen; instead, the body is long and the abdomen can move and expand during inhalation as the diaphragm descends (see figure 1). If the person holds their abdomen tight or it is constricted by clothing or a belt, it cannot expand during inhalation. Abdominal breathing occurs more easily when the person feels safe and expanded versus unsafe or fearful and collapsed or constricted.

Figure 1. Erect versus collapsed posture note that there is less space for the abdomen to expand in the protective collapsed position. Reproduced by permission from: Clinical Somatics (http://www.clinicalsomatics.ie/
When a person breathes slower and lower it encourages blood and lymph flow through the abdomen. As the person continues to practice slower, lower breathing, it reduces the arousal and vigilance. This is the opposite state of the flight, fight, freeze response so that blood flow is increased in abdomen, and peristalsis re-occurs. When the person practices slow exhalation and breathing and they slightly tighten the oblique and transverse abdominal muscles as well as the pelvic floor and allow these muscles to relax during inhalation. When they breathe in this pattern effortless they, they often will experience an increase in abdominal warmth and an initiation of abdominal sounds (stomach rumble or borborygmus) which indicates that peristalsis has begun to move food through the intestines (Peper et al., 2016). For a detailed description see https://peperperspective.com/2016/04/26/allow-natural-breathing-with-abdominal-muscle-biofeedback-1-2/
What can you do to reduce IBS
There are many factors that cause and effect IBS, some of which we have control over and some which are our out of our control, such as genetics. The purpose of proposed suggestions is to focus on those things over which you have control and reduce risk factors that negatively affect the gastrointestinal track. Generally, begin by integrating self-healing strategies that promote health which have no negative side effects before agreeing to do more aggressive pharmaceutical or even surgical interventions which could have negative side effects. Along the way, work collaboratively with your health care provider. Experiment with the following:
- Avoid food and drinks that may irritate the gastrointestinal tract. These include coffee, hot spices, dairy products, wheat and many others. If you are not sure whether you are reacting to a food or drink, keep a detailed log of what you eat and drink and how you feel. Do self-experimentation by eating or drinking the specific food by itself as the first food in the morning. Then observe how you feel in the next two hours. If possible, eat only organic foods that have not been contaminated by herbicides and pesticides (see: https://peperperspective.com/2015/01/11/are-herbicides-a-cause-for-allergies-immune-incompetence-and-adhd/).
- Identify and resolve stressors, conflicts and problems that negatively affect you and drain your energy. Keep a log to identify situations that drain or increase your subjective energy. Then do problem solving to reduce those situations that drain your energy and increase those situations that increase your energy. For a detailed description of the practice see https://peperperspective.com/2012/12/09/increase-energy-gains-decrease-energy-drains/
Often the most challenging situations that we cannot stomach are those where we feel defeated, helpless, hopeless and powerless or situations where we feel threatened– we do not feel safe. Reach out to other both friends and social services to explore how these situations can be resolved. In some cases, there is nothing that can be done except to accept what is and go on.
- Feel safe. As long as we feel unsafe, we have to be vigilant and are stressed which affects the GI track. Explore the following:
- What does safety mean for you?
- What causes you to feel unsafe from the past or the present?
- What do you need to feel safe?
- Who can offer support that you feel safe?
Reflect on these questions and then explore and implement ways by which you can create feeling more safe.
- Take breaks to regenerate. During the day, at work and at home, monitor yourself. Are you pushing yourself to complete tasks. In a 24/7 world with many ongoing responsibilities, we are unknowingly vigilant and do not allow ourselves to rest and relax to regenerate. Do not wait till you feel tired or exhausted. Stop earlier and take a short break. The break can be a short walk, a cup of tea or soup, or looking outside at a tree. During this break, think about positive events that have happened or people who love you and for whom you feel love. When you smile and think of someone who loves you, such as a grandparent, you may relax and for that moment as you feel safe which allows regeneration to begin.
- Observe how you inhale. Take a deep breath. If you feel you are moving upward and becoming a little bit taller, your breathing is wrong. Put one hand on your lower abdomen and the other on your chest and take a deep breath. If you observe your chest lifted upward and stomach did not expand, your breathing is wrong. You are not breathing diaphragmatically. Watch the following video, The correct way to breathe in, on how to observe your breathing and how to breathe diaphragmatically.
- Learn diaphragmatic breathing. Take time to practice diaphragmatic breathing. Practice while lying down and sitting or standing. Let the breathing rate slow down to about six breaths per minute. Exhale to the count of four and then let it trail off for two more counts, and inhale to the count of three and let it trail for another count. Practice this sitting and lying down (for more details on breathing see: https://peperperspective.com/2014/09/11/a-breath-of-fresh-air-improve-health-with-breathing/.
- Sitting position. Exhale by feeling your abdomen coming inward slightly for the count of four and trailing off for the count of two, then allow the lower ribs to widen, abdomen expand–the whole a trunk expands–as you inhale while the shoulders stay relaxed for a count of three. Allow it to trail off for one more count before you again begin to exhale. Be gentle, do not rush or force yourself. Practice this slower breathing for five minutes. Focus more on the exhalation and allowing the air to just flow in. Give yourself time during the transition between inhalation and exhalation.
- Lying down position. While lying on your back, place a two to five-pound weight such as a bag of rice on your stomach as shown in Figure 2.

Figure 2. Lying down and practicing breathing with two to five-pound weight on stomach (reproduced by permission from Gorter and Peper, 2011.
As you inhale push the weight upward and also feel your lower ribs widen. Then allow exhalation to occur by the weight pushing the abdominal content down which pushes the diaphragm upward. This causing the breath to flow out. As you exhale, imagine the air flowing out through your legs as if there were straws inside your legs. When your attention wanders, smile and bring it back to imagining the air flowing down your legs during exhalation. Practice this for twenty minutes. Many people report that during the practice the gurgling in their abdomen occurs which is a sign that peristalsis and healing is returning.
- Observe and change your breathing during the day. Observe your breathing pattern during the day. Each time you hold your breath, gasp or breathe in your chest, interrupt the pattern and substitute slow diaphragmatic breathing for the next five breaths. Do this the whole day long. Many people observe that when they think of stressor or are worried, they hold their breath or shallow breathe in the chest. If this occurs, acknowledge the worry and focus on changing your breathing. This does not mean that you dismiss the concern, instead for this moment you focus on breathing and then explore ways to solve the problem.
If you observed that under specific circumstance you held your breath or breathed shallowly in your chest, then whenever you anticipate that the same event will occur again, begin to breathe diaphragmatically. To do this consistently is very challenging and most people report that initially they only seem to breathe incorrectly. It takes practice, practice and practice—mindful practice– to change. Yet those who continue to practice often report a decrease in symptoms and feel more energy and improved quality of life.
Summary
Changing habitual health behaviors such as diet and breathing can be remarkably challenging; however, it is possible. Give yourself enough time, and practice it many times until it becomes automatic. It is no different from learning to play a musical instrument or mastering a sport. Initially, it feels impossible, and with lot of practice it becomes more and more automatic. We continue to be impressed that healing is possible. Among our students at San Francisco State University, who practice their self-healing skills for five weeks, approximately 80% report a significant improvement in their health (Peper et al., 2014).
* This blog was adapted and expanded from: Peper, E., Mason, L., & Huey, C. (2017). Healing irritable bowel syndrome with diaphragmatic breathing. Biofeedback. 45(4), 83-87. DOI: 10.5298/1081-5937-45.4.04 https://biofeedbackhealth.files.wordpress.com/2018/02/a-healing-ibs-published.pdf
References
Chey, W. D., Kurlander, J., & Eswaran, S. (2015). Irritable bowel syndrome: a clinical review. Jama, 313(9), 949-958.
Chitkara, D. K., Rawat, D. J., & Talley, N. J. (2005). The epidemiology of childhood recurrent abdominal pain in Western countries: a systematic review. American journal of Gastroenterology, 100(8), 1868-1875.
Dupont, H. L. (2014). Review article: evidence for the role of gut microbiota in irritable bowel syndrome and its potential influence on therapeutic targets. Alimentary pharmacology & therapeutics, 39(10), 1033-1042.
Gibney, H.K. & Peper, E. (2003). Taking control: Strategies to reduce hot flashes and premenstrual mood swings. Biofeedback, 31(3), 20-24.
Gorter, R. & Peper, E. (2011). Fighting Cancer-A NonToxic Approach to Treatment. Berkeley: North Atlantic.
Peper, E., Booiman, A., Lin, I-M, Harvey, R., & Mitose, J. (2016). Abdominal SEMG Feedback for Diaphragmatic Breathing: A Methodological Note. Biofeedback. 44(1), 42-49.
Peper, E., Lin, I-M, Harvey, R., Gilbert, M., Gubbala, P., Ratkovich, A., & Fletcher, F. (2014). Transforming chained behaviors: Case studies of overcoming smoking, eczema and hair pulling (trichotillomania). Biofeedback, 42(4), 154-160.
Sapolsky, R. (2004). Why Zebras Don’t Get Ulcers. New York: Owl Books
Sowder, E., Gevirtz, R., Shapiro, W., & Ebert, C. (2010). Restoration of vagal tone: a possible mechanism for functional abdominal pain. Applied psychophysiology and biofeedback, 35(3), 199-206.
Vlieger, A. M., Blink, M., Tromp, E., & Benninga, M. A. (2008). Use of complementary and alternative medicine by pediatric patients with functional and organic gastrointestinal diseases: results from a multicenter survey. Pediatrics, 122(2), e446-e451.
Freeing the neck and shoulders*
Posted: April 6, 2017 Filed under: Neck and shoulder discomfort, self-healing, Uncategorized | Tags: computer, flexibility, Holistic health, neck pain, relaxation, repetitive strain injurey, shoulder pain, somatic practices, stress 5 CommentsStress, incorrect posture, poor vision and not knowing how to relax may all contribute to neck and shoulder tension. More than 30% of all adults experience neck pain and 45% of girls and 19% of boys 18 year old, report back, neck and shoulder pain (Cohen, 2015; Côté, Cassidy, & Carroll, 2003; Hakala, Rimpelä, Salminen, Virtanen, & Rimpelä, 2002). Shoulder pain affects almost a quarter of adults in the Australian community (Hill et al, 2010). Most employees working at the computer experience neck and shoulder tenderness and pain (Brandt et al, 2014), more than 33% of European workers complained of back-ache (The European Agency for Safety and Health at Work, 2004), more than 25% of Europeans experience work-related neck-shoulder pain, and 15% experience work-related arm pain (Blatter & De Kraker, 2005; Eijckelhof et al, 2013), and more than 90% of college students report some muscular discomfort at the end of the semester especially if they work on the computer (Peper & Harvey, 2008).
The stiffness in the neck and shoulders or the escalating headache at the end of the day may be the result of craning the head more and more forward or concentrating too long on the computer screen. Or, we are unaware that we unknowingly tighten muscles not necessary for the task performance—for example, hunching our shoulders or holding our breath. This misdirected effort is usually unconscious, and unfortunately, can lead to fatigue, soreness, and a buildup of additional muscle tension.
The stiffness in the neck and shoulders or the escalating headache at the end of the day may be the result of craning the head more and more forward or concentrating too long on the computer screen. Poor posture or compromised vision can contribute to discomfort; however, in many cases stress is major factor. Tightening the neck and shoulders is a protective biological response to danger. Danger that for thousands of years ago evoke a biological defense reaction so that we could run from or fight from the predator. The predator is now symbolic, a deadline to meet, having hurry up sickness with too many things to do, anticipating a conflict with your partner or co-worker, worrying how your child is doing in school, or struggling to have enough money to pay for the rent.
Mind-set also plays a role. When we’re anxious, angry, or frustrated most of us tighten the muscles at the back of the neck. We can also experience this when insecure, afraid or worrying about what will happen next. Although this is a normal pattern, anticipating the worst can make us stressed. Thus, implement self-care strategies to prevent the occurrence of discomfort.
What can you do to free up the neck and shoulder?
Become aware what factors precede the neck and shoulder tension. For a week monitor yourself, keep a log during the day and observe what situations occur that precede the neck and should discomfort. If the situation is mainly caused by:
- Immobility while sitting and being captured by the screen. Interrupt sitting every 15 to 20 minutes and move such as walking around while swinging your arms.
- Ergonomic factors such as looking down at the computer or laptop screen while working. Change your work environment to optimize the ergonomics such as using a detached keyboard and raising the laptop screen so that the top of the screen is at eyebrow level.
- Emotional factors. Learn strategies to let go of the negative emotions and do problem solving. Take a slow deep breath and as you exhale imagine the stressor to flow out and away from you. Be willing to explore and change ask yourself: “What do I have to have to lose to change?”, “Who or what is that pain in my neck?”, or “What am I protecting by being so rigid?”
Regardless of the cause, explore the following five relaxation and stretching exercises to free up the neck and shoulders. Be gentle, do not force and stop if your discomfort increases. When moving, continue to breathe.
1. WIGGLE. Wiggle and shake your body many times during the day. The movements can be done surreptitiously such as, moving your feet back and forth in circles or tapping feet to the beat of your favorite music, slightly arching or curling your spine, sifting the weight on your buttock from one to the other, dropping your hands along your side while moving and rotating your fingers and wrists, rotating your head and neck in small unpredictable circles, or gently bouncing your shoulders up and down as if you are giggling. Every ten minutes, wiggle to facilitate blood flow and muscle relaxation.
2. SHAKE AND BOUNCE. Stand up, bend your knees slightly, and let your arms hang along your trunk. Gently bounce your body up and down by bending and straightening your knees. Allow the whole body to shake and move for about one minute like a raggedy Ann doll. Then stop bouncing and alternately reach up with your hand and arm to the ceiling and then let the arm drop. Be sure to continue to breathe.
3. ROTATION MOVEMENT (Adapted from the work by Sue Wilson and reproduced by permission from: Gorter, R. & Peper, E. (2011). Fighting Cancer- A Nontoxic Approach to Treatment).
Pre-assessment: Stand up and give yourself enough space, so that when you lift your arms to shoulder level and rotate, you don’t touch anything. Continue to stand in the same spot during the exercise as shown in figures 1a and 1b.
Lift your arms and hold them out, so that they are at shoulder level, positioned like airplane wings. Gently rotate your arms to the left as far as you can without discomfort. Look along your left arm to your fingertips and beyond to a spot on the wall and remember that spot. Rotate back to center and drop your arms to your sides and relax.
 Figures 1a and 1b. Rotating the arms as far as is comfortable (photos by Jana Asenbrennerova)
Figures 1a and 1b. Rotating the arms as far as is comfortable (photos by Jana Asenbrennerova)
Movement practice. Again, lift your arms to the side so that they are like airplane wings pointing to the left and right. Gently rotate your trunk, keeping your arms fixed at a right angle to your body. Rotate your arms to the right and turn your head to the left. Then reverse the direction and rotate your arms in a fixed position to the left and turn your head to the right. Do not try to stretch or push yourself. Repeat the sequence three times in each direction and then drop your arms to your sides and relax.
With your arms at your sides, lift your shoulders toward your ears while you keep your neck relaxed. Feel the tension in your shoulders, and hold your shoulder up for five seconds. Let your shoulders drop and relax. Then relax even more. Stay relaxed for ten seconds.
Repeat this sequence, lifting, dropping, and relaxing your shoulders two more times. Remember to keep breathing; and each time you drop your shoulders, relax even more after they have dropped.
Repeat the same sequence, but this time, very slowly lift your shoulders so that it takes five seconds to raise them to your ears while you continue to breathe. Keep relaxing your neck and feel the tension just in your shoulders. Then hold the tension for a count of three. Now relax your shoulders very slowly so that it takes five seconds to lower them. Once they are lowered, relax them even more and stay relaxed for five seconds. Repeat this sequence two more times.
Now raise your shoulders quickly toward your ears, feel the tension in your upper shoulders, and hold it for the count of five. Let the tension go and relax. Just let your shoulders drop. Relax, and then relax even more.
Post-assessment. Lift your arms up to the side so that they are at shoulder level and are positioned like airplane wings. Gently rotate without discomfort to the left as far as you can while you look along your left arm to your fingers and beyond to a spot on the wall.
Almost everyone reports that when they rotate the last time, they rotated significantly further than the first time. The increased flexibility is the result of loosening your shoulder muscles.
4. TAPPING FEET (adapted from the work of Servaas Mes)
Diagonal movements underlie human coordination and if your coordination is in sync, this will happen as a reflex without thought. There are many examples of these basic reflexes, all based on diagonal coordination such as arm and leg movement while walking. To restore this coordination, we use exercises that emphasize diagonal movements. This will help you reverse unnecessary tension and use your body more efficiently and thereby reducing “sensory motor amnesia” and dysponesis (Hanna, 2004). Remember to do the practices without straining, with a sense of freedom, while you continue relaxed breathing. If you feel pain, you have gone too far, and you’ll want to ease up a bit. This practice offers brief, simple practices to avoid and reverse dysfunctional patterns of bracing and tension and reduce discomfort. Practicing healthy patterns of movement can reestablish normal tone and reduce tension and pain. This is a light series of movements that involve tapping your feet and turning your head. You’ll be able to do the entire exercise in less than twenty seconds.
Pre-assessment. Sit erect at the edge of the chair with your hands on your lap and your feet shoulders’ width apart, with your heels beneath your knees.
First, notice your flexibility by gently rotating your head to the right as far as you can. Now look at a spot on the wall as a measure of how far you can comfortably turn your head and remember that spot. Then rotate back to the center.
Practicing rotating feet and head. Become familiar with the feet movement, lift the balls of your feet so your feet are resting on your heels. Lightly pivot the balls of your feet to the right, tap the floor, and then stop and relax your feet for just a second. Now lift the balls of your feet, pivot your feet to the left, tap, relax, and pivot back to the right.
Just let your knees follow the movement naturally. This is a series of ten light, quick, relaxed pivoting movements—each pivot and tap takes only about one or two seconds.
Add head rotation. Turn your head in the opposite direction of your feet. This series of movements provides effortless stretches that you can do in less than half a minute as shown in figures 2a and 2b.
 Figures 2a and 2b. Rotating the feet and head in opposite directions (photos by Gary Palmer)
Figures 2a and 2b. Rotating the feet and head in opposite directions (photos by Gary Palmer)
When you’re facing right, move your feet to the left and lightly tap. Then face left and move your feet to the right and tap.
- Continue the tapping movement, but each time pivot your head in the opposite direction. Don’t try to stretch or force the movement.
- Do this sequence ten times. Now stop, face straight head, relax your legs, and just keep breathing.
Post assessment. Rotate your head to the right as far as you can see and look at a spot on the wall. Notice how much more flexibility/rotation you have achieved.
Almost everyone reports being able to rotate significantly farther after the exercise than before. They also report that they have less stiffness in their neck and shoulders.
5. SHOULDER AWARENESS PRACTICE. Sit comfortably with your hands on your lap. Allow your jaw to hang loose and breathe diaphragmatically. Continue to breathe slowly as you do the following:
- Shrug, raising your shoulders towards your ears to 70% of maximum effort and hold them up for about 10 seconds (note the sensations of tension).
- Let your shoulders drop and relax for 10 to 20 seconds
- Shrug, raising your shoulders towards your ears to 50% of maximum effort and hold them up for about 10 seconds (note the sensations of tension).
- Let your shoulders drop and relax for 10 to 20 seconds
- Shrug, raising your shoulders towards your ears to 25% of maximum effort and hold them up for about 10 seconds (note the sensations of tension).
- Let your shoulders drop and relax for 10 to 20 seconds
- Shrug, raising your shoulders towards ears to 5% of maximum effort and hold them up for about 10 seconds (note the sensations of tension).
- Let your shoulders drop and relax for 10 to 20 seconds
- Pull your shoulders down to 25% of maximum effort and hold them up for about 10 seconds (note the sensations of tension).
- Allow your shoulders to come back up and relax for 10 to 20 seconds
Remember to relax your shoulders completely after each incremental tightening. If you tend to hold your breath while raising your shoulders, gently exhale and continue to breathe. When you return to work, check in occasionally with your shoulders and ask yourself if you can feel any of the sensations of tension. If so, drop your shoulders and relax for a few seconds before resuming your tasks.
In summary, when employees and students change their environment and integrate many movements during the day, they report a significant decrease in neck and shoulder discomfort and an increase in energy and health. As one employee reported, after taking many short movement breaks while working at the computer, that he no longer felt tired at the end of the day, “Now, there is life after five”.
To explore how prevent and reverse the automatic somatic stress reactions, read Thomas Hanna‘s book, Somatics: Reawakening The Mind’s Control of Movement, Flexibility, and Health. For easy to do neck and shoulder guided instructions stretches, see the following ebsite: http://greatist.com/move/stretches-for-tight-shoulders
References:
Blatter, B. M., & Kraker, H. D. (2005). Prevalentiecijfers van RSI-klachten en het vóórkomen van risicofactoren in 15 Europese landen. Tijdschrift voor gezondheidswetenschappen, 1, 83, 8-15.
Côté, P., Cassidy, J. D., & Carroll, L. (2003). The epidemiology of neck pain: what we have learned from our population-based studies. The Journal of the Canadian Chiropractic Association, 47(4), 284. http://www.pain-initiative-un.org/doc-
European Agency for Safety and Health at Work (2004). http://europa.eu.int/comm/employment_social/news/2004/nov/musculoskeletaldisorders_en.html
Paoli, P., Merllié, D., & Fundação Europeia para a Melhoria das Condições de Vida e de Trabalho. (2001). Troisième enquête européenne sur les conditions de travail, 2000.
*I thank Sue Wilson and Servaas Mes for teaching me these somatic practices.
