Corporations: The new(old) disease vectors as they choose profits over health
Posted: February 24, 2026 Filed under: Breathing/respiration, cancer, health | Tags: cancer, environment, environmental toxins, food, health, herbicides, investigative reporting, nutrition, pollution, public health, smoking, wellness 1 Comment
“We can invest in preventing illness now by reducing our exposure to environmental toxins — or we can pay a far higher price later trying to treat the resulting chronic and often debilitating diseases.”
Ever since the 1962 publication of Rachel Carson’s groundbreaking book, Silent Spring, which documented the harm environmental pollution caused, government has, often reluctantly, set limits intended to protect Americans from exposure to harmful chemicals in our food, air and water (Carson, 1964). These regulations did not emerge easily. As the governmental regulations were being proposed and implemented, they were consistently challenged by the very large corporations that manufactured and profited from these chemicals.
History reminds us how slowly public health protections can unfold. Consider how long it took for smoking to be prohibited in public spaces even though the harmful effects had been documented since the 1950s (Doll and Hill, 1954; Doll & Hill, 1964; Wynder & Graham,1985). For decades, the science was clear, yet policy and governmental actions were delayed. Only in the early 2000s did many states began banning smoking in workplaces, restaurants, and bars. The shift in public policy saved many lives and the reduction in smoking has been the major reason for the decrease in cancer mortality over the last twenty-five years.
We are going backwards
The Trump administration has rescinded the 2009 U.S. Environmental Protection Agency endangerment finding on greenhouse gases, loosening vehicle emission standards, and weakening pollution controls on power plants and oil and gas operations (Tabuchi, 2026). The health consequences may not appear immediately; however, they are predictable. The increased exposure today will again contribute to increased rates of cancer, respiratory illness, cardiovascular disease, and developmental disorders tomorrow.
To understand how the government regulations have been revised so that once again Americans will be more exposed to toxins in their food, air, and water, read the superb investigative report published by U.S. Right to Know whose mission is to pursuing truth and transparency for public health.
Their most recent report, Tracing Bayer’s ties to power in Trump’s Washington, describes in detail the hidden social connections, lobbying and political donations that lead “The White House to invokes the Defense Production Act to guarantee supplies of elemental phosphorus and glyphosate-based herbicides. Regulators reapprove dicamba, a Bayer herbicide twice blocked by federal courts, and clear the way for new pesticides containing toxic, persistent PFAS “forever” chemicals (Malkan, 2026).“
When regulatory safeguards weaken, corporations can once again function as disease vectors-not through infection, but through environmental exposure. By loosening the pollution standards, federal policy will negatively affect the health of both present and future generations.
I encourage you to explore many superb investigative reports and practical suggestions how to avoid these toxins exposure that are available on U.S. Right to Know website:
One exposure. Twenty generations later, the damage is still unfolding
Glyphosate: Cancer, liver disease, endocrine disruption and other health concerns
Big Food ‘transparency’ campaign seeks to block tough new food safety laws
Ultra-processed foods damage health in ways that calories don’t explain, new study says
See also the following blogs
References
Carson, R. (1962). Silent spring. Houghton Mifflin. https://www.amazon.com/Silent-Spring-Rachel-Carson/dp/B002E8JF6G/
Doll, R., & Hill, A. B. (1954). The mortality of doctors in relation to their smoking habits: A preliminary report. British Medical Journal, 1(4877), 1451–1455. https://doi.org/10.1136/bmj.1.4877.1451
Doll, R., & Hill, A. B. (1964). Mortality in relation to smoking: Ten years’ observations of British doctors. British Medical Journal, 1(5396), 1460–1467. https://doi.org/10.1136/bmj.1.5396.1460
Malkan, S. (2026). Tracing Bayer’s ties to power in Trump’s Washington. U.S. Right to Know. Accessed February 24, 2026. https://usrtk.org/pesticides/tracing-bayers-ties-to-power-in-trumps-washington/
Tabuchi, H. (2026). Historic Climate Rollback Makes U.S. a Global Outlier on Tailpipe Rules. The New York Times, February 16, 2026. Accessed February 24, 2026 https://www.nytimes.com/2026/02/16/climate/endangerment-finding-auto-emissions-regulations.html
Wynder, E.L., & Graham, A. (1985). JAMA, 253 (20), 2986-2994. https://doi.org/10.1001/jama.1985.03350440064033
Fever can save your life
Posted: March 22, 2025 Filed under: attention, cancer, health, Pain/discomfort, Uncategorized | Tags: acetaminophen, books, classical conditioning, fever, food, immune response, lifestyle, mental-health, self-care, travel 3 CommentsErik Peper, PhD and Robert Gorter, MD, PhD
Adapted from: Peper, E. & Gorter, R. (2025). Fever can save your life. Townsend Letter-Innovative Health Perspective. Published March 27, 2025. https://townsendletter.com/fever-can-save-your-life/

My child’s fever was 102 F° and I was worried. I made my daughter comfortable, gave her some liquids and applied a lemon wrap around the calves. Fifteen minutes later the fever was down by a degree and a half to 100.5 F.° I continue to check how my child was doing. I touched her forehead and noted that it became slightly cooler. By the next day the fever had broken, and my daughter felt much better.
Most people are worried when they or their children have a fever, as it may indicates an illness. They quickly rush to take a Tylenol or other medications to reduce the fever and discomfort. We question whether this almost automatic response to inhibit fever is the best approach. It is important to note that fever is seldom the cause of illness; instead, fever is the body’s response to support healing by activating the immune system so that it can fight the infection. In most cases, the fever may last for a day or two and then disappears. Watchful waiting does not mean, not seeking medical help. It means careful monitoring so that the fever does not go too high versus automatically taking medications to suppress the fever.
Although fever can be uncomfortable, in most casest is not something to be feared. Rather than suppressing it, allow the fever to run its course, as fevers can improve clinical outcomes. Research findings indicate that individuals who experience an increase in body temperature (i.e., a fever) have higher survival rates following infection (Repasky et al., 2013). Spontaneous remissions of cancer—altogether a rarer event—have been observed repeatedly in connection with febrile infectious diseases, especially those of bacterial origin (Kienle, 2012). Late in 19th and early 20th century, Prof Coley observed that in patients who had wound fever or fevers that were induced by injecting bacterial toxins, their cancer sometimes disappeared (Kienle, 2012). In the early 20th century, inducing fever with injecting a bacterial toxin became an acceptable and somewhat successful treatment strategy for treating cancer (Karamanou, et al., 2013; Kendell et al, 1969). It was even a fairly successful treatment for neuro-syphilis before advent of antibiotics. Malaria-induced fevers were used as a treatment for neurosyphilis from the 1920s until the 1950s,—the spiking fevers associated with malaria killed the bacteria that caused the syphilitic infection (Gambino, 2015). The fever therapy slowly disappeared as antibiotics (penicillin), chemotherapy and radiation tended to be more effective.
Although suppressing fever with medication may make you feel more comfortable, and in some cases allow a child to go to day care, it may be harmful. Dr. Schulman and colleagues at the University of Miami Leonard M. Miller School of Medicine demonstrated in a randomized controlled study that, among similar patients admitted to the ICU, the risk of death was seven times higher for those who received fever-reducing medication compared to those who did not (Schulman et al., 2005).(Schulman et al., 2005).
Fever reducing medication may in rare cases lead to complications. For example, aspirin may cause stomach irritation and ulcers as well as being cofactor in Reye’s syndrome (Temple, 1981; Schrör 2007). While acetaminophen (also known as paracetamol), often given to young children, may increase the risk of allergic rhinitis and possibly asthma by the age of six (Caballero, et al., 2015; McBride, 2011). As McBride point out, there appears to be a correlation between acetaminophen use and asthma across all groups, ages and location. This correlation even holds up for mothers who took acetaminophen during pregnancy as their children have increased risk for asthma by age six.
As Bauer and colleagues (Bauer et al., 2021) point out: “Paracetamol (N-acetyl-p-aminophenol (APAP), otherwise known as acetaminophen) is the active ingredient in more than 600 medications (Excedrine) used to relieve mild to moderate pain and reduce fever. Research suggests that prenatal exposure to APAP might alter fetal development, which could increase the risks of some neurodevelopmental, reproductive and urogenital disorders. Pregnant women should be cautioned at the beginning of pregnancy to: forego APAP unless its use is medically indicated. This Consensus Statement reflects our concerns and is currently supported by 91 scientists, clinicians and public health professionals from across the globe.”
Finally, we wonder whether active fever suppression during childhood might condition the immune system not to initiate a fever response through the process of classical conditioning, thereby reducing the immune system’s overall competence. This could be a contributing factor to the increasing rates of allergies, immune disorders, and the earlier onset of certain cancers (Gorter & Peper, 2011). Specifically, if a person begins to develop a fever and medication was used to reduce it, over time the fever response may become automatically inhibited through covert classical conditioning.
Simple home remedy when having a fever?
- Practice watchful waiting. This means monitoring the person and only use medication to reduce fever if necessary. When in doubt contact your physician. Remember, in almost all cases, fever is not the illness; it is the body’s response to fight the illness and regain health.
- Hydrate. When having a fever, we perspire and need more fluids. Thus, increase fluid intake. Almost all cultural traditions recommend drinking some fluids such as hot water with lemon juice and honey, chicken soup broth, etc.
- Reframe the experience as a healing experience versus an illness experience. For example, when a fever, reframe it possitively such as, I feel pleased that my body is responding and I trust that my body is fighting the illness well (or even better).
- Implement the following gentle self-care approaches (Schirm, 2018).
Lemon wrap around calves or feet may help reduce fevers by using the cooling properties of lemon and evaporating water. How to make lemon wraps:
• Fill a bowl with water that’s 2–3° C below your fever temperature.
• Add 1–2 lemon halves.
• Score the lemon peel with a knife to release essential oils.
• Mash the lemons in the water.
• Soak a cloth in the lemon water.
• Wrap the cloth around your calves from ankle to knee.
• Cover with a blanket and rest for 10–15 minutes.
• Repeat as needed.
“Tips for using lemon wraps
• Change the wraps when they become warm.
• If your feet get cold, stop using the wraps.
• Don’t over-bundle a child with blankets, as babies can’t regulate their body temperatures as well as adults.
The information in this blog is designed for educational purposes only and is not intended to be a substitute for informed medical advice or care. This information should not be used to diagnose or treat any health problems or illnesses without consulting a doctor. Consult with a health care practitioner before relying on any information in this article or on this website.
References
Bauer, A.Z., Swan, S.H., Kriebel, D. et al. Paracetamol use during pregnancy — a call for precautionary action. Nat Rev Endocrinol (2021). https://doi.org/10.1038/s41574-021-00553-7
Caballero, N., Welch, K. C., Carpenter, P. S., Mehrotra, S., O’Connell, T. F., & Foecking, E. M. (2015). Association between chronic acetaminophen exposure and allergic rhinitis in a rat model. Allergy & rhinology (Providence, R.I.), 6(3), 162–167. https://doi.org/10.2500/ar.2015.6.0131
Gambino, M. (2015). Fevered Decisions: Race, Ethics, and Clinical Vulnerability in the Malarial Treatment of Neurosyphilis, 1922-1953. Hastings Center Report. https://doi.org/10.1002/hast.451
Gorter, R. & Peper, E. (2011). Fighting Cancer: A Nontoxic Approach to Treatment. Berkeley, CA: North Atlantic Books. https://www.amazon.com/Fighting-Cancer-Nontoxic-Approach-Treatment/dp/1583942483
Karamanou, M., Liappas, I., Antoniou, C.h, Androutsos, G., & Lykouras, E. (2013). Julius Wagner-Jauregg (1857-1940): Introducing fever therapy in the treatment of neurosyphilis. Psychiatrike = Psychiatriki, 24(3), 208–212. https://pubmed.ncbi.nlm.nih.gov/24185088/
Kendell, H. W., Rose, D. L., & Simpson, W. M. (1969). Fever therapy technique in syphilis and gonococcic infections. Archives of physical medicine and rehabilitation, 50(10), 603–608. https://pubmed.ncbi.nlm.nih.gov/4981888/
Kienle G. S. (2012). Fever in Cancer Treatment: Coley’s Therapy and Epidemiologic Observations. Global advances in health and medicine, 1(1), 92–100. https://doi.org/10.7453/gahmj.2012.1.1.016
McBride, J.T. (2011). The Association of Acetaminophen and Asthma Prevalence and Severity. Pediatrics, 128(6), 1181–1185. https://doi.org/10.1542/peds.2011-1106
Repasky, E. A., Evans, S. S., & Dewhirst, M. W. (2013). Temperature matters! And why it should matter to tumor immunologists. Cancer immunology research, 1(4), 210–216. https://doi.org/10.1158/2326-6066.CIR-13-0118
Schirm, J. (2018). Essentials of homecare-A gentle approach to healing. Holistic Essence. https://www.amazon.com/Essentials-Home-Care-II-Approach/dp/0692121250
Schulman, C. I., Namias, N., Doherty, J., Manning, R. J., Li, P., Elhaddad, A., Lasko, D., Amortegui, J., Dy, C. J., Dlugasch, L., Baracco, G., & Cohn, S. M. (2005). The effect of antipyretic therapy upon outcomes in critically ill patients: a randomized, prospective study. Surgical infections, 6(4), 369–375. https://doi.org/10.1089/sur.2005.6.369
Schrör K. (2007). Aspirin and Reye syndrome: a review of the evidence. Paediatric drugs, 9(3), 195–204. https://doi.org/10.2165/00148581-200709030-00008
Temple, A.R. (1981). Acute and Chronic Effects of Aspirin Toxicity and Their Treatment. Arch Intern Med, 141(3), 364–369. https://doi.org/10.1001/archinte.1981.00340030096017
Use the power of your mind to transform health and aging
Posted: February 18, 2025 Filed under: attention, behavior, cancer, CBT, cognitive behavior therapy, COVID, education, health, meditation, mindfulness, Pain/discomfort, placebo, stress management, Uncategorized | Tags: health, imimune function, longevity, mental-health, mind-body, nutrition, Reframing, wellness Leave a commentMost of the time when I drive or commute by BART, I listen to podcasts (e.g., Freakonomics, Hidden Brain, this podcast will kill you, Science VS, Huberman Lab). although many of the podcasts are highly informative; , rarely do I think that everyone could benefit from it. The recent podcast, Using your mind to control your health and longevity, is an exception. In this podcast, neuroscientist Andrew Huberman interviews Professor Ellen Langer. Although it is three hours and twenty-two minute long, every minute is worth it (just skip the advertisements by Huberman which interrupts the flow). Dr. Langer delves into how our thoughts, perceptions, and mindfulness practices can profoundly influence our physical well-being.
She presents compelling evidence that our mental states are intricately linked to our physical health. She discusses how our perceptions of time and control can significantly impact healing rates, hormonal balance, immune function, and overall longevity. By reframing our understanding of mindfulness—not merely as a meditative practice but as an active, moment-to-moment engagement with our environment—we can harness our mental faculties to foster better health outcomes. The episode also highlights practical applications of Dr. Langer’s research, offering insights into how adopting a mindful approach to daily life can lead to remarkable health benefits. By noticing new things and embracing uncertainty, individuals can break free from mindless routines, reduce stress, and enhance their overall quality of life. This podcast is a must-listen for anyone interested in the profound connection between mind and body. It provides valuable tools and perspectives for those seeking to take an active role in their health and well-being through the power of mindful thinking. It will change your perspective and improve your health. Listen to or watch the interview:
Youtube: https://www.youtube.com/watch?v=QYAgf_lfio4

Useful blogs to reduce stress
Rethink the monies spent on cancer screening tests
Posted: November 24, 2023 Filed under: behavior, cancer, Evolutionary perspective, healing, health, Nutrition/diet, self-healing | Tags: breast canceer, Cancer screening, environmental toxins, immune competence, Life style, lifestyle modification, mammography, organic foods, overdiagnosis 3 CommentsErik Peper, PhD and Richard Harvey, PhD

Adapted from: Peper, E. & Harvey, R. (2024). Rethinking the monies spent on cancer screening tests. Townsend e-Letter, Townsend Letters. The Examiner of Alternative Medicine, May 18, 2024. https://www.townsendletter.com/e-letter-34-are-we-reducing-cancer-or-just-looking-for-it/
Abstract
While cancer screening tests are commonly promoted for early detection and treatment, evidence increasingly suggests that widespread screening of asymptomatic individuals may not significantly extend lifespan and could contribute to overdiagnosis, overtreatment, and harm. Although billions are spent annually on screenings—$40 billion for colon, $15 billion for breast, and $4 billion for prostate cancer—some of these money might be more effectively invested in lifestyle interventions that reduce cancer risk and improve longevity. Meta-analyses indicate that only sigmoidoscopy for colorectal cancer shows a clear benefit in extending life, while other common screenings (e.g., mammography, PSA, FOBT) show minimal or no effect on overall mortality. Interestingly, breast cancer mortality declines have occurred in similarly European countries that delayed screening implementation as compared to countries that started screen earlier. This suggests that other contributing factors such as improved lifestyle, nutrition, and environmental changes may be the major factor in the reduction of breast cancer. We recommend shifting from profit-driven, generalized screening toward personalized, risk-adjusted methods using multi-omics technology and preventative lifestyle patterns. More critically, the focus should be prevention through diet, physical activity, stress management, sleep hygiene, environmental protections, and social support; since, it is estimated that 70 percent of all cancers are related to diet and environmental factors. Thus, resources need to be allocated toward empowering individuals and communities to adopt health-promoting behaviors and thereby reduce cancer incidence.
Keywords: cancer screening, overdiagnosis, lifestyle modification, preventive health,
immune competence
Cancer screening tests are based upon the rational that early detection of fatal cancers enables earlier and more effective treatments (Kowalski, 2021), however, there is some controversy. Early screening may increase the risk of over diagnosis, treating false positives (people who did not have the cancer but the test indicates they have cancer) and potentially fatal treatment of cancers that would never progress to increase morbidity or mortality (Kowalski, 2021).
Today about $40 billion spent on colon cancer screening, $15 billion spent on breast cancer screening, and $4 billion spent on prostate cancer screening annually (CSPH, 2021). A question is raised whether the billions and billions of dollars spent on screening asymptomatic participants would be more wisely spent on promoting and supporting life style changes that reduce cancer risks and actually extend life span? That cancer screening is expensive does not mean no one should be screened. Instead, the argument is that the majority of healthcare dollars could be spent on health promotion practices and reserving screening for those people who are at highest risk for developing cancers.
What is the evidence that screening prolongs life?
Cancer screening tests appear correlated with preventing deaths since deaths due to cancers in the USA have decreased by about 28% from 1999 to 2020 (CDC, 2023a). Although cancer causes many of the deaths in the USA, overall life expectancy has increased by less than 1% from 1999 to 2020. If cancer screening were more effective, the life expectancy should have increased more because cancer is the second leading cause of death (CDC, 2023b). Consider also that deaths due to cancers may be coincident and or comorbid with other circumstances. For example, during the last four years, overall life expectancy in the USA has precipitously declined in part due to other causes of death such as the COVID pandemic and opioid overdose epidemic (Lewis, 2022). Decline in life expectancy in the USA has many contributing factors, including the ‘harms’ associated with cancer screening procedures. For example, perforations during colon cancer screening can lead to internal bleeding, or complications related to surgeries, radiotherapies or chemotherapies. Bretthauer et al., (2023) commented: “A cancer screening test may reduce cancer-specific mortality but fail to increase longevity if the harms for some individuals outweigh the benefits for others or if cancer-specific deaths are replaced by deaths from competing cause” (p. 1197).
Bretthauer et al. (2023) conducted a systematic review and meta-analysis of 18 long-term randomized clinical trials involving 2.1 million Individuals with more than nine years of follow-up reporting on all-cause mortality. They reported that“…this meta-analysis suggest that current evidence does not substantiate the claim that common cancer screening tests save lives by extending lifetime, except possibly for colorectal cancer screening with sigmoidoscopy.”
Following is a summary of Bretthauer et al. (2023) findings:
- The only cancer screening with a significant lifetime gain (approximately 3 months) was sigmoidoscopy.
- There was no significant difference between harms of screening and benefits of screening for:
- mammography
- prostate cancer screening
- FOBT (fecal occult blood test) screening every year or every other year
- lung cancer screening Pap test cytology for cervical cancer screening, no randomized clinical trials with cancer-specific or all-cause mortality end points and long term follow-up were identified.
Potential for loss or harm (e.g., iatrogenic and nosocomial) versus potential for benefit and extended life
More than 35 years ago a significant decrease in breast cancer mortality was observed after mammography was implemented. The correlation suggested a causal relationship that screening reduced mortality (Fracheboud, 2004). This correlation made logical sense since the breast cancer screening test identified cancers early which could then be treated and thereby would result in a decrease in mortality.
How much money is spent on screening that may correlate with unintended harms?
The annual total expenditure for cancer screening is estimated to be between $40-$50 billion annually (CSPH, 2021). Below are some of the estimated expenditures for common tests other than colorectal cancer screening, which arguably is costly; however, has potential benefits that outweigh potential harms.
- $10.37-13.94 billion for mammography to screen 50% of eligible women (Badal et al, 2023).
- $2-4 billion for prostate cancer (Ma et al., 2014)
- $1-2 billion for lung cancer (Taylor et al., 2022)
What is the correlation between initiation of mammography and decrease in breast cancer mortality?
The conclusion that mammography reduced breast cancer mortality was based upon studies without control groups; however, this relationship could be causal or synchronistic. The ambiguity of correlation or causation was resolved with the use of natural experimental control groups. Some European countries began screening 10 years earlier than other countries. Using statistical techniques such as propensity score matching when comparing the data from countries that initiated mammography screening early (Netherlands, Sweden and Northern Ireland) to countries that started screening 10 year later (Belgium, Norway and Republic of Ireland), the effectiveness of screening could be compared.
The comparisons showed no difference in the decrease of breast cancer mortality in countries that initiated breast cancer screening early or late. For example, there was no difference in the decrease of breast cancer mortality rates of women who lived in the Netherlands that started screening early versus those who lived in Belgium that began screening 10 years later, as is shown Figure 1 (Autier et al, 2011).

Figure 1. No difference in age adjust breast cancer mortality between the two adjacent countries even though breast cancer screening began ten years earlier in the Netherlands than in Belgium (graph reproduced from Autier et al, 2011).
The observations are similar when comparing neighboring countries: Sweden (early screening) to Norway (late screening) as well as Northern Ireland, UK (early screening) compared to the Republic of Ireland (late screening). The systematic comparisons showed that screening did not account for the decrease in breast cancer mortality. To what extent could the decrease in mortality be related to other factors such as better prenatal and early childhood diet and life style, improved nutrition, reduction in environmental pollutants, and other unidentified life style and environmental factors which improve immune competence?
A simplistic model to reduce the risk of cancers is described in the following equation (Gorter & Peper, 2011).

Cancer risk can be reduced, arguably by influencing risk factors that contribute to cancers as well as increasing factors to enhance immune competence. In the simple model above, ‘Cancer burden’ refers to the set of exposures that increase the odds of cancer formations. Categories include exposures to oncoviruses, environmental exposures (e.g., ionizing radiation, carcinogenic chemicals) as well as genetic (e.g., chromosomal aberrations, replication errors) and epigenetic factors (e.g., lifestyle categories related to eating, exercising, sleeping, and relaxing). In the model above, ‘Immune competence’ refers to a set of categories of immune functioning related to DNA repair, orderly cell death (i.e., processes of apoptosis), expected autophagy, as well as ‘metabolic rewiring,’ also called cellular energetics, that would allow the body to be able to reduce manage cancers from progressing (Fouad & Aanei, 2017) .
How do we examine the cancer burden/immune competence relationship?
Schmutzler et al., (2022) have suggested personalized and precision-medicine risk-adjusted cancer screening incorporating “… high-throughput “multi-omics” technologies comprising, among others, genomics, transcriptomics, and proteomics, which have led to the discovery of new molecular risk factors that seem to interact with each other and with non-genetic risk factors in a multiplicative manner.” The argument is that ‘profit-centered’ medicine could incorporate ‘multi-omics’ into risk-adjusted cancer screening as a way to reduce potential loss or harm due to other cancer screening procedures. Rather than simply screening for cancers using currently invasive or toxic procedures which may do more harm than good, consider more nuanced screening tests aimed at the so-called ‘hallmarks of cancer?’ For example, Hanahan (2022) suggests some technical targets for the multi-omics technologies. The following are some of the precision screening tests possible topersonalized medicine of 14 factors or processes related to:
- cells evading growth suppression
- non-mutational epigenetic reprogramming
- avoiding immune destruction
- enabling replicative immortality
- tumor-promoting inflammation
- polymorphic microbiomes
- activating invasion and metastasis
- inducing or accessing vasculature formation/angiogenesis
- cellular senescence
- genome instability and mutation
- resisting cell death
- deregulating cellular metabolism
- unlocking phenotypic plasticity
- sustaining proliferative signaling
Of the listed categories above, ‘phenotypic plasticity’ (cf. Feinberg, 2007; Gupta et al., 2019) suggests that lifestyle behaviors and environmental exposures play a role in cancer progression and regression.
Lifestyle and environmental factors can contribute to the development of cancers.
The 2008-2009 report from the President’s Cancer Panel appraised the National Cancer Program in accordance with the National Cancer Act of 1971 stated (Reuben, 2010):
“We have grossly underestimated the link between environmental toxins, plastics, chemicals, and cancer risk. It is estimated that 70 percent of all cancers were related to diet and environment “
Multiple research studies have shown that a healthy life style pattern is associated with decreased cancer risks and increased longevity. Lifestyle factors that have been documented to increase cancer risks in the United Kingdom (UK) as shown in figure 2.

Figure 2. Percentages of cancer cases in the UK attributable to different exposures. Adapted from Brown et al., 2018 and reproduced by permission from Key et al., 2020.
Similar findings have been reported by Song et al. (2016) from the long term follow-up of 126901 adult health care professionals. People who never smoked, drank no alcohol or moderate alcohol (< 1 drink/d for women; < 2 drinks/d for men}, had a body-mass index (BMI) of at least 18.5 but lower than 27.5, did weekly aerobic physical activity of at least 75 vigorous-intensity minutes or 150 150 moderate-intensity minutes compared to those who smoked, drank, had high BMI and did not exercise had nearly half the cancer death rate. Song et al (2016) concludes:
“…about 20% to 40% of carcinoma cases and about half of carcinoma deaths can be potentially prevented through lifestyle modification. Not surprisingly, these figures increased to 40% to 70% when assessed with regard to the population of US whites which has a much worse lifestyle pattern than other cohorts. Notably, approximately 80% to 90% of lung cancer deaths can be avoided if Americans adopted the lifestyle of the low-risk group, mainly by quitting smoking. For other cancers, a range of 10% to 70% of deaths can be prevented. These results provide strong support for the importance of environmental factors in cancer risk and reinforce the enormous potential of primary prevention for cancer control.”
Said another way, primary prevention should remain a priority for cancer control.
Given that many cancers are related to diet, environment and lifestyle, it is estimated that 50% of all cancers and cancer deaths could be prevented by modifying personal behavior. Thus, the monies spent on screening or even developing new treatments could better be spent on prevention along with implementing programs that promote a healthier environment, diet and personal behavior (AACR, 2011).
What can be done? Addressing systems not symptoms
From a ‘systems perspective,’ the first step is to reduce the cancer burden and carcinogenic agents that occur in our environment such environmental pollution (Turner et al., 2022). In many cases, governmental regulations that reduce cancer risk factors have been weakened, delayed, and contested for years through industry’s lobbying. It often takes more than 30 years after risk factors have been observed and documented before government regulations are successfully implemented, as exemplified in the battle over tobacco or, air pollution regulations related to particulates from burning fossil fuels (Stratton et al, 2001).
Sadly, we cannot depend upon governments or industries to implement regulations known to reduce cancer risks. More within our control is implementing lifestyle changes that enhance immune competence and promote health.
Implement a healthy life style that enhances immune competence and, supports health and well-being
Paraphrasing a trope of what some physicians may state: ‘Take two pills, and call me in the morning. Oh, and eat well, exercise, and get good rest.’ Broadly stated, the following are some controllable lifestyle behaviors that can decrease cancer risks and promotes health. Implementing environmental and lifestyle changes are very challenging because they are highly related to socio economic factors, cultural factors, industry push for profits over health, and self-care challenges since there are no immediate results experienced by behavior and lifestyle changes.
In many cases, the effects of harmful life-style and environment factors are only observed twenty or more years later (e.g., diabetes, lung cancer, cirrhosis of the liver). The individual does not experience immediate benefits of lifestyle changes thus it is more challenging to know that your healthy life style has an effect. The process is even more complex because in most cases it is not a single factor but the interaction of multiple factors (genetics, lifestyle, and environment). The complexity of causality so often conflicts with the simplistic research studies to identify only one isolated risk factor. Instead of waiting for the definitive governmental guidelines and regulations, adopt a ‘precautionary principle’ which means do not take an action when there is uncertainty about its potential harm (Goldstein, 2001). Do not wait for screening; instead, take charge of your health and implement as many of the following behaviors and strategies to enhance immune competence and thereby reduce cancer risks.
Eat organic foods, especially vegetable and fruits.
Many studies have suggested that eating organic foods and in particular more fruits and vegetable such as a Mediterranean diet is associated with increased health and longevity. Similarly, people who eat do not eat highly-processed or ultra-processed foods have better health status (Van Tulleken, 2023). For example, In the large prospective study of 68, 946 participants, adults who consumed the most organic fruits, vegetables, dairy products, meat and other foods had 25% fewer cancers when compared with adults who never ate organic food (Baudry et al., 2018; Rabin, 2018). Similarly, many studies have reported that those who adhere consistently to a Mediterranean diet have a significantly lower incidence of chronic diseases (such as cardiovascular diseases, diabetes, etc.) and cancers compared to those who do not adhere to a Mediterranean diet (Mentella et al., 2019).
Reduce environmental pollution exposure
Air pollution and the exposure to airborne carcinogens are a significant risk factor for cancers as illustrated by the increased cancer rates among smokers. In the USA, the reduction of smoking has significantly decreased the lung cancer deaths (US Department of Health and Human Services, 2014).
Increase movement and exercise
Many studies have documented that people who exercise regularly and are otherwise non–sedentary but are active their entire lives have the lowest risk for breast cancers and colon cancers. Women who exercise 3 hours a week or more have a 30-40% lower risk of developing breast cancer (NIH NCI, 2023). The NIH National Cancer Institute summary concludes that exercises also significantly benefited the following cancer survivors (NIH NCI, 2023):
- Breast cancer: In a 2019 systematic review and meta-analysis of observational studies, breast cancer survivors who were the most physically active had a 42% lower risk of death from any cause and a 40% lower risk of death from breast cancer than those who were the least physically active (Spei et al, 2019).
- Colorectal cancer: Evidence from multiple epidemiologic studies suggests that physical activity after a colorectal cancer diagnosis is associated with a 30% lower risk of death from colorectal cancer and a 38% lower risk of death from any cause (Patel et al., 2019).
- Prostate cancer: Limited evidence from a few epidemiologic studies suggests that physical activity after a prostate cancer diagnosis is associated with a 33% lower risk of death from prostate cancer and a 45% lower risk of death from any cause ((Patel et al., 2019).
- Implement stress management.
Chronic stress may reduce immune competence and increase the risk of cancers as well as hinders healing from cancer treatments (Dai et al., 2020). The results of numerous studies have shown that implementing stress management spractices uch as Cognitive-behavioral stress management (CBSM) improves mood and lowers distress during treatment and, is also associated with longer survival compared to control groups in the 8-15 year follow up (Stagl et al., 2015).
Respect your biological rhythm.
The International Agency for Research on Cancer (IARC) reports that, when the human circadian clock is disrupted, the likelihood of developing cancers, including lung cancers, intestinal cancers, and breast cancers, dramatically increases (Huang, et al., 2023). Go to bed at the same time and, have about 8 hours of sleep. As much as possible avoid night shifts at work along with frequent jet lag as that highly disrupts the circadian rhythm.
Increase social connections and be part of a social community
Absence of social support, feeling lonely and socially isolated tends reduces immune competence and increases cancer mortality risk while having more social support satisfaction is associated with lower mortality risks (Salazaor et al., 2023; Boen et al., 2018). Meta-analysis of 148 studies (308,849 participants) found that that on the average there is a 50% increased likelihood of survival for participants with stronger social relationships (Holt-Lunstad et al., 2010).
Live a life with meaning and purpose
Having meaning and purpose make each moment worth living and may contribute to improving immune function and possible cancer survival (LeShan, 1994; Rosenbaum & Rosenbaum, 2023).
Summary
The research suggests that cancer screening does not extend life span unless specifically performed for certain diagnostic purposes or, with individuals who are at high risk of developing cancers (e.g., have a genetic predisposition). Implementing self-care health behaviors that have been identified to promote health and increase lifespan. Implementing health behaviors is challenging since there is limited governmental and corporate support. Thus, take charge and implement a holistic self-care lifestyle that reduces cancer risk factors and supports health.
See also the following blogs:
References
AACR. (2011). AACR Cancer Progress Report 2011. American Association for Cancer Research. http://www.aacr.org/Uploads/DocumentRepository/2011CPR/2011_AACR_CPR_Text_web.pdf
American Cancer Society. (2021). History of ACS Recommendations for the Early Detection of Cancer in People Without Symptoms. Accessed November 11, 2023. https://www.cancer.org/health-care-professionals/american-cancer-society-prevention-early-detection-guidelines/overview/chronological-history-of-acs-recommendations.html
Autier, P., Boniol, M., Gavin, A,, & Vatten, L.J. (2011) Breast cancer mortality in neighbouring European countries with different levels of screening but similar access to treatment: trend analysis of WHO mortality database. BMJ. 343, d4411. https://doi.org/10.1136/bmj.d4411
Badal., K., Staib, J., Tice,J., Kim, M-O., Eklund, M., DaCosta Byfield, S., Catlett,K., Wilson,L., et al, (2023). Cost of breast cancer screening in the USA: Comparison of current practice, advocated guidelines, and a personalized risk-based approach. Journal of Clinical Oncology, 41: 16_suppl, 3 18917 :16_suppl, e18917. https://doi.org/10.1200/JCO.2023.41.16_suppl.e18917
Baudry, J., Assmann, K.E., Touvier, M., et al. (2018). Association of Frequency of Organic Food Consumption With Cancer Risk: Findings From the NutriNet-Santé Prospective Cohort Study. JAMA Intern Med, 178(12), 1597–1606. https://doi.org/10.1001/jamainternmed.2018.4357
Boen, C.E., Barrow, D..A, Bensen, J.T., Farnan, L., Gerstel, A., Hendrix, L.H., Yang, Y.C. (2018). Social Relationships, Inflammation, and Cancer Survival. Cancer. Epidemiol Biomarkers Prev, 27(5), 541-549. https://doi.org/10.1158/1055-9965.EPI-17-0836
Bretthauer M, Wieszczy P, Løberg M, et al. (2023). Estimated Lifetime Gained With Cancer Screening Tests: A Meta-Analysis of Randomized Clinical Trials. JAMA Intern Med. 183(11),1196–1203. https://doi.org/10.1001/jamainternmed.2023.3798Brown, K.F., Rumgay, H., Dunlop, C. et al. (2018). The fraction of cancer attributable to modifiable risk factors in England, Wales, Scotland, Northern Ireland, and the United Kingdom in 2015. Br J Cancer, 118, 1130–1141. https://doi.org/10.1038/s41416-018-0029-6
CDC. (2023a). U.S. Cancer Statistics Working Group. U.S. Cancer Statistics Data Visualizations Tool, based on 2022 submission data (1999-2020): U.S. Department of Health and Human Services, Centers for Disease Control and Prevention and National Cancer Institute; released in November 2023. https://www.cdc.gov/cancer/dataviz
CDC. (2023b). Leading Causes of Death. National Center for health statistics, Centers for disease control and prevention. Accessed November 20, 2023. https://www.cdc.gov/nchs/fastats/leading-causes-of-death.htm
CSPH. (2021). Estimating annual expenditures for cancer screening in the United States. Center for Surgery and Public Health. Assessed November 14, 2023. https://csph.brighamandwomens.org/wp-content/uploads/2021/12/Estimating-Annual-Expenditures-for-Cancer-Screening-in-the-United-States.pdf
Dai, S., Mo, Y., Wang, Y., Xiang, B., Liao, Q., Zhou, M., Li, X., Li, Y., Xiong. W., Li, G., Guo, C., & Zeng, Z. (2020). Chronic Stress Promotes Cancer Development. Front Oncol. 10, 1492. https://doi.org/10.3389/fonc.2020.01492
Feinberg, A. P. (2007). Phenotypic plasticity and the epigenetics of human disease. Nature, 447(7143), 433-440. https://doi.org/10.1038/nature05919
Fouad, Y. A., & Aanei, C. (2017). Revisiting the hallmarks of cancer. American journal of cancer research, 7(5), 1016. https://pubmed.ncbi.nlm.nih.gov/28560055/
Fracheboud, J. et al. (2004). Decreased rates of advanced breast cancer due to mammography screening in The Netherlands, British Journal of Cancer (2004) 91, 861–867. https://doi,org/10.1038/sj.bjc.6602075
Goldstein, B.D. (2001). The precautionary principle also applies to public health actions. Am J Public Health, 91(9),1358-61. https://doi.org/10.2105/ajph.91.9.1358
Gorter, R. & Peper, E. (2011). Fighting Cancer-A None Toxic Approach to Treatment. Berkeley: North Atlantic/New York: Random House. https://www.amazon.com/Fighting-Cancer-Nontoxic-Approach-Treatment/dp/1583942483
Gupta, P. B., Pastushenko, I., Skibinski, A., Blanpain, C., & Kuperwasser, C. (2019). Phenotypic plasticity: driver of cancer initiation, progression, and therapy resistance. Cell Stem Cell, 24(1), 65-78. https://doi.org/10.1016/j.stem.2018.11.011
Hanahan, Douglas. (2022): Hallmarks of cancer: new dimensions. Cancer discovery, 12(1), 31-46. https://doi.org/10.1158/2159-8290.CD-21-1059
Holt-Lunstad, J., Smith, T.B., & Layton, J.B. (2010). Social Relationships and Mortality Risk: A Meta-analytic Review, PLoS Med 7(7), e1000316. https://doi.org/10.1371/journal.pmed.1000316
Huang, C., Zhang, C,, Cao, Y., Li, J., & Bi, F. (2023). Major roles of the circadian clock in cancer. Cancer Biol Med, 20(1):1–24. https://doi.org/10.20892/j.issn.2095-3941.2022.0474
Kalaf, J.M. (2014). Mammography: a history of success and scientific enthusiasm. Radiol Bras. 47(4):VII-VIII. https://doi.org/10.1590/0100-3984.2014.47.4e2
Key TJ, Bradbury KE, Perez-Cornago A, Sinha R, Tsilidis KK, Tsugane S. Diet, nutrition, and cancer risk: what do we know and what is the way forward? BMJ. 2020 Mar 5;368:m511. https://doi.org/10.1136/bmj.m511
Kowalski, A.E. (2021). Mammograms and mortality: How has the evidence evolved? J Econ Perspect, 35(2), 119-140. https://doi.org/10.1257/jep.35.2.119
LeShan, L. (1994). Cancer as a turning point. New York: Plume. https://www.amazon.com/Cancer-As-Turning-Point-Professionals/dp/0452271371
Lewis, T. (2022). The U.S. just lost 26 years’ worth of progress on life expectancy. Scientific American. October 17, 2022. Accessed November 11, 2023. https://www.scientificamerican.com/article/the-u-s-just-lost-26-years-worth-of-progress-on-life-expectancy/
Ma, X., Wang, R., Long, J.B., Ross, J.S., Soulos, P.R., Yu, J.B., Makarov, D.V., Gold, H.T. and Gross, C.P. (2014), The cost implications of prostate cancer screening in the Medicare population. Cancer, 120: 96-102. https://doi.org/10.1002/cncr.28373
Mentella, M.C., Scaldaferri, F., Ricci, C., Gasbarrini, A., & Miggiano, G.A.D. (2019). Cancer and Mediterranean Diet: A Review. Nutrients,11(9):2059. https://doi.org/10.3390/nu11092059
NIH NCI (2023). Physical Activity and Cancer. National Institutes of Health National Cancer Institute. Accessed November 18, 2023. https://www.cancer.gov/about-cancer/causes-prevention/risk/obesity/physical-activity-fact-sheet
Patel, A,V., Friedenreich, C.M., Moore, S.C, et al. (2019). American College of Sports Medicine Roundtable Report on physical activity, sedentary behavior, and cancer prevention and control. Medicine and Science in Sports and Exercise, 51(11), 2391-2402. https://doi.org/10.1249/MSS.0000000000002117
Rabin, R.C. (2018). Can eating organic food lower your cancer risk? The New York Times. Oct 23, 2018. Accessed November 17, 2023. https://www.nytimes.com/2018/10/23/well/eat/can-eating-organic-food-lower-your-cancer-risk.html
Reuben, S.H. (2010). Reducing environmental cancer risk – What We Can Do Now. The President’s Cancer Panel Report. Washington, D.C: U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES, National Institutes of Health, National Cancer Institute. https://deainfo.nci.nih.gov/advisory/pcp/annualReports/pcp08-09rpt/PCP_Report_08-09_508.pdf
Rosenbaum, E. H. & Rosenbaum, I.R. (2023) The Will to Live. Stanford Center for Integrative Medicine. Surviving Cancer. Accessed November 23, 2023. https://med.stanford.edu/survivingcancer/cancers-existential-questions/cancer-will-to-live.html
Salazar, S.M.D.C., Dino, M.J.S., & Macindo, J.R.B. (2023). Social connectedness and health-related quality of life among patients with cancer undergoing chemotherapy: a mixed method approach using structural equation modelling and photo-elicitation. J Clin Nurs. Published online March 9, 2023. https://doi.org/10.1111/jocn.16675
Schmutzler, R. K., Schmitz-Luhn, B., Borisch, B., Devilee, P., Eccles, D., Hall, P., … & Woopen, C. (2022). Risk-adjusted cancer screening and prevention (RiskAP): complementing screening for early disease detection by a learning screening based on risk factors. Breast Care, 17(2), 208-223. https://doi.org/10.1159/000517182
Song, M., & Giovannucci, E. (2016). Preventable incidence and mortality of carcinoma associated with lifestyle factors among white adults in the United States. JAMA Ooncology, 2(9), 1154-1161. https://doi.org/10.1001/jamaoncol.2016.0843
Spei, M.E., Samoli, E., Bravi, F., et al. (2019). Physical activity in breast cancer survivors: A systematic review and meta-analysis on overall and breast cancer survival. Breast, 44,144-152. https://doi.org/10.1016/j.breast.2019.02.001
Stagl, J.M., Lechner, S.C., Carver, C.S. et al. (2015). A randomized controlled trial of cognitive-behavioral stress management in breast cancer: survival and recurrence at 11-year follow-up. Breast Cancer Res Treat, 154, 319–328. https://doi.org/10.1007/s10549-015-3626-6
Stratton, K., Shetty, P., Wallace, R., et al., eds. (2001). Institute of Medicine (US) Committee to Assess the Science Base for Tobacco Harm Reduction. Washington (DC): National Academies Press (US). https://www.ncbi.nlm.nih.gov/books/NBK222369/
Tailor, T.D,, Bell, S., Fendrick, A.M., & Carlos, R.C. (2022) Total and Out-of-Pocket Costs of Procedures After Lung Cancer Screening in a National Commercially Insured Population: Estimating an Episode of Care. J Am Coll Radiol. 19(1 Pt A), 35-46. https://doi.org/10.1016/j.jacr.2021.09.015
Turner, M.C., Andersen, Z.J., Baccarelli, A., Diver, W.R., Gapstur, S.M., Pope, C.A 3rd, Prada, D., Samet, J., Thurston, G., & Cohen, A. (2020). Outdoor air pollution and cancer: An overview of the current evidence and public health recommendations. CA Cancer J Clin, 10.3322/caac.21632. https://doi.org/10.3322/caac.21632
US Department of Health and Human Services (2014). The Health Consequences of Smoking: 50 Years of Progress. A Report of the Surgeon General. Atlanta, GA: :
US Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health. https://aahb.org/Resources/Pictures/Meetings/2014-Charleston/PPT%20Presentations/Sunday%20Welcome/Abrams.AAHB.3.13.v1.o.pdf
Van Tulleken, C. (2023). Ultra-processed people. The science behind food that isn’t food. New Yoerk: W.W. Norton & Company. https://www.amazon.com/gp/product/1324036729/ref=ox_sc_act_title_1?smid=ATVPDKIKX0DER&psc=1
Are food companies responsible for the epidemic in diabetes, cancer, dementia and chronic disease and do their products need to be regulated like tobacco? Is it time for a class action suit?
Posted: July 15, 2023 Filed under: behavior, cancer, Evolutionary perspective, health, Nutrition/diet, self-healing | Tags: dementia, diabetes, diet, high fructose corn syrup, mortality, obsity, smoking, sugar, ultra-processed foods, UPF 4 CommentsAdapted from: Peper, E. & Harvey, R. (2024). Are Food Companies Responsible for the Epidemic in Diabetes, Cancer, Dementia and Chronic Disease and Do Their Products Need to Be Regulated Like Tobacco? Is It Time for a Class Action Suit? Thownsend Letter-the examiner of alternative medicine. https://www.townsendletter.com/e-letter-26-ultra-processed-foods-and-health-issues/
Erik Peper, PhD and Richard Harvey, PhD

Why are one third of young Americans becoming obese and at risk for diabetes?
Why are heart disease, cancer, and dementias occurring earlier and earlier? Is it genetics, environment, foods, or lifestyle?
Is it individual responsibility or the result of the quest for profits by agribusiness and the food industry?
Like the tobacco industry that sells products regulated because of their public health dangers, is it time for a class action suit against the processed food industry? The argument relates not only to the regulation of toxic or hazardous food ingredients (e.g., carcinogenic or obesogenic chemicals) but also to the regulation of consumer vulnerabilities. Addressing vulnerabilities to tobacco products include regulations such as how cigarette companies may not advertise their products for sale within a certain distance from school grounds.
Is it time to regulate nationally the installation of vending machines on school grounds selling sugar-sweetened beverages? Students have sensitivity to the enticing nature of advertised, and/or conveniently available consumable products such as ‘fast foods’ that are highly processed (e.g., packaged, preserved and practically imperishable). Whereas ‘processed foods’ have some nutritive value, and may technically pass as ‘nutritious’ food, the quality of processed ‘nutrients’ can be called into question. For the purpose of this blog other important questions to raise relate to ingredients which, alone or in combination, may contribute to the onset of or, the acceleration of a variety of chronic health outcomes related to various kinds of cancers, cardiovascular diseases, and diabetes.
It may be an over statement to suggest that processed food companies are directly responsible for the epidemic in diabetes, cancer, dementia and chronic disease and need to be regulated like tobacco. On the other hand, processed food companies should become much more regulated than they are now.
More than 80 years ago, smoking was identified as a significant factor contributing to lung cancer, heart disease and many other disorders. In 1964 the Surgeon Generals’ report officially linked smoking to deaths of cancer and heart disease (United States Public Health Service, 1964). Another 34 years pased before California prohibited smoking in restaurants in 1998 and, eventually inside all public buildings. The harms of smoking tobacco products were well known, yet many years passed with countless deaths and suffering which could have been prevented before regulation of tobacco products took place. Reviewing historical data there is about a 20 year delay (e.g., a whole generation) before death rates decrease in relation to when regulations became effective and smoking rates decreased, as shown in figure 1.

Figure 1. The relationship between smoking and lung cancer. Reproduced by permission from Roser, M. (2021). Smoking: How large of a global problem is it? And how can we make progress against it? Our world in data.
During those interim years before government actions limited smoking more effectively, tobacco companies hid data regarding the harmful effects of smoking. Arguably, the ‘Big Tobacco’ industry paid researchers to publish data which could confuse readers about tobacco product harm. There is evidence of some published articles suggesting that the harm of cigarette smoking was a hoax– all for the sake of boosting corporate profits (Bero, 2005).
Now we are experiencing a similar problem with the processed food industry. It has been suggested that alongside smoking and vaping, opioid use, a sedentary ‘couch potato’ lifestyle, and lack of exercise, ultra-processed food (UPF) that we eat severely affects our health.
Ultra-processed foods, which for many constitutes a majority of calories ranging from 55% to over 80% of the food they eat, contain chemical additives that trick the tastebuds, mouth and eventually our brain to desire those processed foods and eat more of them (Srour et al., 2022).
What are ultra-processed foods? Any foods that your great grandmother would not recognize as food. This includes all soft drinks, highly processed chips, additives, food coloring, stabilizers, processed proteins, etc. Even oils such as palm oil, canola oil, or soybean are ultra processed since they heated, highly processed with phosphoric acid to remove gums and waxes, neutralized with chemicals, bleached, and deodorized with high pressure steam (van Tulleken, 2023).
The data is clear! Since the 1970s obesity and inflammatory disease have exploded after ultra-processed foods became the constituents of the modern diet as shown in figure 2.
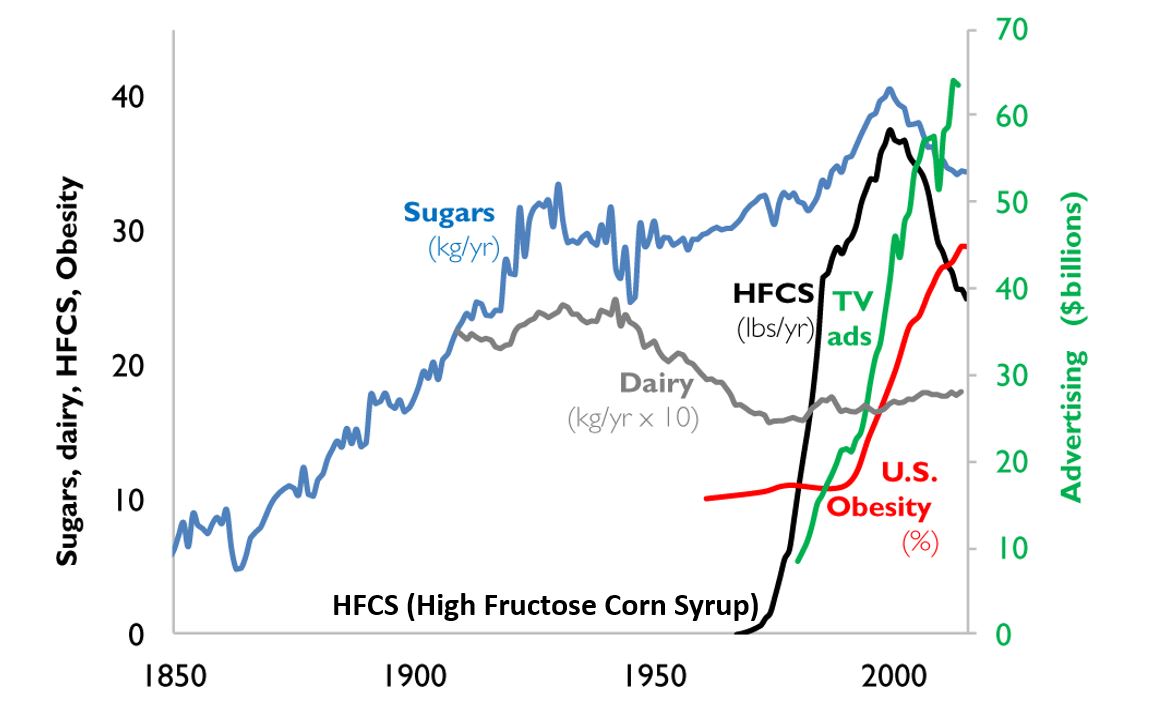
Figure 2. A timeline from 1850 to 2000 reflects the increase in use of refined sugar and high fructose corn syrup (HFCS) to the U.S. diet, together with the increase in U.S. obesity rate. The data for sugar, dairy and HFCS consumption per capita are from USDA Economic Research Service (Johnson et al., 2009) and reflects historical estimates before 1967 (Guyenet et al., 2017). The obesity data (% of U.S. adult population) are from the Robert Wood Johnson Foundation’s Trust for America’s Health. (stateofobesity.org). Total U.S. television advertising data are from the World Advertising Research Center (www.warc.com). The vertical measure (y–axis) for kilograms per year (kg/yr) on the left covers all data except advertising expenditures, which uses the vertical measure for advertising on the right. Reproduced by permission from Bentley et al, 2018.
This graph clearly shows a close association between the years that high fructose corn syrups (HFCS) were introduced into the American diet and an increase in TV advertising with corresponding increase in obesity. HFCS is an ultra-processed food and is a surrogate marker for all other ultra-processed foods. The best interpretation is that ultra-processed foods, which often contain HFCS, are a causal factor of the increase in obesity, and diabetes and in turn are risk factors for heart disease, cancers and dementias.
Ultra-processed foods are novel from an evolutionary perspective.
The human digestive system has only recently encountered sources of calories which are filled with so many unnatural chemicals, textures and flavors. Ultra-processed foods have been engineered, developed and product tested to increase the likelihood they are wanted by consumers and thereby increase sales and profits for the producers. These foods contain the ‘right amount’ processed materials to evoke the taste, flavor and feel of desired foods that ‘trick’ the consumer it eat them because they activate evolutionary preference for survival. Thus, these ultra-processed foods have become an ‘evolutionary trap’ where it is almost impossible not to eat them. We eat the food because it capitalized on our evolutionary preferences even though doing so is ultimately harmful for our health (for a detailed discussion on evolutionary traps, see Peper, Harvey & Faass, 2020).
An example is a young child wanting the candy while waiting with her parents at the supermarket checkout line. The advertised images of sweet foods trigger the cue to eat. Remember, breast milk is sweet and most foods in nature that are sweet in taste, provide calories for growth and survival and are not harmful. Calories are essential of growth. Thus, we have no intrinsic limit on eating sweets unlike foods that taste bitter.
As parents, we wish that our children (and even adults) have self-control and no desire to eat the candy or snacks that is displayed at eye level (eye candy) especially while waiting at the cashier. When reflecting about food advertising and the promotion of foods that are formulated to take advantage of ‘evolutionary traps’, who is responsible? Is it the child, who does not yet have the wisdom and self-control or, is it the food industry that ultra-processes the foods and adds ingredients into foods which can be harmful and then displays them to trigger an evolutionary preference for food that have been highly processed?
Every country that has adapted the USA diet of ultra-processed foods has experienced similar trends in increasing obesity, diabetes, cardiovascular disease, etc. The USA diet is replacing traditional diets as illustrated by the availability of Coca-Cola. It is sold in over 200 countries and territories (Coca-Cola, 2023).
An increase in ultra-processed foods by 10 percent was associated with a 25 percent increase in the risk of dementia and a 14 per cent increase in the risk of Alzheimers’s (Li et al., 2022). More importantly, people who eat the highest proportion of their diet in ultra-processed foods had a 22%-62% increased risk of death compared to the people who ate the lowest proportion of processed foods (van Tulleken, 2023). In the USA, counties with the highest food swamp scores (the availability of fast food outlets in a county) had a 77% increased odds of high obesity-related cancer mortality (Bevel et al., 2023). The increase risk has also been observed for cardiovascular disease, coronary heart disease, cerebrovascular disease and all cause mortality as is shown in figure 3 (Srour et al., 2019; Rico-Campà et al., 2019).

Figure 3. Association between consumption of ultra-processed foods and all cause mortality. Reproduced from Rico-Campà et al, 2019.
The harmful effects of UPF holds up even when correcting for the amount of sugars, carbohydrates or fats in the diet and controlling for socio economic variables.
The logic that underlies this perspective is based upon the writing by Nassim Taleb (2012) in his book, Antifragile: Things That Gain from Disorder (Incerto). He provides an evolutionary perspective and offers broad and simple rules of health as well as recommendations for reducing UPF risk factors:
- Assume that anything that was not part of our evolutionary past is probably harmful.
- Remove the unnatural/unfamiliar (e.g. smoking/ e-cigarettes, added sugars, textured proteins, gums, stabilizers (guar gum, sodium alginate), emulsifiers (mono-and di-glycerides), modified starches, dextrose, palm stearin, and fats, colors and artificial flavoring or other ultra-processed food additives).
What can we do?
The solutions are simple and stated by Michael Pollan in his 2007 New York Times article, “Eat food. Not too much. Mostly Plants.” Eat foods that your great grandmother would recognize as foods (Pollan, 2009). Do not eat any of the processed foods that fill a majority of a supermarket’s space.
- Buy only whole organic natural foods and prepare them yourself.
- Request that food companies only buy and sell non-processed foods.
- Demand government action to tax ultra-processed food and limit access to these foods. In reality, it is almost impossible to expect people to choose healthy, organic foods when they are more expensive and not easily available in the American ‘food swamps and deserts’ (the presence of many fast food outlets or the absence of stores that have fresh produce and non-processed foods). We do have a choice. We can spend more money now for organic, health promoting foods or, pay much more later to treat illness related to UPF.
- It is time to take our cues from the tobacco wars that led to regulating tobacco products. We may even need to start class action suits against producers and merchants of UPF for causing increased illness and premature morbidity.
For more background information and the science behind this blog, read, the book, Ultra-processed people, by Chris van Tulleken.

Look at the following blogs for more background information.
References
Bentley, R.A., Ormerod, P. & Ruck, D.J. (2018). Recent origin and evolution of obesity-income correlation across the United States. Palgrave Commun 4, 146. https://doi.org/10.1057/s41599-018-0201-x
Bero, L. A. (2005). Tobacco Industry Manipulation of Research. Public Health Reports (1974-), 120(2), 200–208. http://www.jstor.org/stable/20056773
Bevel, M.S., Tsai, M., Parham, A., Andrzejak, S.E., Jones, S., & Moore, J.X. (2023). Association of Food Deserts and Food Swamps With Obesity-Related Cancer Mortality in the US. JAMA Oncol. 9(7), 909–916. https://doi.org/10.1001/jamaoncol.2023.0634
Coca-Cola. (2023). More on Coca-Cola. Accessed July 14, 2023. https://www.coca-cola.co.uk/our-business/faqs/how-many-countries-sell-coca-cola-is-there-anywhere-in-the-world-that-doesnt
Johnson, R.K., Appel, L.J., Brands, M., Howard, B.V., Lefevre, M., Lustig, R.H., Sacks, F., Steffen, L.M., & Wylie–Rosett, J. (2009). Dietary sugars intake and cardiovascular health: a scientific statement from the American Heart Association. Circulation, 120(10), 1011–1020. https://doi.org/10.1161/CIRCULATIONAHA.109.192627
Li, H., Li, S., Yang, H., et al, 2022. Association of ultraprocessed food consumption with the risk of dementia: a prospective cohort study. Neurology, 99, e1056-1066. https://doi.org/10.1212/WNL.0000000000200871
Peper, E., Harvey, R. & Faass, N. (2020). TechStress: How Technology is Hijacking Our Lives, Strategies for Coping, and Pragmatic Ergonomics. Berkeley: North Atlantic Books, pp 18-22, 151. https://www.amazon.com/Beyond-Ergonomics-Prevent-Fatigue-Burnout/dp/158394768X/ref=sr_1_1?crid=1U9Y82YO4DKKP&keywords=erik+peper&qid=1689372466&sprefix=erik+peper%2Caps%2C187&sr=8-1
Pollan, M. (2007). Unhappy meals. The New York Times Magazine. https://www.nytimes.com/2007/01/28/magazine/28nutritionism.t.html
Pollan, M. (2009). Food Rules: An Eater’s Manual. New York: Penguin Books. https://www.amazon.com/Food-Rules-Eaters-Michael-Pollan/dp/014311638X/ref=tmm_pap_swatch_0?_encoding=UTF8&qid=1689373484&sr=8-2
Rico-Campà, A., Martínez-González, M. A., Alvarez-Alvarez, I., de Deus Mendonça, R., Carmen de la Fuente-Arrillaga, C., Gómez-Donoso, C., & Bes-Rastrollo, M. (2019). Association between consumption of ultra-processed foods and all cause mortality: SUN prospective cohort study. BMJ; 365: l1949 https://doi.org/10.1136/bmj.l1949
Roser, M. (2021).Smoking: How large of a global problem is it? And how can we make progress against it? Our world in data. Assessed July 13, 2023. https://ourworldindata.org/smoking-big-problem-in-brief
Srour, B., Fezeu, L.K., Kesse-Guyot, E.,Alles, B., Mejean, C…(2019). Ultra-processed food intake and risk of cardiovascular disease: prospective cohort study (NutriNet-Santé) BMJ,365:l1451. https://doi.org/10.1136/bmj.l1451
Srour, B., Kordahi, M. C., Bonazzi, E., Deschasaux-Tanguy, M., Touvier, M., & Chassaing, B. (2022). Ultra-processed foods and human health: from epidemiological evidence to mechanistic insights. The Lancet Gastroenterology & Hepatology. https://doi.org/10.1016/S2468-1253(22)00169-8
Taleb, N. N. (2012). Antifragile: Things That Gain from Disorder (Incerto). New York: Random House Publishing Group. (Kindle Locations 5906-5908). https://www.amazon.com/Antifragile-Things-Disorder-ANTIFRAGILE-Hardcover/dp/B00QOJ6MLC/ref=sr_1_4?crid=3BISYYG0RPGW5&keywords=Antifragile%3A+Things+That+Gain+from+Disorder+%28Incerto%29&qid=1689288744&s=books&sprefix=antifragile+things+that+gain+from+disorder+incerto+%2Cstripbooks%2C158&sr=1-4
Van Tulleken, C. (2023). Ultra-processed people. The science behind food that isn’t food. New Yoerk: W.W. Norton & Company. https://www.amazon.com/gp/product/1324036729/ref=ox_sc_act_title_1?smid=ATVPDKIKX0DER&psc=1
United States Public Health Service. (1964). The 1964 Report on Smoking and Health. United States. Public Health Service. Office of the Surgeon General. https://profiles.nlm.nih.gov/spotlight/nn/catalog?f%5Bexhibit_tags%5D%5B%5D=smoking
Useful resources about breathing, phytonutrients and exercise
Posted: June 30, 2021 Filed under: behavior, Breathing/respiration, cancer, Evolutionary perspective, health, Nutrition/diet, self-healing, Uncategorized | Tags: diet, exercise, immune system, nasal breathing, phytonutrients, respiration 1 Comment
Dysfunctional breathing, eating highly processed foods, and lack of movement contribute to development of illnesses such as cancer, diabetes, cardiovascular disease and many chronic diseases. They also contributes to immune dysregulation that increases vulnerability to infectious diseases, allergies and autoimmune diseases. If you wonder what breathing patterns optimize health, what foods have the appropriate phytonutrients to support your immune system, or what the evidence is that exercise reduces illness and promotes longevity, look at the following resources.
Breath: the mind-body connector that underlies health and illness
Read the outstanding article by Martin Petrus (2021). How to breathe.
https://psyche.co/guides/how-to-breathe-your-way-to-better-health-and-transcendence
You are the food you eat
Watch the superb webinar presentation by Deanna Minich, MS., PHD., FACN, CNS, (2021) Phytonutrient Support for a Healthy Immune System.
Movement is life
Explore the summaries of recent research that has demonstrated the importance of exercise to increase healthcare saving and reduce hospitalization and death.
Cell phone radio frequency radiation increases cancer risk*
Posted: November 12, 2018 Filed under: cancer, digital devices, self-healing, Uncategorized | Tags: cellphones, digital devices, Radio frequency radiation, technology 3 Comments
Be safe rather than sorry. Cellphone radio frequency radiation is harmful!
The National Toxicology Program (NTP) released on October 31, 2018 their final report on rat and mouse studies of radio frequency radiation like that used with cellphones. The $30 million NTP studies took more than 10 years to complete and are the most comprehensive assessments to date of health effects in animals exposed to Radio Frequency Radiation (RFR) with modulations used in 2G and 3G cell phones. 2G and 3G networks were standard when the studies were designed and are still used for phone calls and texting.
The report concluded there is clear evidence that male rats exposed to high levels of radio frequency radiation (RFR) like that used in 2G and 3G cell phones developed cancerous heart tumors, according to final reports. There was also some evidence of tumors in the brain and adrenal gland of exposed male rats. For female rats, and male and female mice, the evidence was equivocal as to whether cancers observed were associated with exposure to RFR.
“The exposures used in the studies cannot be compared directly to the exposure that humans experience when using a cell phone,” said John Bucher, Ph.D., NTP senior scientist. “In our studies, rats and mice received radio frequency radiation across their whole bodies. By contrast, people are mostly exposed in specific local tissues close to where they hold the phone. In addition, the exposure levels and durations in our studies were greater than what people experience.”
In the NTP study, the lowest exposure level used in the studies was equal to the maximum local tissue exposure currently allowed for cell phone users. This power level rarely occurs with typical cell phone use. The highest exposure level in the studies was four times higher than the maximum power level permitted. Butcher state, “We believe that the link between radio frequency radiation and tumors in male rats is real, and the external experts agreed.”
I interpret that their results support the previous–often contested–observations that brain cancers were more prevalent in high cell phone users especially on the side of the head they held the cellphone.
More some women who have habitually stashed their cell phone in their bra have been diagnosed with a rare breast cancer located beneath the area of the breast where they stored their cell phone. Watch the heart breaking TV interview with Tiffany. She was 21 years old when she developed breast cancer which was located right beneath the breast were she had kept her cell phone against her bare skin for the last 6 years.
While these rare cases could have occurred by chance, they could also be an early indicator of risk. Previously, most research studies were based upon older adults who have tended to use their mobile phone much less than most young people today. The average age a person acquires a mobile phone is ten years old (this data was from 2016 and many children now have cellphones even earlier). Often infants and toddlers are entertained by smartphones and tablets–the new technological babysitter. The possible risk may be much greater for a young people since their bodies and brains are still growing rapidly. I wonder if the antenna radiation may be one of the many initiators or promoters of later onset cancers. We will not know the answer; since, most cancer take twenty or more years to develop.
What can you do to reduce risk?
Act now and reduce the exposure to the antenna radiation by implementing the following suggestions:
- Keep your phone, tablet or laptop in your purse, backpack or briefcase. Do not keep it on or close to your body.
- Use the speakerphone or earphones with microphone while talking. Do not hold it against the side of your head, close to your breast or on your lap.
- Text while the phone is on a book or on a table away from your body.
- Put the tablet and laptop on a table and away from the genitals.
- Set the phone to airplane mode.
- Be old fashioned and use a cable to connect to your home router instead of relying on the WiFi connection.
- Keep your calls short and enjoy the people in person.
- Support legislation to label wireless devices with a legible statement of possible risk and the specific absorption rate (SAR) value. Generally, higher the SAR value, the higher the exposure to antenna radiation.
- Support the work by the Environmental Health Trust.
For an radio interview on this topic, listen to my interview on Deborah Quilter’s radio show. http://www.blogtalkradio.com/rsihelp/2018/11/20/why-you-should-keep-your-cell-phone-away-from-your-body-with-dr-erik-peper
For more information on NTP study see:
*The blog is adapted in part from the November 1, 2018 news release from the National Toxicology Program (NTP)1, National Institute of Environmental Health Sciences2, National Institute of Health (NIH)3.
- About the National Toxicology Program (NTP):NTP is a federal, interagency program headquartered at NIEHS, whose goal is to safeguard the public by identifying substances in the environment that may affect human health. For more information about NTP and its programs, visit niehs.nih.gov.
- About the National Institute of Environmental Health Sciences (NIEHS): NIEHS supports research to understand the effects of the environment on human health and is part of NIH. For more information on environmental health topics, visit niehs.nih.gov. Subscribe to one or more of the NIEHS news lists (www.niehs.nih.gov/news/newsroom/newslist/index.cfm) to stay current on NIEHS news, press releases, grant opportunities, training, events, and publications.
- About the National Institutes of Health (NIH):NIH, the nation’s medical research agency, includes 27 Institutes and Centers and is a component of the U.S. Department of Health and Human Services. NIH is the primary federal agency conducting and supporting basic, clinical, and translational medical research, and is investigating the causes, treatments, and cures for both common and rare diseases. For more information about NIH and its programs, visit nih.gov.
Cancer: What you can do to prevent and support healing
Posted: April 22, 2018 Filed under: cancer, self-healing, Uncategorized | Tags: cancer, healing, Holistic health, prevention, self-care, stress Leave a commentAre you curious to know if there is anything you can do to help prevent cancer?
Are you searching for ways to support your healing process and your immune system?
If yes, watch the invited lecture presented October 14, 2017, at the Caribbean Active Aging Congress, Oranjestad, Aruba, http://www.caacaruba.com
Cancer: A modern scourge or the cost of being a multi-cell organism?
Posted: September 27, 2013 Filed under: cancer, Uncategorized | Tags: cancer, evolution, Immune function 1 CommentAlthough I knew intellectually that cancer was not a new disease since it had been described in early medical texts, I always thought that it was more a scourge of recent times. The tweets, the news reports, the innumerable stories of new cancer treatments promoted on the web, the ongoing recommendations for specific foods, vitamin supplements, and lifestyle recommendations to prevent cancer, and the heart wrenching stories of celebrities telling their personal cancer saga, all suggested that cancer rates are increasing and definitely a modern disease.
It is difficult to make sense out of this maelstrom of pessimistic and optimist news about the war on cancer. Yet, if one can take a broader perspective, cancer is not the number one killer–that honor belongs to heart disease. And, although breast cancer is terrifying, many more women die of heart disease than breast cancer (Jemal, et al, 2008).
Most likely, cancer has been with us since we evolved from a single cell—it may express the fundamental life force of a cell when it becomes threatened or is no longer subservient and supportive for the maintenance of its community of cells. It is humbling to realize that cancer transcends our human history. It has even been found in dinosaur bones. If it was in the bones, then other cancers probably also occurred in the dinosaur’s soft tissue. It is equally humbling to recognize that although environmental and dietary factors can affect carcinogenesis, in most cases the data is much less clear. So often one study finds a beneficial effect and then a few years later another study reports the opposite finding. Yes, some behaviors are generally harmful-smoking increases the risk of lung cancer significantly although most smokers do not die of lung cancer. And, most likely the major significant factor in the recent decrease in breast cancer death rate is that women are smoking less and stopped using hormone replacement therapy.
One thing is clear, cancer is part of our human biology and it has occurred since multi-cellular organisms (e.g., morula) evolved to deal with cellular stress (Boaz, 2002). To grasp the biological complexity, the confusion that exists and appreciate how to perceive different perspectives, I strong recommend reading the remarkable book, The Cancer Chronicles: Unlocking Medicine’s Deepest Mystery, by the award winning science writer George Johnson. (Johnson, 2013).
References:
Boaz, N.T. (2002). Evolving Health: The origins of illness and how the modern world is making us sick. New York: John Wiley & Sons.
Jemal, A., Siegel, R., Ward, E., Hao, Y., Xu, J., Murray, T. and Thun, M. J. (2008), Cancer Statistics, 2008. CA: A Cancer Journal for Clinicians, 58: 71–96. doi: 10.3322/CA.2007.0010 http://onlinelibrary.wiley.com/doi/10.3322/CA.2007.0010/full
Johnson, G. (2013). The Cancer Chronicles: Unlocking Medicine’s Deepest Mystery. New York: Alfred A. Knopf. http://talaya.net/chronicles/
