Cellphones affects social communication, vision, breathing, and health: What to do!
Posted: September 4, 2024 Filed under: ADHD, attention, behavior, Breathing/respiration, cellphone, computer, digital devices, educationj, ergonomics, health, laptops, Neck and shoulder discomfort, posture, screen fatigue, self-healing, stress management, techstress, Uncategorized, vision, zoom fatigue | Tags: communication, myopia, pedestrian deaths, peripheral vision, text neck 7 CommentsAdapted from: Peper, E. & Harvey, R. (2024). Cell phones affects social communication, vision, breathing, and mental and physical health: What to do! TownsendLetter-The Examiner of Alternative Medicine,September 15, 2024. https://townsendletter.com/smartphone-affects-social-communication-vision-breathing-and-mental-and-physical-health-what-to-do/

Abstract
Smartphones are an indispensable part of our lives. Unfortunately too much of a ‘good thing’ regarding technology can work against us, leading to overuse, which in turn influences physical, mental and emotional development among current ‘Generation Z’ and ‘Millennial’ users (e.g., born 1997-2012, and 1981-1996, respectively). Compared to older technology users, Generation Z report more mental and physical health problems. Categories of mental health include attentional deficits, feelings of depression, anxiety social isolation and even suicidal thoughts, as along with physical health complaints such as sore neck and shoulders, eyestrain and increase in myopia. Long duration of looking downward at a smartphone affects not only eyestrain and posture but it also affects breathing which burden overall health. The article provides evidence and practices so show how technology over use and slouching posture may cause a decrease in social interactions and increases in emotional/mental and physical health symptoms such as eyestrain, myopia, and body aches and pains. Suggestions and strategies are provided for reversing the deleterious effects of slouched posture and shallow breathing to promote health.
We are part of an uncontrolled social experiment
We, as technology users, are all part of a social experiment in which companies examine which technologies and content increase profits for their investors (Mason, Zamparo, Marini, & Ameen, 2022). Unlike University research investigations which have a duty to warn of risks associated with their projects, we as participants in ‘profit-focused’ experiments are seldom fully and transparently informed of the physical, behavioral and psychological risks (Abbasi, Jagaveeran, Goh, & Tariq, 2021; Bhargava, & Velasquez, 2021). During university research participants must be told in plain language about the risks associated with the project (Huh-Yoo & Rader, 2020; Resnik, 2021). In contrast for-profit technology companies make it possible to hurriedly ‘click through’ terms-of-service and end-user-license-agreements, ‘giving away’ our rights to privacy, then selling our information to the highest bidder (Crain, 2021; Fainmesser, Galeotti, & Momot, 2023; Quach et al., 2022; Yang, 2022).
Although some people remain ignorant and or indifferent (e.g., “I don’t know and I don’t care”) about the use of our ‘data,’ an unintended consequence of becoming ‘dependent’ on technology overuse includes the strain on our mental and physical health (Abusamak, Jaber & Alrawashdeh, 2022; Padney et al., 2020). We have adapted new technologies and patterns of information input without asking the extent to which there were negative side effects (Akulwar-Tajane, Parmar, Naik & Shah, 2020; Elsayed, 2021). As modern employment shifted from predominantly blue-collar physical labor to white collar information processing jobs, people began sitting more throughout the day. Workers tended to look down to read and type. ‘Immobilized’ sitting for hours of time has increased as people spend time working on a computer/laptop and looking down at smartphones (Park, Kim & Lee, 2020). The average person now sits in a mostly immobilized posture 10.4 hours/day and modern adolescents spent more than two thirds of their waking time sitting and often looking down at their smartphones (Blodgett, et al., 2024; Arundell et al., 2019).
Smartphones are an indispensable part of our lives and is changing the physical and mental emotional development especially of Generation Z who were born between 1997-2012 (Haidt, 2024). They are the social media and smartphone natives (Childers & Boatwright, 2021). The smartphone is their personal computer and the gateway to communication including texting, searching, video chats, social media (Hernandez-de-Menendez, Escobar Díaz, & Morales-Menendez, 2020; Nichols, 2020; Schenarts, 2020; Szymkowiak et al., 2021). It has 100,000 times the processing power of the computer used to land the first astronauts on the moon on July 20, 1969 according to University of Nottingham’s computer scientist Graham Kendal (Dockrill, 2020). More than one half of US teens spend on the average more than 7 hours on daily screen time that includes watching streaming videos, gaming, social media and texting and their attention span has decreased from 150 seconds in 2004 to an average of 44 seconds in 2021 (Duarte, F., 2023; Mark, 2022, p. 96).
For Generation Z, social media use is done predominantly with smartphones while looking down. It has increased mental health problems such as attentional deficits, depression, anxiety suicidal thoughts, social isolation as well as decreased physical health (Haidt, 2024; Braghieri et al., 2023; Orsolini, Longo & Volpe, 2023; Satılmış, Cengız, & Güngörmüş, 2023; Muchacka-Cymerman, 2022; Fiebert, Kistner, Gissendanner & DaSilva, 2021; Mohan et al., 2021; Goodwin et al., 2020).
The shift in communication from synchronous (face-to-face) to asynchronous (texting) has transformed communications and mental health as it allows communication while being insulated from the other’s reactions (Lewis, 2024). The digital connection instead of face-to-face connection by looking down at the smart phone also has decreased the opportunity connect with other people and create new social connections, with three typical hypotheses examining the extent to which digital technologies (a) displace/ replace; (b) compete/ interfere with; and/or, (c) complement/ enhance in-person activities and relationships (Kushlev & Leitao, 2020).
As described in detail by Jonathan Haidt (2024), in his book, The Anxious Generation, the smartphone and the addictive nature of social media combined with the reduction in exercise, unsupervised play and childhood independence was been identified as the major factors in the decrease in mental health in your people (Gupta, 2023). This article focuses less on distraction such as attentional deficits, or dependency leading to tolerance, withdrawal and cravings (e.g., addiction-like symptoms) and focuses more on ‘dysregulation’ of body awareness (posture and breathing changes) and social communication while people are engaged with technology (Nawaz,Bhowmik, Linden & Mitchell, 2024).
The excessive use of the smartphones is associated with a significant reduction of physical activity and movement leading to a so-called sedentarism or increases of sitting disease (Chandrasekaran & Ganesan, 2021; Nakshine, Thute, Khatib, & Sarkar, 2022). Unbeknown to the smartphone users their posture changes, as they looks down at their screen, may also affect their mental and physical health (Aliberti, Invernizzi, Scurati & D’lsanto, 2020).
(1) Explore how looking at your smartphone affects you (adapted from: Peper, Harvey, & Rosegard, 2024)
For a minute, sit in your normal slouched position and look at your smartphone while intensely reading the text or searching social media. For the next minute sit tall and bring the cell phone in front of you so you can look straight ahead at it. Again, look at your smartphone while intensely reading the text or searching social media.
Compare how the posture affects you. Most likely, your experience is similar to the findings from students in a classroom observational study. Almost all experienced a reduction in peripheral awareness and breathed more shallowly when they slouched while looking at their cellphone.
Decreased peripheral awareness and increased shallow breathing that affects physical and mental health and performance. The students reported looking down position reduces the opportunity of creating new social connections. Looking down my also increases the risk for depression along with reduced cognitive performance during class (Peper et al., 2017; Peper et al., 2018).
(2) Explore how posture affects eye contact (adapted from the exercise shared by Ronald Swatzyna, 2023)[2]
Walk around your neighborhood or through campus either looking downwards or straight ahead for 30 minutes while counting the number of eye contacts you make.
Most likely, when looking straight ahead and around versus slouched and looking down you had the same experience as Ronald Swatzyna (2023), Licensed Clinical Social Worker. He observed that when he walked a three-mile loop around the park in a poor posture with shoulders forward in a head down position, and then reversed direction and walked in good posture with the shoulders back and the head level, he would make about five times as many eye contacts with a good posture compared to the poor posture.
Anecdotal observations, often repeated by many educators, suggest before the omnipresent smartphone, students would look around and talk to each other before a university class began. Now, when Generation Z students enter an in-person class, they sit down, look down at their phone and tend not to interact with other students.
(3) Experience the effect of face-to-face in-person communication
During the first class meeting, ask students to put their cellphones away, meet with three or four other students for a few minutes, and share a positive experience that happened to them last week as well as what they would like to learn in the class. After a few minutes, ask them to report how their energy and mood changed.
In our observational class study with 24 junior and senior college students in the in-person class and 54 students in the online zoom class, almost all report that that their energy and positive mood increased after they interacted with each other. The effects were more beneficial for the in-person small group sharing than the online breakout groups sharing on Zoom as shown in Figure 1.

Figure 1. Change in subjective energy and mood after sharing experiences synchronously in small groups either in-person or online.
Without direction of a guided exercise to increase social connections, students tend to stay within their ‘smartphone bubble’ while looking down (Bochicchio et al., 2022). As a result, they appear to be more challenged to meet and interact with other people face-to-face or by phone as is reflected in the survey data that Generation Z is dating much less and more lonely than the previous generations (Cox et al., 2023).
What to do:
- Put the smartphone away so that you do not see it in social settings such as during meals or classes. This means that other people can be present with you and the activity of eating or learning.
- Do not permit smartphones in the classroom including universities unless it is required for a class assignment.
- In classrooms and in the corporate world, create activities that demands face-to-face synchronous communication.
- Unplug from the audio programs when walking and explore with your eyes what is going on around you.
(4) Looking down increases risk of injury and death
Looking down at a close screen reduces peripheral awareness and there by increases the risk of accidents and pedestrian deaths. Pedestrian deaths are up 69% since 2011 (Cova, 2024) and have consistently increased since the introduction of the iPhone in 2007 as shown in Figure 3.

Figure 3. Increase in pedestrian death since the introduction of the iphone (data plotted from https://www.iihs.org/topics/fatality-statistics/detail/pedestrians)
In addition, the increase use of mobile phones is also associated with hand and wrist pain from overuse and with serious injuries such as falls and texting while driving due to lack of peripheral awareness. McLaughlin et al (2023) reports an increase in hand and wrist injuries as well serious injuries related to distracted behaviors, such as falls and texting while driving. The highest phone related injuries (lacerations) as reported from the 2011 to 2020 emergency room visits were people in the age range from 11–20 years followed by 21–30 years.
What to do:
- Do not walk while looking at your smartphone. Attend to the environment around you.
- Unplug from the audio podcasts when walking and explore with your eyes what is going on around you.
- Sit or stop walking when answering the smartphone to reduce the probability of an accident.
- For more pragmatic suggestions, see the book, TechStress: How Technology is Hijacking Our Lives, Strategies for Coping, and Pragmatic Ergonomics, by Peper, Harvey and Faass (2020).
(5) Looking at screens increases the risk of myopia
Looking at a near screen for long periods of time increases the risk of myopia (near sightedness) which means that distant vision is more blurry. Myopia has increased as children predominantly use computers or, smartphones with smaller screen at shorter distances. By predominantly focusing on nearby screens without allowing the eye to relax remodels the eyes structure. Consequently, myopia has increase in the U.S. from 25 percent in the early 1970s to nearly 42 percent three decades later (OHSU, 2022).
Looking only at nearby screens, our eyes converge and the ciliary muscles around the lens contract and remain contracted until the person looks at the far distance. The less opportunity there is to allow the eyes to look at distant vision, the more myopia occurs. in Singapore 80 per cent of young people aged 18 or below have nearsightedness and 20 % of the young people have high myopia as compared to 10 years ago (Singapore National Eye Centre, 2024). The increase in myopia is a significant concern since high myopia is associated with an increased risk of vision loss due to cataract, glaucoma, and myopic macular degeneration (MMD). MMD is rapidly increasing and one of the leading causes of blindness in East Asia that has one of the highest myopia rates in the world (Sankaridurg et al., 2021).
What to do:
- Every 20 minutes stop looking at the screen and look at the far distance to relax the eyes for 20 seconds.
- Do not allow young children access to cellphones or screens. Let them explore and play in nature where they naturally alternate looking at far and near objects.
- Implement the guided eye regenerating practices descrubed in the article, Resolve eyestrain and screen fatigue, by Peper (2021).
- Read Meir Schneider’s (2016) book, Vision for Life, for suggestions how to maintain and improve vision.
(6) Looking down increases tech neck discomfort
Looking down at the phone while standing or sitting strains the neck and shoulder muscles because of the prolonged forward head posture as illustrated in the YouTube video, Tech Stress Symptoms and Causes (DeWitt, 2018). Using a smartphone while standing or walking causes a significant increase in thoracic kyphosis and trunk (Betsch et al., 2021). When the head is erect, the muscle of the neck balance a weight of about 10 to 12 pounds or, approximately 5 kilograms; however, when the head is forward at 60 degrees looking at your cell phone the forces on the muscles are about 60 pound or more than 25 kilograms, as illustrated in Figure 4 (Hansraj, 2014).

Figure 4. The head forward position puts as much as sixty pounds of pressure on the neck muscles and spine (by permission from Dr. Kenneth Hansraj, 2014).
This process is graphically illustrated in the YouTube video, Text Neck Symptoms and Causes Video, produced by Veritas Health (2020).
What to do:
- Keep the phone in front of you so that you do not slouch down by having your elbow support on the table.
- Every ten minutes stretch, look up and roll your shoulders backwards.
- Wear a posture feedback device such as the UpRight Go 2 to remind you when you slouch to change posture and activity (Peper et al., 2019; Stuart, Godfrey & Mancini, 2022).
- Take Alexander Technique lessons to improve your posture (Cacciatore, Johnson, & Cohen, 2020; AmAT, 2024; STAT, 2024).
(7) Looking down increases negative memory recall and depression
In our previous research, Peper et al. (2017) have found that recalling hopeless, helpless, powerless, and defeated memories is easier when sitting in a slouched position than in an upright position. Recalling positive memories is much easier when sitting upright and looking slightly upward than sitting slouched position. If attempting to recall positive memories the brain has to work hard as indicated by an significantly higher amplitudes of beta2, beta3, and beta4 EEG (i.e., electroencephalograph) when sitting slouched then when sitting upright (Tsai et al., 2016).
Not only does the postural position affect memory recall, it also affects mental math under time-pressure performance. When students sit in a slouched position, they report that is much more difficult to do mental math (serial 7ths) than when in the upright position (Peper et al., 2018). The effect of posture is most powerful for the 70% of students who reported that they blanked out on exams, were anxious, or worried about class performance or math. For the 30% who reported no performance anxiety, posture had no significant effect. When students become aware of slouching thought posture feedback and then interrupt their slouching by sitting up, they report an increase in concentration, attention and school performance (Peper et al., 2024).
How we move and walk also affects our subjective energy. In most cases, when people sit for a long time, they report feeling more fatigue; however, if participants interrupt sitting with short movement practices they report becoming less fatigue and improved cognition (Wennberg et al., 2016). The change in subjective energy and mood depends upon the type of movement practice. Peper & Lin (2012) reported that when students were asked to walk in a slow slouching pattern looking down versus to walk quickly while skipping and looking up, they reported that skipping significantly increased their subjective energy and mood while the slouch walking decreased their energy. More importantly, student who had reported that they felt depressed during the last two years had their energy decrease significantly more when walking very slowly while slouched than those who did not report experiencing depression. Regardless of their self-reported history of depression, when students skipped, they all reported an increase in energy (Peper & Lin, 2012; Miragall et al., 2020).
What to do:
- Walk with a quick step while looking up and around.
- Wear a posture feedback device such as the UpRight Go 2 to remind you when you slouch to change posture and activity (Peper et al., 2019; Roggio et al., 2021).
- When sitting put a small pillow in the mid back so that you can sit more erect (for more suggestions, see the article by Peper et al., 2017a, Posture and mood: Implications and applications to therapy).
- Place photo and other objects that you like to look a slightly higher on your wall so that you automatically look up.
(8) Shallow breathing increases the risk for anxiety
When slouching we automatically tend to breathe slightly faster and more shallowly. This breathing pattern increases the risk for anxiety since it tends to decrease pCO2 (Feinstein et al., 2022; Meuret, Rosenfield, Millard & Ritz, 2023; Paulus, 2013; Smits et al., 2022; Van den Bergh et al., 2013). Sitting slouched also tends to inhibit abdominal expansion during the inhalation because the waist is constricted by clothing or a belt –sometimes labeled as ‘designer jean syndrome’ and may increase abdominal symptoms such as acid reflux and irritable bowel symptoms (Engeln & Zola, 2021; Peper et al., 2016; Peper et al., 2020). When students learn diaphragmatic breathing and practice diaphragmatic breathing whenever they shallow breathe or hold their breath, they report a significant decrease in anxiety, abdominal symptoms and even menstrual cramps (Haghighat et al., 2020; Peper et al., 2022; Peper et al., 2023).
What to do:
- Loosen your belt and waist constriction when sitting so that the abdomen can expand.
- Learn and practice effortless diaphragmatic breathing to reduce anxiety.
Conclusion
There are many topics related to postural health and technology overuse that were addressed in this article. Some topics are beyond the scope of the article, and therefore seen as limitations. These relate to diagnosis and treatment of attentional deficits, or dependency leading to tolerance, withdrawal and cravings (e.g., addiction-like symptoms), or of modeling relationships between factors that contribute to the increasing epidemic of mental and physical illness associated with smartphone use and social media, such as hypotheses examining the extent to which digital technologies (a) displace/ replace; (b) compete/ interfere with; and/or, (c) complement/ enhance in-person activities and relationships. Typical pharmaceutical ‘treat-the-symptom’ approaches for addressing ‘tech stress’ related to technology overuse includes prescribing ‘anxiolytics, pain-killers and muscle relaxants’ (Kazeminasab et al., 2022; Kim, Seo, Abdi, & Huh, 2020). Although not usually included in diagnosis and treatment strategies, suggesting improving posture and breathing practices can significantly affect mental and physical health. By changing posture and breathing patterns, individuals may have the option to optimize their health and well-being.
See the book, TechStress-How Technology is Hijacking our Lives, Strategies for Coping and Pragmatic Ergonomics by Erik Peper, Richard Harvey and Nancy Faass. Available from: https://www.amazon.com/Beyond-Ergonomics-Prevent-Fatigue-Burnout/dp/158394768X/
Explore the following blogs for more background and useful suggestions
References
Abbasi, G. A., Jagaveeran, M., Goh, Y. N., & Tariq, B. (2021). The impact of type of content use on smartphone addiction and academic performance: Physical activity as moderator. Technology in Society, 64, 101521. https://doi.org/10.1016/j.techsoc.2020.101521
Abusamak, M., Jaber, H. M., & Alrawashdeh, H. M. (2022). The effect of lockdown due to the COVID-19 pandemic on digital eye strain symptoms among the general population: a cross-sectional survey. Frontiers in Public Health, 10, 895517. https://doi.org/10.3389/fpubh.2022.895517
Akulwar-Tajane, I., Parmar, K. K., Naik, P. H., & Shah, A. V. (2020). Rethinking screen time during COVID-19: impact on psychological well-being in physiotherapy students. Int J Clin Exp Med Res, 4(4), 201-216. https://doi.org/10.26855/ijcemr.2020.10.014
Aliberti, S., Invernizzi, P. L., Scurati, R., & D’Isanto, T. (2020). Posture and skeletal muscle disorders of the neck due to the use of smartphones. Journal of Human Sport and Exercise , 15 (3proc), S586-S598. https://www.jhse.ua.es/article/view/2020-v15-n3-proc-posture-skeletal-muscle-disorders-neck-smartpho; https://air.unimi.it/retrieve/handle/2434/774436/1588570/HSE%20-%20Posture%20and%20skeletal%20muscle%20disorders.pdf
AmSAT. (2024). American Society for the Alexander Technique. Accessed July 27, 2024. https://alexandertechniqueusa.org/
Arundell, L., Salmon, J., Koorts, H. et al. (2019). Exploring when and how adolescents sit: cross-sectional analysis of activPAL-measured patterns of daily sitting time, bouts and breaks. BMC Public Health 19, 653. https://doi.org/10.1186/s12889-019-6960-5
Bhargava, V. R., & Velasquez, M. (2021). Ethics of the attention economy: The problem of social media addiction. Business Ethics Quarterly, 31(3), 321-359. https://doi.org/10.1017/beq.2020.32
Betsch, M., Kalbhen, K., Michalik, R., Schenker, H., Gatz, M., Quack, V., Siebers, H., Wild, M., & Migliorini, F. (2021). The influence of smartphone use on spinal posture – A laboratory study. Gait Posture, 85, 298-303. https://doi.org/10.1016/j.gaitpost.2021.02.018
Blodgett, J.M., Ahmadi, M.N., Atkin, A.J., Chastin, S., Chan, H-W., Suorsa, K., Bakker, E.A., Hettiarcachchi, P., Johansson, P.J., Sherar,L. B., Rangul, V., Pulsford, R.M…. (2024). ProPASS Collaboration , Device-measured physical activity and cardiometabolic health: the Prospective Physical Activity, Sitting, and Sleep (ProPASS) consortium, European Heart Journal, 45(6) 458–471, https://doi.org/10.1093/eurheartj/ehad717
Bochicchio, V., Keith, K., Montero, I., Scandurra, C., & Winsler, A. (2022). Digital media inhibit self-regulatory private speech use in preschool children: The “digital bubble effect”. Cognitive Development, 62, 101180. https://doi.org/10.1016/j.cogdev.2022.101180
Braghieri, L., Levy, R., & Makarin, A. (2022). Social Media and Mental Health (July 28, 2022). Available at SSRN: https://ssrn.com/abstract=3919760 or http://dx.doi.org/10.2139/ssrn.3919760
Cacciatore, T. W., Johnson, P. M., & Cohen, R. G. (2020). Potential mechanisms of the Alexander technique: Toward a comprehensive neurophysiological model. Kinesiology Review, 9(3), 199-213. https://doi.org/10.1123/kr.2020-0026
Chandrasekaran, B., & Ganesan, T. B. (2021). Sedentarism and chronic disease risk in COVID 19 lockdown–a scoping review. Scottish Medical Journal, 66(1), 3-10. https://doi.org/10.1177/0036933020946336
Childers, C., & Boatwright, B. (2021). Do digital natives recognize digital influence? Generational differences and understanding of social media influencers. Journal of Current Issues & Research in Advertising, 42(4), 425-442. https://doi.org/10.1080/10641734.2020.1830893
Cox, D.A., Hammond, K.E., & Gray, K. (2023). Generation Z and the Transformation of American Adolescence: How Gen Z’s Formative Experiences Shape Its Politics, Priorities, and Future. Survey Center of American Life, November 23, 2023. Accessed July 4, 2024. https://www.americansurveycenter.org/research/generation-z-and-the-transformation-of-american-adolescence-how-gen-zs-formative-experiences-shape-its-politics-priorities-and-future/
Crain, M. (2021). Profit over privacy: How surveillance advertising conquered the internet. U of Minnesota Press. https://www.amazon.com/Profit-over-Privacy-Surveillance-Advertising/dp/1517905044
Cova, E. (2024). Pedestrian fatalities at historic high. Smart Growth America (data from U.S. Department of Transportation (USDOT). Accessed July 2, 2024. https://smartgrowthamerica.org/pedestrian-fatalities-at-historic-high/
Duarte, F. (2023). Average Screen Time for Teens (2024). Exploding Topics. Accessed July 5, 2024. https://explodingtopics.com/blog/screen-time-for-teens#average
DeWitt, D. (2018). How Does Text Neck Cause Pain? Spine-Health October 26, 2018. Accessed July 5, 2024. https://www.spine-health.com/conditions/neck-pain/how-does-text-neck-cause-pain
Dockrill, P. (2020). Your laptop charger is more powerful than Apollo11’s computer, says apple developer. Science Alert, Janural 12, 2020. Accessed July 4, 2024. https://www.sciencealert.com/apollo-11-s-computer-was-less-powerful-than-a-usb-c-charger-programmer-discovers
Elsayed, W. (2021). Covid-19 pandemic and its impact on increasing the risks of children’s addiction to electronic games from a social work perspective. Heliyon, 7(12). https://doi.org/10.1016/j.heliyon.2021.e08503
Engeln, R., & Zola, A. (2021). These boots weren’t made for walking: gendered discrepancies in wearing painful, restricting, or distracting clothing. Sex roles, 85(7), 463-480. https://doi.org/10.1007/s11199-021-01230-9
Fainmesser, I. P., Galeotti, A., & Momot, R. (2023). Digital privacy. Management Science, 69(6), 3157-3173. https://doi.org/10.1287/mnsc.2022.4513
Feinstein, J. S., Gould, D., & Khalsa, S. S. (2022). Amygdala-driven apnea and the chemoreceptive origin of anxiety. Biological psychology, 170, 108305. https://10.1016/j.biopsycho.2022.108305
Fiebert, I., Kistner, F., Gissendanner, C., & DaSilva, C. (2021). Text neck: An adverse postural phenomenon. Work, 69(4), 1261-1270. https://doi.org/10.3233/WOR-213547
Goodwin, R. D., Weinberger, A. H., Kim, J. H., Wu. M., & Galea, S. (2020). Trends in anxiety among adults in the United States, 2008–2018: Rapid increases among young adults. Journal of Psychiatric Research. 130, 441–446. https://doi.org/10.1016/j.jpsychires.2020.08.014
Gupta, N. (2023). Impact of smartphone overuse on health and well-being: review and recommendations for life-technology balance. Journal of Applied Sciences and Clinical Practice, 4(1), 4-12. https://doi.org/10.4103/jascp.jascp_40_22
Haghighat, F., Moradi, R., Rezaie, M., Yarahmadi, N., & Ghaffarnejad, F. (2020). Added Value of Diaphragm Myofascial Release on Forward Head Posture and Chest Expansion in Patients with Neck Pain: A Randomized Controlled Trial. Research Square. https://doi.org/10.21203/rs.3.rs-53279/v1
Haidt, J. (2024). The Anxious generation: How the great rewiring of childhood is causing an epidemic of mental illness. New York: Penguin Press. https://www.anxiousgeneration.com/book
Hansraj, K.K. (2014). Assessment of stresses in the cervical spine caused by posture and position of the head. Surg Technol Int. 25, 277-279. https://pubmed.ncbi.nlm.nih.gov/25393825/
Hernandez-de-Menendez, M., Escobar Díaz, C. A., & Morales-Menendez, R. (2020). Educational experiences with Generation Z. International Journal on Interactive Design and Manufacturing (IJIDeM), 14(3), 847-859. https://doi.org/10.1007/s12008-020-00674-9
Huh-Yoo, J., & Rader, E. (2020). It’s the Wild, Wild West: Lessons learned from IRB members’ risk perceptions toward digital research data. Proceedings of the ACM on Human-Computer Interaction, 4(CSCW1), 1-22. https://doi.org/10.1145/3392868
IIHS (2024). Fatality Facts 2022Pedestrians. The Insurance Institute for Highway Safety (IIHS). Accessed July 2, 2024. https://www.iihs.org/topics/fatality-statistics/detail/pedestrians
Kazeminasab, S., Nejadghaderi, S. A., Amiri, P., Pourfathi, H., Araj-Khodaei, M., Sullman, M. J., … & Safiri, S. (2022). Neck pain: global epidemiology, trends and risk factors. BMC musculoskeletal disorders, 23, 1-13. https://doi.org/10.1186/s12891-021-04957-4
Kim, K. H., Seo, H. J., Abdi, S., & Huh, B. (2020). All about pain pharmacology: what pain physicians should know. The Korean journal of pain, 33(2), 108-120. https://doi.org/10.3344/kjp.2020.33.2.108
Kushlev, K., & Leitao, M. R. (2020). The effects of smartphones on well-being: Theoretical integration and research agenda. Current opinion in psychology, 36, 77-82. https://doi.org/10.1016/j.copsyc.2020.05.001
Lewis, H.R. (2024). Mechanical intelligence and counterfeit humanity. Harvard Magazine, 126(6), 38-40. https://www.harvardmagazine.com/2024/07/harry-lewis-computers-humanity#google_vignette
Mark, G. (2023). Attention Span: A Groundbreaking Way to Restore Balance, Happiness and Productivity. Toronto, Canada: Hanover Square Press. https://www.amazon.com/Attention-Span-Finding-Fighting-Distraction-ebook/dp/B09XBJ29W9
Mason, M. C., Zamparo, G., Marini, A., & Ameen, N. (2022). Glued to your phone? Generation Z’s smartphone addiction and online compulsive buying. Computers in Human Behavior, 136, 107404. https://doi.org/10.1016/j.chb.2022.107404
McLaughlin, W.M., Cravez, E., Caruana, D.L., Wilhelm, C., Modrak, M., & Gardner, E.C. (2023). An Epidemiological Study of Cell Phone-Related Injuries of the Hand and Wrist Reported in United States Emergency Departments From 2011 to 2020. J Hand Surg Glob, 5(2),184-188. https://doi.org/10.1016/j.jhsg.2022.11.009
Meuret, A. E., Rosenfield, D., Millard, M. M., & Ritz, T. (2023). Biofeedback Training to Increase Pco2 in Asthma With Elevated Anxiety: A One-Stop Treatment of Both Conditions?. Psychosomatic medicine, 85(5), 440-448. https://doi.org/10.1097/PSY.0000000000001188
Miragall, M., Borrego, A., Cebolla, A., Etchemendy, E., Navarro-Siurana, J., Llorens, R., … & Baños, R. M. (2020). Effect of an upright (vs. stooped) posture on interpretation bias, imagery, and emotions. Journal of Behavior Therapy and Experimental Psychiatry, 68, 101560. https://doi.org/10.1016/j.jbtep.2020.101560
Mohan, A., Sen, P., Shah, C., Jain, E., & Jain, S. (2021). Prevalence and risk factor assessment of digital eye strain among children using online e-learning during the COVID-19 pandemic: Digital eye strain among kids (DESK study-1). Indian journal of ophthalmology, 69(1), 140-144. https://doi.org/10.4103/ijo.IJO_2535_20
Muchacka-Cymerman, A. (2022). ‘I wonder why sometimes I feel so angry’ The associations between academic burnout, Facebook intrusion, phubbing, and aggressive behaviours during pandemic Covid 19. Polish Psychological Bulletin, 53(4). https://doi.org/10.24425/ppb.2022.143376
Nakshine, V. S., Thute, P., Khatib, M. N., & Sarkar, B. (2022). Increased screen time as a cause of declining physical, psychological health, and sleep patterns: a literary review. Cureus, 14(10). https://doi.org/10.7759/cureus.30051
Nawaz, S., Bhowmik, J., Linden, T., & Mitchell, M. (2024). Validation of a modified problematic use of mobile phones scale to examine problematic smartphone use and dependence. Heliyon, 10(2). https://doi.org/10.1016/j.heliyon.2024.e24832
Nicholas, A. J. (2020). Preferred learning methods of generation Z. Faculty and Staff – Articles & Papers. Digital Commons @ Salve Regina. Salve Regina University. https://digitalcommons.salve.edu/fac_staff_pub/74
OHSU. (2022). Myopia on the rise, especially among children. Casey Eye Institute. Oregan Health and Science University. Accessed July 7, 2024. https://www.ohsu.edu/casey-eye-institute/myopia-rise-especially-among-children
Orsolini, L., Longo, G., & Volpe, U. (2023). The mediatory role of the boredom and loneliness dimensions in the development of problematic internet use. International Journal of Environmental Research and Public Health, 20(5), 4446. https://doi.org/10.3390/ijerph20054446
Pandey, R., Gaur, S., Kumar, R., Kotwal, N., & Kumar, S. (2020). Curse of the technology-computer related musculoskeletal disorders and vision syndrome: a study. International Journal of Research in Medical Sciences, 8(2), 661. https://doi.org/10.18203/2320-6012.ijrms20200253
Park, J. C., Kim, S., & Lee, H. (2020). Effect of work-related smartphone use after work on job burnout: Moderating effect of social support and organizational politics. Computers in human behavior, 105, 106194. https://doi.org/10.1016/j.chb.2019.106194
Paulus, M.P. (2013). The breathing conundrum-interoceptive sensitivity and anxiety. Depress Anxiety.30(4), 315-20. https://doi.org/10.1002/da.22076
Peper, E. (2021). Resolve eyestrain and screen fatigue. Well Being Journal, 30(1), 24-28. https://wellbeingjournal.com/resolve-eyestrain-and-screen-fatigue/
Peper, E., Booiman, A., Lin, I-M, Harvey, R., & Mitose, J. (2016). Abdominal SEMG Feedback for Diaphragmatic Breathing: A Methodological Note. Biofeedback. 44(1), 42-49. https://doi.org/10.5298/1081-5937-44.1.03
Peper, E., Chen, S., Heinz, N. & Harvey, R. (2023). Hope for menstrual cramps (dysmenorrhea) with breathing. Biofeedback, 51(2), 44–51. https://doi.org/10.5298/1081-5937-51.2.04
Peper, E., Harvey, R., Cuellar, Y., & Membrila, C. (2022). Reduce anxiety. NeuroRegulation, 9(2), 91–97. https://doi.org/10.15540/nr.9.2.91
Peper, E., Harvey, R. & Faass, N. (2020). TechStress: How Technology is Hijacking Our Lives, Strategies for Coping, and Pragmatic Ergonomics. Berkeley: North Atlantic Books. https://www.amazon.com/Beyond-Ergonomics-Prevent-Fatigue-Burnout/dp/158394768X
Peper, E., Harvey, R., & Mason, L. (2019). “Don’t slouch!” Improve health with posture feedback. Townsend Letter-The Examiner of Alternative Medicine, 436, 58-61. https://www.researchgate.net/publication/337424599_Don%27t_slouch_Improve_health_with_posture_feedback
Peper, E., Harvey, R., Mason, L., & Lin, I.-M. (2018). Do better in math: How your body posture may change stereotype threat response. NeuroRegulation, 5(2), 67–74. http://dx.doi.org/10.15540/nr.5.2.67
Peper, E., Harvey, R. & Rosegard, E. (2024). Increase attention, concentration and school performance with posture feedback. Biofeedback, 52(2). https://doi.org/10.5298/1081-5937-52.02.07
Peper, E. & Lin, I-M. (2012). Increase or decrease depression-How body postures influence your energy level. Biofeedback, 40 (3), 126-130. https://doi.org/10.5298/1081-5937-40.3.01
Peper, E., Lin, I-M, & Harvey, R. (2017a). Posture and mood: Implications and applications to therapy. Biofeedback, 35(2), 42-48. https://doi.org/10.5298/1081-5937-45.2.03
Peper, E., Lin, I-M., Harvey, R., & Perez, J. (2017). How posture affects memory recall and mood. Biofeedback.45 (2), 36-41. https://doi.org/10.5298/1081-5937-45.2.01
Peper, E., Mason, L., Harvey, R., Wolski, L, & Torres, J. (2020). Can acid reflux be reduced by breathing? Townsend Letters-The Examiner of Alternative Medicine, 445/446, 44-47. https://www.townsendletter.com/article/445-6-acid-reflux-reduced-by-breathing/
Quach, S., Thaichon, P., Martin, K. D., Weaven, S., & Palmatier, R. W. (2022). Digital technologies: tensions in privacy and data. Journal of the Academy of Marketing Science, 50(6), 1299-1323. https://doi.org/10.1007/s11747-022-00845-y
Resnik, D. B. (2021). Standards of evidence for institutional review board decision-making. Accountability in research, 28(7), 428-455. https://doi.org/10.1080/08989621.2020.1855149
Roggio, F., Ravalli, S., Maugeri, G., Bianco, A., Palma, A., Di Rosa, M., & Musumeci, G. (2021). Technological advancements in the analysis of human motion and posture management through digital devices. World journal of orthopedics, 12(7), 467. https://doi.org/10.5312/wjo.v12.i7.467
Sankaridurg, P., Tahhan, N., Kandel, H., Naduvilath, T., Zou, H., Frick,K.D., Marmamula, S., Friedman, D.S., Lamoureux, e. Keeffe, J. Walline, J.J., Fricke, T.R., Kovai, V., & Resnikoff, S. (2021) IMI Impact of Myopia. Invest. Ophthalmol. Vis. Sci, 62(5), 2. https://doi.org/10.1167/iovs.62.5.2
Satılmış, S. E., Cengız, R., & Güngörmüş, H. A. (2023). The relationship between university students’ perception of boredom in leisure time and internet addiction during social isolation process. Bağımlılık Dergisi, 24(2), 164-173. https://doi.org/10.51982/bagimli.1137559
Schenarts, P. J. (2020). Now arriving: surgical trainees from generation Z. Journal of surgical education, 77(2), 246-253. https://doi.org/10.1016/j.jsurg.2019.09.004
Schneider, M. (2016). Vision for life. Ten Steps to Natural Eyesight Improvement. Berkeley: North Atlantic books. https://www.amazon.com/Vision-Life-Revised-Eyesight-Improvement/dp/1623170087
Singapore National Eye Centre. (2024). Severe myopia cases among children in Singapore almost doubled in past decade. CAN. Accessed July 4, 2024. https://www.channelnewsasia.com/singapore/myopia-children-cases-almost-double-glasses-eye-checks-4250266
Smits, J. A., Monfils, M. H., Otto, M. W., Telch, M. J., Shumake, J., Feinstein, J. S., … & Exposure Therapy Consortium. (2022). CO2 reactivity as a biomarker of exposure-based therapy non-response: study protocol. BMC psychiatry, 22(1), 831. https://doi.org/10.1186/s12888-022-04478-x
STAT (2024). The society of teachers of the Alexander Technique. Assessed July 27, 2024. https://alexandertechnique.co.uk/
Stuart, S., Godfrey, A., & Mancini, M. (2022). Staying UpRight in Parkinson’s disease: A pilot study of a novel wearable postural intervention. Gait & Posture, 91, 86-93. https://doi.org/10.1016/j.gaitpost.2021.09.202
Swatzyna, R. (2023). Personal communications.
Szymkowiak, A., Melović, B., Dabić, M., Jeganathan, K., & Kundi, G. S. (2021). Information technology and Gen Z: The role of teachers, the internet, and technology in the education of young people. Technology in Society, 65, 101565. https://doi.org/10.1016/j.techsoc.2021.101565
Tsai, H. Y., Peper, E., & Lin, I. M.*(2016). EEG patterns under positive/negative body postures and emotion recall tasks. NeuroRegulation, 3(1), 23-27. https://doi.org/10.15540/nr.3.1.23
Van den Bergh, O., Zaman, J., Bresseleers, J., Verhamme, P., Van Diest, I. (2013). Anxiety, pCO2 and cerebral blood flow, International Journal of Psychophysiology, 89 (1), 72-77. https://doi.org/10.1016/j.ijpsycho.2013.05.011
Veritas Health. (2020). Text Neck Symptoms and Causes Video. YouTube video, accessed August 29, 2024. https://www.spine-health.com/conditions/neck-pain/how-does-text-neck-cause-pain?source=YT
Wennberg, P., Boraxbekk, C., Wheeler, M., et al. (2016). Acute effects of breaking up prolonged sitting on fatigue and cognition: a pilot study. BMJ Open, 6, e009630. https://doi.org/10.1136/bmjopen-2015-009630
Yang, K. H. (2022). Selling consumer data for profit: Optimal market-segmentation design and its consequences. American Economic Review, 112(4), 1364-1393. https://www.aeaweb.org/articles/pdf/doi/10.1257/aer.20210616
[1] Correspondence should be addressed to: Erik Peper, Ph.D., Institute for Holistic Health Studies, Department of Recreation, Parks, Tourism and Holistic Health, San Francisco State University, 1600 Holloway Avenue, San Francisco, CA 94132 Email: epeper@sfsu.edu; web: www.biofeedbackhealth.org; blog: www.peperperspective.com
[2] I thank Ronald Swatzyna (2023), Licensed Clinical Social Worker for sharing this exercise with me. He discovered that a difference in the number of eye contacts depending how he walked. When he walked a 3.1 mile loop around the park in a poor posture- shoulders forward, head down position- and then reversed direction and walked in good posture with the shoulders back and the head level, that that he make about 5 times as many eye contacts with good posture compared to the poor posture. He observed that he make about five times as many eye contacts with good posture as compared to the poor posture.
Increase attention, concentration and school performance
Posted: August 15, 2024 Filed under: ADHD, attention, behavior, Breathing/respiration, digital devices, education, ergonomics, posture, screen fatigue, stress management, vision, zoom fatigue | Tags: cellphone, concentration 5 CommentsReproduced from: Peper, E., Harvey, R., & Rosegard, E. (2024). Increase attention, concentration and school performance with posture feedback. Biofeedback, 52(2), 48-52. https://doi.org/10.5298/1081-5937-52.02.07

When I sit with good posture on my computer, I am significantly more engaged in what I’m doing. When I slouch on my computer I tend to procrastinate, go on my phone, and get distracted so it ends up taking much longer to do my work when my posture is bad.…I have ADHD and I struggle a lot with my mind wandering when I should be paying attention. Having good posture really helps me to lock in and focus.—22 year old male student.
Over the past two decades, there has been a significant increase in the prevalence of attention-deficit/hyperactivity disorder (ADHD), anxiety, and depression. ADHD rates have increased from 6% in 1997 to approximately 10% in 2018 (CDC, 2022). The rates of anxiety among 18–25 year-olds have also increased from 7.97% in 2008 to 14.66% in 2018 (Goodwin et al., 2020). Students are more distracted, stressed and exhausted (Hanscom, 2022; Hoyt et al., 2021). The more students are distracted, the lower their academic achievement (Feng et al., 2019). In our recent class survey of more than 100 junior and senior college students on the first day of class, 54% reported that they were tired and dreading the day when they woke up. When you are tired and stressed it is difficult to focus attention and have clarity of thought. Their self-report is similar to the mental health trends in the United States by age group in 2008–2019. Mental health of young people has significantly deteriorated over the last 15 years (Braghieri et al., 2021/2023).
The increase in psychological distress is most prevalent in people ages 18–29 and who were brought up with the cellphone (the iPhone was introduced in 2007) and social media. Now when students enter a class, they tend to sit down, look down at their cellphone while slouching, and they do not make contact with most other students unless instructed or reminded by the instructor. When instructed to talk to another student for less than 5 minutes (e.g., share something positive that happened to you this week), 93% of the students reported an increase in subjective energy and alertness (Peper, 2024).
As a group, students are social media and cell phone natives and thus have many distractions and stimuli to which they continuously respond. It is not surprising that the average attention span has decreased from 150 seconds in 2004 to 44 seconds in 2021 (Mark, 2023). More importantly, they now tend to sit in a slouched collapsed position, which facilitates access to hopeless, helpless, powerless and defeated thoughts and memories (Tsai et al., 2016; Peper et al., 2017) and reduces cognitive performance when performing mental math (Peper et al., 2018). Sitting slouched and looking down also reduces peripheral awareness and increases shallow thoracic breathing—a breathing pattern that increases the risk of anxiety. Experience this yourself.
For a minute, look at your cellphone while intensely reading the text or searching social media in the following two positions: sitting straight up and looking straight ahead at your cell phone or slouching and looking down at your cell phone, as shown in Figure 1. Most likely, your experience is similar to the findings from the classroom observational study in which half the students looked down and the other half looked straight ahead and then reversed their positions (Peper, unpublished). They then compared the subjective experience associated with the position. In the slouched position, most experienced a reduction in peripheral awareness and breathed more shallowly (see Figure 1).
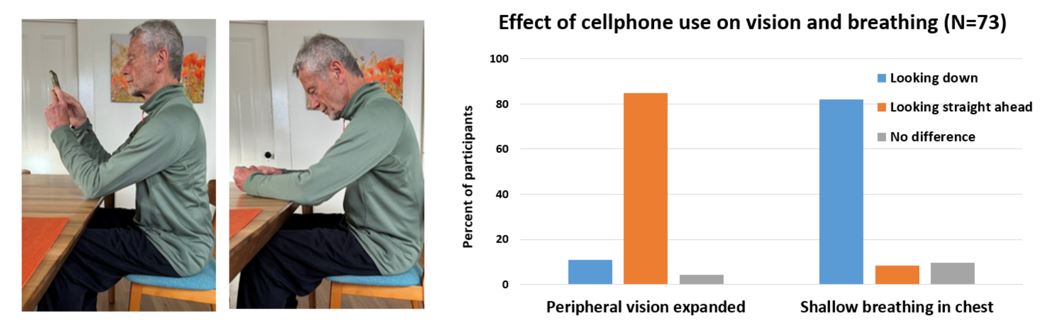
Figure 1. Effect of slouching or looking straight ahead on vision and breathing.
The slouched position reduces social awareness and decreases awareness of external stimuli as illustrated in Steve Cutts’ superb animation, Mobile world (https://www.youtube.com/watch?v=wUW1wjlKvmY).
Given the constant stimulation, distractions and shortened attention span, it is more challenging to be calm and have clarity of mind when having to study or take an exam at school. As educators, we constantly explore ways to engage students and support their learning and especially share quick skills they can use to optimize performance (Peper& Wilson, 2021). In previous research, Harvey et al., 2020 showed that students who used posture feedback improved their health scores compared to the control group. The purpose of this paper is to share a 4-week class assignment by which numerous students reported an increase in attention, concentration, confidence, school performance and a decrease in stress.
Participants: 18 undergraduate students (7 males and 11 females, average age 22 [STDEV 2.2]) enrolled in an upper division class. As a report about an effort to improve the quality of a classroom activity, this report of findings was exempted from Institutional Review Board oversight.
Equipment: Wearable posture feedback device, UpRight Go 2, which the person wears on their neck and which provides vibratory feedback whenever they slouch, as shown in Figure 2. It is used in conjunction with the cellphone app that allows them to calibrate the feedback device.

Figure 2. Attachment of posture feedback device on neck or spine and the app to calibrate the device.
Procedure: Students attended the 3-hour weekly class that explored autogenic training, somatic awareness, psychobiology of stress, the role of posture, and the psychophysiology of respiration. The lectures included short experiential practices demonstrating the body-mind connections such as imagining a lemon to increase salivation, the effect of slouched versus erect posture on evoking positive/empowering or hopeless/helpless/powerless/defeated thoughts, and the effect of sequential 70% exhalation for 30 seconds on increasing anxiety (Tsai et al., 2016; Peper et al., 2017).
Each week for 4 weeks the students were assigned a self-practice that they would implement daily at home and record their experiences. At the end of the week, they reviewed their own log and summarized their own observations (benefits, difficulties). During the next class session, they met in small groups of 5 to 6 students to discuss their experiences and extract common themes.
The 4-week curriculum was sequenced as follows:
Week 1
- Lecture on the benefits/harms of posture with experiential practices (effect of slouching vs erect on access to hopeless/helpless/powerless thoughts versus optimistic and empowering thoughts; posture and arm strength (Peper, 2022).
- Homework assignments:
- Watch the great Ted Talk and one of the most viewed by Amy Cuddy (2013), “Your body language shapes who you are.”
- Keep a detailed log to monitor situations where they slouched and identify situations that were associated with slouching.
Week 2
- Lecture on psychophysiology and class discussion in which students shared their experiences of slouching; namely, what were the triggers, how it affected them and what they could do to change.
- Demonstration, explanation, and how to use the posture feedback device, UpRight Go 2.
- Homework assignment: Wear UpRight Go 2 during the day, use it in different settings (studying, walking, work), and keep a log. When it vibrates (slouching) observe what was going on and change your behavior such as when tired>get rest or do exercise; when depressed>change internal language; ergonomic issues>change the environment, posture>give yourself lower back support.
Week 3
- Class discussion on what to do when slouching is triggered by tiredness, negative and hopeless thoughts, ergonomics such as laptop placement and chair. Students meet in groups to share their experiences and what they did in response to the vibratory feedback.
- Homework assignment: Continue to wear the UpRight Go 2 during the day and keep a log.
Week 4
- Class discussion in groups of five students about their experiences of slouching, what to do and how it affects them.
- Homework assignment: Wear UpRight Go 2 during the day and keep a log. Submit a paper that describes their experience with the posture feedback from the UpRight Go 2 and fill out a short anonymous survey in which they rated their change in experience since using the posture feedback device on a scale from 3 (worse) to 0 (no change) to 3 (better) .
Results
All students reported that wearing the feedback device increased attention and concentration as shown in Figure 3.

Figure 3.
Amount of time using the UpRight Go 2:On the average the students used the device 4.8 days a week (STDEV 2.0) and 2.2 hours per day (STDEV 1.3).
Location of use:Although most students practiced sitting in front of their computer, they also reported using it while at work, playing pool or doing yoga and even while seeing a therapist.
Discussion
All the students reported that the posture feedback helped them to become more aware of slouching and when they then interrupted their slouching, they experienced an increase in energy and a decrease in stress. As a 21-year-old male student said: “I felt more engaged with whatever I was doing. I tend to … daydream and get distracted, but I experience much less of that when I sit with good posture.”
Many reported that it helped identify their emotions when they were feeling overwhelmed. Then they could sit up, shift their perspective, and many reported a decrease in back and neck pain as well as a decrease in tiredness. When participants wear non-invasive wearables that provide accurate feedback, they are often surprised what triggers are associated with feedback or how their performance improves when they respond to the feedback signal by changing their thoughts and behavior. This posture self-awareness project should be embedded in strategies that optimize the learning state as described by Peper & Wilson (2021).
To the students’ surprise, they were often unaware that they started to slouch, nor were they aware of how much this slouching was connected to their emotions, mental state or external factors. For example, one student reported that he wore the device while being in a therapy session. All of a sudden, it vibrated. At that moment, he realized that he was becoming anxious, although he and therapist were unaware. He then shared what happened with the therapist, and that helped the therapeutic process.
The benefits may not only be due to posture change but that the students became aware and interrupted their habitual pattern. This process is similar to that described by Charles Stroebel (1985) when he taught patients the Quieting Reflect that reduced numerous somatic symptoms ranging from headaches to hypertension.
The posture feedback intervention is both simple and challenging since it requires the participants to wear the device, identify factors that trigger the slouching, and interrupt their automatic patterns by changing posture and behavior whenever they felt the vibratory feedback. The awareness gave them the opportunity to change posture and thoughts. By shifting to an upright posture, they experienced that they could concentrate more and have increased energy. As a 19-year-old female student wrote: “My breathing was better and sitting in an upright position gave me more energy when doing tasks.”
Conclusion
We recommend that a 4-week home practice module that incorporates wearable posture feedback is offered to all students to enhance their well-being. With the posture feedback, participants can increase their awareness of slouching, identify situations that trigger slouch, and learn strategies to shift their posture, thoughts, emotions and external environment to optimize maintaining an empowered position. As a 20-year old male student reported, “The app helped me when I was feeling overwhelmed and then I would sit up. When I had it on, I did a lot of work. I was more concentrated.”
Explore the following blogs for more background and useful suggestions
References
Braghieri, L., Levy, R., & Makarin, A. (2023). Media and mental health (July 28, 2022). SSRN. (Original work published 2021). https://ssrn.com/abstract=3919760 or http://dx.doi.org/10.2139/ssrn.3919760
Centers for Disease Control and Prevention. (n.d.). ADHD through the years. Attention-Deficit / Hyperactivity Disorder (ADHD). Retrieved March 27, 2023, from https://www.cdc.gov/ncbddd/adhd/timeline.html
Cuddy, A. (2012) Your body language may shape who you are. TED Talk. Retrieved March 16, 2024 from https://www.youtube.com/watch?v=Ks-_Mh1QhMc
Feng, S., Wong, Y. K., Wong, L. Y., & Hossain, L. (2019). The internet and Facebook usage on academic distraction of college students, Computers & Education, 134, 41-49. https://doi.org/10.1016/j
Goodwin, R. D., Weinberger, A. H., Kim, J. H., Wu. M., & Galea, S. (2020). Trends in anxiety among adults in the United States, 2008–2018: Rapid increases among young adults. Journal of Psychiatric Research. 130, 441–446. https://doi.org/10.1016/j.jpsychires.2020.08.014
Hanscom, N. (2022). Students, staff notice higher levels of student distraction this school year, reflect on potential causes. Retrieved September 28, 2023, from https://dgnomega.org/13162/feature/students-staff-notice-higher-levels-of-student-distraction-this-school-year-reflect-on-potential-causes/
Harvey, R., Peper, E., Mason, L., & Joy, M. (2020). Effect of posture feedback training on health. Applied Psychophysiology and Biofeedback, 45(1), 59–65. https://doi.org/10.1007/s10484-020-09457-0
Hoyt, L. T., Cohen, A. K., Dull, B., Castro, E. M., & Yazdani, N. (2021). “Constant stress has become the new normal”: Stress and anxiety inequalities among U.S. college students in the time of COVID-19. Journal of Adolescent Health. 68(2), 270–276. https://doi.org/10.1016/j.jadohealth.2020.10.030
Mark, G. (2023). Attention span: A groundbreaking way to restore balance, happiness and productivity. Hanover Square Press.
Peper, E. (2022, March 4). A breath of fresh air: Breathing and posture to optimize health. [Conference presentation at the 2nd Virtual Ergonomics Summit], Krista Burns, PhD. https://www.youtube.com/watch?v=PhV7Ulhs38s
Peper, E. (2024a). Change in energy and alertness after talking with each other versus looking at cellphone. Data collected from HH380 class fall 2023. Unpublished.
Peper, E. (2024b). Changes in vision and breathing when looking down or straight ahead at the cellphone. Data collected from HH380 class, Spring, 2024, San Francisco State University. Unpublished.
Peper, E., Harvey, R., Mason, L., & Lin, I.-M. (2018). Do better in math: How your body posture may change stereotype threat response. NeuroRegulation, 5(2), 67–74. http://dx.doi.org/10.15540/nr.5.2.67
Peper, E., Lin, I.-M., Harvey, R., & Perez, J. (2017). How posture affects memory recall and mood. Biofeedback.45(2), 36–41. https://doi.org/10.5298/1081-5937-45.2.01
Peper, E. & Wilson, V. (2021). Optimize the learning state: Techniques and habits. Biofeedback, 49(2), 46-49. https://doi.org/10.5298/1081-5937-49-2-04
Stroebel, C. F. (1985). QR: The Quieting Reflex. Berkley. https://www.amazon.com/Qr-Quieting-Charles-M-D-Stroebel/dp/0399126570
Tsai, H. Y., Peper, E., & Lin, I.-M.(2016). EEG patterns under positive/negative body postures and emotion recall tasks. NeuroRegulation, 3(1), 23–27. https://doi.org/10.15540/nr.3.1.23
Grandmother Therapy: A Common-Sense Approach to Health and Wellness
Posted: July 24, 2024 Filed under: ADHD, attention, behavior, education, Evolutionary perspective, Exercise/movement, Nutrition/diet, Pain/discomfort, relaxation, self-healing | Tags: anxiety, depression, epilepsy, exhaustion, grandmother therapy, health, insomnia, life style change, mental-health, therapy 1 CommentErik Peper, PhD and Angelika Sadar, MA

In today’s fast-paced world, college students and young adults often struggle with various health issues. From anxiety and depression to ADHD and epilepsy, these challenges can significantly impact their daily lives. But what if the solution to many of these problems lies in something as simple as “Grandmother Therapy”?
What is Grandmother Therapy? Grandmother Therapy is all about going back to basics and establishing healthy lifestyle habits. It’s the common-sense approach that our grandmothers might have suggested: regular sleep patterns, balanced nutrition, increased social connections, and regular physical activity.
The Problem: Many college students:
- Skip breakfast before their first class
- Rely on fast food and sugary stimulants
- Have irregular sleep schedules
- Spend excessive time on gaming and social media
The Medical Approach: Often, the quick solution is medication:
- Depression? Take antidepressants.
- Insomnia? Use sleeping pills.
- Anxiety? Try anti-anxiety medication.
- ADHD? Prescribe Ritalin or similar drugs.
While these treatments may help manage symptoms, they often overlook the underlying lifestyle factors contributing to these issues.
The Grandmother Therapy Approach:
- Establish regular sleep patterns
- Adopt healthy eating habits
- Increase social connections
- Incorporate regular physical activity
- Reduce gaming and social media use
Case Study #1: The Power of Sleep
This illustrates the simple intervention of having a bedtime routine. A college student in a holistic health class complained that she was tired most of the time and had difficulty focusing her attention and continuously drifted off in class.
Here is her reported sleep schedule:
- last night I went to bed at 3am and woke up 7;
- the day before, I went to bed at 1pm and woke up at 6,
- two nights before, I went to bed at 4pm and woke up at 10 am.
Holistic treatment approach:
Set a sleep schedule: she was provided with information about the importance of having a regular pattern of sleep and waking. Namely, go to bed at the same time and get up 8 hours later. She agreed to do an experiment for a week to go to bed at 12 and wake up at 8m. To her surprise, she felt so much more energized and could pay attention in class during the week of the experiment.
Case Study #2: Beyond Seizures: A Holistic Approach to Treating Psychogenic Nonepileptic Seizures
This case study highlights the importance of a comprehensive, lifestyle-based approach to treating psychogenic nonepileptic seizures (PNES). It follows a 24-year-old male student initially diagnosed with intractable epilepsy, experiencing over 10 seizures per week that didn’t respond to medication.
Key points:
1. Initial misdiagnosis: Despite normal MRI and EEG results, the client was initially treated for epilepsy.
2. Limited assessment: Traditional medical evaluations focused solely on seizure descriptions and diagnostics, overlooking crucial lifestyle factors.
3. Comprehensive evaluation: A psychophysiological assessment revealed high sympathetic arousal, including rapid breathing, sweaty palms, and muscle tension.
4. Lifestyle factors: The client’s diet consisted of high-glycemic fast foods, excessive caffeine, alcohol, and daily marijuana use. He also had significant student debt and a history of abdominal surgery.
Holistic treatment approach:
– Dietary changes: Switching to unprocessed, low-glycemic foods and increasing vegetable and fruit intake
– Breathing techniques: Learning and practicing slow diaphragmatic breathing
– Stress management: Addressing underlying stressors and practicing relaxation techniques
– Supplements: Adding omega-3 and multivitamins to support brain health
Remarkable results: Within four months, the patient became seizure-free, reduced marijuana use significantly, and decreased medication dosage.
Summary
These cases underscore the potential of integrating lifestyle modifications and stress management techniques in treating attention, anxiety and even psychogenic nonepileptic seizures; offering hope for patients who don’t respond to traditional treatments alone. Before turning to medication or complex treatments, consider the power of Grandmother Therapy. By addressing fundamental lifestyle factors, we can often improve our health and well-being significantly. Remember, sometimes the most effective solutions are the simplest ones.
The Challenges of Simplicity: While Grandmother Therapy may seem straightforward, its simplicity can make it challenging to implement. It requires commitment and a willingness to change long-standing habits.
Implement many Life Style Changes at once: Recommending one change at the time is logical; however, participants will more likely experience rapid benefits and are more motivated to continue when they change multiple lifestyle factors at once.
Call to Action: Are you struggling with health issues? Try implementing some aspects of Grandmother Therapy in your life. Implement changes and see how they impact your overall well-being.
Please let us know your experience with implementing Grandmother Therapy.
See the following blogs for more background information
A Must read: The Anxious Generation by Jonathan Haidt
Posted: July 11, 2024 Filed under: ADHD, attention, behavior, computer, digital devices, education, Evolutionary perspective, health, screen fatigue, Uncategorized | Tags: addiction, books, cellphones, child development, gaming, jonathan-haidt, mental-health, smartphone, social media, streaming videos; blog posts, technology, texting 3 CommentsDo you wonder why mental health of teenagers plunged in the in the early 2010s (e.g., increase in anxiety, depression, suicidal thoughts) with a decrease in actual social interactions (e.g., dating or leaving home to live independently)? I was aware of, and have done research on, the negative impact of smartphones and other screens such as the hours of scrolling social media, gaming, texting, watching streaming videos or user generated videos on Instagram, TicTok, YouTube. When decreasing phone use, health, well-being and productivity often improves. Illustrated by the report of a 23-year male student who choose to reduce his smartphone use from more than 7 hours to three hours per day for five weeks as part of a class project.
When I observed that I used my phone 7 hours and 38 minutes a day, I was a bit ashamed; since, I believe this time could be used more efficiently. I believed what really made my anxiety higher than normal was being stuck in a loop. I felt my brain so wired to mindlessly scrolling on my phone.
For my self-healing project, my goal was to spend no more than 1 hour daily on social apps. As a result, I lowered my phone use to less than 3 hours each day for five weeks. By the third week of this practice, I have begun to find it easier. I now place my phone in another room so that I can focus on my assignments. I once again found myself being more productive but I also felt another benefit. Improved sleep quality. Previously, I tended to use the phone right before bed. By cutting down on usage, especially in the evening, I find it easier to fall asleep.
I’ve began to feel comfortable with putting my phone away and hanging out more with friends in person. I’ve notice that when I’m out in public I’m less shy and more open to people. Constantly checking my phone detracted from being fully present in the moment. I am more engaged in face-to-face interactions with friends, family, and colleagues, and strengthening connections. I’ve also experienced improvements in my passion. I find it much easier to come up with more creative ideas when writing and brainstorming ideas in film for my class. I am glad with the positive effects resulting from decrease by phone use. It opened my eyes to the negative impact of smartphones.
Read Jonathan Haidt’s superb book, Anxious Generation-How the great rewiring of childhood is causing an epidemic of mental illness, and implement his pragmatic suggestions to support the development of health and well-being of young people. Phone use is only part of the problem. The other is the shift in the American culture from “play-based childhood” to “phone-based childhood”. As Jonathan Haidt points thetwo trends-overprotection in the real world and underprotection in the virtual world-are the major reasons why children born after 1995 became the anxious generation.

Explore the following blogs for more background and useful suggestions
Reflections on the increase in Autism, ADHD, anxiety and depression: Part 2- Exposure to neurotoxins and ultra-processed foods
Posted: June 30, 2024 Filed under: ADHD, attention, behavior, CBT, digital devices, education, emotions, Evolutionary perspective, health, mindfulness, neurofeedback, Nutrition/diet, Uncategorized | Tags: ADHD, anxiety, depression, diet, glyphosate, herbicide, herbicites, mental-health, neurofeedback, pesticides, supplements', ultraprocessed foods, vitamins 4 CommentsAdapted from: Peper, E. & Shuford, J. (2024). Reflections on the increase in Autism, ADHD, anxiety and depression: Part 2- Exposure to neurotoxins and ultra-processed foods. NeuroRegulation, 11(2), 219–228. https://doi.org/10.15540/nr.11.2.219
Look at your hand and remember that every cell in your body including your brain is constructed out the foods you ingested. If you ingested inferior foods (raw materials to be built your physical structure), then the structure can only be inferior. If you use superior foods, you have the opportunity to create a superior structure which provides the opportunity for superior functioning. -Erik Peper
Summary
Mental health symptoms of attention deficit hyperactivity disorder (ADHD), Autism, anxiety and depression have increased over the last 15 years. An additional risk factor that may affect mental and physical health is the foods we eat. Even though, our food may look and even taste the same as compared to 50 years ago, it contains herbicide and pesticide residues and often consist of ultra-processed foods. These foods (low in fiber, and high in sugar, animal fats and additives) are a significant part of the American diet and correlate with higher levels of inattention and hyperactivity in children with ADHD. Due to affluent malnutrition, many children are deficient in essential vitamins and minerals. We recommend that before beginning neurofeedback and behavioral treatments, diet and lifestyle are assessed (we call this Grandmother therapy assessment). If the diet appears low in organic foods and vegetable, high in ultra-processed foods and drinks, then nutritional deficiencies should be assessed. Then the next intervention step is to reduce the nutritional deficiencies and implement diet changes from ultra-processed foods to organic whole foods. Meta-analysis demonstrates that providing supplements such as Vitamin D, etc. and reducing simple carbohydrates and sugars and eating more vegetables, fruits and healthy fats during regular meals can ameliorate the symptoms and promote health.
The previous article and blog, Reflections on the increase in Autism, ADHD, anxiety and depression: Part 1-bonding, screen time, and circadian rhythms, pointed out how the changes in bonding, screen time and circadian rhythms affected physical and mental health (Peper, 2023a; Peper, 2023b). However, there are many additional factors including genetics that may contribute to the increase is ADHD, autism, anxiety, depression, allergies and autoimmune illnesses (Swatzyna et al., 2018). Genetics contribute to the risk of attention deficit hyperactivity disorder (ADHD); since, family, twin, and adoption studies have reported that ADHD runs in families (Durukan et al., 2018; Faraone & Larsson, 2019). Genetics is in most cases a risk factor that may or may not be expressed. The concept underlying this blog is that genetics loads the gun and environment and behavior pulls the trigger as shown in Figure 1.

Figure 1. Interaction between Genetics and Environment
The pandemic only escalated trends that already was occurring. For example, Bommersbach et al (2023) analyzed the national trends in mental health-related emergency department visits among USA youth, 2011-2021. They observed that in the USA, Over the last 10 years, the proportion of pediatric ED visits for mental health reasons has approximately doubled, including a 5-fold increase in suicide-related visits. The mental health-related emergency department visits increased an average of 8% per year while suicide related visits increased 23.1% per year. Similar trends have reported by Braghieri et al (2022) from the National Survey on Drug Use and Health as shown in Figure 2.

Figure 2. Mental health trends in the United States by age group in 2008–2019. The data come from the National Survey on Drug Use and Health. Reproduced with permission from Braghieri, Luca and Levy, Ro’ee and Makarin, Alexey, Social Media and Mental Health (July 28, 2022) https://ssrn.com/abstract=3919760 or http://dx.doi.org/10.2139/ssrn.3919760
The trends reported from this data shows an increase in mental health illnesses for young people ages 18-23 and 24-29 and no changes for the older groups which could be correlated with the release of the first iPhone 2G on June 29, 2007. Thus, the Covid 19 pandemic and social isolation were not THE CAUSE but an escalation of an ongoing trend. For the younger population, the cellphone has become the vehicle for personal communication and social connections, many young people communicate more with texting than in-person and spent hours on screens which impact sleep (Peper, 2023a). At the same time, there are many other concurrent factors that may contributed to increase of ADHD, autism, anxiety, depression, allergies and autoimmune illnesses.
Without ever signing an informed consent form, we all have participated in lifestyle and environmental changes that differ from that evolved through the process of evolutionary natural selection and promoted survival of the human species. Many of those changes in lifestyle are driven by demand for short-term corporate profits over long-term health of the population. As exemplified by the significant increase in vaping in young people as a covert strategy to increase smoking (CDC, 2023) or the marketing of ultra-processed foods (van Tulleken, 2023).
This post focusses how pesticides and herbicides (exposure to neurotoxins) and changes in our food negatively affects our health and well-being and is may be another contributor to the increase risk for developing ADHD, autism, anxiety and depression. Although our food may look and even taste the same compared to 50 years ago, it is now different–more herbicide and pesticide residues and is often ultra-processed. lt contains lower levels of nutrients and vitamins such as Vitamin C, Vitamin B2, Protein, Iron, Calcium and Phosphorus than 50 years ago (Davis et al, 2004; Fernandez-Cornejo et al., 2014). Non-organic foods as compared to organic foods may reduce longevity, fertility and survival after fasting (Chhabra et al., 2013).
Being poisoned by pesticide and herbicide residues in food
Almost all foods, except those labeled organic, are contaminated with pesticides and herbicides. The United States Department of Agriculture reported that “Pesticide use more than tripled between 1960 and 1981. Herbicide use increased more than tenfold (from 35 to 478 million pounds) as more U.S. farmers began to treat their fields with these chemicals” (Fernandez-Cornejo, et al., 2013, p 11). The increase in herbicides and pesticides is correlated with a significant deterioration of health in the United States (Swanson, et al., 2014 as illustrated in the following Figure 3.


Figure 3. Correlation between Disease Prevalence and Glyphosate Applications (reproduced with permission from Swanson et al., 2014.
Although correlation is not causation and similar relationships could be plotted by correlating consumption of ultra-refined foods, antibiotic use, decrease in physical activity, increase in computer, cellphone and social media use, etc.; nevertheless, it may suggest a causal relationship. Most pesticides and herbicides are neurotoxins and can accumulate in the person over time this could affect physical and mental health (Bjørling-Poulsen et al., 2008; Arab & Mostaflou, 2022). Even though the United States Environmental Protection Agency (EPA) has determined that the residual concentrations in foods are safe, their long-term safety has not been well established (Leoci & Ruberti, 2021). Other countries, especially those in which agribusiness has less power to affect legislation thorough lobbying, and utilize the research findings from studies not funded by agribusiness, have come to different conclusions…
For example, the USA allows much higher residues of pesticides such as, Round-Up, with a toxic ingredient glyphosate (0.7 parts per million) in foods than European countries (0.01 parts per million) (Wahab et al., 2022; EPA, 2023; European Commission, 2023) as is graphically illustrated in figure 4.

Figure 4: Percent of Crops Sprayed with Glyphosate and Allowable Glyphosate Levels in the USA versus the EU
The USA allows this higher exposure than the European Union even though about half of the human gut microbiota are vulnerable to glyphosate exposure (Puigbo et al., 2022). The negative effects most likely would be more harmful in a rapidly growing infant than for an adult. Most likely, some individuals are more vulnerable than others and are the “canary in mine.” They are the early indicators for possible low-level long-term harm. Research has shown that fetal exposure from the mother (gestational exposure) is associated with an increase in behaviors related to attention-deficit/hyperactivity disorders and executive function in the child when they are 7 to 12 years old (Sagiv et al., 2021). Also, organophosphate exposure is correlated with ADHD prevalence in children (Bouchard et al., 2010). We hypothesize this exposure is one of the co-factors that have contributed to the decrease in mental health of adults 18 to 29 years.
At the same time as herbicides and pesticides acreage usage has increased, ultra-processed food have become a major part of the American diet (van Tulleken, 2023). Eating a diet high in ultra-processed foods, low in fiber, high sugar, animal fats and additives has been associated with higher levels of inattention and hyperactivity in children with ADHD; namely, high consumption of sugar, candy, cola beverages, and non-cola soft drinks and low consumption of fatty fish were also associated with a higher prevalence of ADHD diagnosis (Ríos-Hernández et al., 2017).
In international studies, less nutritional eating behaviors were observed in ADHD risk group as compared to the normal group (Ryu et al., 2022). Artificial food colors and additives are also a public health issue and appear to increase the risk of hyperactive behavior (Arnold et al., 2012). In a randomized double-blinded, placebo controlled trial 3 and 8/9 year old children had an increase in hyperactive behavior for those whose diet included extra additives (McCann et al., 2007). The risk may occur during fetal development since poor prenatal maternal is a critical factor in the infants neurodevelopment and is associated with an increased probability of developing ADHD and autism (Zhong et al., 2020; Mengying et al., 2016).
Poor nutrition even affects your unborn grandchild
Poor nutrition not only affects the mother and the developing fetus through epigenetic changes, it also impacts the developing eggs in the ovary of the fetus that can become the future granddaughter (Wilson, 2015). At birth, the baby has all of her eggs. Thus, there is a scientific basis for the old wives tale that curses may skip a generation. Providing maternal support is even more important since it affects the new born and the future grandchild. The risk may even begin a generation earlier since the grandmother’s poor nutrition as well as stress causes epigenetic changes in the fetus eggs. Thus 50% of the chromosomes of the grandchild were impacted epigenetically by the mother’s and grandmother’s dietary and health status .
Highly processed foods
Highly refined foods have been processed to remove many of their nutrients. These foods includes white bread, white rice, pasta, and sugary drinks and almost all the fast foods and snacks. These foods are low in fiber, vitamins, and minerals, and they are high in sugars, unhealthy fats, and calories. In addition, additives may have been added to maximize taste and mouth feel and implicitly encourage addiction to these foods. A diet high in refined sugars and carbohydrates increases the risk of diabetes and can worsen the symptoms of ADHD, autism, depression, anxiety and increase metabolic disease and diabetes (Woo et al., 2014; Lustig, 2021; van Tulleken, 2023). Del-Ponte et al. (2019) noted that a diet high in refined sugar and saturated fat increased the risk of symptoms of ADHD, whereas a healthy diet, characterized by high consumption of fruits and vegetables, would protect against the symptoms.
Most likely, a diet of highly refined foods may cause blood sugar to spike and crash, which can lead to mood swings, irritability, anxiety, depression and cognitive decline and often labeled as “hangryness” (the combination of anger and hunger) (Gomes et al., 2023; Barr et al., 2019). At the same time a Mediterranean diet improves depression significantly more than the befriending control group (Bayles et al., 2022). In addition, refined foods are low in essential vitamins and minerals as well as fiber. Not enough fiber can slow down digestion, affect the human biome, and makes it harder for the body to absorb nutrients. This can lead to nutrient deficiencies, which can contribute to the symptoms of ADHD, autism, depression, and anxiety. Foods do impact our mental and physical health as illustrated by foods that tend to reduce depression (LaChance & Ramsey, 2018; MacInerney et al., 2017). By providing appropriate micronutrients such as minerals (Iron, Magnesium Zinc), vitamins (B6, B12, B9 and D), Omega 3s (Phosphatidylserine) and changing our diet, ADHD symptoms can be ameliorated.
Many children with ADHD, anxiety, depression are low on essential vitamins and minerals. For example, low levels of Omega-3 fatty acids and vitamin D may be caused by eating ultra-refined foods, fast foods, and drinking soft drink. At the same time, the children are sitting more in indoors in front of the screen and thereby have lower sun exposure that is necessary for the vitamin D production.
“Because of lifestyle changes and sunscreen use, about 42% of Americans are deficient in vitamin D. Among children between 1 to 11 years old, an estimated 15% have vitamin D deficiency. And researchers have found that 17% of adolescents and 32% of young adults were deficient in vitamin D.” (Porto and Abu-Alreesh, 2022).
Reduced sun exposure is even more relevant for people of color (and older people); since, their darker skin (increased melanin) protects them from ultraviolet light damage but at the same time reduces the skins production of vitamin D. Northern Europeans were aware of the link between sun exposure and vitamin D production. To prevent rickets (a disease caused by vitamin D deficiency) and reduce upper respiratory tract infections the children were given a tablespoon of cod liver oil to swallow (Linday, 2010). Cod liver oil, although not always liked by children, is more nutritious than just taking a Vitamin D supplements. It is a whole food and a rich source of vitamin A and D as well as containing a variety of Omega 3 fatty acids (eicosapentaenoic acid (EPA) (USDA, 2019).
Research studies suggest that ADHD can be ameliorated with nutrients, and herbs supplements (Henry & CNS, 2023). Table 1 summarizes some of the nutritional deficits observed and the reduction of ADHD symptoms when nutritional supplements were given (adapted from Henry, 2023; Henry & CNS, 2023).
| Nutritional deficits observed in people with ADHD | Decrease in ADHD symptoms with nutritional supplements |
| Vitamin D: In meta-analysis with a total number of 11,324 children, all eight trials reported significantly lower serum concentrations of 25(OH)D in patients diagnosed with ADHD compared to healthy controls. (Kotsi et al, 2019) | After 8 weeks children receiving vitamin D (50,000 IU/week) plus magnesium (6 mg/kg/day) showed a significant reduction in emotional problems as observed in a randomized, double blind, placebo-controlled clinical trial (Hemamy et al., 2021). |
| Iron: In meta-analysis lower serum ferritin was associated with ADHD in children (Wang et al., 2017) and the mean serum ferritin levels are lower in the children with ADHD than in the controls (Konofal et al., 2004). | After 12 weeks of supplementation with Iron (ferrous sulfate) in double-blind, randomized placebo-controlled clinical trial, clinical trials symptoms of in children with ADHD as compared to controls were reduced (Tohidi et al., 2021; Pongpitakdamrong et all, 2022). |
| Omega 3’s: Children with ADHD are more likely to be deficient in omega 3’s than children without ADHD (Chang et al., 2017). | Adding Omega-3 supplements to their diet resulted in an improvement in hyperactivity, impulsivity, learning, reading and short term memory as compared to controls in 16 randomized controlled trials including 1514 children and young adults with ADHD (Derbyshire, 2017) |
| Magnesium: In meta-analysis, subjects with ADHD had lower serum magnesium levels compared with to their healthy controls (Effatpahah et al., 2019) | 8 weeks of supplementation with Vitamin D and magnesium caused a significant decrease in children with conduct problems, social problems, and anxiety/shy scores (Hemamy et al., 2020). |
| Vitamin B2, B6, B9 and B12deficiency has been found in many patients with Attention Deficit and Hyperactivity Disorder (Landaas et al, 2016; Unal et al., 2019). | Vitamin therapy appears to reduce symptoms of ADHD and ASD (Poudineh et al., 2023; Unal et al., 2019). An 8 weeks supplementing with Vitamin B6 and magnesium decreased hyperactivity and hyperemotivity/aggressiveness. When supplementation was stopped, clinical symptoms of the disease reappeared in few weeks (Mousain-Bosc et al., 2006). |
Table 1. Examples of vitamin and mineral deficiencies associated with symptoms of ADHD and supplementation to reduction of ADHD symptoms.
Supplementation of vitamins and minerals in many cases consisted of more than one single vitamin or mineral. For an in-depth analysis and presentation, see the superb webinar by Henry & CNS (2023): https://divcom-events.webex.com/recordingservice/sites/divcom-events/recording/e29cefcae6c1103bb7f3aa780efee435/playback? (Henry & CNS, 2023).
Whole foods are more than the sum of individual parts (the identified individual constituents/nutrients). The process of digestion is much more complicated than ingesting simple foods with added vitamins or minerals. Digestion is the interaction of many food components (many of which we have not identified) which interact and affect the human biome. A simple added nutrient can help; however, eating whole organic foods it most likely be healthier. For example, whole-wheat flour is much more nutritious. Whole wheat is rich in vitamins B-1, B-3, B-5, riboflavin, folate well as fiber while refined white flour has been bleached and stripped of fiber and nutrients to which some added vitamins and iron are added.
Recommendation
When working with clients, follow Talib’s principles as outlined in Part 1 by Peper (2023) which suggests that to improve health first remove the unnatural which in this case are the ultra-processed foods, simple carbohydrates, exposure to pesticides and herbicides (Taleb, 2014). The approach is beneficial for prevention and treatment. This recommendation to optimize health is both very simple and very challenging. The simple recommendation is to eat only organic foods and as much variety as possible as recommended by Professor Michael Pollan in his books, Omnivore’s Dilemma: A Natural History of Four Meals and Food Rules (Pollan, 2006; Pollan, 2011).
Do not eat foods that contain herbicides and pesticide residues or are ultra-processed. Although organic foods especially vegetable and fruits are often much more expensive, you have choice: You can pay more now to optimize health or pay later to treat disease. Be safe and not sorry. This recommendation is similar to the quote, “Let food be thy medicine and medicine be thy food,” that has been attributed falsely since the 1970s to Hippocrates, the Greek founder of western medicine (5th Century, BC) (Cardenas, 2013).
There are many factors that interfere with implementing these suggestions; since, numerous people live in food deserts (no easy access to healthy unprocessed foods ) or food swamps (a plethora of fast food outlets) and 54 million Americans are food insecure (Ney, 2022). In addition, we and our parents have been programmed by the food industry advertising to eat the ultra- processed foods and may no longer know how to prepare healthy foods such as exemplified by a Mediterranean diet. Recent research by Bayles et al (2022) has shown that eating a Mediterranean diet improves depression significantly more than the befriending control group. In addition, highly processed foods and snacks are omnipresent, often addictive and more economical.
Remember that clients are individuals and almost all research findings are based upon group averages. Even when the data implies that a certain intervention is highly successful, there are always some participants for whom it is very beneficial and some for whom it is ineffective or even harmful. Thus, interventions need to be individualized for which there is usually only very limited data. In most cases, the original studies did not identify the characteristics of those who were highly successful or those who were unsuccessful. In addition, when working with specific individuals with ADHD, anxiety, depression, etc. there are multiple possible causes.
Before beginning specific clinical treatment such as neurofeedback and/or medication, we recommend the following:
- “Grandmother assessment” that includes and assessment of screen time, physical activity, outdoor sun exposure, sleep rhythm as outlined in Part 1 by Peper (2023). Then follow-up with a dietary assessment that investigates the prevalence of organic/non organic foods, ingestion of fast foods, ultra-processed foods, soft drinks, high simple carbohydrate and sugar, salty/sugary/fatty snacks, fruits, vegetables, and eating patterns (eating with family or by themselves in front of screens). Be sure to include an assessment of emotional reactivity and frequency of irritability and “hangryness”.
- If the assessment suggest low level of organic whole foods and predominance of ultra- refined foods, it may be possible that the person is deficient in vitamins and minerals. Recommend that the child is tested for the vitamin deficiencies. If vitamin deficiencies identified, recommend to supplement the diet with the necessary vitamins and mineral and encourage eating foods that naturally include these substances (Henry & CNS, 2023). If there is a high level of emotional reactivity and “hangryness,” a possible contributing factor could be hypoglycemic rebound from a high simple carbohydrate (sugar) intake or not eating breakfast combined with hyperventilation (Engel et al., 1947; Barr et al., 2019). Recommend eliminating simple carbohydrate breakfast and fast food snacks and substitute organic foods that include complex carbohydrates, protein, fats, vegetables and fruit. Be sure to eat breakfast.
- Implement “Grandmother Therapy”. Encourage the family and child to change their diet to eating a whide variety of organic foods (vegetables, fruits, some fish, meat and possibly dairy) and eliminate simple carbohydrates and sugars. This diet will tend to reduce nutritional deficits and may eliminate the need for supplements.
- Concurrent with the stabilization of the physiology begin psychophysiological treatment strategies such as neurofeedback biofeedback and cognitive behavior therapy.
Relevant blogs
Author Disclosure
Authors have no grants, financial interests, or conflicts to disclose.
References
Arnold, L, Lofthouse, N., & Hurt, E. (2012). Artificial food colors and attention-deficit/hyperactivity symptoms: conclusions to dye for. Neurotherapeutics, 9(3), 599-609. https://doi.org/10.1007/s13311-012-0133-x
Arab, A. & Mostafalou, S. (2022). Neurotoxicity of pesticides in the context of CNS chronic diseases. International Journal of Environmental Health Research, 32(12), 2718-2755. https://doi.org/10.1080/09603123.2021.1987396
Barr, E.A., Peper, E., & Swatzyna, R.J. (2019). Slouched Posture, Sleep Deprivation, and Mood Disorders: Interconnection and Modulation by Theta Brain Waves. NeuroRegulation, 6(4), 181–189. https://doi.org/10.15540/nr.6.4.181
Bayes. J., Schloss, J., Sibbritt, D. (2022). The effect of a Mediterranean diet on the symptoms of depression in young males (the “AMMEND: A Mediterranean Diet in MEN with Depression” study): a randomized controlled trial. Am J Clin Nutr. 116(2), 572-580. https://doi.org/10.1093/ajcn/nqac106
Bjørling-Poulsen, M., Andersen, H.R. & Grandjean, P. Potential developmental neurotoxicity of pesticides used in Europe. Environ Health 7, 50 (2008). https://doi.org/10.1186/1476-069X-7-50
Bommersbach, T.J., McKean, A.J., Olfson, M., Rhee, T.G. (2023). National Trends in Mental Health–Related Emergency Department Visits Among Youth, 2011-2020. JAMA, 329(17):1469–1477. https://doi.org/10.1001/jama.2023.4809
Bouchard, M.F., Bellinger, D.C., Wright, R.O., & Weisskopf, M.G. (2010). Attention-deficit/hyperactivity disorder and urinary metabolites of organophosphate pesticides. Pediatrics, 125(6), e1270-7. https://doi.org/10.1542/peds.2009-3058
Braghieri, L., Levy, R., & Makarin, A. (2022). Social Media and Mental Health (July 28, 2022). Available at SSRN: https://ssrn.com/abstract=3919760 or http://dx.doi.org/10.2139/ssrn.3919760
Cardenas, D. (2013). Let not thy food be confused with thy medicine: The Hippocratic misquotation. e-Spen Journal, 8(6), 3260-3262. https://doi.org/10.1016/j.clnme.2013.10.002
CDC, (2023). Quick Facts on the Risks of E-cigarettes for Kids, Teens, and Young Adults. CDC. Centers for Disease Control and Prevention. Accessed September 23, 2023. https://www.cdc.gov/tobacco/basic_information/e-cigarettes/Quick-Facts-on-the-Risks-of-E-cigarettes-for-Kids-Teens-and-Young-Adults.html
Chang, J.C., Su, K.P., Mondelli, V. et al. Omega-3 Polyunsaturated Fatty Acids in Youths with Attention Deficit Hyperactivity Disorder: a Systematic Review and Meta-Analysis of Clinical Trials and Biological Studies. Neuropsychopharmacol. 43, 534–545. https://doi.org/10.1038/npp.2017.160
Chhabra, R., Kolli, S., & Bauer, J.H. (2013). Organically Grown Food Provides Health Benefits to Drosophila melanogaster. PLoS ONE, 8(1): e52988. https://doi.org/10.1371/journal.pone.0052988
Davis, D. R., Epp, M. D., & Riordan, H. D. (2004). Changes in USDA food composition data for 43 garden crops, 1950 to 1999. Journal of the American College of Nutrition, 23(6), 669-682. https://doi.org/10.1080/07315724.2004.10719409
Derbyshire, E. (2017). Do Omega-3/6 Fatty Acids Have a Therapeutic Role in Children and Young People with ADHD? J Lipids. 6285218. https://doi.org/10.1155/2017/6285218
Del-Ponte, B., Quinte, G.C., Cruz, S., Grellert, M., & Santos, I. S. Dietary patterns and attention deficit/hyperactivity disorder (ADHD): A systematic review and meta-analysis. Journal of Affective Disorders, 252, 160-173. https://doi.org/10.1016/j.jad.2019.04.061
Durukan, İ., Kara, K., Almbaideen, M., Karaman, D., & Gül, H. (2018). Alexithymia, depression and anxiety in parents of children with neurodevelopmental disorder: Comparative study of autistic disorder, pervasive developmental disorder not otherwise specified and attention deficit-hyperactivity disorder. Pediatrics International, 60(3), 247–253. https://doi.org/10.1111/ped.13510
Effatpanah, M., Rezaei, M., Effatpanah, H., Effatpanah, Z., Varkaneh, H.K., Mousavi. S.M., Fatahi, S., Rinaldi, G., & Hashemi, R. (2019). Magnesium status and attention deficit hyperactivity disorder (ADHD): A meta-analysis. Psychiatry Res, 274, 228-234. https://doi.org/10.1016/j.psychres.2019.02.043
Engel, G.L., Ferris, E.B., & Logan, M. (1947). Hyperventilation; analysis of clinical symptomatology. Ann Intern Med, 27(5), 683-704. https://doi.org/10.7326/0003-4819-27-5-683
EPA. (2023). Glyphosate. United States Environmental Protection Agency. Accessed April 1, 2023. https://www.epa.gov/ingredients-used-pesticide-products/glyphosate
European Commission. (2023). EU legislation on MRLs.Food Safety. Assessed April 1, 2023. https://food.ec.europa.eu/plants/pesticides/maximum-residue-levels/eu-legislation-mrls_en#:~:text=A%20general%20default%20MRL%20of,e.g.%20babies%2C%20children%20and%20vegetarians
Faraone, S.V. & Larsson, H. (2019). Genetics of attention deficit hyperactivity disorder. Mol Psychiatry, 24(4), 562-575. https://doi.org/10.1038/s41380-018-0070-0
Fernandez-Cornejo, J. Nehring, R, Osteen, C., Wechsler, S., Martin, A., & Vialou, A. (2014). Pesticide use in the U.S. Agriculture: 21 Selected Crops, 1960-2008. Economic Information Bulletin Number 123, United State Department of Agriculture. https://www.ers.usda.gov/webdocs/publications/43854/46734_eib124.pdf
Gomes, G. N., Vidal, F. N., Khandpur. N., et al. (2023). Association Between Consumption of Ultraprocessed Foods and Cognitive Decline. JAMA Neurol, 80(2),142–150. https://doi.org/10.1001/jamaneurol.2022.4397
Hemamy, M., Heidari-Beni, M., Askari, G., Karahmadi, M., & Maracy, M. (2020). Effect of Vitamin D and Magnesium Supplementation on Behavior Problems in Children with Attention-Deficit Hyperactivity Disorder. Int J Prev Med, 11(1), 4. https://doi.org/10.4103/ijpvm.IJPVM_546_17
Henry, K. (2023). An Integrative Medicine Approach to ADHD. Rupa Health. Accessed September 30, 2023. https://www.rupahealth.com/post/an-integrative-medicine-approach-to-adhd
Henry, K. & CNS, L.A. (2023). Natural treatments for ADHD. Webinar Presentation by IntegrativePractitioner.com and sponsored by Rupa Health, June 6, 2023 https://divcom-events.webex.com/recordingservice/sites/divcom-events/recording/e29cefcae6c1103bb7f3aa780efee435/playback?
Hemamy, M., Pahlavani, N., Amanollahi, A. et al. (2021). The effect of vitamin D and magnesium supplementation on the mental health status of attention-deficit hyperactive children: a randomized controlled trial. BMC Pediatr, 21, 178. https://doi.org/10.1186/s12887-021-02631-1
Konofal, E., Lecendreux, M., Arnulf, I., & Mouren, M. (2004). Iron Deficiency in Children With Attention-Deficit/Hyperactivity Disorder. Arch Pediatr Adolesc Med, 158(12), 1113–1115. https://doi.org/10.1001/archpedi.158.12.1113
Kotsi, E., Kotsi, E. & Perrea, D.N. (2019). Vitamin D levels in children and adolescents with attention-deficit hyperactivity disorder (ADHD): a meta-analysis. ADHD Atten Def Hyp Disord, 11, 221–232. https://doi.org/10.1007/s12402-018-0276-7
LaChance, L.R. & Ramsey, D. (2018). Antidepressant foods: An evidence-based nutrient profiling system for depression. World J Psychiatr, 8(3): 97-104. World J Psychiatr., 8(3): 97-104. https://doi.org/10.5498/wjp.v8.i3.97
Landaas, E.T., Aarsland, T.I., Ulvik, A., Halmøy, A., Ueland. P.M., & Haavik, J. (20166). Vitamin levels in adults with ADHD. BJPsych Open, 2(6), 377-384. https://doi.org/10.1192/bjpo.bp.116.003491
Linday, L.A. (2010). Cod liver oil, young children, and upper respiratory tract infections. J Am Coll Nutr, 29(6), 559-62. https://doi.org/10.1080/07315724.2010.10719894
Leoci, R. & Ruberti, M. (2021) Pesticides: An Overview of the Current Health Problems of Their Use. Journal of Geoscience and Environment Protection, 9, 1-20. https://doi.org/10.4236/gep.2021.98001
Lustig, R.H. (2021). Metaboical: The lure and the lies of processed food, nutrition, and modern medicine. New York: Harper Wave. https://www.amazon.com/Metabolical-processed-poisons-people-planet/dp/1529350077
MacInerney, E. K., Swatzyna, R. J., Roark, A. J., Gonzalez, B. C., & Kozlowski, G. P. (2017). Breakfast choices influence brainwave activity: Single case study of a 12-year-old female. NeuroRegulation, 4(1), 56–62. https://doi.org/10.15540/nr.4.1.56
McCann, D., Barrett, A., Cooper, A., Crumpler, D., Dalen, L., Grimshaw, K., et al. (2007). Food additives and hyperactive behavior in 3-year old and 8/9-year-old children in the community: a randomized, double-blinded, placebo-controlled trial. Lancet, 370(9598), 1560-1567. https://doi.org/10.1016/S0140-6736(07)61306-3
Mengying, L.I, Fallin, A, D., Riley,A., Landa, R., Walker, S.O., Silverstein, M., Caruso, D., et al. (2016). The Association of Maternal Obesity and Diabetes With Autism and Other Developmental Disabilities. Pediatrics, 137(2), e20152206. https://doi.org/10.1542/peds.2015-2206
Mousain-Bosc, M., Roche, M., Polge, A., Pradal-Prat, D., Rapin, J., & Bali, J.P. (2006). Improvement of neurobehavioral disorders in children supplemented with magnesium-vitamin B6. I. Attention deficit hyperactivity disorders. Magnes Res. 19(1), 46-52. https://pubmed.ncbi.nlm.nih.gov/16846100/#:~:text=In%20almost%20all%20cases%20of,increase%20in%20Erc%2DMg%20values.
Ney, J. (2022). Food Deserts and Inequality. Social Policy Data Lab. Updated: Jan 24, 2022. Accessed September, 23, 2023. https://www.socialpolicylab.org/post/grow-your-blog-community
Peper, E. (2023a). Reflections on the increase in Autism, ADHD, anxiety and depression: Part 1-bonding, screen time, and circadian rhythms. the peperperspective July 2, 2023. Accessed august 8, 2024, https://peperperspective.com/2023/07/04/reflections-on-the-increase-in-autism-adhd-anxiety-and-depression-part-1-bonding-screen-time-and-circadian-rhythms/
Peper, E. (2023b). Reflections on the increase in Autism, ADHD, anxiety and depression: Part 1-bonding, screen time, and circadian rhythms. NeuroRegulation, 10(2), 134-138. https://doi.org/10.15540/nr.10.2.134
Pollan, M. (2006). Omnivore’s Dilemma: A Natural History of Four Meals and Food Rules. New York Penguin Press. https://www.amazon.com/Omnivores-Dilemma-Natural-History-Meals/dp/1594200823/ref=tmm_hrd_swatch_0?_
Pollan, M. (2011). Food rules. New York Penguin Press. https://www.amazon.com/Food-Rules-Eaters-Michael-Pollan/dp/B00VSBILFG/ref=tmm_hrd_swatch_0?
Pongpitakdamrong, A., Chirdkiatgumchai, V., Ruangdaraganon, N., Roongpraiwan, R., Sirachainan, N., Soongprasit, M., & Udomsubpayakul, U. (2022). Effect of Iron Supplementation in Children with Attention-Deficit/Hyperactivity Disorder and Iron Deficiency: A Randomized Controlled Trial. Journal of Developmental & Behavioral Pediatrics, 43(2), 80-86., https://doi.org/10.1097/DBP.0000000000000993
Porto, A. & Abu-Alreesh, S. (2022). Vitamin D for babies, children & adolescents. Health Living. Healthychildren.org. Accessed September 24, 2023. https://www.healthychildren.org/English/healthy-living/nutrition/Pages/vitamin-d-on-the-double.aspx#
Poudineh, M., Parvin, S., Omidali, M., Nikzad, F., Mohammadyari, F., Sadeghi Poor Ranjbar, F., F., Nanbakhsh, S., & Olangian-Tehrani, S. (2023). The Effects of Vitamin Therapy on ASD and ADHD: A Narrative Review. CNS & Neurological Disorders – Drug Targets (Formerly Current Drug Targets – CNS & Neurological Disorders), (22), 5, 2023, 711-735. https://doi.org/10.2174/1871527321666220517205813
Puigbò, P., Leino, L. I., Rainio, M. J., Saikkonen, K., Saloniemi, I., & Helander, M. (2022). Does Glyphosate Affect the Human Microbiota?. Life, 12(5), 707. https://doi.org/10.3390/life12050707
Ríos-Hernández, A., Alda, J.A., Farran-Codina, A., Ferreira-García, E., & Izquierdo-Pulido, M. (2017). The Mediterranean Diet and ADHD in Children and Adolescents. Pediatrics, 139(2):e20162027. https://doi.org/10.1542/peds.2016-2027
Ryu, S.A., Choi, Y.J., An, H., Kwon, H.J., Ha, M., Hong, Y.C., Hong, S.J., & Hwang, H.J. (2022). Associations between Dietary Intake and Attention Deficit Hyperactivity Disorder (ADHD) Scores by Repeated Measurements in School-Age Children. Nutrients, 14(14), 2919. https://doi.org/10.3390/nu14142919
Sagiv, S.K., Kogut, K., Harley, K., Bradman, A., Morga, N., & Eskenazi, B. (2021). Gestational Exposure to Organophosphate Pesticides and Longitudinally Assessed Behaviors Related to Attention-Deficit/Hyperactivity Disorder and Executive Function, American Journal of Epidemiology, 190(11), 2420–2431. https://doi.org/10.1093/aje/kwab173
Swanson, N.L., Leu, A., Abrahamson, J., & Wallet, B. (2014). Genetically engineered crops, glyphosate and the deterioration of health in the United States of America. Journal of Organic Systems, 9(2), 6-17. https://www.organic-systems.org/journal/92/JOS_Volume-9_Number-2_Nov_2014-Swanson-et-al.pdf
Swatzyna, R. J., Boutros, N. N., Genovese, A. C., MacInerney, E. K., Roark, A. J., & Kozlowski, G. P. (2018). Electroencephalogram (EEG) for children with autism spectrum disorder: Evidential considerations for routine screening. European Child & Adolescent Psychiatry, 28(5), 615–624. https://doi.org/10.1007/s00787-018-1225-x
Taleb, N. N. (2014). Antifragile: Things That Gain from Disorder (Incerto). New York: Random House Publishing Group. https://www.amazon.com/Antifragile-Things-That-Disorder-Incerto/dp/0812979680/ref=tmm_pap_swatch_0
Tohidi, S., Bidabadi, E., Khosousi, M.J., Amoukhteh, M., Kousha, M., Mashouf, P., Shahraki, T. (2021). Effects of Iron Supplementation on Attention Deficit Hyperactivity Disorder in Children Treated with Methylphenidate. Clin Psychopharmacol Neurosci, 19(4), 712-720. https://doi.org/10.9758/cpn.2021.19.4.712
Unal, D. Çelebi, F., Bildik,H.N., Koyuncu, A., & Karahan, S. (2019). Vitamin B12 and haemoglobin levels may be related with ADHD symptoms: a study in Turkish children with ADHD, Psychiatry and Clinical Psychopharmacology, 29(4), 515-519. https://doi.org/10.1080/24750573.2018.1459005
USDA. (2019). Fish oil, cod liver. FoodData Central. USDA U.S> Department of Agriculture. Published 4/1/2019. Accessed September 24, 2024. https://fdc.nal.usda.gov/fdc-app.html#/food-details/173577/nutrients
Van Tulleken, C. (2023). Ultra-Processed People. The Science Behind Food That Isn’t Food. New York: W.W. Norton & Company. https://www.amazon.com/Ultra-Processed-People-Science-Behind-Food/dp/1324036729/ref=asc_df_1324036729/?
Wahab, S., Muzammil, K., Nasir, N., Khan, M.S., Ahmad, M.F., Khalid, M., Ahmad, W., Dawria, A., Reddy, L.K.V., & Busayli, A.M. (2022). Advancement and New Trends in Analysis of Pesticide Residues in Food: A Comprehensive Review. Plants (Basel), 11(9), 1106. https://doi.org/10.3390/plants11091106
Wang. Y., Huang, L., Zhang, L., Qu, Y., & Mu, D. (2017). Iron Status in Attention-Deficit/Hyperactivity Disorder: A Systematic Review and Meta-Analysis. PLoS One, 12(1):e0169145. https://doi.org/10.1371/journal.pone.0169145
Wilson, L. (2015). Mothers, beware: Your lifestyle choices will even affect your grandkids.
News Corp Australia Network. Accessed Jun 24, 2024. https://www.news.com.au/lifestyle/parenting/kids/mothers-beware-your-lifestyle-choices-will-even-affect-your-grandkids/news-story/3f326f457546cfb32af5c409f335fb56
Woo, H.D.,; Kim, D.W., Hong, Y.-S., Kim, Y.-M.,Seo, J.-H.,; Choe, B.M., Park, J.H.,; Kang, J.-W., Yoo, J.-H.,; Chueh, H.W., et al. (2014). Dietary Patterns in Children with Attention Deficit/Hyperactivity Disorder (ADHD). Nutrients, 6, 1539-1553. https://doi.org/10.3390/nu6041539
Zhong, C., Tessing, J., Lee, B.K., Lyall, K. Maternal Dietary Factors and the Risk of Autism Spectrum Disorders: A Systematic Review of Existing Evidence. Autism Res,13(10),1634-1658. https://doi.org/10.1002/aur.2402
Playful practices to enhance health with biofeedback
Posted: May 4, 2024 Filed under: attention, behavior, biofeedback, Breathing/respiration, computer, Exercise/movement, health, Neck and shoulder discomfort, Pain/discomfort, self-healing, Uncategorized | Tags: exercise, Feldenkrais, pain, Play, somatics 1 CommentAdapted from: Gibney, K.H. & Peper, E. (2003). Exercise or play? Medicine of fun. Biofeedback, 31(2), 14-17.

Homework assignments are sometimes viewed as chore and one more thing to do. Changing the perception from that of work to fun by encouraging laughter and joy often supports the healing process. This blog focusses on utilizing childhood activities and paradoxical movement to help clients release tension patterns and improve range of motion. A strong emphasis is placed on linking diaphragmatic breathing to movement.
When I went home I showed my granddaughter how to be a tree swaying in the wind, she looked at me and said, “Grandma, I learned that in kindergarten!”
‘Betty’ laughed heartily as she relayed this story. Her delight in being able to sway her arms like the limbs of a tree starkly contrasted with her demeanor only a month prior. Betty was referred for biofeedback training after a series of 9 surgeries – wrists, fingers, elbows and shoulders. She arrived at her first session in tears with acute, chronic pain accompanied by frequent, incapacitating spasms in her shoulders and arms. She was unable to abduct her arms more than a few inches without triggering more painful spasms. Her protective bracing and rapid thoracic breathing probably exacerbated her pain and contributed to a limited range of motion of her arms. Unable to work for over a year, she was coping not only with pain, but also with weight gain, poor self-esteem and depression.
The biofeedback training began with effortless, diaphragmatic breathing which is often the foundation of health (Peper and Gibney, 1994). Each thoracic breath added to Betty’s chronic shoulder pain. Convincing Betty to drop her painful bracing pattern and to allow her arms to hang freely from her shoulders as she breathed diaphragmatically was the first major step in regaining mobility. She discovered in that first session that she could use her breathing to achieve control over muscle spasms when she initiated the movement during the exhalation phase of breathing as shown in Figure 1.

Figure 1. Initiate the physical activity after exhaling has begun and body is relaxing especially if the movement or procedure such as an injection would cause pain. Pause the movement when inhaling and then continue the movement again during the exhalation phase. The simple rule is to initiate the activity slightly after beginning exhaling and when the heart rate started to decrease (reproduced with permission from Gorter & Peper, 2012).
During the first week, she practiced her breathing assiduously at home and had fewer spasms. Betty was able to move better during her physical therapy sessions. Each time she felt the onset of muscle spasms she would stop all activity for a moment and ‘go into my trance’ to prevent a recurrence. For the first time in many months, she was feeling optimistic.
Subsequent sessions built upon the foundation of diaphragmatic breathing: boosting Betty’s confidence, increasing range of motion (ROM), and bringing back some fun in life. Activities included many childhood games: tossing a ball, swaying like a tree in the wind, pretending to conduct an orchestra, bouncing on gym balls, playing “Simon Says” (following the movements of the therapist), and dancing. Laughter and childlike joy became a common occurrence. She looked forward to receiving the sparkly star stickers she was given after successful sessions. With each activity, Betty gained more confidence, gradually increased ROM, and began losing weight. Although she had some days where the pain was strong and spasms threatened, Betty reframed the pain as occurring as a result of healing and expanding her ROM—she was no longer a victim of the pain. In addition, her family was proud of her, she was doing more fun activities, and she felt confident that she would return to work.
Betty’s story is similar to other clients whom we have seen. The challenge presented to therapists is to help the client better cope with pain, increase ROM, regain function and, often the most important, to reclaim a “joie de vivre”. Increasing function includes using the minimum amount of effort necessary for the task, allowing unnecessary muscles to remain relaxed (inhibition of dysponesis[i]), and quickly releasing muscle tension when the muscle is no longer required for the activity (work/rest) (Whatmore & Kohli, 1974; Peper et al, 2010; Sella, 2019). The challenge is to perform the task without concurrent evocation of components of the alarm reaction, which tend to be evoked when “we try to do it perfectly,” or “it has to work,” “If I do not do it correctly,” or “I will be judged.” For example, when people learn how to implement micro-breaks (1–2 second rest periods) at the computer, they often sit quietly believing that they are relaxed; however, they may continue a bracing pattern (Peper et al, 2006). Alternatively, tossing a small ball rather than resting at the keyboard will generally evoke laughter, encourage generalization of skills, and covertly induce more relaxation. In some cases, therapists in their desire to help clientss to get well assign structured exercises as homework that evoke striving for performance and boredom—this striving to perform the structured exercises may inhibit healing. Utilizing tools other than those found in the work setting helps the client achieve a broader perspective of the healing/preventive concepts that are taught.
To optimize success, clients are active participants in their own healing process which means that they learn the skills during the therapeutic session and practice at home and at work. Home practices are assigned to integrate the mastery of news skills into daily life. To help clients achieve increased health through physical activity three different approaches are often used: movement reeducation, youthful play, and pure exercise. How the client performs the activity may be monitored with surface electromyography (SEMG) to identify muscles tightening that are not needed for the task and how the muscle relaxes when not needed for the task performance. This monitoring can be done with a portable biofeedback device or multi-channel system when walking or performing the exercises. Clients can even use a single channel SEMG at home.
When working to improve ROM and physical function, explore the following:
- Maintain diaphragmatic breathing – rhythm or tempo may change but the breath must be generated from the diaphragm with emphasis on full exhalation. Use strain gauge feedback and/or SEMG feedback to monitor and train effortless breathing (Peper et al., 2016). Strain gauge feedback is used to teach a slower and diaphragmatic breathing pattern, while SEMG recorded from the scalene to trapezius is used to teach how to reduce shoulder and ancillary muscle tension during inhalation
- Perform activities or stretching/strengthening exercises so slowly that they don’t trigger or aggravate pain during the exhalation phase of breathing.
- Use the minimum amount of tension necessary for the task and let unnecessary muscles remain relaxed. Use SEMG feedback recorded from muscles not needed for the performance of the task to teach clients awareness of inappropriate muscle tension and to learn relaxation of those muscles.
- Release muscle tension immediately when the task is accomplished. Use SEMG feedback to monitor that the muscles are completely relaxed. If rapid relaxation is not achieved, first teach the person to relax the muscles before repeating the muscle activity.
- Perform the exercises as if you have never performed them and do them with a childlike, beginner’s mind, and exploratory attitude (Kabat-Zinn, 1990).
- Create exercises that are totally new and novel so that the participant has no expectancy of outcome can be surprised by their own experience. This approach is part of many somatic educational and therapeutic approaches such as Feldenkrais or Somatics (Hanna, 2004; Feldenkrais, 2009).
Movement and exercise can be taught as pure physical exercise, movement reeducation or youthful playing. Physical exercise is necessary for strength and endurance and at the same time, improves our mood (Thayer, 1996; Mahindru et al., 2023). However, many exercises are considered a burden and are often taught without a sense of lightness and fun, which results in the client thinking in terms that are powerless and helpless (depressive)—“I have to do them.” Helping your clients to understand that exercise is simply a part of every day life, that it encourages healing and improves health, and that they can “cheat” at it, may help them to reframe their attitudes toward it and accomplish their healing goals.
Pure Physical Exercise—Enjoyment through Strength and Flexibility
The major challenge of structured exercises is that the person is very serious and strives too hard to attain the goal. In the process of striving, the body is often held rigid: Breath is shallow and halted and shoulders are slightly braced. Maintaining a daily chart is an excellent tool to show improvement (e.g., more repetitions, more weight, increased flexibility; since, structured exercises are very helpful for improving ROM and strength. When using pure exercise, remember that injured person may have a sense of urgency – they want to get well quickly and, if work stress was a factor in developing pain, they often rush when they need to meet a deadline.
As much as possible make the exercise fun. Help the client understand that he/she can be quick while not rushed. For example, monitor SEMG from an upper trapezius muscle using a portable electromyography. For example, begin by walking slowly. Add a ramp or step to ensure that there is no bracing when climbing (a common occurrence). Walk around the room, down the hall, around the block. Maintain relaxed shoulders, an even swing of the arms, and diaphragmatic breathing. Walk more quickly while emphasizing relaxation with speed rather than rushing. Go faster and faster. Up the stairs. Down the stairs. Walk backward. Skip. Hop. Laugh.
Movement Reeducation – Be ‘Oppositional’ And Do It Differently
Movement reeducation, such as Feldenkrais, Alexander Technique or Hannah Somatics, involves conscious awareness of movement (Alexander, 2001; Hanna, 2004; Murphy, 1993). Many daily patterns of movement become imbedded in our consciousness and, over the years, may include a pain trigger. A common trigger is lifting the shoulders when reaching for the keyboard or mouse, people suffering from thoracic outlet syndrome (TOS) often have such patterns (Peper & Harvey, 2021). A keyboard can often inadvertently cue the client to trigger this dysponetic, and frequently painful, pattern. Have the client do movement reeducation exercises as they are guided through practices in which they have no expectancy and the movements are novel. The focus is on awareness without triggering any fight/flight or startle responses.
Ask the client to explore performing many functional activities with the opposite hand, such as brushing his/her hair or teeth, eating, blowing his/her hair dry, or doing household chores, such as vacuuming. (Explore this for yourself, as well!). Be aware of how much shoulder muscle tension is needed to raise the arms for combing or blow-drying the hair. Explore how little effort is required to hold a fork or knife (you might want to do this in the privacy of your own home!).
Do movements differently such as, practicing alternating hands when leading with the vacuum or when sweeping, changing routes when driving/walking to work or the store, getting out of bed differently. Break up habitual conditioned reflex patterns such as eye, head and hand coordination. For example, slowly rotate your head from left to right and simultaneously shift your eyes in the opposite direction (e.g., turn your head fully to the right while shifting your eyes fully to the left, and then reverse) or before reaching forward, drop your elbows to your sides then, bend your elbows and touch your shoulders with your thumbs then, reach forward. Often, when we change our patterns we increase our flexibility, inhibit bracing and reduce discomfort.
Free Your Neck and Shoulders (adapted from a demonstration by Sharon Keane and developed by Ilana Rubenfeld, 2001)
–Push away from the keyboard and sit at the edge of the chair with your knees bent at right angles and your feet shoulder-width apart and flat on the floor. Do the following movements slowly. Do NOT push yourself if you feel discomfort. Be gentle with yourself.
–Look to the right and gently turn your head and body as far as you can go to the right. When you have gone as far as you can comfortably go, look at the furthest spot on the wall and remember that spot. Gently rotate your head back to center. Close your eyes and relax.
–Reach up with your left hand; pass it over the top of your head and hold on to your right ear. Then, gently bend to the left lowering your elbow towards the floor. Slowly straighten up. Repeat for a few times feeling as if you are a sapling flexing in the breeze. Observe what your body is doing as it bends and comes back up to center. Notice the movements in your ribs, back and neck. Then, drop your arm to your lap and relax. Make sure you continue to breathe diaphragmatically throughout the exercise.
–Reach up with your right hand and pass it over the top of your head and hold on to your left ear. Repeat as above except bending to the right.
–Reach up with your left hand and pass it over the top of your head and hold on to your right ear. Then, look to the left with your eyes and rotate your head to the left as if you are looking behind you. Return to center and repeat the movement a few times. Then, drop your arm to your lap and relax for a few breaths.
–Again, reach over your head with your left hand and hold onto your right ear. Repeat the same rotating motion of your head to the left except that your eyes look to the right. Repeat this a few times then, drop your arm to your lap and relax for a few breaths.
–Reach up with your right hand and pass it over the top of your head and hold on to your left ear. Then, look to the right with your eyes and rotate your head to the right as if you are looking behind you. Return to center and repeat a few times. Then, drop your arm to your lap and relax for a few breaths.
–Again, reach over your head with your right hand and hold onto your left ear. Repeat the same rotating motion of your head to the right except that your eyes look to the left. Repeat this a few times then, drop your arm to your lap and relax for a few breaths.
–Now, look to the right and gently turn your head and body as far as you can go. When you can not go any further, look at that point on the wall. Did you rotate further than at the beginning of the exercise?
–Gently rotate your head back to center, close your eyes, relax and notice the feeling in your neck, shoulders and back.
Youthful Playing – Pavlovian Practice
Evoking positive past memories and actually acting them out may enhance health as is illustrated by the recovery of serious illness of Ivan Pavlov, the discovery of classical conditioning. When Pavlov quietly lay in his hospital bed, many, including his family, thought he was slipping into death. He then ask the nurse to get him a bowl of water with earth in it and the whole night long he gently played with the mud. He recreated the experience when as a child he was playing in mud along a river’s bank. Pavlov knew that evoking the playful joy of childhood would help to encourage mental and physical healing. The mud in hands was the conditioned stimulus to evoke the somatic experience of wellness (Peper, Gibney, & Holt, 2002).
Having clients play can encourage laughter and joie de vivre, which may help in physical healing. Being involved in childhood games and actually playing these games with children removes one from worries and concerns—both past and future—and allows one to be simply in the present. Just being present is associated with playfulness, timelessness, passive attention, creativity and humor. A state in which one’s preconceived mental images and expectancies—the personal, familial, cultural, and healthcare provider’s hypnotic suggestions—are by-passed and for that moment, the present and the future are yet undefined. This is often the opposite of the client’s expectancy; since, remembering the past experiences and the diagnosis creates a fixed mental image that may expect pain and limitation.
Explore some of the following practices as strategies to increase movement and flexibility without effort and to increase joy. Use your creativity and explore your own permutations of the practices. Observe how your mood improves and your energy increases when you play a childhood game instead of an equivalent exercise. For example, instead of dropping your hands to your lap or stretching at the computer terminal during a micro- or meso-break[ii], go over to your coworker and play “pattycake.” This is the game in which you and your partner face each other and then clap your hands and then touch each other’s palms. Do this in all variations of the game.
For increased ROM in the shoulders explore some of the following (remember the basics: diaphragmatic breathing, minimum effort, rapid release) in addition, do the practices to the rhythm of the music that you enjoyed as a young person.
Ball Toss: a hand-sized ball that is easily squeezed is best for this exercise. Monitor respiration patterns, and SEMG forearm extensors and/or flexors, and upper trapezii muscles. Sit quietly in a chair and focus on a relaxed breathing rhythm. Toss the ball in the air with your right hand and catch it with your left hand. As soon as you catch the ball, drop both hands to your lap. Toss the ball back only when you achieve relaxation—both with the empty hand and the hand holding the ball. Watch for over-efforting in the upper trapezii. Begin slowly and increase the pace as you train yourself to quickly release unnecessary muscle tension. Go faster and faster (just about everyone begins to laugh, especially each time they drop the ball).
Ball Squeeze/Toss: Expand upon the above by squeezing the ball prior to tossing. When working with a client, call out different degrees of pressure (e.g., 50%, 10%, 80%, etc.). The same rules apply as with the ball toss.
Ball Hand to Hand: Close your eyes and hand the ball back and forth. Go faster and faster and add ball squeezes prior to passing the ball.
Gym Ball Bounces: Sit on a gym ball and find your balance. Begin bouncing slowly up and down. Reach up and lower your left then, right hand. Abduct your arms forward then, laterally. Turn on the radio and bounce to music.
Simon Says: This can be done standing, sitting in a chair or on a gym ball. When on a gym ball, bounce during the game. Have your client do a mirror image of your movements: reaching up, down, left, right, forward or backward. Touch your head, nose, knees or belly. Have fun and go more quickly.
Back-To-Back Massage: With a partner, stand back-to-back. Lean against each other’s back so that you provide mutual support. Then each rub your back against each other’s back. Enjoy the wiggling movement and stimulation. Be sure to continue to breathe.
Summary: An Attitude of Fun
In summary, it is not what you do; it is also the attitude by which you do it that affects health. From this perspective,when exercises are performed playfully, flexibility, movement and health are enhanced while discomfort is decreased. Inducing laughter promotes healing and disrupts the automatic negative hypnotic suggestion/self-images of what is expected. The clients begins to live in the present moment and thereby decreases the anticipatory bracing and dysponetic activity triggered by striving. By decreasing striving and concern for results, clients may allow themselves to perform the practices with a passive attentive attitude that may facilitate healing. For that moment, the client forgets the painful past and a future expectances that are fraught with promises of continued pain and inactivity. At moment, the pain cycle is interrupted which provides hope for a healthier future.
References
Alexander, F.M. (2001). The Use of the Self. London: Orion Publishing. https://www.amazon.com/Use-Self-F-M-Alexander/dp/0752843915
Feldenkrais, M. (2009). Awareness Through Movement Easy-to-Do Health Exercises to Improve Your Posture, Vision, Imagination, and Personal Awareness. New York: HarperOne. https://www.amazon.com/Awareness-Through-Movement-Easy-Do/dp/0062503227
Gibney, K.H. & Peper, E. (2003). Exercise or play? Medicine of fun. Biofeedback, 31(2), 14-17. https://www.researchgate.net/publication/380317304_EXERCISE_OR_PLAY_MEDICINE_OF_FUN
Gorter, R. & Peper, E. (2012). Fighting Cancer- A Nontoxic Approach to Treatment. Berkeley: North Atlantic Books. https://www.amazon.com/Fighting-Cancer-Nontoxic-Approach-Treatment/dp/1583942483
Hanna, T. (2004). Somatics: Reawakening The Mind’s Control Of Movement, Flexibility, And Health. Da Capo Press. https://www.amazon.com/Somatics-Reawakening-Control-Movement-Flexibility/dp/0738209570
Kabat-Zinn, J. (1990). Full catastrophe living. New York: Delacorte Press.
Mahindru, A., Patil, P., & Agrawal, V. (2023). Role of Physical Activity on Mental Health and Well-Being: A Review. Cureus, I5(1), e33475. https://doi.org/10.7759/cureus.33475
Murphy, M. (1993). The future of the body. New York: Jeremy P. Tarcher/Perigee. https://www.amazon.com/Future-Body-Explorations-Further-Evolution/dp/0874777305
Peper, E., Booiman, A., Lin, I-M, Harvey, R., & Mitose, J. (2016). Abdominal SEMG Feedback for Diaphragmatic Breathing: A Methodological Note. Biofeedback. 44(1), 42-49. https://www.researchgate.net/publication/300365890_Abdominal_SEMG_Feedback_for_Diaphragmatic_Breathing_A_Methodological_Note
Peper, E., Booiman, A., Tallard, M., & Takebayashi, N. (2010). Surface electromyographic biofeedback to optimize performance in daily life: Improving physical fitness and health at the worksite. Japanese Journal of Biofeedback Research, 37(1), 19-28. https://doi.org/10.20595/jjbf.37.1_19
Peper, E., Gibney, K. & Holt, C. (2002). Make health happen: Training yourself to create wellness. Dubuque, IA: Kendall-Hunt. https://he.kendallhunt.com/product/make-health-happen-training-yourself-create-wellness
Peper, E. & Harvey, R. (2021). Causes of TechStress and ‘Technology-Associated Overuse’ Syndrome and Solutions for Reducing Screen Fatigue, Neck and Shoulder Pain, and Screen Addiction. Townsend Letter-The examiner of Alternative Medicine, Oct 28, 2021. https://www.townsendletter.com/article/459-techstress-how-technology-is-hurting-us
Peper, E., Harvey, R. & Tylova, H. (2006). Stress protocol for assessing computer related disorders. Biofeedback. 34(2), 57-62. https://www.researchgate.net/publication/242549995_FEATURE_Stress_Protocol_for_Assessing_Computer-Related_Disorders
Peper, E. & Tibbetts, V. (1994). Effortless diaphragmatic breathing. Physical Therapy Products. 6(2), 67-71. Also in: Electromyography: Applications in Physical Therapy. Montreal: Thought Technology Ltd. https://www.bfe.org/protocol/pro10eng.htm
Rubenfeld, I. (2001). The listening hands: Self-healing through Rubenfeld Synergy method of talk and touch. New York: Random House. https://www.amazon.com/Listening-Hand-Self-Healing-Through-Rubenfeld/dp/0553379836
Sella, G. E. (2019). Surface EMG (SEMG): A Synopsis. Biofeedback, 47(2), 36–43. https://doi.org/10.5298/1081-5937-47.1.05
Thayer, R.E. (1996). The origin of everyday moods—Managing energy, tension, and stress. New York: Oxford University Press. https://www.amazon.com/Origin-Everyday-Moods-Managing-Tension/dp/0195118057
Whatmore, G. and Kohli, D. The Physiopathology and Treatment of Functional Disorders. New York: Grune and Stratton, 1974. https://www.amazon.com/physiopathology-treatment-functional-disorders-biofeedback/dp/0808908510
[i] Dysponesis involves misplaced muscle activities or efforts that are usually covert and do not add functionally to the movement. From: Dys” meaning bad, faulty or wrong, and “ponos” meaning effort, work or energy (Whatmore and Kohli, 1974)
[ii] A meso-break is a 10 to 90 second break that consists of a change in work position, movement or a structured activity such as stretching that automatically relaxes those muscles that were previously activated while performing a task.
360-Degree Belly Breathing with Jamie McHugh
Posted: April 26, 2024 Filed under: attention, Breathing/respiration, emotions, healing, health, meditation, mindfulness, Pain/discomfort, relaxation, self-healing | Tags: abdominal braething, belly breathing, daiphragm, effortless breathing, passive attention, self-acceptance, somatic awreness 4 Comments
Breathing is a whole mind-body experience and reflects our physical, cognitive and emotional well-being. By allowing the breath to occur effortlessly, we provide ourselves the opportunity to regenerate. Although there are many directed breathing practices that specifically directs us to inhale or exhale at specific rhythms or depth to achieve certain goals, healthy breathing is whole body experience. Many focus on being paced at a specific rhythm such as 5.5 breath per minute; however, effortless breathing is dynamic and constantly changing. It is contstantly adapting to the body’s needs: sometimes the breath is slightly slower, sometimes slightly faster, sometimes slightly deeper, sometimes slightly more shallower. The breathing process is effortless. This process can be described by the Autogenic training phrase, “It breathes me” (Luthe, 1969; Luthe, 1979; Luthe & de Rivera, 2015). Read the essay by Jamie McHugh, Registered Master Somatic Movement Therapist and then let yourself be guided in this non-striving somatic approach to allow effortless 360 degree belly breathing for regeneration.
The 360 degree belly breathing by Jamie McHugh, MSMT, is a somatic exploration to experience that breathing is not just abdominal breathing by letting the belly expand forward, but a rhythmic 360 degree increase and decrease in abdominal volume without effort. This effortless breathing pattern can often be observed in toddlers when they sit peacefully erect on the floor. This pattern of breathing not only enhances gas exchange, more importantly, it enhances abdominal blood and lymph circulation.
“The usual psychodynamic foundation for the self-experience is that of hunger, not breath. The body is experienced as an alien entity that has to be kept satisfied; the way an anxious mother might experience a new baby. When awareness is shifted from appetite to breath, the anxieties about not being enough are automatically attenuated. It requires a settling down or relaxing into one’s own body. When this fluidity moves to the forefront of awareness…there is a relaxation of the tensed self…and the emergence of a simpler, breath-based self that is capable of surrender to the moment.” – Mark Epstein (2013).
The intention behind 360 Degree Belly Breathing is to access and express the movement of the breath in all three dimensions. This is the basis for all subsequent somatic explorations within the Embodied Mindfulness protocol, a body-based approach to traditional meditation practices I have developed over the past 20 years (McHugh, 2016). Embodied Mindfulness explores the inner landscape of the body with the essential somatic technologies of breath, vocalization, self-contact, stillness and subtle movement. We focus and sustain mental attention while pleasurably cultivating bodily calm and clarity as a daily practice for survival in these turbulent times. Coupled with individual variations and experimentation, this practice becomes a reliable sanctuary from overwhelm, scattered attention, and emotional turmoil.
The Central Diaphragm

The central diaphragm, a dome-shaped muscular sheath that divides the thorax (chest) and the abdomen (belly), is the primary mechanism for breathing. It is the floor for your heart and lungs and the ceiling for your belly. The central diaphragm is a mostly impenetrable divide, with a few openings through it for the aorta, vena cava and the esophagus. Each time you inhale, the diaphragm contracts and flattens out a bit as it presses down towards your pelvis. Each time you exhale, the diaphragm relaxes and floats back up towards your heart. The motion of the diaphragm impacts the barometric pressure in your chest: the downward movement of the diaphragm on the inhale pulls oxygen into your lungs, and the subsequent exhale expels carbon dioxide into the world as the diaphragm releases upwards.
The movement of the diaphragm is twofold: involuntary and voluntary. Involuntary, ordinary breathing is a homebase and a point of return. Breathing just automatically happens – you don’t have to think about it. Breathing is also voluntary; you can choose to change the tempo (quick or slow), the duration (short or long) and quality (smooth or sharp) of this movement to “charge up and chill out” at will. Knowing how to collaborate with your diaphragm, discovering your own rhythm of diaphragmatic action, and undulating between the automatic and the chosen is a foundation for physiological equilibrium and emotional “self-soothing”.
Watch these two brief videos to get a visual image of your diaphragm in motion:
Beginning Sitting Practice
“When your back becomes straight, your mind will become quiet.” – Shunryu Suzuki
What does it mean to have a “straight back”? What are the inner coordinates and outer parameters of this position in space? And what kind of environment is needed to support this uprightness? This simple orientation to sitting can create more comfort, ease and support in your structure, which will stimulate more fluidity in your breathing and your thinking.
As you sit on a chair, consider two points of focus: body and environment. Can I sit upright with ease and comfort on this chair? If not, what changes can I make with my body and how can I adapt the environment of this chair to meet my needs? Since we are all various heights, it is not surprising a one-size-fits-all chair would need adaptation. Don’t be content with your first solution – experiment until you find just the right configuration. Valuing and seeking bodily comfort and ease are simple yet profound acts of self-kindness.
Do you need to move your pelvis forward on the chair or back? If you move your pelvis back, do you get the necessary support from the back of the chair for your pelvic bowl? If the back of the chair is too far away and/or makes you lean back into space, place a small cushion or two between the back of the chair and the base of your spine. With your back supported, are your feet on the floor? If not, place a folded blanket or a cushion under them.
With pelvis and feet in place, take a few full breaths to stabilize your pelvis and let your weight drop down through your sitz bones into the chair. The upper body receives more support from the core muscles of the lower body when your center of gravity drops – you don’t have to work so hard to maintain uprightness. Finally, rock on your sitz bones forward, backward, and side-to-side. Movement awakens bodily feedback so you can feel where center is in this moment. That sense of center will continue to change throughout the duration of the practice period so feel free to periodically adjust your position.
After this initial structural orientation, the next step is attending to the combination of breath and self-contact to fill out our self-perception. Self-contact is like using a magnifying glass – focusing the mind by feeling the substance of the belly’s movement in our hands. Since the diaphragm is a 360-degree phenomenon that generates movement in our sides and our back as well as our front, spreading awareness out not only creates different patterns of muscular activation – it also changes the brain’s map of the body and how we perceive ourselves. This change of orientation over time recalibrates our alignment and how we settle in ourselves, with awareness of our back in equal proportion to our front and sides.
360-Degree Belly Breath
“To stop your mind does not mean to stop the activities of the mind. It means your mind pervades your whole body.” – Shunryu Suzuki
Read text below or be guided by the audio file or YouTube video. http://somaticexpression.com/classes/360DegreeBreathingwithJamieMcHugh.mp3
Sit comfortably and place your hands on the front of your belly. With each inhale, become aware of the forward movement of your belly swelling. Then, with each exhale, notice the release of your belly and the settling back to center. Give this action and each subsequent action at least 5-7 breath cycles. Intersperse this way of breathing with ordinary, effortless breathing by letting the body breathe automatically. Return time and again to ordinary breathing, letting go of the focus and the effort to rest in the aftermath.
Now, slide your hands to the sides of your belly. Notice with each breath cycle how your belly moves laterally out to the sides on the inhale and then settles back to center again on the exhale.
Now, slide your hands to the back of your belly. You may wish to make contact with the back of your hands instead of your palms if it is more comfortable. With each inhale, focus on the movement into the backspace – this will be much smaller than the movement to the front; and with each exhale, the movement settling back to center.
Finally, connect all three directions: your belly radiates out 360 degrees on the horizon with each inhale, simultaneously moving forward, backward, and out to both sides, and then settles inward with each exhale.
Finish with open awareness – scanning your whole inner landscape from feet to head, back to front, and center to extremities, and letting your body breathe itself, as you notice what is alive in you now.
Inhale – Belly Radiates Outwards; Exhale – Belly Settles Inwards
“The belly is an extraordinary diagnostic instrument. It displays the armoring of the heart as a tension in the belly. Trying tightens the belly. Trying stimulates judgment. Hard belly is often judging belly. Observing the relative openness or closedness of the belly gives insight into when and how we are holding (on) to our pain. The deeper our relationship to the belly, the sooner we discover if we are holding in the mind or opening into the heart.” – Steven Levine (1991)
The contact of your hands on your belly helps the mind pay attention to the subtle movement created by the inhale-exhale cycle of the diaphragm. The combination of tactility and interoceptive awareness focusing on the belly shifts attention into our “second brain” (the enteric nervous system) and signals the mind it can rest and soften. More pleasurable sensation is often accompanied by an emergent feeling of safety as you settle into sensing the rhythm of a slower, more even breath, creating a feedback loop between bodily/somatic ease and mental calm. Giving yourself some daily “breathing room” in this way can help you build the calm muscle!
Naturally, there can be hiccups along the way so it is not all unicorns and rainbows! By giving the mind bodily tasks to accomplish, particularly in relationship to deepening and expanding the movement of the breath, we ease the self into a slower, more receptive state of being. Yet, in this receptive state of ease, whatever is in the background of awareness can arise and slip through the “border control”, sometimes taking us by surprise and causing distress. Depending upon the nature of the information, there are layers of action strategies that can be progressively taken to modulate and buffer what arises:
Tether your awareness to the breath rhythm with hands on your belly to stay present as a witness. Next step up: open your eyes softly and look around to orient in your present environment. Further step up: breath flow, hands-on belly, eyes open a wee bit looking around, and adding simple movement, like rocking a bit in all directions or expressing an exhale as a sigh, a yawn or a hum.
Note: If you find your personal resources are insufficient, find a guide to work with one-on-one to discover your own individual path for increasing the “window of capacity”. Above all, be gentle with yourself – take your time – cultivate your garden – and enjoy your breath!
References
Epstein, M. (2013) Thoughts without a Thinker: Psychotherapy from a Buddhist Perspective. New York: Basic Books. https://www.amazon.com/Thoughts-Without-Thinker-Psychotherapy-Perspective/dp/0465050948
Levine, S. (1991). Guided Meditations, Explorations and Healings. New York: Anchor. https://www.amazon.com/Guided-Meditations-Explorations-Healings-Stephen/dp/0385417373
Luthe, W. (1969). Autogenic Therapy Volume 1 Autogenic Methods. New York: Grune and Stratton. https://www.amazon.com/Autogenic-Therapy-1-Methods/dp/B0013457B4/
Luthe, W. (1979). About the Methods of Autogenic Therapy. In: Peper, E., Ancoli, S., Quinn, M. (eds). Mind/Body Integration. Springer, Boston, MA. https://doi.org/10.1007/978-1-4613-2898-8_12
Luthe, W. & de Rivera, L. (2015). Wolfgang Luthe Introductory workshop: Introduction to the Methods of Autogenic Training, Therapy and Psychotherapy (Autogenic Training & Psychotherapy). CreateSpace Independent Publishing Platform. https://www.amazon.com/WOLFGANG-LUTHE-INTRODUCTORY-WORKSHOP-Psychotherapy/dp/1506008038/
Quick Rescue Techniques When Stressed
Posted: February 4, 2024 Filed under: attention, behavior, biofeedback, Breathing/respiration, CBT, cognitive behavior therapy, education, emotions, Evolutionary perspective, Exercise/movement, health, mindfulness, Neck and shoulder discomfort, posture, relaxation, stress management, Uncategorized | Tags: alarm reaction, anxiety, box breathing, Breathing, conditioning, defense reaction, health, huming, Parasympathetic response, rumination, safety, sniff inhale, somatic practices, stress, sympathetic arousal, tactical breathing, Toning, yoga 9 CommentsErik Peper, PhD, Yuval Oded, PhD, and Richard Harvey, PhD
Adapted from Peper, E., Oded, Y, & Harvey, R. (2024). Quick somatic rescue techniques when stressed. Biofeedback, 52(1), 18–26. https://doi.org/10.5298/982312 https://www.researchgate.net/publication/380481426

“If a problem is fixable, if a situation is such that you can do something about it, then there is no need to worry. If it’s not fixable, then there is no help in worrying. There is no benefit in worrying whatsoever.” ― Dalai Lama XIV
To implement the Dalai Lama’s quote is challenging. When caught up in an argument, being angry, extremely frustrated, or totally stressed, it is easy to ruminate, worry. It is much more challenging to remember to stay calm. When remembering the message of the Dalai Lama’s quote, it may be possible to shift perspective about the situation although a mindful attitude may not stop ruminating thoughts. The body typically continues to reacti to the torrents of thoughts that may occur when rehashing rage over injustices, fear over physical or psychological threats, or profound grief and sadness over the loss of a family member. Some people become even more agitated and less rational as illustrated in the following examples.
I had an argument with my ex and I am still pissed off. Each time I think of him or anticipate seeing them, my whole body tightened. I cannot stomach seeing him and I already see the anger in his face and voice. My thoughts kept rehashing the conflict and I am getting more and more upset.
A car cut right in front of me to squeeze into my lane. I had to slam on my brakes. What an idiot! My heart rate was racing and I wanted to punch the driver.
When threatened, we respond quickly in our thoughts and body with a defense reaction that may negatively affect those around us as well as ourselves. What can we do to interrupt negative stress reactions?
Background
Many approaches exist that allow us to become calmer and less reactive. General categories include techniques of cognitive reappraisal (seeing the situation from the other person’s point of view and labeling your own feelings and emotions) and stress management techniques. Practices that are beneficial include mindfulness meditation, benign humor (versus gallows humor), listening to music, taking a time out while implementing a variety of self-soothing practices, or incorporating slow breathing (e.g., heart rate variability and/or box breathing) throughout the day.
No technique fits all as we respond differently to our stressful life circumstances. For example, some people during stress react with a “tend and befriend stress response” (Cohen & Lansing, 2021; Taylor et al., 2000). This response appears to be mostly mediated by the hormone oxytocin acting in ways that sooth or calm the nervous system as an analgesic. These neurophysiological mechanisms of the soothing with the calming analgesic effects of oxytocin have been characterized in detail by Xin, et al. (2017).
The most common response is a fight/flight/freeze stress response that is mediated by excitatory hormones such as adrenalin and inhibitory neurotransmitters such as gamma amino butyric acid (GABA). There is a long history of fight/flight/freeze stress response research, which is beyond the scope of this blog with major theories and terms such as interior milleau (Bernard, 1872); homeostasis and fight/flight (Cannon, 1929); general adaptation syndrome (Selye, 1951); polyvagal theory (Porges, 1995); and, allostatic load (McEwen, 1998). A simplified way to start a discussion about stress reactions begins with the fight/flight stress response. When stressed our defense reactions are triggered. Our sympathetic nervous system becomes activated our mind and body stereotypically responds as illustrated in Figure 1.

Figure 1. An intense confrontation tends to evoke a stress response (reproduced from Peper et al., 2020).
The flight/fight response triggers a cascade of stress hormones or neurotransmitters (e.g., hypothalamus-pituitary-adrenal cascade) and produces body changes such as the heart pounding, quicker breathing, an increase in muscle tension and sweating. Our body mobilizes itself to protect itself from danger. Our focus is on immediate survival and not what will occur in the future (Porges, 2021; Sapolsky, 2004). It is as if we are facing an angry lion—a life-threatening situation—and we feel threatened and unsafe.
Rather than sitting still, a quick effective strategy is to interrupt this fight/flight response process by completing the alarm reaction such as by moving our muscles (e.g., simulating a fight or flight behavior) before continuing with slower breathing or other self-soothing strategies. Many people have experienced their body tension is reduced and they feel calmer when they do vigorous exercise after being upset, frustrated or angry. Similarly, athletes often have reported that they experience reduced frequency and/or intensity of negative thoughts after an exhausting workout (Thayer, 2003; Liao et al., 2015; Basso & Suzuki, 2017).
Becoming aware of the escalating cascades of physical, behavioral and psychological responses to a stressor is the first step in interrupting the escalating process. After becoming aware, reduce the body’s arousal and change the though patterns using any of the techniques described in this blog. The self-regulation skills presented in this blog are ideally over-learned and automated so that these skills can be rapidly implemented to shift from being stressed to being calm. Examples of skills that can shift from sympathetic neervous system overarousal to parasympathetic nervous system calm include techniques of autogenic traing (Schulz & Luthe, 1959), the quieting reflex developed by Charles Stroebel in 1985 or more recently rescue breathing developed by Richard Gevirtz (Stroebel, 1985; Gevirtz, 2014; Peper, Gibney & Holt, 2002; Peper & Gibney, 2003).
Concepts underlying the rescue techniques
- Psychophysiological principle: “Every change in the physiological state is accompanied by an appropriate change in the mental-emotional state, conscious or unconscious, and conversely, every change in the mental-emotional state, conscious or unconscious, is accompanied by an appropriate change in the physiological state” (Green et al. 1970, p. 3).
- Posture evokes memories and feelings associated with the position. When the body posture is erect and tall while looking slightly up. It is easier to evoke empowering, positive thoughts and feelings. When looking down it is easier to evoke hopeless, helpless and powerless thoughts and feelings (Peper et al., 2017).
- Healing occurs more easily when relaxed and feeling safe. Feeling safe and nurtured enhances the parasympathetic state and reduces the sympathetic state. Use memory recall to evoke those experiences when you felt safe (Peper, 2021).
- Interrupting thoughts is easier with somatic movement than by redirecting attention and thinking of something else without somatic movement.
- Focus on what you want to do not want to do. Attempting to stop thinking or ruminating about something tends to keeps it present (e.g., do not think of pink elephants. What color is the elephant? When you answer, “not pink,” you are still thinking pink). A general concept is to direct your attention (or have others guide you) to something else (Hilt & Pollak, 2012; Oded, 2018; Seo, 2023).
- Skill mastery takes practice and role rehearsal (Lally et al., 2010; Peper & Wilson, 2021).
- Use classical conditioning concepts to facilitate shifting states. Practice the skills and associate them with an aroma, memory, sounds or touch cues. Then when you the situation occurs, use these classical conditioned cues to facilitate the regeneration response (Peper & Wilson, 2021).
Rescue techniques
Coping When Highly Stressed and Agitated
- Complete the alarm/defense reaction with physical activity (Be careful when you do these physical exercises if you have back, hip, knee, or ankle problems).
- Acknowledge you have reacted and have chosen to interrupt your automatic response.
- Check whether the situation is actually a threat. If yes, then do anything to get out of immediate danger (yell, scream, fight, run away, or dial 911).
- If there is no actual physical threat, then leave the situation and perform vigorous physical activity to complete your alarm reaction, such as going for a run or walking quickly up and down stairs. As you do the exercise, push yourself so that the muscles in your thighs are aching, which focusses your attention on the sensations in your thighs. In our experience, an intensive run for 20 minutes quiets the brain while it often takes 40 minutes when walking somewhat quickly.
- After recovering from the exhaustive exercise, explore new options to resolve the conflict.
- Complete the alarm/defense reaction and evoke calmness with the S.O.S™ technique (Oded, 2023)
- Acknowledge you have reacted and have chosen to interrupt your automatic response.
- Squat against a wall (similar to the wall-sit many skiers practice). While tensing your arms and fists as shown in Figure 2, gaze upward because it is more difficult to engage in negative thinking while looking upwards. If you continue to ruminate, then scan the room for object of a certain color or feature to shift visual attention and be totally present on the visual object.
- Do this set of movements for 7 to 10 seconds or until you start shaking. Than stand up and relax hands and legs. While standing, bounce up and down loosely for 10 to 15 seconds as you become aware of the vibratory sensations in your arms and shoulders, as shown in Figure 3.

Figure 2.Defense position wall-sit to tighten muscles in the protective defense posture (Oded, 2023). Figure 3. Bouncing up and down to loosen muscles ((Oded, 2023).
- Acknowledge you have reacted and have chosen to interrupt your automatic response. Swing your arms back and forth for 20 seconds. Allow the arms to swing freely as illustrated in Figure 4.

Figure 4. Swinging the arms to loosen the body and spine (Oded, 2023).
- Rest and ground. Lie on the floor and put your calves and feet on a chair seat so that the psoas muscle can relax, as illustrated in Figure 5. Allow yourself to be totally supported by the floor and chair. Be sure there is a small pillow under your head and put your hand on your abdomen so that you can focus on abdominal breathing.

Figure 5. Lying down to allow the psoas muscle to relax and feel grounded (Oded, 2023).
- While lying down, imagine a safe place or memory and make it as real as possible. It is often helpful to listen to a guided imagery or music. The experience can be enhanced if cues are present that are associated with the safe place, such as pictures, sounds, or smells. Continue to breathe effortlessly at about six breaths per minute. If your attention wanders, bring it back to the memory or to the breathing. Allow yourself to rest for 10 minutes.
In most cases, thoughts stop and the body’s parasympathetic activity becomes dominant as the person feels safe and calm. Usually, the hands warm and the blood volume pulse amplitude increases as an indicator of feeling safe, as shown in Figure 6.

Figure 6. Blood volume pulse increases as the person is relaxing, feels safe and calm.
Coping When You Can’t Get Away (adapted from Peper, Harvey & Faass, 2020)
In many cases, it is difficult or embarrassing to remove yourself from the situation when you are stressed out such as at work, in a business meeting or social gathering.
- Become aware that you have reacted.
- Excuse yourself for a moment and go to a private space, such as a restroom. Going to the bathroom is one of the only acceptable social behaviors to leave a meeting for a short time.
- In the bathroom stall, do the 5-minute Nyingma exercise, which was taught by Tarthang Tulku Rinpoche in the tradition of Tibetan Buddhism, as a strategy for thought stopping (see Figure 7). Stand on your toes with your heels touching each other. Lift your heels off the floor while bending your knees. Place your hands at your sides and look upward. Breathe slowly and deeply (e.g., belly breathing at six breaths a minute) and imagine the air circulating through your legs and arms. Do this slow breathing and visualization next to a wall so you can steady yourself if necessary to keep balance. Stay in this position for 5 minutes or longer. Do not straighten your legs—keep squatting despite the discomfort. In a very short time, your attention is captured by the burning sensation in your thighs. Continue. After 5 minutes, stop and shake your arms and legs.

Figure 7. Stressor squat Nyingma exercise (reproduced from Peper et al., 2020).
- Follow this practice with slow abdominal breathing to enhance the parasympathetic response. Be sure that the abdomen expands as the inhalation occurs. Breathe in and out through the nose at about six breaths per minute.
- Once you feel centered and peaceful, return to the room.
- After this exercise, your racing thoughts most likely will have stopped and you will be able to continue your day with greater calm.
What to do When Ruminating, Agitated, Anxious or Depressed
(adapted from Peper, Harvey, & Hamiel, 2019).
- Shift your position by sitting or standing erect in a power position with the back of the head reaching upward to the ceiling while slightly gazing upward. Then sniff quickly through nose, hold and again sniff quickly then very slowly exhale. Be sure as you exhale your abdomen constricts. Then sniff again as your abdomen gets bigger, hold, and sniff one more time letting the abdomen get even bigger. Then, very slow, exhale through the nose to the internal count of six (adapted from Balban et al., 2023). When you sniff or gasp, your racing thoughts will stop (Peper et al., 2016).
- Continue with box breathing (sometimes described as tactical breathing or battle breathing) by exhaling slowly through your nose for 4 seconds, holding your breath for 4 seconds, inhaling slowly for 4 seconds through your nose, holding your breath for 4 seconds and then repeating this cycle of breathing for a few minutes (Röttger et al., 2021; Balban et al., 2023). Focusing your attention on performing the box breathing makes it almost impossible to think of anything else. After a few minutes, follow this with slow effortless diaphragmatic breathing at about six breaths per minute. While exhaling slowly through your nose, look up and when you inhale imagine the air coming from above you. Then as you exhale, imagine and feel the air flowing down and through your arms and legs and out the hands and feet.
- While gazing upward, elicit a positive memory or a time when you felt safe, powerful, strong and/or grounded. Make the positive memory as real as possible.
- Implement cognitive strategies such as reframing the issue, sending goodwill to the person, seeing the problem from the other person’s point of view, and ask is this problem worth dying over (Peper, Harvey, & Hamiel, 2019).
What to Do When Thoughts Keep Interrupting
Practice humming or toning. When you are humming or toning, your focus is on making the sound and the thoughts tend to stop. Generally, breathing will slow down to about six breaths per minute (Peper, Pollack et al., 2019). Explore the following:
- Box breathing (Röttger et al., 2021; Balban et al., 2023)
- Humming also known as bee breath (Bhramari Pranayama) (Abishek et al., 2019; Yoga, 2023) – Allow the tongue to rest against the upper palate, sit tall and erect so that the back of the head is reaching upward to the ceiling, and inhale through your nose as the abdomen expands. Then begin humming while the air flows out through your nose, feel the vibration in the nose, face and throat. Let humming last for about 7 seconds and then allow the air to blow in through the nose and then hum again. Continue for about 5 minutes.
- Toning – Inhale through your nose and then vocalize a single sound such as Om. As you vocalize the lower sound, feel the vibration in your throat, chest and even going down to the abdomen. Let each toning exhalation last for about 6 to 7 seconds and then inhale through your nose. Continue for about 5 minutes (Peper, al., 2019).
Many people report that after practice these skills, they become aware that they are reacting and are able to reduce their automatic reaction. As a result, they experience a significant decrease in their stress levels, fewer symptoms such as neck and holder tension and high blood pressure, and they feel an increase in tranquility and the ability to communicate effectively.
Practicing these skills does not resolve the conflicts; they allow you to stop reacting automatically. This process allows you a time out and may give you the ability to be calmer, which allows you to think more clearly. When calmer, problem solving is usually more successful. As phrased in a popular meme, “You cannot see your reflection in boiling water. Similarly, you cannot see the truth in a state of anger. When the waters calm, clarity comes” (author unknown).

Boiling water (photo modified from: https://www.facebook.com/photo/?fbid=388991500314839&set=a.377199901493999)
Below are additional resources that describe the practices. Please share these resources with friends, family and co-workers.
Stressor squat instructions
Toning instructions
Diaphragmatic breathing instructions
Reduce stress with posture and breathing
Conditioning
References
Abishek, K., Bakshi, S. S., & Bhavanani, A. B. (2019). The efficacy of yogic breathing exercise bhramari pranayama in relieving symptoms of chronic rhinosinusitis. International Journal of Yoga, 12(2), 120–123. https://doi.org/10.4103/ijoy.IJOY_32_18
Balban, M. Y., Neri, E., Kogon, M. M., Weed, L., Nouriani, B., Jo, B., Holl, G., Zeitzer, J. M., Spiegel, D., Huberman, A. D. (2023). Brief structured respiration practices enhance mood and reduce physiological arousal. Cell Reports Medicine, 4(1), 10089. https://doi.org/10.1016/j.xcrm.2022.100895
Basso, J. C. & Suzuki, W. A. (2017). The effects of acute exercise on mood, cognition, neurophysiology, and neurochemical pathways: A review. Brain Plast, 2(2), 127–152. https://doi.org/10.3233/BPL-160040
Bernard, C. (1872). De la physiologie générale. Paris: Hachette livre. https://www.amazon.ca/PHYSIOLOGIE-GENERALE-BERNARD-C/dp/2012178596
Cannon, W. B. (1929). Organization for Physiological Homeostasis. Physiological Reviews, 9, 399–431. https://doi.org/10.1152/physrev.1929.9.3.399
Cohen, L. & Lansing, A. H. (2021). The tend and befriend theory of stress: Understanding the biological, evolutionary, and psychosocial aspects of the female stress response. In: Hazlett-Stevens, H. (eds), Biopsychosocial Factors of Stress, and Mindfulness for Stress Reduction. pp. 67–81, Springer, Cham. https://doi.org/10.1007/978-3-030-81245-4_3
Gevirtz, R. (2014). HRV Training and its Importance – Richard Gevirtz, Ph.D., Pioneer in HRV Research & Training. Thought Technology. Accessed December 29, 2023. https://www.youtube.com/watch?v=9nwFUKuJSE0
Green, E. E., Green, A. M., & Walters, E. D. (1970). Voluntary control of internal states: Psychological and physiological. Journal of Transpersonal Psychology, 2, 1–26. https://atpweb.org/jtparchive/trps-02-70-01-001.pdf
Hilt, L. M., & Pollak, S. D. (2012). Getting out of rumination: comparison of three brief interventions in a sample of youth. Journal of Abnormal Child Psychology, 40(7), 1157–1165.
https://doi.org/10.1007/s10802-012-9638-3
Lally, P., VanJaarsveld, C. H., Potts, H. W., & Wardle, J. (2010). How habits are formed: Modelling habit formation the real world. European Journal of Social Psychology, 40, 998–1009. https://doi.org/10.1002/ejsp.674
Liao, Y., Shonkoff, E. T., & Dunton, G. F. (2015). The acute relationships between affect, physical feeling states, and physical activity in daily life: A review of current evidence. Frontiers in Psychology. 6, 1975. https://doi.org/10.3389/fpsyg.2015.01975
McEwen, B. S. (1998). Stress, adaptation, and disease: Allostasis and allostatic load. Annals of the New York Academy of Sciences, 840(1), 33–44.
https://doi.org/10.1111/j.1749-6632.1998.tb09546.x
Oded, Y. (2018). Integrating mindfulness and biofeedback in the treatment of posttraumatic stress disorder. Biofeedback, 46(2), 37-47. https://doi.org/10.5298/1081-5937-46.02.03
Oded, Y. (2023). Personal communication. S.O.S 1™ technique is part of the Sense Of Safety™ method. www.senseofsafety.co
Peper, E. (2021). Relive memory to create healing imagery. Somatics, XVIII(4), 32–35.https://www.researchgate.net/publication/369114535_Relive_memory_to_create_healing_imagery
Peper, E., Gibney, K.H. & Holt. C. (2002). Make Health Happen: Training Yourself to Create Wellness. Dubuque, IA: Kendall-Hunt. https://he.kendallhunt.com/product/make-health-happen-training-yourself-create-wellness
Peper, E., & Gibney, K.H. (2003). A teaching strategy for successful hand warming. Somatics. XIV(1), 26–30. https://www.researchgate.net/publication/376954376_A_teaching_strategy_for_successful_hand_warming
Peper, E., Harvey, R., & Faass, N. (2020). TechStress: How Technology is Hijacking Our Lives, Strategies for Coping, and Pragmatic Ergonomics. North Atlantic Books. https://www.amazon.com/Beyond-Ergonomics-Prevent-Fatigue-Burnout/dp/158394768X
Peper, E., Harvey, R., & Hamiel, D. (2019). Transforming thoughts with postural awareness to increase therapeutic and teaching efficacy. NeuroRegulation, 6(3),153–160. https://doi.org/10.15540/nr.6.3.153
Peper, E., Lee, S., Harvey, R., & Lin, I-M. (2016). Breathing and math performance: Implication for performance and neurotherapy. NeuroRegulation, 3(4), 142–149. http://dx.doi.org/10.15540/nr.3.4.142
Peper, E., Lin, I-M, Harvey, R., & Perez, J. (2017). How posture affects memory recall and mood. Biofeedback, 45(2), 36–41. https://doi.org/10.5298/1081-5937-45.2.01
Peper, E., Pollack, W., Harvey, R., Yoshino, A., Daubenmier, J. & Anziani, M. (2019). Which quiets the mind more quickly and increases HRV: Toning or mindfulness? NeuroRegulation, 6(3), 128–133. https://www.neuroregulation.org/article/view/19345/13263
Peper, E. & Wilson, V. (2021). Optimize the learning state: Techniques and habits. Biofeedback, 9(2), 46–49. https://doi.org/10.5298/1081-5937-49-2-04
Porges, S. W. (1995). Orienting in a defensive world: Mammalian modifications of our evolutionary heritage. A polyvagal theory. Psychophysiology, 32(4), 301–318. https://doi.org/10.1111/j.1469-8986.1995.tb01213.x
Porges, S.W. (2021) Cardiac vagal tone: a neurophysiological mechanism that evolved in mammals to dampen threat reactions and promote sociality. World Psychiatry, 20(2),296-298. Porges SW. Cardiac vagal tone: a neurophysiological mechanism that evolved in mammals to dampen threat reactions and promote sociality. World Psychiatry. 2021 Jun;20(2):296-298. https://doi.org10.1002/wps.20871
Röttger, S., Theobald, D. A., Abendroth, J., & Jacobsen, T. (2021). The effectiveness of combat tactical breathing as compared with prolonged exhalation. Applied Psychophysiology and Biofeedback, 46, 19–28. https://doi.org/10.1007/s10484-020-09485-w
Sapolsky, R. (2004). Why zebras don’t get ulcers (3rd ed.). New York:Holt. https://www.amazon.com/Why-Zebras-Dont-Ulcers-Third/dp/0805073698/
Schultz, J. H., & Luthe, W. (1959). Autogenic training: A psychophysiologic approach to psychotherapy. Grune & Stratton. https://www.google.com/books/edition/Autogenic_Training/y8SwQgAACAAJ?hl=en
Selye, H. (1951). The general-adaptation-syndrome. Annual Review of Medicine, 2(1), 327–342. https://doi.org/10.1146/annurev.me.02.020151.001551
Seo, H. (2023). How to stop ruminating. The New York Times. Accessed January 3, 2024. https://www.nytimes.com/2023/02/01/well/mind/stop-rumination-worry.html
Stroebel, C. F. (1985). QR: The Quieting Reflex. Berkley. https://www.amazon.com/Qr-quieting-reflex-Charles-Stroebel/dp/0425085066
Taylor, S. E., Klein, L. C., Lewis, B. P., Gruenewald, T. L., Gurung, R. A. R., & Updegraff, J. A. (2000). Biobehavioral responses to stress in females: Tend-and-befriend, not fight-or-flight. Psychological Review, 107(3), 411–429. https://doi.org/10.1037/0033-295X.107.3.411
Thayer, R. E. (2003). Calm energy: How people regulate mood with food and exercise. Oxford University Press. https://www.amazon.com/Calm-Energy-People-Regulate-Exercise/dp/0195163397
Xin, Q., Bai, B., & Liu, W. (2017). The analgesic effects of oxytocin in the peripheral and central nervous system. Neurochemistry International, 103, 57–64. https://doi.org/10.1016/j.neuint.2016.12.021
Yoga, N. (2023). This simple breath practice is scientifically proven to calm your mind. The nomadic yogi. Accessed December 31, 2023. https://www.leahsugerman.com/blog/bhramari-pranayama-humming-bee-breath#
Reduce the risk for colds and flu and superb science podcasts
Posted: January 24, 2024 Filed under: attention, behavior, education, Evolutionary perspective, Exercise/movement, healing, health, Nutrition/diet, self-healing, stress management, Uncategorized, vision | Tags: colds, darkness, flu, influenza, light 2 Comments
What can we do to reduce the risk of catching a cold or the flu? It is very challenging to make sense out of all the recommendations found on internet and the many different media site such as X(Twitter), Facebook, Instagram, or TikTok. The following podcasts are great sources that examine different topics that can affect health. They are in-depth presentations with superb scientific reasoning.
Huberman Lab podcasts discusses science and science based tools for everyday life. https://www.hubermanlab.com/podcast. Select your episode and they are great to listen to on your cellphone.
THE PODCAST episode, How to prevent and treat cold and flu, is outstanding. Skip the long sponsor introductdion and start listening at the 6 minute point. In this podcast, Professor Andrew Huberman describes behavior, nutrition and supplementation-based tools supported by peer-reviewed research to enhance immune system function and better combat colds and flu. I also dispel common myths about how the cold and flu are transmitted and when you and those around you are contagious. I explain if common preventatives and treatments such as vitamin C, zinc, vitamin D and echinacea work. I also highlight other compounds known to reduce contracting and duration of colds and flu. I discuss how to use exercise and sauna to bolster the immune response. This episode will help listeners understand how to reduce the chances of catching a cold or flu and help people recover more quickly from and prevent the spread of colds and flu.
PODCAST, ScienceVS, is an outstanding podcast series that takes on fads, trends, and opinionated mob to find out what’s fact, what’s not, and what’s somewhere in between. Select your episode and listen.
Link: https://gimletmedia.com/shows/science-vs/episodes#show-tab-picker

PODCAST episode, The Journal club podcast and Youtube, presentation from Huberman Lab is a example of outstanding scientific reasoning. In this presentation, Professor Andrew Huberman and Dr. Peter Attia (author of Outlive: The Science and Art of Longevity) discuss two peer-reviewed scientific papers in-depth. The first discussion explores the role of bright light exposure during the day and dark exposure during the night and its relationship to mental health. The second paper explores a novel class of immunotherapy treatments to combat cancer.
Is mindfulness training old wine in new bottles?
Posted: January 11, 2024 Filed under: attention, behavior, biofeedback, Breathing/respiration, CBT, cognitive behavior therapy, healing, health, meditation, self-healing, stress management | Tags: anxiety, autogenic training, biofeedback, health, meditation, mental-health, mindfulness, pain, passive attention, progressive muscle relaxation, wellness, yoga 2 CommentsAdapted from: Peper, E., Harvey, R., & Lin, I-M. (2019). Mindfulness training has themes common to other technique. Biofeedback. 47(3), 50-57. https://doi.org/10.5298/1081-5937-47.3.02
This extensive blog discusses the benefits of mindfulness-based meditation (MM) techniques and explores how similar beneficial outcomes occur with other mind-centered practices such as transcendental meditation, and body-centered practices such as progressive muscle relaxation (PMR), autogenic training (AT), and yoga. For example, many standardized mind-body techniques such as mindfulness-based stress reduction and mindfulness-based cognitive therapy (a) are associated with a reduction in symptoms of symptoms such as anxiety, pain and depression. This article explores the efficacy of mindfulness based techniques to that of other self-regulation techniques and identifies components shared between mindfulness based techniques and several previous self-regulation techniques, including PMR, AT, and transcendental meditation. The authors conclude that most of the commonly used self-regulation strategies have comparable efficacy and share many elements.
Mindfulness-based strategies are based in ancient Buddhist practices and have found acceptance as one of the major contemporary behavioral medicine techniques (Hilton et al, 2016; Khazan, 2013). Throughout this blog the term mindfulness will refer broadly to a mental state of paying total attention to the present moment, with a non-judgmental awareness of the inner and/ or outer experiences (Baer et al., 2004; Kabat-Zinn, 1994).
In 1979, Jon Kabat-Zinn introduced a manual for a standardized Mindfulness-Based Stress Reduction (MBSR) program at the University of Massachusetts Medical Center (Kabat-Zinn, 1994, 2003). The eight-week program combined mindfulness as a form of insight meditation with specific types of yoga breathing and movements exercises designed to focus on awareness of the mind and body, as well as thoughts, feelings, and behaviors.
There is a substantial body of evidence that mindfulness-based cognitive therapy (MBCT); Teasdale et al., 1995) and mindfulness-based stress reduction (MBSR) (Kabat-Zinn, 1994, 2003) have combined with skills of cognitive therapy for ameliorating stress symptoms such as negative thinking, anxiety and depression. For example, MBSR and MBCT has been confirmed to be clinical beneficial in alleviating a variety of mental and physical conditions, for people dealing with anxiety, depression, cancer-related pain and anxiety, pain disorder, or high blood pressure (The following are only a few of the hundred studies published: Andersen et al., 2013; Carlson et al., 2003; Fjorback et al., 2011; Greeson, & Eisenlohr-Moul, 2014; Hoffman et al., 2012; Marchand, 2012; Baer, 2015; Demarzo et al., 2015; Khoury et al, 2013; Khoury et al, 2015; Chapin et al., 2014; Witek Janusek et al., 2019). Currently, MBSR and MBCT techniques that are more standardized are widely applied in schools, hospitals, companies, prisons, and other environments.
The Relationship Between Mindfulness and Other Self-Regulation Techniques
This section addresses two questions: First, how do mindfulness-based interventions compare in efficacy to older self-regulation techniques? Second, and perhaps more basically, how new and different are mindfulness-based therapies from other self-regulation-oriented practices and therapies?
Is mindfulness more effective than other mind/body body/mind approaches?
Although mindfulness-based meditation (MM) techniques are effective, it does not mean that is is more effective than other traditional meditation or self-regulation approaches. To be able to conclude that MM is superior, it needs to be compared to equivalent well-coached control groups where the participants were taught other approaches such as progressive relaxation, autogenic training, transcendental meditation, or biofeedback training. In these control groups, the participants would be taught by practitioners who were self-experienced and had mastered the skills and not merely received training from a short audio or video clip (Cherkin et al, 2016). The most recent assessment by the National Centere for Complementary and Integrative Health, National Institutes of Health (NCCIH-NIH, 2024) concluded that generally “the effects of mindfulness meditation approaches were no different than those of evidence-based treatments such as cognitive behavioral therapy and exercise especially when they include how to generalize the skills during the day” (NCCIH, 2024). Generalizing the learned skills into daily life contributes to the successful outcome of Autogenic Training, Progressive Relaxation, integrated biofeedback stress management training, or the Quieting Response (Luthe, 1979; Davis et al., 2019; Wilson et al., 2023; Stroebel, 1982).
Unfortunately, there are few studies that compare the effective of mindfulness meditation to other sitting mental techniques such as Autogenic Training, Transcendental Meditation or similar meditative practices that are used therapeutically. When the few randomized control studies of MBSR versus autogenic training (AT) was done, no conclusions could be drawn as to the superior stress reduction technique among German medical students (Kuhlmann et al., 2016).
Interestingly, Tanner, et al (2009) in a waitlist study of students in Washington, D.C. area universities practicing TM used the concept of mindfulness, as measured by the Kentucky Inventory of Mindfulness Skills (KIM) (Baer et al, 2004) as a dependent variable, where TM practice resulted in greater degrees of ‘mindfulness.’ More direct comparisons of MM with body-focused techniques, such as progressive relaxation, or Autogenic training mindfulness-based approaches, have not found superior benefit. For example, Agee et al (2009) compared the stress management effects of a five-week Mindfulness Meditation (MM) to a five-week Progressive Muscle Relaxation (PMR) course and found no meaningful reports of superiority of one over the other program; both MM and PMR were effective in reducing symptoms of stress.
In a persuasive meta-analysis comparing MBSR with other similar stress management techniques used among military service members, Crawford, et al (2013) described various multimodal programs for addressing post-traumatic stress disorder (PTSD) and other military or combat-related stress reactions. Of note, Crawford, et al (2013) suggest that all of the multi-modal approaches that include Autogenic Training, Progressive Muscle Relaxation, movement practices including Yoga and Tai Chi, as well as Mindfulness Meditation, and various types of imagery, visualization and prayer-based contemplative practices ALL provide some benefit to service members experiencing PTSD.
An important observation by Crawford et al (2013) pointed out that when military service members had more physical symptoms of stress, the meditative techniques appeared to work best, and when the chief complaints were about cognitive ruminations, the body techniques such as Yoga or Tai Chi worked best to reduce symptoms. Whereas it may not be possible to say that mindfulness meditation practices are clearly superior to other mind-body techniques, it may be possible to raise questions about mechanisms that unite the mind-body approaches used in therapeutic settings.
Could there be negative side effects?
Another point to consider is the limited discussion of the possible absence of benefit or even harms that may be associated with mind-body therapies. For example, for some people, meditation does not promote prosocial behavior (Kreplin et al, 2018). For other people, meditation can evoke negative physical and/or psychological outcomes (Lindahl et al, 2017; Britton et al., 2021). There are other struggles with mind-body techniques when people only find benefit in the presence of a skilled clinician, practitioner, or guru, suggesting a type of psychological dependency or transference, rather than the ability to generalize the benefits outside of a set of conditions (e.g. four to eight weeks of one to four hour trainings) or a particular setting (e.g. in a natural and/or quiet space).
Whereas the detailed instructions for many mindfulness meditation trainings, along with many other types of mind-body practices (e.g. Transcendental Meditation, Autogenic Training, Progressive Muscle Relaxation, Yoga, Tai Chi…) create conditions that are laudable because they are standardized, a question is raised as to ‘critical ingredients’, using the metaphor of baking. The difference between a chocolate and a vanilla cake is not ingredients such as flour, or sugar, etc., which are common to all cakes, but rather the essential or critical ingredient of the chocolate or vanilla flavoring. So what are the essential or critical ingredients in mind-body techniques? Extending the metaphor, Crawford, et al (2013, p. 20) might say the critical ingredient common to the mind-body techniques they studied was that people “can change the way their body and mind react to stress by changing their thoughts, emotions, and behaviors…” with techniques that, relatively speaking, “involve minimal cost and training time.”
The skeptical view suggested here is that MM techniques share similar strategies with other mind-body approaches that encouraging learners to ‘pay attention and shift intention.’ This strategy is part of the instructions when learning Progressive Relaxation, Autogenic Training, Transcendental Meditation, movement meditation of Yoga and Tai Chi and, with instrumented self-regulation techniques such as bio/neurofeedback. In this sense, MM training repackages techniques that have been available for millennia and thus becomes ‘old wine sold in new bottles.’
We wonder if a control group for compassionate mindfulness training would report more benefits if they were asked not only to meditate on compassionate acts, but actually performed compassionate tasks such as taking care of person in pain, helping a homeless person, or actually writing and delivering a letter of gratitude to a person who has helped them in the past? The suggestion is to titrate the effects of MM techniques, moving from a more basic level of benefit to a more fully actualized level of benefit, generalizing their skill beyond a training setting, as measured by the Baer et al (2004) Kentucky Inventory of Mindfulness Skills.
Each generation of clinicians and educators rediscover principles without always recognizing that the similar principles were part of the previous clinical interventions. The analogies and language has changed; however, the underlying concepts may be the same. Mindfulness interventions are now the new, current and popular approach. Some of the underlying ‘mindfulness’ concepts that are shared in common with successfully other mind-body and self-regulation approaches include:
The practitioner must be self-experienced in mindfulness practice. This means that the practitioners do not merely believe the practice is effective; they know it is effective from self-experience. Inner confidence conveyed to clients and patients enhances the healing/placebo effect. It is similar to having sympathy or empathy for clients and patients that occurs from have similar life experiences, such as when a clinician speaks to a patient. For example, a male physician speaking to a female patient who has had a mastectomy may be compassionate; however, empathy occurs more easily when another mastectomy patient (who may also be a physician) shares how she struggled overcame her doubts and can still be loved by her partner.
There may also be a continuum of strengthening beliefs about the benefits of mindfulness techniques that leads to increase benefits for the approach. Knowing there are some kinds of benefits from initiating a practice of mindfulness increases empathy/compassion for others as they learn. Proving that mindfulness techniques are causing benefits after systematically comparing their effectiveness with other approaches strengthens the belief in the mindfulness approaches. Note that a similar process of strengthening one’s belief in an approach occurs gradually, over time as clients and patients progress through beginner, intermediate and advanced levels of mind-body practices.
Observing thoughts without being captured. Being a witness to the thoughts, emotions, and external events results in a type of covert global desensitization and skill mastery of NOT being captured by those thoughts and emotions. This same process of non-attachment and being a witness is one of the underpinnings of techniques that tacitly and sometime covertly support learning ways of controlling attention, such as with Autogenic Training; namely how to passively attend to a specific body part without judgment and, report on the subjective experience without comparison or judgment.
Ongoing daily practice. Participants take an active role in their own healing process as they learn to control and focus their attention. Participants are often asked to practice up to one hour a day and apply the practices during the day as mini-practices or awareness cues to interrupt the dysfunctional behavior. For example in Autogenic training, trainees are taught to practice partial formula (such my “neck and shoulders are heavy”) during the day to bring the body/mind back to balance. While with Progressive Relaxation, the trainee learns to identify when they tighten inappropriate muscles (dysponesis) and then inhibit this observed tension.
Peer support by being in a group. Peer support is a major factor for success as people can share their challenges and successes. Peer support tends to promote acceptance of self-and others and provides role modeling how to cope with stressors. It is possible that some peer support groups may counter the benefits of a mind-body technique, especially when the peers do not provide support or may in fact impede progress when they complain of the obstacles or difficulties in their process.
These concepts are not unique to Mindfulness Meditation (MM) training. Similar instructions have been part of the successful/educational intervention of Progressive Relaxation, Autogenic Training, Yogic practices, and Transcendental Meditation. These approaches have been most successful when the originators, and their initial students, taught their new and evolving techniques to clients and patients; however, they became less successful as later followers and practitioners used these approaches without learning an in-depth skill mastery. For example, Progressive relaxation as taught by Edmund Jacobson consisted of advanced skill mastery by developing subtle awareness of different muscle tension that was taught over 100 sessions (Mackereth & Tomlinson, 2010). It was not simply listening once to a 20-minute audio recording about tightening and relaxing muscles. Similarly, Autogenic training is very specific and teaches passive attention over a three to six-month time-period while the participant practices multiple times daily. Stating the obvious, learning Autogenic Training, Mindfulness, Progressive Relaxation, Bio/Neurofeedback or any other mind-body technique is much more than listening to a 20-minute audio recording.
The same instructions are also part of many movement practices. For many participants focusing on the movement automatically evoked a shift in attention. Their attention is with the task and they are instructed to be present in the movement.
Areas to explore.
Although Mindfulness training with clients and patients has resulted in remarkable beneficial outcomes for the participants, it is not clear whether mindfulness training is better than well taught PR, AT, TM or other mind/body or body/mind approaches. There are also numerous question to explore such as: 1) Who drops out, 2) Is physical exercise to counter sitting disease and complete the alarm reaction more beneficial, and 3) Strategies to cope with wandering attention.
- Who drops out?
We wonder if mindfulness is appropriate for all participants as sometimes participants drop out or experience negative abreactions. It not clear who those participants are. Interestingly, hints for whom the techniques may be challenging can be found in the observations of Autogenic Training that lists specific guidelines for contra-, relative- and non-indications (Luthe, 1970).
- Physical movement to counter sitting disease and complete the alarm reaction.
Although many mindfulness meditation practices may include yoga practices, most participants practice it in a sitting position. It may be possible that for some people somatic movement practices such as a slow Zen walk may quiet the inner dialogue more quickly. In our experience, when participants are upset and highly stressed, it is much easier to let go of agitation by first completing the triggered fight/flight response with vigorous physical activity such as rapidly walking up and downs stairs while focusing on the burning sensations of the thigh muscles. Once the physical stress reaction has been completed and the person feels physically calmer then the mind is quieter. Then have the person begin their meditative practice.
- Strategies to cope with wandering attention.
Some participants have difficulty staying on task, become sleepy, worry, and/or are preoccupied. We observed that first beginning with physical movement practices or Progressive Relaxation appears to be a helpful strategy to reduce wandering thoughts. If one has many active thoughts, progressive relaxation continuously pulls your attention to your body as you are directed to tighten and let go of muscle groups. Being guided supports developing the passive focus of attention to bring awareness back to the task at hand. Once internally quieter, it is easier hold their attention while doing Autogenic Training, breathing or Mindfullness Meditation.
By integrating somatic components with the mindfulness such as done in Progressive Relaxation or yoga practices facilitates the person staying present. Similarly, when teaching slower breathing, if a person has a weight on their abdomen while practicing breathing, it is easier to keep attending to the task: allow the weight to upward when inhaling and feeling the exhalation flowing out through the arms and legs.
Therapeutic and education strategies that implicitly incorporate mindfulness
Progressive relaxation
In the United States during the 1920 progressive relaxation (PR) was developed and taught by Edmund Jacobson (1938). This approach was clinically very successful for numerous illnesses ranging from hypertension, back pain, gastrointestinal discomfort, and anxiety; it included 50 year follow-ups. Patients were active participants and practiced the skills at home and at work and interrupt their dysfunctional patterns during the day such as becoming aware of unnecessary muscle tension (dyponetic activity) and then release the unnecessary muscle tension (Whatmore & Kohli, 1968). This structured approach is totally different than providing an audio recording that guides clients and patients through a series of tightening and relaxing of their muscles. The clinical outcome of PR when taught using the original specific procedures described by Jacobson (1938) was remarkable. The incorporation of Progressive Relaxation as the homework practice was an important cofactor in the successful outcome in the treatment of muscle tension headache using electromyography (EMG) biofeedback by Budzynski, Stoyva and Adler (1970).
Autogenic Training
In 1932 Johannes Schultz in Germany published a book about Autogenic Training describing the basic training procedure. The basic autogenic procedure, the standard exercises, were taught over a minimum period of three month in which the person practiced daily. In this practice they directed theri passive attention to the following cascading sequence: heaviness of their arms, warmth of their arms, heart beat calm and regular, breathing calm and regular or it breathes me, solar plexus is warm, forehead is cool, and I am at peace (Luthe, 1979). Three main principles of autonomic training mentioned by Luthe (1979) are: (1) mental repetition of topographically oriented verbal formulae for brief periods; (2) passive concentration; and (3) reduction of exteroceptive and proprioceptive afferent stimulation. The underlying concepts of Autogenic Therapy include as described by Peper and Williams (1980):
The body has an innate capacity for self-healing and it is this capacity that is allowed to become operative in the autogenic state. Neither the trainer nor trainee has the wisdom necessary to direct the course of the self-balancing process; hence, the capacity is allowed to occur and not be directed.
- Homeostatic self-regulation is encouraged.
- Much of the learning is done by the trainee at home; hence, the responsibility for the training lies primarily with the trainee.
- The trainer/teacher must be self-experience in the practice.
- The attitude necessary for successful practice is one of passive attention; active striving and concern with results impedes the learning process. An attitude of acceptance is cultivated, letting be whatever comes up. This quality of attention is known as “mindfulness’ in meditative traditions.
The clinical outcome for autogenic therapy is very promising. The detailed guided self-awareness training and uncontrolled studies showed benefits across a wide variety of psychosomatic illness such as asthma, cancer, hypertension, anxiety, pain irritable bowel disease, depression (Luthe & Schultz, 1970a; Luthe & Schultz, 1970b). Autogenic training components have also been integrated in biofeedback training. Elmer and Alice Green included the incorporation of autogenic training phrases with temperature biofeedback for the very successful treatment of migraines (Green & Green, 1989). Autonomic training combine with biofeedback in clinical practices produced better results than control group for headache population (Luthe, 1979). Empirical research found that autonomic training was applied efficiently in emotional and behavioral problems, and physical disorder (Klott, 2013), such as skin disorder (Klein & Peper, 2013), insomnia (Bowden et al., 2012), Meniere’s disease (Goto, Nakai, & Ogawa, 2011) and the multitude of stress related symptoms (Wilson et al., 2023).
Bio/neurofeedback training
Starting in the late 1960s, biofeedback procedures have been developed as a successful treatment approach for numerous illnesses ranging from headaches, hypertension, to ADHD (Peper et al., 1979; Peper & Shaffer, 2010; Khazan, 2013). In most cases, the similar instructions that are part of mindfulness meditation are also embedded in the bio/neurofeedback instructions. The participants are instructed to learn control over some physiological parameter and then practice the same skill during daily life. This means that during the learning process, the person learn passive attention and is not be captured by marauding thoughts and feeling. and during the day develop awareness Whenever they become aware of dysfunctional patterns, thoughts, emotions, they initiated their newly learned skill. The ongoing biological feedback signals continuously reminds them to focus.
Transcendental meditation
The next fad to hit the American shore was Transcendental Meditation (TM)– a meditation practice from the ancient Vedic tradition in India. The participant were given a mantra that they mentally repeated and if their attention wanders, they go back to repeating the mantra internally. The first study that captured the media’s attention was by Wallace (1970) published in the Journal Science which reported that “During meditation, oxygen consumption and heart rate decreased, skin resistance increased, and the electroencephalogram showed specific changes in certain frequencies. These results seem to distinguish the state produced by Transcendental Meditation from commonly encountered states of consciousness and suggest that it may have practical applications.” (Wallace, 1970).
The participants were to practice the mantra meditation twice a day for about 20 minutes. Meta-analysis studies have reported that those who practiced TM as compared to the control group experienced significant improved of numerous disorders such as CVD risk factors, anxiety, metabolic syndrome, drug abuse and hypertension (Paul-Labrador et al, 2006; Rainforth et al., 2007; Hawkins, 2003).
To make it more acceptable for the western audience, Herbert Benson, MD, adapted and simplified techniques from TM training and then labelled a core element, the ‘relaxation response’ (Benson et al., 1974) Instead of giving people a secret mantra and part of a spiritual tradition, he recommend using the word “one” as the mantra. Numerous studies have demonstrated that when patients practice the relaxation response, many clinical symptoms were reduced. The empirical research found that practiced transcendental meditation caused increasing prefrontal low alpha power (8-10Hz) and theta power of EEG; as well as higher prefrontal alpha coherence than other locations at both hemispheres. Moreover, some individuals also showed lower sympathetic activation and higher parasympathetic activation, increased respiratory sinus arrhythmic and frontal blood flow, and decreased breathing rate (Travis, 2001, 2014). Although TM and Benson’s relaxation response continues to be practiced, mindfulness has taking it place.
Conclusion
Mindfulness-Based Stress Reduction (MBSR) and Mindfulness-Based Cognitive Therapy (MBCT) are very beneficial and yet may be considered ‘old wine in new bottles’ where the metaphor refers to millennia old meditation techniques as ‘old wine’ and the acronyms such as MBSR or MBCT as ‘new bottles’. Like many other ‘new’ therapeutic approaches or for that matter, many other ‘new’ medications, use it now before it becomes stale and loses part of its placebo power. As long as the application of a new technique is taught with the intensity and dedication of the promotors of the approach, and as long as the participants are required to practice while receiving support, the outcomes will be very beneficial, and most likely similar in effect to other mind-body approaches.
The challenge facing mindfulness practices just as those from Autogenic Training, Progressive Relaxation and Transcendental Meditation, is that familiarity breeds contempt and that clients and therapists are continuously looking for a new technique that promises better outcome. Thus as Mindfulness training is taught to more and more people, it may become less promising. In addition, as mindfulness training is taught in less time, (e.g. fewer minutes and/or fewer sessions), and with less well-trained instructors, who may offer less support and supervision for people experiencing possible negative effects, the overall benefits may decrease. Thus, mindfulness practice, Autogenic training, progressive relaxation, Transcendental Meditation, movement practices, meditation, breathing practices as well as the many spiritual practices all appear to share common fate of fading over time. Whereas the core principles of mind-body techniques are ageless, the execution is not always assured.
References
Agee, J. D., Danoff-Burg, S., & Grant, C. A. (2009). Comparing brief stress management courses in a community sample: Mindfulness skills and progressive muscle relaxation. Explore: The Journal of Science and Healing, 5(2), 104-109. https://doi.org/10.1016/j.explore.2008.12.004
Andersen, S. R., Würtzen, H., Steding-Jessen, M., Christensen, J., Andersen, K. K., Flyger, H., … & Dalton, S. O. (2013). Effect of mindfulness-based stress reduction on sleep quality: Results of a randomized trial among Danish breast cancer patients. Acta Oncologica, 52(2), 336-344. https://doi.org/10.3109/0284186X.2012.745948
Alvarez-Jimenez, M., Gleeson, J. F., Bendall, S., Penn, D. L., Yung, A. R., Ryan, R. M., … Nelson, B. (2018). Enhancing social functioning in young people at Ultra High Risk (UHR) for psychosis: A pilot study of a novel strengths and mindfulness-based online social therapy. Schizophrenia Research, 202, 369-377 https://doi.org/10.1016/j.schres.2018.07.022
Baer, R. A. (2003). Mindfulness training as a clinical intervention: A conceptual and empirical review. Clinical Psychology: Science and Practice, 10, 125–143. https://doi.org/10.1093/clipsy/bpg015
Baer, R. A.. (2015). Mindfulness-based treatment approaches: Clinician’s guide to evidence base and applications. New York: Elsevier. https://www.elsevier.com/books/mindfulness-based-treatment-approaches/baer/978-0-12-416031-6
Baer, R., Smith, G., & Allen, K. (2004). Assessment of mindfulness by self-report: The Kentucky Inventory of Mindfulness Skills. Assessment, 11, 191–206. https://doi.org/10.1177/1073191104268029
Benson, H., Beary, J. F., & Carol, M. P. (1974).The Relaxation Response. Psychiatry, 37(1), 37-46. https://www.tandfonline.com/loi/upsy20
Bowden, A., Lorenc, A., & Robinson, N. (2012). Autogenic Training as a behavioural approach to insomnia: A prospective cohort study. Primary Health Care Research & Development, 13, 175-185. https://doi.org/10.1017/S1463423611000181
Britton, W.B., Lindahl, J.R., Coope, D.J., Canby, N.K., & Palitsky, R. (2021). Defining and Measuring Meditation-Related Adverse Effects in Mindfulness-Based Programs. Clinical Psychological Science, 9(6), 1185-1204. https://doi.org/10.1177/2167702621996340
Budzynski, T., Stoyva, J., & Adler, C. (1970). Feedback-induced muscle relaxation: Application to tension headache. Journal of Behavior Therapy and Experimental Psychiatry, 1(3), 205-211. https://doi.org/10.1016/0005-7916(70)90004-2
Carlson, L. E., Speca, M., Patel, K. D., & Goodey, E. (2003). Mindfulness‐based stress reduction in relation to quality of life, mood, symptoms of stress, and immune parameters in breast and prostate cancer outpatients. Psychosomatic Medicine, 65(4), 571-581. https://doi.org/10.1097/01.psy.0000074003.35911.41
Chapin, H. L., Darnall, B. D., Seppala, E. M., Doty, J. R., Hah, J. M., & Mackey, S. C. (2014). Pilot study of a compassion meditation intervention in chronic pain. J Compassionate Health Care, 1(4), 1-12. https://doi.org/10.1186/s40639-014-0004-x
Cherkin, D. C., Sherman, K. J., Balderson, B. H., Cook, A. J., Anderson, M. L., Hawkes, R. J., … & Turner, J. A. (2016). Effect of mindfulness-based stress reduction vs cognitive behavioral therapy or usual care on back pain and functional limitations in adults with chronic low back pain: A randomized clinical trial. JAMA, 315(12), 1240-1249. https://doi.org/10.1001/jama.2016.2323
Crawford, C., Wallerstedt, D. B., Khorsan, R., Clausen, S. S., Jonas, W. B., & Walter, J. A. (2013). A systematic review of biopsychosocial training programs for the self-management of emotional stress: Potential applications for the military. Evidence-Based Complementary and Alternative Medicine, 747694: 1-23. https://doi.org/10.1155/2013/747694
Davis, M., Eshelman, E.R., & McKay, M. (2019). The Relaxation and Stress Reduction Workbook. Oakland, CA: New Harbinger Publications. https://www.amazon.com/Relaxation-Reduction-Workbook-Harbinger-Self-Help/dp/1684033349
Demarzo, M. M., Montero-Marin, J., Cuijpers, P., Zabaleta-del-Olmo, E., Mahtani, K. R., Vellinga, A., Vincens, C., Lopez del Hoyo, Y., & García-Campayo, J. (2015). The efficacy of mindfulness-based interventions in primary care: A meta-analytic review. The Annals of Family Medicine, 13(6), 573-582. https://doi.org/10.1370/afm.1863
Fjorback, L. O., Arendt, M., Ørnbøl, E., Fink, P., & Walach, H. (2011). Mindfulness‐Based Stress Reduction and Mindfulness‐Based Cognitive Therapy–A systematic review of randomized controlled trials. Acta Psychiatrica Scandinavica, 124(2), 102-119. https://doi.org/10.1111/j.1600-0447.2011.01704.x
Goto, F., Nakai, K., & Ogawa, K. (2011). Application of autogenic training in patients with Meniere disease. European Archives of Oto-Rhino-Laryngology, 268(10), 1431-1435. https://doi.org/10.1007/s00405-011-1530-1
Greeson, J., & Eisenlohr-Moul, T. (2014). Mindfulness-based stress reduction for chronic pain. In R. A. Baer (Ed.), Mindfulness-Based Treatment Approaches: Clinician’s Guide to Evidence Base and Applications, 269-292. San Diego, CA: Academic Press. https://psycnet.apa.org/record/2014-40932-000
Green, E. and Green, A. (1989). Beyond Biofeedback. New York: Knoll. https://www.amazon.com/Beyond-Biofeedback-Elmer-Green/dp/0940267144
Hawkins, M. A. (2003). Effectiveness of the Transcendental Meditation program in criminal rehabilitation and substance abuse recovery. Journal of Offender Rehabilitation, 36(1-4), 47- 65. https://doi.org/10.1300/J076v36n01_03
Hilton, L., Hempel, S., Ewing, B. A., Apaydin, E., Xenakis, L., Newberry, S., …Maglione, M. A. (2016). Mindfulness meditation for chronic pain: Systematic review and meta-analysis. Annals of Behavioral Medicine, 51(2), 199-213. https://doi.org/10.1007/s12160-016-9844-2
Hoffman, C. J., Ersser, S. J., Hopkinson, J. B., Nicholls, P. G., Harrington, J. E., & Thomas, P. W. (2012). Effectiveness of mindfulness-based stress reduction in mood, breast-and endocrine-related quality of life, and well-being in stage 0 to III breast cancer: A randomized, controlled trial. Journal of Clinical Oncology, 30(12), 1335-1342. https://doi.org/10.1200/JCO.2010.34.0331
Jacobson, E. (1938). Progressive relaxation. Chicago, IL: University of Chicago Press. https://www.amazon.com/Progressive-Relaxation-Physiological-Investigation-Significance/dp/0226390594
Kabat-Zinn, J. (1994). Wherever you go, there you are: Mindfulness meditation in everyday life. New York: Hyperion. https://www.amazon.com/Wherever-You-There-Are-Mindfulness/dp/0306832011
Kabat-Zinn, J. (2003). Mindfulness-based stress reduction (MBSR). Constructivism in the Human Sciences, 8, 73–107. https://psycnet.apa.org/record/2004-19791-008
Khazan, I. Z. (2013). The clinical handbook of biofeedback: A step-by-step guide for training and practice with mindfulness. New York: John Wiley & Sons. https://www.amazon.com/Clinical-Handbook-Biofeedback-Step-Step/dp/1119993717
Klein, A., & Peper, E. (2013). There Is hope: Autogenic biofeedback training for the treatment of psoriasis. Biofeedback, 41 (4), 194-201. https://doi.org/10.5298/1081-5937-41.4.01
Khoury, B., Lecomte, T., Fortin, G., Masse, M., Therien, P., Bouchard, V., Chapleau, M., Paquin, K., & Hofmann, S. G. (2013). Mindfulness-based therapy: A comprehensive meta-analysis. Clinical Psychology Review, 33(6), 763-771. https://doi.org/10.1016/j.cpr.2013.05.005
Khoury, B., Sharma, M., Rush, S. E., & Fournier, C. (2015). Mindfulness-based stress reduction for healthy individuals: A meta-analysis. Journal of Psychosomatic Research, 78(6), 519-528.
Klott, O. (2013). Autogenic Training–a self-help technique for children with emotional and behavioural problems. Therapeutic Communities: The International Journal of Therapeutic Communities, 34(4), 152-158. https://doi.org/10.1108/TC-09-2013-0027
Kreplin, U., Farias, M., & Brazil, I. A. (2018). The limited prosocial effects of meditation: A systematic review and meta-analysis. Sci Rep, 8, 2403. https://doi.org/10.1038/s41598-018-20299-z
Kuhlmann, S. M., Huss, M., Bürger, A., & Hammerle, F. (2016). Coping with stress in medical students: results of a randomized controlled trial using a mindfulness-based stress prevention training (MediMind) in Germany. BMC Medical Education, 16(1), 316. https://doi.org/10.1186/s12909-016-0833-8
Lindahl, J. R., Fisher, N. E., Cooper, D. J., Rosen, R. K, & Britton, W. B. (2017). The varieties of contemplative experience: A mixed-methods study of meditation-related challenges in Western Buddhists. PLoSONE, 12(5): e0176239. https://doi.org/10.1371/journal.pone.0176239
Luthe, W. (1970). Autogenic therapy: Research and theory. New York: Grune and Stratton. https://www.cambridge.org/core/journals/the-british-journal-of-psychiatry/article/abs/autogenic-therapy-edited-by-wolfgang-luthe-volume-4-research-and-theory-by-wolfgang-luthe-grune-and-stratton-new-york-1970-pp-276-price-1475/6C8521C36C37254A08AAD1F2FE08211C
Luthe, W. (1979). About the Methods of Autogenic Therapy. In: Peper, E., Ancoli, S., Quinn, M. (eds). Mind/Body Integration. Springer, Boston, MA. https://doi.org/10.1007/978-1-4613-2898-8_12
Luthe, W. & Schultz, J. H. (1970a). Autogenic therapy: Medical applications. New York: Grune and Stratton. https://www.amazon.com/Autogenic-Therapy-II-Medical-Applications/dp/B001J9W7L6
Luthe, W. & Schultz, J. H. (1970b). Autogenic therapy: Applications in psychotherapy. New York: Grune and Stratton. https://www.amazon.com/Autogenic-Therapy-Applications-Psychotherapy-v/dp/0808902725
Mackereth, P.A. & Tomlinson, L. (2010). Progressive muscle relaxation. In Cawthorn, A. & Mackereth, P.A. eds. Integrative Hypnotherapy. London: Churchill Livingstone. https://www.amazon.com/Integrative-Hypnotherapy-Complementary-approaches-clinical/dp/0702030821
Marchand, W. R. (2012). Mindfulness-based stress reduction, mindfulness-based cognitive therapy, and Zen meditation for depression, anxiety, pain, and psychological distress. Journal of Psychiatric Practice, 18(4), 233-252. https://doi.org/10.1097/01.pra.0000416014.53215.86
NCCIH (2024). Meditation and Mindfulness: What You Need To Know. National Center for Complementary and Integrative Health, National Institutes of Health. Accessed January 31, 2024. https://www.nccih.nih.gov/health/meditation-and-mindfulness-what-you-need-to-know?
Paul-Labrador, M., Polk, D., Dwyer, J.H. et al. (2006). Effects of a randomized controlled trial of Transcendental Meditation on components of the metabolic syndrome in subjects with coronary heart disease. Archive of Internal Medicine, 166(11), 1218-1224. https://doi.org/10.1001/archinte.166.11.1218
Peper, E., Ancoli, S. & Quinn, M. (Eds). (1979). Mind/Body Integration: Essential Readings in Biofeedback. New York: Plenum. https://www.amazon.com/Mind-Body-Integration-Essential-Biofeedback/dp/0306401029
Peper, E. & Shaffer, F. (2010). Biofeedback History: An Alternative View. Biofeedback, 38 (4): 142–147. https://doi.org/10.5298/1081-5937-38.4.03
Peper, E., & Williams, E.A. (1980). Autogenic therapy. In A. C. Hastings, J. Fadiman, & J. S. Gordon (Eds.), Health for the whole person (pp137-141).. Boulder: Westview Press. https://biofeedbackhealth.files.wordpress.com/2016/02/autogenic-therapy-peper-and-williams.pdf
Rainforth, M.V., Schneider, R.H., Nidich, S.I., Gaylord-King, C., Salerno, J.W., & Anderson, J.W. (2007). Stress reduction programs in patients with elevated blood pressure: A systematic review and meta-analysis. Current Hypertension Reports, 9(6), 520–528. https://doi.org/10.1007/s11906-007-0094-3
Stroebel, C. (1982). QR: The Quieting Reflex. New York: Putnam Pub Group. https://www.amazon.com/Qr-Quieting-Charles-M-D-Stroebel/dp/0399126570
Tanner, M. A., Travis, F., Gaylord‐King, C., Haaga, D. A. F., Grosswald, S., & Schneider, R. H. (2009). The effects of the transcendental meditation program on mindfulness. Journal of Clinical Psychology 65(6), 574-589. https://doi.org/10.1002/jclp.20544
Teasdale, J. D., Segal, Z., & Williams, J. M. (1995). How does cognitive therapy prevent depressive relapse and why should attentional control (mindfulness) training help? Behaviour Research and Therapy, 33, 25–39. https://doi.org/10.1016/0005-7967(94)e0011-7
Travis, F. (2001). Autonomic and EEG patterns distinguish transcending from other experiences during transcendental meditation practice. International Journal of Psychophysiology, 42, 1–9. https://doi.org/10.1016/s0167-8760(01)00143-x
Travis, F. (2014). Transcendental experiences during meditation practice. Annals of the New York Academy of Sciences, 1307, 1–8. https://doi.og10.1111/nyas.12316
Wallace, K.W. (1970). Physiological Effects of Transcendental Meditation. Science, 167 (3926), 1751-1754. https://doi.org/10.1126/science.167.3926.1751
Whatmore, G. B., & Kohli, D. R. (1968). Dysponesis: A neurophysiologic factor in functional disorders. Behavioral Science, 13(2), 102–124. https://doi.org/10.1002/bs.3830130203
Wilson, V., Somers, K. & Peper, E. (2023). Differentiating Successful from Less Successful Males and Females in a Group Relaxation/Biofeedback Stress Management Program. Biofeedback, 51(3), 53–67. https://doi.org/10.5298/608570
Witek Janusek, L., Tel,l D., & Mathews, H.L. (2019). Mindfulness based stress reduction provides psychological benefit and restores immune function of women newly diagnosed with breast cancer: A randomized trial with active control. Brain Behav Immun, 80:358-373. https://doi.org/10.1016/j.bbi.2019.04.012
