Rethink the monies spent on cancer screening tests
Posted: November 24, 2023 Filed under: behavior, cancer, Evolutionary perspective, healing, health, Nutrition/diet, self-healing | Tags: breast canceer, Cancer screening, environmental toxins, immune competence, Life style, lifestyle modification, mammography, organic foods, overdiagnosis 3 CommentsErik Peper, PhD and Richard Harvey, PhD

Adapted from: Peper, E. & Harvey, R. (2024). Rethinking the monies spent on cancer screening tests. Townsend e-Letter, Townsend Letters. The Examiner of Alternative Medicine, May 18, 2024. https://www.townsendletter.com/e-letter-34-are-we-reducing-cancer-or-just-looking-for-it/
Abstract
While cancer screening tests are commonly promoted for early detection and treatment, evidence increasingly suggests that widespread screening of asymptomatic individuals may not significantly extend lifespan and could contribute to overdiagnosis, overtreatment, and harm. Although billions are spent annually on screenings—$40 billion for colon, $15 billion for breast, and $4 billion for prostate cancer—some of these money might be more effectively invested in lifestyle interventions that reduce cancer risk and improve longevity. Meta-analyses indicate that only sigmoidoscopy for colorectal cancer shows a clear benefit in extending life, while other common screenings (e.g., mammography, PSA, FOBT) show minimal or no effect on overall mortality. Interestingly, breast cancer mortality declines have occurred in similarly European countries that delayed screening implementation as compared to countries that started screen earlier. This suggests that other contributing factors such as improved lifestyle, nutrition, and environmental changes may be the major factor in the reduction of breast cancer. We recommend shifting from profit-driven, generalized screening toward personalized, risk-adjusted methods using multi-omics technology and preventative lifestyle patterns. More critically, the focus should be prevention through diet, physical activity, stress management, sleep hygiene, environmental protections, and social support; since, it is estimated that 70 percent of all cancers are related to diet and environmental factors. Thus, resources need to be allocated toward empowering individuals and communities to adopt health-promoting behaviors and thereby reduce cancer incidence.
Keywords: cancer screening, overdiagnosis, lifestyle modification, preventive health,
immune competence
Cancer screening tests are based upon the rational that early detection of fatal cancers enables earlier and more effective treatments (Kowalski, 2021), however, there is some controversy. Early screening may increase the risk of over diagnosis, treating false positives (people who did not have the cancer but the test indicates they have cancer) and potentially fatal treatment of cancers that would never progress to increase morbidity or mortality (Kowalski, 2021).
Today about $40 billion spent on colon cancer screening, $15 billion spent on breast cancer screening, and $4 billion spent on prostate cancer screening annually (CSPH, 2021). A question is raised whether the billions and billions of dollars spent on screening asymptomatic participants would be more wisely spent on promoting and supporting life style changes that reduce cancer risks and actually extend life span? That cancer screening is expensive does not mean no one should be screened. Instead, the argument is that the majority of healthcare dollars could be spent on health promotion practices and reserving screening for those people who are at highest risk for developing cancers.
What is the evidence that screening prolongs life?
Cancer screening tests appear correlated with preventing deaths since deaths due to cancers in the USA have decreased by about 28% from 1999 to 2020 (CDC, 2023a). Although cancer causes many of the deaths in the USA, overall life expectancy has increased by less than 1% from 1999 to 2020. If cancer screening were more effective, the life expectancy should have increased more because cancer is the second leading cause of death (CDC, 2023b). Consider also that deaths due to cancers may be coincident and or comorbid with other circumstances. For example, during the last four years, overall life expectancy in the USA has precipitously declined in part due to other causes of death such as the COVID pandemic and opioid overdose epidemic (Lewis, 2022). Decline in life expectancy in the USA has many contributing factors, including the ‘harms’ associated with cancer screening procedures. For example, perforations during colon cancer screening can lead to internal bleeding, or complications related to surgeries, radiotherapies or chemotherapies. Bretthauer et al., (2023) commented: “A cancer screening test may reduce cancer-specific mortality but fail to increase longevity if the harms for some individuals outweigh the benefits for others or if cancer-specific deaths are replaced by deaths from competing cause” (p. 1197).
Bretthauer et al. (2023) conducted a systematic review and meta-analysis of 18 long-term randomized clinical trials involving 2.1 million Individuals with more than nine years of follow-up reporting on all-cause mortality. They reported that“…this meta-analysis suggest that current evidence does not substantiate the claim that common cancer screening tests save lives by extending lifetime, except possibly for colorectal cancer screening with sigmoidoscopy.”
Following is a summary of Bretthauer et al. (2023) findings:
- The only cancer screening with a significant lifetime gain (approximately 3 months) was sigmoidoscopy.
- There was no significant difference between harms of screening and benefits of screening for:
- mammography
- prostate cancer screening
- FOBT (fecal occult blood test) screening every year or every other year
- lung cancer screening Pap test cytology for cervical cancer screening, no randomized clinical trials with cancer-specific or all-cause mortality end points and long term follow-up were identified.
Potential for loss or harm (e.g., iatrogenic and nosocomial) versus potential for benefit and extended life
More than 35 years ago a significant decrease in breast cancer mortality was observed after mammography was implemented. The correlation suggested a causal relationship that screening reduced mortality (Fracheboud, 2004). This correlation made logical sense since the breast cancer screening test identified cancers early which could then be treated and thereby would result in a decrease in mortality.
How much money is spent on screening that may correlate with unintended harms?
The annual total expenditure for cancer screening is estimated to be between $40-$50 billion annually (CSPH, 2021). Below are some of the estimated expenditures for common tests other than colorectal cancer screening, which arguably is costly; however, has potential benefits that outweigh potential harms.
- $10.37-13.94 billion for mammography to screen 50% of eligible women (Badal et al, 2023).
- $2-4 billion for prostate cancer (Ma et al., 2014)
- $1-2 billion for lung cancer (Taylor et al., 2022)
What is the correlation between initiation of mammography and decrease in breast cancer mortality?
The conclusion that mammography reduced breast cancer mortality was based upon studies without control groups; however, this relationship could be causal or synchronistic. The ambiguity of correlation or causation was resolved with the use of natural experimental control groups. Some European countries began screening 10 years earlier than other countries. Using statistical techniques such as propensity score matching when comparing the data from countries that initiated mammography screening early (Netherlands, Sweden and Northern Ireland) to countries that started screening 10 year later (Belgium, Norway and Republic of Ireland), the effectiveness of screening could be compared.
The comparisons showed no difference in the decrease of breast cancer mortality in countries that initiated breast cancer screening early or late. For example, there was no difference in the decrease of breast cancer mortality rates of women who lived in the Netherlands that started screening early versus those who lived in Belgium that began screening 10 years later, as is shown Figure 1 (Autier et al, 2011).

Figure 1. No difference in age adjust breast cancer mortality between the two adjacent countries even though breast cancer screening began ten years earlier in the Netherlands than in Belgium (graph reproduced from Autier et al, 2011).
The observations are similar when comparing neighboring countries: Sweden (early screening) to Norway (late screening) as well as Northern Ireland, UK (early screening) compared to the Republic of Ireland (late screening). The systematic comparisons showed that screening did not account for the decrease in breast cancer mortality. To what extent could the decrease in mortality be related to other factors such as better prenatal and early childhood diet and life style, improved nutrition, reduction in environmental pollutants, and other unidentified life style and environmental factors which improve immune competence?
A simplistic model to reduce the risk of cancers is described in the following equation (Gorter & Peper, 2011).

Cancer risk can be reduced, arguably by influencing risk factors that contribute to cancers as well as increasing factors to enhance immune competence. In the simple model above, ‘Cancer burden’ refers to the set of exposures that increase the odds of cancer formations. Categories include exposures to oncoviruses, environmental exposures (e.g., ionizing radiation, carcinogenic chemicals) as well as genetic (e.g., chromosomal aberrations, replication errors) and epigenetic factors (e.g., lifestyle categories related to eating, exercising, sleeping, and relaxing). In the model above, ‘Immune competence’ refers to a set of categories of immune functioning related to DNA repair, orderly cell death (i.e., processes of apoptosis), expected autophagy, as well as ‘metabolic rewiring,’ also called cellular energetics, that would allow the body to be able to reduce manage cancers from progressing (Fouad & Aanei, 2017) .
How do we examine the cancer burden/immune competence relationship?
Schmutzler et al., (2022) have suggested personalized and precision-medicine risk-adjusted cancer screening incorporating “… high-throughput “multi-omics” technologies comprising, among others, genomics, transcriptomics, and proteomics, which have led to the discovery of new molecular risk factors that seem to interact with each other and with non-genetic risk factors in a multiplicative manner.” The argument is that ‘profit-centered’ medicine could incorporate ‘multi-omics’ into risk-adjusted cancer screening as a way to reduce potential loss or harm due to other cancer screening procedures. Rather than simply screening for cancers using currently invasive or toxic procedures which may do more harm than good, consider more nuanced screening tests aimed at the so-called ‘hallmarks of cancer?’ For example, Hanahan (2022) suggests some technical targets for the multi-omics technologies. The following are some of the precision screening tests possible topersonalized medicine of 14 factors or processes related to:
- cells evading growth suppression
- non-mutational epigenetic reprogramming
- avoiding immune destruction
- enabling replicative immortality
- tumor-promoting inflammation
- polymorphic microbiomes
- activating invasion and metastasis
- inducing or accessing vasculature formation/angiogenesis
- cellular senescence
- genome instability and mutation
- resisting cell death
- deregulating cellular metabolism
- unlocking phenotypic plasticity
- sustaining proliferative signaling
Of the listed categories above, ‘phenotypic plasticity’ (cf. Feinberg, 2007; Gupta et al., 2019) suggests that lifestyle behaviors and environmental exposures play a role in cancer progression and regression.
Lifestyle and environmental factors can contribute to the development of cancers.
The 2008-2009 report from the President’s Cancer Panel appraised the National Cancer Program in accordance with the National Cancer Act of 1971 stated (Reuben, 2010):
“We have grossly underestimated the link between environmental toxins, plastics, chemicals, and cancer risk. It is estimated that 70 percent of all cancers were related to diet and environment “
Multiple research studies have shown that a healthy life style pattern is associated with decreased cancer risks and increased longevity. Lifestyle factors that have been documented to increase cancer risks in the United Kingdom (UK) as shown in figure 2.

Figure 2. Percentages of cancer cases in the UK attributable to different exposures. Adapted from Brown et al., 2018 and reproduced by permission from Key et al., 2020.
Similar findings have been reported by Song et al. (2016) from the long term follow-up of 126901 adult health care professionals. People who never smoked, drank no alcohol or moderate alcohol (< 1 drink/d for women; < 2 drinks/d for men}, had a body-mass index (BMI) of at least 18.5 but lower than 27.5, did weekly aerobic physical activity of at least 75 vigorous-intensity minutes or 150 150 moderate-intensity minutes compared to those who smoked, drank, had high BMI and did not exercise had nearly half the cancer death rate. Song et al (2016) concludes:
“…about 20% to 40% of carcinoma cases and about half of carcinoma deaths can be potentially prevented through lifestyle modification. Not surprisingly, these figures increased to 40% to 70% when assessed with regard to the population of US whites which has a much worse lifestyle pattern than other cohorts. Notably, approximately 80% to 90% of lung cancer deaths can be avoided if Americans adopted the lifestyle of the low-risk group, mainly by quitting smoking. For other cancers, a range of 10% to 70% of deaths can be prevented. These results provide strong support for the importance of environmental factors in cancer risk and reinforce the enormous potential of primary prevention for cancer control.”
Said another way, primary prevention should remain a priority for cancer control.
Given that many cancers are related to diet, environment and lifestyle, it is estimated that 50% of all cancers and cancer deaths could be prevented by modifying personal behavior. Thus, the monies spent on screening or even developing new treatments could better be spent on prevention along with implementing programs that promote a healthier environment, diet and personal behavior (AACR, 2011).
What can be done? Addressing systems not symptoms
From a ‘systems perspective,’ the first step is to reduce the cancer burden and carcinogenic agents that occur in our environment such environmental pollution (Turner et al., 2022). In many cases, governmental regulations that reduce cancer risk factors have been weakened, delayed, and contested for years through industry’s lobbying. It often takes more than 30 years after risk factors have been observed and documented before government regulations are successfully implemented, as exemplified in the battle over tobacco or, air pollution regulations related to particulates from burning fossil fuels (Stratton et al, 2001).
Sadly, we cannot depend upon governments or industries to implement regulations known to reduce cancer risks. More within our control is implementing lifestyle changes that enhance immune competence and promote health.
Implement a healthy life style that enhances immune competence and, supports health and well-being
Paraphrasing a trope of what some physicians may state: ‘Take two pills, and call me in the morning. Oh, and eat well, exercise, and get good rest.’ Broadly stated, the following are some controllable lifestyle behaviors that can decrease cancer risks and promotes health. Implementing environmental and lifestyle changes are very challenging because they are highly related to socio economic factors, cultural factors, industry push for profits over health, and self-care challenges since there are no immediate results experienced by behavior and lifestyle changes.
In many cases, the effects of harmful life-style and environment factors are only observed twenty or more years later (e.g., diabetes, lung cancer, cirrhosis of the liver). The individual does not experience immediate benefits of lifestyle changes thus it is more challenging to know that your healthy life style has an effect. The process is even more complex because in most cases it is not a single factor but the interaction of multiple factors (genetics, lifestyle, and environment). The complexity of causality so often conflicts with the simplistic research studies to identify only one isolated risk factor. Instead of waiting for the definitive governmental guidelines and regulations, adopt a ‘precautionary principle’ which means do not take an action when there is uncertainty about its potential harm (Goldstein, 2001). Do not wait for screening; instead, take charge of your health and implement as many of the following behaviors and strategies to enhance immune competence and thereby reduce cancer risks.
Eat organic foods, especially vegetable and fruits.
Many studies have suggested that eating organic foods and in particular more fruits and vegetable such as a Mediterranean diet is associated with increased health and longevity. Similarly, people who eat do not eat highly-processed or ultra-processed foods have better health status (Van Tulleken, 2023). For example, In the large prospective study of 68, 946 participants, adults who consumed the most organic fruits, vegetables, dairy products, meat and other foods had 25% fewer cancers when compared with adults who never ate organic food (Baudry et al., 2018; Rabin, 2018). Similarly, many studies have reported that those who adhere consistently to a Mediterranean diet have a significantly lower incidence of chronic diseases (such as cardiovascular diseases, diabetes, etc.) and cancers compared to those who do not adhere to a Mediterranean diet (Mentella et al., 2019).
Reduce environmental pollution exposure
Air pollution and the exposure to airborne carcinogens are a significant risk factor for cancers as illustrated by the increased cancer rates among smokers. In the USA, the reduction of smoking has significantly decreased the lung cancer deaths (US Department of Health and Human Services, 2014).
Increase movement and exercise
Many studies have documented that people who exercise regularly and are otherwise non–sedentary but are active their entire lives have the lowest risk for breast cancers and colon cancers. Women who exercise 3 hours a week or more have a 30-40% lower risk of developing breast cancer (NIH NCI, 2023). The NIH National Cancer Institute summary concludes that exercises also significantly benefited the following cancer survivors (NIH NCI, 2023):
- Breast cancer: In a 2019 systematic review and meta-analysis of observational studies, breast cancer survivors who were the most physically active had a 42% lower risk of death from any cause and a 40% lower risk of death from breast cancer than those who were the least physically active (Spei et al, 2019).
- Colorectal cancer: Evidence from multiple epidemiologic studies suggests that physical activity after a colorectal cancer diagnosis is associated with a 30% lower risk of death from colorectal cancer and a 38% lower risk of death from any cause (Patel et al., 2019).
- Prostate cancer: Limited evidence from a few epidemiologic studies suggests that physical activity after a prostate cancer diagnosis is associated with a 33% lower risk of death from prostate cancer and a 45% lower risk of death from any cause ((Patel et al., 2019).
- Implement stress management.
Chronic stress may reduce immune competence and increase the risk of cancers as well as hinders healing from cancer treatments (Dai et al., 2020). The results of numerous studies have shown that implementing stress management spractices uch as Cognitive-behavioral stress management (CBSM) improves mood and lowers distress during treatment and, is also associated with longer survival compared to control groups in the 8-15 year follow up (Stagl et al., 2015).
Respect your biological rhythm.
The International Agency for Research on Cancer (IARC) reports that, when the human circadian clock is disrupted, the likelihood of developing cancers, including lung cancers, intestinal cancers, and breast cancers, dramatically increases (Huang, et al., 2023). Go to bed at the same time and, have about 8 hours of sleep. As much as possible avoid night shifts at work along with frequent jet lag as that highly disrupts the circadian rhythm.
Increase social connections and be part of a social community
Absence of social support, feeling lonely and socially isolated tends reduces immune competence and increases cancer mortality risk while having more social support satisfaction is associated with lower mortality risks (Salazaor et al., 2023; Boen et al., 2018). Meta-analysis of 148 studies (308,849 participants) found that that on the average there is a 50% increased likelihood of survival for participants with stronger social relationships (Holt-Lunstad et al., 2010).
Live a life with meaning and purpose
Having meaning and purpose make each moment worth living and may contribute to improving immune function and possible cancer survival (LeShan, 1994; Rosenbaum & Rosenbaum, 2023).
Summary
The research suggests that cancer screening does not extend life span unless specifically performed for certain diagnostic purposes or, with individuals who are at high risk of developing cancers (e.g., have a genetic predisposition). Implementing self-care health behaviors that have been identified to promote health and increase lifespan. Implementing health behaviors is challenging since there is limited governmental and corporate support. Thus, take charge and implement a holistic self-care lifestyle that reduces cancer risk factors and supports health.
See also the following blogs:
References
AACR. (2011). AACR Cancer Progress Report 2011. American Association for Cancer Research. http://www.aacr.org/Uploads/DocumentRepository/2011CPR/2011_AACR_CPR_Text_web.pdf
American Cancer Society. (2021). History of ACS Recommendations for the Early Detection of Cancer in People Without Symptoms. Accessed November 11, 2023. https://www.cancer.org/health-care-professionals/american-cancer-society-prevention-early-detection-guidelines/overview/chronological-history-of-acs-recommendations.html
Autier, P., Boniol, M., Gavin, A,, & Vatten, L.J. (2011) Breast cancer mortality in neighbouring European countries with different levels of screening but similar access to treatment: trend analysis of WHO mortality database. BMJ. 343, d4411. https://doi.org/10.1136/bmj.d4411
Badal., K., Staib, J., Tice,J., Kim, M-O., Eklund, M., DaCosta Byfield, S., Catlett,K., Wilson,L., et al, (2023). Cost of breast cancer screening in the USA: Comparison of current practice, advocated guidelines, and a personalized risk-based approach. Journal of Clinical Oncology, 41: 16_suppl, 3 18917 :16_suppl, e18917. https://doi.org/10.1200/JCO.2023.41.16_suppl.e18917
Baudry, J., Assmann, K.E., Touvier, M., et al. (2018). Association of Frequency of Organic Food Consumption With Cancer Risk: Findings From the NutriNet-Santé Prospective Cohort Study. JAMA Intern Med, 178(12), 1597–1606. https://doi.org/10.1001/jamainternmed.2018.4357
Boen, C.E., Barrow, D..A, Bensen, J.T., Farnan, L., Gerstel, A., Hendrix, L.H., Yang, Y.C. (2018). Social Relationships, Inflammation, and Cancer Survival. Cancer. Epidemiol Biomarkers Prev, 27(5), 541-549. https://doi.org/10.1158/1055-9965.EPI-17-0836
Bretthauer M, Wieszczy P, Løberg M, et al. (2023). Estimated Lifetime Gained With Cancer Screening Tests: A Meta-Analysis of Randomized Clinical Trials. JAMA Intern Med. 183(11),1196–1203. https://doi.org/10.1001/jamainternmed.2023.3798Brown, K.F., Rumgay, H., Dunlop, C. et al. (2018). The fraction of cancer attributable to modifiable risk factors in England, Wales, Scotland, Northern Ireland, and the United Kingdom in 2015. Br J Cancer, 118, 1130–1141. https://doi.org/10.1038/s41416-018-0029-6
CDC. (2023a). U.S. Cancer Statistics Working Group. U.S. Cancer Statistics Data Visualizations Tool, based on 2022 submission data (1999-2020): U.S. Department of Health and Human Services, Centers for Disease Control and Prevention and National Cancer Institute; released in November 2023. https://www.cdc.gov/cancer/dataviz
CDC. (2023b). Leading Causes of Death. National Center for health statistics, Centers for disease control and prevention. Accessed November 20, 2023. https://www.cdc.gov/nchs/fastats/leading-causes-of-death.htm
CSPH. (2021). Estimating annual expenditures for cancer screening in the United States. Center for Surgery and Public Health. Assessed November 14, 2023. https://csph.brighamandwomens.org/wp-content/uploads/2021/12/Estimating-Annual-Expenditures-for-Cancer-Screening-in-the-United-States.pdf
Dai, S., Mo, Y., Wang, Y., Xiang, B., Liao, Q., Zhou, M., Li, X., Li, Y., Xiong. W., Li, G., Guo, C., & Zeng, Z. (2020). Chronic Stress Promotes Cancer Development. Front Oncol. 10, 1492. https://doi.org/10.3389/fonc.2020.01492
Feinberg, A. P. (2007). Phenotypic plasticity and the epigenetics of human disease. Nature, 447(7143), 433-440. https://doi.org/10.1038/nature05919
Fouad, Y. A., & Aanei, C. (2017). Revisiting the hallmarks of cancer. American journal of cancer research, 7(5), 1016. https://pubmed.ncbi.nlm.nih.gov/28560055/
Fracheboud, J. et al. (2004). Decreased rates of advanced breast cancer due to mammography screening in The Netherlands, British Journal of Cancer (2004) 91, 861–867. https://doi,org/10.1038/sj.bjc.6602075
Goldstein, B.D. (2001). The precautionary principle also applies to public health actions. Am J Public Health, 91(9),1358-61. https://doi.org/10.2105/ajph.91.9.1358
Gorter, R. & Peper, E. (2011). Fighting Cancer-A None Toxic Approach to Treatment. Berkeley: North Atlantic/New York: Random House. https://www.amazon.com/Fighting-Cancer-Nontoxic-Approach-Treatment/dp/1583942483
Gupta, P. B., Pastushenko, I., Skibinski, A., Blanpain, C., & Kuperwasser, C. (2019). Phenotypic plasticity: driver of cancer initiation, progression, and therapy resistance. Cell Stem Cell, 24(1), 65-78. https://doi.org/10.1016/j.stem.2018.11.011
Hanahan, Douglas. (2022): Hallmarks of cancer: new dimensions. Cancer discovery, 12(1), 31-46. https://doi.org/10.1158/2159-8290.CD-21-1059
Holt-Lunstad, J., Smith, T.B., & Layton, J.B. (2010). Social Relationships and Mortality Risk: A Meta-analytic Review, PLoS Med 7(7), e1000316. https://doi.org/10.1371/journal.pmed.1000316
Huang, C., Zhang, C,, Cao, Y., Li, J., & Bi, F. (2023). Major roles of the circadian clock in cancer. Cancer Biol Med, 20(1):1–24. https://doi.org/10.20892/j.issn.2095-3941.2022.0474
Kalaf, J.M. (2014). Mammography: a history of success and scientific enthusiasm. Radiol Bras. 47(4):VII-VIII. https://doi.org/10.1590/0100-3984.2014.47.4e2
Key TJ, Bradbury KE, Perez-Cornago A, Sinha R, Tsilidis KK, Tsugane S. Diet, nutrition, and cancer risk: what do we know and what is the way forward? BMJ. 2020 Mar 5;368:m511. https://doi.org/10.1136/bmj.m511
Kowalski, A.E. (2021). Mammograms and mortality: How has the evidence evolved? J Econ Perspect, 35(2), 119-140. https://doi.org/10.1257/jep.35.2.119
LeShan, L. (1994). Cancer as a turning point. New York: Plume. https://www.amazon.com/Cancer-As-Turning-Point-Professionals/dp/0452271371
Lewis, T. (2022). The U.S. just lost 26 years’ worth of progress on life expectancy. Scientific American. October 17, 2022. Accessed November 11, 2023. https://www.scientificamerican.com/article/the-u-s-just-lost-26-years-worth-of-progress-on-life-expectancy/
Ma, X., Wang, R., Long, J.B., Ross, J.S., Soulos, P.R., Yu, J.B., Makarov, D.V., Gold, H.T. and Gross, C.P. (2014), The cost implications of prostate cancer screening in the Medicare population. Cancer, 120: 96-102. https://doi.org/10.1002/cncr.28373
Mentella, M.C., Scaldaferri, F., Ricci, C., Gasbarrini, A., & Miggiano, G.A.D. (2019). Cancer and Mediterranean Diet: A Review. Nutrients,11(9):2059. https://doi.org/10.3390/nu11092059
NIH NCI (2023). Physical Activity and Cancer. National Institutes of Health National Cancer Institute. Accessed November 18, 2023. https://www.cancer.gov/about-cancer/causes-prevention/risk/obesity/physical-activity-fact-sheet
Patel, A,V., Friedenreich, C.M., Moore, S.C, et al. (2019). American College of Sports Medicine Roundtable Report on physical activity, sedentary behavior, and cancer prevention and control. Medicine and Science in Sports and Exercise, 51(11), 2391-2402. https://doi.org/10.1249/MSS.0000000000002117
Rabin, R.C. (2018). Can eating organic food lower your cancer risk? The New York Times. Oct 23, 2018. Accessed November 17, 2023. https://www.nytimes.com/2018/10/23/well/eat/can-eating-organic-food-lower-your-cancer-risk.html
Reuben, S.H. (2010). Reducing environmental cancer risk – What We Can Do Now. The President’s Cancer Panel Report. Washington, D.C: U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES, National Institutes of Health, National Cancer Institute. https://deainfo.nci.nih.gov/advisory/pcp/annualReports/pcp08-09rpt/PCP_Report_08-09_508.pdf
Rosenbaum, E. H. & Rosenbaum, I.R. (2023) The Will to Live. Stanford Center for Integrative Medicine. Surviving Cancer. Accessed November 23, 2023. https://med.stanford.edu/survivingcancer/cancers-existential-questions/cancer-will-to-live.html
Salazar, S.M.D.C., Dino, M.J.S., & Macindo, J.R.B. (2023). Social connectedness and health-related quality of life among patients with cancer undergoing chemotherapy: a mixed method approach using structural equation modelling and photo-elicitation. J Clin Nurs. Published online March 9, 2023. https://doi.org/10.1111/jocn.16675
Schmutzler, R. K., Schmitz-Luhn, B., Borisch, B., Devilee, P., Eccles, D., Hall, P., … & Woopen, C. (2022). Risk-adjusted cancer screening and prevention (RiskAP): complementing screening for early disease detection by a learning screening based on risk factors. Breast Care, 17(2), 208-223. https://doi.org/10.1159/000517182
Song, M., & Giovannucci, E. (2016). Preventable incidence and mortality of carcinoma associated with lifestyle factors among white adults in the United States. JAMA Ooncology, 2(9), 1154-1161. https://doi.org/10.1001/jamaoncol.2016.0843
Spei, M.E., Samoli, E., Bravi, F., et al. (2019). Physical activity in breast cancer survivors: A systematic review and meta-analysis on overall and breast cancer survival. Breast, 44,144-152. https://doi.org/10.1016/j.breast.2019.02.001
Stagl, J.M., Lechner, S.C., Carver, C.S. et al. (2015). A randomized controlled trial of cognitive-behavioral stress management in breast cancer: survival and recurrence at 11-year follow-up. Breast Cancer Res Treat, 154, 319–328. https://doi.org/10.1007/s10549-015-3626-6
Stratton, K., Shetty, P., Wallace, R., et al., eds. (2001). Institute of Medicine (US) Committee to Assess the Science Base for Tobacco Harm Reduction. Washington (DC): National Academies Press (US). https://www.ncbi.nlm.nih.gov/books/NBK222369/
Tailor, T.D,, Bell, S., Fendrick, A.M., & Carlos, R.C. (2022) Total and Out-of-Pocket Costs of Procedures After Lung Cancer Screening in a National Commercially Insured Population: Estimating an Episode of Care. J Am Coll Radiol. 19(1 Pt A), 35-46. https://doi.org/10.1016/j.jacr.2021.09.015
Turner, M.C., Andersen, Z.J., Baccarelli, A., Diver, W.R., Gapstur, S.M., Pope, C.A 3rd, Prada, D., Samet, J., Thurston, G., & Cohen, A. (2020). Outdoor air pollution and cancer: An overview of the current evidence and public health recommendations. CA Cancer J Clin, 10.3322/caac.21632. https://doi.org/10.3322/caac.21632
US Department of Health and Human Services (2014). The Health Consequences of Smoking: 50 Years of Progress. A Report of the Surgeon General. Atlanta, GA: :
US Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health. https://aahb.org/Resources/Pictures/Meetings/2014-Charleston/PPT%20Presentations/Sunday%20Welcome/Abrams.AAHB.3.13.v1.o.pdf
Van Tulleken, C. (2023). Ultra-processed people. The science behind food that isn’t food. New Yoerk: W.W. Norton & Company. https://www.amazon.com/gp/product/1324036729/ref=ox_sc_act_title_1?smid=ATVPDKIKX0DER&psc=1
The Digital Detox Blueprint: How To Win The War Against Your Smartphone Today
Posted: October 30, 2023 Filed under: attention, behavior, biofeedback, Breathing/respiration, cognitive behavior therapy, computer, digital devices, ergonomics, Evolutionary perspective, health, laptops, screen fatigue, vision, zoom fatigue | Tags: attention, insomnia, social connections 1 CommentWatch the presentation or Listen to the podcast, The Digital Detox Blueprint: How To Win The War Against Your Smartphone Today, produced by The Root Cause Medicine Podcast, and dive deeply into the following topics.
1. The role of technology and stress in our lives
2. What is tech stress?
3. Practical strategies for managing tech stress
4. The connection between technology and eye health
5. The negative effects of social media
6. How to use technology for personal health and well-being
7. The importance of sleep for overall well-being
To watch:
To listen: apple.co/46QaoAu

The episode is available on all podcast platforms (Apple Podcasts, Spotify, Google Podcasts, etc) and have posted to the episode on the Rupa Website.
Be Skeptical: Finding and Evaluating Online Health Resources
Posted: October 22, 2023 Filed under: Evolutionary perspective, healing, health, Nutrition/diet, placebo | Tags: advertising, clinial trialslinical efficacy, critical thinking, efficacy, health information, mobile apps, online resources, research methodology, social media 2 CommentsAdapted from: Peper, E. & Harvey, R. (2023). Be skeptical: Finding and evaluating online health resources. Townsend Letters. The Examiner of Alternative Medicine, October 21, 2023. https://www.townsendletter.com/e-letter-20-evaluate-sources-to-make-informed-choices/
Erik Peper, PhD, BCB and Richard Harvey, PhD

Source: https://live.staticflickr.com/65535/48445803437_726b61e3d1_b.jpg
An unprecedented flood of information is available today at our fingertips in the form of cell phone apps, news stories, blog posts, social media feeds, advertisements, websites, videos, and audio resources. Artificial intelligence (AI) applications such as ChatGPT are also capable of curating health and wellness information all proclaiming to optimize our health or treat our illnesses. This article provides strategies to determine how to trust the information. It offers strategies for assessing information, reasons to have a skeptical perspective, suggestions for finding credible resources and includes a framework to identify beneficial health information, which may be used for improving activities of daily living. The recommendations are based upon an evolutionary perspective in which anything that was not part of our evolutionary past should be viewed with healthy skepticism.
“It is simply no longer possible to believe much of the clinical research that is published, or to rely on the judgment of trusted physicians or authoritative medical guidelines. I take no pleasure in this conclusion, which I reached slowly and reluctantly over my two decades as an editor of The New England Journal of Medicine.” —Dr. Marcia Angell (2009), the first woman editor of the highly respected New England Journal of Medicine.
How to make sense of the flood of health information
An unprecedented flood of health information is available today proclaiming useful information to optimize our health or treat our illnesses, A simple question is, “How do we know which information is accurate?” To what extent do we trust the information in an era of fake news, commercial health apps trying to sell us things, and news stories from publishers and media conglomerates that are dependent on advertising revenues? This article offers strategies for assessing information, reasons to have a skeptical perspective, and suggestions for finding relevant and accurate information.
Skepticism about health information takes many forms including ‘conspiracy theories’ about vaccines such as when people claim a SARS-COVID-19 vaccine will kill you, to when people doubt the efficacy of HIV or similar vaccines. Several authors have suggested political as well as individual personality factors which explain conspiratorial skepticism about health information, most commonly about vaccines (Crescenzi-Lanna, Valente, Cataldi, & Martire, 2023; Koinig, & Kohler, 2021; Putois, & Helms,. 2022). This article takes a broader view of health information skepticism, focusing on perspective building as well as asking relevant, accurate and meaningful questions about health care decisions.
Take a skeptical perspective and ask, “What is the evidence that the product, procedure, or treatment is going to be effective for me compared to others?” The answer could appear obvious: published peer-reviewed systematic meta-analyses of double blind, randomized, controlled trials describing specific products or procedures. However, the answer is more complex. In numerous cases, finding relevant reports can be challenging. In some cases, it may be unethical or impossible to run double blind, randomized, controlled trials to detect the scope of effectiveness or generalize the finding from animal studies to human beings. For example, surgery cannot be evaluated in a double-blind study. (Would you really want your surgeon not to be aware of what he/she was doing?). Although treatment effectiveness can be studied using a matched comparison or a control group receiving mock surgery, in those cases the surgeon would still be aware of the procedure.
The Challenges of Assessing Clinical Efficacy
It is challenging to know what actually contributes to the beneficial outcomes as well as how to measure the outcome. Some of the factors that affect the outcomes include:
Placebo interactions: Intrinsic to all procedures are placebo and nocebo components. In some cases the direct benefit effects of a drug or procedure demonstrated in a randomized controlled trial may still not be due solely to the direct effects of the drug or procedure, but rather due to positive indirect effects triggered by the placebo response to non-specific side effects (Peper and Harvey, 2017).
Lack of evidence is not proof that it does not work. Lack of replicable evidence for some cases implies that a positive response will not occur in all cases. Unfortunately, commercial interests may bias interpretations of research studies when the efforts to replicate a study had limitations in the first place, or the replication efforts did not retain transferable conditions to the next study. In other words, ‘ceteris paribus’ may not apply as all things are not always equal during replication studies. Similarly, individual differences that are outliers or extreme values during a study (e.g. positive benefit from placebo) can be ‘explained away’ with statistics because statistics may also skew the interpretations based on the biases of the researchers.
Clinical trials are very expensive. The average clinical trial for a new therapeutic agent, 2015–2017, was $48 million dollars (Moore et al., 2020). The cost of achieving Food and Drug Administration (FDA) approval is so high that it is often out of reach for small companies. It is no wonder that most clinical trials are funded by the pharmaceutic industry and only for those drugs for which they foresee significant profits. The estimated research and development investment to bring a new medicine to market is estimated to range between $314 million to $2.8 billion (Wouters et al, 2020). To be financially viable, this usually means that drugs must be used by a large consumer base and ideally be taken for the rest of the individual’s life. Non-drug approaches may be less profitable, so without a profit incentive, investigations of non-drug efficacy accumulates less evidence compared to multi-million dollar trials.
Human beings are not rats, mice, or monkeys. The findings from animal studies in numerous studies provide some useful insights into the effects of medications or procedures on living organisms. Unfortunately, many results from animal studies could not be replicated in humans or, the findings may not apply to human beings. The basic assumption that animal studies could mimic human studies may not be valid since almost all test animals are not typical of normal animals, implying test animals are ‘abnormal’ in terms of results. For example, the animals such as rats are usually housed in small cages 24 hours a day which is analogous to a human being held in solitary confinement without social contact or ability to move for a lifetime. Thus, their physiology and their response to interventions are often different from healthy free ranging animals (Shaw, 2023).
Even when animal studies show that the medications are not harmful, they could be harmful for some human beings. For example, thalidomide was approved for use in Germany, so doctors prescribed it to treat morning sickness in pregnant women. However, in humans Thalidomide interfered with embryonic and fetal development in ways not observed in rodent tests (Tantibanchachai & Yang, 2019).
Statistical significance may not indicate meaningful clinical improvement. Many clinical studies demonstrate that the studied interventions have contributed to improvement. However, does the improvement make a quality of life (QOL) difference and/or clinically relevant difference for the person? For example, a successful study that demonstrated lowering of patients’ systolic pressure by 5 mm from 175 mm/Hg to 170mm/Hg may be statistically significant, but is not clinically meaningful, since, a resting systolic blood pressure of 170 mm/Hg is still a cause for concern.
Similarly, in the recent systematic review by Arciero et al. (2021) of approved oncology therapies, 40% of Food and Drug Administration (FDA)-approved as well as 58% of European Medicine Agency (EMA)-approved indications had published QOL evidence. However, only 6% of FDA- and 11% of EMA-approved indications had clinically meaningful improvements in QOL beyond minimally clinically relevant differences. This means that medication therapies are often approved without demonstrating Quality of Life improvement for the long term.
Statistics which describe how large an effect is may be referred to as an ‘effect size estimate, which is a better index of efficacy compared to other statistics such as a difference in statistical mean values. The effect size can be assessed by using various statistics such as Cohen’s d-statistic (Mean A minus Mean B divided by pooled standard deviation; Cohen, 1988)[i].
Number of people need to be treated for one person to benefit. Effect size calculation estimates the average number of people in a trial needing treatment so that one of them experiences benefit. This statistic can be referred to as the number needed to treat (NNT) (Mendes et al., 2017). To calculate the NNT, divide 1 by the control event rate (CER) minus the treatment event rate (TER) or 1/CER-TER. For example, the number patients needed to be treated for five years with cholesterol lowering (e.g., statin drugs) medications to prevent one coronary heart disease event ranges from 53 (high risk group) to 146 (low risk group) (Rossignol et al., 2018). This means that many of the participants could experience negative side effects related to the medications while only one participant benefits from the prevention of a heart attack.
Focus on short-term versus long-term benefits. Many studies measure outcomes under highly controlled conditions of a study and are conducted for a relatively short time period—often for less than 3 months. However, effects that may be beneficial in the short term may not be beneficial or may even be harmful in the long term. For example, opioid medications are very useful in the short term to alleviate intense pain. However, over time, drug dependency may develop, contributing to addiction, inability to function, or death. Shockingly, opioid-related deaths in the U.S. numbered more than 100,000 people in 2022 (CDC, 2022).
Benefits do not enhance quality of life. If the data indicate benefits of treatment, do the interventions improve quality of life and not simply prolong life for a few days, weeks, or months? Does the patient or client value quality of life over quantity of days lived (e.g., ”palliative care with shorter life, but some relief from pain and suffering versus prolonged life with pain and suffering”)?
Results may only apply to a select group. Biochemical individuality means that each person is unique to some degree, differing genetically, biochemically, and physiologically. Similarly, responses vary widely to medical procedures, medications, and other substances. A common example is alcohol sensitivity— the genetic predisposition to metabolizing alcohol breakdown— manifesting in highly visible facial flushing which occurs in 47%-85% of Asians and 3%-29% of Caucasians (Chan, 1986). In the context of medicine, individual differences that influence clinical outcomes include genetic predisposition, as well as age, gender, income, education level, job status, geographic region (e.g., climate and food sources) and other demographic factors, individually or in combination.
Consider that many interventions and medications have only been tested on narrowly defined subgroups such college students (true of most psychological studies), or men (true for most pharmaceuticals since women could be pregnant or in different phases of their menstrual cycle). The promise of personalized or ‘precision’ medicine will likely advance in the coming years, making medications more tailored to individual differences based on age, sex, and other demographic factors.
There is no free lunch. Similar to the concept of short-term versus long-term benefits, when a drug offers a quick improvement, it may be effective, but may cause long-term harm. A representative example is the use of high-dose and multi-doses of anabolic steroids to increase muscle mass and athletic performance. There is a potential cost: “High and multi-doses of anabolic steroids used for athletic enhancement can lead to serious and irreversible organ damage” (Maravelias, et al., 2005).
Risks of hazardous exposures and risks associated with the treatment. Could the procedure or medication result in loss or harm? Given bio-individuality, there can be broad “variability” in response and outcome, which depends on the vulnerability of a given individual (their adaptive capacity) and the risks involved. Additionally, there are sometimes important variables that have not been investigated deliberately because those important variables complicate interpretation, and or, there may be important variables that are missed The most obvious example of omission is when animal studies were or are conducted exclusively on male animals because interpreting results can be more complicated given female reproductive hormones. Beside sex variables other important variables that may be missed include covert illnesses and co-morbidities which are unknown at the time of the study. Taken together, studies which oversimplify variables may make it difficult interpret the results for individuals.
Below is a set of images relevant to climate change and farming, depicting the relationship between the exposure to hazards of systemic climate change and the vulnerabilities, sensitivities, and adaptive capacities of individuals and the community (Wilhelmi and Hayden, 2016).

Use “Uncommon” Sense
The attractive look and feel of a website are not evidence of accuracy or credibility. Rather, good design simply means it was developed by a skilled web designer or that the client paid a great deal of money to have it created. It does not make the content valid. The comments of Yucha (2002) and Yucha and Montgomery (2008) remind readers to increase literacy regarding ”health claims” made on websites, especially a commercial website intended to sell products or services.
Evaluating dietary supplements. If you’re thinking about using a dietary supplement, check the recommendations from reliable sources. Make it a point to purchase a reputable brand, since some supplements contain ingredients not listed on the label. In addition, they may interact with medications or other supplements. Share and discuss all your supplements you are taking with your healthcare provider. For example, vitamin E acts as anticoagulants and may increase clotting time and bleeding especially if one is taking “blood thinners.”
Follow the money. Ask who would financially benefit from the product or service? For example, physicians increase their referrals for lab testing, MRIs (Magnetic Resonance Images), or other diagnostic procedures if they have ownership in those testing centers or, if they receive significant reimbursement for those services, although there is no evidence that patients benefit more (Bishop et al, 2010).
Beware of advertised claims. Most highly advertised drugs are largely no better at treating a disease than generic medication or other options (Patel et al., 2023). Pharmaceutical companies in 2021 spend $6.88 billion for direct to consumer advertising (Faria, 2023). The advertisement suggests that their branded medication is better; however, generics are about 80% cheaper and have the same active ingredient and are similar in their action (AAM, 2020).
If the claims seem unbelievable, they are probably are unbelievable. If it is too good to be true, it probably is not true. Historically, Thomas Lupton (1580) wrote a thoughtful inquiry about religion and utopian societies, introducing a skeptics point of view, describing people and societies that are ”too good to be true.” Modern skeptics consider the preponderance of evidence based on scientific replicability (the replication of findings in subsequent clinical trials) as proof of what they believe to be true.

Source: Indiana University of Pennsylvania, last accessed March 3, 2023 https://www.iup.edu/instructional-design/images/assessment.jpg
Assessing Online Information
What do we know about the accuracy of online health information? A skeptical viewpoint is that bias exists in sources of information from a wide range of commercial, organizational, governmental and educational institutions (identified by ending with .com, .org, .gov and .edu, respectively). Most all institutions set out to prove their own bias; however, people working in educational institutions by and large require their investigators go through a peer-review process, so they tend to be more trusted as sources of information. Commercial, organizational, and governmental institutions all have biased perspectives. However, they are less likely to reveal their biases, simply stating that “a study was conducted” without providing enough information who funded the study or the importance of positive results to achieve academic recognition.
“A lot of what is published is incorrect … much of the scientific literature, perhaps half, may simply be untrue. Afflicted by studies with small sample sizes, tiny effects, invalid exploratory analyses, and flagrant conflicts of interest, together with an obsession for pursuing fashionable trends of dubious importance, science has taken a turn towards darkness.” Dr. Richard Horton (2015), Editor-in-Chief of The Lancet.
Be skeptical of university or published research findings that are directly or indirectly funded/influenced by industry or commercial sources. Government research published in highly respected scientific journals may not be replicable because the investigations were narrowly designed to favor a particular bias. For example, industries that produce pharmaceuticals and medical devices, as well as agribusinesses that produce tobacco and sugar products, have been accused of a ”profit-first” bias (Bruening, 2019; Hill et al., 2019). These industries often support studies conducted by “independent” researchers at universities. However, grant funding quickly disappears if the findings are negative which may affect the career of the researcher because many university faculty positions and promotions depend upon the faculty member’s ability to garner grants.
Compare US safety guidelines to those of the EU. In many cases, the acceptable values are different. The safety limits for herbicide and pesticide residues in foods are often much lower in the EU than in the US (e.g., safer with lower exposure levels). For example, the US allows six times as much residue of the pesticide, Round-Up, with a toxic ingredient, glyphosate, in foods consumed in the American diet (Tano, 2016). The USA allows this higher exposure even though about half of the human gut microbiota are vulnerable to glyphosate exposure (Puigbo et al., 2022). A skeptical view of research could adapt a precautionary principle such as “if you think it could cause harm then do not use it until proven safe.”
Government guidelines and directions may not always be accurate. For example, after 9/11 the CDC initially announced that the particulate dust from the World Trade Center collapse was not harmful The CDC made this claim without any data, in efforts to reassure the public. In fact, the dust was harmful. More recently, some of the politicization of the CDC COVID-19 recommendations have raised questions. For example at the beginning of the pandemic, the CDC publicly recommended “If you are NOT sick: You do not need to wear a facemask unless you are caring for someone who is sick (and they are not able to wear a facemask)” which suggested that masks were not necessary. (McReynolds, 2020). Most likely, the statement was made so that more masks would be available for medical workers. The statement would have engendered more trust if the CDC had stated, Masks are useful; however, please make your own, since the medical-grade n95 masks are in very short supply and needed to protect the frontline health professionals who are most at risk.
The National Personal Protective Technology Laboratory (NPPTL) describes the types of masks needed to protect medical and other types of workers such as fire fighters, where the numbers represent the percentage of particulates filtered (e.g., 95%, 99%, 100%) and the letters represent the types of particles (e.g., N = not resistant to oils, R = resistant to oils and, P = strongly resistant to oils). Other countries have similar mask standards, where a N95 mask in the United States (i.e., N95; NIOSH-42 CRF 84) is equivalent to masks in Europe (FFP2; EN149-2001), China (KN95; GB2626-2019), Australia (P2; AS/NZ 1716-2012), Korea (KF94; KMOEL 2017-64), Japan (DS2; JMIHLW 214-2018) and, Brazil (PFF2; ABNT/NBR 13.698.2011). The reason for including the technical details about masks is to remind the reader that both governments as well as other sources of health information may hide some of the information about potentials for loss or harm behind lots of technical details, so knowing how to compare information becomes relevant when making health decisions.
Patient population in the research study may not represent the average patient (referred to as Berkson’s bias). Research study subjects may have multiple co-morbidities or may all be healthy young males. In either case, they may not be representative of the general patient population nor of individuals (Westreich, 2012).
The data does not discuss or excludes outliers? Positive findings, even in randomized, placebo-controlled studies, mean that the treatment approach is more beneficial than the control condition. In almost all cases, some participants respond extremely well and some very poorly, often referred to as statistical outliers. What is usually not reported are the characteristic of the ‘super responders’ or ‘non-responders.’ Have more trust in studies that provide a full range or a wider range of information about the positive and negative responders, rather than simply reporting about the average response.
The research review is highly selective. Meta-analyses and review articles evaluate the outcomes of multiple research studies. However, typically they include only well designed randomized controlled trials. In many of these studies, 95% of the published articles are excluded because they did not fit the narrow criteria of the randomized selection. Thus, these meta-analyses may exclude conditions under which the treatment approach would be highly beneficial to a specific set of people. When the meta-analyses identify the studies that are excluded and why, it is possible to learn of the biases of the meta-analyses.
Funding for research or clinical trials favors products or technologies which can be patented, commercialized and support industry profits. There is extensive funding for new drug development for the treatment of COVID-19 or hypertension, but limited funding for diet or lifestyle changes that could optimize the immune system. If a product or drug is beneficial however not patentable, it is unlikely that a pharmaceutical company will further develop and market it because competitors could easily produce it. For example, pharmaceutical companies do not advertise vitamin D3 supplements because it is not patent protected even though a preponderance of independent research has clearly demonstrated that the incidence of symptoms following metastatic cancer diagnosis is reduced with vitamin D3 supplements (Chandler et al., 2020).
Be aware of the revolving door. The top administrators of numerous US regulating agencies such as the Food and Drug Administration (FDA) and the US Department of Agriculture (USDA) are often rewarded with well-paying jobs in the pharmaceutical, healthcare, and agribusiness industries after leaving jobs in the US government. For example,
- Scott Gottleib, MD was head of the FDA 2017-2019 before leaving the government in 2019 and then has been a board member of Pfizer pharmaceuticals as independent director. (https://www.pfizer.com/people/leadership/board_of_directors/scott_gottlieb-md).
- Stephen Han was the FDA commissioner under President Trump and approved the emergency use of the Moderna vaccine. Six months later, he quit and joined Flagship Pioneering, the firm behind Moderna. (https://www.fiercebiotech.com/biotech/six-months-after-granting-moderna-covid-19-eua-ex-fda-commish-joins-biotech-s-founding).
- Joby Youn, who served as chief of staff to former U.S. Department of Agriculture Secretary Sonny Perdue, went on to work for the American Farm Bureau Federation. (McVan, 2022).
A skeptical question to be raised is to what extent does the promise of well-paying jobs impact the decisions of administrators who are in charge of regulating industries that may offer a high paying job in the future. Would you avoid antagonizing those companies thereby risk a future financial windfall? Similar conflicts of interest may be at play in other industries. For example, Boeing’s close relationship with the Federal Aviation Administration (FAA) by giving initial approval of Boeing 737 Max airplane that may have contributed to the two fatal airplane crashes (Cassidy, 2020).
Use critical thinking and don’t rely solely on the first internet search results resources when making decisions about your health. Many commercial companies (e.g., internet resources ending with ‘.com’) will pay to be on the first page of an internet search. Consider using more advanced internet search results that access ‘scholarly’ information, often available from ‘.edu’ sources. Consult with your health care provider when you are considering complementary health care approaches if you have a medical condition. Remember that some health providers may have personal biases as well as financial incentives in keeping you as their patient. Request evidence on which the provider is making their judgements and be sure to discuss the following two kinds of questions: (1) What are the risks, costs and benefit as well as potential for loss or harm? (2) Does the product or service interfere with other treatments? If not, then do what you think is useful. At worst, all you will lose is money.

Source: http://library.med.utah.edu/blog/eccles/files/2011/08/logoHealthLiteracy.png
Finding Health Information on the Internet
The following guidelines have been adapted from an online paper from the National Center for Complementary and Integrative Health (NCCIH) entitled, Finding and Evaluating Online Resources. The text in italic is reproduced directly from the online paper (NCCIH, 2023).
“Your search for published and online health information may start at a known, trusted site, but after following several links, you may find yourself on an unfamiliar site. Can you trust this site? Here are some key questions you need to ask.”
When checking online sources of health information, ask the following questions:
Who operates and pays for the website? Can you trust them? Any reliable health-related website should make it easy for you to learn who is responsible for the site. You should be able to find out who runs a website and its purpose on the “About Us” page. For example, on the NCCIH Website, each major page identifies NCCIH and, because NCCIH is part of the NIH, provides a link to the NIH home page.
Does the site sell advertising? Or Why does the site or app exist? Is it sponsored by a company that sells dietary supplements, markets drugs, provides other product, or services? Confirm any information you find on a site that sells products with an independent site that is not a commercial site.
What is the source of the information? Many health or medical sites post information collected from other websites or sources, and that information should be identified. For example, the Health Topics A-Z page on the NCCIH site provides links to documents that NCCIH did not create—but names the sources of the documents.
How do you know if the information is accurate? Is it based on scientific research? The site should describe the evidence (such as articles in medical journals) on which the material is based. Opinions or advice should be clearly set apart from information that is evidence-based (based on research results). For example, if a site discusses health benefits you can expect from a treatment, look for references to scientific research that clearly support what is said. Keep in mind that testimonials, anecdotes, unsupported claims, and opinions are not the same as objective, evidence-based information. [It is important to remember that this does not mean that it is incorrect; it just may mean the appropriate study was not done as there was no funding for it.]
Is the content a sales pitch masquerading as a news report? Some of these reports are reliable, but others are confusing, conflicting, misleading, or missing important information. For insight on how to evaluate news stories about health, wellness, and complementary therapies, visit our interactive module Know the Science: The Facts About Health News Stories.
Has the information been reviewed by experts? You can be more confident in the quality of medical information on a website if health experts reviewed it. Some websites have an editorial board that reviews content. Others put the names and credentials of reviewers in an Acknowledgments section near the end of the page and declare any conflict of interest. [Yet, even this is challenging as stated in the previous quotes by the Lancet journal editor-in-chief Horton. Thus having sign-off by someone with an advanced degree may not guarantee veracity.]
How current is the information? When was the information written or reviewed? Outdated medical information can be misleading or even dangerous. Responsible health websites review and update much of their content on a regular basis. Content such as news reports or meeting summaries that describe an event usually is not updated. To find out whether information is outdated, look for a date on the page (it’s often near the bottom). [However, old information does not mean that it is incorrect. Information from the past may be valid and even fundamental and foundational. Sometimes an older medication may be more effective; however, it is no longer recommended because it has outlasted the time period of its patent protection and, the pharmaceutical company has created a slightly new variation which may or may not be more effective.]
What is the website or smartphone app promising or offering? When claims seem too good to be true, the claims probably are not true.
Useful websites for information resources. Start with one of these organized collections of quality resources suggested by the University of Utah (2023):
- Google Scholar ( https://scholar.google.com/ ) provides access to many peer-reviewed resources.
- MedlinePlus, (https://medlineplus.gov/) sponsored by the National Library of Medicine, which is part of the National Institutes of Health (NIH)
- healthfinder.gov, sponsored by the Office of Disease Prevention and Health Promotion in the U.S. Department of Health and Human Services.
- National Center for Complementary and Integrative Health (NCCIH), (https://www.nccih.nih.gov/) the Federal Government’s lead agency for scientific research on complementary and integrative health approaches. Keep in mind that many integrative health and complementary techniques have not been assessed because of a lack of research and funding, however, the procedures can be highly beneficial. The absence of controlled studies does not mean the absence of benefit.
- Follow NCCIH on Facebook, Twitter, Pinterest, and Instagram. These accounts are updated and managed by NCCIH and provide the latest resources on a variety of complementary health approaches.
- For information on dietary supplements, visit the NIH Office of Dietary Supplements website (https://ods.od.nih.gov/factsheets/list-all/). [Remember that many of the dietary values were initially identified as the minimum value to prevent the develop of the vitamin deficiency disease. This value may only prevent an obvious disease. It may not be the appropriate value for optimum health. Most of the data was based on healthy young Caucasian males and the values may not be accurate for women, other age groups, or genetic phenotypes and most likely need to be significantly higher.]
Finding Health Information on Social Media
Credible sources of health information may be found on some social media websites. One suggestion by Kington et al., (2021) is to apply the ‘CRAP’ test developed originally by librarian Molly Beestrum at Northwestern University using four major considerations labeled: “Currency/Credibility, Reliability, Authority, and Purpose/Point of View.” Also, consider the following:
- Check the sponsor’s website. Health information on social networking sites is often very brief. For more information, go to the sponsoring organization’s website. On Twitter, look for a link to the website in the header; on Facebook, look in the About section.
- Verify that social media accounts are what they claim to be. Some social networking sites have a symbol that an account has been verified. For example, Twitter uses a blue badge but people now pay fee for this badge. Is it really verified or only demonstrates that the person paid a fee. Use the link from the organization’s official website to go to its social networking sites.
Finding Health Information on Mobile Health Apps
The National Academy of Medicine (NAM, 2023) builds on the Kington et al. (2021) article about identifying credible sources of health information. Some of the reminders suggested in the NAM website (cf. https://nam.edu/identifying-credible-sources-of-health-information-in-social-media-principles-and-attributes/) are paraphrased below:
There are thousands of mobile apps (a software program you access using your phone or other mobile device) that provide health information you can read on your mobile devices. Almost 20 percent of smartphone owners had at least one health app on their phones in 2012. Keep these things in mind when using a mobile health app:
- The content of most apps is not written or reviewed by medical experts. The information could be inaccurate and unsafe. In addition, the information you enter when using an app may not be secure in terms of protecting personal or private health information (PHI) . [Even if the content is written by medical experts, remember they most likely got paid for it or received university grants from these companies.]
- There is little research on the benefits, risks, and the impact of apps as a source of health information. For example, the ketogenic diet has been found to improve certain medical conditions such as intractable epilepsy. However, for individuals who tend to put weight on easily with a high fat diet, the sudden versus gradual use of a ketogenic diet may be potentially harmful and could shorten lifespan.
- How secure is the technology?It’s not always easy to know what personal information on an app will accessed by third parties or how personal information will be stored or transferred in an unsecure manner.
- Consider the source. Before you download an app, find out if the store you get the app from says who created it. Don’t trust the app if contact or website information for the creator isn’t available. Health apps created by Government agencies can be found by visiting: Centers for Disease Control and Prevention.
- What is the site’s policy about linking to other sites? Some sites don’t link to any other sites, some link to any site that asks or pays for a link, and others link only to sites that meet certain criteria. You may be able to find information on the site about its linking policy. (For example, NCCIH’s linking policy is available on the NCCIH Website Information and Policies page.) Unless the site’s linking policy is strict, don’t assume that the sites that it links to are reliable. You should evaluate the linked sites just as you would any other site that you’re visiting for the first time.
- How does the site collect and handle personal information? Today, most websites track what pages you’re looking at. They may also ask you to “subscribe” or “become a member.” Any credible site collecting this kind of information should tell you exactly what it will and won’t do with your information.
- Will they sell your data? Many commercial sites sell aggregated data about their users’ demographics to other companies (for example, information such as the percentage of their users that are men over 40 or under 25). In some cases, they may collect and reuse information that’s “personally identifiable,” such as your ZIP Code, gender, and birth date. Read any privacy policy or similar language on the site, and don’t sign up for anything you don’t fully understand. You can find NICCIH’s privacy policy on the NCCIH website.
- Is the site encrypted? See if the address (URL) for the site starts with “https://” instead of “http://.” Sites that use HTTPS (Secure Hyper Text Transfer Protocol) are encrypted, less likely to be hacked, and more likely to protect your privacy.
- Can you communicate with the owner of the website? You should always be able to contact the site owner if you run across problems or have questions or feedback. If the site hosts online discussion forums or message boards, the site should explain the terms of use.
Are You Reading News or Advertising?
The Federal Trade Commission (FTC) has warned the public about fake online news sites. The site may look real, but is actually an advertisement. The site may use the logos of legitimate news organizations or similar names and web addresses. To get you to sign up for whatever they’re selling, they may describe an “investigation” into the effectiveness of the product. But everything is fake: there is no reporter, no news organization, and no investigation. Only the links to a sales site are real. Fake news sites have promoted questionable products, including weight loss products, work-at-home opportunities, and debt reduction plans. You should suspect that a news site may be fake if it:
- Endorses a product. Real news organizations generally don’t do this.
- Only quotes people who say good things about the product (includes only positive reader comments, and you can’t add a comment of your own).
- Presents research findings that seem too good to be true. (If something seems too good to be true, it usually is too good to be true.)
- Contains links to a sales site.
Use common sense and incorporate an Evolutionary Perspective in making decisions
To make sense of the flood of information use critical thinking and ask yourself whether the claims make sense in context of human evolution. Over millions of years of evolution, nature has “performed” ongoing experiments through natural selection to improve reproductive fitness. As (Talib, 2014) stated, “It [is] an insult to Mother Nature to override her programmed reactions unless we [have] a good reason to do so, backed by proper empirical testing to show that we humans can do better; the burden of evidence falls on us humans.”

Source: https://www.publicdomainpictures.net/pictures/130000/velka/darwin-evolution.jpg
How can we improve health with some simple procedures or drugs when nature has experimented for millions of years. Adapt the rules to maintain health as described by Talib (2014) in the book, Antifragile: Things That Gain from Disorder (2014), summarized with the following points:
- Anything that was not part of our evolutionary past should be viewed with healthy skepticism. There is a good possibility that it is harmful, because there has not been sufficient time for humanity to adapt genetically to the new variation. For example, the addition of altered trans fats to commercially available foods, which are not recognized by the human immune system and a result, can promote inflammation, cardiovascular disease, and cancer.
- We do not need evidence of harm to claim that a drug or an unnatural procedure involves potential risk. Take a cautionary approach with a healthy dose of skepticism. If possible then wait until more evidence is discovered. If evidence of harm does not exist, that does not mean harm does not exist.
- Only resort to medical techniques when the health payoff is very large (i.e., to save a life). Does the intervention exceed its potential harm, in cases such as emergency surgery or a lifesaving medicine (e.g., penicillin).
Take charge of your health—talk with your health care providers about any complementary health approaches you use. Together, you can make shared, well-informed decisions.
Key Background Source material for the NCCIH (2023) article, “Finding and Evaluating Online Resources“
- Albrecht, U.V., Von Jan, U., & Praman, O..(2013). Standard reporting for medical apps. Studies in Health Technology and Informatics. 190, 201-203. https://pubmed.ncbi.nlm.nih.gov/23823422/
- Office of Dietary Supplements. How to Evaluate Health Information on the Internet: Questions and Answers. Office of Dietary Supplements website. Accessed July 10, 2023 https://ods.od.nih.gov/HealthInformation/How_To_Evaluate_Health_Information_on_the_Internet_Questions_and_Answers.aspx
- Plaza, I, Demarzo, M.M., Herrera-Mercadal, P., et al. (2013). Mindfulness-based mobile applications: literature review and analysis of current features. JMIR mHealth and uHealth, 1(2), e24. https://doi.org/10.2196/mhealth.2733
- Subhi, Y., Bube, S.H., Rolskov Bojsen, S., et al. (2015). Expert involvement and adherence to medical evidence in medical mobile phone apps: a systematic review. JMIR mHealth and uHealth, 3(3),e79. https://doi.org/10.2196/mhealth.4169
Recommended sources for the NIH (2023) article, “Finding and Evaluating Online Resources“
- Boulos, M.N., Brewer, A.C., Karimkhani, C., et al. (2014). Mobile medical and health apps: state of the art, concerns, regulatory control and certification. Online Journal of Public Health Informatics, 5(3), 229. https://doi.org/10.5210/ojphi.v5i3.4814. eCollection 2014
- Buying health products and services online. Federal Trade Commission website. Accessed July 10, 2023 https://consumer.ftc.gov/articles/0023-buying-health-products-services-online
- Carissoli, C., Villani, D., & Riva. G. (2015). Does a meditation protocol supported by a mobile application help people reduce stress? Suggestions from a controlled pragmatic trial. Cyberpsychology, Behavior and Social Networking, 8(1), :46-53. https://doi.org/10.1089/cyber.2014.0062
- Comprar productos y servicios para la salud en internet. Federal Trade Commission website. Accessed July 10, 2023 https://consumidor.ftc.gov/articulos/s0023-comprar-productos-y-servicios-para-la-salud-en-internet
- How to Spot Fake Online Reviews. Consumer Reports website. Accessed July 10, 2023. https://www.consumerreports.org/money/customer-reviews-ratings/how-to-spot-fake-online-reviews-a1345282053/
- Find quality resources. HealthIT.gov website. Accessed July 10, 2023. https://www.healthit.gov/topic/health-it-resources
- Mani, M., Kavanagh, D.J., Hides, L., et al. (2015). Review and evaluation of mindfulness-based iPhone apps. JMIR mHealth and uHealth, I(3), e82. https://doi.org/10.2196/mhealth.4328
- Marcano Belisario, J.S., Huckvale, K., Greenfield, G., et al. (2016). Smartphone and tablet self management apps for asthma. Cochrane Database of Systematic Reviews. (11) :CD010013. https://doi.org/10.1002/14651858.CD010013.pub2
- Martínez-Pérez, B., de la Torre-Díez, I., & López-Coronado, M. (2015). Privacy and security in mobile health apps: a review and recommendations. Journal of Medical Systems, 39(1), 181. https://doi.org/10.1007/s10916-014-0181-3
- Wallace, L.S. & Dhingra, L.K. (2014). A systematic review of smartphone applications for chronic pain available for download in the United States. Journal of Opioid Management, 10(1), 63-68. https://doi.org/10.5055/jom.2014.0193
References
- AAM (2020). 2020 Report: Generic Drug and Biosimilars Access and Savings in the U.S.,” Association for Accessible Medicines, last accessed March 3, 2023,
https://accessiblemeds.org/2020-Access-Savings-Report - Angell, M. (2009). Drug companies & doctors: A story of corruption. The New York Review of Books, 56(1), 8-12. http://www.nybooks.com/articles/2009/01/15/drug-companies-doctorsa-story-of-corruption/
- Arciero, V., Delos Santos, S., Koshy, L., et al. (2021). Assessment of Food and Drug Administration– and European Medicines Agency–Approved Systemic Oncology Therapies and Clinically Meaningful Improvements in Quality of Life: A Systematic Review. JAMA Netw Open, 4(2):e2033004. https://doi.org/10.1001/jamanetworkopen.2020.33004
- Benbrook, C.M. (2016). Trends in glyphosate herbicide use in the United States and globally. Environ Sci Eur, 28(3). https://doi.org/10.1186/s12302-016-0070-0
- Bishop, T.F., Federman, A.D., Ross, J.S. (2010). Laboratory test ordering at physician offices with and without on-site laboratories. J Gen Intern Med.25(10, 1057-63. https://doi.org/10.1007/s11606-010-1409-7
- Bruening, Z. L. (2019). Profits over People: Flaws in Regulating the Pharmaceutical Industry and Controlled Substances (Doctoral dissertation, Utica College). https://www.proquest.com/openview/ae5178804f2e7a86bd2cf0db62ee2854/1?pq-origsite=gscholar&cbl=18750&diss=y
- Cassidy, J. (2020). How Boeing and the F.A.A. Created the 737 MAX Catastrophe, The New Yorker, September 17, 2020. https://www.newyorker.com/news/our-columnists/how-boeing-and-the-faa-created-the-737-max-catastrophe
- CDC Center for Disease Control and Prevention (May11, 2022). U.S. Overdose Deaths In 2021 Increased Half as Much as in 2020 – But Are Still Up 15%, last accessed 12/12/2022. https://www.cdc.gov/nchs/pressroom/nchs_press_releases/2022/202205.htm
- Chan, A.W. (1986). Racial differences in alcohol sensitivity. Alcohol Alcohol. 21(1), 93-104. https://pubmed.ncbi.nlm.nih.gov/2937417/
- Chandler, P.D., Chen, W.Y., Ajala, O.N., et al. (2020). Effect of Vitamin D3 Supplements on Development of Advanced Cancer: A Secondary Analysis of the VITAL Randomized Clinical Trial. JAMA Netw Open, 3(11):e2025850. https://doi.org/10.1001/jamanetworkopen.2020.25850
- Cohen, J. (1988). Statistical power analysis for the behavioral sciences. 2nd ed. New York: Routledge. https://doi.org/10.4324/9780203771587
- Crescenzi-Lanna, L., Valente, R., Cataldi, S., & Martire, F. (2023). Predictors of young people’s anti-vaccine attitudes in the context of the COVID-19 pandemic. Public Understanding of Science, 09636625231179830. https://doi.org/10.1177/09636625231179830
- Faria, J. (2023). Pharama DTC ad spend in the U.S. 2012-2021. Statista, last accessed March 2, 2023. https://www.statista.com/statistics/686906/pharma-ad-spend-usa/#:~:text=The%20pharmaceutical%20industry%20in%20the,invested%20into%20big%20pharma%20ads.
- Hill, J. A., Agewall, S., Baranchuk, A., Booz, G. W., Borer, J. S., Camici, P. G., … & Vrints, C. (2019). Medical misinformation: Vet the message!. Journal of the American Heart Association, 8(3), e011838. https://doi.org/10.1161/JAHA.118.011838
- Horton, R. (2015). Offline: What is medicine’s 5 sigma? The Lancet, 385(9976), 1380.
https://doi.org/10.1016/S0140-6736(15)60696-1 - Kington, R. S., Arnesen, S., Chou, W. Y. S., Curry, S. J., Lazer, D., & Villarruel, A. M. (2021). Identifying credible sources of health information in social media: Principles and attributes. NAM perspectives, 2021. https://doi.org/10.31478/202107a
- Koinig, I., & Kohler, S. (2021). On the Relationship Between Skepticism Towards and Reactance to Health Messages: The Special Case of Online Communication on Tick-Borne Encephalitis. Frontiers in Communication, 6, 170. https://doi.org/10.3389/fcomm.2021.737800
- Lupton, Thomas (1580). Siuqila too good, to be true : omen : though so at a vewe yet all I tolde you is true, I vpholde you, now cease to aske why? for I can not lye : herein is shewed by way of dialogue, the wonderful maners of the people of Mauqsun, with other talke not friuolous. Printed at London: By H. Bynneman, dwelling in Thames Streate, neere vnto Baynards Castell, 1580. https://www.amazon.com/Siuqila-too-good-true-vpholde/dp/1171274114
- Maravelias, C., Dona, A., Stefanidou, M., & Spiliopoulou, C. (2005). Adverse effects of anabolic steroids in athletes: A constant threat. Toxicology Letters, 158(3), 167-175. https://doi.org/10.1016/j.toxlet.2005.06.005
- McReynolds, T. (2020). CDC: An about face on face masks? Last accessed February 22, 2023. https://www.aaha.org/publications/newstat/articles/2020-03/cdc-an-about-face-on-face-masks/
- Mcvan, M. (2022), In Washington, agricultural policymakers circulate among Farm Bureau, USDA and industry. Missouri Independent, September 6, 2022. https://missouriindependent.com/category/energy-environment/
- Mendes, D., Alves, C., & Batel-Marques, F. (2017). Number needed to treat (NNT) in clinical literature: an appraisal. BMC Med, 15(1), 112. https://doi.org/10.1186/s12916-017-0875-8
- Moore, T.J., Heyward, J., Anderson, G., & Alexander, G.C. (2020). Variation in the estimated costs of pivotal clinical benefit trials supporting the US approval of new therapeutic agents, 2015-2017: a cross-sectional study. BMJ Open. Jun 11;10(6):e038863. https://doi.org/10.1136/bmjopen-2020-038863
- National Academy of Medicine, Identifying Credible Sources of Health Information, last accessed July 5, 2023. https://nam.edu/identifying-credible-sources-of-health-information-in-social-media-principles-and-attributes/
- NCCIH (2023). National Center for Complementary and Integrative Health. Finding and Evaluating Online Resources, Last accessed February 22, 2023. https://www.nccih.nih.gov/health/finding-and-evaluating-online-resources?nav=govd
- Patel, N.G., Hwang , T.J., Woloshin, S., & Kesselheim, A.S. (2023). Therapeutic Value of Drugs Frequently Marketed Using Direct-to-Consumer Television Advertising, 2015 to 2021. JAMA Netw Open, 6(1):e2250991. https://doi.org/10.1001/jamanetworkopen.2022.50991
- Peper, E. & Harvey, R. (2017). The fallacy of the placebo controlled clinical trials: Are positive outcomes the result indirect treatment side effects? NeuroRegulation. 4(3–4,102–113.https://doi.org/10.15540/nr.4.3-4.102
- Perrier, E. T., Armstrong, L. E., Bottin, J. H., Clark, W. F., Dolci, A., Guelinckx, I., … & Péronnet, F. (2021). Hydration for health hypothesis: a narrative review of supporting evidence. European journal of nutrition, 60(3), 1167-1180. https://doi.org/10.1007/s00394-020-02296-z
- Puigbò, P., Leino, L. I., Rainio, M. J., Saikkonen, K., Saloniemi, I., & Helander, M. (2022). Does Glyphosate Affect the Human Microbiota?. Life, 12(5), 707. https://doi.org/10.3390/life12050707
- Putois, O., & Helms, J. (2022). The Role of Denial in Vaccine Skeptics and “Anti-vax” Blame: A Psychodynamic Approach. Frontiers in Psychology, 13, 886368. https://doi.org/10.3389/fpsyg.2022.886368
- Rossignol, M., Labrecque, M., Cauchon, M., Breton, M., & Poirier, P. (2018). Number of patients needed to prescribe statins in primary cardiovascular prevention: mirage and reality, Family Practice, 35(4), 376-382. https://doi.org/10.1093/fampra/cmx124
- Shaw, S. (2023 February 18). The case for free-range lab mice. The New Yorker. Last accessed March 1, 2023. https://www.newyorker.com/culture/annals-of-inquiry/the-case-for-free-range-lab-mice
- Talib, N. N. (2014). Antifragile: Things That Gain from Disorder (Incerto). New York: Random House. https://www.amazon.com/Antifragile-Things-That-Disorder-Incerto/dp/0812979680#:~:text=Antifragile%20is%20a%20standalone%20book,world%20we%20don’t%20understand.
- Tano, B. The Layman’s Guide to Integrative Immunity. Integrative Medical Press; 2016. https://www.amazon.com/Laymans-Guide-Integrative-Immunity-Discover/dp/0983419299
- Tantibanchachai, C, & Yang, J. (2019). Studies of thalidomide’s effects on rodent embryos from 1962-2008. The Embryo Project Encyclopedia. https://embryo.asu.edu/pages/studies-thalidomides-effects-rodent-embryos-1962-2008
- Westreich, D. (2012). Berkson’s bias, selection bias, and missing data. Epidemiology (Cambridge, Mass.), 23(1), 159. https://doi.org/10.1097/EDE.0b013e31823b6296
- Wilhelmi, O. & Hayden, M. (2016). Reducing vulnerability to extreme heat through interdisciplinary research and stakeholder engagement. In Extreme Weather, Health, and Communities (pp. 165-186). Springer, Cham. https://convergence.unc.edu/wp-content/uploads/sites/381/2017/03/wilhelmi-hayden_2016_reducing-vuln-to-extreme-heat-interdiscip-research-stakeholder-engagement.pdf
- Wouters, O. J., McKee, M., & Luyten, J. (2020). Estimated Research and Development Investment Needed to Bring a New Medicine to Market, 2009-2018. JAMA, 323(9), 844-853. https://doi.org/10.1001/jama.2020.1166
- Yucha, C. B. (2002). Problems inherent in assessing biofeedback efficacy studies. Applied psychophysiology and biofeedback, 27(1), 99-106. https://doi.org/10.1023/a:1014528622061
- Yucha, C., & Montgomery, D. (2008). Evidence-based practice in biofeedback and neurofeedback. Wheat Ridge, CO: AAPB. https://www.advantagehcs.com/wp-content/uploads/2018/11/EvidenceBasedYuchaMontgomeryW.pdf
[i]This is a measure of size of the association as measured by as statistic such as Cohen’ d; namely, if it is small–although statistically significant– it probably would not be clinically meaningful. Cohen (1988) suggested a ”d” statistic (e.g. Cohen’s d) comparing the group differences (e.g. treatment group vs. comparison group change scores; [M2 – M1]) divided by the standard deviation of both groups [square root of SD1+SD2]/2], interpreting moderate effects between 0.50 and 0.79 and larger effects above 0.80. Treatment group vs comparison group effects are also estimated by examining percentages. Relative risk ratio or odds ratio is a single number that reflects the increased or decreased risk. For example, a doubled risk would be expressed as a relative risk of 2. Risk decreased by 50% would be expressed as RR 0.5. This number is calculated as the percent of people with clinically meaningful outcomes divided by percent of people without clinically meaningful outcomes. This provides a ‘relative’ estimate of effectiveness, where a ratio close to 1 indicates no difference between treatment and comparison groups, and ratios greater than 3 to 1 (e.g. treatment group was twice as effective as comparison group) are considered moderate effects and 4 to 1 are considered larger effects.
About the Authors
Erik Peper’s teaching and research focuses on self-healing strategies, illness prevention, the effects of posture and respiration, and how to use biofeedback and wearable devices. Each year he mentors undergraduate student researchers to create and complete studies that are presented at scientific meetings. He is an international authority on biofeedback and self-regulation and author of scientific articles and books such as Make Health Happen, Fighting Cancer-A Nontoxic Approach to Treatment, and Biofeedback Mastery. His most recent co-authored book is, TechStress: How Technology is Hijacking Our Lives, Strategies for Coping, and Pragmatic Ergonomics. He publishes the blog, The Peper Perspective–ideas on illness, health and well-being (peperperspective.com). In 2013 was received the Biofeedback Distinguished Scientist Award in recognition of outstanding career & scientific contributions from the Association for Applied Psychophysiology.
Richard Harvey has a Ph.D. for the UC Irvine Social Ecology program. His research includes developing stress-reduction interventions which promote psychological courage and hardiness. Before teaching at SF State, he was a research fellow at the UC Irvine Transdisciplinary Tobacco Use Research Center for five years, developed and ran the UC Irvine Counseling Center Biofeedback and Stress Management Program, and worked as a Maternal, Child and Adolescent Health Research Analyst in Orange County. He is the co-chair of the American Public Health Association, Alternative and Complementary Health Practices Special Interest Group, as well as a board member of the Biofeedback Society of California and the San Francisco Psychological Association. He has published in the areas of biofeedback, stress and computer-related disorders, tobacco cessation, and the psychology of hardiness and courage.
Copyright © 2023 Townsend Letter
TechStress: Building Healthier Computer Habits
Posted: August 30, 2023 Filed under: ADHD, behavior, biofeedback, Breathing/respiration, cognitive behavior therapy, computer, digital devices, education, emotions, ergonomics, Evolutionary perspective, Exercise/movement, health, laptops, Neck and shoulder discomfort, Pain/discomfort, posture, screen fatigue, stress management, Uncategorized, vision, zoom fatigue | Tags: cellphone, fatigue, gaming, mobile devices, screens 5 CommentsBy Erik Peper, PhD, BCB, Richard Harvey, PhD, and Nancy Faass, MSW, MPH
Adapted by the Well Being Journal, 32(4), 30-35. from the book, TechStress: How Technology is Hijacking Our Lives, Strategies for Coping, and Pragmatic Ergonomics by Erik Peper, Richard Harvey, and Nancy Faass.

Every year, millions of office workers in the United States develop occupational injuries from poor computer habits—from carpal tunnel syndrome and tension headaches to repetitive strain injury, such as “mouse shoulder.” You’d think that an office job would be safer than factory work, but the truth is that many of these conditions are associated with a deskbound workstyle.
Back problems are not simply an issue for workers doing physical labor. Currently, the people at greatest risk of injury are those with a desk job earning over $70,000 annually. Globally, computer-related disorders continue to be on the rise. These conditions can affect people of all ages who spend long hours at a computer and digital devices.
In a large survey of high school students, eighty-five percent experienced tension or pain in their neck, shoulders, back, or wrists after working at the computer. We’re just not designed to sit at a computer all day.
Field of Ergonomics
For the past twenty years, teams of researchers all over the world have been evaluating workplace stress and computer injuries—and how to prevent them. As researchers in the fields of holistic health and ergonomics, we observe how people interact with technology. What makes our work unique is that we assess employees not only by interviewing them and observing behaviors, but also by monitoring physical responses.
Specifically, we measure muscle tension and breathing, in the moment, in real-time, while they work. To record shoulder pain, for example, we place small sensors over different muscles and painlessly measure the muscle tension using an EMG (electromyograph)—a device that is employed by physicians, physical therapists, and researchers. Using this device, we can also keep a record of their responses and compare their reactions over time to determine progress.
What we’ve learned is that people get into trouble if their muscles are held in tension for too long. Working at a computer, especially at a stationary desk, most people maintain low-level chronic tension for much of the day. Shallow, rapid breathing is also typical of fine motor tasks that require concentration, like data entry.
Muscle tension and breathing rate usually increase during data entry or typing without our awareness.
When these patterns are paired with psychological pressure due to office politics or job insecurity, the level of tension and the risk of fatigue, inflammation, pain, or injury increase. In most cases, people are totally unaware of the role that tension plays in injury. Of note, the absolute level of tension does not predict injury—rather, it is the absence of periodic rest breaks throughout the day that seems to correlate with future injuries.
Restbreaks
All of life is the alternation between movement and rest, inhaling and exhaling, sleeping and waking. Performing alternating tasks or different types of activities and movement is one way to interrupt the couch potato syndrome—honoring our evolutionary background.
Our research has confirmed what others have observed: that it’s important to be physically active, at least periodically, throughout the day. Alternating activity and rest recreate the pattern of our ancestors’ daily lives. When we alternate sedentary tasks with physical activity, and follow work with relaxation, we function much more efficiently. In short, move your body more.
Better Computer Habits: Alternate Periods of Rest and Activity
As mentioned earlier, our workstyle puts us out of sync with our genetic heritage. Whether hunting and gathering or building and harvesting, our ancestors alternated periods of inactivity with physical tasks that required walking, running, jumping, climbing, digging, lifting, and carrying, to name a few activities. In contrast, today many of us have a workstyle that is so immobile we may not even leave our desk for lunch.
As health researchers, we have had the chance to study workstyles all over the world. Back pain and strain injuries now affect a large proportion of office workers in the US and in high-tech firms worldwide. The vast majority of these jobs are sedentary, so one focus of the research is on how to achieve a more balanced way of working.
A recent study on exercise looked at blood flow to the brain. Researchers Carter and colleagues found that if people sit for four hours on the job, there’s a significant decrease in blood flow to the brain. However, if every thirty or forty minutes they get up and move around for just two minutes, then brain blood flow remains steady. The more often you interrupt sitting with movement, the better.
It may seem obvious that to stay healthy, it’s important to take breaks and be physically active from time to time throughout the day. Alternating activity and rest recreate the pattern of our ancestors’ daily lives. The goal is to alternate sedentary tasks with physical activity and follow work with relaxation. When we keep this type of balance going, most people find that they have more energy, are more productive, and can be more effective.
Genetics: We’re Hardwired Like Ancient Hunters

Despite a modern appearance, we carry the genes of our forebearers—for better and for worse. (Art courtesy of Peter Sis). Reproduced from Peper, E., Harvey, R., & Faass (2020). TechStress: How Technology is Hijacking Our Lives, Strategies for Coping, and Pragmatic Ergonomics. Berkeley: North Atlantic Books.
In the modern workplace, most of us find ourselves working indoors, in small office spaces, often sitting at a computer for hours at a time. In fact, the average Westerner spends more than nine hours per day sitting indoors, yet we’re still genetically programmed to be physically active and spend time outside in the sunlight most of the day, like the nomadic hunters and gatherers of forty thousand years ago.
Undeniably, we inherently conserve energy in order to heal and regenerate. This aspect of our genetic makeup also helps burn fewer calories when food is scarce. Hence the propensity for lack of movement and sedentary lifestyle (sitting disease).
In times of famine, the habit of sitting was essential because it reduced calorie expenditure, so it enabled our ancestors to survive. In a prehistoric world with a limited food supply, less movement meant fewer calories burned. Early humans became active when they needed to search for food or shelter. Today, in a world where food and shelter are abundant for most Westerners, there is no intrinsic drive to initiate movement.
It is also true that we have survived as a species by staying active. Chronic sitting is the opposite of our evolutionary pattern in which our ancestors alternated frequent movement while hunting or gathering food with periods of rest. Whether they were hunters or farmers, movement has always been an integral aspect of daily life. In contrast, working at the computer—maintaining static posture for hours on end—can increase fatigue, muscle tension, back strain, and poor circulation, putting us at risk of injury.
Quit a Sedentary Workstyle
Almost everyone is surprised by how quickly tension can build up in a muscle, and how painful it can become. For example, we tend to hover our hands over the keyboard without providing a chance for them to relax. Similarly, we may tighten some of the big muscles of our body, such as bracing or crossing our legs.
What’s needed is a chance to move a little every few minutes—we can achieve this right where we sit by developing the habit of microbreaks. Without regular movement, our muscles can become stiff and uncomfortable. When we don’t take breaks from static muscle tension, our muscles don’t have a chance to regenerate and circulate oxygen and necessary nutrients.
Build a variety of breaks into your workday:
- Vary work tasks
- Take microbreaks (brief breaks of less than thirty seconds)
- Take one-minute stretch breaks
- Fit in a moving break
Varying Work Tasks
You can boost physical activity at work by intentionally leaving your phone on the other side of the desk, situating the printer across the room, or using a sit-stand desk for part of the day. Even a few minutes away from the desk makes a difference, whether you are hand delivering documents, taking the long way to the bathroom, or pacing the room while on a call.
When you alternate the types of tasks and movement you do, using a different set of muscles, this interrupts the contractions of muscle fibers and allows them to relax and regenerate. Try any of these strategies:
- Alternate computer work with other activities, such as offering to do a coffee run
- Schedule walking meetings with coworkers
- Vary keyboarding and hand movements
Ultimately, vary your activities and movements as much as possible. By changing your posture and making sure you move, you’ll find that your circulation and your energy improve, and you’ll experience fewer aches and pains. In a short time, it usually becomes second nature to vary your activities throughout the day.
Experience It: “Mouse Shoulder” Test
You can test this simple mousing exercise at the computer or as a simulation. If you’re at the computer, sit erect with your hand on the mouse next to the keyboard. To simulate the exercise, sit with erect posture as if you were in front of your computer and hold a small object you can use to imitate mousing.
With the mouse (or a sham mouse), simulate drawing the letters of your name and your street address, right to left. Be sure each letter is very small (less than half an inch in height). After drawing each letter, click the mouse.
As part of the exercise, draw the letters and numbers as quickly as possible for ten to fifteen seconds. What did you observe? In almost all cases, you may note that you tightened your mousing shoulder and your neck, stiffened your trunk, and held your breath. All this occurred without awareness while performing the task. Over time, this type of muscle tension can contribute to discomfort, soreness, pain, or eventual injury.
Microbreaks
If you’ve developed an injury—or have chronic aches and pains—you’ll probably find split-second microbreaks invaluable. A microbreak means taking brief periods of time that last just a few seconds to relax the tension in your wrists, shoulders, and neck.
For example, when typing, simply letting your wrists drop to your lap for a few seconds will allow the circulation to return fully to help regenerate the muscles. The goal is to develop a habit that is part of your routine and becomes automatic, like driving a car. To make the habit of microbreaks practical, think about how you can build the breaks into your workstyle. That could mean a brief pause after you’ve completed a task, entered a column of data, or before starting typing out an assignment.
For frequent microbreaks, you don’t even need to get up—just drop your hands in your lap or shake them out, move your shoulders, and then resume work. Any type of shaking or wiggling movement is good for your circulation and kind of fun.
In general, a microbreak may be defined as lasting one to thirty seconds. A minibreak may last roughly thirty seconds to a few minutes, and longer large-movement breaks are usually greater than a few minutes. Popular microbreaks:
- Take a few deep breaths
- Pause to take a sip of water
- Rest your hands in your lap
- Stretch
- Let your arms drop to your sides
- Shake out your hands (wrists and fingers)
- Perform a quick shoulder or neck roll
Often, we don’t realize how much tension we’ve been carrying until we become more mindful of it. We can raise our awareness of excess tension—this is a learned skill—and train ourselves to let go of excess muscle tension. As we increase our awareness, we’re able to develop a new, more dynamic workstyle that better fits our goals and schedule.
One-Minute Stretch Breaks

We all benefit from a brief break, even with the best of posture (left). One approach is to totally release your muscles (middle). That release can be paired with a series of brief stretches (right). Reproduced from Peper, E., Harvey, R., & Faass (2020). TechStress: How Technology is Hijacking Our Lives, Strategies for Coping, and Pragmatic Ergonomics. Berkeley: North Atlantic Books.
The typical mini-stretch break lasts from thirty seconds to a few minutes, and ideally you want to take them several times per hour. Similar to microbreaks, mini-stretch breaks are especially important for people with an injury or those at risk of injury. Taking breaks is vital, especially if you have symptoms related to computer stress or whenever you’re working long hours at a sedentary job. To take a stretch break:
Begin with a big stretch, for example, by reaching high over your head then drop your hands in your lap or to your sides.
Look away from the monitor, staring at near and far objects, and blink several times. Straighten your back and stretch your entire backbone by lifting your head and neck gently, as if there were an invisible string attached to the crown of your head.
Stretch your mind and body. Sitting with your back straight and both feet flat on the floor, close your eyes and listen to the sounds around you, including the fan on the computer, footsteps in the hallway, or the sounds in the street.
Breathe in and out over ten seconds (breathe in for four or five seconds and breathe out for five or six seconds), making the exhale slightly longer than the inhale. Feel your jaw, mouth, and tongue muscles relax. Feel the back and bottom of the chair as your body breathes all around you. Envision someone in your mind’s eye who is kind and reassuring, who makes you feel safe and loved, and who can bring a smile to your face inwardly or outwardly.
Do a wiggling movement. When you take a one-minute break, wiggling exercises are fast and easy, and especially good for muscle tension or wrist pain. Wiggle all over—it feels good, and it’s also a great way to improve circulation.
Building Exercise and Movement into Every Day
Studies show that you get more benefit from exercising ten to twenty minutes, three times a day, than from exercising for thirty to sixty minutes once a day. The implication is that doing physical activities for even a few minutes can make a big difference.
Dunstan and colleagues have found that standing up three times an hour and then walking for just two minutes reduced blood sugar and insulin spikes by twenty-five percent.Fit in a Moving Break
Fit in a Moving Break
Once we become conscious of muscle tension, we may be able to reverse it simply by stepping away from the desk for a few minutes, and also by taking brief breaks more often. Explore ways to walk in the morning, during lunch break, or right after work. Ideally, you also want to get up and move around for about five minutes every hour.
Ultimately, research makes it clear that intermittent movement, such as brief, frequent stretching throughout the day or using the stairs rather than elevator, is more beneficial than cramming in a couple of hours at the gym on the weekend. This explains why small changes can have a big impact—it’s simply a matter of reminding yourself that it’s worth the effort.
Workstation Tips
Your ability to see the display and read the screen is key to reducing neck and eye strain. Here are a few strategic factors to remember:
Monitor height: Adjust the height of your monitor so the top is at eyebrow level, so you can look straight ahead at the screen.
Keyboard height: The keyboard height should be set so that your upper arms hang straight down while your elbows are bent at a 90-degree angle (like the letter L) with your forearms and wrists held horizontally.
Typeface and font size: For email, word processing, or web content, consider using a sans serif typeface. Fonts that have fewer curved lines and flourishes (serifs) tend to be more readable on screen.
Checking your vision: Many adults benefit from computer glasses to see the screen more clearly. Generally, we do not recommend reading glasses, bifocals, trifocals, and progressive lenses as they tend to allow clear vision at only one focal length. To see through the near-distance correction of the lens requires you to tilt your head back. Although progressive lenses allow you to see both close up and at a distance, the segment of the lens for each focal length is usually too narrow for working at the computer.
Wearing progressive lenses requires you to hold your head in a fixed position to be in focus. Yet you may be totally unaware that you are adapting your eye and head movements to sustain your focus. When that is the case, most people find that special computer glasses are a good solution.
Consider computer glasses if you must either bring your nose to the screen to read the text, wear reading glasses and find that their focal length is inappropriate for the monitor distance, wear bi- or trifocal glasses, or are older than forty.
Computer glasses correct for the appropriate focal distance to the computer. Typically, monitor distance is about twenty-three to twenty-eight inches, whereas reading glasses correct for a focal length of about fifteen inches. To determine your individual, specific focal length, ask a coworker to measure the distance from the monitor to your eyes. Provide this personal focal distance at the eye exam with your optometrist or ophthalmologist and request that your computer glasses be optimized for that distance.
Remembering to blink: As we focus on the screen, our blinking rate is significantly reduced. Develop the habit of blinking periodically: at the end of a paragraph, for example, or when sending an email.
Resting your eyes: Throughout the day, pause and focus on the far distance to relax your eyes. When looking at the screen, your eyes converge, which can cause eyestrain. Each time you look away and refocus, that allows your eyes to relax. It’s especially soothing to look at green objects such as a tree that can be seen through a window.
Minimizing glare: If the room is lit with artificial light, there may be glare from your light source if the light is right in front of you or right behind you, causing reflection on your screen. Reflection problems are minimized when light sources are at a 90-degree angle to the monitor (with the light coming from the side). The worst situations occur when the light source is either behind or in front of you.
An easy test is to turn off your monitor and look for reflections on the screen. Everything that you see on the monitor when it’s turned off is there when you’re working at the monitor. If there are bright reflections, they will interfere with your vision. Once you’ve identified the source of the glare, change the location of the reflected objects or light sources, or change the location of the monitor.
Contrast: Adjust the light contrast in the room so that it is neither too bright nor too dark. If the room is dark, turn on the lights. If it is too bright, close the blinds or turn off the lights. It is exhausting for your eyes to have to adapt from bright outdoor light to the lighting of your computer screen. You want the light intensity of the screen to be somewhat similar to that in the room where you’re working. You also do not want to look from your screen to a window lit by intense sunlight.
Don’t look down at phone: According to Kenneth Hansraj, MD, chief of spine surgery at New York Spine Surgery and Rehabilitation Medicine, pressure on the spine increases from about ten pounds when you are holding your head erect, to sixty pounds of pressure when you are looking down. Bending forward to look at your phone, your head moves out of the line of gravity and is no longer balanced above your neck and spine. As the angle of the face-forward position increases, this intensifies strain on the neck muscles, nerves, and bones (the vertebrae).
The more you bend your neck, the greater the stress since the muscles must stretch farther and work harder to hold your head up against gravity. This same collapsed head-forward position when you are seated and using the phone repeats the neck and shoulder strain. Muscle strain, tension headaches, or neck pain can result from awkward posture with texting, craning over a tablet (sometimes referred to as the iPad neck), or spending long hours on a laptop.
A face-forward position puts as much as sixty pounds of pressure on the neck muscles and spine.
Repetitive strain of neck vertebrae (the cervical spine), in combination with poor posture, can trigger a neuromuscular syndrome sometimes diagnosed as thoracic outlet syndrome. According to researchers Sharan and colleagues, this syndrome can also result in chronic neck pain, depression, and anxiety.
When you notice negative changes in your mood or energy, or tension in your neck and shoulders, use that as a cue to arch your back and look upward. Think of a positive memory, take a mindful breath, wiggle, or shake out your shoulders if you’d like, and return to the task at hand.
Strengthen your core: If you find it difficult to maintain good posture, you may need to strengthen your core muscles. Fitness and sports that are beneficial for core strength include walking, sprinting, yoga, plank, swimming, and rowing. The most effective way to strengthen your core is through activities that you enjoy.
Final Thoughts
If these ideas resonate with you, consider lifestyle as the first step. We need to build dynamic physical activity into our lives, as well as the lives of our children. Being outside is usually an uplift, so choose to move your body in natural settings whenever possible, whatever form that takes. Being outside is the factor that adds an energetic dimension. Finally, share what you learn, and help others learn and grow from your experiences.
If you spend time in front of a computeror using a mobile device, read the book, TechStress: How Technology is Hijacking Our Lives, Strategies for Coping, and Pragmatic Ergonomics. It provides practical, easy-to-use solutions for combating the stress and pain many of us experience due to technology use and overuse. The book offers extremely helpful tips for ergonomic use of technology, it
goes way beyond that, offering simple suggestions for improving muscle health that seem obvious once you read them, but would not have thought of yourself: “Why didn’t I think of that?” You will learn about the connection between posture and mood, reasons for and importance of movement breaks, specific movements you can easily perform at your desk, as well as healthier ways to utilize technology in your everyday life.
See the book, TechStress-How Technology is Hijacking our Lives, Strategies for Coping and Pragmatic Ergonomics by Erik Peper, Richard Harvey and Nancy Faass. Available from: https://www.amazon.com/Beyond-Ergonomics-Prevent-Fatigue-Burnout/dp/158394768X/
Additional resources
Healing a Shoulder/Chest Injury
Posted: August 14, 2023 Filed under: behavior, biofeedback, Breathing/respiration, emotions, Exercise/movement, healing, Neck and shoulder discomfort, Pain/discomfort, relaxation, self-healing, Uncategorized | Tags: electromyograph, guided imagery, shoulder pain Leave a commentAdapted from Peper, E. & Fuhs, M. (2004). Applied psychophysiology for therapeutic use: Healing a shoulder injury, Biofeedback, 32(2), 11-18.

“It has been an occurrence of the third dimension for me! How come my pain — that lasted for more than 10 days and was still so strong that I really had difficulties in breathing, couldn’t laugh without pain nor move my arm not even to fulfil my daily routines such as dressing and eating — disappeared within one single session of 20 minutes? And not only that, I was able to freely rotate my arm as if it had never been injured before.” —23 year old woman
The participant T., aged 23, was a psychology student who participated in an educational workshop for Healthy Computing. She volunteered to be a subject for a surface electromyographic (SEMG) monitoring and feedback demonstration. Ten days prior to this workshop, she had a severe skiing accident. She described the accident as follows:
I went skiing and may be I had too much snow in my ski-binding and while turning, I slipped out of my binding and fell head first down into the hill. As I fell, I landed on my ski pole which hit my left upper chest and breast area. Afterwards, my head was humming and I assumed that I had a light concussion. I stopped skiing and stayed in bed for a while. The next day it started hurting and I couldn’t turn my head or put my shoulders back (they were rotated forward). Also, I couldn’t ski as I was not able to look down to my feet–my muscles were too contracted and I felt searing pain whenever I moved. I hoped that it would go away however, the pain and left forward shoulder rotation stayed.
Assessment
Observation and Palpation
T.´s left shoulder was rolled forward (adducted and in internal rotation). She was not able to breathe or laugh without pain or move her arm freely. All movements in vertical and horizontal directions and rotations were restricted by at least 50 % as compared to her right arm (limitations in shoulder extension, flexion and external rotation). Also, her hands were ice-cold and she breathed very shallowly and rapidly in her chest. She was not able to stand in an upright position or sit in a comfortable position without maintaining her left upper extremity in a protected position. Her left shoulder blade (scapula) was winging.
After visually observing her, the instructor placed his left hand on her left shoulder and pectoralis muscles and his right hand on the back of her shoulder. Using palpation and anchoring her back with his leg so that she could not rotate her trunk, he explored the existing range of shoulder movement. He also attempted to rotate the left shoulder outward and back–not by forcing or pulling—but by very gentle traction. No change in mobility was observed and the pectoralis muscle felt tight (SEMG monitoring is helpful to the therapist during such a diagnostic assessment by helping to identify the person’s reactivity and avoiding to evoke and condition even more bracing). T. reported afterwards that she was very scared by this assessment because there was one point in the back which was highly reactive to touch. T. appeared to tighten automatically out of fear and trigger a general flexor contraction pattern—a process that commonly occurs if a person is guarding an area.
Often a traumatic injury first induces a general shock that triggers an automatic freeze and fear reaction. Therefore, an intervention needed to be developed that did not trigger vigilance or fear and thereby allowed the muscle to relax. If pain is experienced or increased, it is another negative reinforcement for generalizing guarding and bracing and tightening the muscles. This guarding decreases mobility – a common reaction that may occur when health professionals in the process of assessment increase the client’s discomfort. T.’s vigilance was also “telegraphed” to the therapist by her ice-cold hands and very shallow chest breathing. Therefore, it was important to increase her comfort level and to not induce any further pain. We hypothesized that only if she felt safe it would be possible for her muscle tension to decrease and thereby increase her mobility.
Underlying concept: The very cold hands and shallow breathing probably indicated excessive vigilance and arousal—a possible indicator of a catabolic state that could limit regeneration. The chronic cold hands most likely implied that she was very sensitive to other people’s emotions and continuously searches/scans the environment for threats. In addition, she indicated that she liked to do/perform her best which induced more anxiety and fear of judgement.
Single Channel Surface Electromyographic (SEMG)Assessment
The triode electrode with sensor was placed over the left pectoralis muscle area as shown in Figure 1. The equipment was a MyoTrac™ produced by Thought Technology Ltd. which is a small portable SEMG with the preamplifiers at the triode sensor to eliminate electrode lead and movement artefacts (Peper & Gibney, 2006). Such a device is an inexpensive option for people who may use biofeedback for demonstrating and teaching awareness and control over muscle tension from a single electrode location.

Figure 1. Location of the Triode electrode placement on the left pectoralis muscle area of another participant.
The MyoTrac was placed on a table within view, so that the therapist and the subject could simultaneously see the visual feedback signal and observe what was going on as well as demonstrate expected changes. The feedback was used for T. as a tool to see if she could reduce her SEMG activity. It was also used by the therapist to guide his interventions: To keep the SEMG activity low and to stop any intervention that would increase the SEMG activity as this would prevent bracing as a possible reaction to, or anticipation of, pain.
1. Assessment of Muscle Reactivity. After the electrode was attached on her pectoralis muscle and with her arm resting on her lap, she was asked to roll her left shoulder slightly more forward, hold the tension for the count of 10 and then let go and relax. Even with feedback, the muscle activity stayed high and did not relax and return to a lower level of activity as shown in Figure 2. This lack of return to baseline is often a diagnostic indicator of muscle irritability or injury (Sella, 1998; Sella, 2006). If the muscle does not relax immediately after contraction, movement or exercise should not be prescribed, since it may aggravate the injury. Instead, the person first needs to learn how to relax and then learn how to relax between activation and tensing of the muscle. The general observation of T. was that at the initiation of any movement (active or passive) muscle tension increased and did not return to baseline for more than two minutes.

Figure 2. Simulation of the effect on the pectoralis sEMG (this is a recording from another subject who showed a similar response pattern that was visually observed from T. with the Myotrac). After the muscle is contracted it takes a long time to return to baseline level
2. Exploration. Self-exploration with feedback was encouraged. T. was instructed to let go of muscle tension in her left shoulder girdle. In addition the therapist tried to induce her letting go by gently and passively rocking her left arm. The increased SEMG activity and the protective bracing in her shoulder showed that she couldn’t reduce the muscle tension. Each time her arm was moved, however slightly, she helped with the movement and kept control. In addition, T. was asked to reduce the muscle tension using the biofeedback signal; again she was not able to reduce her muscle tension with feedback.
3. Passive Stretch and Movements. The next step was to passively stretch the pectoralis muscle by holding the shoulder between both hands and very gently externally rotate the shoulder — a process derived from the Alexander technique (Barlow, 1991). Each time the instructor attempted to rotate her shoulder, the SEMG increased and T. reported an increased fear of pain. T.’s SEMG response most likely consisted of the following components:
- Movement induced pain
- Increased splinting and guarding
- Increased arousal/vigilance to perform well
These three assessment and self-regulation procedures were unsuccessful in reducing muscle tension or increasing shoulder movement. This suggested that another therapeutic intervention would need to be developed to allow the left pectoralis area to relax. The SEMG could be used as an indicator whether the intervention was successful as indicated by a reduction in SEMG activity. Finally, the inability to relax after tightening (bracing and splinting) probably aggravated her discomfort.
Multiple levels of injury: The obvious injury and discomfort was due to her left chest wall being hit by the ski pole. She then guarded the area by bracing the muscles to protect it which limited movement. The guarding tightened the muscles and limited blood circulation and lymphatic flow which increased local ischemia, irritation and pain. This led to a self-perpetuating cycle: Pain triggers guarding and guarding increases pain and impedes self-healing.
As the SEMG and passive stretching assessment were performed, the therapist concurrently discussed the pain process. Namely, from this perspective, there were at least two types of pains:
- Pain caused by the physiological injury
- Pain as the result of guarding
The pain from the guarding is similar to having exercised for a long time after not having exercised. The next day you feel sore. However, if you feel sore, you know that it was due to the exercise therefore it is defined as a good pain. In T.’s case, the pain indicated that something was wrong and did not heal and therefore she would need to protect it. We discussed this process as a way to use cognitive reframing to change her attitude toward guarding and pain.
Rationale: The intention was to interrupt her negative image of pain that acted as a post hypnotic suggestion. The objective was to change her image and thoughts from “pain indicates the muscle is damaged” to “pain indicates the muscle has worked too hard and long and needs time to regenerate.”
Treatment interventions
The initial intervention focused upon shifting shallow thoracic breathing to diaphragmatic breathing. Generally, when people breathe rapidly and predominantly in their chest, they usually tighten their neck and shoulder muscles during inhalation. One of the reasons T. breathed in her chest was that her clothing–very tight jeans–constricted her waist (MacHose & Peper, 1991; Peper et al., 2015). This breathing pattern probably contributed to sub-clinical hyperventilation and was part of a fear or flexor response pattern. When she loosened the upper buttons of her jeans and allowed her stomach to expand her pectoralis muscle relaxed as she breathed as shown in Figure 3. As she began to breathe in this pattern, each time she exhaled her pectoralis muscle tension decreased.

Figure 3. Illustration of the effect of loosening tight waist constriction (eliminating designer’s jean syndrome) on blood flow and pectoralis sEMG. Abdominal breathing became possible and finger temerature increased (this recording is from another subject whose physiological responses were similar to that was observed with the Myotrac from T.)
Following the demonstration that breathing significantly lowered her chest muscle tension, the discussion focussed on the importance of effortless diaphragmatic breathing for health and reduction of vigilance. Being awkward and uncomfortable at loosening her pants, she struggled with allowing her abdomen to expand and her pants to be looser because she thought that she looked much more attractive in tight clothing. Yet, she agreed that her boy friend would love her regardless whether she wore loose or tight clothing. To encourage an acceptance for wearing looser clothing and thereby permit diaphragmatic breathing during the day, an informal discussion focused on “designer jeans syndrome” (chest breathing induced by tight clothing) with humorous examples such as discussing the name of the room that is located on top of the stairs in the Victorian houses in San Francisco. It is called the fainting room–in the 19th century women who wore corsets and had to climb the stairs would have to breathe rapidly and then would faint when they reached the top of the stairs (Peper, 1990).
Rationale: Rapid shallow chest breathing can induce a catabolic state that inhibits healing while diaphragmatic breathing may induce an anabolic state that promotes regeneration. Moreover, effortless diaphragmatic breathing would increase respiratory sinus arhythmia (RSA)–heart rate variability linked to breathing– and thereby facilitate sympathetic-parasympathetic balance that would promote self-healing.
The discussion included the use of the YES set which meant asking a person questions in such a way that she/he answers the question with YES. When a person answers YES at least three times in a row rapport is often facilitated (Erikson, 1983, pp. 237-238). Questions were framed in such a way that the client would answer with YES. For example, if the therapist thought the person did not do their homework, a yes question could be framed as, “It must have been difficult to find time to do the homework this week?” In T.’s case, the therapist said, “I see, you would rather wear tight clothing than allow your shoulder to heal.” She answered, “Yes.” This was the expected answer, however, the question was framed in an intuitive guess on the therapist’s part. Nevertheless, the strategy would have been successful either way because if she had answered “No,” it would have broken the “Yes: set, but she would then be committed to change her clothing.
Throughout this discussion, the therapist placed his left hand on her abdomen over her belly button and overtly and covertly guided her breathing movement. As she exhaled, he pressed gently on her abdomen; as she inhaled he drew his hand away–as if her abdomen was like a balloon that inflated during inhalation and deflated during exhalation. To enhance learning diaphragmatic breathing and slower exhalation, the therapist covertly breathed at the same rhythm and gently exhaled as she exhaled while allowing the breathing movement to be mainly in his abdomen. In this process, learning occurred without demand for performance and she could imitate the breathing process that was covertly modelled by the therapist.
The Change
The central observation was that each time she tried to relax or do something, she would slight brace which increased her pectoralis SEMG activity. The chronic tension from guarding probably induced localized ischemia, inhibited lymphatic flow and drainage, and reduced blood circulation which would increase tissue irritation. Whenever the therapist began to move her arm, she would anticipate and try to help with the movement. Overall she was vigilant (also indicated by her very cold hands) and wanted to perform very well (a possible need for approval). Her muscle bracing and helping with movement was reframed as a combined activity that consisted of guarding to prevent further injury and as a compliment that she would like to perform well.
Labelling her activity as a “compliment” was part of a continuing YES set approach. The therapist was deliberately framing whatever happened as adaptive behaviour, with positive intent. Further, if one tries and does something with too much effort while being vigilant, the arousal would probably induce hand cooling. If the activity can be performed with passive attention, then increased blood flow and warmth may occur. The therapeutic challenge was how to reduce vigilance, perfectionism and guarding so that the muscles that were guarding the traumatized area would relax.
Therapeutic concept: If a direct approach does not work, an indirect approach needs to be employed. Through an indirect approach, the person experiences a change without trying to focus on doing or achieving it. Underlying this approach is the guideline: If something does not work, try it once more and then if it does not work, do something completely different. This is analogous to sexual arousal: If you demand from a male to have an erection: The more performance you demand the less likely will there be success. On the other hand, if you remove the demand for performance and allow the person to become interested and thereby feel an erotic experience an erection may occur without effort.
The shift to an indirect intervention was done through active somatic visualization. T. was encouraged to visualize and remember a positive image or memory from her past. She chose a memory of a time when she was in Paris with her grandmother. While T. visualized being with her grandmother, the therapist asked another older women participant to help and hold T’s right hand in a grandmother-like way as if she was her grandmother. The “grandmother” then moved T.’s hand in a playful way as if dancing with T.’s right arm. Through this kinesthetic experience, T. became more and more absorbed in her memory experience. At the same time, T´s left hand was being held and gently rocked by the therapist. During this gentle rocking, the SEMG activity decreased completely in her left pectoralis area. The therapist used the SEMG feedback to guide him in the gentle rocking motion of T.’s left arm and very slowly increased the range of her arm and shoulder motion. Gentle movement was done only as long as the SEMG activity did not increase. It allowed the muscle to stay relaxed and facilitated the experience of trust. The following is T. report two days later of what happened.
“Initially it was very difficult for me to let go of control because I found this idea somewhat strange and I was puzzled. I expected the therapist to intervene and I felt frightened. The therapist’s soft and gentle touch and his very soft voice in this kind of meditation helped me to let go of control and I was surprised about my own courage to give myself into the process without knowing what would happen next.”
Rationale: Every corresponding thought and emotion has an associated body response and every body response has an associated mental/emotional response (Green & Green, 1977; Green, 1999). Therefore, an image and experience of a happy and safe past memory will allow the body to evoke the same state and vigilance can be abated. The intensity of the experience is increased when multi-sensory cues are included such as actual handholding. The more senses are involved, the more the experience can become real. In addition, the tactile sensation of feeling the grandmother’s hand diverted her attention away from her shoulder into her hand and thereby reduced her active efforts of trying to relax the shoulder and pectoralis area. Doing something she did not expect to happen also helped her loose control – an implicit confusion approach.
SEMG feedback was used as the guide for controlling the movement. The therapist gently increased the range of the movements in abduction and external rotation directions while continuously rocking her arm until her injured arm was able to move unrestricted in full range of motion. The arm and shoulder relaxation and continuous subtle movement without evoking any SEMG activation facilitated blood flow and lymphatic drainage which probably reduced congestion. After a few minutes, the therapist gently dropped her arm on her lap. After her arm was resting on her lap, she reported that it felt very heavy and relaxed and that she didn’t feel any pain. However, she initially didn’t really realize that her mobility had increased dramatically.
Rationale: When previous movements that had been associated with pain are linked to an experience of pleasure, the movement is often easier. The conditioned muscle bracing patterns associated with anticipation of pain and/or concern for improvement/results are reduced.
Process to deepen and generalize the relaxation and breathing. She was asked to imagine breathing the air down and through her arms and legs–a strategy that she could then do at home with her boyfriend. We wanted to involve another person because it is often difficult to do homework practices without striving and concern for results and focussing on the area of discomfort. Her response to asking if her boyfriend would help was an automatic “naturally” (the continuation of the YES set). With her agreement, we role played how her boyfriend was to encourage diaphragmatic breathing. He was to gently stroke down her legs as she exhaled. She could then just focus on the sensations and allow the air to flow down her legs. Then, while she continued to breathe effortlessly, he would gently rock and move her arm.
To be sure that she knew how to give the instructions, the therapist role played her boyfriend and then asked her to rock his arm so that she would know how to teach her boy friend how to move her arm. The therapist sat on her left side, and, as she now held his right arm and gently rocked it with her left arm, the therapist gently moved backwards. This meant that she externally rotated her left arm and shoulder more and more. He moved in such a way that in the process of rocking his arm, she moved her “previously injured shoulder” in all directions (up, down, forward and backwards) and was unaware that she could move her arm and shoulder as she did not experience any discomfort. Afterwards, we shared our observations and she was asked to move her arm and shoulder. She moved it without any restrictions or discomfort.
Rationale: By focusing outside herself and not being concerned about herself, she did not think of herself or of trying to move her arm and shoulder. Hence, she did not evoke the anticipatory guarding and thus significantly increased her flexibility.
Process of acceptance. Often after an injury, we are frustrated with our bodies. This frustration may interfere with healing. Therefore, the session concluded by asking her to be appreciative of her shoulder and arm. She was asked to think of all the positive things her shoulder, chest and arm have done for her in the past instead of the many limitations and pains caused by the injury. Instead of being angry at her shoulder that it had not healed or restricted her movement, we suggested that she should appreciate her shoulder and pectoralis area for all it had done without her awareness such as: How the shoulder moved her arm during love-making, how without complaining her shoulder moved during walking, writing, skiing, eating, etc., and how many times in the past she had abused her shoulder without giving it proper respect and appreciation. This process reframes the way one symbolically relates to the injured area. Every thought of discomfort or negative judgement becomes the trigger and is transformed into breathing lower and slower and evokes an appreciation of the positive nice things her shoulder has done for her in the past.
Rationale: When injured we often evoke negative mental and emotional images which become post- hypnotic suggestions. Those negative thoughts, images and emotions interfere with healing while positive thoughts, images and emotions tend to promote healing. A possible energetic process that occurs when injured is that we withdraw awareness/ consciousness from the injured area which reduces blood and lymph circulation. Caring and positive feelings about an area tends to increase blood flow and warmth (a heart-warming experience) and promotes healing.
RESULTS
She left the initial session without any pain and with total range of motion. At the two week follow-up she reported continued pain relief and complete range of motion. T.s reflection of the experience was:
“I really was not aware that I could move my arm freely like before the accident, I was just feeling a kind of trance and was happy to not feel any pain and to feel much more upright than before. Then I watched the faces of the two other therapists who sat there with big eyes and a grin on their face and then become aware of my own arms position which was rotated backwards and up, a movement that was impossible to do before. I remember this evening that I left with this feeling of trance and that I often tried to go back to my collapsed posture but this was not possible anymore and I felt very tall and straight. Now two weeks later I still feel like that and know that I had an amazing experience which I will store in my brain!
My father who is an orthopedic surgeon tested me and found out, that I had hurt my rib. He said that I have a contusion and it will go away in a few weeks. Before this experience, I would say that he was not open to Biofeedback. However he was so captivated by my experiences that he spontaneously promised me to pay for my own biofeedback equipment and to support me with my educational program and even offered me a job in his practice to do this work!”
Psychophysiological Follow-up: 3 Weeks Later
The physiological assessment included monitoring thoracic and abdominal breathing patterns, blood volume pulse, heart rate and SEMG from her left pectoralis muscle while she was asked to roll her left shoulder forward (adducted and internally rotated) for the count of 10 and then relax. The physiological recording showed that she breathed more diaphragmatically and that her pectoralis muscle relaxed and returned directly to baseline after rotation as shown in Fig. 4.

Figure 4. Physiological profile during the rolling left shoulder forward (tense) and relaxing at thethree week follow-up. Note that the pectoralis sEMG activity returned rapidly to baseline after contracting and her breathing pattern is abdomninal and slower.
Summary
This case example demonstrates the usefulness of a simple one-channel SEMG biofeedback device to guide the interventions during assessment and treatment. It suggests that the therapist and client can use the SEMG activity as an indicator of guarding–a visual representation of the subjective experience of fear, pain and range of mobility–that can be evoked during assessment and therapeutic interventions. The anticipation of increased pain commonly occurs during diagnosis and treatment and often becomes an obstacle for healing because increased pain may increase anticipation of pain and trigger even more bracing. To avoid triggering this vicious circle of guarding/fear, the feedback signal allows the therapist and the client to explore strategies that reduce muscle activity by indirect interventions.
By using an indirect approach that the client may not expect, the interventions shift the focus of attention and striving and may allow increased freedom and relaxation. The biofeedback signal may guide the therapeutic process to reduce the patterns of fear, panic, and bracing that are commonly associated with injury and illnesses. Once this excessive sympathetic activity is reduced, the actual pathophysiology may become obvious (in most cases is much less then before) and the healing process may be accelerated. This case description may offer an approach in diagnosis and treatment for many therapists and open a door for a gentle, painless and yet successful way of treatment and encourage therapists to be creative and use both experience/technique and intuition.
For additional intervention approaches see the following two blogs.
References
Barlow, W. (1991). The Alexander technique: How to use your body without stress. Rochester, VT: Healing Arts Press https://www.amazon.com/Alexander-Technique-Your-without-Stress/dp/0892813857#:~:text=Barlow%2C%20the%20foremost%20exponent%20and,and%20movement%20in%20everyday%20activities.
Erikson, M. H. (1983). Healing in hypnosis, volume 1 (Edited by E. L. Rossi, M. O. Ryan, M. & F. A. Sharp). New York: Irvington Publishers, Inc.. https://www.amazon.com/Hypnosis-Seminars-Workshops-Lectures-Erickson/dp/0829007393/ref=sr_1_1?keywords=9780829007398&linkCode=qs&qid=1692038804&s=books&sr=1-1
Green, E. (1999). Psychophysical Principal. Accessed August 14, 2023 https://www.elmergreenfoundation.org/psychophysiological-principal/
Green, E., & Green, A. (1977). Beyond biofeedback. New York:
Delacorte Press/Seymour. https://elmergreenfoundation.org/wp-content/uploads/2019/02/Beyond-Biofeedback-Green-Green-Searchable.pdf
MacHose, M., & Peper, E. (1991). The effect of clothing on inhalation volume. Biofeedback and Self-Regulation. 16(3), 261-265. https://doi.org/10.1007/BF01000020
Peper, E. (1990). Breathing for health. Montreal: Thought Technology Ltd.
Peper, E. & Gibney, K.H. (2006). Muscle biofeedback at the computer-A manual to prevent repetitive strain injury (RSI) by taking the guesswwork out of assessment, monitoring and training. Biofeedback Foundation of Europe. https://thoughttechnology.com/muscle-biofeedback-at-the-computer-book-t2245/
Peper, E., Gilbert, C.D., Harvey, R. & Lin, I-M. (2015). Did you ask about abdominal surgery or injury? A learned disuse risk factor for breathing dysfunction. Biofeedback. 34(4), 173-179. https://doi.org/10.5298/1081-5937-43.4.06
Sella, G. E. (2006). SEMG: Objective methodology in muscular dysfunction investigation and rehabilitation. Weiner’s pain management: A practical guide for clinicians, CRC Press, 645-662. https://www.taylorfrancis.com/chapters/edit/10.1201/b14253-45/semg-objective-methodology-muscular-dysfunction-investigation-rehabilitation-gabriel-sella
Sella, G. E. (1998). Towards an Integrated Approach of sEMG Utilization: Quantative Protocols of Assessment and Biofeedback. Electromyography: Applications in Physical Medicine. Thought Technology, 13. https://www.bfe.org/protocol/pro13eng.htm
[1] We thank Theresa Stockinger for her significant contribution and Candy Frobish for her helpful comments.
Are food companies responsible for the epidemic in diabetes, cancer, dementia and chronic disease and do their products need to be regulated like tobacco? Is it time for a class action suit?
Posted: July 15, 2023 Filed under: behavior, cancer, Evolutionary perspective, health, Nutrition/diet, self-healing | Tags: dementia, diabetes, diet, high fructose corn syrup, mortality, obsity, smoking, sugar, ultra-processed foods, UPF 4 CommentsAdapted from: Peper, E. & Harvey, R. (2024). Are Food Companies Responsible for the Epidemic in Diabetes, Cancer, Dementia and Chronic Disease and Do Their Products Need to Be Regulated Like Tobacco? Is It Time for a Class Action Suit? Thownsend Letter-the examiner of alternative medicine. https://www.townsendletter.com/e-letter-26-ultra-processed-foods-and-health-issues/
Erik Peper, PhD and Richard Harvey, PhD

Why are one third of young Americans becoming obese and at risk for diabetes?
Why are heart disease, cancer, and dementias occurring earlier and earlier? Is it genetics, environment, foods, or lifestyle?
Is it individual responsibility or the result of the quest for profits by agribusiness and the food industry?
Like the tobacco industry that sells products regulated because of their public health dangers, is it time for a class action suit against the processed food industry? The argument relates not only to the regulation of toxic or hazardous food ingredients (e.g., carcinogenic or obesogenic chemicals) but also to the regulation of consumer vulnerabilities. Addressing vulnerabilities to tobacco products include regulations such as how cigarette companies may not advertise their products for sale within a certain distance from school grounds.
Is it time to regulate nationally the installation of vending machines on school grounds selling sugar-sweetened beverages? Students have sensitivity to the enticing nature of advertised, and/or conveniently available consumable products such as ‘fast foods’ that are highly processed (e.g., packaged, preserved and practically imperishable). Whereas ‘processed foods’ have some nutritive value, and may technically pass as ‘nutritious’ food, the quality of processed ‘nutrients’ can be called into question. For the purpose of this blog other important questions to raise relate to ingredients which, alone or in combination, may contribute to the onset of or, the acceleration of a variety of chronic health outcomes related to various kinds of cancers, cardiovascular diseases, and diabetes.
It may be an over statement to suggest that processed food companies are directly responsible for the epidemic in diabetes, cancer, dementia and chronic disease and need to be regulated like tobacco. On the other hand, processed food companies should become much more regulated than they are now.
More than 80 years ago, smoking was identified as a significant factor contributing to lung cancer, heart disease and many other disorders. In 1964 the Surgeon Generals’ report officially linked smoking to deaths of cancer and heart disease (United States Public Health Service, 1964). Another 34 years pased before California prohibited smoking in restaurants in 1998 and, eventually inside all public buildings. The harms of smoking tobacco products were well known, yet many years passed with countless deaths and suffering which could have been prevented before regulation of tobacco products took place. Reviewing historical data there is about a 20 year delay (e.g., a whole generation) before death rates decrease in relation to when regulations became effective and smoking rates decreased, as shown in figure 1.

Figure 1. The relationship between smoking and lung cancer. Reproduced by permission from Roser, M. (2021). Smoking: How large of a global problem is it? And how can we make progress against it? Our world in data.
During those interim years before government actions limited smoking more effectively, tobacco companies hid data regarding the harmful effects of smoking. Arguably, the ‘Big Tobacco’ industry paid researchers to publish data which could confuse readers about tobacco product harm. There is evidence of some published articles suggesting that the harm of cigarette smoking was a hoax– all for the sake of boosting corporate profits (Bero, 2005).
Now we are experiencing a similar problem with the processed food industry. It has been suggested that alongside smoking and vaping, opioid use, a sedentary ‘couch potato’ lifestyle, and lack of exercise, ultra-processed food (UPF) that we eat severely affects our health.
Ultra-processed foods, which for many constitutes a majority of calories ranging from 55% to over 80% of the food they eat, contain chemical additives that trick the tastebuds, mouth and eventually our brain to desire those processed foods and eat more of them (Srour et al., 2022).
What are ultra-processed foods? Any foods that your great grandmother would not recognize as food. This includes all soft drinks, highly processed chips, additives, food coloring, stabilizers, processed proteins, etc. Even oils such as palm oil, canola oil, or soybean are ultra processed since they heated, highly processed with phosphoric acid to remove gums and waxes, neutralized with chemicals, bleached, and deodorized with high pressure steam (van Tulleken, 2023).
The data is clear! Since the 1970s obesity and inflammatory disease have exploded after ultra-processed foods became the constituents of the modern diet as shown in figure 2.
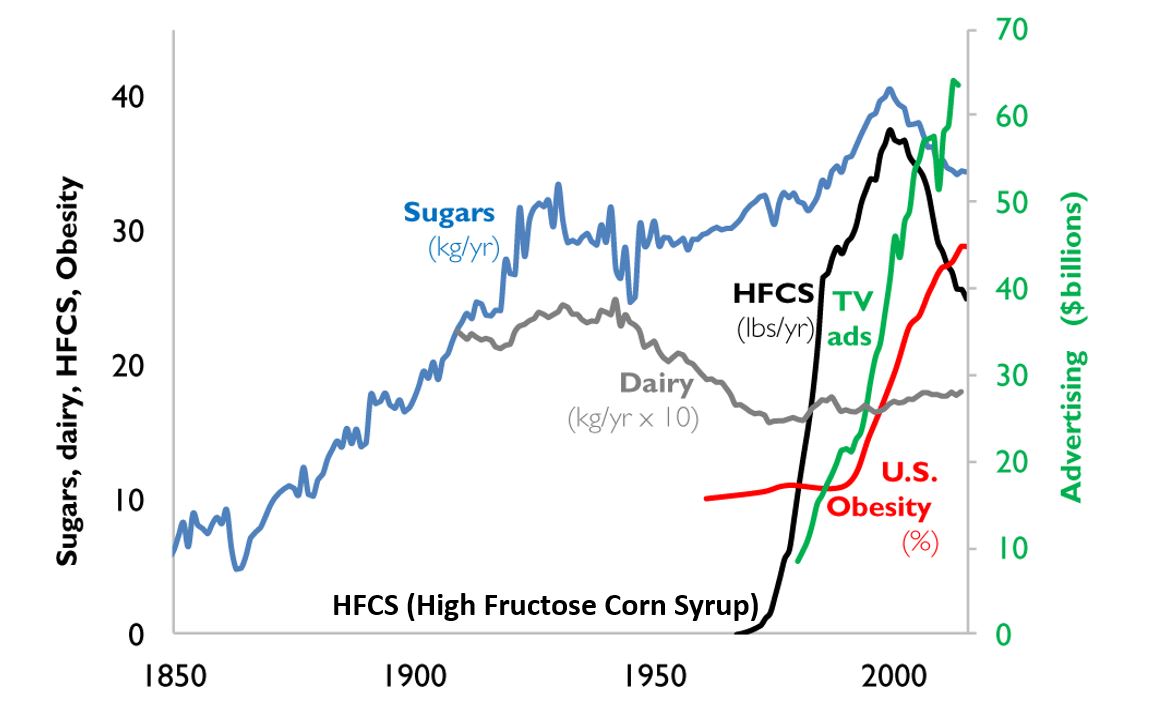
Figure 2. A timeline from 1850 to 2000 reflects the increase in use of refined sugar and high fructose corn syrup (HFCS) to the U.S. diet, together with the increase in U.S. obesity rate. The data for sugar, dairy and HFCS consumption per capita are from USDA Economic Research Service (Johnson et al., 2009) and reflects historical estimates before 1967 (Guyenet et al., 2017). The obesity data (% of U.S. adult population) are from the Robert Wood Johnson Foundation’s Trust for America’s Health. (stateofobesity.org). Total U.S. television advertising data are from the World Advertising Research Center (www.warc.com). The vertical measure (y–axis) for kilograms per year (kg/yr) on the left covers all data except advertising expenditures, which uses the vertical measure for advertising on the right. Reproduced by permission from Bentley et al, 2018.
This graph clearly shows a close association between the years that high fructose corn syrups (HFCS) were introduced into the American diet and an increase in TV advertising with corresponding increase in obesity. HFCS is an ultra-processed food and is a surrogate marker for all other ultra-processed foods. The best interpretation is that ultra-processed foods, which often contain HFCS, are a causal factor of the increase in obesity, and diabetes and in turn are risk factors for heart disease, cancers and dementias.
Ultra-processed foods are novel from an evolutionary perspective.
The human digestive system has only recently encountered sources of calories which are filled with so many unnatural chemicals, textures and flavors. Ultra-processed foods have been engineered, developed and product tested to increase the likelihood they are wanted by consumers and thereby increase sales and profits for the producers. These foods contain the ‘right amount’ processed materials to evoke the taste, flavor and feel of desired foods that ‘trick’ the consumer it eat them because they activate evolutionary preference for survival. Thus, these ultra-processed foods have become an ‘evolutionary trap’ where it is almost impossible not to eat them. We eat the food because it capitalized on our evolutionary preferences even though doing so is ultimately harmful for our health (for a detailed discussion on evolutionary traps, see Peper, Harvey & Faass, 2020).
An example is a young child wanting the candy while waiting with her parents at the supermarket checkout line. The advertised images of sweet foods trigger the cue to eat. Remember, breast milk is sweet and most foods in nature that are sweet in taste, provide calories for growth and survival and are not harmful. Calories are essential of growth. Thus, we have no intrinsic limit on eating sweets unlike foods that taste bitter.
As parents, we wish that our children (and even adults) have self-control and no desire to eat the candy or snacks that is displayed at eye level (eye candy) especially while waiting at the cashier. When reflecting about food advertising and the promotion of foods that are formulated to take advantage of ‘evolutionary traps’, who is responsible? Is it the child, who does not yet have the wisdom and self-control or, is it the food industry that ultra-processes the foods and adds ingredients into foods which can be harmful and then displays them to trigger an evolutionary preference for food that have been highly processed?
Every country that has adapted the USA diet of ultra-processed foods has experienced similar trends in increasing obesity, diabetes, cardiovascular disease, etc. The USA diet is replacing traditional diets as illustrated by the availability of Coca-Cola. It is sold in over 200 countries and territories (Coca-Cola, 2023).
An increase in ultra-processed foods by 10 percent was associated with a 25 percent increase in the risk of dementia and a 14 per cent increase in the risk of Alzheimers’s (Li et al., 2022). More importantly, people who eat the highest proportion of their diet in ultra-processed foods had a 22%-62% increased risk of death compared to the people who ate the lowest proportion of processed foods (van Tulleken, 2023). In the USA, counties with the highest food swamp scores (the availability of fast food outlets in a county) had a 77% increased odds of high obesity-related cancer mortality (Bevel et al., 2023). The increase risk has also been observed for cardiovascular disease, coronary heart disease, cerebrovascular disease and all cause mortality as is shown in figure 3 (Srour et al., 2019; Rico-Campà et al., 2019).

Figure 3. Association between consumption of ultra-processed foods and all cause mortality. Reproduced from Rico-Campà et al, 2019.
The harmful effects of UPF holds up even when correcting for the amount of sugars, carbohydrates or fats in the diet and controlling for socio economic variables.
The logic that underlies this perspective is based upon the writing by Nassim Taleb (2012) in his book, Antifragile: Things That Gain from Disorder (Incerto). He provides an evolutionary perspective and offers broad and simple rules of health as well as recommendations for reducing UPF risk factors:
- Assume that anything that was not part of our evolutionary past is probably harmful.
- Remove the unnatural/unfamiliar (e.g. smoking/ e-cigarettes, added sugars, textured proteins, gums, stabilizers (guar gum, sodium alginate), emulsifiers (mono-and di-glycerides), modified starches, dextrose, palm stearin, and fats, colors and artificial flavoring or other ultra-processed food additives).
What can we do?
The solutions are simple and stated by Michael Pollan in his 2007 New York Times article, “Eat food. Not too much. Mostly Plants.” Eat foods that your great grandmother would recognize as foods (Pollan, 2009). Do not eat any of the processed foods that fill a majority of a supermarket’s space.
- Buy only whole organic natural foods and prepare them yourself.
- Request that food companies only buy and sell non-processed foods.
- Demand government action to tax ultra-processed food and limit access to these foods. In reality, it is almost impossible to expect people to choose healthy, organic foods when they are more expensive and not easily available in the American ‘food swamps and deserts’ (the presence of many fast food outlets or the absence of stores that have fresh produce and non-processed foods). We do have a choice. We can spend more money now for organic, health promoting foods or, pay much more later to treat illness related to UPF.
- It is time to take our cues from the tobacco wars that led to regulating tobacco products. We may even need to start class action suits against producers and merchants of UPF for causing increased illness and premature morbidity.
For more background information and the science behind this blog, read, the book, Ultra-processed people, by Chris van Tulleken.

Look at the following blogs for more background information.
References
Bentley, R.A., Ormerod, P. & Ruck, D.J. (2018). Recent origin and evolution of obesity-income correlation across the United States. Palgrave Commun 4, 146. https://doi.org/10.1057/s41599-018-0201-x
Bero, L. A. (2005). Tobacco Industry Manipulation of Research. Public Health Reports (1974-), 120(2), 200–208. http://www.jstor.org/stable/20056773
Bevel, M.S., Tsai, M., Parham, A., Andrzejak, S.E., Jones, S., & Moore, J.X. (2023). Association of Food Deserts and Food Swamps With Obesity-Related Cancer Mortality in the US. JAMA Oncol. 9(7), 909–916. https://doi.org/10.1001/jamaoncol.2023.0634
Coca-Cola. (2023). More on Coca-Cola. Accessed July 14, 2023. https://www.coca-cola.co.uk/our-business/faqs/how-many-countries-sell-coca-cola-is-there-anywhere-in-the-world-that-doesnt
Johnson, R.K., Appel, L.J., Brands, M., Howard, B.V., Lefevre, M., Lustig, R.H., Sacks, F., Steffen, L.M., & Wylie–Rosett, J. (2009). Dietary sugars intake and cardiovascular health: a scientific statement from the American Heart Association. Circulation, 120(10), 1011–1020. https://doi.org/10.1161/CIRCULATIONAHA.109.192627
Li, H., Li, S., Yang, H., et al, 2022. Association of ultraprocessed food consumption with the risk of dementia: a prospective cohort study. Neurology, 99, e1056-1066. https://doi.org/10.1212/WNL.0000000000200871
Peper, E., Harvey, R. & Faass, N. (2020). TechStress: How Technology is Hijacking Our Lives, Strategies for Coping, and Pragmatic Ergonomics. Berkeley: North Atlantic Books, pp 18-22, 151. https://www.amazon.com/Beyond-Ergonomics-Prevent-Fatigue-Burnout/dp/158394768X/ref=sr_1_1?crid=1U9Y82YO4DKKP&keywords=erik+peper&qid=1689372466&sprefix=erik+peper%2Caps%2C187&sr=8-1
Pollan, M. (2007). Unhappy meals. The New York Times Magazine. https://www.nytimes.com/2007/01/28/magazine/28nutritionism.t.html
Pollan, M. (2009). Food Rules: An Eater’s Manual. New York: Penguin Books. https://www.amazon.com/Food-Rules-Eaters-Michael-Pollan/dp/014311638X/ref=tmm_pap_swatch_0?_encoding=UTF8&qid=1689373484&sr=8-2
Rico-Campà, A., Martínez-González, M. A., Alvarez-Alvarez, I., de Deus Mendonça, R., Carmen de la Fuente-Arrillaga, C., Gómez-Donoso, C., & Bes-Rastrollo, M. (2019). Association between consumption of ultra-processed foods and all cause mortality: SUN prospective cohort study. BMJ; 365: l1949 https://doi.org/10.1136/bmj.l1949
Roser, M. (2021).Smoking: How large of a global problem is it? And how can we make progress against it? Our world in data. Assessed July 13, 2023. https://ourworldindata.org/smoking-big-problem-in-brief
Srour, B., Fezeu, L.K., Kesse-Guyot, E.,Alles, B., Mejean, C…(2019). Ultra-processed food intake and risk of cardiovascular disease: prospective cohort study (NutriNet-Santé) BMJ,365:l1451. https://doi.org/10.1136/bmj.l1451
Srour, B., Kordahi, M. C., Bonazzi, E., Deschasaux-Tanguy, M., Touvier, M., & Chassaing, B. (2022). Ultra-processed foods and human health: from epidemiological evidence to mechanistic insights. The Lancet Gastroenterology & Hepatology. https://doi.org/10.1016/S2468-1253(22)00169-8
Taleb, N. N. (2012). Antifragile: Things That Gain from Disorder (Incerto). New York: Random House Publishing Group. (Kindle Locations 5906-5908). https://www.amazon.com/Antifragile-Things-Disorder-ANTIFRAGILE-Hardcover/dp/B00QOJ6MLC/ref=sr_1_4?crid=3BISYYG0RPGW5&keywords=Antifragile%3A+Things+That+Gain+from+Disorder+%28Incerto%29&qid=1689288744&s=books&sprefix=antifragile+things+that+gain+from+disorder+incerto+%2Cstripbooks%2C158&sr=1-4
Van Tulleken, C. (2023). Ultra-processed people. The science behind food that isn’t food. New Yoerk: W.W. Norton & Company. https://www.amazon.com/gp/product/1324036729/ref=ox_sc_act_title_1?smid=ATVPDKIKX0DER&psc=1
United States Public Health Service. (1964). The 1964 Report on Smoking and Health. United States. Public Health Service. Office of the Surgeon General. https://profiles.nlm.nih.gov/spotlight/nn/catalog?f%5Bexhibit_tags%5D%5B%5D=smoking
Reflections on the increase in Autism, ADHD, anxiety and depression: Part 1-bonding, screen time, and circadian rhythm
Posted: July 4, 2023 Filed under: ADHD, behavior, computer, digital devices, education, emotions, Evolutionary perspective, health, laptops, screen fatigue, Uncategorized | Tags: anxiety, autism, bonding, circadian rhythms, depression, nature, still face experiment 10 Comments
Adapted from: Peper, E. Reflections on the increase in Autism, ADHD, anxiety and depression: Part 1-bonding, screen time, and circadian rhythms. NeuroRegulation,10(2), 134-138. https://doi.org/10.15540/nr.10.2.134
Over the past two decades, there has been a significant increase in the prevalence of autism, Attention-Deficit/hyperactivity disorder (ADHD), anxiety, depression, and pediatric suicidal behavior. Autism rates have risen from 1 in 150 children in 2000 to 1 in 36 children in 2020 (CDC, 2023), while ADHD rates have increased from 6% in 1997 to approximately 10% in 2018 (CDC, 2022). The rates of anxiety among 18-25 year-olds have also increased from 7.97% in 2008 to 14.66% in 2018 (Goodwin et al., 2020), and depression rates for U.S. teens ages 12-17 have increased from 8% in 2007 to 13% in 2017 (Geiger & Davis, 2019; Walrave et al., 2022). Pediatric suicide attempts have also increased by 163% from 2009 to 2019 (Arakelyan et al., 2023), and during the COVID-19 pandemic, these rates have increased by more than 25% (WHO, 2022; Santomauro et al., 2021). In addition, the prevalence of these disorders has tripled for US adults during the pandemic compared to before (Ettman et al., 2020).
The rapid increase of these disorders is not solely due to improved diagnostic methods, genetic factors or the COVID-19 pandemic. The pandemic amplified pre-existing increasing trends. More likely, individuals who were at risk had their disorders triggered or amplified by harmful environmental and behavioral factors. Conceptually, Genetics loads the gun; epigenetics, behavior, and environment pull the trigger.
While behavioral strategies such as neurofeedback, Cognitive Behavior Therapy, biofeedback, meditation techniques, and pharmaceuticals can treat or ameliorate these disorders, the focus needs to be on risk reduction. In some ways, treatment can be likened to closing the barn doors after the horses have bolted.
Evolutionary perspective to reduce risk factors
Nassim Taleb (2012) in his book, Antifragile: Things That Gain from Disorder (Incerto), provides an evolutionary perspective and offers simple rules of health by reducing risk factors:
- Assume that anything that was not part of our evolutionary past is probably harmful.
- Remove the unnatural/unfamiliar (e.g. smoking/ e-cigarettes, sugar, digital media).
- We do not need evidence of harm to claim that a drug or an unnatural procedure is dangerous. If evidence of harm does not exist, it does not mean harm does not exist.
- Only resort to medical techniques when the health payoff is very large (to save a life), exceeds its potential harm, such as incontrovertibly needed surgery or life-saving medicine (penicillin).
- Avoid the iatrogenics and negative side effects of prescribed medication.
Writer and scholar Taleb’s suggestions are reminiscent of the perspective described by the educator Joseph C. Pearce (1993) in his book, Evolution’s End. Pearce argued that modern lifestyles have negatively affected the secure attachment and bonding between caregivers and infants. The lack of nurturing and responsive caregiving in early childhood may lead to long-term emotional and psychological problems. He points out that we have radically adapted behaviors that differ from those that evolved over thousands of generations and that allowed us to thrive and survive. In the last 100 years, babies have often been separated from their mothers at birth or early infancy by being put in a nursery or separate room, limited or no breastfeeding with the use of formula, exposure to television for entertainment, lack of exploratory play outdoors, and the absence of constant caretakers in high-stress and unsafe environments.
As Pearce pointed out, “If you want true learning, learning that involves the higher frontal lobes – the intellectual, creative brain – then again, the emotional environment must be positive and supportive. This is because at the first sign of anxiety the brain shifts its functions from the high, prefrontal lobes to the old defenses of the reptilian brain… These young people need audio-vocal communication, nurturing, play, body movement, eye contact, sweet sounds and close heart contact on a physical level” (Mercogliano & Debus, 1999).
To optimize health, eliminate or reduce those factors that have significantly changed or were not part of our evolutionary past. The proposed recommendations are based upon Talib’s perspective that anything that was not part of our evolutionary past is probably harmful; thus, it is wise to remove the unnatural/unfamiliar and adopt the precautionary principle, which states that if evidence of harm does not exist, it does not mean harm does not exist (Kriebel et al., 2010).
This article is the first of a three-part series. Part 1 focuses on increasing reciprocal communication between infant and caretaker, reducing screen time, and re-establishing circadian rhythms; Part 2 focuses on reducing exposure to neurotoxins, eliminating processed foods, and supporting the human biome; and Part 3 focuses on respiration and movement.
Part 1- Increase bonding, reduce screen time, and re-establish circadian rhythms
Increase bonding between infant and caretaker
Infants develop emotional communication through reciprocal interactions with their caregivers, during which the caregiver responds to the infant’s expressions. When this does not occur, it can be highly stressful and detrimental to the infant’s development. Unfortunately, more and more babies are emotionally and socially isolated while their caregivers are focussed on, and captured by, the content on their digital screens. Moreover, infants and toddlers are entertained (babysat) by cellphones and tablets instead of dynamically interacting with their caretakers. Screens do not respond to the child’s expressions; the screen content is programmed to capture the infant’s attention through rapid scene changes. Without reciprocal interaction, babies often become stressed, as shown by the research of developmental psychologist Professor Edward Tronick, who conducted the “Still Face” experiment (Tronick & Beeghly, 2011; Weinberg et al, 2008).
The “Still Face” experiment illustrated what happens when caregivers are not responding to infants’ communication. The caregivers were asked to remain still and unresponsive to their babies, resulting in the infants becoming increasingly distressed and disengaged from their surroundings. Not only does this apply to infants but also to children, teenagers and older individuals. Watch the short Still Face experiment, which illustrates what happens when the caretaker is not responding to the infant’s communication.
Recommendation. Do not use cellphone and digital media while being with an infant in the first two years of life. It is important for caregivers to limit their cellphone use and prioritize reciprocal interactions with their infants for healthy emotional and psychological development.
Reduce screen time (television, social media, streaming videos, gaming)[1]
From an evolutionary perspective, screen time is an entirely novel experience. Television, computers, and cellphones are modern technologies that have significantly impacted infants’ and young people’s development. To grow, infants, toddlers, and children require opportunities to explore the environment through movement, touch, and play with others, which is not possible with screens. Research has shown that excessive screen time can negatively affect children’s motor development, attention span, socialization skills, and contribute to obesity and other health problems (Hinkley et al., 2014; Carson et al., 2016; Mark, 2023).
When four-year-olds watch fast-paced videos, they exhibit reduced executive functions and impulse control, which may be a precursor for ADHD, compared to children who engage in activities such as drawing (Lillard & Peterson, 2011; Mark, 2023).
Furthermore, excessive screen time and time spent on social media are causal in increasing depression in young adults-–as was discovered when Facebook became available at selected universities. Researchers compared the mental health of students at similar universities where Facebook was or was not available and observed how the students’ mental health changed when Facebook became available (Braghieri et al., 2022). Their research showed that “College-wide access to Facebook led to an increase in severe depression by 7% and anxiety disorders by 20%. In total, the negative effect of Facebook on mental health appeared to be roughly 20% the magnitude of what is experienced by those who lose their job” (Walsh, 2022).
Exposure to digital media has also significantly reduced our attention span from 150 seconds in 2004 to an average of 44 seconds in 2021. The shortening of attention span may contribute to the rise of ADHD and anxiety (Mark, 2022, p. 96).
Recommendations: Reduce time spent on social media, gaming, mindlessly following one link after the other, or watching episode after episode of streaming videos. Instead, set time limits for screen use, turn off notifications, and prioritize in-person interactions with friends, family and colleagues while engaging in collaborative activities. Encourage children to participate in physical and social activities and to explore nature.
To achieve this, follow the guidelines from the American Academy of Pediatrics’ recommendation on screen time (Council on Communications and Media, 2016), which suggest these limits on screen time for children of different age groups:
- Children under 18 months of age should avoid all screen time, except for video chatting with family and friends.
- Children aged 18-24 months should have limited screen time, and only when watched together with a caretaker.
- Children aged 2 to 5 years should have no more than one hour of screen time per day with parental supervision.
- For adolescents, screen and social media time should be limited to no more than an hour a day.
In our experience, when college students reduce their time spent on social media, streaming videos, and texting, they report that it is challenging; however, they then report an increase in well-being and performance over time (Peper et al., 2021). It may require more effort to provide children with actual experiential learning and entertainment than allowing them to use screens, but it is worthwhile. Having children perform activities and play outdoors–in a green nature environment–appears to reduce ADHD symptoms (Louv, 2008; Kuo & Taylor, 2004).
Reestablish circadian (daily) rhythms
Our natural biological and activity rhythms were regulated by natural light until the 19th century. It is hard to imagine not having light at night to read, to work on the computer, or to answer email. However, light not only illuminates, but also affects our physiology by regulating our biological rhythms. Exposure to light at night can interfere with the production of melatonin, which is essential for sleep. Insufficient sleep affects 30% of toddlers, preschoolers, and school-age children, as well as the majority of adolescents. The more media is consumed at bedtime, the more bedtime is delayed and total sleep time is reduced (Hale et al., 2018). Reduced sleep is a contributing factor to increased ADHD symptoms of inattention, hyperactivity and impulsivity (Cassoff et al., 2012).
Recommendations: Support the circadian rhythms. Avoid screen time one hour before bedtime. This will reduce exposure to blue light and reduce sympathetic arousal triggered by the content on the screen or reactions to social media and emails. Sleep in total darkness, and establish a regular bedtime and waking time to avoid “social jetlag,” which can negatively affect health and performance (Caliandro et al., 2021). Implement sleep hygiene strategies such as developing a bedtime ritual to improve sleep quality (Stager et al., 2023; Suni, 2023). Thus, go to bed and wake up at the same time each day, including weekends. Avoid large meals, caffeine, and alcohol before bedtime. Consistency is key to success.
Conclusion
To optimize health, eliminate or reduce those factors that have significantly changed or were not part of our evolutionary past, and explore strategies that support behaviors that have allowed the human being to thrive and survive. Improve clinical outcomes and optimize health by enhancing reciprocal communication interactions, reducing screen time and re-establishing the circadian rhythm.
References
Arakelyan, M., Freyleue, S., Avula, D., McLaren, J.L., O’Malley, A.J., & Leyenaar, J.K. (2023). Pediatric Mental Health Hospitalizations at Acute Care Hospitals in the US, 2009-2019. JAMA, 329(12), 1000–1011. https://doi.org/10.1001/jama.2023.1992
Braghieri, L., Levy, R., & Makarin, A. (2022). Social Media and Mental Health (July 28, 2022). Available at SSRN: https://ssrn.com/abstract=3919760 or http://dx.doi.org/10.2139/ssrn.3919760
Caliandro, R., Streng, A.A., van Kerkhof, L.W.M., van der Horst, G.T.J., & Chaves, I. (2021). Social Jetlag and Related Risks for Human Health: A Timely Review. Nutrients, 13(12), 4543. https://doi.org/10.3390/nu13124543
Carson, V., Tremblay, M.S., Chaput, J.P., & Chastin, S.F. (2016). Associations between sleep duration, sedentary time, physical activity, and health indicators among Canadian children and youth using compositional analyses. Appl Physiol Nutr Metab, 41(6 Suppl 3), S294-302. https://doi.org/10.1139/apnm-2016-0026
Cassoff, J., Wiebe, S.T., & Gruber, R. (2012). Sleep patterns and the risk for ADHD: a review. Nat Sci Sleep, 4, 73-80. https://doi.org/10.2147/NSS.S31269
CDC. (2022). Attention-Deficit/hyperactivity disorder (ADHD): ADHD through the years. Centers for Disease Control and Prevention. Assessed March 27, 2023. https://www.cdc.gov/ncbddd/adhd/timeline.html
CDC. (2023). Data & Statistics on Autism Spectrum Disorder. CDC Centers for Disease Control and Prevention. Assessed March 25, 2023. https://www.cdc.gov/ncbddd/autism/data.html
Council on Communications and Media. (2016). Media and young minds. Pediatrics, 138(5), e20162591. https://doi.org/10.1542/peds.2016-2591
Ettman, C.K., Abdalla, S.M., Cohen, G.H., Sampson, L., Vivier, P.M.,& Galea, S. (2020), Prevalence of Depression Symptoms in US Adults Before and During the COVID-19 Pandemic. JAMA Netw Open, 3(9):e2019686. https://doi.org/10.1001/jamanetworkopen.2020.19686
Geiger, A.W. & Davis, L. (2019). A growing number of American teenagers-particularly girls-are facing depression. Pew Research Center. Accessed March 28, 2023.
Goodwin, R.D., Weinberger, A.H., Kim, J.H., Wu. M., & Galea, S. (2020). Trends in anxiety among adults in the United States, 2008-2018: Rapid increases among young adults. J Psychiatr Res. 130, 441-446. https://doi.org/10.1016/j.jpsychires.2020.08.014
Hale, L., Kirschen, G/W., LeBourgeois, M.K., Gradisar, M., Garrison, M.M., Montgomery-Downs, H., Kirschen, H., McHale, S.M., Chang, A.M., & Buxton, O.M. (2018). Youth Screen Media Habits and Sleep: Sleep-Friendly Screen Behavior Recommendations for Clinicians, Educators, and Parents. Child Adolesc Psychiatr Clin N Am, 27(2),229-245. https://doi.org/10.1016/j.chc.2017.11.014
Hinkley, T., Verbestel, V., Ahrens, W., Lissner, L., Molnár, D., Moreno, L.A., Pigeot, I., Pohlabeln, H., Reisch, L.A., Russo, P., Veidebaum, T., Tornaritis, M., Williams, G., De Henauw, S., De Bourdeaudhuij, I; IDEFICS Consortium. (2014). Early childhood electronic media use as a predictor of poorer well-being: a prospective cohort study. JAMA Pediatr,. May;168(5):485-92. https://doi.org/10.1001/jamapediatrics.2014.94
Kriebel, D., Tickner, J., Epstein, P., Lemons, J., Levins, R., Loechler, E.L., Quinn, M., Rudel, R., Schettler, T., Stoto, M. (2001). The precautionary principle in environmental science. Environ Health Perspect, 109(9):871-6. https://doi.org/10.1289/ehp.01109871
Kuo. F.E. & Taylor, A.F. (2004). A potential natural treatment for attention-deficit/hyperactivity disorder: evidence from a national study. Am J Public Health. 94(9),1580-6. https://doi.org/10.2105/ajph.94.9.1580
Lillard, A.S. & Peterson, J. The immediate impact of different types of television on young children’s executive function. Pediatrics, 128(4), 644-9. https://doi.org/10.1542/peds.2010-1919
Louv, R. (2008). Last Child in the Woods: Saving Our Children from Nature-Deficit Disorder. Algonquin Books. Chapel Hill, NC: Algonquin Books
Mark, G. (2023). Attention Span: A Groundbreaking Way to Restore Balance, Happiness and Productivity. Toronto, Canada: Hanover Square Press.
Mercogliano, C. & Debus, K. (1999). Nurturing Heart-Brain Development Starting With Infants 1999 Interview with Joseph Chilton Pearce. Journal of Family Life, 5(1). https://www.michaelmount.co.za/nurturing-heart-brain-development-starting-with-infants-1999-interview-with-joseph-chilton-pearce/
Pearce, J.C. (1993). Evolutions’s End. New York: HarperOne.
Peper, E., Wilson, V., Martin, M., Rosegard, E., & Harvey, R. (2021). Avoid Zoom fatigue, be present and learn. NeuroRegulation, 8(1), 47–56. https://doi.org/10.15540/nr.8.1.47
Santomauro, D.F., Mantilla Herrera, A.M., Shadid, J., Zheng, P., Ashbaugh, C., Pigott, D.M., Abbafati, C., Adolph, C., …. (2021). Global prevalence and burden of depressive and anxiety disorders in 204 countries and territories in 2020 due to the COVID-19 pandemic. The Lancet, 398(103121700-1712., https://doi.org/10.1016/S0140-6736(21)02143-7
Stager, L.M., Caldwell, A., Bates, C., & Laroche, H. (2023). Helping kids get the sleep they need. Society of Behavioral Medicine. Accessed March 29, 2023 https://www.sbm.org/healthy-living/helping-kids-get-the-sleep-they-need?gclid=Cj0KCQjww4-hBhCtARIsAC9gR3ZM7v9VSvqaFkLnceBOH1jIP8idiBIyQcqquk5y_RZaNdUjAR9Wpx4aAhTBEALw_wcB
Suni, E. (2023). Sleep hygiene- What it is, why it matters, and how to revamp your habits to get better nightly sleep. Sleep Foundation. Accessed March 29, 2023. https://www.sleepfoundation.org/sleep-hygiene
Taleb, N. N. (2012). Antifragile: Things That Gain from Disorder (Incerto) Random House Publishing Group. (Kindle Locations 5906-5908).
Tronick, E. & Beeghly, M. (2011).Infants’ meaning-making and the development of mental health problems. Am Psychol, 66(2),107-19. https://doi.org/10.1037/a0021631
Walrave, R., Beerten, S.G., Mamouris, P. et al. Trends in the epidemiology of depression and comorbidities from 2000 to 2019 in Belgium. BMC Prim. Care 23, 163 (2022). https://doi.org/10.1186/s12875-022-01769-w
Walsh, D. (2022 September 14). Study: Social media use linked to decline in mental health. MIT Management Ideas Made to Matter. Accessed March 28, 2023. https://mitsloan.mit.edu/ideas-made-to-matter/study-social-media-use-linked-to-decline-mental-health#:~:text=College%2Dwide%20access%20to%20Facebook,with%20either%20psychotherapy%20or%20antidepressants
Weinberg, M.K., Beeghly, M., Olson, K.L., & Tronick, E. (2008). A Still-face Paradigm for Young Children: 2½ Year-olds’ Reactions to Maternal Unavailability during the Still-face. J Dev Process, 3(1):4-22. https://pubmed.ncbi.nlm.nih.gov/22384309/
WHO (2022). COVID-19 pandemic triggers 25% increase in prevalence of anxiety and depression worldwide. World Health Organization. Assessed march 26, 2023. https://www.who.int/news/item/02-03-2022-covid-19-pandemic-triggers-25-increase-in-prevalence-of-anxiety-and-depression-worldwide
[1] The critique of social media does not imply that there are no benefits. If used judiciously, it is a powerful tool to connect with family and friends or access information.
Mouth breathing and tongue position: a risk factor for health
Posted: June 8, 2023 Filed under: ADHD, behavior, Breathing/respiration, cognitive behavior therapy, Evolutionary perspective, healing, health, Nutrition/diet, self-healing, Uncategorized | Tags: babies, breastfeedging, development, infants, jaw, mouth breathing, neurocognitive develoment, nose breathing, sleep, tongue-tie Leave a commentErik Peper, PhD, BCB and Ron Swatzyna, PhD, LCSW, BCB, BCN
Adapted from: Peper, E., Swatzyna, R., & Ong, K. (2023). Mouth breathing and tongue position: a risk factor for health. Biofeedback. 51(3), 74–78 https://doi.org/10.5298/912512

Breathing usually occurs without awareness unless there are problems such as asthma, emphysema, allergies, or viral infections. Infant and child development may affect how we breathe as adults. This blog discusses the benefits of nasal breathing, factors that contribute to mouth breathing, how babies’ breastfeeding and chewing decreases the risk of mouth breathing, recommendations that parents may implement to support healthy development of a wider palate, and the embedded video presentation, How the Tongue Informs Healthy (or Unhealthy) Neurocognitive Development, by Karindy Ong, MA, CCC-SLP, CFT, .
Benefits of nasal breathing
Breathing through the nose filters, humidifies, warms, or cools the inhaled air as well as reduces the air turbulence in the upper airways. In addition, the epithelial cells of the nasal cavities produce nitric oxide that are carried into the lungs when inhaling during nasal breathing (Lundberg & Weitzberg, 1999). The nitric oxide contributes to healthy respiratory function by promoting vasodilation, aiding in airway clearance, exerting antimicrobial effects, and regulating inflammation. Breathing through the nose is associated with deeper and slower breathing rate than mouth breathing. This slower breathing also facilitates sympathetic parasympathetic balance and reduces airway irritation.
Mouth breathing
Some people breathe predominantly through their mouth although nose breathing is preferred and health promoting. Mouth breathing negatively impacts the ability to perform during the day as well as affect our cognitions and mood (Nestor, 2020). It contributes to disturbed sleep, snoring, sleep apnea, dry mouth upon waking, fatigue, allergies, ear infections, attention deficit disorders, crowded mis-aligned teeth, and poorer quality of life (Kahn & Ehrlich, 2018). Even the risk of ear infections in children is 2.4 time higher for mouth breathers than nasal breathers (van Bon et al, 1989) and nine and ten year old children who mouth breath have significantly poorer quality of life and have higher use of medications (Leal et al, 2016).
One recommendation to reduce mouth breathing is to tape the mouths closed with mouth tape (McKeown, 2021). Using mouth tape while sleeping bolsters nose breathing and may help people improve sleep, reduce snoring, and improves alertness when awake (Lee et al, 2022).
Experience how mouth breathing affects the throat and upper airway
Inhale quickly, like a gasp, as much air as possible through your open mouth. Exhale letting the air flow out through your mouth. Repeat once more.
Inhale quickly as much air through the nose, then exhale by allow the airflow out through the nose. Repeat once more.
What did you observe? Many people report that rapidly inhaling through the mouth causes the back of the throat and even upper airways to feel drier and irritated. This does not occur when inhaling through the nose. This simple experiment illustrates how habitual mouth breathing may irritate the airways.
Developmental behavior that contributes to mouth breathing
The development of mouth breathing may begin right at birth when the mouth, tongue, jaw and nasal area are still developing. The arch of the upper palate forms the roof of the oral cavity that separates the oral and nasal cavities. When the palate and jaw narrows, the arch of the palate increases and pushes upwards into the nasal area. This reduces space in the nasal cavity for the air to flow and obstructs nasal breathing. The highly vaulted palate is not only genetically predetermined but also by how we use our tongue and jaw from birth. The highly arched palate is only a recent anatomical phenomena since the physical structure of the upper palate and jaw from the pre- industrial era was wider (less arched upper palate) than many of our current skulls (Kahn & Ehrlich, 2018).
The role of the tongue in palate development
After babies are born, they breastfeed by sucking with the appropriate tongue movements that help widen the upper palate and jaw. On the other hand, when babies are bottle fed, the tongue tends to move differently which causes the cheek to pull in and the upper palate to arch which may create a high narrow upper palate and making the jaw narrower. There are many other possible factors that could cause mouth breathing such as tongue-tie (ankyloglossia), septal deviation, congenital malformation, enlarged adenoids and tonsils (Aden tonsillar hyperplasia), inflammatory diseases such as allergic rhinitis (Trabalon et al, 2012). Whatever the reasons, the result of the impoverished tongue movement and jaw increases the risk for having a higher arched upper palate that impedes nasal breathing and contributes to habitual mouth breathing.
The forces that operate on the mouth, jaw and palate during bottle feeding may be similar to when you suck on straw and the cheeks coming in with the face narrowing. The way the infants are fed will change the development of the physical structure that may result in lifelong problems and may contribute to developing a highly arched palate with a narrow jaw and facial abnormalities such as long face syndrome (Tourne, 1990).
To widen the upper palate and jaw, the infant needs to chew, chew and tear the food with their gums and teeth. Before the industrialization of foods, children had to tear food with their teeth, chew fibrous foods or gnaw at the meat on bones. The chewing forces allows the jaw to widen and develop so that when the permanent teeth are erupting, they would more likely be aligned since there would be enough space–eliminating the need for orthodontics. On the other hand, when young children eat puréed and highly processed soft foods (e.g., cereals soaked in milk, soft breads), the chewing forces are not powerful enough to encourage the widening of the palate and jaw.
Although the solution in adults can be the use of mouth tape to keep the mouth closed at night to retrain the breathing pattern, we should not wait until we have symptoms. The focus needs to be on prevention. The first step is an assessment whether the children’s tongue can do its job effectively or limited by tongue-tie and the arch of the palate. These structures are not totally fixed and can change depending on our oral habits. The field of orthodontics is based upon the premise that the physical structure of the jaw and palate can be changed, and teeth can be realigned by applying constant forces with braces.
Support healthy development of the palate and jaw
Breastfeed babies (if possible) for the first year of life and do NOT use bottle feeding. When weaning, provide chewable foods (fruits, vegetable, roots, berries, meats on bone) that was traditionally part of our pre-industrial diet. These foods support in infants’ healthy tongue and jaw development, which helps to support the normal widening of the palate to provide space for nasal breathing.
Provide fresh organic foods that children must tear and chew. Avoid any processed foods which are soft and do not demand chewing. This will have many other beneficial health effects since processed foods are high in simple carbohydrates and usually contain color additives as well as traces of pesticides and herbicides. The highly processed foods increase the risk of developing depression, type 2 diabetes, inflammatory disease, and colon cancer (Srour et al., 2019).
Sadly, the USA allows much higher residues of pesticide and herbicides that act as neurotoxins than are allowed in by the European Union. For example, the acceptable level of the herbicide glyphosate (Round-Up) is 0.7 parts per million in the USA while in the acceptable level is 0.01 parts per million in European countries (Tano, 2016; EPA, 2023; European Commission, 2023). The USA allows this higher exposure even though about half of the human gut microbiota are vulnerable to glyphosate exposure (Puigbò et al., 2022).
The negative effects of herbicides and pesticides are harmful for growing infants. Even fetal exposure from the mother (gestational exposure) is associated with an increase in behaviors related to attention-deficit/hyperactivity disorders and executive function in the child when they are 7 to 12 years old (Sagiv et al., 2021) and organophosphate exposure is correlated with ADHD prevalence in children (Bouchard et al., 2010).
To implement these basic recommendations are very challenging. It means the mother has to breastfeed her infant during the first year of life. This is often not possible because of socioeconomic inequalities; work demands and medical complications. It also goes against the recent cultural norm that fathers should participate in caring for the baby by giving the baby a bottle of stored breast milk or formula.
From our perspective, women who give birth must have a year paid maternity leave to provide their infants with the best opportunity for health (e.g., breast-feeding, emotional bonding, and reduced financial stress). As a society, we have the option to pay the upfront cost now by providing a year- long maternity leave to mothers or later pay much more costs for treating chronic conditions that may have developed because we did not support the natural developmental process of babies.
Relevance to the field of neurofeedback and biofeedback
Clinicians often see clients, especially children with diagnostic labels such as ADHD who have failed to respond to numerous psychotherapies and pharmacotherapies. In the recent umbrella review and meta-analytic evaluation of recent meta-analyses, Leichsenring et al. (2022) found only small benefits overall for both types of intervention. They suggest that a paradigm shift in research seems to be required to achieve further progress in resolving mental health issues. As the past director of National Institute of Health, Dr. Thomas Insel pointed out that the Diagnostic and Statistical Manual of Mental Disorders (DSM) is not a valid instrument and should be a big wake up call for all of us to think outside the box (Insel, 2009). One factor that starts right at birth is the oral cavity development by dysfunctional tongue movements.
We want to make all of you aware of a serious issue in children that you may come across. For those of us who work with children children, we need to ask their parents about the following: tongue-tie, mouth breathing, bedwetting, high-vaulted palate, thumb sucking, abnormal eating issues, apraxia, dysarthria, and hypotonia. Research suggests that the palates of these children are so arched that the tongue cannot do its job effectively, causing multiple issues which may be related.
Please view the webinar from May 17, 2023. Presented by Karindy Ong, MA, CCC-SLP, CFT, How the Tongue Informs Healthy (or Unhealthy) Neurocognitive Development. The presentation explains the developmental process of the role the tongue plays and how it contributes to nasal breathing. Please pass it on to others who may have interest.
References
Bouchard, M.F., Bellinger, D.C., Wright, R.O., & Weisskopf, M.G. (2010). Attention-deficit/hyperactivity disorder and urinary metabolites of organophosphate pesticides. Pediatrics, 125(6), e1270-7. https://doi.org/10.1542/peds.2009-3058
EPA. (2023). Glyphosate. United States Environmental Protection Agency. Accessed April 1, 2023. https://www.epa.gov/ingredients-used-pesticide-products/glyphosate
European Commission. (2023). EU legislation on MRLs.Food Safety. Assessed April 1, 2023. https://food.ec.europa.eu/plants/pesticides/maximum-residue-levels/eu-legislation-mrls_en#:~:text=A%20general%20default%20MRL%20of,e.g.%20babies%2C%20children%20and%20vegetarians.
Insel, T.R. (2009). Translating scientific opportunity into public health impact: a strategic plan for research on mental illness. Arch Gen Psychiatry, 66(2), 128-133. https://doi.org/10.1001/archgenpsychiatry.2008.540
Kahn, S. & Ehrlich, P.R. (2018). Jaws. Stanford, CA: Stanford University Press. https://www.amazon.com/Jaws-Hidden-Epidemic-Sandra-Kahn/dp/1503604136/ref=tmm_hrd_swatch_0?_encoding=UTF8&qid=1685135054&sr=1-1
Leal, R.B., Gomes, M.C., Granville-Garcia, A.F., Goes, P.S.A., & de Menezes, V.A. (2016). Impact of Breathing Patterns on the Quality of Life of 9- to 10-year-old Schoolchildren. American Journal of Rhinology & Allergy, 30(5):e147-e152. https://doi.org/10.2500/ajra.2016.30.4363
Lee, Y.C., Lu, C.T., Cheng, W.N., & Li, H.Y. (2022).The Impact of Mouth-Taping in Mouth-Breathers with Mild Obstructive Sleep Apnea: A Preliminary Study. Healthcare (Basel), 10(9), 1755. https://doi.org/10.3390/healthcare10091755
Leichsenring, F., Steinert, C., Rabung, S. and Ioannidis, J.P.A. (2022), The efficacy of psychotherapies and pharmacotherapies for mental disorders in adults: an umbrella review and meta-analytic evaluation of recent meta-analyses. World Psychiatry, 21: 133-145. https://doi.org/10.1002/wps.20941
Lundberg, J.O. & Weitzberg, E. (1999). Nasal nitric oxide in man. Thorax. (10):947-52. https://doi.org/10.1136/thx.54.10.947
McKeown, P. (2021). The Breathing Cure: Develop New Habits for a Healthier, Happier, and Longer Life. Boca Raton, Fl “Humanix Books. https://www.amazon.com/BREATHING-CURE-Develop-Healthier-Happier/dp/1630061972/
Nestor, J. (2020). Breath: The New Science of a Lost Art. New York: Riverhead Books. https://www.amazon.com/Breath/dp/0593191358/ref=tmm_pap_swatch_0?_encoding=UTF8&qid=1686191995&sr=8-1
Puigbò, P., Leino, L. I., Rainio, M. J., Saikkonen, K., Saloniemi, I., & Helander, M. (2022). Does Glyphosate Affect the Human Microbiota?. Life, 12(5), 707. https://doi.org/10.3390/life12050707
Sagiv, S.K., Kogut, K., Harley, K., Bradman, A., Morga, N., & Eskenazi, B. (2021). Gestational Exposure to Organophosphate Pesticides and Longitudinally Assessed Behaviors Related to Attention-Deficit/Hyperactivity Disorder and Executive Function, American Journal of Epidemiology, 190(11), 2420–2431. https://doi.org/10.1093/aje/kwab173
Srour, B. et al. (2019). Ultra-processed food intake and risk of cardiovascular disease: prospective cohort study (NutriNet-Santé).BMJ, 365. https://doi.org/10.1136/bmj.l1451
Tano, B. (2016). The Layman’s Guide to Integrative Immunity. Integrative Medical Press. https://www.amazon.com/Laymans-Guide-Integrative-Immunity-Discover/dp/0983419299/_
Tourne, L.P. (1990). The long face syndrome and impairment of the nasopharyngeal airway. Angle Orthod, 60(3):167-76. https://doi.org/10.1043/0003
Trabalon, M. & Schaal, B. (2012). It takes a mouth to eat and a nose to breathe: abnormal oral respiration affects neonates’ oral competence and systemic adaptation. Int J Pediatr, 207605. https://doi.org/10.1155/2012/207605
van Bon, M.J., Zielhuis, G.A., Rach, G.H., & van den Broek, P. (1989). Otitis media with effusion and habitual mouth breathing in Dutch preschool children. Int J Pediatr Otorhinolaryngol, (2), 119-25. https://doi.org/10.1016/0165-5876(89)90087-6
Healing from vulvodynia
Posted: May 4, 2023 Filed under: behavior, biofeedback, Breathing/respiration, emotions, healing, health, Pain/discomfort, relaxation, self-healing, Uncategorized | Tags: muscle tension, pelvic floor pain, therapeutic relationship, triggers for illness, vulvodynia 1 CommentPamela Jertberg and Erik Peper
Adapted from: Jertberg, P. & Peper, E. (2023). The healing of vulvodynia from the client’s perspective. Biofeedback, 51 (1), 18–21. https://doi.org/10.5298/1081-5937-51.01.02

This introspective report describes how a young woman who experienced a year-long struggle with vulvodynia, or vulvar vestibulitis, regained her health through biofeedback training and continues to be symptom-free 7 years after the intervention. This perspective may offer insight into factors that promote health and healing and provide an approach to reduce symptoms and promote health. The methodology of this case was described previously by Peper et al. (2015).
The Client’s Experience
I have been a healthy young woman my whole life. Growing up in a loving, dedicated family, I always ate home-cooked meals, went to bed at a reasonable time, and got plenty of exercise by playing with my family members and friends. I never once thought that at age 23 I might be at risk of undergoing vulvar surgery. There are many factors that contributed to the genesis of my vulvar pain, and many other factors that worsened this pain. Traditional medicine did not help me, and I did not find relief until I met my biofeedback practitioner, who taught me biofeedback. Through the many strategies I learned, such as visualization, diaphragmatic breathing techniques, diet tips, and skills to reframe my thoughts, I finally began to feel relief and hope. Practicing all these elements every day helped me overcome my physical pain and enjoy a normal life once again. Today, I do not have any vulvar discomfort. I am so grateful to my biofeedback practitioner for the many skills he taught me. I can enjoy my daily activities once again without experiencing pain. I have been given a second chance at loving life, and now I have learned the techniques that will help me sustain a more balanced path for the rest of my life. Seven years later, I am healthy and have no symptoms.
Triggers for Illness
Not Having a Positive Relationship with the Doctor
The first factor that aggravated my pain was having a doctor with whom I did not have a good relationship. Although the vulvar specialist I was referred to had treated hundreds of women with vulvar vestibulitis, his methods were very traditional: medicine, low oxalate diet, ointments, and surgery. Whenever I left his office, I would cry and feel like surgery was the only option. Vaginal surgery at 23 was one of the scariest and most unexpected thoughts my brain had ever considered. The doctor never thought of the impact that his words and treatment would have on my mental state.
Depression
Being depressed also triggered more pain. Whenever I would have feelings of hopelessness and create irrational beliefs in my mind (“I will never get better,” “I will never have sex again,” “I am not a woman anymore”), my physical pain would increase. Having depression only triggered more depression and pain, and this became a vicious cycle. The depression deeply affected my relationships with my boyfriend, friends, and family and my performance in my college classes.
Being Sedentary
Being sedentary and not exercising also increased my pain. At first, I believed that the mere act of sitting down hurt me due to the direct pressure on the area, but after a few months I came to realize that it was inactivity itself that triggered pain. Whenever I would sit for too long writing a paper or I would stay home all day because of my depression, my pain would increase, perhaps because I was inhibiting circulation. Still, when I am inactive most of the day, I feel lethargic and bloated. When I exercise, the pain goes away 100%. Exercise is almost magical.
Stress
Stress is the worst trigger for pain. Throughout my life, I always strived to be perfect in every way, meaning I was stressed about the way I looked, performed in school, drove, etc. Through the sessions with my biofeedback practitioner, I learned that my body was in a state of perpetual stress and tightness, which induced pain in certain areas. My body’s way of releasing such tension was to send pain signals to my vulvar area, perhaps because of a yeast infection a couple of months back. Still, if I become very stressed, I will feel pain or tightness in certain parts of my body, but now I have strategies for performing proper stress-relieving techniques.
Processed Foods
Junk food affects me instantly. When I eat processed foods for a week straight, I feel groggy, bloated, lethargic, and in pain. Processed sugar, white flour, and salt are a few of the foods that make the pain increase. I used to love sugar, so I would enjoy the occasional milkshake and cheeseburger and feel mostly okay. However, in times of stress it became crucial for me to learn to refrain from any junk food, because it would worsen my vulvar pain and increase my overall stress levels.
Menstruation
Menstruation is unavoidable, and unfortunately it would always worsen my vulvar pain. Right about the time of my period, my sensitivity and pain would massively increase. Sometimes as my pain would increase incredibly, I would question myself: “What am I doing wrong?” Then, I would remember: “Oh yes, I am getting my period in a few days.” The whole area became very sensitive and would get irritated easily. It became imperative to listen to my body and nurture myself especially around that time of the month.
Triggers for Healing
A Good Doctor
Just as I learned which factors triggered the pain, I also learned how to reduce it. The most important factor that helped me find true relief was meeting a good health professional (which could be a healer, nurse, or professor). The first time I met my biofeedback practitioner and told him about my issues, he really listened, gave me positive feedback, and even made jokes with me. To this day we still have a friendship, which has really aided me in getting better. In contrast to the vulvar specialist, I would leave the biofeedback practitioner’s office feeling powerful, able to defeat vulvodynia, and truly happy. Just having this support from a professional (or a friend, boyfriend, or relative) can make all the difference in the world. I don’t know where I would be right now if I hadn’t worked with him.
Positive Thoughts and Beliefs
Along with having a good support group, having positive thoughts and believing in a positive result helped me greatly. When I actually set my mind to feel “happy” and to believe that I was getting better, I began to really heal. After months of being depressed and feeling incomplete, when I began to practice mantras such as “I am healing,” “I am healthy,” and “I am happy,” my pain began to go away, and I was able to reclaim my life.
Journaling
One of the ways in which “happiness” became easier to achieve was to journal every day. I would write everything: from my secrets to what I ate, my pain levels, my goals for the day, and my symptoms. Writing down everything and knowing that no one would ever read it but me gave me relief, and my journal became my confidante. I still journal every day, and if I forget to write, the next day I will write twice as much. Now that writing has become a habit and a hobby, it is hard to imagine my life without that level of introspection.
Meditation
Although I would do yoga often, I would never sit and meditate. I began to use Dr. Peper’s guided meditations and Dr. Kabat-Zinn’s CD (Kabat-Zinn, 2006; Peper et al., 2002). The combination of these meditation techniques, whether on different days or on the same day, helped me focus on my breathing and relax my muscles and mind. Today, I meditate at least 20 min each day, and I feel that it helps me see life through a more willing and patient perspective. In addition, through meditation and deep breathing I have learned to control my pain levels, concentration, and awareness.
Imagery and Visualization
Imagery is a powerful tool that allowed me to heal faster. My biofeedback practitioner instructed me to visualize how I wanted to feel and look. In addition, he suggested that I draw and color how I was feeling at any given moment, my imagined healing process, and how I would look and feel after the healing process had traveled throughout my body (Peper et al., 2022). It is still amazing to me how much imagery helped me. Even visualizing here and there throughout the day helped. Now I envision how I want to feel as a healthy woman, I take a deep breath, and as a I breathe out I let my imagined healing process go through my body into all my tight areas along with the exhalation.
Biofeedback
Biofeedback is the single strategy that helped me the most. During my first session with my biofeedback practitioner, he pointed out that my muscles were always contracted and stressed and that I was not breathing diaphragmatically. As I learned how to take deep belly breaths, I began to feel the tight areas in my body loosen up. I started to practice controlled breathing 20 min every day. Through biofeedback, my body and muscles became more relaxed, promoting circulation and ultimately reducing the vulvar pain.
Regular Exercise and Yoga
Exercising daily decreased my pain and improved the quality of my life greatly. When I first started experiencing significant vulvar pain, I stopped exercising because I felt that movement would aggravate the pain. To my surprise, the opposite was true. Being sedentary increased the feelings of discomfort, whereas exercising released the tension. The exercise I found most helpful was yoga because it is meditation in movement. I became so focused on my breathing and the poses that my brain did not have time to think about anything else. After attending every yoga class, I felt like I could take on anything. Swimming, Pilates, and gentle cardiovascular exercises have also helped me greatly in reducing stress and feeling great.
Sex
Although sex was impossible for almost a year due to the pain, it became possible and even enjoyable after implementing other relaxation strategies. When I first reintroduced sex back into my life, my partner at the time and I would go gently and stop if it hurt my vulvar area at all. Today, sex again is joyful. Being able to engage in intercourse has boosted my self-esteem and helped me feel sexy again, which empowers me to keep practicing the relaxation techniques.
Listening to the Mind-Body Connection
The mind-body connection is present in all of us, but I am fortunate to have a very strong connection. My thoughts influence my body almost instantly, which is why when I would get depressed my pain would increase, and when I would see my biofeedback practitioner or believe in a good outcome, my pain would decrease. Being aware of this connection is crucial because it can help me or hurt me greatly. After a few months of practicing the relaxation strategies, I saw a different gynecologist and one dermatologist. Both professionals said that there was nothing wrong with my vulvar area—that maybe I just felt some irritation due to the medicines I had previously taken and my current stress. They said that there was no way I needed surgery. When I heard these opinions, I began to feel instantly better—thus proving that my thoughts (and even others’ thoughts) affect my body in significant ways.
Although today I am 100% better, I still experience pain and tightness in my body when I experience the “illness factors” I mentioned above. I still have to remember that feeling healthy and good is a process, not a result, and that even if I feel better one day that does not mean I can stop all my new healthy habits. To completely cure vulvodynia, I needed to change my life habits, perspective, and attitude toward the illness and life. I needed to make significant changes, and now my biggest challenge is to stick to those changes. Biofeedback, imagery, meditation, good food, and exercise are not just treatments that I begin and end on a certain day, but rather they have become essential components of my life forever.
My life with vulvodynia was ultimately a journey of introspection, decision making, and life-changing habits. I struggled with vulvar pain for over a year, and during that year I experienced severe symptoms, depression, and the loss of several friendships and relationships. I felt old, hopeless, useless, and powerless. When I began to incorporate biofeedback, relaxation techniques, journaling, visualization, a proper diet, and regular exercise, life took a turn for the better. Not only did my vulvar pain begin to decrease, but the quality of my overall life improved and I regained the self-confidence I had lost. I became happy, hopeful, and proactive. Even though I practiced the relaxation strategies every day, the pain did not go away in a day or even a month. It took me several months of diligent practice to truly heal my vulvar pain. Even today, such practices have carried on to all areas of my life, and now there is not a day when I do not meditate, even for 5 min.
As paradoxical as it may seem, vulvodynia was a blessing in disguise. I believe that vulvodynia was my body’s way of signaling to me that many areas of my life were in perpetual stress: my pelvic floor, my thoracic breathing, my romantic relationship at the time, etc. When I learned to let go and truly embrace my life, I began to feel relief. I became less irritable and more patient and understanding, with both my body and the outside world. The best advice I can give a woman with vulvar symptoms or any person with otherwise inexplicable chronic pain is to apply the strategies that work for you and stick to them every day—even on the days when you want to go astray. When I started to focus on what my body needed to be nurtured and to live my life and do the things I truly wanted to do, I became free. Today, I live in a way that allows me to find peace, serenity, pride, and fun. I live exactly the way I want to, and I find the time to follow my passions. Vulvodynia, or any kind of chronic pain, does not define who we are. We define who we are.
Conclusion
This introspective account of the client’s personal experience with biofeedback suggests that healing is multidimensional. We suggest that practitioners use a holistic approach, which can provide hope and relief to clients who suffer from vulvodynia or other disorders that are often misunderstood and underreported.
Useful blogs
References
Kabat-Zinn, J. (2006). Coming to our senses: Healing ourselves and the world through mindfulness. Hachette Books
Peper, E., Cosby, J. & Almendras, M. (2022). Healing chronic back pain. NeuroRegulation, 9(3), 164–172. https://doi.org/10.15540/nr.9.3.164
Peper, E., Gibney, K.H, & Holt, C.F. (2002. Make health happen: Training yourself to create wellness. Kendall/Hunt.
Peper, E. Martinex, Aranda, P. & Moss, D. (2015). Vulvodynia treated successfully with breathing biofeedback and integrated stress reduction: A case report. Biofeedback, 43(2), 103–109. https://doi.org/10.5298/1081-5937-43.2.04
Hope for menstrual cramps (dysmenorrhea) with breathing
Posted: April 22, 2023 Filed under: behavior, biofeedback, Breathing/respiration, healing, health, meditation, Pain/discomfort, posture, relaxation, self-healing, stress management, Uncategorized | Tags: dysmenorrhea, Imagery, menstrual cramps, stroking, visualization 6 CommentsAdapted from: Peper, E., Chen, S., Heinz, N., & Harvey, R. (2023). Hope for menstrual cramps (dysmenorrhea) with breathing. Biofeedback, 51(2), 44–51. https://doi.org/10.5298/1081-5937-51.2.04; Republished in Townsend E-Letter – 18 November, 2023 https://www.townsendletter.com/e-letter-22-breath-affects-stress-and-menstrual-cramps/ Google NotebookLM generated podcast:

“I have always had extremely painful periods. They would get so painful that I would have to call in sick and take some time off from school. I have been to many doctors and medical professionals, and they told me there is nothing I could do. I am currently on birth control, and I still get some relief from the menstrual pain, but it would mess up my moods. I tried to do the diaphragmatic breathing so that I would be able to continue my life as a normal woman. And to my surprise it worked. I was simply blown away with how well it works. I have almost no menstrual pain, and I wouldn’t bloat so much after the diaphragmatic breathing.” -22 year old student
Each semester numerous students report that their cramps and dysmenorrhea symptoms decrease or disappear during the semester when they implement the relaxation and breathing practices that are taught in the semester long Holistic Health class. Given that so many young women suffer from dysmenorrhea, many young women could benefit by using this integrated approach as the first self-care intervention before relying on pain reducing medications or hormones to reduce pain or inhibit menstruation. Another 28-year-old student reported:
“Historically, my menstrual cramps have always required ibuprofen to avoid becoming distracting. After this class, I started using diaphragmatic breath after pain started for some relief. True benefit came when I started breathing at the first sign of discomfort. I have not had to use any pain medication since incorporating diaphragmatic breath work.”
This report describes students practicing self-regulation and effortless breathing to reduce stress symptoms, explores possible mechanisms of action, and suggests a protocol for reducing symptoms of menstrual cramps. Watch the short video how diaphragmatic breathing eliminated recurrent severe dysmenorrhea (pain and discomfort associated with menstruation).
Background: What is dysmenorrhea?
Dysmenorrhea is one of the most common conditions experienced by women during menstruation and affects more than half of all women who menstruate (Armour et al., 2019). Most commonly dysmenorrhea is defined by painful cramps in the lower abdomen often accompanied by pelvic pain that starts either a couple days before or at the start of menses. Symptoms also increase with stress (Wang et al., 2003) with pain symptoms usually decreasing in severity as women get older and, after pregnancy.
Economic cost of dysmenorrhea
Dysmenorrhea can significantly interfere with a women’s ability to be productive in their occupation and/or their education. It is “one of the leading causes of absenteeism from school or work, translating to a loss of 600 million hours per year, with an annual loss of $2 billion in the United States” (Itani et al, 2022). For students, dysmenorrhea has a substantial detrimental influence on academic achievement in high school and college (Thakur & Pathania, 2022). Despite the frequent occurrence and negative impact in women’s lives, many young women struggle without seeking or having access to medical advice or, without exploring non-pharmacological self-care approaches (Itani et al, 2022).
Treatment
The most common pharmacological treatments for dysmenorrhea are nonsteroidal anti-inflammatory drugs (NSAIDs) (e.g., Ibuprofen, Aspirin, and Naproxen Sodium) along with hormonal contraceptives. NSAIDs act by preventing the action of cyclooxygenase which prevents the production of prostaglandins. Itani et al (2022) suggested that prostaglandin production mechanisms may be responsible for the disorder. Hormonal contraceptives also prevent the production of prostaglandins by suppressing ovulation and endometrial proliferation.
The pharmacological approach is predominantly based upon the model that increased discomfort appears to be due to an increase in intrauterine secretion of prostaglandins F2α and E2 that may be responsible for the pain that defines this condition (Itani et al, 2022). Pharmaceuticals which influence the presence of prostaglandins do not cure the cause but mainly treat the symptoms.
Treatment with medications has drawbacks. For example, NSAIDs are associated with adverse gastrointestinal and neurological effects and also are not effective in preventing pain in everyone (Vonkeman & van de Laar, 2010). Hormonal contraceptives also have the possibility of adverse side effects (ASPH, 2023). Acetaminophen is another commonly used treatment; however, it is less effective than other NSAID treatments.
Self-regulation strategies to reduce stress and influence dysmenorrhea
Common non-pharmacological treatments include topical heat application and exercise. Both non-medication approaches can be effective in reducing the severity of pain. According to Itani et al. (2022), the success of integrative holistic health treatments can be attributed to “several mechanisms, including increasing pelvic blood supply, inhibiting uterine contractions, stimulating the release of endorphins and serotonin, and altering the ability to receive and perceive pain signals.”
Although less commonly used, self-regulation strategies can significantly reduce stress levels associated menstrual discomfort as well as reduce symptoms. More importantly, they do not have adverse side effects, but the effectiveness of the intervention varies depending on the individual.
- Autogenic Training (AT), is a hundred year old treatment approach developed by the German psychiatrist Johannes Heinrich Schultz that involves three 15 minute daily practice of sessions, resulted in a 40 to 70 percent decrease of symptoms in patient suffering from primary and secondary dysmenorrhea (Luthe & Schultz, 1969). In a well- controlled PhD dissertation, Heczey (1978) compared autogenic training taught individually, autogenic training taught in a group, autogenic training plus vaginal temperature training and a no treatment control in a randomized controlled study. All treatment groups except the control group reported a decrease in symptoms and the most success was with the combined autogenic training and vaginal temperature training in which the subjects’ vaginal temperature increased by .27 F degrees.
- Progressive muscle relaxation developed by Edmund Jacobson in the 1920s and imagery are effective treatments for dysmenorrhea (Aldinda et al., 2022; Chesney & Tasto, 1975; Çelik, 2021; Jacobson, 1938; Proctor et al., 2007).
- Rhythmic abdominal massage as compared to non-treatment reduces dysmenorrhea symptoms (Suryantini, 2022; Vagedes et al., 2019):
- Biofeedback strategies such as frontalis electromyography feedback (EMG) and peripheral temperature training (Hart, Mathisen, & Prater, 1981); trapezius EMG training (Balick et al, 1982); lower abdominal EMG feedback training and relaxation (Bennink, Hulst, & Benthem, 1982); and integrated temperature feedback and autogenic training (Dietvorts & Osborne, 1978) all successfully reduced the symptoms of dysmenorrhea.
- Breathing relaxation for 5 to 30 minutes resulted in a decrease in pain or the pain totally disappeared in adolescents (Hidayatunnafiah et al., 2022). While slow deep breathing in combination with abdominal massage is more effective than applying hot compresses (Ariani et al., 2020). Slow pranayama (Nadi Shodhan) breathing the quality of life and pain scores improved as compared to fast pranayama (Kapalbhati) breathing and improved quality of life and reduces absenteeism and stress levels (Ganesh et al. 2015). When students are taught slow diaphragmatic breathing, many report a reduction in symptoms compared to the controls (Bier et al., 2005).
Observations from Integrated stress management program
This study reports on changes in dysmenorrhea symptoms by students enrolled in a University Holistic Health class that included homework assignment for practicing stress awareness, dynamic relaxation, and breathing with imagery.
Respondents: 32 college women, average age 24.0 years (S.D. 4.5 years)
Procedure: Students were enrolled in a three-unit class in which they were assigned daily home practices which changed each week as described in the book, Make Health Happen (Peper, Gibney & Holt, 2002). The first five weeks consisted of the following sequence: Week 1 focused on monitoring one’s reactions to stressor; week 2 consisted of daily practice for 30 minutes of a modified progressive relaxation and becoming aware of bracing and reducing the bracing during the day; Week 3 consisted of practicing slow diaphragmatic breathing for 30 minutes a day and during the day becoming aware of either breath holding or shallow chest breath and then use that awareness as cue to shift to lower slower diaphragmatic breathing; week 4 focused on evoking a memory of wholeness and relaxing; and week 5 focused on learning peripheral hand warming.
During the class, students observed lectures about stress and holistic health and met in small groups to discuss their self-regulation experiences. During the class discussion, some women discussed postures and practices that were beneficial when experiencing menstrual discomfort, such as breathing slowly while lying on their back, focusing on slow abdominal awareness in which their abdomen expanded during inhalation and contracted during exhalation. While exhaling they focused on imagining a flow of air initially going through their arms and then through their abdomen, down their legs and out their feet. This kinesthetic feeling was enhanced by first massaging down the arm while exhaling and then massaging down their abdomen and down their thighs when exhaling. In most cases, the women also experienced that their hands and feet warmed. In addition, they were asked to shift to slower diaphragmatic breathing whenever they observed themselves gasping, shallow breathing or holding their breath. After five weeks, the students filled out a short assessment questionnaire in which they rated the change in dysmenorrhea symptoms since the beginning of the class.
Results.
About two-thirds of all respondents reported a decrease in overall discomfort symptoms. In addition to any ‘treatment as usual’ (TAU) strategies already being used (e.g. medications or other treatments such as NSAIDs or birth control pills), 91% (20 out 22 women) who reported experiencing dysmenorrhea reported a decrease in symptoms when they practiced the self-regulation and diaphragmatic breathing techniques as shown in Figure 1.

Figure 1. Self-report in dysmenorrhea symptoms after 5 weeks.
Discussion
Many students reported that their symptoms were significantly reduced and they could be more productive. Generally, the more they practiced the relaxation and breathing self-regulation skills, the more they experienced a decrease in symptoms. The limitation of this report is that it is an observational study; however, the findings are similar to those reported by earlier self-care and biofeedback approaches. This suggests that women should be taught the following simple self-regulation strategies as the first intervention to prevent and when they experience dysmenorrhea symptoms.
Why would breathing reduce dysmenorrhea?
Many women respond by ‘curling up’ a natural protective defense response when they experience symptoms. This protective posture increases abdominal and pelvic muscle tension, inhibits lymph and blood flow circulation, increases shallow breathing rate, and decreases heart rate variability. Intentionally relaxing the abdomen with slow lower breathing when lying down with the legs extended is often the first step in reducing discomfort.
By focusing on diaphragmatic breathing with relaxing imagery, it is possible to restore abdominal expansion during inhalation and slight constriction during exhalation. This dynamic breathing while lying supine would enhance abdominal blood and lymph circulation as well as muscle relaxation (Peper et al., 2016). While practicing, participants were asked to wear looser clothing that did not constrict the waist to allow their abdomen to expand during inhalation; since, waist constriction by clothing (designer jean syndrome) interferes with abdominal expansion. Allowing the abdomen to fully extend also increased acceptance of self, that it was okay to let the abdomen expand instead of holding it in protectively. The symptoms were reduced most likley by a combination of the following factors.
- Abdominal movement is facilitated during the breathing cycle. This means reducing the factors that prevent the abdomen expanding during inhalation or constricting during exhalation (Peper et al., 2016).
- Eliminate‘Designer jean syndrome’ (the modern girdle). Increase the expansion of your abdomen by loosening the waist belt, tight pants or slimming underwear (MacHose & Peper, 1991).
- Accept yourself as you are. Allow your stomach to expand without pulling it in.
- Free up learned disuse: Allow the abdomen to expand and constrict instead of inhibiting movement to avoid pain that occurred following a prior abdominal injury/surgery (e.g., hernia surgery, appendectomy, or cesarean operation), abdominal pain (e.g., irritable bowel syndrome, recurrent abdominal pain, ulcers, or acid reflux), pelvic floor pain (e.g., pelvic floor pain, pelvic girdle pain, vulvodynia, or sexual abuse).
- The ‘defense response’ is reduced. Many students described that they often would curl up in a protective defense posture when experiencing menstrual cramps. This protective defense posture would maintain pelvic floor muscle contractions and inhibit blood and lymph flow in the abdomen, increase shallow rapid thoracic breathing and decrease pCO2 which would increase vasoconstriction and muscle constriction (Peper et al., 2015; Peper et al., 2016). By having the participant lie relaxed in a supine position with their legs extended while practicing slow abdominal breathing, the pelvic floor and abdominal wall muscles can relax and thereby increase abdominal blood and lymph circulation and parasympathetic activity. The posture of lying down implies feeling safe which is a state that facilitates healing.
- The pain/fear cycle is interrupted. The dysmenorrhea symptoms may trigger more symptoms because the person anticipates and reacts to the discomfort. The breathing and especially the kinesthetic imagery where the attention goes from the abdomen and area of discomfort to down the legs and out the feet acts as a distraction technique (not focusing on the discomfort).
- Support sympathetic-parasympathetic balance. The slow breathing and kinesthetic imagery usually increases heart rate variability and hand and feet temperature and supports sympathetic parasympathetic balance.
- Interrupt the classical conditioned response of the defense reaction. For some young girls, the first menstruation occurred unexpectedly. All of a sudden, they bled from down below without any understanding of what is going on which could be traumatic. For some this could be a defense reaction and a single trial condition response (somatic cues of the beginning of menstruation triggers the defense reaction). Thus, when the girl later experiences the initial sensations of menstruation, the automatic conditioned response causes her to tense and curl up which would amplify the discomfort. Informal interviews with women suggests that those who experienced their first menstruation experience as shameful, unexpected, or traumatic (“I thought I was dying”) thereafter framed their menstruation negatively. They also tended to report significantly more symptoms than those women who reported experiencing their first menstruation positively as a conformation that they have now entered womanhood.
How to integrate self-care to reduce dysmenorrhea
Be sure to consult your healthcare provider to rule out treatable underlying conditions before implementing learning effortless diaphragmatic breathing.
- Allow the abdomen to expand during inhalation and become smaller during exhalation. This often means, loosen belt and waist constriction, acceptance of allowing the stomach to be larger and reversing learned disuse and protective response caused by stress.
- Master diaphragmatic breathing (see: Peper & Tibbetts, 1994 and the blogs listed at the end of the article).
- Practice slow effortless diaphragmatic breathing lying down with warm water bottle on stomach in a place that feels safe.
- Include kinesthetic imagery as you breathe at about 6 breaths per minute (e.g. slowly inhale for 4 or 5 seconds and then exhale for 5 or 6 seconds, exhaling slightly longer than inhaling). Imaging that when you exhale you can sense healing energy flow through your abdomen, down the legs and out the feet.
- If possible, integrate actual touch with the exhalation can provide added benefit. Have a partner first stroke or massage down the arms from the shoulder to your fingertips as you exhale and, then on during next exhalation stroke gently from your abdomen down your legs and feet. Stroke in rhythm the exhalation.
- Exhale slowly and shift to slow and soft diaphragmatic breathing each time you become aware of neck and shoulder tension, breath holding, shallow breathing, or anticipating stressful situations. At the same time imagine /sense when exhaling a streaming going through the abdomen and out the feet when exhaling. Do this many times during the day.
- Practice and apply general stress reduction skills into daily life since stress can increase symptoms. Anticipate when stressful event could occur and implement stress reducing strategies.
- Be respectful of the biological changes that are part of the menstrual cycle. In some cases adjust your pace and slow down a bit during the week of the menstrual cycle; since, the body needs time to rest and regenerate. Be sure to get adequate amount of rest, hydration, and nutrition to optimize health.
- Use self-healing imagery and language to transform negative association with menstruation to positive associations (e.g., “curse” to confirmation “I am healthy”).
Conclusion
There are many ways to alleviate dysmenorrhea. Women can find ways to anticipate and empower themselves by practicing stress reduction, wearing more comfortable clothing, using heat compression, practicing daily diaphragmatic breathing techniques, visualizing relaxed muscles, and positive perception towards menstrual cycles to reduce the symptoms of dysmenorrhea. These self-regulation methods should be taught as a first level intervention to all young women starting in middle and junior high school so that they are better prepared for the changes that occur as they age.
“I have been practicing the breathing techniques for two weeks prior and I also noticed my muscles, in general, are more relaxed. Of course, I also avoided the skinny jeans that I like to wear and it definitely helped.
I have experienced a 90% improvement from my normal discomfort. I was still tired – and needed more rest and sleep but haven’t experienced any “terrible” physical discomfort. Still occasionally had some sharp pains or bloating but minor discomfort, unlike some days when I am bedridden and unable to move for half a day. – and this was a very positive experience for me “ — Singing Chen (Chen, 2023)
Useful blogs to learn diaphragmatic breathing
References
Aldinda, T. W., Sumarni, S., Mulyantoro, D. K., & Azam, M. (2022). Progressive muscle relaxation application (PURE App) for dysmenorrhea. Medisains Jurnal IlmiahLlmiah LLmu-LLmu Keshatan, 20(2), 52-57. https://doi.org/10.30595/medisains.v20i2.14351
Ariani, D., Hartiningsih, S.S., Sabarudin, U. Dane, S. (2020). The effectiveness of combination effleurage massage and slow deep breathing technique to decrease menstrual pain in university students. Journal of Research in Medical and Dental Science, 8(3), 79-84. https://www.jrmds.in/articles/the-effectiveness-of-combination-effleurage-massage-and-slow-deep-breathing-technique-to-decrease-menstrual-pain-in-university-stu-53607.html
Armour, M., Parry, K., Manohar, N., Holmes, K., Ferfolja, T., Curry, C., MacMillan, F., & Smith, C. A. (2019). The prevalence and academic impact of dysmenorrhea in 21,573 young women: a systematic review and meta-analysis. Journal of women’s health, 28(8), 1161-1171.https://doi.org/10.1089/jwh.2018.7615
ASPH. (2023). Estrogen and Progestin (Oral Contraceptives). MedlinePlus. Assessed March 3, 2023. https://medlineplus.gov/druginfo/meds/a601050.html
Balick, L., Elfner, L., May. J., Moore, J.D. (1982). Biofeedback treatment of dysmenorrhea. Biofeedback Self Regul, 7(4), 499-520. https://doi.org/10.1007/BF00998890
Bennink, C.D., Hulst, L.L. & Benthem, J.A. (1982). The effects of EMG biofeedback and relaxation training on primary dysmenorrhea. J Behav Med, 5(3), 329-341.https://doi.org/10.1007/BF00846160
Bier, M., Kazarian, D. & Peper, E. (2005). Reducing PMS through biofeedback and breathing. Poster presentation at the 36th Annual Meeting of the Association for Applied Psychophysiology and Biofeedback. Abstract published in: Applied Psychophysiology and Biofeedback. 30 (4), 411-412.
Çelik, A.S. & Apay, S.E. (2021). Effect of progressive relaxation exercises on primary dysmenorrhea in Turkish students: A randomized prospective controlled trial. Complement Ther Clin Pract, Feb 42,101280. https://doi.org/10.1016/j.ctcp.2020.101280
Chen, S. (2023). Diaphragmatic breathing reduces dysmenorrhea symptoms-a testimonial. YouTube. Accessed March 3, 2023. https://youtu.be/E45iGymVe3U
De Sanctis, V., Soliman, A., Bernasconi, S., Bianchin, L., Bona, G., Bozzola, M., Buzi, F., De Sanctis, C., Tonini, G., Rigon, F., & Perissinotto, E. (2015). Primary Dysmenorrhea in Adolescents: Prevalence, Impact and Recent Knowledge. Pediatr Endocrinol Rev. 13(2), 512-20. PMID: 26841639. https://pubmed.ncbi.nlm.nih.gov/26841639/
De Sanctis, V., Soliman, A. T., Daar, S., Di Maio, S., Elalaily, R., Fiscina, B., & Kattamis, C. (2020). Prevalence, attitude and practice of self-medication among adolescents and the paradigm of dysmenorrhea self-care management in different countries. Acta Bio Medica: Atenei Parmensis, 91(1), 182. https://doi.org/10.23750/abm.v91i1.9242
Dietvorst, T.F. & Osborne, D. (1978). Biofeedback-Assisted Relaxation Training
for Primary Dysmenorrhea: A Case Study. Biofeedback and Self-Regulation, 3(3), 301-305. https://doi.org/10.1007/BF00999298
Chesney, M. A., & Tasto, D. L. (1975).The effectiveness of behavior modification with spasmodic and congestive dysmenorrhea. Behaviour Research and Therapy, 13, 245-253. https://doi.org/10.1016/0005-7967(75)90029-7
Ganesh, B.R., Donde, M.P., & Hegde, A.R. (2015). Comparative study on effect of slow and fast phased pranayama on quality of life and pain in physiotherapy girls with primary dysmenorrhea: Randomize clinical trial. International Journal of Physiotherapy and Research, 3(2), 960-965. https://doi.org/10.16965/ijpr.2015.115
Hart, A.D., Mathisen, K.S. & Prater, J.S. A comparison of skin temperature and EMG training for primary dysmenorrhea. Biofeedback and Self-Regulation 6, 367–373 (1981). https://doi.org/10.1007/BF01000661
Heczey, M. D. (1978). Effects of biofeedback and autogenic training on menstrual experiences: relationship among anxiety, locus of control and dysmenorrhea. City University of New York ProQuest Dissertations Publishing, 7805763. https://www.proquest.com/openview/088e0d68511b5b59de1fa92dec832cc8/1?pq-origsite=gscholar&cbl=18750&diss=y
Hidayatunnafiah, F., Mualifah, L., Moebari, M., & Iswantiningsih, E. (2022). The Effect of Relaxation Techniques in Reducing Dysmenorrhea in Adolescents. The International Virtual Conference on Nursing. in The International Virtual Conference on Nursing, KnE Life Sciences, 473–480. https://doi.org/10.18502/kls.v7i2.10344
Itani, R., Soubra, L., Karout, S., Rahme, D., Karout, L., & Khojah, H.M.J. (2022). Primary Dysmenorrhea: Pathophysiology, Diagnosis, and Treatment Updates. Korean J Fam Med, 43(2), 101-108. https://doi.org/10.4082/kjfm.21.0103
Jacobson, E. (1938). Progressive Relaxation: A Physiological and Clinical Investigation of Muscular States and Their Significance in Psychology and Medical Practice. Chicago: University of Chicago Press
Ju, H., Jones, M., & Mishra, G. (2014). The prevalence and risk factors of dysmenorrhea. Epidemiol Rev, 36, 104-13. https://doi.org/10.1093/epirev/mxt009
Karout, S., Soubra, L., Rahme, D. et al. Prevalence, risk factors, and management practices of primary dysmenorrhea among young females. BMC Women’s Health 21, 392 (2021). https://doi.org/10.1186/s12905-021-01532-w
Iacovides, S., Avidon,I, & Baker, F.C. (2015).What we know about primary dysmenorrhea today: a critical review, Human Reproduction Update, 21(6), 762–778. https://doi.org/10.1093/humupd/dmv039
Luthe, W. & Schultz, J.H. (1969). Autogenic Therapy, Volume II Medical Applications. New York: Grune & Stratton, pp144-148.
MacHose, M. & Peper, E. (1991). The effect of clothing on inhalation volume. Biofeedback and Self-Regulation, 16(3), 261–265. https://doi.org/10.1007/BF01000020
Peper, E., Booiman, A., Lin, I-M, Harvey, R., & Mitose, J. (2016). Abdominal SEMG Feedback for Diaphragmatic Breathing: A Methodological Note. Biofeedback. 44(1), 42-49. https://doi.org/10.5298/1081-5937-44.1.03
Peper, E., Gibney, H. K. & Holt, C. (2002). Make Health Happen. Dubuque, Iowa: Kendall-Hunt. ISBN: 978-0787293314 https://he.kendallhunt.com/make-health-happen
Peper, E., Gilbert, C.D., Harvey, R. & Lin, I-M. (2015). Did you ask about abdominal surgery or injury? A learned disuse risk factor for breathing dysfunction. Biofeedback. 34(4), 173-179. https://doi.org/10.5298/1081-5937-43.4.06
Peper, E. & Tibbetts, V. (1994). Effortless diaphragmatic breathing. Physical Therapy Products. 6(2), 67-71. Also in: Electromyography: Applications in Physical Therapy. Montreal: Thought Technology Ltd. https://biofeedbackhealth.files.wordpress.com/2011/01/peper-and-tibbets-effortless-diaphragmatic.pdf
Proctor, M. & Farquhar, C. (2006). Diagnosis and management of dysmenorrhoea. BMJ. 13, 332(7550), 1134-8. https://doi.org/10.1136/bmj.332.7550
Proctor, M.L, Murphy, P.A., Pattison, H.M., Suckling, J., & Farquhar, C.M. (2007). Behavioural interventions for primary and secondary dysmenorrhoea. Cochrane Database Syst Rev, (3):CD002248. https://doi.org/10.1002/14651858.CD002248.pub3
Suryantini, N. P. (2022). Effleurage Massage: Alternative Non-Pharmacological Therapy in Decreasing Dysmenorrhea Pain. Women, Midwives and Midwifery, 2(3), 41-50. https://wmmjournal.org/index.php/wmm/article/view/71/45
Thakur, P. & Pathania, A.R. (2022). Relief of dysmenorrhea – A review of different types of pharmacological and non-pharmacological treatments. MaterialsToday: Proceedings.18, Part 5, 1157-1162. https://doi.org/10.1016/j.matpr.2021.08.207
Vagedes, J., Fazeli, A., Boening, A., Helmert, E., Berger, B. & Martin, D. (2019). Efficacy of rhythmical massage in comparison to heart rate variability biofeedback in patients with dysmenorrhea—A randomized, controlled trial. Complementary Therapies in Medicine, 42, 438-444. https://doi.org/10.1016/j.ctim.2018.11.009
Vonkeman, H.E. & van de Laar, M,A. (2010). Nonsteroidal anti-inflammatory drugs: adverse effects and their prevention, Semin Arthritis Rheum, 39(4), 294-312. https://doi.org/10.1016/j.semarthrit.2008.08.001
Wang, L., Wand, X., Wang, W., Chen, C. Ronnennberg, A.G., Guang, W. Huang, A. Fang, Z. Zang, T., Wang, L. & Xu, X. (2003).Stress and dysmenorrhoea: a population based prospective study. Occupation and Environmental Medicine, 61(12). http://dx.doi.org/10.1136/oem.2003.012302

{kind=link}
{kind=link}
{kind=link}
{kind=link}